
Longitudinal Changes and Predictive Value of Multiparametric MRI Features for Prostate Cancer Patients Treated with MRI-Guided Lattice Extreme Ablative Dose (LEAD) Boost Radiotherapy

Abstract
Simple Summary
Abstract
1. Introduction
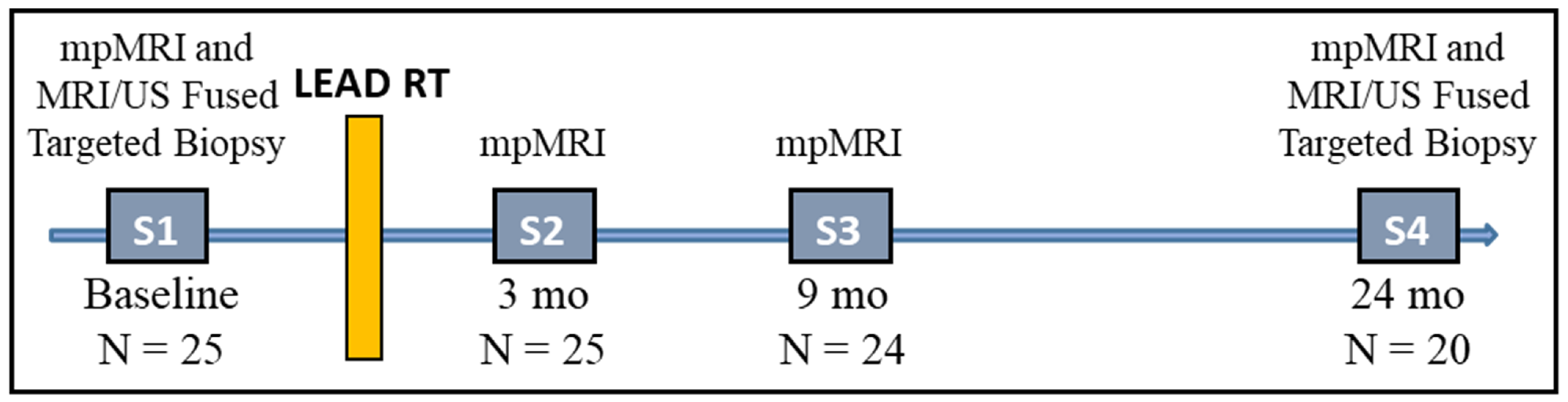
2. Materials and Methods
2.1. Patients
2.2. MpMRI Acquisition
2.3. Endpoint Biopsy
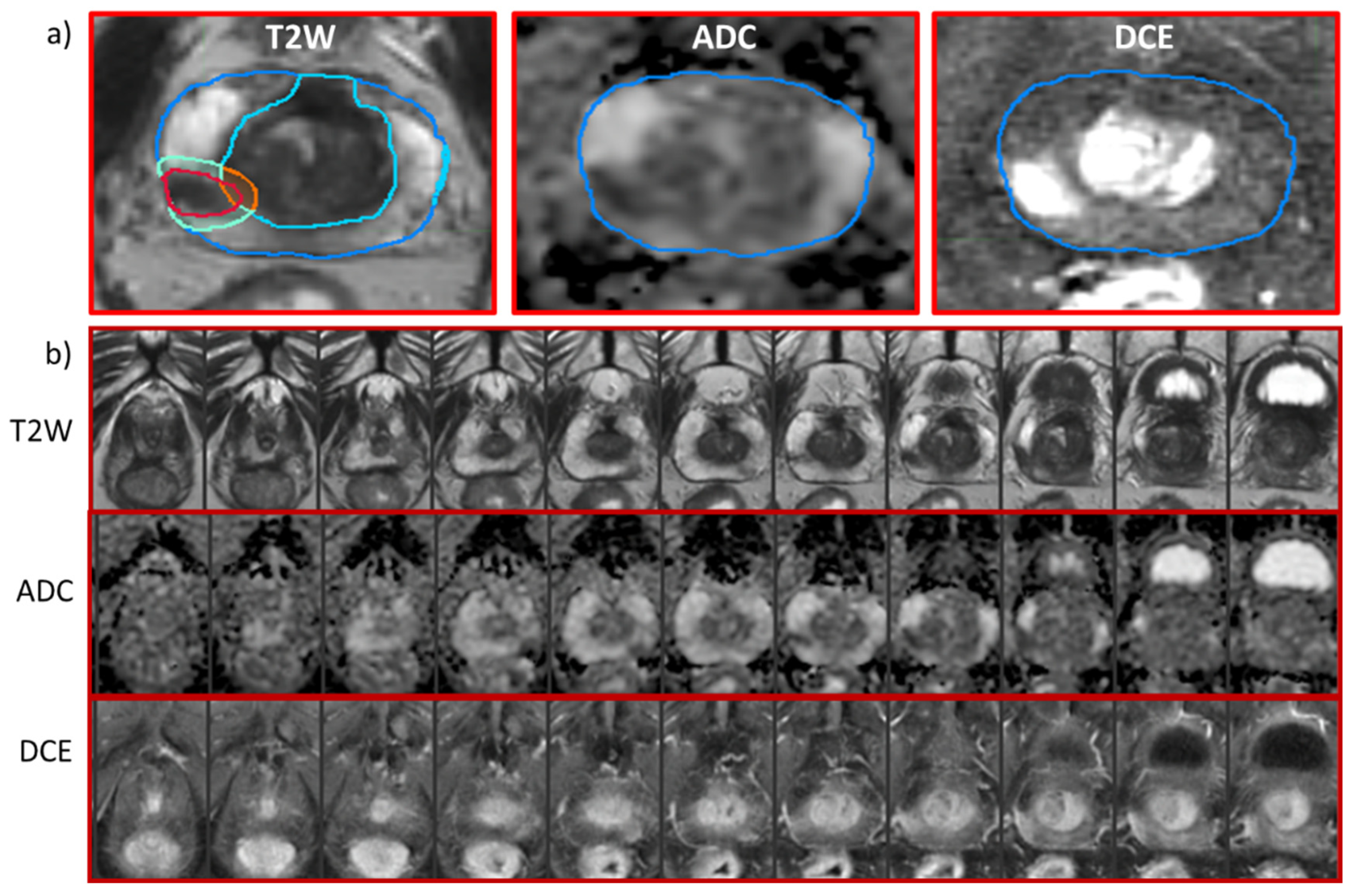
2.4. Prostate and GTVs Segmentations
2.5. Radiomic Features Extraction
2.6. Modeling and Statistical Analysis
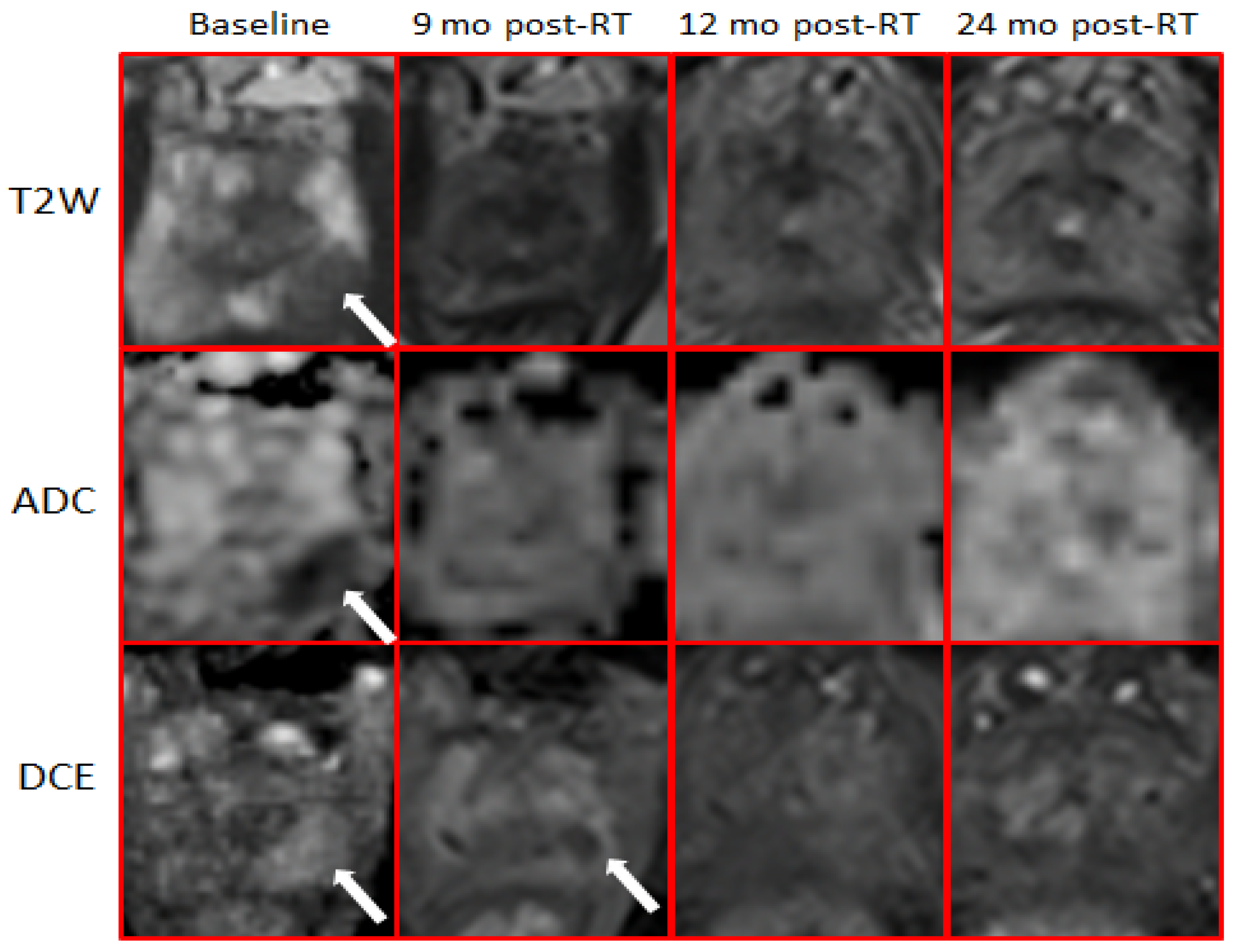
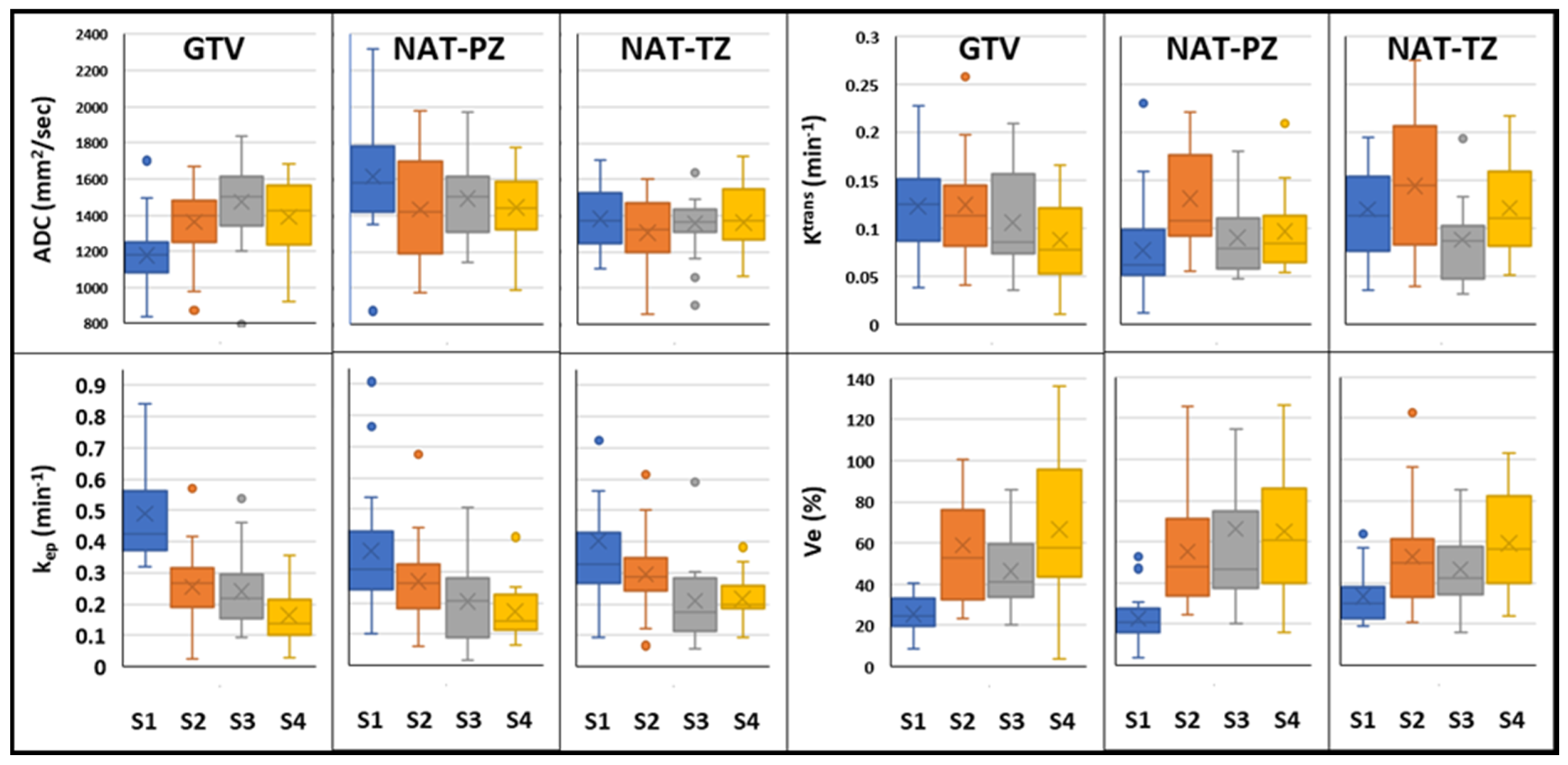
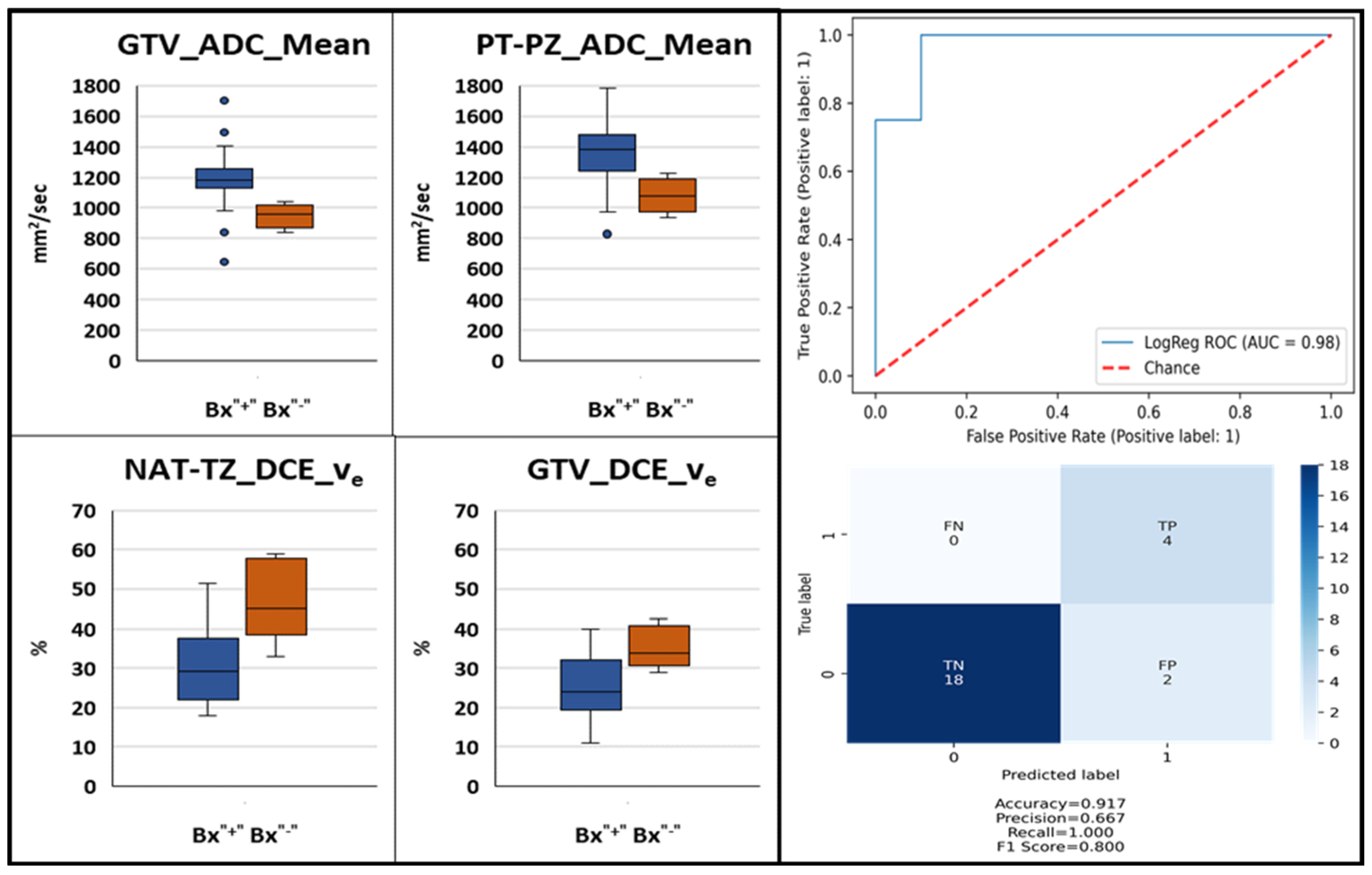
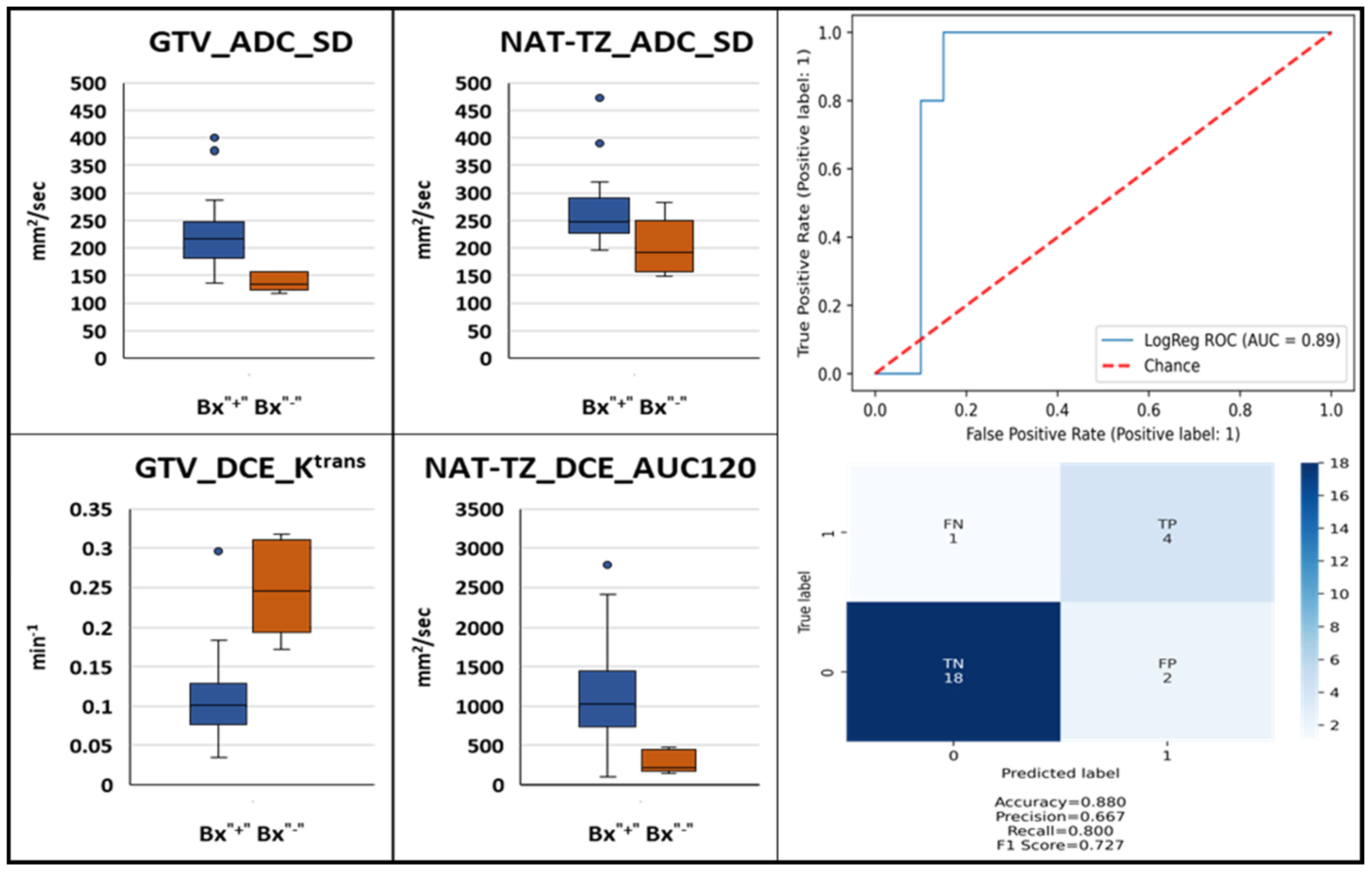
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scanner | Parameters | T2W | DWI | DCE |
|---|---|---|---|---|
| GE-Discovery | Pulse Sequence | FSE | EPI | SPRG |
| TR (ms) | 10763 | 9500 | 4.052 | |
| TE (ms) | 104.944 | 52.6 | 1.78 | |
| Pixel size (mm) | 1.25 × 1.25 × 2.5 | 1.25 × 1.25 × 2.5 | 1.25 × 1.25 × 2.5 | |
| Matrix | 256 × 256 × 72 | 256 × 256 × 36 | 256 × 256 × 72 | |
| b-values | 50–500–1000 | |||
| DCE-MRI Temporal resolution (sec) | 27–36 | |||
| Siemens-Skyra | Pulse Sequence | FSE | EPI | GR SP |
| TR (ms) | 6100 | 6600 | 5.24 | |
| TE (ms) | 114 | 91 | 2.33 | |
| Pixel size (mm) | 0.7 × 0.7 × 2.5 | 2.93 × 2.93 × 2.5 | 0.7 × 0.7 × 2.5 | |
| Matrix | 512 × 384 × 72 | 128 × 96 × 38 | 512 × 384 × 72 | |
| b-values | 50–500–1400 | |||
| DCE-MRI Temporal resolution (sec) | 30–35 | |||
| Feature | GTV | NAT-PZ | NAT-TZ |
|---|---|---|---|
| ADC | |||
| GTV | 0 | ||
| NAT-PZ | <0.0001 * | 0 | |
| NAT-TZ | 0.002 * | 0.004 * | 0 |
| Ktrans | |||
| GTV | 0 | ||
| NAT-PZ | 0.003 * | 0 | |
| NAT-TZ | 0.832 | 0.017 * | 0 |
| kep | |||
| GTV | 0 | ||
| NAT-PZ | 0.025 * | 0 | |
| NAT-TZ | 0.233 | 0.631 | 0 |
| ve | |||
| GTV | 0 | ||
| NAT-PZ | 0.372 | 0 | |
| NAT-TZ | 0.020 * | 0.006 * | 0 |
| Features | GTV | NAT-PZ | NAT-TZ |
|---|---|---|---|
| ADC | |||
| S21 | 0.010 * | 0.001 * | 0.825 |
| S31 | 0.001 * | 0.347 | 0.674 |
| S32 | 0.106 | 0.010 * | 0.402 |
| S41 | 0.012 * | 0.197 | 0.699 |
| S42 | 0.696 | 0.039 * | 0.474 |
| S43 | 0.270 | 0.643 | 0.959 |
| Ktrans | |||
| S21 | 0.946 | 0.292 | 0.222 |
| S31 | 0.285 | 0.559 | 0.092 |
| S32 | 0.346 | 0.472 | 0.005 * |
| S41 | 0.033 * | 0.350 | 0.939 |
| S42 | 0.075 | 0.910 | 0.246 |
| S43 | 0.306 | 0.500 | 0.055 |
| kep | |||
| S21 | <0.001 * | 0.060 | 0.126 |
| S31 | <0.001 * | 0.004 * | 0.013 * |
| S32 | 0.734 | 0.133 | 0.038 * |
| S41 | <0.001 * | 0.001 * | 0.017 * |
| S42 | 0.020 * | 0.014 * | 0.026 * |
| S43 | 0.042 * | 0.382 | 0.882 |
| ve | |||
| S21 | <0.001 * | <0.001 * | 0.003 * |
| S31 | <0.001 * | 0.002 * | 0.011 * |
| S32 | 0.178 | 0.440 | 0.398 |
| S41 | <0.001 * | <0.001 * | <0.001 * |
| S42 | 0.513 | 0.287 | 0.410 |
| S43 | 0.050 | 0.944 | 0.076 |
References
- Johansson, J.E. Natural History of Early, Localized Prostate Cancer. JAMA 2004, 291, 2713–2719. [Google Scholar] [CrossRef]
- Barbosa, F.G.; Queiroz, M.A.; Nunes, R.F.; Viana, P.C.C.; Marin, J.F.G.; Cerri, G.G.; Buchpiguel, C.A. Revisiting Prostate Cancer Recurrence with PSMA PET: Atlas of Typical and Atypical Patterns of Spread. RadioGraphics 2019, 39, 186–212. [Google Scholar] [CrossRef] [PubMed]
- Ma, T.M.; Chu, F.-I.; Sandler, H.; Feng, F.Y.; Efstathiou, J.A.; Jones, C.U.; Roach, M.; Rosenthal, S.A.; Pisansky, T.; Michalski, J.M.; et al. Local Failure Events in Prostate Cancer Treated with Radiotherapy: A Pooled Analysis of 18 Randomized Trials from the Meta-analysis of Randomized Trials in Cancer of the Prostate Consortium (LEVIATHAN). Eur. Urol. 2022; in press. [Google Scholar] [CrossRef] [PubMed]
- Roach, M.; Hanks, G.; Thames, H.; Schellhammer, P.; Shipley, W.U.; Sokol, G.H.; Sandler, H. Defining biochemical failure following radiotherapy with or without hormonal therapy in men with clinically localized prostate cancer: Recommendations of the RTOG-ASTRO Phoenix Consensus Conference. Int. J. Radiat. Oncol. 2006, 65, 965–974. [Google Scholar] [CrossRef] [PubMed]
- Kuban, D.A.; Tucker, S.L.; Dong, L.; Starkschall, G.; Huang, E.H.; Cheung, M.R.; Lee, A.K.; Pollack, A. Long-term results of the M. D. Anderson randomized dose-escalation trial for prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 67–74. [Google Scholar] [CrossRef]
- Pollack, A.; Li, T.; Buyyounouski, M.; Horwitz, E.; Price, R.; Feigenberg, S.; Konski, A.; Greenberg, R.; Uzzo, R.; Ma, C. Hypofractionation for Prostate Cancer: Interim Results of a Randomized Trial. Int. J. Radiat. Oncol. 2009, 75, S81–S82. [Google Scholar] [CrossRef]
- Crook, J.M.; Malone, S.; Perry, G.; Eapen, L.; Owen, J.; Robertson, S.; Ludgate, C.; Fung, S.; Lockwood, G. Twenty-four-month postradiation prostate biopsies are strongly predictive of 7-year disease-free survival: Results from a Canadian randomized trial. Cancer 2009, 115, 673–679. [Google Scholar] [CrossRef]
- Scardino, P.T.; Frankel, J.M.; Wheeler, T.M.; Meacham, R.B.; Hoffman, G.S.; Seale, C.; Wilbanks, J.H.; Easley, J.; Carlton, C.E. The Prognostic Significance of Post-Irradiation Biopsy Results in Patients with Prostatic Cancer. J. Urol. 1986, 135, 510–515. [Google Scholar] [CrossRef]
- Zelefsky, M.J.; Goldman, D.A.; Reuter, V.; Kollmeier, M.; McBride, S.; Zhang, Z.; Varghese, M.; Pei, X.; Fuks, Z. Long-Term Implications of a Positive Posttreatment Biopsy in Patients Treated with External Beam Radiotherapy for Clinically Localized Prostate Cancer. J. Urol. 2019, 201, 1127–1133. [Google Scholar] [CrossRef]
- Krauss, D.J.; Hu, C.; Bahary, J.-P.; Souhami, L.; Gore, E.M.; Chafe, S.M.J.; Leibenhaut, M.H.; Narayan, S.; Torres-Roca, J.; Michalski, J.; et al. Importance of Local Control in Early-Stage Prostate Cancer: Outcomes of Patients with Positive Post-Radiation Therapy Biopsy Results Treated in RTOG 9408. Int. J. Radiat. Oncol. 2015, 92, 863–873. [Google Scholar] [CrossRef]
- Vance, W.; Tucker, S.L.; de Crevoisier, R.; Kuban, D.A.; Cheung, M.R. The predictive value of 2-year posttreatment biopsy after prostate cancer radiotherapy for eventual biochemical outcome. Int. J. Radiat. Oncol. 2007, 67, 828–833. [Google Scholar] [CrossRef]
- Kass-Iliyya, A.; Jovic, G.; Murphy, C.; Fisher, C.; Syndikus, I.; Jose, C.; Scrase, C.D.; Graham, J.D.; Nicol, D.; Sydes, M.R.; et al. Two-years Postradiotherapy Biopsies: Lessons from MRC RT01 Trial. Eur. Urol. 2018, 73, 968–976. [Google Scholar] [CrossRef] [PubMed]
- Stoyanova, R.; Pahlajani, N.H.; Egleston, B.; Buyyounouski, M.K.; Chen, D.Y.T.; Horwitz, E.M.; Pollack, A. The impact of dose-escalated radiotherapy plus androgen deprivation for prostate cancer using 2 linked nomograms. Cancer 2012, 119, 1080–1088. [Google Scholar] [CrossRef] [PubMed]
- Takeda, T.; Tin, A.L.; Corradi, R.B.; Mamoor, M.; Benfante, N.E.; Sjoberg, D.D.; Scardino, P.T.; Eastham, J.A.; Fine, S.W.; Touijer, K.A. Topography of Prostate Cancer Recurrence after Radiation Therapy: A Detailed Mapping Study of Salvage Radical Prostatectomy Specimens. Eur. Urol. 2017, 73, 488–490. [Google Scholar] [CrossRef] [PubMed]
- Cellini, N.; Morganti, A.G.; Mattiucci, G.C.; Valentini, V.; Leone, M.; Luzi, S.; Manfredi, R.; Dinapoli, N.; Digesu’, C.; Smaniotto, D. Analysis of intraprostatic failures in patients treated with hormonal therapy and radiotherapy: Implications for conformal therapy planning. Int. J. Radiat. Oncol. 2002, 53, 595–599. [Google Scholar] [CrossRef]
- Chatterjee, A.; Turchan, W.T.; Fan, X.; Griffin, A.; Yousuf, A.; Karczmar, G.S.; Liauw, S.L.; Oto, A. Can Pre-treatment Quantitative Multi-parametric MRI Predict the Outcome of Radiotherapy in Patients with Prostate Cancer? Acad. Radiol. 2022, 29, 977–985. [Google Scholar] [CrossRef]
- Bjurlin, M.A.; Carroll, P.R.; Eggener, S.; Fulgham, P.F.; Margolis, D.J.; Pinto, P.A.; Rosenkrantz, A.B.; Rubenstein, J.N.; Rukstalis, D.B.; Taneja, S.S.; et al. Update of the Standard Operating Procedure on the Use of Multiparametric Magnetic Resonance Imaging for the Diagnosis, Staging and Management of Prostate Cancer. J. Urol. 2020, 203, 706–712. [Google Scholar] [CrossRef]
- Benz, M.R.; Vargas, H.A.; Sala, E. Functional MR Imaging Techniques in Oncology in the Era of Personalized Medicine. Magn. Reson. Imaging Clin. N. Am. 2015, 24, 1–10. [Google Scholar] [CrossRef]
- Lenkinski, R.E.; Bloch, B.N.; Liu, F.; Frangioni, J.V.; Perner, S.; Rubin, M.A.; Genega, E.M.; Rofsky, N.M.; Gaston, S.M. An illustration of the potential for mapping MRI/MRS parameters with genetic over-expression profiles in human prostate cancer. Magn. Reson. Mater. Phys. Biol. Med. 2008, 21, 411–421. [Google Scholar] [CrossRef][Green Version]
- Singanamalli, A.; Rusu, M.; Sparks, R.E.; Shih, N.N.; Ziober, A.; Wang, L.P.; Tomaszewski, J.; Rosen, M.; Feldman, M.; Madabhushi, A. Identifying in vivo DCE MRI markers associated with microvessel architecture and gleason grades of prostate cancer: MRI Markers of Microvessel Architecture in Prostate Cancer. J. Magn. Reson. Imaging 2016, 43, 149–158. [Google Scholar] [CrossRef]
- Tofts, P. Modeling tracer kinetics in dynamic Gd-DTPA MR imaging. J. Magn. Reson. Imaging 1997, 7, 91–101. [Google Scholar] [CrossRef]
- Tofts, P.S.; Brix, G.; Buckley, D.; Evelhoch, J.L.; Henderson, E.; Knopp, M.V.; Larsson, H.B.; Lee, T.-Y.; Mayr, N.A.; Parker, G.; et al. Estimating kinetic parameters from dynamic contrast-enhanced t1-weighted MRI of a diffusable tracer: Standardized quantities and symbols. J. Magn. Reson. Imaging 1999, 10, 223–232. [Google Scholar] [CrossRef]
- Mohiuddin, M.; Fujita, M.; Regine, W.F.; Megooni, A.S.; Ibbott, G.S.; Ahmed, M.M. High-dose spatially-fractionated radiation (GRID): A new paradigm in the management of advanced cancers. Int. J. Radiat. Oncol. Biol. Phys. 1999, 45, 721–727. [Google Scholar] [CrossRef]
- Kanagavelu, S.; Gupta, S.; Wu, X.; Philip, S.; Wattenberg, M.M.; Hodge, J.W.; Couto, M.D.; Chung, K.D.; Ahmed, M.M. In Vivo Effects of Lattice Radiation Therapy on Local and Distant Lung Cancer: Potential Role of Immunomodulation. Radiat. Res. 2014, 182, 149–162. [Google Scholar] [CrossRef] [PubMed]
- Pollack, A.; Chinea, F.M.; Bossart, E.; Kwon, D.; Abramowitz, M.C.; Lynne, C.; Jorda, M.; Marples, B.; Patel, V.N.; Wu, X.; et al. Phase I Trial of MRI-Guided Prostate Cancer Lattice Extreme Ablative Dose (LEAD) Boost Radiation Therapy. Int. J. Radiat. Oncol. 2020, 107, 305–315. [Google Scholar] [CrossRef]
- Epstein, J.I.; Amin, M.B.; Fine, S.W.; Algaba, F.; Aron, M.; Baydar, D.E.; Beltran, A.L.; Brimo, F.; Cheville, J.C.; Colecchia, M.; et al. The 2019 Genitourinary Pathology Society (GUPS) White Paper on Contemporary Grading of Prostate Cancer. Arch. Pathol. Lab. Med. 2020, 145, 461–493. [Google Scholar] [CrossRef] [PubMed]
- Kryvenko, O.N.; Epstein, J.I. Prostate Cancer Grading: A Decade after the 2005 Modified Gleason Grading System. Arch. Pathol. Lab. Med. 2016, 140, 1140–1152. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, J.S.; Smith, S.C.; Paner, G.P.; McKenney, J.K.; Sekhri, R.; Osunkoya, A.O.; Baras, A.S.; DeMarzo, A.M.; Cheville, J.C.; Rafael, J.E.; et al. Reporting Practices and Resource Utilization in the Era of Intraductal Carcinoma of the Prostate: A Survey of Genitourinary Subspecialists. Am. J. Surg. Pathol. 2020, 44, 673–680. [Google Scholar] [CrossRef] [PubMed]
- Kryvenko, O.N.; Punnen, S.; Udayakumar, T.S.; Gaston, S.M.; Tao, W.; Ma, W.; Stoyanova, R.; Pollack, A. Experimental Support for the Possibility of Retrograde Genesis of Intraductal Carcinoma of the Prostate. Int. J. Surg. Pathol. 2022. [Google Scholar] [CrossRef]
- Barentsz, J.O.; Weinreb, J.C.; Verma, S.; Thoeny, H.C.; Tempany, C.M.; Shtern, F.; Padhani, A.R.; Margolis, D.; Macura, K.J.; Haider, M.A.; et al. Synopsis of the PI-RADS v2 Guidelines for Multiparametric Prostate Magnetic Resonance Imaging and Recommendations for Use. Eur. Urol. 2015, 69, 41–49. [Google Scholar] [CrossRef]
- Algohary, A.; Shiradkar, R.; Pahwa, S.; Purysko, A.; Verma, S.; Moses, D.; Shnier, R.; Haynes, A.-M.; Delprado, W.; Thompson, J.; et al. Combination of Peri-Tumoral and Intra-Tumoral Radiomic Features on Bi-Parametric MRI Accurately Stratifies Prostate Cancer Risk: A Multi-Site Study. Cancers 2020, 12, 2200. [Google Scholar] [CrossRef]
- Kwon, D.; Reis, I.M.; Breto, A.L.; Tschudi, Y.; Gautney, N.; Zavala-Romero, O.; Lopez, C.; Ford, J.C.; Punnen, S.; Pollack, A.; et al. Classification of suspicious lesions on prostate multiparametric MRI using machine learning. J. Med. Imaging 2018, 5, 034502. [Google Scholar] [CrossRef]
- Parker, G.J.; Roberts, C.; Macdonald, A.; Buonaccorsi, G.A.; Cheung, S.; Buckley, D.L.; Jackson, A.; Watson, Y.; Davies, K.; Jayson, G.C. Experimentally-derived functional form for a population-averaged high-temporal-resolution arterial input function for dynamic contrast-enhanced MRI. Magn. Reson. Med. 2006, 56, 993–1000. [Google Scholar] [CrossRef] [PubMed]
- Tofts, P.; Stoyanova, R. Modelling Slow DCE Data from Prostate: Rate Constant (kep) and Extracellular Extravascular Space (EES: ve) Both Distinguish Hypoxic Regions in the Tumour; European Society for Magnetic Resonance in Medicine and Biology (ESMRMB) Congress: Vienna, Austria, 2011. [Google Scholar]
- Bourne, R.M.; Kurniawan, N.; Cowin, G.; Stait-Gardner, T.; Sved, P.; Watson, G.; Price, W.S. Microscopic diffusivity compartmentation in formalin-fixed prostate tissue: Microscopic Diffusion Compartmentation in Prostate Tissue. Magn. Reson. Med. 2012, 68, 614–620. [Google Scholar] [CrossRef] [PubMed]
- Bono, A.V.; Celato, N.; Cova, V.; Salvadore, M.; Chinetti, S.; Novario, R. Microvessel density in prostate carcinoma. Prostate Cancer Prostatic Dis. 2002, 5, 123–127. [Google Scholar] [CrossRef]
- Alizadeh, F.; Hadi, M.; Khorrami, M.; Yazdani, M.; Joozdani, R.H.; Tadayyon, F.; Mellat, M. Prostate cancer: Relationship between vascular diameter, shape and density and Gleason score in needle biopsy specimens. Adv. Biomed. Res. 2013, 2, 3. [Google Scholar] [CrossRef]
- Noworolski, S.M.; Vigneron, D.B.; Chen, A.P.; Kurhanewicz, J. Dynamic contrast-enhanced MRI and MR diffusion imaging to distinguish between glandular and stromal prostatic tissues. Magn. Reson. Imaging 2008, 26, 1071–1080. [Google Scholar] [CrossRef]
- Pasquier, D.; Henni, A.H.; Escande, A.; Tresch, E.; Reynaert, N.; Colot, O.; Lartigau, E.; Betrouni, N. Diffusion weighted MRI as an early predictor of tumor response to hypofractionated stereotactic boost for prostate cancer. Sci. Rep. 2018, 8, 10407. [Google Scholar] [CrossRef]
- Foltz, W.D.; Wu, A.; Chung, P.; Catton, C.; Bayley, A.; Milosevic, M.; Bristow, R.; Warde, P.; Simeonov, A.; Jaffray, D.A.; et al. Changes in apparent diffusion coefficient and T2relaxation during radiotherapy for prostate cancer. J. Magn. Reson. Imaging 2012, 37, 909–916. [Google Scholar] [CrossRef]
- Franiel, T.; Lüdemann, L.; Taupitz, M.; Böhmer, D.; Beyersdorff, D. MRI before and after external beam intensity-modulated radiotherapy of patients with prostate cancer: The feasibility of monitoring of radiation-induced tissue changes using a dynamic contrast-enhanced inversion-prepared dual-contrast gradient echo sequence. Radiother. Oncol. 2009, 93, 241–245. [Google Scholar] [CrossRef]
- Zelefsky, M.J.; Reuter, V.E.; Fuks, Z.; Scardino, P.; Shippy, A. Influence of Local Tumor Control on Distant Metastases and Cancer Related Mortality after External Beam Radiotherapy for Prostate Cancer. J. Urol. 2008, 179, 1368–1373. [Google Scholar] [CrossRef] [PubMed]
- Pollack, A.; Zagars, G.K.; Antolak, J.A.; Kuban, D.A.; Rosen, I.I. Prostate biopsy status and PSA nadir level as early surrogates for treatment failure: Analysis of a prostate cancer randomized radiation dose escalation trial. Int. J. Radiat. Oncol. 2002, 54, 677–685. [Google Scholar] [CrossRef]
- Pollack, A.; Walker, G.; Horwitz, E.M.; Price, R.; Feigenberg, S.; Konski, A.A.; Stoyanova, R.; Movsas, B.; Greenberg, R.E.; Uzzo, R.G.; et al. Randomized Trial of Hypofractionated External-Beam Radiotherapy for Prostate Cancer. J. Clin. Oncol. 2013, 31, 3860–3868. [Google Scholar] [CrossRef] [PubMed]
- Avkshtol, V.; Ruth, K.J.; Ross, E.A.; Hallman, M.A.; Greenberg, R.E.; Price, R.A., Jr.; Leachman, B.; Uzzo, R.G.; Ma, C.; Chen, D.; et al. Ten-Year Update of a Randomized, Prospective Trial of Conventional Fractionated Versus Moderate Hypofractionated Radiation Therapy for Localized Prostate Cancer. J. Clin. Oncol. 2020, 38, 1676–1684. [Google Scholar] [CrossRef]
- Akin, O.; Gultekin, D.H.; Vargas, H.A.; Zheng, J.; Moskowitz, C.; Pei, X.; Sperling, D.; Schwartz, L.H.; Hricak, H.; Zelefsky, M.J. Incremental value of diffusion weighted and dynamic contrast enhanced MRI in the detection of locally recurrent prostate cancer after radiation treatment: Preliminary results. Eur. Radiol. 2011, 21, 1970–1978. [Google Scholar] [CrossRef][Green Version]
- Donati, O.F.; Jung, S.I.; Vargas, H.A.; Gultekin, D.H.; Zheng, J.; Moskowitz, C.S.; Hricak, H.; Zelefsky, M.J.; Akin, O. Multiparametric Prostate MR Imaging with T2-weighted, Diffusion-weighted, and Dynamic Contrast-enhanced Sequences: Are All Pulse Sequences Necessary to Detect Locally Recurrent Prostate Cancer after Radiation Therapy? Radiology 2013, 268, 440–450. [Google Scholar] [CrossRef]
- Huang, K.T.; Stoyanova, R.; Walker, G.; Sandler, K.; Studenski, M.T.; Dogan, N.; Al-Saleem, T.; Buyyounouski, M.K.; Horwitz, E.M.; Pollack, A. Post-radiotherapy prostate biopsies reveal heightened apex positivity relative to other prostate regions sampled. Radiother. Oncol. 2015, 115, 101–106. [Google Scholar] [CrossRef]
- Meshman, J.; Farnia, B.; Stoyanova, R.; Reis, I.; Abramowitz, M.; Dal Pra, A.; Horwitz, E.; Pollack, A. Post-Treatment Biopsy Positivity In Prostate Cancer Patients Undergoing MpMRI-Targeted Radiation Dose Escalation. Int. J. Radiat. Oncol. Biol. Phys. 2020, 108, e870. [Google Scholar] [CrossRef]
- Yamaguchi, H.; Hori, M.; Suzuki, O.; Seo, Y.; Isohashi, F.; Yoshioka, Y.; Sumida, I.; Uemura, M.; Fujita, K.; Nagahara, A.; et al. Clinical Significance of the Apparent Diffusion Coefficient Ratio in Prostate Cancer Treatment with Intensity-modulated Radiotherapy. Anticancer Res. 2016, 36, 6551–6556. [Google Scholar] [CrossRef]
- Liu, L.; Wu, N.; Ouyang, H.; Dai, J.-R.; Wang, W.-H. Diffusion-weighted MRI in early assessment of tumour response to radiotherapy in high-risk prostate cancer. Br. J. Radiol. 2014, 87, 20140359. [Google Scholar] [CrossRef]
- Padhani, A.R.; Liu, G.; Mu-Koh, D.; Chenevert, T.L.; Thoeny, H.C.; Takahara, T.; Dzik-Jurasz, A.; Ross, B.D.; Van Cauteren, M.; Collins, D.; et al. Diffusion-Weighted Magnetic Resonance Imaging as a Cancer Biomarker: Consensus and Recommendations. Neoplasia 2009, 11, 102–125. [Google Scholar] [CrossRef] [PubMed]
- Hötker, A.M.; Mazaheri, Y.; Zheng, J.; Moskowitz, C.S.; Berkowitz, J.; Lantos, J.; Pei, X.; Zelefsky, M.J.; Hricak, H.; Akin, O. Prostate Cancer: Assessing the effects of androgen-deprivation therapy using quantitative diffusion-weighted and dynamic contrast-enhanced MRI. Eur. Radiol. 2015, 25, 2665–2672. [Google Scholar] [CrossRef] [PubMed]
- Stoyanova, R.; Lopez, C.; Breto, A.; Xu, I.; Kwon, D.; Franco, G.; Pra, A.D.; Abramowitz, M.; Punnen, S.; Pollack, A. The Effects of Androgen-Deprivation Therapy on MRI Delta Radiomics Features in a Prospective Radiotherapy Treatment Trial for Prostate Cancer. Int. J. Radiat. Oncol. 2020, 108, e354. [Google Scholar] [CrossRef]






| ROI | ADC | DCE |
|---|---|---|
| Gross Tumor Volume (GTV) Peritumoral GTV in PZ zone (PT-PZ) Peritumoral GTV in TZ zone (PT-TZ) Normally-Appearing Peripheral Zone (NAT-PZ) Normally-Appearing Transition Zone (NAT-TZ) | 10% 25% 50% 75% 90% Mean Standard deviation (SD) Kurtosis (Kurt) Skewness (Skew) | Ktrans kep ve AUC90 AUC120 tonset |
| N (%) | |
|---|---|
| Age, years (mean ± stdev) | 68 ± 8 |
| Ethnicity | |
| Hispanic | 8 (32%) |
| Non-Hispanic | 17 (68%) |
| PSA, ng/mL (mean ± stdev) | 7.54 ± 3.51 |
| Grade Group | |
| GG1 | 11 (44%) |
| GG2 | 6 (24%) |
| GG3 | 4 (16%) |
| GG4 | 3 (12%) |
| GG5 | 1 (4%) |
| T-category | |
| T1c | 16 (64%) |
| T2a | 5 (20%) |
| T2b | 3 (12%) |
| T2c | 1 (4%) |
| Number of GTVs | |
| 1 | 12 (48%) |
| 2 | 11 (44%) |
| 3 | 2 (8%) |
| Zonal location of GTVs | |
| PZ | 34 (85%) |
| TZ | 3 (7.5%) |
| PZ/TZ | 3 (7.5%) |
| Number of post-RT exams | |
| 2 | 6 (24%) |
| 3 | 19 (76%) |
| Total MRI exams | 94 |
| MRI scanner | |
| Discovery | 64 (68%) |
| Skyra | 24 (26%) |
| Symphony | 1 (1%) |
| TrioTim | 5 (5%) |
| GTV | NAT-PZ | NAT-TZ | |||
|---|---|---|---|---|---|
| Sequence | Feature | MRI Scan | Mean ± Stdev | Mean ± Stdev | Mean ± Stdev |
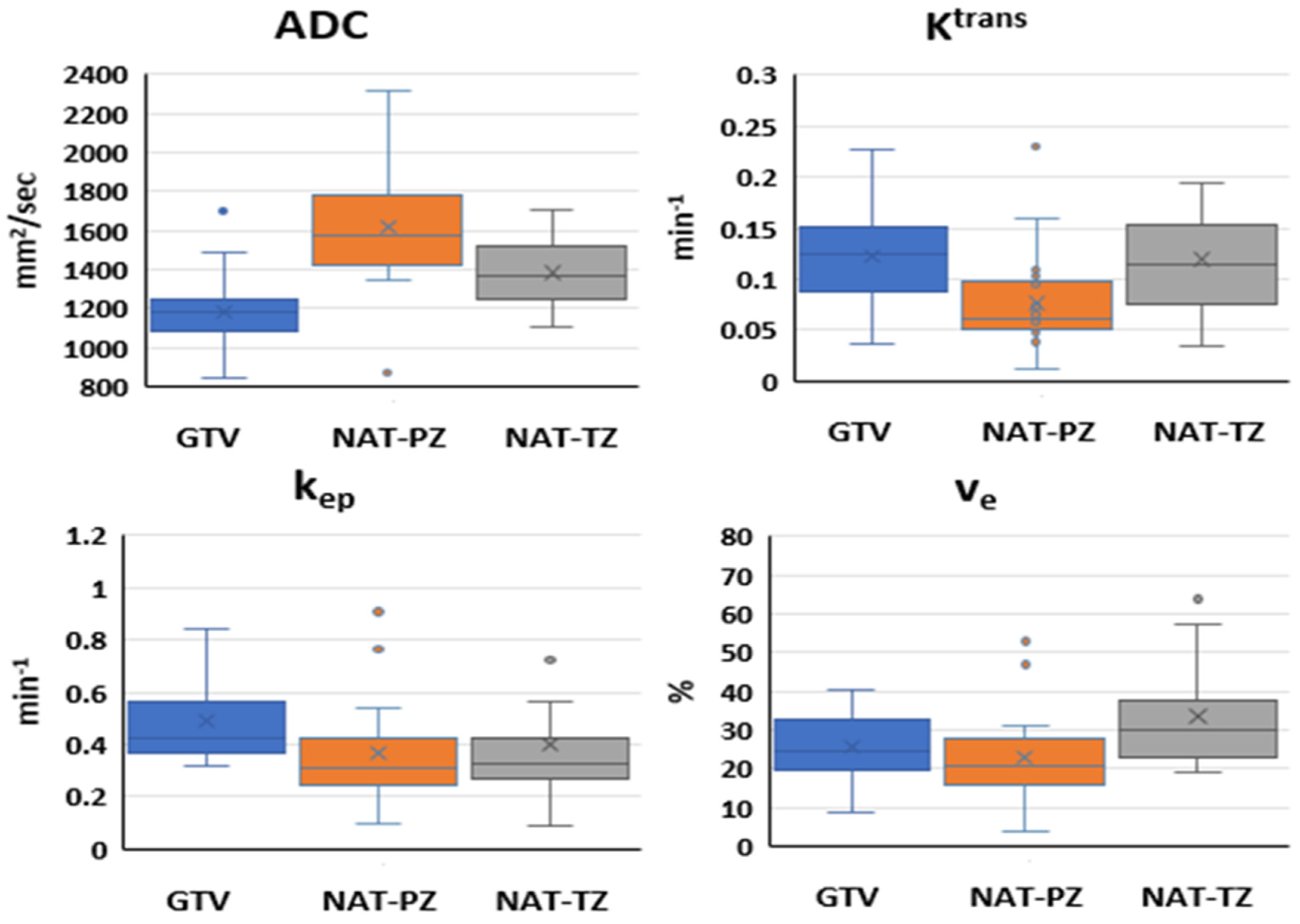
| DWI | ADC (mm2/sec) | Baseline | 1177.84 ± 217.12 | 1616.37 ± 304.02 | 1381.76 ± 170.34 |
| 3 months post-RT | 1362.45 ± 191.93 | 1435.44 ± 290.54 | 1303.92 ± 226.71 | ||
| 9 months post-RT | 1474.76 ± 241.12 | 1493.89 ± 217.73 | 1357.37 ± 171.65 | ||
| 24 months post-RT | 1388.68 ± 212.14 | 1445.18 ± 206.83 | 1361.00 ± 251.03 | ||
| DCE | Ktrans (min−1) | Baseline | 0.12 ± 0.05 | 0.08 ± 0.05 | 0.12 ± 0.06 |
| 3 months post-RT | 0.12 ± 0.07 | 0.13 ± 0.05 | 0.14 ± 0.07 | ||
| 9 months post-RT | 0.11 ± 0.05 | 0.09 ± 0.04 | 0.09 ± 0.05 | ||
| 24 months post-RT | 0.09 ± 0.05 | 0.10 ± 0.04 | 0.12 ± 0.05 | ||
| kep (min−1) | Baseline | 0.49 ± 0.15 | 0.37 ± 0.19 | 0.40 ± 0.29 | |
| 3 months post-RT | 0.25 ± 0.13 | 0.27 ± 0.13 | 0.30 ± 0.12 | ||
| 9 months post-RT | 0.24 ± 0.12 | 0.20 ± 0.13 | 0.21 ± 0.13 | ||
| 24 months post-RT | 0.16 ± 0.09 | 0.17 ± 0.08 | 0.22 ± 0.07 | ||
| ve (%) | Baseline | 25.54 ± 8.21 | 22.82 ± 11.12 | 33.55 ± 12.73 | |
| 3 months post-RT | 58.80 ± 34.19 | 55.13 ± 25.12 | 52.66 ± 25.03 | ||
| 9 months post-RT | 46.37 ± 18.85 | 66.34 ± 60.06 | 46.62 ± 17.72 | ||
| 24 months post-RT | 66.58 ± 37.17 | 65.15 ± 31.30 | 59.30 ± 22.60 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Algohary, A.; Alhusseini, M.; Breto, A.L.; Kwon, D.; Xu, I.R.; Gaston, S.M.; Castillo, P.; Punnen, S.; Spieler, B.; Abramowitz, M.C.; et al. Longitudinal Changes and Predictive Value of Multiparametric MRI Features for Prostate Cancer Patients Treated with MRI-Guided Lattice Extreme Ablative Dose (LEAD) Boost Radiotherapy. Cancers 2022, 14, 4475. https://doi.org/10.3390/cancers14184475
Algohary A, Alhusseini M, Breto AL, Kwon D, Xu IR, Gaston SM, Castillo P, Punnen S, Spieler B, Abramowitz MC, et al. Longitudinal Changes and Predictive Value of Multiparametric MRI Features for Prostate Cancer Patients Treated with MRI-Guided Lattice Extreme Ablative Dose (LEAD) Boost Radiotherapy. Cancers. 2022; 14(18):4475. https://doi.org/10.3390/cancers14184475
Chicago/Turabian StyleAlgohary, Ahmad, Mohammad Alhusseini, Adrian L. Breto, Deukwoo Kwon, Isaac R. Xu, Sandra M. Gaston, Patricia Castillo, Sanoj Punnen, Benjamin Spieler, Matthew C. Abramowitz, and et al. 2022. "Longitudinal Changes and Predictive Value of Multiparametric MRI Features for Prostate Cancer Patients Treated with MRI-Guided Lattice Extreme Ablative Dose (LEAD) Boost Radiotherapy" Cancers 14, no. 18: 4475. https://doi.org/10.3390/cancers14184475
APA StyleAlgohary, A., Alhusseini, M., Breto, A. L., Kwon, D., Xu, I. R., Gaston, S. M., Castillo, P., Punnen, S., Spieler, B., Abramowitz, M. C., Dal Pra, A., Kryvenko, O. N., Pollack, A., & Stoyanova, R. (2022). Longitudinal Changes and Predictive Value of Multiparametric MRI Features for Prostate Cancer Patients Treated with MRI-Guided Lattice Extreme Ablative Dose (LEAD) Boost Radiotherapy. Cancers, 14(18), 4475. https://doi.org/10.3390/cancers14184475