
Radiation-Induced Esophagitis in Non-Small-Cell Lung Cancer Patients: Voxel-Based Analysis and NTCP Modeling

 ,
,  ,
,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Cohort
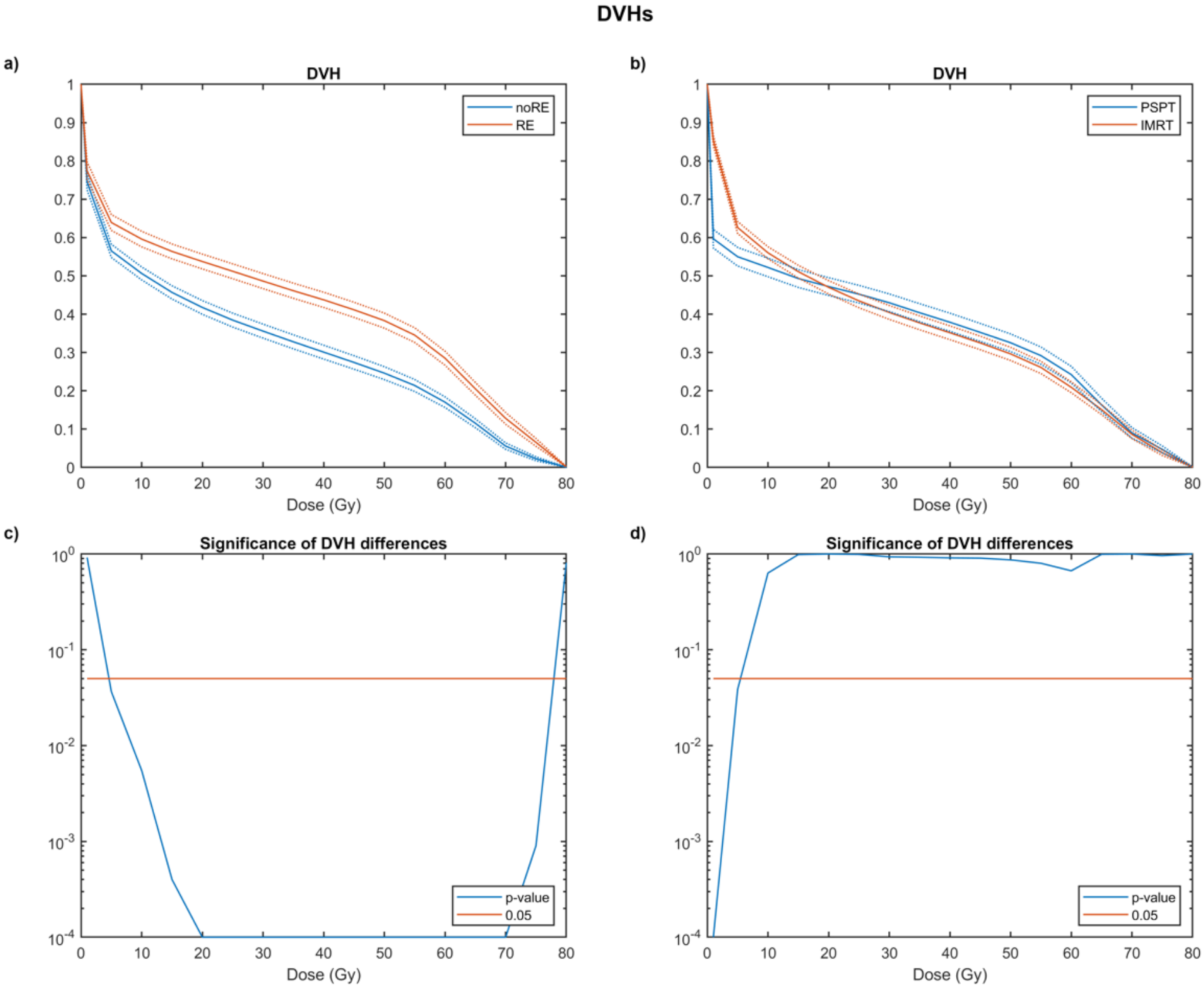
2.2. Dose-Volume Histogram Analysis
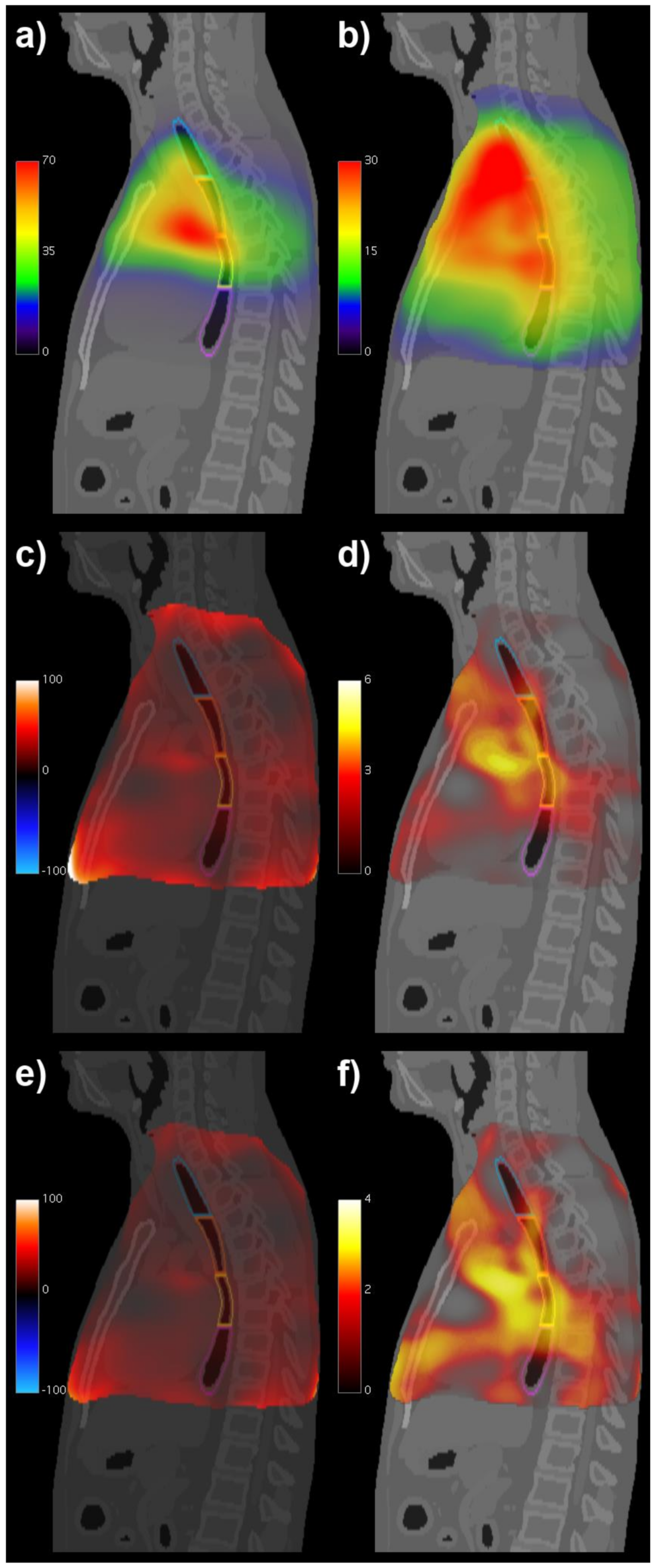
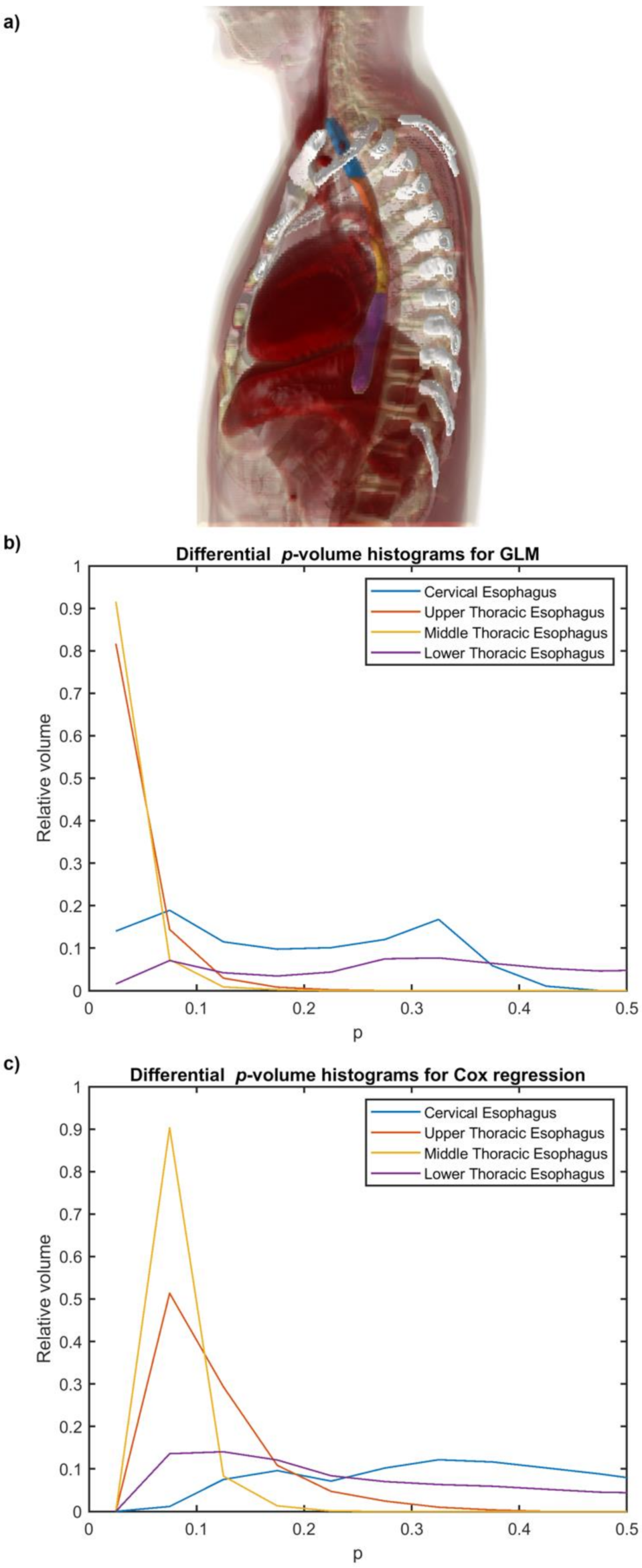
2.3. Voxel-Based Analyses
2.4. Normal Tissue Complication Probability (NTCP) Modeling
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pacelli, R.; Caroprese, M.; Palma, G.; Oliviero, C.; Clemente, S.; Cella, L.; Conson, M. Technological evolution of radiation treatment: Implications for clinical applications. Semin. Oncol. 2019, 46, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Cella, L.; Lomax, A.; Miralbell, R. New techniques in hadrontherapy: Intensity modulated proton beams. Phys. Med. 2001, 17 (Suppl. 1), 100–102. [Google Scholar] [PubMed]
- Baker, S.; Fairchild, A. Radiation-induced esophagitis in lung cancer. Lung Cancer Targets Ther. 2016, 7, 119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubin, P.; Constine, L.S.; Marks, L.B. ALERT-Adverse Late Effects of Cancer Treatment; Springer: Berlin/Heidelberg, Germany, 2014. [Google Scholar]
- O’Rourke, N.; Roque, I.F.M.; Farre Bernado, N.; Macbeth, F. Concurrent chemoradiotherapy in non-small cell lung cancer. Cochrane Database Syst. Rev. 2010, 6, CD002140. [Google Scholar] [CrossRef] [PubMed]
- Werner-Wasik, M.; Yorke, E.; Deasy, J.; Nam, J.; Marks, L.B. Radiation dose-volume effects in the esophagus. Int. J. Radiat. Oncol. Biol Phys. 2010, 76, S86–S93. [Google Scholar] [CrossRef] [Green Version]
- Luna, J.M.; Chao, H.H.; Shinohara, R.T.; Ungar, L.H.; Cengel, K.A.; Pryma, D.A.; Chinniah, C.; Berman, A.T.; Katz, S.I.; Kontos, D.; et al. Machine learning highlights the deficiency of conventional dosimetric constraints for prevention of high-grade radiation esophagitis in non-small cell lung cancer treated with chemoradiation. Clin. Transl. Radiat. Oncol. 2020, 22, 69–75. [Google Scholar] [CrossRef] [Green Version]
- Belderbos, J.; Heemsbergen, W.; Hoogeman, M.; Pengel, K.; Rossi, M.; Lebesque, J. Acute esophageal toxicity in non-small cell lung cancer patients after high dose conformal radiotherapy. Radiother. Oncol. 2005, 75, 157–164. [Google Scholar] [CrossRef]
- De Ruysscher, D.; Dehing, C.; Bremer, R.H.; Bentzen, S.M.; Koppe, F.; Pijls-Johannesma, M.; Harzee, L.; Minken, A.; Wanders, R.; Hochstenbag, M.; et al. Maximal neutropenia during chemotherapy and radiotherapy is significantly associated with the development of acute radiation-induced dysphagia in lung cancer patients. Ann. Oncol. 2007, 18, 909–916. [Google Scholar] [CrossRef]
- Wijsman, R.; Dankers, F.; Troost, E.G.; Hoffmann, A.L.; van der Heijden, E.H.; de Geus-Oei, L.F.; Bussink, J. Multivariable normal-tissue complication modeling of acute esophageal toxicity in advanced stage non-small cell lung cancer patients treated with intensity-modulated (chemo-)radiotherapy. Radiother. Oncol. 2015, 117, 49–54. [Google Scholar] [CrossRef]
- Paximadis, P.; Schipper, M.; Matuszak, M.; Feng, M.; Jolly, S.; Boike, T.; Grills, I.; Kestin, L.; Movsas, B.; Griffith, K.; et al. Dosimetric predictors for acute esophagitis during radiation therapy for lung cancer: Results of a large statewide observational study. Pract. Radiat. Oncol. 2018, 8, 167–173. [Google Scholar] [CrossRef]
- Bourbonne, V.; Da-Ano, R.; Jaouen, V.; Lucia, F.; Dissaux, G.; Bert, J.; Pradier, O.; Visvikis, D.; Hatt, M.; Schick, U. Radiomics analysis of 3D dose distributions to predict toxicity of radiotherapy for lung cancer. Radiother. Oncol. 2021, 155, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Jelvehgaran, P.; Steinberg, J.D.; Khmelinskii, A.; Borst, G.; Song, J.Y.; de Wit, N.; de Bruin, D.M.; van Herk, M. Evaluation of acute esophageal radiation-induced damage using magnetic resonance imaging: A feasibility study in mice. Radiat. Oncol. 2019, 14, 188. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.; Brink, C.; Knap, M.; Khalil, A.A.; Nyhus, C.H.; McCulloch, T.; Holm, B.; Wu, Y.L.; Schytte, T.; Hansen, O. Acute esophagitis for patients with local-regional advanced non small cell lung cancer treated with concurrent chemoradiotherapy. Radiother. Oncol. 2016, 118, 465–470. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; He, T.; Yang, R.; Ji, T.; Li, G. Clinical, dosimetric, and position factors for radiation-induced acute esophagitis in intensity-modulated (chemo)radiotherapy for locally advanced non-small-cell lung cancer. Onco Targets Ther. 2018, 11, 6167–6175. [Google Scholar] [CrossRef] [Green Version]
- Palma, G.; Monti, S.; Cella, L. Voxel-based analysis in radiation oncology: A methodological cookbook. Phys. Med. 2020, 69, 192–204. [Google Scholar] [CrossRef]
- Shortall, J.; Palma, G.; Mistry, H.; Vasquez Osorio, E.; McWilliam, A.; Choudhury, A.; Aznar, M.; van Herk, M.; Green, A. Flogging a Dead Salmon? Reduced Dose Posterior to Prostate Correlates With Increased PSA Progression in Voxel-Based Analysis of 3 Randomized Phase 3 Trials. Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 696–699. [Google Scholar] [CrossRef]
- Ebert, M.A.; Gulliford, S.; Acosta, O.; de Crevoisier, R.; McNutt, T.; Heemsbergen, W.D.; Witte, M.; Palma, G.; Rancati, T.; Fiorino, C. Spatial descriptions of radiotherapy dose: Normal tissue complication models and statistical associations. Phys. Med. Biol. 2021, 66, 12TR01. [Google Scholar] [CrossRef]
- Palma, G.; Monti, S.; D’Avino, V.; Conson, M.; Liuzzi, R.; Pressello, M.C.; Donato, V.; Deasy, J.O.; Quarantelli, M.; Pacelli, R.; et al. A Voxel-Based Approach to Explore Local Dose Differences Associated With Radiation-Induced Lung Damage. Int. J. Radiat. Oncol. Biol. Phys. 2016, 96, 127–133. [Google Scholar] [CrossRef] [Green Version]
- McWilliam, A.; Kennedy, J.; Hodgson, C.; Vasquez Osorio, E.; Faivre-Finn, C.; van Herk, M. Radiation dose to heart base linked with poorer survival in lung cancer patients. Eur. J. Cancer. 2017, 85, 106–113. [Google Scholar] [CrossRef]
- Monti, S.; Palma, G.; D’Avino, V.; Gerardi, M.; Marvaso, G.; Ciardo, D.; Pacelli, R.; Jereczek-Fossa, B.A.; Alterio, D.; Cella, L. Voxel-based analysis unveils regional dose differences associated with radiation-induced morbidity in head and neck cancer patients. Sci. Rep. 2017, 7, 7220. [Google Scholar] [CrossRef]
- Mylona, E.; Acosta, O.; Lizee, T.; Lafond, C.; Crehange, G.; Magne, N.; Chiavassa, S.; Supiot, S.; Ospina Arango, J.D.; Campillo-Gimenez, B.; et al. Voxel-Based Analysis for Identification of Urethrovesical Subregions Predicting Urinary Toxicity After Prostate Cancer Radiation Therapy. Int. J. Radiat. Oncol. Biol. Phys. 2019, 104, 343–354. [Google Scholar] [CrossRef] [PubMed]
- Cella, L.; Monti, S.; Xu, T.; Liuzzi, R.; Stanzione, A.; Durante, M.; Mohan, R.; Liao, Z.; Palma, G. Probing thoracic dose patterns associated to pericardial effusion and mortality in patients treated with photons and protons for locally advanced non-small-cell lung cancer. Radiother. Oncol. 2021, 160, 148–158. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.; Kim, Y.; Chamseddine, I.; Lee, W.H.; Kim, H.R.; Lee, I.J.; Hong, M.H.; Cho, B.C.; Lee, C.G.; Cho, S.; et al. Lymphocyte dynamics during and after chemo-radiation correlate to dose and outcome in stage III NSCLC patients undergoing maintenance immunotherapy. Radiother. Oncol. 2022, 168, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Monti, S.; Xu, T.; Liao, Z.; Mohan, R.; Cella, L.; Palma, G. On the interplay between dosiomics and genomics in radiation-induced lymphopenia of lung cancer patients. Radiother. Oncol. 2021, 167, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Liao, Z.; Lee, J.J.; Komaki, R.; Gomez, D.R.; O’Reilly, M.S.; Fossella, F.V.; Blumenschein, G.R., Jr.; Heymach, J.V.; Vaporciyan, A.A.; Swisher, S.G.; et al. Bayesian Adaptive Randomization Trial of Passive Scattering Proton Therapy and Intensity-Modulated Photon Radiotherapy for Locally Advanced Non-Small-Cell Lung Cancer. J. Clin. Oncol. 2018, 36, 1813–1822. [Google Scholar] [CrossRef]
- Palma, G.; Monti, S.; Xu, T.; Scifoni, E.; Yang, P.; Hahn, S.M.; Durante, M.; Mohan, R.; Liao, Z.; Cella, L. Spatial Dose Patterns Associated With Radiation Pneumonitis in a Randomized Trial Comparing Intensity-Modulated Photon Therapy With Passive Scattering Proton Therapy for Locally Advanced Non-Small Cell Lung Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2019, 104, 1124–1132. [Google Scholar] [CrossRef]
- Schaffner, B.; Pedroni, E.; Lomax, A. Dose calculation models for proton treatment planning using a dynamic beam delivery system: An attempt to include density heterogeneity effects in the analytical dose calculation. Phys. Med. Biol. 1999, 44, 27–41. [Google Scholar] [CrossRef]
- Deasy, J.O.; Blanco, A.I.; Clark, V.H. CERR: A computational environment for radiotherapy research. Med. Phys. 2003, 30, 979–985. [Google Scholar] [CrossRef]
- Monti, S.; Pacelli, R.; Cella, L.; Palma, G. Inter-patient image registration algorithms to disentangle regional dose bioeffects. Sci. Rep. 2018, 8, 4915. [Google Scholar] [CrossRef]
- Palma, G.; Monti, S.; Thor, M.; Rimner, A.; Deasy, J.O.; Cella, L. Spatial signature of dose patterns associated with acute radiation-induced lung damage in lung cancer patients treated with stereotactic body radiation therapy. Phys. Med. Biol. 2019, 64, 155006. [Google Scholar] [CrossRef]
- Segars, W.P.; Sturgeon, G.; Mendonca, S.; Grimes, J.; Tsui, B.M. 4D XCAT phantom for multimodality imaging research. Med. Phys. 2010, 37, 4902–4915. [Google Scholar] [CrossRef] [PubMed]
- Conson, M.; Cella, L.; Pacelli, R.; Comerci, M.; Liuzzi, R.; Salvatore, M.; Quarantelli, M. Automated delineation of brain structures in patients undergoing radiotherapy for primary brain tumors: From atlas to dose-volume histograms. Radiother. Oncol. 2014, 112, 326–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monti, S.; Paganelli, C.; Buizza, G.; Preda, L.; Valvo, F.; Baroni, G.; Palma, G.; Cella, L. A novel framework for spatial normalization of dose distributions in voxel-based analyses of brain irradiation outcomes. Phys. Med. 2020, 69, 164–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palma, G.; Monti, S.; Conson, M.; Xu, T.; Hahn, S.; Durante, M.; Mohan, R.; Liao, Z.; Cella, L. NTCP Models for Severe Radiation Induced Dermatitis After IMRT or Proton Therapy for Thoracic Cancer Patients. Front. Oncol. 2020, 10, 344. [Google Scholar] [CrossRef]
- Colson, Y.; Krasna, M.J.; Bueno, R.; Sugarbaker, D.J.; Jaklitsch, M.; Mentzer, S. Adult Chest Surgery, 2nd ed.; McGraw-Hill Education: New York, NY, USA, 2015. [Google Scholar]
- Cella, L.; Monti, S.; Thor, M.; Rimner, A.; Deasy, J.O.; Palma, G. Radiation-Induced Dyspnea in Lung Cancer Patients Treated with Stereotactic Body Radiation Therapy. Cancers 2021, 13, 3734. [Google Scholar] [CrossRef] [PubMed]
- Alterio, D.; Gerardi, M.A.; Cella, L.; Spoto, R.; Zurlo, V.; Sabbatini, A.; Fodor, C.; D’Avino, V.; Conson, M.; Valoriani, F.; et al. Radiation-induced acute dysphagia: Prospective observational study on 42 head and neck cancer patients. Strahlenther. Onkol. 2017, 193, 971–981. [Google Scholar] [CrossRef]
- Pastore, F.; Conson, M.; D’Avino, V.; Palma, G.; Liuzzi, R.; Solla, R.; Farella, A.; Salvatore, M.; Cella, L.; Pacelli, R. Dose-surface analysis for prediction of severe acute radio-induced skin toxicity in breast cancer patients. Acta Oncol. 2016, 55, 466–473. [Google Scholar] [CrossRef] [Green Version]
- Cella, L.; Oh, J.H.; Deasy, J.O.; Palma, G.; Liuzzi, R.; D’Avino, V.; Conson, M.; Picardi, M.; Salvatore, M.; Pacelli, R. Predicting radiation-induced valvular heart damage. Acta Oncol. 2015, 54, 1796–1804. [Google Scholar] [CrossRef]
- Palma, G.; Taffelli, A.; Fellin, F.; D’Avino, V.; Scartoni, D.; Tommasino, F.; Scifoni, E.; Durante, M.; Amichetti, M.; Schwarz, M.; et al. Modelling the risk of radiation induced alopecia in brain tumor patients treated with scanned proton beams. Radiother. Oncol. 2020, 144, 127–134. [Google Scholar] [CrossRef]
- D’Avino, V.; Palma, G.; Liuzzi, R.; Conson, M.; Doria, F.; Salvatore, M.; Pacelli, R.; Cella, L. Prediction of gastrointestinal toxicity after external beam radiotherapy for localized prostate cancer. Radiat. Oncol. 2015, 10, 80. [Google Scholar] [CrossRef] [Green Version]
- Steyerberg, E. Clinical Prediction Models. Statistics for Biology and Health; Springer: Berlin/Heidelberg, Germany, 2009. [Google Scholar]
- Bentzen, S.M. Preventing or reducing late side effects of radiation therapy: Radiobiology meets molecular pathology. Nat. Rev. Cancer 2006, 6, 702–713. [Google Scholar] [CrossRef] [PubMed]
- Palma, G.; Monti, S.; Conson, M.; Pacelli, R.; Cella, L. Normal tissue complication probability (NTCP) models for modern radiation therapy. Semin. Oncol. 2019, 46, 210–218. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.J.; Kahn, D.; Zhou, S.; Yu, X.; Hollis, D.; Shafman, T.D.; Marks, L.B. Dosimetric and clinical predictors for radiation-induced esophageal injury. Int. J. Radiat. Oncol. Biol. Phys. 2005, 61, 335–347. [Google Scholar] [CrossRef] [PubMed]
- Berk, L. Radiation-induced Esophagitis in Lung Cancer—A Common Problem with Limited Therapeutic Options. Oncol. Hematol. Rev. 2020, 16, 95–99. [Google Scholar] [CrossRef]
- Wang, Z.; Chen, M.; Sun, J.; Jiang, S.; Wang, L.; Wang, X.; Sahoo, N.; Gunn, G.B.; Frank, S.J.; Nguyen, Q.N.; et al. Lyman-Kutcher-Burman normal tissue complication probability modeling for radiation-induced esophagitis in non-small cell lung cancer patients receiving proton radiotherapy. Radiother. Oncol. 2020, 146, 200–204. [Google Scholar] [CrossRef]
- Palma, G.; Monti, S.; Pacelli, R.; Liao, Z.; Deasy, J.O.; Mohan, R.; Cella, L. Radiation Pneumonitis in Thoracic Cancer Patients: Multi-Center Voxel-Based Analysis. Cancers 2021, 13, 3553. [Google Scholar] [CrossRef] [PubMed]
- Palma, D.A.; Senan, S.; Oberije, C.; Belderbos, J.; de Dios, N.R.; Bradley, J.D.; Barriger, R.B.; Moreno-Jimenez, M.; Kim, T.H.; Ramella, S.; et al. Predicting esophagitis after chemoradiation therapy for non-small cell lung cancer: An individual patient data meta-analysis. Int. J. Radiat. Oncol. Biol. Phys. 2013, 87, 690–696. [Google Scholar] [CrossRef]
- Palma, G.; Monti, S.; Buonanno, A.; Pacelli, R.; Cella, L. PACE: A Probabilistic Atlas for Normal Tissue Complication Estimation in Radiation Oncology. Front. Oncol. 2019, 9, 130. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | 173 pts | p-Value * | Cox-p-Value |
|---|---|---|---|
| Continuous Variables | Median (Range) | ||
| Age at RT (yr) | 66 (33–85) | 0.48 | 0.36 |
| Weight (Kg) | 79.3 (47.0–131.0) | 0.59 | 0.89 |
| KPS baseline | 80 (60–100) | 0.31 | 0.10 |
| Categorical variables | N (%) | ||
| Gender | |||
| Female | 77 (44) | 0.28 | 0.35 |
| Male | 96 (56) | ||
| Smoker | |||
| No | 15 (9) | 0.59 | 0.39 |
| Yes | 158 (91) | ||
| Induction chemotherapy | |||
| No | 116 (67) | 0.073 | 0.037 |
| Yes | 57 (33) | ||
| Adjuvant chemotherapy | |||
| No | 132 (76) | ||
| Yes | 40 (23) | 0.86 | 0.71 |
| Missing | 1 (1) | ||
| RT modality | |||
| IMRT | 109 (63) | 0.013 | 0.025 |
| PSPT | 64 (37) | ||
| Prescription dose | |||
| 66 Gy | 68 (39) | 0.87 | 0.57 |
| 74 Gy | 105 (61) | ||
| Tumor Histology | |||
| Adenocarcinoma | 89 (51) | ||
| Squamous cell carcinoma | 58 (34) | ||
| NSC NOS | 19 (11) | 0.53 | |
| Large Cell | 3 (2) | ||
| Unknown | 4 (2) | ||
| Tumor localization | |||
| Left lung | 64 (37) | 0.74 | 0.64 |
| Right lung | 109 (63) | ||
| Lower/middle lobe | 53 (30) | 0.13 | 0.12 |
| Upper lobe | 109 (67) |
| NTCP1 | NTCP2 | ||||||
|---|---|---|---|---|---|---|---|
| Model Variables | Coefficient | SE | p | Model Variables | Coefficient | SE | p |
| V55Gy | 5.26 | 1.14 | <0.001 | Dmean (Gy) | 0.06 | 0.01 | <0.001 |
| RT modality | −0.81 | 0.35 | 0.02 | RT modality | −0.90 | 0.35 | 0.01 |
| Constant | −1.18 | 0.41 | 0.004 | Constant | −2.50 | 0.69 | <0.001 |
| Performance | Value | CI/SE | Performance | Value | CI/SE | ||
| AUC | 0.74 | [0.66, 0.81] | AUC | 0.75 | [0.67, 0.81] | ||
| CV-AUC | 0.70 | [0.62, 0.78] | CV-AUC | 0.73 | [0.65, 0.80] | ||
| Calibration slope | 0.79 | 0.11 | Calibration slope | 0.91 | 0.15 | ||
| Calibration intercept | −0.03 | 0.11 | Calibration intercept | −0.02 | 0.15 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Monti, S.; Xu, T.; Mohan, R.; Liao, Z.; Palma, G.; Cella, L. Radiation-Induced Esophagitis in Non-Small-Cell Lung Cancer Patients: Voxel-Based Analysis and NTCP Modeling. Cancers 2022, 14, 1833. https://doi.org/10.3390/cancers14071833
Monti S, Xu T, Mohan R, Liao Z, Palma G, Cella L. Radiation-Induced Esophagitis in Non-Small-Cell Lung Cancer Patients: Voxel-Based Analysis and NTCP Modeling. Cancers. 2022; 14(7):1833. https://doi.org/10.3390/cancers14071833
Chicago/Turabian StyleMonti, Serena, Ting Xu, Radhe Mohan, Zhongxing Liao, Giuseppe Palma, and Laura Cella. 2022. "Radiation-Induced Esophagitis in Non-Small-Cell Lung Cancer Patients: Voxel-Based Analysis and NTCP Modeling" Cancers 14, no. 7: 1833. https://doi.org/10.3390/cancers14071833
APA StyleMonti, S., Xu, T., Mohan, R., Liao, Z., Palma, G., & Cella, L. (2022). Radiation-Induced Esophagitis in Non-Small-Cell Lung Cancer Patients: Voxel-Based Analysis and NTCP Modeling. Cancers, 14(7), 1833. https://doi.org/10.3390/cancers14071833