
Immune Response and Outcome of High-Risk Neuroblastoma Patients Immunized with Anti-Idiotypic Antibody Ganglidiomab: Results from Compassionate-Use Treatments

 , ,
, , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Patient Characteristics, Vaccinations and Side Effect Subsection
3.2. Side Effects
3.3. Immune Response
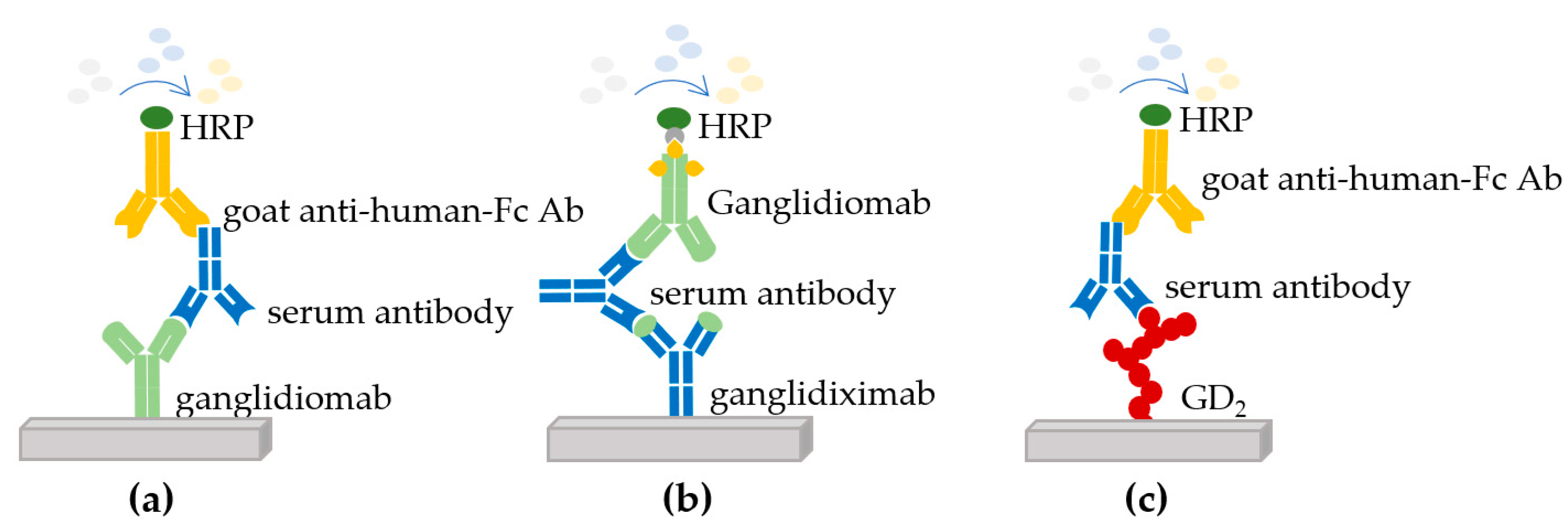
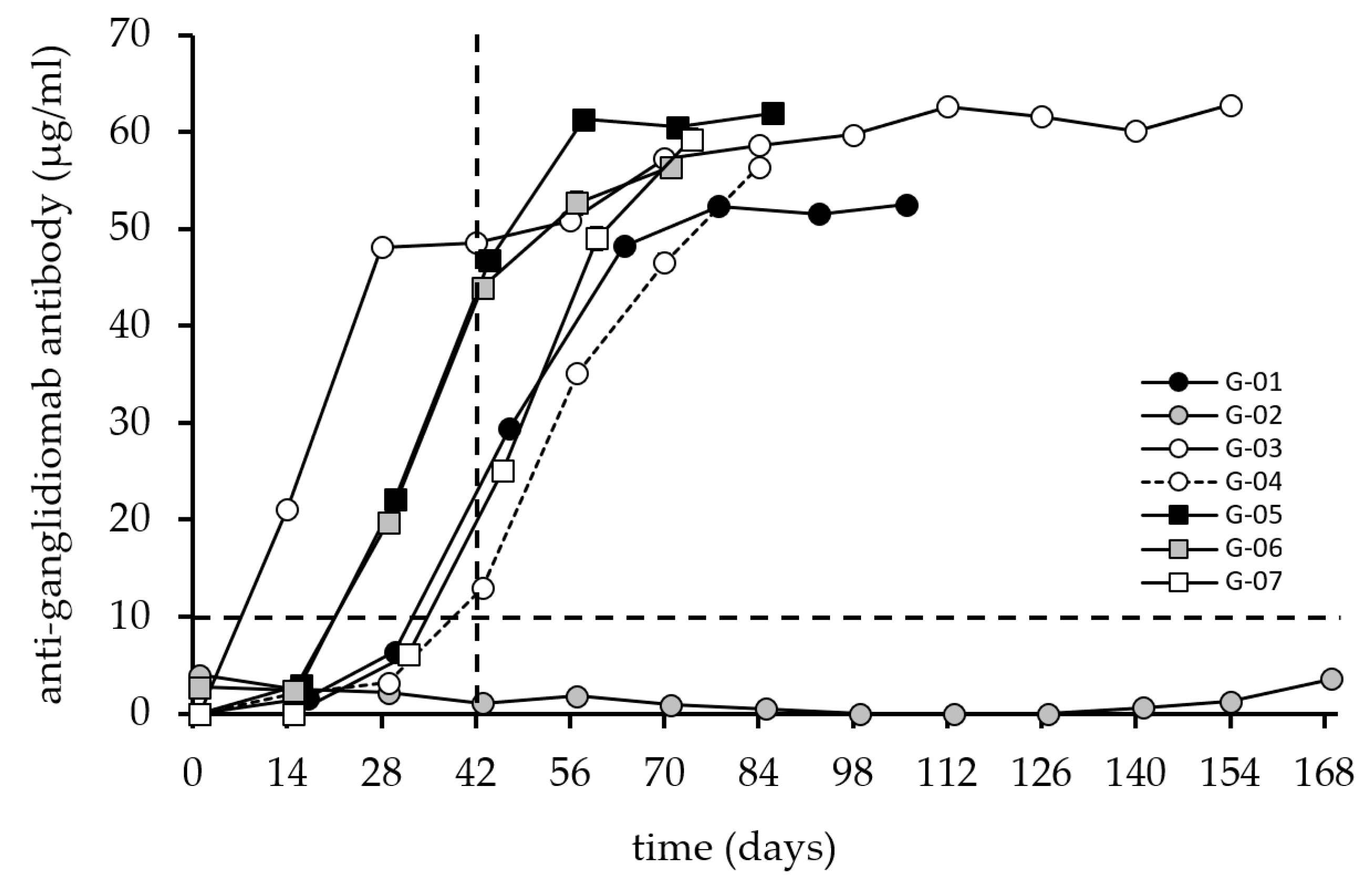
3.3.1. Anti-Ganglidiomab Immune Response
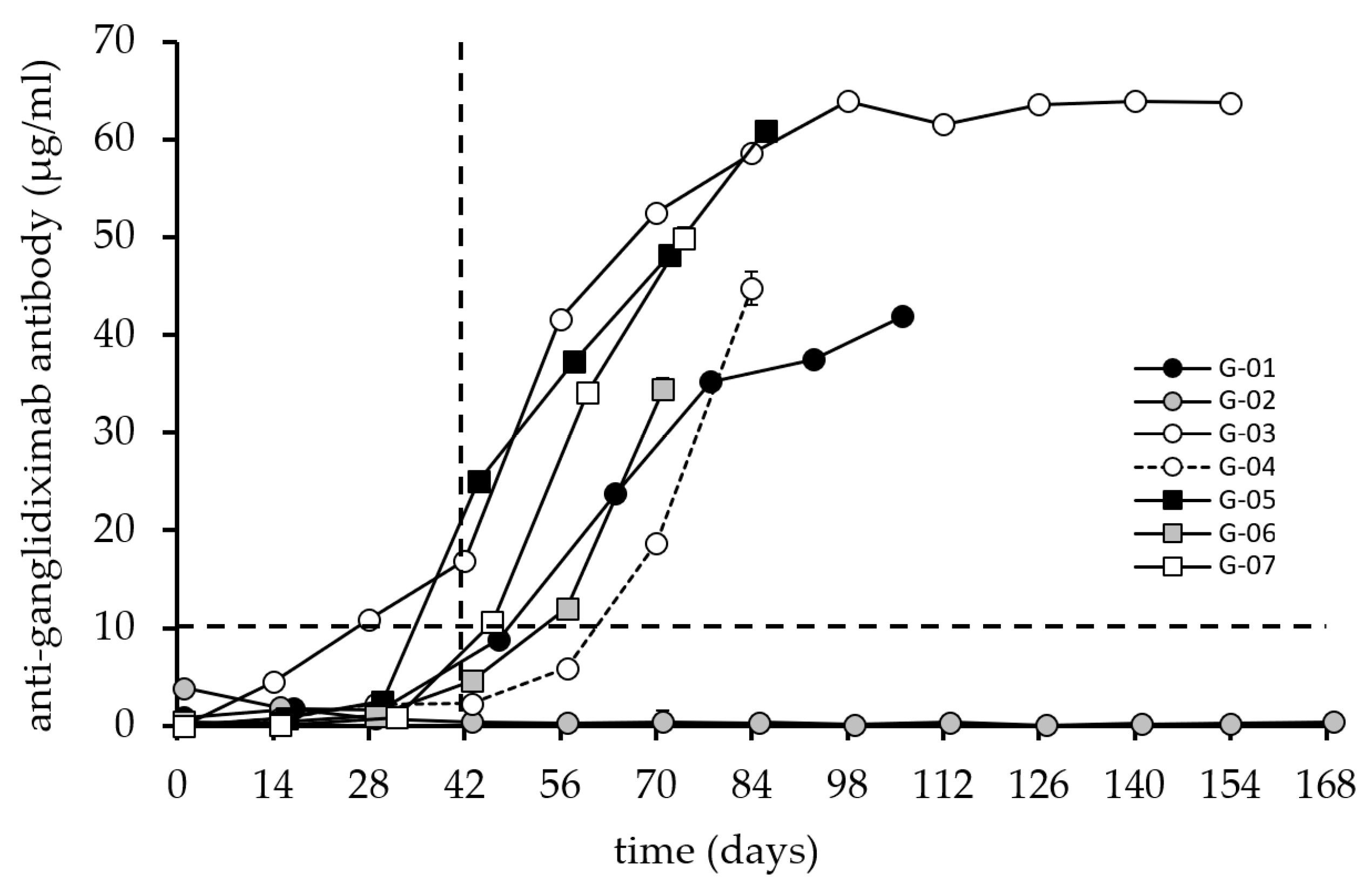
3.3.2. Anti-Ganglidiximab Immune Response
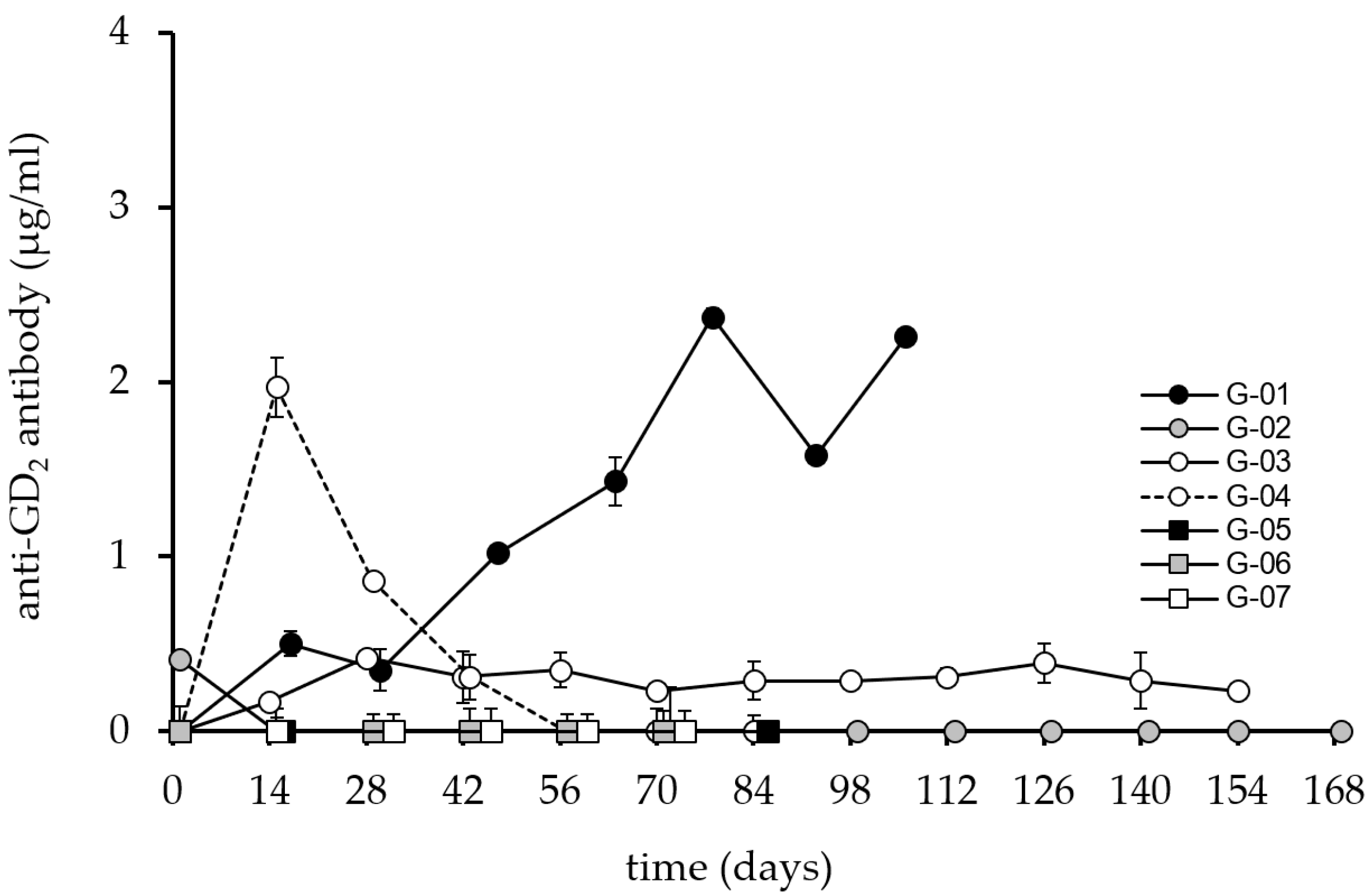
3.3.3. Anti-GD2 Immune Response
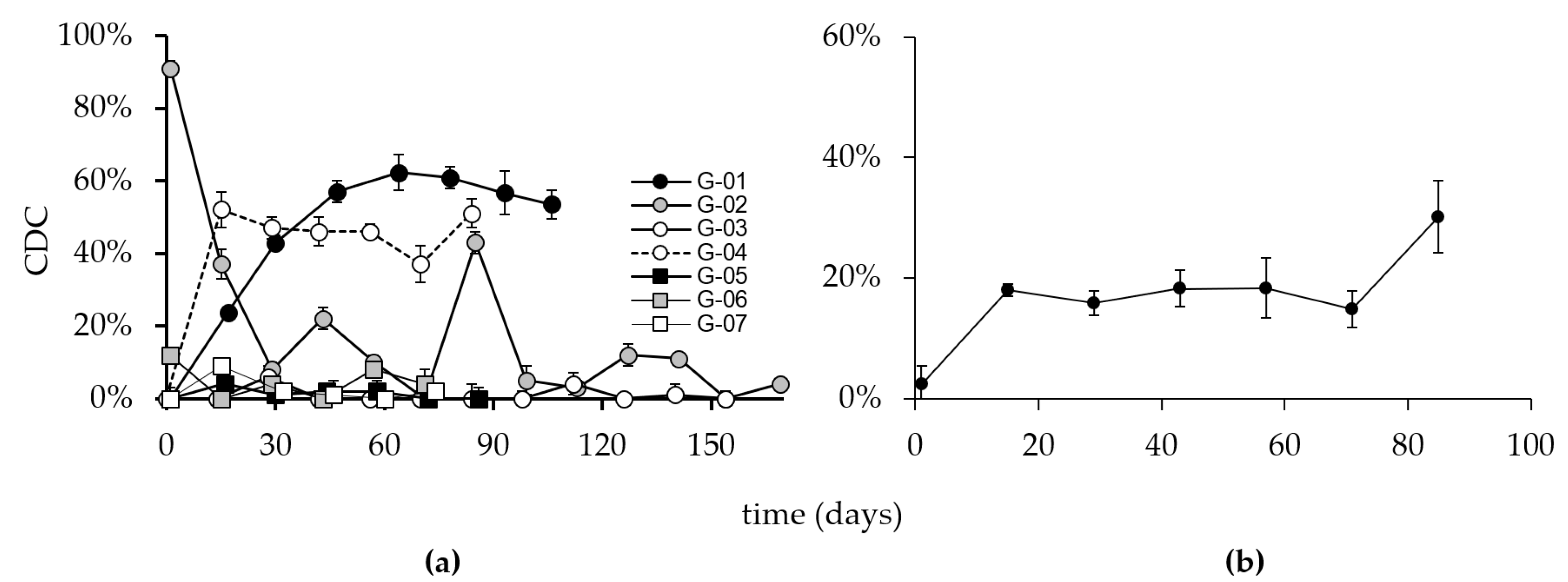
3.3.4. Complement Dependent Cytotoxicity
3.3.5. Survival of Immunized Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Armideo, E.; Callahan, C.; Madonia, L. Immunotherapy for High-Risk Neuroblastoma: Management of Side Effects and Complications. J. Adv. Pract. Oncol. 2017, 8, 44–55. [Google Scholar] [PubMed]
- Thorsten, S.; Hero, B.; Schulte, J.H.; Deubzer, H.; Hundsdoerfer, P.; Schweinitz, D.; Fuchs, J.; Schmidt, M.; Prasad, V.; Krug, B.; et al. GPOH Guidelines for Diagnosis and Treatment of Patients with Neuroblastic Tumors. Klin. Pediatr. 2017, 229, 147–167. [Google Scholar]
- MacFarland, S.; Bagatell, R. Advances in neuroblastoma therapy. Curr. Opin. Pediatr. 2019, 31, 14–21. [Google Scholar] [CrossRef]
- Lode, H.N.; Schmidt, M.; Seidel, D.; Huebener, N.; Brackrock, D.; Bleeke, M.; Reker, D.; Brandt, S.; Mueller, H.-P.; Helm, C. Vaccination with anti-idiotype antibody ganglidiomab mediates a GD(2)-specific anti-neuroblastoma immune response. Cancer Immunol. Immunother. 2013, 62, 999–1010. [Google Scholar] [CrossRef] [PubMed]
- Ladenstein, R.; Pötschger, U.; Valteau-Couanet, D.; Luksch, R.; Castel, V.; Ash, S.; Laureys, G.; Brock, P.; Michon, J.M.; Owens, C.; et al. Investigation of the Role of Dinutuximab Beta-Based Immunotherapy in the SIOPEN High-Risk Neuroblastoma 1 Trial (HR-NBL1). Cancers 2020, 12, 309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matthay, K.K.; Maris, J.M.; Schleiermacher, G.; Nakagawara, A.; Mackall, C.L.; Diller, L. Neuroblastoma. Nat. Rev. Dis. Primers 2016, 2, 16078. [Google Scholar] [CrossRef] [PubMed]
- Pinto, N.R.; Applebaum, M.A.; Volchenboum, S.L.; Matthay, K.K.; London, W.B.; Ambros, P.F.; Nakagawara, A.; Berthold, F.; Schleiermacher, G.; Park, J.R.; et al. Advances in Risk Classification and Treatment Strategies for Neuroblastoma. J. Clin. Oncol. 2015, 33, 3008–3017. [Google Scholar] [CrossRef] [Green Version]
- Wu, Z.L.; Schwartz, E.; Seeger, R.; Ladisch, S. Expression of GD2 ganglioside by untreated primary human neuroblastomas. Cancer Res. 1986, 46, 440–443. [Google Scholar] [PubMed]
- Suzuki, M.; Cheung, N.K.V. Disialoganglioside GD2 as a therapeutic target for human diseases. Expert Opin. Ther. Targets 2015, 19, 349–362. [Google Scholar] [CrossRef]
- Cheung, N.K.V.; Neely, J.E.; Landmeier, B.; Nelson, D.; Miraldi, F. Targeting of ganglioside GD2 monoclonal antibody to neuroblastoma. J. Nucl. Med. 1987, 28, 1577–1583. [Google Scholar] [PubMed]
- Garcia-Garcia, E.; Rosales, C. Signal transduction during Fc receptor-mediated phagocytosis. J. Leukoc. Biol. 2002, 72, 1092–1108. [Google Scholar] [CrossRef]
- Tong, W.; Maira, M.; Roychoudhury, R.; Galan, A.; Brahimi, F.; Gilbert, M.; Saragovi, H.U.; Cunningham, A.-M.; Josephy, S.; Pirvulescu, I.; et al. Vaccination with Tumor-Ganglioside Glycomimetics Activates a Selective Immunity that Affords Cancer Therapy. Cell Chem. Biol. 2019, 26, 1013–1026. [Google Scholar] [CrossRef] [PubMed]
- Cheung, I.Y.; Cheung, N.-K.V.; Modak, S.; Mauguen, A.; Feng, Y.; Basu, E.; Roberts, S.S.; Ragupathi, G.; Kushner, B.H. Survival Impact of Anti-GD2 Antibody Response in a Phase II Ganglioside Vaccine Trial Among Patients With High-Risk Neuroblastoma With Prior Disease Progression. J. Clin. Oncol. 2021, 39, 215–226. [Google Scholar] [CrossRef]
- Siebert, N.; Eger, C.; Seidel, D.; Jüttner, M.; Lode, H.N. Validated detection of human anti-chimeric immune responses in serum of neuroblastoma patients treated with ch14.18/CHO. J. Immunol. Method. 2014, 407, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Eger, C.; Siebert, N.; Seidel, D.; Zumpe, M.; Jüttner, M.; Brandt, S.; Müller, H.-P.; Lode, H.N. Generation and Characterization of a Human/Mouse Chimeric GD2-Mimicking Anti-Idiotype Antibody Ganglidiximab for Active Immunotherapy against Neuroblastoma. PLoS ONE 2016, 11, e0150479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siebert, N.; Seidel, D.; Eger, C.; Jüttner, M.; Lode, H.N. Functional bioassays for immune monitoring of high-risk neuroblastoma patients treated with ch14.18/CHO anti-GD2 antibody. PLoS ONE 2014, 9, e0107692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brodeur, G.M.; Seeger, R.C.; Barrett, A.; Berthold, F.; Castleberry, R.P.; Bernardi, G.D.; Evans, A.E.; Favrot, M.; Freeman, A.I. International criteria for diagnosis, staging and response to treatment in patients with neuroblastoma. Prog. Clin. Biol. Res. 1988, 271, 509–524. [Google Scholar] [CrossRef] [Green Version]
- Sait, S.; Modak, S. Anti-GD2 immunotherapy for neuroblastoma. Expert Rev. Anticancer Ther. 2017, 17, 889–904. [Google Scholar] [CrossRef]
- Ladenstein, R.; Pötschger, U.; Valteau-Couanet, D.; Luksch, R.; Castel, V.; Yaniv, I.; Lode, H.N. Interleukin 2 with anti-GD2 antibody ch14.18/CHO (dinutuximab beta) in patients with high-risk neuroblastoma (HR-NBL1/SIOPEN): A multicentre, randomised, phase 3 trial. Lancet Oncol. 2018, 19, 1617–1629. [Google Scholar] [CrossRef]
- Bremm, M.; Cappel, C.; Erben, S.; Jarisch, A.; Schumm, M.; Arendt, A.; Huenecke, S. Generation and flow cytometric quality control of clinical-scale TCRalphabeta/CD19-depleted grafts. Cytom. B Clin. Cytom. 2017, 92, 126–135. [Google Scholar] [CrossRef] [Green Version]
- Illhardt, T.; Toporski, J.; Feuchtinger, T.; Turkiewicz, D.; Teltschik, H.M.; Ebinger, M.; Lang, P. Haploidentical Stem Cell Transplantation for Refractory/Relapsed Neuroblastoma. Biol. Blood Marrow Transpl. 2018, 24, 1005–1012. [Google Scholar] [CrossRef] [PubMed]
- Corre, E.; Carmagnat, M.; Busson, M.; Latour, R.P.; Robin, M.; Ribaud, P.; Toubert, A.; Rabian, C.; Socié, G. Long-term immune deficiency after allogeneic stem cell transplantation: B-cell deficiency is associated with late infections. Haematologica 2010, 95, 1025–1029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- London, W.B.; Bagatell, R.; Weigel, B.J.; Fox, E.; Guo, D.J.; Ryn, C.V.; Naranjo, A.; Park, J.R. Historical time to disease progression and progression-free survival in patients with recurrent/refractory neuroblastoma treated in the modern era on Children’s Oncology Group early-phase trials. Cancer 2017, 123, 4914–4923. [Google Scholar] [CrossRef] [PubMed]
- Jason-Moller, L.; Murphy, M.; Bruno, J. Overview of Biacore systems and their applications. Curr. Protoc. Protein Sci. 2006, 45, 19-13. [Google Scholar] [CrossRef] [PubMed]
- Schneider, C.S.; Bhargav, A.G.; Perez, J.G.; Wadajkar, A.S.; Winkles, J.A.; Woodworth, G.F.; Kim, A.J. Surface plasmon resonance as a high throughput method to evaluate specific and non-specific binding of nanotherapeutics. J. Control Release. 2015, 219, 331–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrovsky, N. Comparative Safety of Vaccine Adjuvants: A Summary of Current Evidence and Future Needs. Drug Saf. 2015, 38, 1059–1074. [Google Scholar] [CrossRef] [PubMed]
- Pulendran, B.; Arunachalam, P.S.; O’Hagan, D.T. Emerging concepts in the science of vaccine adjuvants. Nat. Rev. Drug Discov. 2021, 20, 454–475. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.C.; Diveley, J.P.; Savary, J.R.; Jensen, F.C. Adjuvant activity of incomplete Freund’s adjuvant. Adv. Drug Deliv. Rev. 1998, 32, 173–186. [Google Scholar] [CrossRef] [PubMed]
- Vetvicka, V.; Vannucci, L.; Sima, P. Beta-glucan as a new tool in vaccine development. Scand J. Immunol. 2020, 91, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Fest, S.; Huebener, N.; Weixler, S.; Bleeke, M.; Zeng, Y.; Strandsby, A.; Lode, H.N. Characterization of GD2 peptide mimotope DNA vaccines effective against spontaneous neuroblastoma metastases. Cancer Res. 2006, 66, 10567–10575. [Google Scholar] [CrossRef] [Green Version]
- Bleeke, M.; Fest, S.; Huebener, N.; Landgraf, C.; Schraven, B.; Gaedicke, G.; Volkmer, R.; Lode, H.N. Systematic amino acid substitutions improved efficiency of GD(2)-peptide mimotope vaccination against neuroblastoma. Eur. J. Cancer 2009, 45, 2915–2921. [Google Scholar] [CrossRef]
- Hilpert, K.; Winkler, D.F.; Hancock, R.E. Peptide arrays on cellulose support: SPOT synthesis, a time and cost efficient method for synthesis of large numbers of peptides in a parallel and addressable fashion. Nat. Protoc. 2007, 2, 1333–1349. [Google Scholar] [CrossRef] [PubMed]
- Knittelfelder, R.; Riemer, A.B.; Jensen-Jarolim, E. Mimotope vaccination-from allergy to cancer. Expert Opin. Biol. Ther. 2009, 9, 493–506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fest, S.; Hilt, K.; Huebener, N.; Zeng, Y.; Strandsby, A.; Weixler, S.; Lode, H.N. GD2 peptide mimotope DNA vaccines for anti-neuroblastoma immunotherapy. Blood 2004, 104, 379a–380a. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Age at Diagnosis | Sex | Relapse | BSA 1 | Stage 2 | MYCN Amplification |
|---|---|---|---|---|---|---|
| G-01 | 3 years | M | No | 0.9 m2 | 4 | no |
| G-02 | 25 years | F | Yes | 1.5 m2 | 4 | no |
| G-03 | 1 month | M | No | 0.6 m2 | 4 | yes |
| G-04 | 3 years | F | Yes | 0.6 m2 | 4 | unknown |
| G-05 | 6 months | M | No | 0.5 m2 | 4 | yes |
| G-06 | 7 years | F | No | 1.1 m2 | 4 | yes |
| G-07 | 5 years | M | No | 0.8 m2 | 4 | yes |
| Patient | Time Interval Diagnosis-First Dose | Number of Doses Received |
|---|---|---|
| G-01 | 29 months: 10/2010–11/2012 | 8 |
| G-02 | 40 months: 01/2010–05/2013 | 22 |
| G-03 | 34 months: 05/2011–03/2014 | 12 |
| G-04 | 33 months: 02/2012–11/2014 | 7 |
| G-05 | 22 months: 01/2013–11/2014 | 7 |
| G-06 | 18 months: 05/2013–11/2014 | 6 |
| G-07 | 29 months: 06/2012–11/2014 | 6 |
| Patient | Date of Diagnosis | Date of First Vaccination | Date of Last Vaccination | Date of Last Follow-Up | Range from First Dose to Last Follow-Up | Patient Status |
|---|---|---|---|---|---|---|
| G-01 | 10/2010 | 20/11/2012 | 07/03/2013 | 26/07/2019 | 80 mo, 7 d | NED |
| G-02 1 | 01/2010 | 22/05/2013 | 12/03/2014 | 10/10/2014 2 | 16 mo, 19 d | Dead 3 |
| G-03 | 05/2011 | 25/03/2014 | 26/08/2014 | 28/06/2019 | 63 mo, 4 d | NED |
| G-04 1 | 02/2012 | 12/11/2014 | 07/01/2015 | 31/07/2019 | 56 mo, 20 d | NED |
| G-05 | 01/2013 | 03/11/2014 | 21/01/2015 | 18/11/2018 | 48 mo, 16 d | NED |
| G-06 | 05/2013 | 17/11/2014 | 26/01/2015 | 01/08/2019 | 56 mo, 16 d | NED |
| G-07 | 06/2012 | 14/11/2014 | 09/02/2015 | 01/07/2015 | 7 mo, 18 d | NED |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klingel, L.; Siebert, N.; Troschke-Meurer, S.; Zumpe, M.; Ehlert, K.; Huber, S.; Loibner, H.; Mutschlechner, O.; Lode, H.N. Immune Response and Outcome of High-Risk Neuroblastoma Patients Immunized with Anti-Idiotypic Antibody Ganglidiomab: Results from Compassionate-Use Treatments. Cancers 2022, 14, 5802. https://doi.org/10.3390/cancers14235802
Klingel L, Siebert N, Troschke-Meurer S, Zumpe M, Ehlert K, Huber S, Loibner H, Mutschlechner O, Lode HN. Immune Response and Outcome of High-Risk Neuroblastoma Patients Immunized with Anti-Idiotypic Antibody Ganglidiomab: Results from Compassionate-Use Treatments. Cancers. 2022; 14(23):5802. https://doi.org/10.3390/cancers14235802
Chicago/Turabian StyleKlingel, Leah, Nikolai Siebert, Sascha Troschke-Meurer, Maxi Zumpe, Karoline Ehlert, Stefanie Huber, Hans Loibner, Oliver Mutschlechner, and Holger N. Lode. 2022. "Immune Response and Outcome of High-Risk Neuroblastoma Patients Immunized with Anti-Idiotypic Antibody Ganglidiomab: Results from Compassionate-Use Treatments" Cancers 14, no. 23: 5802. https://doi.org/10.3390/cancers14235802
APA StyleKlingel, L., Siebert, N., Troschke-Meurer, S., Zumpe, M., Ehlert, K., Huber, S., Loibner, H., Mutschlechner, O., & Lode, H. N. (2022). Immune Response and Outcome of High-Risk Neuroblastoma Patients Immunized with Anti-Idiotypic Antibody Ganglidiomab: Results from Compassionate-Use Treatments. Cancers, 14(23), 5802. https://doi.org/10.3390/cancers14235802