
How Should We Treat Meningeal Melanocytoma? A Retrospective Analysis of Potential Treatment Strategies

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
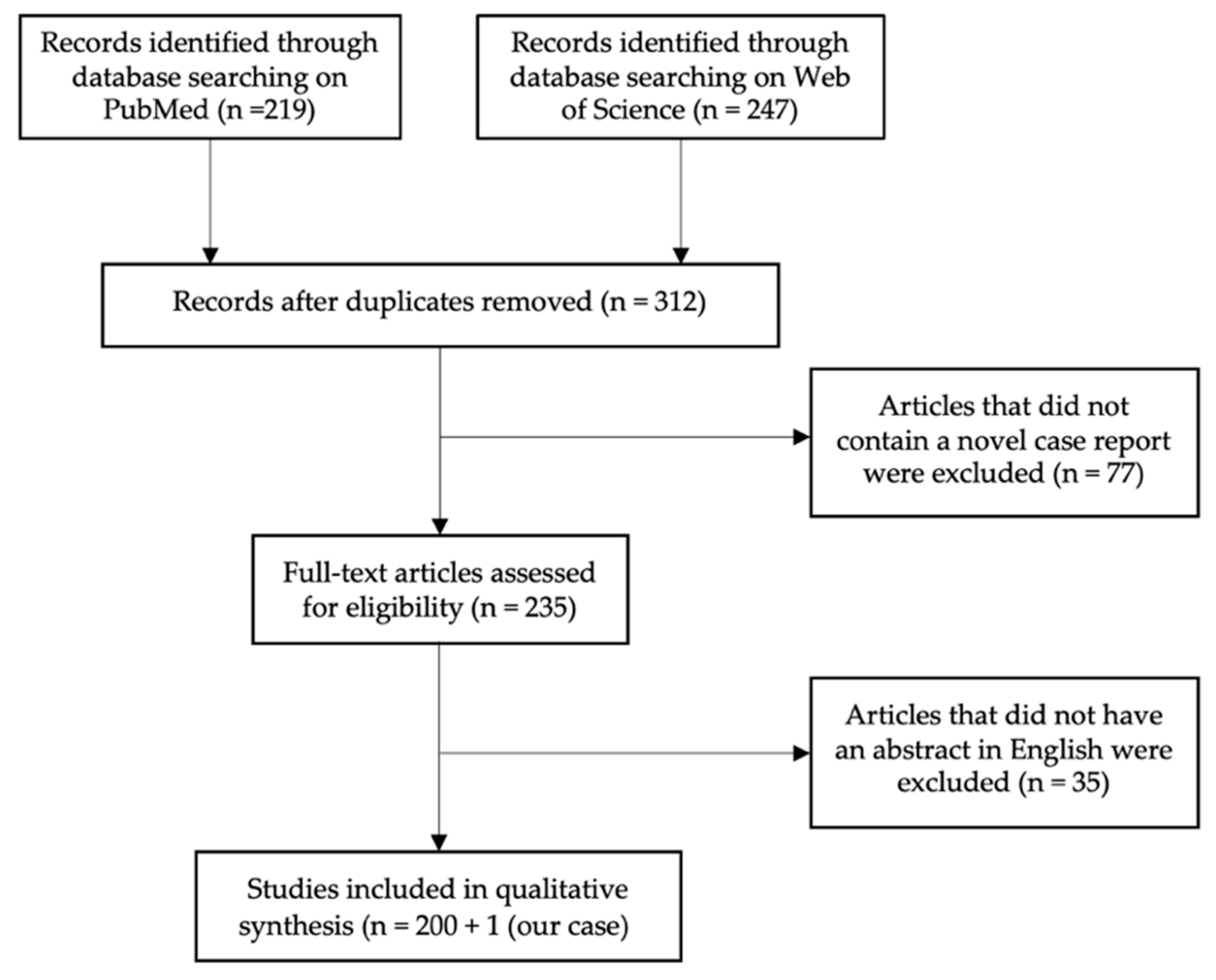
Search Strategy and Statistics
3. Results
3.1. Population
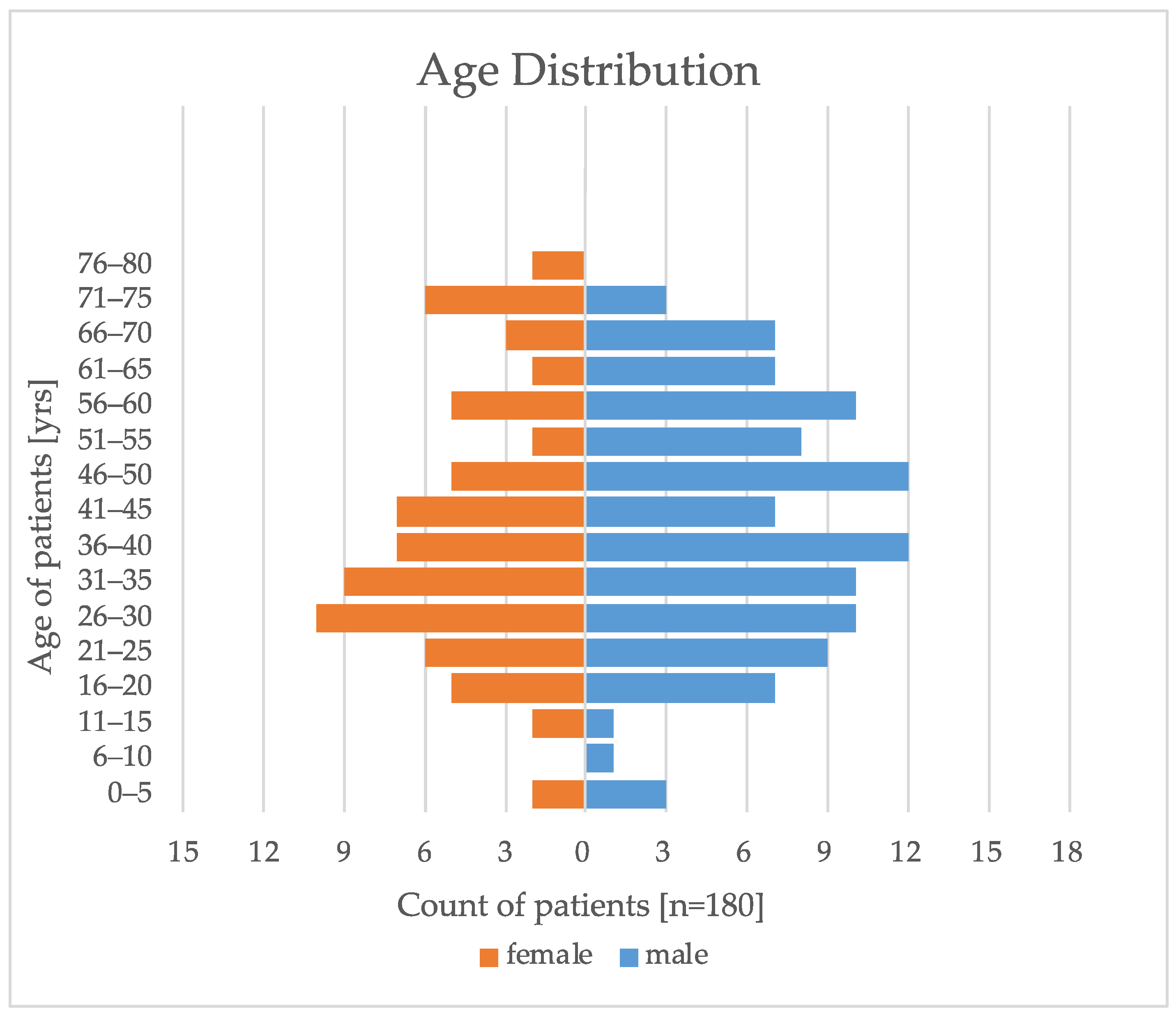
3.1.1. Age and Gender
3.1.2. Location
3.2. Treatment Strategies
3.2.1. Total Resection and Partial Resection
3.2.2. Adjuvant Therapy
3.2.3. Definite Radiotherapy and Radiosurgery

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Age | Sex | Location | Treatment | Outcome |
|---|---|---|---|---|---|
| [17] | 20 | M | Intracranial | PR + RT, Reop + RT + Temolozomide + Cisplatin + Fotemustine | Death |
| [18] | 46 | F | Intracranial | TR, Reop + Fotemustine + Temolozomide | Death |
| [19] | 38 | M | Intracranial | TR, RT + Temolozomide | Death |
| [20] | 79 | F | Spine | PR, RT + Methotrexat | Death |
| [21] | 70 | M | Spine | PR + RT + Nivolumab, Reop + Temozolomide | Death |
| [22] | 43 | F | Intracranial | TR + RT, Reop + RT + Temozolomide + Ipilimumab | Death |
| [23] | 71 | F | Spine | TR + RT, PR + RT + C. parvum + Dactinomycin + Dacarbazine | Tumor progression |
| [25] | 32 | M | Orbita | Radiosurgery + Immunotherapy | Tumor progression |
| [26] | 37 | F | Intracranial | PR, Reop + RT + Temozolomide | Death |
| [27] | 19 | F | Spine | TR, PR + RT + Pembrolizumab + Bevacizumab + Temozolomide | Death |
| [28] | 71 | F | Spine | PR + RT, Reop + C. parvum, Dimethyl Triazeno Imidazole Carboxamide + Actinomycin | Death |
| [29] | 36 | F | Spine | TR, Reop + RT + Nivolumab | Death |
| [30] | 35 | M | Orbita | PR + RT + BCNU + DTIC + Cisplatin | Tumor progression |
| [31] | 49 | M | Orbita | PR + Dacarbazine + Vincristine + Nimustine Hydrochloride | No recurrence |
3.3. Outcome
3.4. Intermediate-Grade and Malignant Transformation
4. Discussion
Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Küsters-Vandevelde, H.V.N.; Küsters, B.; van Engen-van Grunsven, A.C.H.; Groenen, P.J.T.A.; Wesseling, P.; Blokx, W.A.M. Primary Melanocytic Tumors of the Central Nervous System: A Review with Focus on Molecular Aspects. Brain Pathol. 2015, 25, 209–226. [Google Scholar] [CrossRef] [PubMed]
- Limas, C.; Tio, F.O. Meningeal Melanocytoma (“melanotic Meningioma”). Its Melanocytic Origin as Revealed by Electron Microscopy. Cancer 1972, 30, 1286–1294. [Google Scholar] [CrossRef] [PubMed]
- Demirci, A.; Kawamura, Y.; Sze, G.; Duncan, C. MR of Parenchymal Neurocutaneous Melanosis. AJNR Am. J. Neuroradiol. 1995, 16, 603–606. [Google Scholar] [PubMed]
- Malik, A.; Goyal, M.; Gambhir, M.; Patir, R.; Mishra, N.K.; Gaikwad, S.; Sharma, M.C. Imaging Appearances of Meningeal Melanocytoma. J. Clin. Neurosci. 1999, 6, 264–265. [Google Scholar] [CrossRef] [PubMed]
- Gill Naul, L.; Hise, J.H.; Bauserman, S.C.; Todd, F.D. CT and MR of Meningeal Melanocytoma. AJNR Am. J. Neuroradiol. 1991, 12, 315–316. [Google Scholar]
- Marwaha, N.; Batanian, J.R.; Coppens, J.R.; Pierson, M.J.; Richards-Yutz, J.; Ebrahimzadeh, J.; Ganguly, A.; Guzman, M.A. Subcutaneous Melanocytoma Mimicking a Lipoma: A Rare Presentation of a Rare Neoplasm with Histological, Immunohistochemical, Cytogenetic and Molecular Characterization. J. Cutan. Pathol. 2016, 43, 1186–1196. [Google Scholar] [CrossRef] [PubMed]
- Oruckaptan, H.H.; Soylemezoglu, F.; Kutluk, T.; Akalan, N. Benign Melanocytic Tumor in Infancy: Discussion on a Rare Case and Review of the Literature. Pediatr. Neurosurg. 2000, 32, 240–247. [Google Scholar] [CrossRef]
- Wang, F.; Li, X.; Chen, L.; Pu, X. Malignant Transformation of Spinal Meningeal Melanocytoma. Case Report and Review of the Literature. J. Neurosurg. Spine 2007, 6, 451–454. [Google Scholar] [CrossRef] [PubMed]
- Fagundes-Pereyra, W.J.; de Sousa, L.; Carvalho, G.T.C.; Pittella, J.E.H.; de Sousa, A.A. Meningeal Melanocytoma of the Posterior Fossa: Case Report and Literature Review. Surg. Neurol. 2005, 63, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Hino, K.; Nagane, M.; Fujioka, Y.; Shiokawa, Y. Meningeal Melanocytoma Associated with Ipsilateral Nevus of Ota Presenting as Intracerebral Hemorrhage: Case Report. Neurosurgery 2005, 56, E1376. [Google Scholar] [CrossRef]
- Alameda, F.; Lloreta, J.; Galitó, E.; Roquer, J.; Serrano, S. Meningeal Melanocytoma: A Case Report and Literature Review. Ultrastruct. Pathol. 1998, 22, 349–356. [Google Scholar] [CrossRef]
- Wen, D.-R.; Bhuta, S.; Herschman, H.R.; Gaynor, R.B.; Cochran, A.J. S-100 Protein: A Marker for Melanocytic Tumors. Ann. N. Y. Acad. Sci. 1983, 420, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Donato, R. S-100 Proteins. Cell Calcium 1986, 7, 123–145. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.H.; Goldschmidt, M.H.; McManus, P.M. A Comparative Review of Melanocytic Neoplasms. Vet. Pathol. 2002, 39, 651–678. [Google Scholar] [CrossRef]
- Pierson, M.; Marwaha, N.; Guzman, M.; Mikulec, A.A.; Coppens, J.R. Multifocal Melanocytoma of the Posterior Fossa and Subcutaneous Scalp in the Absence of Neurocutaneous Melanosis. Surg. Neurol. Int. 2016, 7, S591–S595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, N.K.; Lee, J.Y.; Wang, K.C.; Kim, D.G.; Park, S.H.; Cheon, J.E.; Phi, J.H.; Kim, S.K. Primary Atypical Melanocytoma Arising from the Cavernous Sinus in a Child. Child’s Nerv. Syst. 2015, 31, 1577–1582. [Google Scholar] [CrossRef] [PubMed]
- Doglietto, F.; Colosimo, C.; Lauriola, L.; Balducci, M.; De Bonis, P.; Montano, N.; Zadeh, G.; Maira, G.; Pallini, R. Intracranial melanocytic meningeal tumours and melanosis oculi: Case report and literature review. BMC Cancer 2012, 12, 220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- San-Miguel, T.; Navarro, L.; Sanchez-Sendra, B.; Megıas, J.; Muñoz-Hidalgo, L.; Santonja, N.; Lopez-Gines, C.; Cerda-Nicolas, M. Identification of a Novel BRCA1 Alteration in Recurrent Melanocytoma Resulting in Increased Proliferation. J. Neuropathol. Exp. Neurol. 2020, 79, 1233–1238. [Google Scholar] [CrossRef] [PubMed]
- Koch, H.J.; Roeber, S.; Zimmermann, U.W.; Schäfer, C.; Villarrubia, V.; Kuchelmeister, K.; Schachenmayr, W.; Bogdahn, U.; Steinbrecher, A. Spinale Und Zerebrale Meningeosis Eines Sekundär Malignisierten Melanozytoms Des Kleinhirnbrückenwinkels. Wien. Med. Wochenschr. 2005, 155, 360–364. [Google Scholar] [CrossRef] [PubMed]
- Bydon, A.; Gutierrez, J.A.; Mahmood, A. Meningeal Melanocytoma: An Aggressive Course for a Benign Tumor. J. Neurooncol. 2003, 64, 259–263. [Google Scholar] [CrossRef] [PubMed]
- Hean, V.; Bouleftour, W.; Ramirez, C.; Forest, F.; Boutet, C.; Rivoirard, R. Nivolumab as Adjuvant Treatment for a Spinal Melanocytoma: A Case Report. Medicine 2021, 100, e25862. [Google Scholar] [CrossRef] [PubMed]
- Küsters-Vandevelde, H.V.N.; Kruse, V.; van Maerken, T.; Boterberg, T.; Pfundt, R.; Creytens, D.; van den Broecke, C.; Machielsen, T.C.; Koelsche, C.; von Deimling, A.; et al. Copy Number Variation Analysis and Methylome Profiling of a GNAQ-Mutant Primary Meningeal Melanocytic Tumor and Its Liver Metastasis. Exp. Mol. Pathol. 2017, 102, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Verma, D.S.; Spitzer, G.; Legha, S.; McCredie, K.B. Chemoimmunotherapy for Meningeal Melanocytoma of the Thoracic Spinal Cord. Report of a Case. JAMA 1979, 242, 2435–2436. [Google Scholar] [CrossRef] [PubMed]
- Classen, J.; Hehr, T.; Paulus, W.; Plate, K.; Bamberg, M. Suprasellar Melanocytoma: A Case of Primary Radiotherapy and Review of the Literature. J. Neuro-Oncol. 2002, 58, 39–46. [Google Scholar] [CrossRef]
- Fernandez, C.; Hoeltzel, G.; Werner-Wasik, M.; Kenyon, L.C.; Shi, W. Definitive Radiotherapy for Meningeal Brainstem Melanocytoma: A Case Report. Br. J. Neurosurg. 2020, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.W.; Tran, A.Q.; North, V.S.; Zagzag, D.; Sen, C.; Kazim, M. GNA11 Mutation in an Intracranial Melanocytoma with Orbital Involvement and Nevus of Ota. Ophthalmic. Plast. Reconstr. Surg. 2021, 38, e47–e49. [Google Scholar] [CrossRef] [PubMed]
- Roser, F.; Nakamura, M.; Brandis, A.; Hans, V.; Vorkapic, P.; Samii, M. Transition from Meningeal Melanocytoma to Primary Cerebral Melanoma. Case Report. J. Neurosurg. 2004, 101, 528–531. [Google Scholar] [CrossRef]
- Deng, S.L.; Wang, Y.B.; Wang, D.H.; Zhan, S.; Jing, Y.; Guan, Y. Malignant Transformation and Metastatic Spread of Dumbbell-Shaped Meningeal Melanocytoma of the Cervical Spine: A Case Report and Literature Review. Front. Surg. 2022, 9, 789256. [Google Scholar] [CrossRef] [PubMed]
- Steinberg, J.M.; Gillespie, J.J.; MacKay, B.; Benjamin, R.S.; Leavens, M.E. Meningeal Melanocytoma with Invasion of the Thoracic Spinal Cord. Case Report. J. Neurosurg. 1978, 48, 818–824. [Google Scholar] [CrossRef] [Green Version]
- Shaikh, S.; Gupta, G.; Mohanty, C.; Deopujari, C. Spinal Nerve Root Extradural Melanocytoma Progressing to Malignant Melanoma: A Case Report with Review of Literature. Asian J. Neurosurg. 2021, 16, 394. [Google Scholar] [CrossRef]
- de Tella, O.I.; Agner, C.; Aguiar, P.H.; Herculano, M.A.; Prandini, M.N.; Stavile, J.N. Aggressive Management of Orbital Meningeal Melanocytoma. Acta Neurochir. 2003, 145, 1121–1126. [Google Scholar] [CrossRef] [PubMed]
- Sato, K.; Kubota, T.; Kodera, T.; Kitai, R.; Takeuchi, H.; Yoshida, K. Melanocytoma in the Orbital Apex. J. Neurooncol. 2009, 92, 107–110. [Google Scholar] [CrossRef] [PubMed]
- Hamasaki, O.; Nakahara, T.; Sakamoto, S.; Kutsuna, M.; Sakoda, K. Intracranial Meningeal Melanocytoma-Case Report. Neurol. Med. Chir. 2002, 42, 504–509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurita, H.; Segawa, H.; Shin, M.; Ueki, K.; Ichi, S.; Sasaki, T.; Tago, M.; Kirino, T. Radiosurgery of Meningeal Melanocytoma. J. Neuro-Oncol. 2000, 46, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Uozumi, Y.; Kawano, T.; Kawaguchi, T.; Kaneko, Y.; Ooasa, T.; Ogasawara, S.; Yoshida, H.; Yoshida, T. Malignant Transformation of Meningeal Melanocytoma: A Case Report. Brain Tumor Pathol. 2003, 20, 21–25. [Google Scholar] [CrossRef]
- Gardiman, M.; Altavilla, G.; Marchioro, L.; Boscolo, L.; Alessio, L.; Piazza, M. Meningeal Melanocytoma: A Rare Lesion of The Central Nervous System. Tumori J. 1996, 82, 494–496. [Google Scholar] [CrossRef]
- Iida, M.; Llena, J.F.; Suarez, M.A.; Malik, S.; Weidenheim, K.M.; Lasala, P.; Hirano, A. Two Cases of Spinal Meningeal Melanocytoma. Brain Tumor Pathol. 2002, 19, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Das, A.; Ratnagopal, P.; Puvanendran, K.; Teo, J.G. Spinal Meningeal Melanocytoma with Hydrocephalus and Intracranial Superficial Siderosis. Intern. Med. J. 2001, 31, 562–564. [Google Scholar] [CrossRef]
- Hirose, T.; Horiguchi, H.; Kaneko, F.; Kusaka, K.; Morizumi, H.; Seki, K.; Sano, T. Melanocytoma of the Foramen Magnum. Pathol. Int. 1997, 47, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Clarke, D.B.; Leblanc, R.; Bertrand, G.; Quartey, G.R.; Snipes, G.J. Meningeal Melanocytoma. Report of a Case and a Historical Comparison. J. Neurosurg. 1998, 88, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Phang, I.; Elashaal, R.; Ironside, J.; Eljamel, S. Primary Cerebellopontine Angle Melanocytoma: Review. J. Neurol. Surg. Rep. 2012, 73, 025–031. [Google Scholar] [CrossRef] [PubMed]
- Sakar, M.; Erdogan, O.; Bozkurt, S.U.; Dagcinar, A. Intermediate-Grade Meningeal Melanocytoma in a 19 Months Old Child with Difficulties in Differential Diagnosis and Management. Turk. Neurosurg. 2022, 32, 166–170. [Google Scholar] [CrossRef] [PubMed]
- Perrini, P.; Caniglia, M.; Pieroni, M.; Castagna, M.; Parenti, G.F. Malignant Transformation of Intramedullary Melanocytoma: Case Report. Neurosurgery 2010, 67, E867–E869. [Google Scholar] [CrossRef]
- Gempt, J.; Buchmann, N.; Grams, A.E.; Zoubaa, S.; Schlegel, J.; Meyer, B.; Ringel, F. Black Brain: Transformation of a Melanocytoma with Diffuse Melanocytosis into a Primary Cerebral Melanoma. J. Neurooncol. 2011, 102, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Fang, J.; Li, G.; Yang, J.; Xu, Y. Primary Scattered Multifocal Melanocytomas in Spinal Canal Mimicking Neurofibromatosis. Spine J. 2016, 16, e553–e559. [Google Scholar] [CrossRef] [PubMed]
- Ferracini, R.; Gardini, G.; Brisigotti, M.; Lanzanova, G.; Manetto, V.; Lorenzini, P. Metastasizing Meningeal Melanocytoma. Tumori 1980, 66, 405–408. [Google Scholar] [CrossRef]
- Barth, A.; Pizzolato, G.P.; Berney, J. Intramedullary Meningeal Melanocytoma. Neurochirurgie 1993, 39, 188–194. [Google Scholar]
- Rades, D.; Heidenreich, F.; Tatagiba, M.; Brandis, A.; Karstens, J.H. Therapeutic Options for Meningeal Melanocytoma. Case Report. J. Neurosurg. 2001, 95, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Horn, E.M.; Nakaji, P.; Coons, S.W.; Dickman, C.A. Surgical Treatment for Intramedullary Spinal Cord Melanocytomas. J. Neurosurg. Spine 2008, 9, 48–54. [Google Scholar] [CrossRef]
- Ibáñez, J.; Weil, B.; Ayala, A.; Jimenez, A.; Acedo, C.; Rodrigo, I. Meningeal Melanocytoma: Case Report and Review of the Literature. Histopathology 1997, 30, 576–581. [Google Scholar] [CrossRef]
- Rahimi-Movaghar, V.; Karimi, M. Meningeal Melanocytoma of the Brain and Oculodermal Melanocytosis (Nevus of Ota): Case Report and Literature Review. Surg. Neurol. 2003, 59, 200–210. [Google Scholar] [CrossRef]
- Painter, T.J.; Chaljub, G.; Sethi, R.; Singh, H.; Gelman, B. Intracranial and Intraspinal Meningeal Melanocytosis. Am. J. Neuroradiol. 2000, 21, 1349–1353. [Google Scholar] [PubMed]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A Summary. Neuro. Oncol. 2021, 23, 1231–1251. [Google Scholar] [CrossRef] [PubMed]
- Navas, M.; Pascual, J.M.; Fraga, J.; Pedrosa, M.; Shakur, S.; Carrasco, R.; Martínez, P.; Manzanares, R.; Sola, R.G. Intracranial Intermediate-Grade Meningeal Melanocytoma with Increased Cellular Proliferative Index: An Illustrative Case Associated with a Nevus of Ota. J. Neurooncol. 2009, 95, 105–115. [Google Scholar] [CrossRef] [PubMed]
- Quatresooz, P.; Piérard-Franchimont, C.; Piérard, G.E. Highlighting the Immunohistochemical Profile of Melanocytomas: Review. Oncol. Rep. 2008, 19, 1367–1372. [Google Scholar]
- El-Khashab, M.; Koral, K.; Bowers, D.C.; Johnson-Welch, S.; Swift, D.; Nejat, F. Intermediate Grade Meningeal Melanocytoma of Cervical Spine. Childs Nerv. Syst. 2009, 25, 407–410. [Google Scholar] [CrossRef] [PubMed]
- Palicelli, A.; Disanto, M.G.; Panzarasa, G.; Veggiani, C.; Galizia, G.; Dal Cin, S.; Gruppioni, E.; Boldorini, R. Orbital Meningeal Melanocytoma: Histological, Immunohistochemical and Molecular Characterization of a Case and Review of the Literature. Pathol. Res. Pract. 2016, 212, 946–953. [Google Scholar] [CrossRef] [PubMed]
- van Raamsdonk, C.D.; Bezrookove, V.; Green, G.; Bauer, J.; Gaugler, L.; O’Brien, J.M.; Simpson, E.M.; Barsh, G.S.; Bastian, B.C. Frequent Somatic Mutations of GNAQ in Uveal Melanoma and Blue Naevi. Nature 2009, 457, 599–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Küsters-Vandevelde, H.V.N.; van Engen-van Grunsven, I.A.C.H.; Küsters, B.; van Dijk, M.R.C.F.; Groenen, P.J.T.A.; Wesseling, P.; Blokx, W.A.M. Improved Discrimination of Melanotic Schwannoma from Melanocytic Lesions by Combined Morphological and GNAQ Mutational Analysis. Acta Neuropathol. 2010, 120, 755–764. [Google Scholar] [CrossRef] [Green Version]
- Griewank, K.G.; Koelsche, C.; van de Nes, J.A.P.; Schrimpf, D.; Gessi, M.; Möller, I.; Sucker, A.; Scolyer, R.A.; Buckland, M.E.; Murali, R.; et al. Integrated Genomic Classification of Melanocytic Tumors of the Central Nervous System Using Mutation Analysis, Copy Number Alterations, and DNA Methylation Profiling. Clin. Cancer Res. 2018, 24, 4494–4504. [Google Scholar] [CrossRef] [Green Version]
- Koelsche, C.; Hovestadt, V.; Jones, D.T.W.; Capper, D.; Sturm, D.; Sahm, F.; Schrimpf, D.; Adeberg, S.; Böhmer, K.; Hagenlocher, C.; et al. Melanotic Tumors of the Nervous System Are Characterized by Distinct Mutational, Chromosomal and Epigenomic Profiles. Brain Pathol. 2015, 25, 202–208. [Google Scholar] [CrossRef]
- Kuznetsov, J.N.; Aguero, T.H.; Owens, D.A.; Kurtenbach, S.; Field, M.G.; Durante, M.A.; Rodriguez, D.A.; King, M.L.; Harbour, J.W. BAP1 Regulates Epigenetic Switch from Pluripotency to Differentiation in Developmental Lineages Giving Rise to BAP1-Mutant Cancers. Sci. Adv. 2019, 5, eaax1738. [Google Scholar] [CrossRef] [Green Version]
- Küsters-Vandevelde, H.V.N.; Creytens, D.; van Engen-van Grunsven, A.C.H.; Jeunink, M.; Winnepenninckx, V.; Groenen, P.J.T.A.; Küsters, B.; Wesseling, P.; Blokx, W.A.M.; Prinsen, C.F.M. SF3B1 and EIF1AX Mutations Occur in Primary Leptomeningeal Melanocytic Neoplasms; yet Another Similarity to Uveal Melanomas. Acta Neuropathol. Commun. 2016, 4, 5. [Google Scholar] [CrossRef]
- van de Nes, J.; Wrede, K.; Ringelstein, A.; Stiller, M.; Horn, S.; Sucker, A.; Möller, I.; Scholz, S.L.; Murali, R.; Gessi, M.; et al. Diagnosing a Primary Leptomeningeal Melanoma by Gene Mutation Signature. J. Invest. Dermatol. 2016, 136, 1526–1528. [Google Scholar] [CrossRef] [Green Version]
- Kinsler, V.A.; Thomas, A.C.; Ishida, M.; Bulstrode, N.W.; Loughlin, S.; Hing, S.; Chalker, J.; McKenzie, K.; Abu-Amero, S.; Slater, O.; et al. Multiple Congenital Melanocytic Nevi and Neurocutaneous Melanosis Are Caused by Postzygotic Mutations in Codon 61 of NRAS. J. Investig. Dermatol. 2013, 133, 2229–2236. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, M.; Küsters-Vandevelde, H.V.N.; Viros, A.; Groenen, P.J.T.A.; Sanchez-Laorden, B.; Gilhuis, J.H.; van Engen-van Grunsven, I.A.; Renier, W.; Schieving, J.; Niculescu-Duvaz, I.; et al. Primary Melanoma of the CNS in Children Is Driven by Congenital Expression of Oncogenic NRAS in Melanocytes. Cancer Discov. 2013, 3, 458–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salgado, C.M.; Basu, D.; Nikiforova, M.; Bauer, B.S.; Johnson, D.; Rundell, V.; Grunwaldt, L.J.; Reyes-Múgica, M. BRAF Mutations Are Also Associated with Neurocutaneous Melanocytosis and Large/Giant Congenital Melanocytic Nevi. Pediatr. Dev. Pathol. 2015, 18, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Botticelli, A.R.; Villani, M.; Angiari, P.; Peserico, L. Meningeal Melanocytoma of Meckel’s Cave Associated with Ipsilateral Ota’s Nevus. Cancer 1983, 51, 2304–2310. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, T.F.; Moran, M.; Miller, J.H.; Hensley, S.D. Meningeal Melanocytoma. An Uncommon Diagnostic Pitfall in Surgical Neuropathology. Arch. Pathol. Lab. Med. 1995, 119, 542–546. [Google Scholar]
- Fan, M.; Wang, J.; Fu, W.; Liu, K.; Li, L.; Sun, P. Primary Meningeal Melanocytoma Located in Foramen Magnum: A Case Report and Review of the Literatures. Chin. Med. Sci. J. 2012, 27, 115–120. [Google Scholar]
- Châabane, M.; Ellouze, S.; Hamrouni, A.; Mlika, N.; ben Hammouda, M.; Khoudja, F. Meningeal Melanocytoma: A Rare Meningeal Tumor. J. Radiol. 2003, 84, 415–416. [Google Scholar] [PubMed]
- Nakahara, K.; Morota, N.; Ihara, S.; Oka, H.; Matsuoka, K.; Nakagawa, A. Meningeal Melanocytoma Extruded From the Skull of a Neonate-Case Report. Neurol. Med. Chir. 2010, 50, 240–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aissaoui, A.; Mosrati, M.A.; Moussa, A.; Belhaj, M.; Bougattas, M.; Zakhama, A.; Chadly, A. Sudden Death and Primary Leptomeningeal Melanocytosis: A Case Report with an Autopsy Diagnosis. Am. J. Forensic. Med. Pathol. 2015, 36, 199–201. [Google Scholar] [CrossRef] [PubMed]
- Maaloul, I.; Moussaoui, M.; Salah, A.; Feki, W.; Fourati, H.; Charfi, N.; Mnif, Z. Suprasellar Melanocytoma with Leptomeningeal Seeding: An Aggressive Clinical Course for a Histologically Benign Tumor. Case Rep. Radiol. 2021, 2021, 7306432. [Google Scholar] [CrossRef]
- Mitchell, P.J.; Funt, S.A.; Gonzales, M.F.; Popovic, E.A. Primary pineal and meningeal malignant melanomatosis. J. Clin. Neurosci. 1998, 5, 353–356. [Google Scholar] [CrossRef]
- Zeiler, F.A.; Krcek, J.P. Plaque-Type Blue Nevus with Meningeal Melanocytomas. Can. J. Neurol. Sci. 2012, 39, 117–120. [Google Scholar] [CrossRef] [Green Version]
- Rousseau, A.; Bernier, M.; Kujas, M.; Varlet, P. Primary Intracranial Melanocytic Tumor Simulating Pituitary Macroadenoma: Case Report and Review of the Literature. Neurosurgery 2005, 57, E369. [Google Scholar] [CrossRef]
- Matsuno, H.; Takasu, S.; Seki, Y. Usefulness of Neuromelanin Sensitive MRI for En Plaque Meningeal Melanocytoma Involving the Cavernous Sinus: A Case Report. NMC Case Rep. J. 2019, 6, 43–46. [Google Scholar] [CrossRef] [Green Version]
- Gupta, A.; Ahmad, F.U.; Sharma, M.C.; Garg, A.; Mehta, V.S. Cerebellopontine Angle Meningeal Melanocytoma: A Rare Tumor in an Uncommon Location. Case Report. J. Neurosurg. 2007, 106, 1094–1097. [Google Scholar] [CrossRef] [PubMed]
- Al-Abdulwahhab, A.H.; Al-Sharydah, A.M.; Al-Suhibani, S.S.; Al-Shayji, H.; Al-Saad, I.; Al-Issawi, W. Primary Pigmented Meningeal Melanocytoma Originating in Meckel Cave in a Patient with Carney Complex: A Case Report. Medicine 2020, 99, e18783. [Google Scholar] [CrossRef]
- Samimi, K.; Gharib, M.H.; Rezaei-Kalantari, K.; Jafari, M. Unusual Tonsillar Herniation in Meningeal Melanocytoma: A Case Report. Iran. J. Radiol. 2012, 9, 227–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, J.; Wang, C.; Shu, Q.; Liu, J.; Mao, G. Case Report A Case Report on Intermediate-Grade Malignant Meningeal Melanocytoma with Elevated Cell Proliferation Index. Int. J. Clin. Exp. Pathol. 2015, 8, 11698. [Google Scholar]
- Maiuri, F.; Iaconetta, G.; Benvenuti, D.; Lamaida, E.; de Caro, M.L. Intracranial Meningeal Melanocytoma: Case Report. Surg. Neurol. 1995, 44, 504–509. [Google Scholar] [CrossRef]
- Sakata, K.; Miyoshi, J.; Takeshige, N.; Komaki, S.; Miyagi, N.; Nakashima, S.; Morioka, M.; Sugita, Y. Primary Meningeal Melanocytoma of the Sellar Region: Review of the Literature and Differential Diagnosis with Special Reference to Angiographical Features. Pituitary 2015, 18, 685–694. [Google Scholar] [CrossRef]
- Kang, S.-G.; Yoo, D.S.; Cho, K.S.; Kim, D.S.; Chang, E.D.; Huh, P.W.; Kim, M.C. Coexisting Intracranial Meningeal Melanocytoma, Dermoid Tumor, and Dandy-Walker Cyst in a Patient with Neurocutaneous Melanosis. Case Report. J. Neurosurg. 2006, 104, 444–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adib, S.D.; Ebner, F.H.; Bornemann, A.; Hempel, J.-M.; Tatagiba, M. Surgical Management of Primary Cerebellopontine Angle Melanocytoma: Outcome, Recurrence and Additional Therapeutic Options. World Neurosurg. 2019, 128, e835–e840. [Google Scholar] [CrossRef]
- O’Brien, D.F.; Crooks, D.; Mallucci, C.; Javadpour, M.; Williams, D.; du Plessis, D.; Broome, J.; Foy, P.; Pizer, B. Meningeal Melanocytoma. Childs Nerv. Syst. 2006, 22, 556–561. [Google Scholar] [CrossRef] [PubMed]
- Ren, Y.; Xiao, A.; Wu, X.; Zhang, Y. Meningeal Melanocytoma of the Middle Cranial Fossa (the Meckel’s Cave). Neurol. India 2015, 63, 260. [Google Scholar] [CrossRef]
- Donofrio, C.A.; Roncaroli, F.; Riccio, L.; Pereira, M.; O’Sullivan, J.; Mayers, H.; Potter, G.M.; Djoukhadar, I.; Rutherford, S.A. A Challenging Case of Sporadic Melanocytoma of the Jugular Foramen. Neurochirurgie 2021, 68, 453–457. [Google Scholar] [CrossRef]
- Franken, S.P.G.; Setz-Pels, W.; Smink-Bol, M.; Gijtenbeek, J.M.M.; Nanda, D.; van der Maazen, R.W.M.; van der Vliet, T.; Bussink, J. Unusual Case of Bifocal Leptomeningeal Melanocytoma in the Posterior Fossa with Seeding in the Spinal Canal. Br. J. Radiol. 2009, 82, e182–e188. [Google Scholar] [CrossRef]
- Pan, H.; Wang, H.; Fan, Y. Intracranial Meningeal Melanocytoma Associated with Nevus of Ota. J. Clin. Neurosci. 2011, 18, 1548–1550. [Google Scholar] [CrossRef]
- Beseoglu, K.; Knobbe, C.B.; Reifenberger, G.; Steiger, H.-J.; Stummer, W. Supratentorial Meningeal Melanocytoma Mimicking a Convexity Meningioma. Acta Neurochir. 2006, 148, 485–490. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-U.; Kim, H.-J.; Choi, J.-Y.; Kim, J.-S. Lower Brainstem Melanocytoma Masquerading as Vestibular Paroxysmia. J. Neurol. 2018, 265, 1222–1225. [Google Scholar] [CrossRef] [PubMed]
- Aimar, E.; Debernardi, A.; Tancioni, F.; di Ieva, A.; Bossi, P.; Gaetani, P.; Rodriguez y Baena, R. Meningeal Melanocytoma of the Temporal Lobe. An Uncommon Tumor in an Unusual Location. Case Report. J. Neurosurg. Sci. 2003, 47, 211. [Google Scholar] [PubMed]
- Albano, L.; Losa, M.; Spatola, G.; Panni, P.; Terreni, M.R.; Barzaghi, L.R.; Mortini, P. Primary Sellar Melanocytoma: Report of Two Cases Treated at the Same Institution and Their Long-Term Outcome. Br. J. Neurosurg. 2019, 1–5. [Google Scholar] [CrossRef]
- Prabhu, S.S.; Lynch, P.G.; Keogh, A.J.; Parekh, H.C. Intracranial Meningeal Melanocytoma: A Report of Two Cases and a Review of the Literature. Surg. Neurol. 1993, 40, 516–521. [Google Scholar] [CrossRef]
- Vreto, G.; Rroji, A.; Xhumari, A.; Leka, L.; Rakacolli, M.; Petrela, M. Meningeal Melanocytoma of the Cerebellopontine Angle as the Unusual Cause of Superficial Siderosis. Neuroradiology 2011, 53, 927–930. [Google Scholar] [CrossRef]
- Cusumano, S.; Marchiofi, G.; Trincia, G.; Barotto, V.; Tonetto, G. Malignant Meningeal Melanoma; Springer: Berlin/Heidelberg, Germany, 1998; Volume 19. [Google Scholar]
- Shin, D.; Lee, K.J.; Adeluwa, T.; Hur, J. Machine Learning-Based Predictive Modeling of Postpartum Depression. J. Clin. Med. 2020, 9, 2899. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Liu, W.; Zhang, S.; Xu, J.; Hui, X. Cerebellar Meningeal Melanocytoma Associated with Nevus of Ota: An Extremely Rare Case. Neurology 2015, 85, 555–556. [Google Scholar] [CrossRef] [Green Version]
- Rai, S.; Sharma, M.; Naik, R.; Sinha, R.; Philipose, R.; Verghese, R. Melanocytoma of Cerebellum. Indian J. Pathol. Microbiol. 2008, 51, 47. [Google Scholar] [CrossRef] [PubMed]
- Elbadry, R.; Elazim, A.A.; Mohamed, K.; Issa, M.; Ayyad, A. Primary Meningeal Melanocytoma of the Cerebellopontine Angle Associated with Ipsilateral Nevus of Ota: A Case Report. Surg. Neurol. Int. 2018, 9, 245. [Google Scholar] [CrossRef] [PubMed]
- González-Tortosa, J.; Ros de San Pedro, J.; Ferri-Ñíguez, B. Melanocitoma Meníngeo Del Ángulo Pontocerebeloso: ¿Un Tumor Benigno? Neurocirugia 2009, 20, 372–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, I.Y.M.; Li, H.; Shi, T.; Hammond, R.R.; Jurkiewicz, M.T. Parietal Convexity Meningeal Melanocytoma: Radiologic-Pathologic Correlation. Can. J. Neurol. Sci. 2021, 48, 719–721. [Google Scholar] [CrossRef] [PubMed]
- Offiah, C.J.; Laitt, R.D. Intracranial Meningeal Melanocytoma: A Cause of High. Signal on T1-and Low Signal on T2-Weighted MRI. Clin. Radiol. 2006, 61, 294–298. [Google Scholar] [CrossRef] [PubMed]
- Yukawa, H.; Seki, H.; Sugawara, T.; Boku, N.; Higuchi, H.; Ono, S. A Case of Primary Meningeal Melanocytoma of the Left Middle Fossa. No Shinkei Geka 2003, 31, 1023–1028. [Google Scholar] [PubMed]
- Faro, S.H.; Koenigsberg, R.A.; Turtz, A.R.; Croul, S.E. Melanocytoma of the Cavernous Sinus: CT and MR Findings. Am. J. Neuroradiol. 1996, 17, 1087–1090. [Google Scholar]
- Wang, F.; Ling, S. Primary Meningeal Melanocytoma in Sellar Region, Simulating a Nonfunctioning Pituitary Adenoma: Case Report and Literature Review. World Neurosurg. 2018, 112, 209–213. [Google Scholar] [CrossRef]
- Shinoda, K.; Hayasaka, S.; Nagaki, Y.; Kadoi, C.; Kurimoto, M.; Okada, E. Melanocytoma of the Left Optic Nerve Head and Right Retrobulbar Optic Neuropathy Compressed by a Tuberculum Sellae Meningioma. Ophthalmologica 2000, 214, 161–163. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.J.; Hsu, Y.I.; Ho, Y.S.; Hsu, Y.H.; Wang, L.J.; Wong, Y.C. Intracranial Meningeal Melanocytoma: CT and MRI. Neuroradiology 1997, 39, 811–814. [Google Scholar] [CrossRef] [PubMed]
- Chow, M.; Clarke, D.B.; Maloney, W.J.; Sangalang, V. Meningeal Melanocytoma of the Planum Sphenoidale. Case Report and Review of the Literature. J. Neurosurg. 2001, 94, 841–845. [Google Scholar] [CrossRef] [PubMed]
- Kuo, K.L.; Lin, C.L.; Wu, C.H.; Chang, C.H.; Tsai, H.P.; Loh, J.K.; Lieu, A.S.; Su, Y.F. Meningeal Melanocytoma Associated with Nevus of Ota: Analysis of Twelve Reported Cases. World Neurosurg. 2019, 127, e311–e320. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Hidalgo, L.; Lopez-Gines, C.; Navarro, L.; Callaghan, R.C.; San Miguel, T.; Gil-Benso, R.; Quilis, V.; Botella, L.; Gonzalez-Darder, J.; Cerda-Nicolas, M. BRAF V600E Mutation in Two Distinct Meningeal Melanocytomas Associated with a Nevus of Ota. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2014, 32, e72–e75. [Google Scholar] [CrossRef] [Green Version]
- Ahluwalia, S.; Ashkan, K.; Casey, A.T.H. Meningeal Melanocytoma: Clinical Features and Review of the Literature. Br. J. Neurosurg. 2003, 17, 347–351. [Google Scholar] [CrossRef] [PubMed]
- Das, K.; Nair, A.; Jaiswal, S.; Sahu, R.; Srivastava, A.; Kumar, R.; Mehrotra, A. Supratentorial Intermediate Grade Meningeal Melanocytoma with Intratumoral Bleed in the Background of Neurocutaneous Melanosis: Report of an Unusual Case and Review of Literature. Asian J. Neurosurg. 2017, 12, 98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samadian, M.; Nejad, A.M.; Bakhtevari, M.H.; Sabeti, S.; Sharifi, G.; Jabbari, R.; Rezaei, O. Primary Meningeal Melanocytoma in the Left Temporal Lobe Associated with Nevus Ota: A Case Report and Review of the Literature. World Neurosurg. 2015, 84, 567–573. [Google Scholar] [CrossRef] [PubMed]
- Piercecchi-Marti, M.-D.; Mohamed, H.; Liprandi, A.; Gambarelli, D.; Grisoli, F.; Pellissier, J.-F. Intracranial Meningeal Melanocytoma Associated with Ipsilateral Nevus of Ota. Case Report. J. Neurosurg. 2002, 96, 619–623. [Google Scholar] [CrossRef]
- Jellinger, K.; Böck, F.; Brenner, H. Meningeal Melanocytoma. Report of a Case and Review of the Literature. Acta Neurochir. 1988, 94, 78–87. [Google Scholar] [CrossRef]
- Litofsky, N.S.; Zee, C.S.; Breeze, R.E.; Chandrasoma, P.T. Meningeal Melanocytoma: Diagnostic Criteria for a Rare Lesion. Neurosurgery 1992, 31, 945–950. [Google Scholar] [CrossRef] [PubMed]
- Kini, J.R.; Jeyraj, V.; Jayaprakash, C.S.; Indira, S.; Naik, C.N.R.; Rao, D. Intraoperative Smear Cytology of Meningeal Melanocytoma of the Posterior Fossa. Cytopathology 2009, 20, 59–62. [Google Scholar] [CrossRef]
- Schindler, C.U.; Kuchelmeister, K.; Richter, H.P.; Schachenmayr, W. Meningeal Melanocytoma. Pathologe 1998, 94, 78–87. [Google Scholar] [CrossRef]
- Wang, F.; Qiao, G.; Lou, X.; Song, X.; Chen, W. Malignant Transformation of Intracranial Meningeal Melanocytoma. Case Report and Review of the Literature. Neuropathology 2011, 31, 414–420. [Google Scholar] [CrossRef] [PubMed]
- Uramaru, K.; Sakata, K.; Shimohigoshi, W.; Kawasaki, T.; Manaka, H. Primary Meningeal Melanocytoma Located in the Craniovertebral Junction: A Case Report and Literature Review. NMC Case Rep. J. 2021, 8, 349–354. [Google Scholar] [CrossRef] [PubMed]
- Czirják, S.; Vitanovic, D.; Slowik, F.; Magyar, A. Primary Meningeal Melanocytoma of the Pineal Region. Case Report. J. Neurosurg. 2000, 92, 461–465. [Google Scholar] [CrossRef] [PubMed]
- Uematsu, Y.; Yukawa, S.; Yokote, H.; Itakura, T.; Hayashi, S.; Komai, N. Meningeal Melanocytoma: Magnetic Resonance Imaging Characteristics and Pathological Features. Case Report. J. Neurosurg. 1992, 76, 705–710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leonardi, M.A.; Lumenta, C.B.; Èlzle, A.S.; Mu, J.; Ècker, È.-H. Unusual Clinical Presentation of a Meningeal Melanocytoma with Seizures: Case Report and Review of the Literature. Acta Neurochir. 1998, 140, 621–628. [Google Scholar] [CrossRef] [PubMed]
- Winston, K.R.; Sotrel, A.; Schnitt, S.J. Meningeal Melanocytoma. Case Report and Review of the Clinical and Histological Features. J. Neurosurg. 1987, 66, 50–57. [Google Scholar] [CrossRef]
- Koenigsmann, M.; Jautzke, G.; Unger, M.; Théallier-Janko, A.; Wiegel, T.; Stoltenburg-Didinger, G. June 2002: 57-Year-Old Male with Leptomeningeal and Liver Tumors Clinical History, Radiology and Microscopic Description. Brain Pathol. 2002, 12, 519. [Google Scholar] [CrossRef]
- Bir, H.; Sodhi, S.; Salunke, P.; Sahoo, S.K.; Radotra, B.D.; Kumar, N. Primary Ventral Foramen Magnum Meningeal Melanocytoma. Neurology 2014, 62, 230. [Google Scholar]
- Lin, B.; Yang, H.; Qu, L.; Li, Y.; Yu, J. Primary Meningeal Melanocytoma of the Anterior Cranial Fossa: A Case Report and Review of the Literature. World J. Surg. Oncol. 2012, 10, 135. [Google Scholar] [CrossRef] [Green Version]
- Gamoh, S.; Tsuno, T.; Akiyama, H.; Kotaki, S.; Nakanishi, T.; Tsuji, K.; Yoshida, H.; Shimizutani, K. Intracranial Meningeal Melanocytoma Diagnosed Using an Interdisciplinary Approach: A Case Report and Review of the Literature. J. Med. Case Rep. 2018, 12, 177. [Google Scholar] [CrossRef] [PubMed]
- Ali, Y.; Rahme, R.; Moussa, R.; Abadjian, G.; Menassa-Moussa, L.; Samaha, E. Multifocal Meningeal Melanocytoma: A New Pathological Entity or the Result of Leptomeningeal Seeding? J. Neurosurg. 2009, 111, 488–491. [Google Scholar] [CrossRef] [Green Version]
- Merciadri, P.; Secci, F.; Sbaffi, P.F.; Zona, G. Multifocal Meningeal Melanocytoma of the Conus Medullaris. Acta Neurochir. 2011, 153, 2283–2285. [Google Scholar] [CrossRef]
- Bourhis, A.; Quintin-Roué, I.; Redon, S.; Bourhis, M.; Magro, E.; Seizeur, R.; Marcorelles, P.; Uguen, A. Transformation d’un Mélanocytome Méningé En Mélanome: Étude Clinique, Histopathologique et Cytogénétique. Ann. Pathol. 2019, 39, 352–356. [Google Scholar] [CrossRef] [PubMed]
- Tewari, M.K.; Radotra, B.D.; Sharma, B.S.; Mathuriya, S.N.; Pathak, A.; Banerjee, A.K.; Kak, V.K. Meningeal Melanocytoma: Report of Two Cases. Indian J. Cancer 1990, 27. [Google Scholar]
- Balmaceda, C.M.; Fetell, M.R.; O’Brien, J.L.; Housepian, E.H. Nevus of Ota and Leptomeningeal Melanocytic Lesions. Neurology 1993, 43, 381. [Google Scholar] [CrossRef]
- Brito, A.B.; Rogerio, F.; Reis, F.; Garmes, H.M.; Vassallo, J.; Lima, C.S. Primary Meningeal Melanocytoma Mimicking a Nonfunctioning Pituitary Adenoma. Clin. Neuropathol. 2016, 35, 158. [Google Scholar] [CrossRef]
- Hou, G.Q.; Sun, J.C.; Zhang, X.J.; Shen, B.X.; Zhu, X.J.; Liang, L.; Zhang, X.L. MR Imaging Findings of the Intraspinal Meningeal Melanocytoma: Correlation with Histopathologic Findings. Am. J. Neuroradiol. 2012, 33, 1525–1529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turhan, T.; Oner, K.; Yurtseven, T.; Akalin, T.; Ovul, I. Spinal Meningeal Melanocytoma. Report of Two Cases and Review of the Literature. J. Neurosurg. 2004, 100, 287–290. [Google Scholar]
- Tregnago, A.C.; Furlan, M.v.; Bezerra, S.M.; Porto, G.C.L.M.; Mendes, G.G.; Henklain, J.V.R.; Pinto, C.A.L.; Kowalski, L.P.; de Carvalho, G.B.; Costa, F.D. Orbital Melanocytoma Completely Resected with Conservative Surgery in Association with Ipsilateral Nevus of Ota: Report of a Case and Review of the Literature. Head Neck 2015, 37, E49–E55. [Google Scholar] [CrossRef] [PubMed]
- Mathai, A.M.; Naik, R.; Pai, M.R.; Kini, J.R.; Kumar, S.; Ballal, C.K. Orbital Melanocytoma. Orbit 2008, 27, 383–387. [Google Scholar] [CrossRef] [PubMed]
- Tsugu, H.; Nabeshima, K.; Matsumoto, S.; Omura, T.; Yahiro, T.; Oshiro, S.; Komatsu, F.; Abe, H.; Fukushima, T.; Inoue, T.; et al. A Case of a Heavily Pigmented Orbital Melanocytoma. Brain Tumor Pathol. 2009, 26, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Rutten, I.; Bolle, S.; Kaschten, B.; Stevenaert, A.; Deneufbourg, J.M.; Deprez, M. Recurrent Intracranial Melanocytoma Associated with a Nevus of Ota. Acta Neurochir. 2005, 147, 313–315. [Google Scholar] [CrossRef] [PubMed]
- Kraft Roverea, R.; Dagnonia, C.; Gomes de Oliveiraa, G.; Sapellia, J. Meningeal Melanocytoma: Case Report and Literature Review. Bol. De La Asoc. Med. De Puerto Rico 2014, 106, 30–32. [Google Scholar]
- Khadilkar, U.N.; Agarwal, N.; Bhat, V. Primary Meningeal Melanocytoma. Kathmandu Univ. Med. J. 2008, 6, 245–247. [Google Scholar]
- Crouzet, J.; Richard, S.; Pillet, G.; Muckensturm, B.; Srour, A.; Pradat, P. Meningeal Melanocytoma or Multiple Pigmented Meningioma of the Spinal Canal. Report of a Case. Review of the Literature. Rev. Rhum. Mal. Osteoartic. 1992, 59, 738–743. [Google Scholar] [PubMed]
- Hioki, A.; Miyamoto, K.; Kato, H.; Hatano, Y.; Asano, N.; Hirose, Y.; Fushimi, K.; Shimizu, K. Sudden Onset of Paraplegia Caused by Subarachnoid Hemorrhage Associated with Meningeal Melanocytoma of the Conus Medullaris: A Case Report of Intraoperative Identification of These Two Pathological Conditions. Eur. J. Orthop. Surg. Traumatol. 2012, 22, 593–596. [Google Scholar] [CrossRef]
- Vaidya, M.; Dhake, R.; Parikh, R.; Sabnis, M.; Sabnis, J. Recurrent Meningeal Melanocytoma of Cervical Spine: A Rare Case. Asian J. Neurosurg. 2021, 16, 159. [Google Scholar] [CrossRef]
- Yang, C.; Fang, J.; Li, G.; Jia, W.; Liu, H.; Qi, W.; Xu, Y. Spinal Meningeal Melanocytomas: Clinical Manifestations, Radiological and Pathological Characteristics, and Surgical Outcomes. J. Neurooncol. 2016, 127, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Sankhla, S.K.; Lynch, P.G.; Davis, C.H. Spinal Meningeal Melanocytoma: A Case Report and Review of the Literature. Br. J. Neurosurg. 1996, 10, 205–210. [Google Scholar] [CrossRef]
- Chacko, G.; Rajshekhar, V. Thoracic Intramedullary Melanocytoma with Long-Term Follow-up: Case Report. J. Neurosurg. Spine 2008, 9, 589–592. [Google Scholar] [CrossRef]
- Tateyama, M.; Fujimoto, T.; Nakamura, T.; Miyamoto, T. Meningeal Melanocytoma Occurring at Epidural Region of the Cervical Spine. Spine Surg. Relat. Res. 2020, 4, 377–379. [Google Scholar] [CrossRef]
- Liu, Z.-Q. World Journal of Clinical Cases. Contents Thrice Mon. 2021, 9, 8280–8626. [Google Scholar]
- Wang, C.; Shao, X.; Zou, Y. Primary Intramedullary Melanocytoma in the Thoracic Cord: A Case Report and Literature Review. Transl. Cancer Res. 2022, 11, 928–934. [Google Scholar] [CrossRef]
- Kinnen, F.; Fleck, S.K.; Baldauf, J.; Hans, V.; Daeschlein, G.; Rathmann, E.; Schroeder, H.W.S.; Marx, S. Primary Leptomeningeal Melanocytic Tumors of the Spine: Report of Two Cases and Review of the Literature. World Neurosurg. 2019, 124, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Eskandari, R.; Schmidt, M.H. Intramedullary Spinal Melanocytoma. Rare Tumors 2010, 2, 64–67. [Google Scholar] [CrossRef] [Green Version]
- Sung Hye Park, M.D.; Heum Rye Park, M.D.; Yong Ko, M.D. Spinal Meningeal Melanocytoma. J. Korean Med. Sci. 1992, 7, 364–368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimoda, H.; Oka, K.; Naoi, Y.; Nishida, S.; Oka, T.; Nakazato, Y.; Mori, N. Primary Melanocytoma Arising from the Thoracic Leptomeninges Case. Clin. Neuropathol. 1999, 18, 80–83. [Google Scholar]
- Salah El-Din, A.M.; Aboul-Ela, H.M.; Alsawy, M.F.; Koheil, A.; Ashry, A.H. Spinal Meningeal Melanocytoma in a 5-Year-Old Child: A Case Report and Review of Literature. Egypt. J. Neurol. Psychiatry Neurosurg. 2018, 54, 13. [Google Scholar] [CrossRef]
- Bhargava, P.; Grewal, S.S.; Dewan, Y.; Jhawar, S.S.; Jain, V.; Gupta, B. Craniovertebral Junction Melanocytoma: A Case Report. Turk. Neurosurg. 2013, 23, 539–542. [Google Scholar] [CrossRef] [Green Version]
- Flores, A.; Gadot, R.; Noorbhai, I.; Hall, H.; Heck, K.A.; Raper, D.M.S.; Xu, D.; Karas, P.; Mandel, J.J.; Ropper, A.E. S-100-Negative, GNA11 Mutation-Positive Intramedullary Meningeal Melanocytoma of the Thoracic Spine: A Radiographic Challenge and Histologic Anomaly. Surg. Neurol. Int. 2021, 12, 315. [Google Scholar] [CrossRef]
- Kim, O.H.; Kim, S.J.; Choo, H.J.; Lee, S.J.; Lee, I.S.; Kim, J.Y.; Kim, H. Spinal Meningeal Melanocytoma with Benign Histology Showing Leptomeningeal Spread: Case Report. Korean J. Radiol. 2013, 14, 470–476. [Google Scholar] [CrossRef] [Green Version]
- Mangels, K.J.; Johnson, M.D.; Weil, R.J. 35-Year-Old Woman with Progressive Bilateral Leg Weakness. Brain Pathol. 2006, 16, 183–184. [Google Scholar] [CrossRef]
- Foit, N.A.; Neidert, M.C.; Woernle, C.M.; Rushing, E.J.; Krayenbü Hl, N. Bifocal Extra- and Intradural Melanocytoma of the Spine: Case Report and Literature Review. Eur. Spine J. 2013, 22, 521–525. [Google Scholar] [CrossRef] [Green Version]
- Goyal, A.; Sinha, S.; Singh, A.K.; Tatke, M.; Kansal, A. Lumbar Spinal Meningeal Melanocytoma of the L3 Nerve Root with Paraspinal Extension: A Case Report. Spine 2003, 28, E140–E142. [Google Scholar] [CrossRef]
- Chen, K.T.K. Crush Cytology of Melanocytoma of the Spinal Cord. A Case Report. Acta Cytol. 2003, 47, 1091–1094. [Google Scholar] [CrossRef]
- Sharma, V.; Bhaskar, S.; Kumar, A.; Bhardwaj, M. Conus Melanocytoma: A Rare Spinal Tumor. Neurology 2019, 67, 591. [Google Scholar] [CrossRef]
- Shownkeen, H.N.; Harmath, C.; Thomas, C. Multiform Cervical Melanocytoma: A Case Report. Neuroradiology 2002, 44, 1008–1010. [Google Scholar] [CrossRef]
- Schembri, M.; Kok, H.K.; Brennan, P.; O’Hare, A.; Thornton, J.; Looby, S.; Asadi, H. Mystery Case: Dural Melanocytoma with Leptomeningeal Melanocytosis. Neurology 2017, 88, e70–e71. [Google Scholar] [CrossRef] [Green Version]
- Srirama Jayamma, S.; Sud, S.; Buxi, T.; Madan, V.; Goyal, A.; Dhawan, S. Cervical Spinal Meningeal Melanocytoma Presenting as Intracranial Superficial Siderosis. Case Rep. Radiol. 2015, 2015, 674868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delhaye, M.; Menei, P.; Rousselet, M.C.; Diabira, S.; Mercier, P. A Case of Intramedullary Primary Melanocytic Tumor: Meningeal Melanocytoma or Malignant Melanoma? Neurochirurgie 2001, 47, 133–136. [Google Scholar]
- Sethi, D.; Duhan, A.; Sen, R.; Goyal, V.; Modi, S. Spinal Meningeal Melanocytoma. Asian J. Neurosurg. 2011, 6, 111. [Google Scholar] [CrossRef] [Green Version]
- Nicolotto, E.; Presas-Rodriguez, S.; Morra, I.; Franchino, F.; Magistrello, M.; Pellerino, A.; Massaro, F.; Pinessi, L.; Rudà, R.; Soffietti, R. Spinal Melanocytoma with Leptomeningeal Spread and Long Survival Following Surgery and Chemotherapy. J. Neurosurg. Sci. 2018, 62, 375–378. [Google Scholar] [CrossRef]
- Gonçjalves, J.; Díaz, P.; Maíllo, A.; Blanco, A.; Subhi-Issa, I. Melanocitoma Meníngeo Cervical Simulando Un Neurinoma de La Raíz C7: Caso Clínico. Neurocirugia 2002, 13, 393–396. [Google Scholar] [CrossRef]
- Shanthi, V.; Ramakrishna, B.A.; Bheemaraju, V.V.; Rao, N.M.; Murthy Athota, V.R. Spinal Meningeal Melanocytoma: A Rare Meningeal Tumor. Ann. Indian Acad. Neurol. 2010, 13, 308–310. [Google Scholar] [CrossRef] [PubMed]
- Lach, B.; Russell, N.; Benoit, B.; Atack, D. Cellular Blue Nevus (“melanocytoma”) of the Spinal Meninges: Electron Microscopic and Immunohistochemical Features. Neurosurgery 1988, 22, 773–780. [Google Scholar] [CrossRef]
- Akgun, M.Y.; Isler, C.; Ulu, M.O. C6-T1 Intradural Extramedullary Ventral Meningeal Melanocytoma Resected Via Anterior Corpectomy with Reconstruction. World Neurosurg. 2020, 138, 457–460. [Google Scholar] [CrossRef]
- Dorwal, P.; Gautam, D.; Mohapatra, I.; Gupta, A. Intramedullary Melanocytoma of Thoracic Spine: A Rare Case Report. Asian J. Neurosurg. 2014, 9, 36. [Google Scholar] [CrossRef] [Green Version]
- Yin, M.; Ma, J.; Ye, J.; Xu, H.; Mo, W. 8-Year Follow-up for Woman with Spinal Meningeal Melanocytoma in S1 Nerve Root: Case Report and Literature Review. World Neurosurg. 2019, 129, 143–147. [Google Scholar] [CrossRef]
- Czarnecki, E.J.; Silbergleit, R.; Gutierrez, J.A. MR of Spinal Meningeal Melanocytoma. Am. J. Neuroradiol. 1997, 18, 180–182. [Google Scholar]
- Muthappan, M.; Muthu, T.; Hussain, Z.; Lamont, D.; Balakrishnan, V. Cervical Intramedullary Melanocytoma: A Case Report and Review of Literature. J. Clin. Neurosci. 2012, 19, 1450–1453. [Google Scholar] [CrossRef]
- Ganesan, S.; Acharya, S.; Kalra, K.; Chahal, R. Intradural Intramedullary Primary Spinal Melanocytoma: A Rare Case Report. Indian J. Neurosurg. 2017, 6, 055–058. [Google Scholar] [CrossRef] [Green Version]
- Tatagiba, M.; Böker, D.K.; Brandis, A.; Samii, M.; Ostertag, H.; Babu, R. Meningeal Melanocytoma of the C8 Nerve Root: Case Report. Neurosurgery 1992, 31, 958–961. [Google Scholar] [CrossRef] [PubMed]
- Asanuma, K.; Kasai, Y.; Takegami, K.; Ito, H.; Yoshikawa, T.; Uchida, A. Spinal Neurocutaneous Melanosis without Cutaneous Nevi. Spine 2008, 33, E798–E801. [Google Scholar] [CrossRef] [PubMed]
- Miura, I.; Kubota, M.; Momosaki, O.; Nyui, M.; Takebayashi, K.; Kawamata, T.; Yuzurihara, M. A Rapidly Growing Cervical Meningeal Melanocytoma with a Dumbbell-Shaped Extension. World Neurosurg. 2020, 134, 90–93. [Google Scholar] [CrossRef] [PubMed]
- Reddy, R.; Krishna, V.; Prasad Sahu, B.; Uppin, M.; Sundaram, C. Multifocal Spinal Meningeal Melanocytoma: An Illustrated Case Review. Turk. Neurosurg. 2012, 22, 791–794. [Google Scholar] [CrossRef] [PubMed]
- Bejarano, B.; Isla, A.; Morales, C.; Paz, J.; Blázquez, M.G. Melanocitoma Meníngeo Espinal. Neurocirugia 1995, 6, 230–232. [Google Scholar] [CrossRef]
- Lee, J.K.; Rho, Y.J.; Jeong, D.M.; Rhim, S.C.; Kim, S.J. Diagnostic Clue of Meningeal Melanocytoma: Case Report and Review of Literature. Yonsei Med. J. 2017, 58, 467–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsumoto, S.; Kang, Y.; Sato, S.; Kawakami, Y.; Oda, Y.; Araki, M.; Kawamura, J.; Uchida, H. Spinal Meningeal Melanocytoma Presenting with Superficial Siderosis of the Central Nervous System. Case Report and Review of the Literature. J. Neurosurg. 1998, 88, 890–894. [Google Scholar] [CrossRef]
- Eun, S.S.; Kim, H.S.; Lee, S.H.; Liu, W.C.; Lee, J.H. Spinal Meningeal Melanocytoma in the S-1 Nerve Root Sheath with Paraspinal Extension Mimicking Schwannoma. World Neurosurg. 2011, 75, 303–306. [Google Scholar] [CrossRef]
- Seo, J.S.; Ahn, S.S.; Choi, J.H.; Choi, H.J. Primary Meningeal Melanocytoma in the Thoracic Spine—A Case Report. Korean J. Spine 2011, 8, 121–124. [Google Scholar] [CrossRef]
- Armocida, D.; Pesce, A.; Berra, L.V.; Marzetti, F.; Antonelli, M.; Santoro, A. Intradural Extramidullary Dorsal Melanocytoma in the Adult: Case Report and Review of the Literature. J. Clin. Neurosci. 2019, 62, 248–253. [Google Scholar] [CrossRef]
- Caruso, R.; Marrocco, L.; Wierzbicki, V.; Salvati, M. Intramedullary Melanocytoma: Case Report and Review of Literature. Tumori 2009, 95, 389–393. [Google Scholar] [CrossRef]
- Ruelle, A.; Tunesi, G.; Andrioli, G. Spinal Meningeal Melanocytoma. Case Report and Analysis of Diagnostic Criteria. Neurosurg. Rev. 1996, 19, 39–42. [Google Scholar] [CrossRef]
- Tsai, M.-H.; Lin, W.-P.; Liao, W.-A.; Chiang, P.-Y.; Lin, Y.-C. Recurrent Spinal Meningeal Melanocytoma at Lumbar Spine Level: A Case Report. Br. J. Neurosurg. 2021. [Google Scholar] [CrossRef] [PubMed]
- Xie, S.; Jiang, Z. Primary Spinal Cord Melanocytoma: A Case Report and Review of Literature. Int. J. Clin. Exp. Pathol. 2019, 12, 669–673. [Google Scholar] [PubMed]
- Hoffmann, M.; Koelsche, C.; Seiz-Rosenhagen, M.; Mai, S.; Lohr, F.; Reuss, D.; Wenz, F.; Gebhardt, C.; Giordano, F.A. The GNAQ in the Haystack: Intramedullary Meningeal Melanocytoma of Intermediate Grade at T9-10 in a 58-Year-Old Woman. J. Neurosurg. 2016, 125, 53–56. [Google Scholar] [CrossRef]
- Kordás, M.; Czirják, S.; Slowik, F. Primary Meningeal Melanocytoma of the Spinal Cord: Report of a Paediatric Case with Benign Course and Review of the Literature. Eur. J. Neurol. 1996, 3, 141–145. [Google Scholar] [CrossRef]





| Therapy | Frequency | Follow–Up No Recurrence |
|---|---|---|
| Total Resection only | 69 (90.8 %) | 47/69 (68.1%) |
| Total Resection + RT | 7 (9.2%) | 5/7 (71.4%) |
| Total | 76 (100%) | 52/76 (68.4%) |
| Therapy | Frequency | Follow–Up No Recurrence |
|---|---|---|
| Partial Resection only | 33 (55.9%) | 18/33 (54.5%) |
| Partial Resection + RT | 21 (35.6%) | 13/21 (61.9%) |
| Partial Resection + Chemo | 1 (1.7%) | 1/1 (100%) |
| Partial Resection + RT + Chemo | 2 (3.4%) | 0/2 (0%) |
| Partial Resection + Radiosurgery | 2 (3.4%) | 2/2 (100%) |
| Total | 59 (100%) | 34/59 (57.6%) |
| Case | Primary Location MM | Location Metastasis | Therapy | Outcome |
|---|---|---|---|---|
| [8] | Spine | Liver, rib | TR, Reop + RT | Tumor progression |
| [17] | Intracranial | Thoracic | PR + RT, Reop + RT + Temolozomide + Cisplatin + Fotemustine | Death |
| [19] | Intracranial | Spine | TR, RT + Temozolomide | Death |
| [22] | Intracranial | Intracranial, Liver, pancreas | TR + RT, Reop + RT; Temozolomide; Ipilimumab; | Death |
| [27] | Spine | Intracranial | TR, Reop + RT + Pembrolizumab + Bevacizumab + Temozolomide | Death |
| [44] | Intracranial | Intracranial | TR, RT | Tumor progression |
| [45] | Spine | Intracranial | PR | Death |
| [46] | Spine | Intracranial | TR | Death |
| [47] | Spine | Spine | Resection | Death |
| [48] | Spine | Intracranial | PR, Reop + RT | Death |
| [49] | Spine | No data | TR, Reop | Tumor progression |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ricchizzi, S.; Gallus, M.; Stummer, W.; Holling, M. How Should We Treat Meningeal Melanocytoma? A Retrospective Analysis of Potential Treatment Strategies. Cancers 2022, 14, 5851. https://doi.org/10.3390/cancers14235851
Ricchizzi S, Gallus M, Stummer W, Holling M. How Should We Treat Meningeal Melanocytoma? A Retrospective Analysis of Potential Treatment Strategies. Cancers. 2022; 14(23):5851. https://doi.org/10.3390/cancers14235851
Chicago/Turabian StyleRicchizzi, Sarah, Marco Gallus, Walter Stummer, and Markus Holling. 2022. "How Should We Treat Meningeal Melanocytoma? A Retrospective Analysis of Potential Treatment Strategies" Cancers 14, no. 23: 5851. https://doi.org/10.3390/cancers14235851
APA StyleRicchizzi, S., Gallus, M., Stummer, W., & Holling, M. (2022). How Should We Treat Meningeal Melanocytoma? A Retrospective Analysis of Potential Treatment Strategies. Cancers, 14(23), 5851. https://doi.org/10.3390/cancers14235851