
COVID-19 and Lung Cancer Survival: An Updated Systematic Review and Meta-Analysis

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Material and Methods
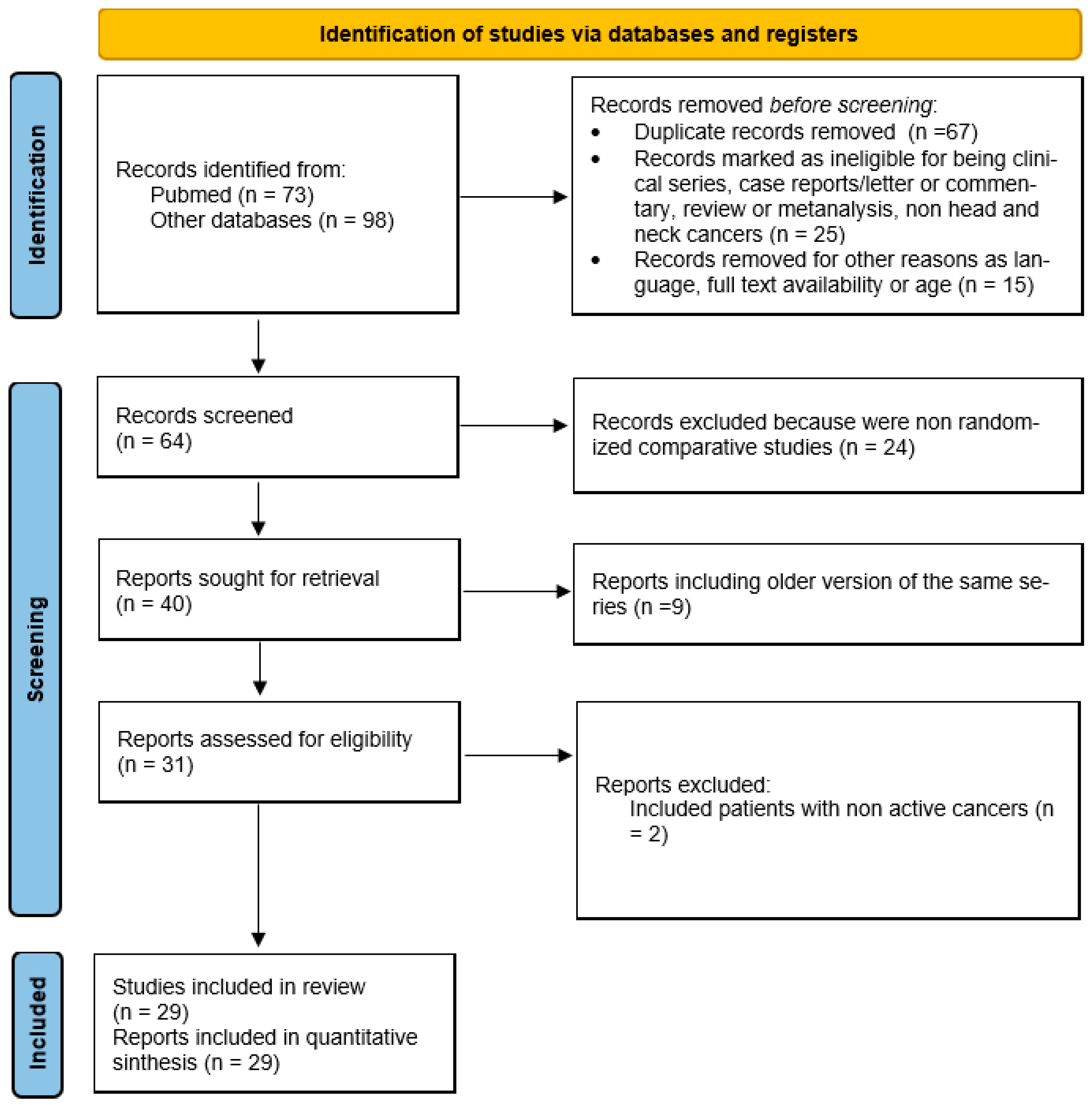
2.1. Search Strategy and Literature Search
2.2. Study Selection
2.3. Data Extraction and Quality Assessment
2.4. Outcomes and Statistical Analysis
3. Results
3.1. Characteristics of Included Studies
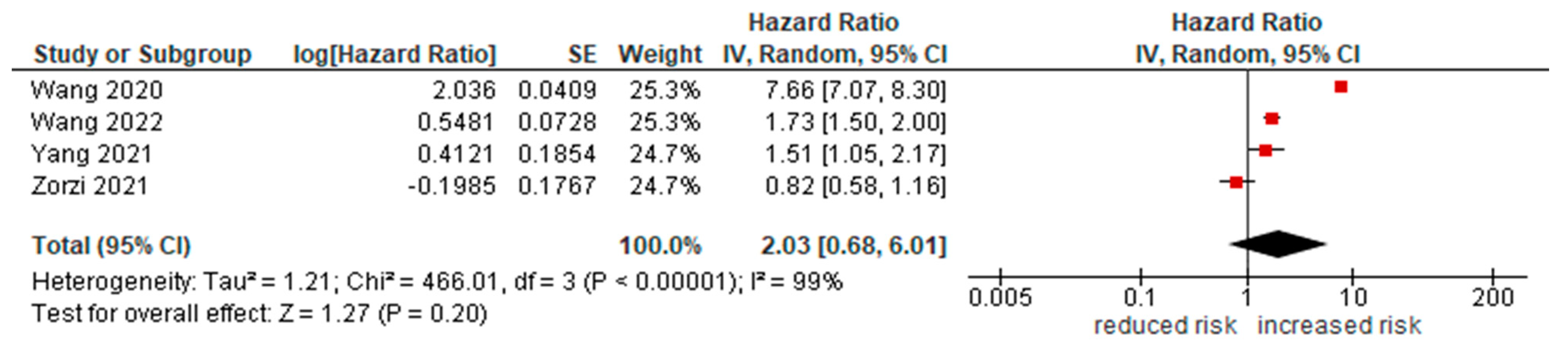
3.2. Infection Risk of Patients with Lung Cancer vs. Control Patients
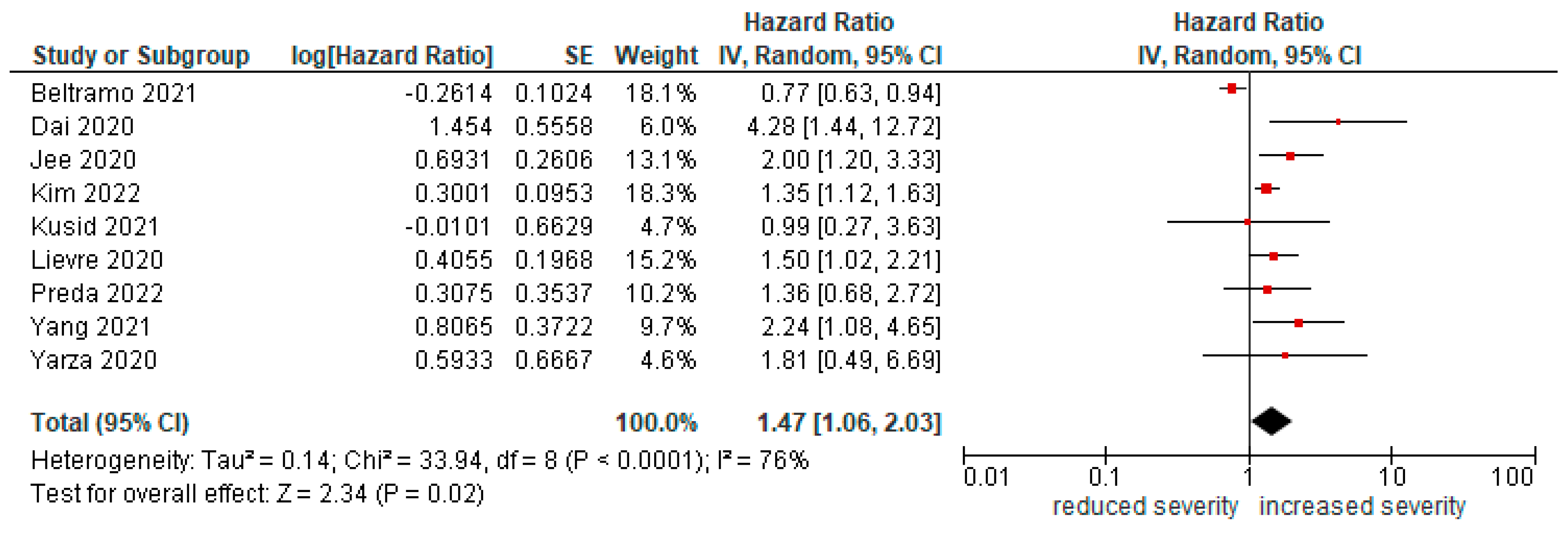
3.3. Severity of COVID-19 with Lung Cancer
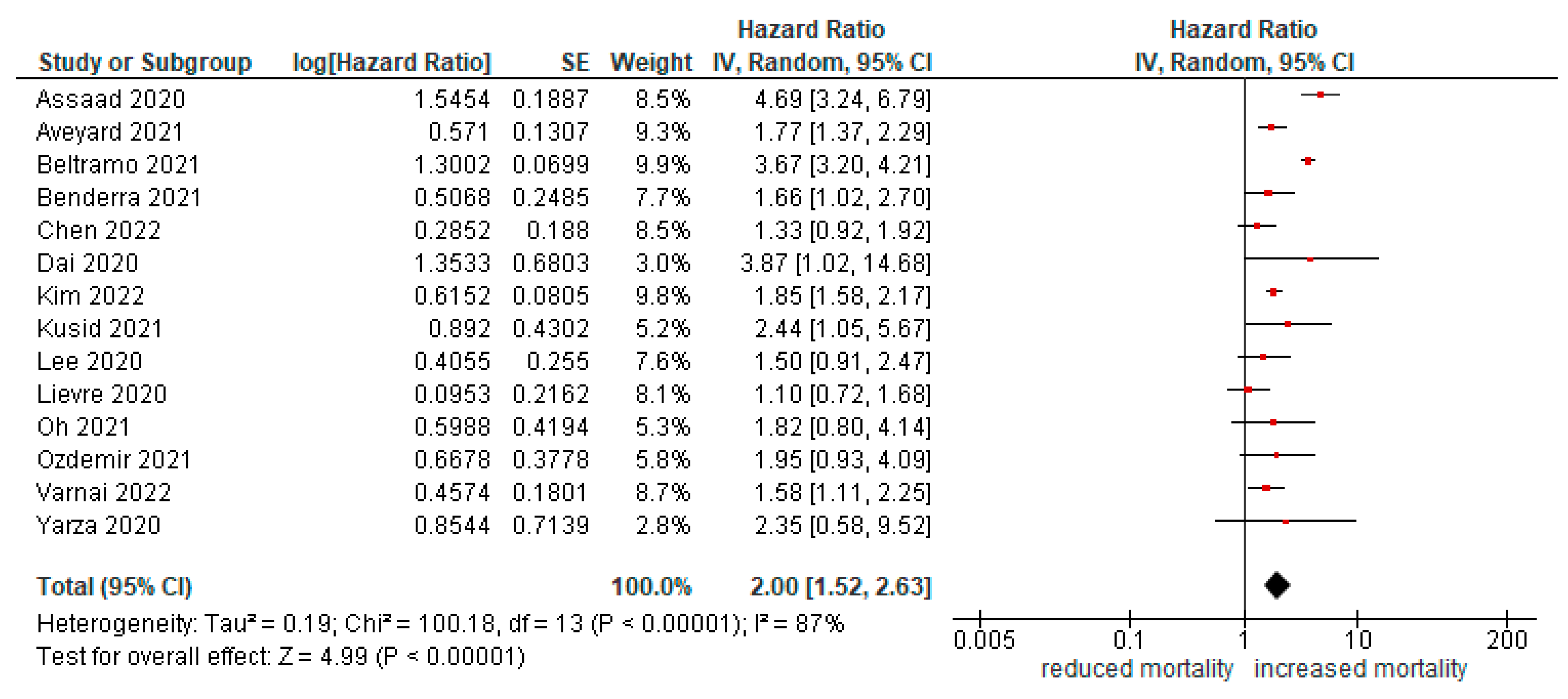
3.4. Mortality of Patients with Lung Cancer vs. Control Patients
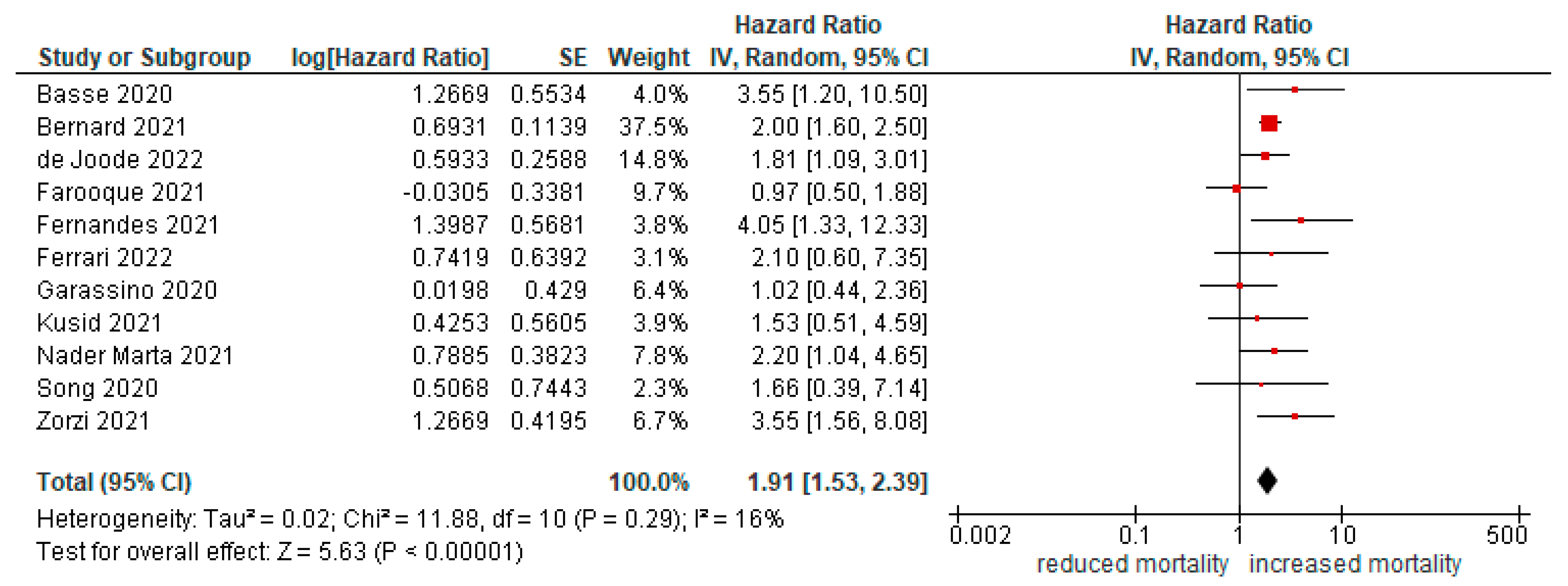
3.5. Mortality of Patients with Lung Cancer vs. Non Lung Cancer Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 13, 782–793. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Addeo, A.; Friedlaender, A. Cancer and COVID-19: Unmasking their ties. Cancer Treat. Rev. 2020, 88, 102041. [Google Scholar] [CrossRef] [PubMed]
- Xiong, B.; Liu, T.; Luo, P.; Wei, Y.; Zhou, Y.; Liu, M.; Zhang, Y.; Wang, H.; Zhang, X.; Wang, X.; et al. Prominent Hypercoagulability Associated With Inflammatory State Among Cancer Patients With SARS-CoV-2 Infection. Front. Oncol. 2020, 10, 1345. [Google Scholar] [CrossRef] [PubMed]
- Shieh, W.-J.; Hsiao, C.-H.; Paddock, C.D.; Guarner, J.; Goldsmith, C.S.; Tatti, K.; Packard, M.; Mueller, L.; Wu, M.-Z.; Rollin, P.; et al. Immunohistochemical, in situ hybridization, and ultrastructural localization of SARS-associated coronavirus in lung of a fatal case of severe acute respiratory syndrome in Taiwan. Hum. Pathol. 2005, 36, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Ding, Y.; He, L.; Zhang, Q.; Huang, Z.; Che, X.; Hou, J.; Wang, H.; Shen, H.; Qiu, L.; Li, Z.; et al. Organ distribution of severe acute respiratory syndrome(SARS) associated coronavirus(SARS-CoV) in SARS patients: Implications for pathogenesis and virus transmission pathways. J. Pathol. 2004, 203, 622–630. [Google Scholar] [CrossRef]
- Nadalin, S.; Flego, V.; Pavlić, S.D.; Volarić, D.; Badovinac, A.R.; Kapović, M.; Ristić, S. Association between the ACE-I/D polymorphism and nicotine dependence amongst patients with lung cancer. Biomed. Rep. 2020, 13, 58. [Google Scholar] [CrossRef]
- Chen, J.; Sun, M.; Zhou, M.; Lu, R. Associations between I/D polymorphism in the ACE gene and lung cancer: An updated systematic review and a meta-analysis. BMC Cancer 2021, 21, 158. [Google Scholar] [CrossRef]
- Zembower, T.R. Epidemiology of Infections in Cancer Patients. In Infectious Complications in Cancer Patients; Stosor, V., Zembower, T.R., Eds.; Springer International Publishing: Berlin/Heidelberg, Germany, 2014; pp. 43–89. [Google Scholar] [CrossRef]
- Assaad, S.; Avrillon, V.; Fournier, M.-L.; Mastroianni, B.; Russias, B.; Swalduz, A.; Cassier, P.; Eberst, L.; Steineur, M.-P.; Kazes, M.; et al. High mortality rate in cancer patients with symptoms of COVID-19 with or without detectable SARS-CoV-2 on RT-PCR. Eur. J. Cancer 2020, 135, 251–259. [Google Scholar] [CrossRef]
- Aveyard, P.; Gao, M.; Lindson, N.; Hartmann-Boyce, J.; Watkinson, P.; Young, D.; Coupland, C.A.C.; Tan, P.S.; Clift, A.K.; Harrison, D.; et al. Association between pre-existing respiratory disease and its treatment, and severe COVID-19: A population cohort study. Lancet Respir. Med. 2021, 9, 909–923. [Google Scholar] [CrossRef]
- Basse, C.; Diakite, S.; Servois, V.; Frelaut, M.; Noret, A.; Bellesoeur, A.; Moreau, P.; Massiani, M.-A.; Bouyer, A.-S.; Vuagnat, P.; et al. Characteristics and Outcome of SARS-CoV-2 Infection in Cancer Patients. JNCI Cancer Spectr. 2021, 5, pkaa090. [Google Scholar] [CrossRef] [PubMed]
- Beltramo, G.; Cottenet, J.; Mariet, A.-S.; Georges, M.; Piroth, L.; Tubert-Bitter, P.; Bonniaud, P.; Quantin, C. Chronic respiratory diseases are predictors of severe outcome in COVID-19 hospitalised patients: A nationwide study. Eur. Respir. J. 2021, 58, 2004474. [Google Scholar] [CrossRef] [PubMed]
- Benderra, M.-A.; Aparicio, A.; Leblanc, J.; Wassermann, D.; Kempf, E.; Galula, G.; Bernaux, M.; Canellas, A.; Moreau, T.; Bellamine, A.; et al. Clinical Characteristics, Care Trajectories and Mortality Rate of SARS-CoV-2 Infected Cancer Patients: A Multicenter Cohort Study. Cancers 2021, 13, 4749. [Google Scholar] [CrossRef] [PubMed]
- Bernard, A.; Cottenet, J.; Bonniaud, P.; Piroth, L.; Arveux, P.; Tubert-Bitter, P.; Quantin, C. Comparison of Cancer Patients to Non-Cancer Patients among COVID-19 Inpatients at a National Level. Cancers 2021, 13, 1436. [Google Scholar] [CrossRef] [PubMed]
- Chen, U.-I.; Xu, H.; Krause, T.M.; Greenberg, R.; Dong, X.; Jiang, X. Factors Associated With COVID-19 Death in the United States: Cohort Study. JMIR Public Health Surveill. 2022, 8, e29343. [Google Scholar] [CrossRef] [PubMed]
- Dai, M.-Y.; Chen, Z.; Leng, Y.; Wu, M.; Liu, Y.; Zhou, F.; Ming, C.; Shao, N.; Liu, M.; Cai, H. Patients With Lung Cancer Have High Susceptibility of COVID-19: A Retrospective Study in Wuhan, China. Cancer Control 2020, 27, 1073274820960467. [Google Scholar] [CrossRef]
- de Joode, K.; Tol, J.; Hamberg, P.; Cloos, M.; Kastelijn, E.A.; Borgers, J.S.; Nuij, V.J.; Klaver, Y.; Herder, G.J.; Mutsaers, P.G.; et al. Life-prolonging treatment restrictions and outcomes in patients with cancer and COVID-19: An update from the Dutch Oncology COVID-19 Consortium. Eur. J. Cancer 2021, 160, 261–272. [Google Scholar] [CrossRef]
- Farooque, I.; Farooque, U.; Karimi, S.; Syed, M.U.S.; Nadeem, Z.; Zulfiqar, A.; Mustafa, S.; Farooque, R.; Sultan, A.A.; Hassan, S.A. Clinical Presentations and Outcomes of Coronavirus Disease 2019 in Patients with Solid Tumors. Cureus 2021, 13, e15452. [Google Scholar] [CrossRef]
- Fernandes, G.A.; Feriani, D.; e Silva, I.L.A.F.; e Silva, D.R.M.; Arantes, P.E.; Canteras, J.D.S.; da Silva, R.R.; Curado, M.P. Differences in mortality of cancer patients with COVID-19 in a Brazilian cancer center. Semin. Oncol. 2021, 48, 171–180. [Google Scholar] [CrossRef]
- Ferrari, B.L.; Gil Ferreira, C.; Menezes, M.; De Marchi, P.; Canedo, J.; de Melo, A.C.; Jácome, A.A.; Reinert, T.; Paes, R.D.; Sodré, B.; et al. Determinants of COVID-19 Mortality in Patients with Cancer From a Community Oncology Practice in Brazil. JCO Glob. Oncol. 2021, 7, 46–55. [Google Scholar] [CrossRef]
- Garassino, M.C.; Whisenant, J.G.; Huang, L.-C.; Trama, A.; Torri, V.; Agustoni, F.; Baena, J.; Banna, G.; Berardi, R.; Bettini, A.C.; et al. COVID-19 in patients with thoracic malignancies (TERAVOLT): First results of an international, registry-based, cohort study. Lancet Oncol. 2020, 21, 914–922. [Google Scholar] [CrossRef]
- Jee, J.; Foote, M.B.; Lumish, M.; Stonestrom, A.J.; Wills, B.; Narendra, V.; Avutu, V.; Murciano-Goroff, Y.R.; Chan, J.E.; Derkach, A.; et al. Chemotherapy and COVID-19 Outcomes in Patients with Cancer. J. Clin. Oncol. 2020, 38, 3538–3546. [Google Scholar] [CrossRef] [PubMed]
- Khusid, J.; Becerra, A.Z.; Gallante, B.; Sadiq, A.S.; Atallah, W.M.; Badani, K.K.; Gupta, M. Cancer, Mortality, and Acute Kidney Injury among Hospitalized Patients with SARS-CoV-2 Infection. Asian Pac. J. Cancer Prev. 2021, 22, 517–522. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Zhu, L.; Zhu, H.; Li, X.; Huang, Y.; Gu, C.; Bush, H.; Chung, C.; Zhang, G.-Q. Characterizing cancer and COVID-19 outcomes using electronic health records. PLoS ONE 2022, 17, e0267584. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.Y.W.; Cazier, J.-B.; Angelis, V.; Arnold, R.; Bisht, V.; Campton, N.A.; Chackathayil, J.; Cheng, V.W.T.; Curley, H.M.; Fittall, M.W.T.; et al. COVID-19 mortality in patients with cancer on chemotherapy or other anticancer treatments: A prospective cohort study. Lancet 2020, 395, 1919–1926. [Google Scholar] [CrossRef]
- Lièvre, A.; Turpin, A.; Ray-Coquard, I.; Le Malicot, K.; Thariat, J.; Ahle, G.; Neuzillet, C.; Paoletti, X.; Bouché, O.; Aldabbagh, K.; et al. Risk factors for Coronavirus Disease 2019 (COVID-19) severity and mortality among solid cancer patients and impact of the disease on anticancer treatment: A French nationwide cohort study (GCO-002 CACOVID-19). Eur. J. Cancer 2020, 141, 62–81. [Google Scholar] [CrossRef]
- Marta, G.N.; Bonadio, R.C.; Sejas, O.N.E.; Watarai, G.; Machado, M.C.M.; Frasson, L.T.; Moniz, C.M.V.; Ito, R.K.D.L.; Peixoto, D.; Hoff, C.O.; et al. Outcomes and Prognostic Factors in a Large Cohort of Hospitalized Cancer Patients with COVID-19. JCO Glob. Oncol. 2021, 7, 1084–1092. [Google Scholar] [CrossRef]
- Oh, T.K.; Song, I.-A. Impact of coronavirus disease-2019 on chronic respiratory disease in South Korea: An NHIS COVID-19 database cohort study. BMC Pulm. Med. 2021, 21, 12. [Google Scholar] [CrossRef]
- Özdemir, N.; Dizdar, Ö.; Yazıcı, O.; Aksoy, S.; Dede, D.S.; Budakoğlu, B.; Metan, G.; Alp, A.; Budakoğlu, I.I.; Öksüzoğlu, B.; et al. Clinical features and outcomes of COVID-19 in patients with solid tumors: Turkish National Registry Data. Int. J. Cancer 2020, 148, 2407–2415. [Google Scholar] [CrossRef]
- Preda, A.; Ciuleanu, T.; Kubelac, P.; Todor, N.; Balacescu, O.; Achimas-Cadariu, P.; Iancu, D.; Mocan, C.; Bandi-Vasilica, M.; Lupse, M.; et al. Outcomes of patients with cancer infected with SARS-CoV-2: Results from the Ion Chiricuţă Oncology Institute series. ESMO Open 2022, 7, 100423. [Google Scholar] [CrossRef]
- Song, K.; Gong, H.; Xu, B.; Dong, X.; Li, L.; Hu, W.; Wang, Q.; Xie, Z.; Rao, Z.; Luo, Z.; et al. Association between recent oncologic treatment and mortality among patients with carcinoma who are hospitalized with COVID-19: A multicenter study. Cancer 2020, 127, 437–448. [Google Scholar] [CrossRef]
- Várnai, C.; Palles, C.; Arnold, R.; Curley, H.M.; Purshouse, K.; Cheng, V.W.T.; Booth, S.; Campton, N.A.; Collins, G.P.; Hughes, D.J.; et al. Mortality Among Adults With Cancer Undergoing Chemotherapy or Immunotherapy and Infected With COVID-19. JAMA Netw. Open 2022, 5, e220130. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Berger, N.A.; Xu, R. Analyses of Risk, Racial Disparity, and Outcomes Among US Patients With Cancer and COVID-19 Infection. JAMA Oncol. 2021, 7, 220. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Kaelber, D.C.; Xu, R.; Berger, N.A. Breakthrough SARS-CoV-2 Infections, Hospitalizations, and Mortality in Vaccinated Patients with Cancer in the US between December 2020 and November 2021. JAMA Oncol. 2022, 8, 1027. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.; Choi, H.; Lee, S.-K.; Chung, S.J.; Yeo, Y.; Shin, Y.M.; Park, D.W.; Park, T.S.; Moon, J.-Y.; Kim, T.-H.; et al. Risk of Coronavirus Disease 2019 Occurrence, Severe Presentation, and Mortality in Patients with Lung Cancer. Cancer Res. Treat. 2021, 53, 678–684. [Google Scholar] [CrossRef]
- Yarza, R.; Bover, M.; Paredes, D.; López-López, F.; Jara-Casas, D.; Castelo-Loureiro, A.; Baena, J.; Mazarico, J.M.; Folgueira, M.D.; Meléndez-Carmona, M.; et al. SARS-CoV-2 infection in cancer patients undergoing active treatment: Analysis of clinical features and predictive factors for severe respiratory failure and death. Eur. J. Cancer 2020, 135, 242–250. [Google Scholar] [CrossRef]
- Zorzi, M.; Guzzinati, S.; Avossa, F.; Fedeli, U.; Calcinotto, A.; Rugge, M. SARS-CoV-2 Infection in Cancer Patients: A Population-Based Study. Front. Oncol. 2021, 11, 4146. [Google Scholar] [CrossRef]
- Arayici, M.E.; Kipcak, N.; Kayacik, U.; Kelbat, C.; Keskin, D.; Kilicarslan, M.E.; Kilinc, A.V.; Kirgoz, S.; Kirilmaz, A.; Kizilkaya, M.A.; et al. Effects of SARS-CoV-2 infections in patients with cancer on mortality, ICU admis-sion and incidence: A systematic review with meta-analysis involving 709,908 participants and 31,732 cancer patients. J. Cancer Res. Clin. Oncol. 2022, 14, 1–14. [Google Scholar]
- Khoury, E.; Nevitt, S.; Madsen, W.R.; Turtle, L.; Davies, G.; Palmieri, C. Differences in Outcomes and Factors Associated with Mortality among Patients with SARS-CoV-2 Infection and Cancer Compared with Those without Cancer: A Systematic Review and Meta-analysis. JAMA Netw. Open 2022, 5, e2210880. [Google Scholar] [CrossRef]
- Tang, L.V.; Hu, Y. Poor clinical outcomes for patients with cancer during the COVID-19 pandemic. Lancet Oncol. 2020, 21, 862–864. [Google Scholar] [CrossRef]
- Pala, L.; Conforti, F.; Saponara, M.; De Pas, T.; Giugliano, F.; Salè, E.O.; Jemos, C.; Rubatto, M.; Agostini, A.; Quaglino, P.; et al. Data of Italian Cancer Centers from two regions with high incidence of SARS CoV-2 infection provide evidence for the successful management of patients with locally advanced and metastatic melanoma treated with immunotherapy in the era of COVID-19. Semin. Oncol. 2020, 47, 302–304. [Google Scholar] [CrossRef] [PubMed]
- Pinato, D.J.; Tabernero, J.; Bower, M.; Scotti, L.; Patel, M.; Colomba, E.; Dolly, S.; Loizidou, A.; Chester, J.; Mukherjee, U.; et al. Prevalence and impact of COVID-19 sequelae on treatment and survival of patients with cancer who recovered from SARS-CoV-2 infection: Evidence from the OnCovid retrospective, multicentre registry study. Lancet Oncol. 2021, 22, 13. [Google Scholar] [CrossRef]
- Jones, D.; Neal, R.D.; Duffy, S.R.; Scott, S.E.; Whitaker, K.L.; Brain, K. Impact of the COVID-19 pandemic on the symptomatic diagnosis of cancer: The view from primary care. The Lancet Oncology 2020, 21, 3. [Google Scholar] [CrossRef]
- London, J.W.; Fazio-Eynullayeva, E.; Palchuk, M.B.; Sankey, P.; McNair, C. Effects of the COVID-19 Pandemic on Can-cer-Related Patient Encounters. JCO Clin. Cancer Inform. 2019, 9, 657–665. [Google Scholar]
- Cantini, L.; Mentrasti, G.; Russo, G.; Signorelli, D.; Pasello, G.; Rijavec, E.; Russano, M.; Antonuzzo, L.; Rocco, D.; Giusti, R.; et al. Evaluation of COVID-19 impact on DELAYing diagnostic-therapeutic pathways of lung cancer patients in Italy (COVID-DELAY study): Fewer cases and higher stages from a real-world scenario. ESMO Open 2022, 7, 100406. [Google Scholar] [CrossRef]
- Sha, Z.; Chang, K.; Mi, J.; Liang, Z.; Hu, L.; Long, F.; Shi, H.; Lin, Z.; Wang, X.; Pei, X. The impact of the COVID-19 pandemic on lung cancer patients. Ann. Palliat. Med. 2020, 9, 3373–3378. [Google Scholar] [CrossRef]
- Bertaglia, V.; Reale, M.L.; Bironzo, P.; Palesandro, E.; Mariniello, A.; Leone, G.; Tabbò, F.; Bungaro, M.; Audisio, M.; Rapetti, S.; et al. Italian survey on the clinical management of non-small cell lung cancer patients during the COVID-19 pandemic: A lesson for the second wave. Crit. Rev. Oncol. 2020, 157, 103189. [Google Scholar] [CrossRef]
- Pinato, D.J.; Ferrante, D.; Aguilar-Company, J.; Bower, M.; Salazar, R.; Mirallas, O.; Sureda, A.; Bertuzzi, A.; Brunet, J.; Lambertini, M.; et al. Vaccination against SARS-CoV-2 protects from morbidity, mor-tality and sequelae from COVID-19 in patients with cancer. Eur. J. Cancer 2022, 12, 64–74. [Google Scholar] [CrossRef]
- Siddiqui, S.; Alhamdi, H.W.S.; Alghamdi, H.A. Recent Chronology of COVID-19 Pandemic. Front. Public Health 2022, 10, 778037. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author/Year | Type of Study | Country | N° Lung Cancer pts | Follow Up | Risk of COVID (HR, 95%CI) | Severe Disease | Mortality % | Quality | Bias (ROBINS) |
|---|---|---|---|---|---|---|---|---|---|
| Assad et al., 2020 [10] | Retrospective study | France | 42 | Median 25 days | NR | NR | ↑ | 6 | Low |
| Aveyard et al., 2021 [11] | Retrospective cohort study | UK | 60 | NR | NR | ↑ * | ↑ * | 5 | Low |
| Basse et al., 2020 [12] | Prospective study | France | 18 | 28 days | NR | NR | ↑ # | 6 | Low |
| Beltramo et al., 2020 [13] | Retrospective cohort study | France | 977 | NR | NR | = * | ↑ * | 5 | Low |
| Benderra et al., 2021 [14] | Retrospective cohort study | France | 85 | 30 days | NR | NR | ↑ * | 6 | Low |
| Bernard et al., 2021 [15] | Retrospective cohort study | France | 873 | NR | NR | NR | ↑ * | 5 | Low |
| Chen et al., 2022 [16] | Cohort study | USA | 10,346 | NR | NR | NR | ↑ * | 5 | Low |
| Dai et al., 2020 [17] | Retrospective multicenter study | China | 31 | 53 days | NR | ↑ | ↑ | 7 | Low |
| De Joode et al., 2022 [18] | Prospective cohort study | Netherland | 117 | NR | NR | NR | ↑ $ | 6 | Low |
| Farooque et al., 2021 [19] | Prospective study | Pakistan | 159 | At least 30 days | NR | NR | ↑ *$ | 6 | Moderate |
| Fernandes et al., 2021 [20] | Retrospective cross-sectional study | Brazil | 18 | NR | NR | NR | ↑ *$ | 5 | Low |
| Ferrari et al., 2022 [21] | Prospective study | Brazil | 16 | Median 61 days | NR | NR | ↑ # | 7 | Low |
| Garassino et al., 2020 [22] | Cross-sectional and longitudinal cohort study | International | 200 | Median 15 days (IQR 8–24) | NR | NR | ↑ ** | 6 | Low |
| Jee et al., 2020 [23] | Retrospective observational study | USA | 29 | NR | NR | ↑ * | NR | 5 | Low |
| Khusid et al., 2021 [24] | Retrospective cohort study | USA | 14 | NR | NR | = * | ↑ * | 5 | Low |
| Kim et al., 2022 [25] | Retrospective study | USA | 887 | At least 30 days | NR | ↑ * | ↑ * | 7 | Low |
| Lee et al., 2020 [26] | Prospective observational study | UK | 90 | Max 39 days | NR | NR | = | 7 | Low |
| Lièvre et al., 2020 [27] | Retro-prospective cohort study | France | 311 | Median 34 days | NR | ↑ * | ↑ *,° | 7 | Low |
| Nader Marta et al., 2021 [28] | Retrospective, single-institute cohort study | Brazil | 42 | NR | NR | NR | ↑ *$ | 6 | Low |
| Oh et al., 2021 [29] | Retrospective study | South Korea | 769 | NR | NR | NR | ↑ *$ | 6 | Low |
| Ozdemir et al., 2021 [30] | Retrospective study | Turkey | 157 | Median 50 days (min 1- max 74) | NR | NR | ↑ *$ | 7 | Low |
| Preda et al., 2022 [31] | Retrospective study | Romania | 66 | NR | NR | NR | Not significant | 6 | Low |
| Song et al., 2020 [32] | Retrospective multicenter study | China | 61 | NR | NR | NR | ↑ $ | 8 | Low |
| Varnai et al., 2022 [33] | Prospective cohort study | UK | 265 | NR | NR | NR | ↑ *$ | 5 | Low |
| Wang et al., 2020 [34] | Retrospective case-control study | USA | 140 | NR | ↑ * | NR | NR | 5 | Low |
| Wang et al., 2022 [35] | Retrospective cohort study | USA | 2849 | NR | ↑ | NR | NR | 6 | Low |
| Yang et al., 2021 [36] | Retrospective cohort study | South Korea | 362 | NR | ↑ * | ↑ * | ↑ * | 4 | Low |
| Yarza et al., 2020 [37] | Retro-prospective study | Spain | 17 | NR | NR | ↑ * | ↑ *$ | 6 | Low |
| Zorzi et al., 2021 [38] | Retrospective population-based study | Italy | 2256 | NR | = * | NR | ↑ *^ | 6 | Low |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oldani, S.; Petrelli, F.; Dognini, G.; Borgonovo, K.; Parati, M.C.; Ghilardi, M.; Dottorini, L.; Cabiddu, M.; Luciani, A. COVID-19 and Lung Cancer Survival: An Updated Systematic Review and Meta-Analysis. Cancers 2022, 14, 5706. https://doi.org/10.3390/cancers14225706
Oldani S, Petrelli F, Dognini G, Borgonovo K, Parati MC, Ghilardi M, Dottorini L, Cabiddu M, Luciani A. COVID-19 and Lung Cancer Survival: An Updated Systematic Review and Meta-Analysis. Cancers. 2022; 14(22):5706. https://doi.org/10.3390/cancers14225706
Chicago/Turabian StyleOldani, Simone, Fausto Petrelli, Giuseppina Dognini, Karen Borgonovo, Maria Chiara Parati, Mara Ghilardi, Lorenzo Dottorini, Mary Cabiddu, and Andrea Luciani. 2022. "COVID-19 and Lung Cancer Survival: An Updated Systematic Review and Meta-Analysis" Cancers 14, no. 22: 5706. https://doi.org/10.3390/cancers14225706
APA StyleOldani, S., Petrelli, F., Dognini, G., Borgonovo, K., Parati, M. C., Ghilardi, M., Dottorini, L., Cabiddu, M., & Luciani, A. (2022). COVID-19 and Lung Cancer Survival: An Updated Systematic Review and Meta-Analysis. Cancers, 14(22), 5706. https://doi.org/10.3390/cancers14225706