


Discovering the Clinical and Prognostic Role of Pan-Immune-Inflammation Values on Oral Cavity Squamous Cell Carcinoma

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Statistical Analysis
3. Results
3.1. Patient Characteristics and Clinicopathological Data
3.2. Association between PIV Groups and Patient Clinicopathological Characteristics
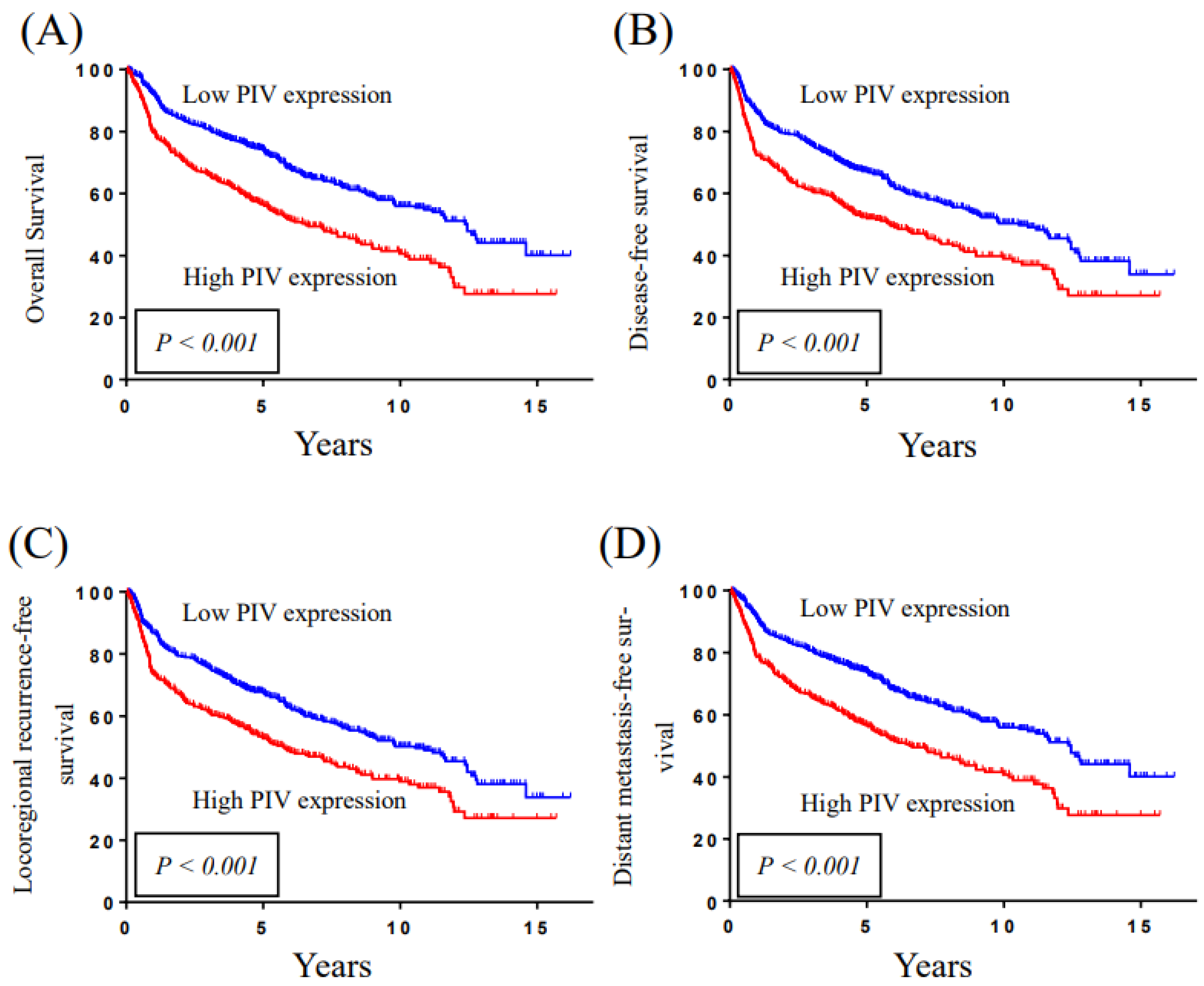
3.3. Association between PIV Groups and Survival Status in OSCC Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kao, H.K.; Lofstrand, J.; Loh, C.Y.; Lao, W.W.; Yi, J.S.; Chang, Y.L.; Chang, K.P. Nomogram based on albumin and neutrophil-to-lymphocyte ratio for predicting the prognosis of patients with oral cavity squamous cell carcinoma. Sci. Rep. 2018, 8, 13081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Machiels, J.P.; Rene Leemans, C.; Golusinski, W.; Grau, C.; Licitra, L.; Gregoire, V. Squamous cell carcinoma of the oral cavity, larynx, oropharynx and hypopharynx: EHNS-ESMO-ESTRO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 1462–1475. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.Y.; Chang, K.P.; Lin, C.Y.; Pai, P.C.; Wang, H.M.; Hsu, C.L.; Liao, C.T.; Yen, T.C.; Fang, T.J.; Huang, S.F.; et al. Prognostic significance of combined pretreatment lymphocyte counts and body mass index in patients with head and neck cancer treated with radiation therapy. Cancer Med. 2018, 7, 2808–2815. [Google Scholar] [CrossRef] [PubMed]
- Singh, N.; Baby, D.; Rajguru, J.P.; Patil, P.B.; Thakkannavar, S.S.; Pujari, V.B. Inflammation and cancer. Ann. Afr. Med. 2019, 18, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Shrotriya, S.; Walsh, D.; Bennani-Baiti, N.; Thomas, S.; Lorton, C. C-Reactive Protein Is an Important Biomarker for Prognosis Tumor Recurrence and Treatment Response in Adult Solid Tumors: A Systematic Review. PLoS One 2015, 10, e0143080. [Google Scholar] [CrossRef]
- Orange, J.S.; Ballas, Z.K. Natural killer cells in human health and disease. Clin. Immunol. 2006, 118, 1–10. [Google Scholar] [CrossRef]
- Mantovani, A. Cancer: Infammation by remote control. Nature 2005, 435, 2. [Google Scholar] [CrossRef]
- Coussens, L.M.; Werb, Z. Inflammation and cancer. Nature 2002, 420, 8. [Google Scholar] [CrossRef]
- Tsai, Y.T.; Ko, C.A.; Chen, H.C.; Hsu, C.M.; Lai, C.H.; Lee, Y.C.; Tsai, M.S.; Chang, G.H.; Huang, E.I.; Fang, K.H. Prognostic Value of CRP-Albumin-Lymphocyte (CALLY) Index in Patients Undergoing Surgery for Oral Cavity Cancer. J. Cancer 2022, 13, 3000–3012. [Google Scholar] [CrossRef]
- Tsai, Y.T.; Hsu, C.M.; Chang, G.H.; Tsai, M.S.; Lee, Y.C.; Huang, E.I.; Lai, C.H.; Fang, K.H. Advanced Lung Cancer Inflammation Index Predicts Survival Outcomes of Patients with Oral Cavity Cancer Following Curative Surgery. Front. Oncol. 2021, 11, 609314. [Google Scholar] [CrossRef]
- Eltohami, Y.I.; Kao, H.K.; Lao, W.W.; Huang, Y.; Abdelrahman, M.; Liao, C.T.; Yen, T.C.; Chang, K.P. The Prediction Value of the Systemic Inflammation Score for Oral Cavity Squamous Cell Carcinoma. Otolaryngol. Head Neck Surg. 2018, 158, 1042–1050. [Google Scholar] [CrossRef]
- Fuca, G.; Guarini, V.; Antoniotti, C.; Morano, F.; Moretto, R.; Corallo, S.; Marmorino, F.; Lonardi, S.; Rimassa, L.; Sartore-Bianchi, A.; et al. The Pan-Immune-Inflammation Value is a new prognostic biomarker in metastatic colorectal cancer: Results from a pooled-analysis of the Valentino and TRIBE first-line trials. Br. J. Cancer 2020, 123, 403–409. [Google Scholar] [CrossRef]
- Ligorio, F.; Fuca, G.; Zattarin, E.; Lobefaro, R.; Zambelli, L.; Leporati, R.; Rea, C.; Mariani, G.; Bianchi, G.V.; Capri, G.; et al. The Pan-Immune-Inflammation-Value Predicts the Survival of Patients with Human Epidermal Growth Factor Receptor 2 (HER2)-Positive Advanced Breast Cancer Treated with First-Line Taxane-Trastuzumab-Pertuzumab. Cancers 2021, 13, 1964. [Google Scholar] [CrossRef]
- Chen, X.; Hong, X.; Chen, G.; Xue, J.; Huang, J.; Wang, F.; Ali, W.; Li, J.; Zhang, L. The Pan-Immune-Inflammation Value predicts the survival of patients with anaplastic lymphoma kinase-positive non-small cell lung cancer treated with first-line ALK inhibitor. Transl. Oncol. 2022, 17, 101338. [Google Scholar] [CrossRef]
- Gambichler, T.; Stang, A.; Mansour, R.; Scheel, C.H.; Nick, C.; Abu Rached, N.; Becker, J.C.; Susok, L. Prognostic Potential of the Baseline Pan-Immune-Inflammation Value and Neutrophil/Lymphocyte Ratio in Stage I to III Melanoma Patients. Cancers 2022, 14, 1964. [Google Scholar] [CrossRef]
- Guven, D.C.; Sahin, T.K.; Erul, E.; Kilickap, S.; Gambichler, T.; Aksoy, S. The Association between the Pan-Immune-Inflammation Value and Cancer Prognosis: A Systematic Review and Meta-Analysis. Cancers 2022, 14, 2675. [Google Scholar] [CrossRef]
- Yazgan, S.C.; Yekeduz, E.; Utkan, G.; Urun, Y. Prognostic role of pan-immune-inflammation value in patients with metastatic castration-resistant prostate cancer treated with androgen receptor-signaling inhibitors. Prostate 2022, 82, 1456–1461. [Google Scholar] [CrossRef]
- Amin, M.B.; Edge, S.B.; Greene, F.L. AJCC Cancer Staging Manual, 8th ed.; Springer: New York, NY, USA, 2017. [Google Scholar]
- Shah, J.P.; Montero, P.H. New AJCC/UICC staging system for head and neck, and thyroid cancer. Rev. Médica Clínica Las Condes 2018, 29, 397–404. [Google Scholar] [CrossRef]
- Teramukai, S.; Kitano, T.; Kishida, Y.; Kawahara, M.; Kubota, K.; Komuta, K.; Minato, K.; Mio, T.; Fujita, Y.; Yonei, T.; et al. Pretreatment neutrophil count as an independent prognostic factor in advanced non-small-cell lung cancer: An analysis of Japan Multinational Trial Organisation LC00-03. Eur. J. Cancer 2009, 45, 1950–1958. [Google Scholar] [CrossRef] [Green Version]
- Phulari, R.G.S.; Rathore, R.S.; Shah, A.K.; Agnani, S.S. Neutrophil: Lymphocyte ratio and oral squamous cell carcinoma: A preliminary study. J. Oral Maxillofac. Pathol. 2019, 23, 78–81. [Google Scholar]
- Tazeen, S.; Prasad, K.; Harish, K.; Sagar, P.; Kapali, A.S.; Chandramouli, S. Assessment of Pretreatment Neutrophil/Lymphocyte Ratio and Platelet/Lymphocyte Ratio in Prognosis of Oral Squamous Cell Carcinoma. J. Oral Maxillofac. Surg. 2020, 78, 949–960. [Google Scholar] [CrossRef] [PubMed]
- Zubair, F.; McMahon, J.; Kryklyas, G.; Wicks, C. Systemic inflammatory response in predicting outcomes of patients undergoing curative resection for oral squamous cell carcinoma. Br. J. Oral Maxillofac. Surg. 2022, 60, 589–595. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.; An, H.; Xu, L.; Zhu, Y.; Yang, Y.; Lin, Z.; Xu, J. Systemic inflammation score predicts postoperative prognosis of patients with clear-cell renal cell carcinoma. Br. J. Cancer 2015, 113, 626–633. [Google Scholar] [CrossRef] [PubMed]
- Sahin, A.B.; Cubukcu, E.; Ocak, B.; Deligonul, A.; Oyucu Orhan, S.; Tolunay, S.; Gokgoz, M.S.; Cetintas, S.; Yarbas, G.; Senol, K.; et al. Low pan-immune-inflammation-value predicts better chemotherapy response and survival in breast cancer patients treated with neoadjuvant chemotherapy. Sci. Rep. 2021, 11, 14662. [Google Scholar] [CrossRef] [PubMed]
- Zeng, R.; Liu, F.; Fang, C.; Yang, J.; Luo, L.; Yue, P.; Gao, B.; Dong, Y.; Xiang, Y. PIV and PILE Score at Baseline Predict Clinical Outcome of Anti-PD-1/PD-L1 Inhibitor Combined with Chemotherapy in Extensive-Stage Small Cell Lung Cancer Patients. Front. Immunol. 2021, 12, 724443. [Google Scholar] [CrossRef]
- Lin, F.; Zhang, L.P.; Xie, S.Y.; Huang, H.Y.; Chen, X.Y.; Jiang, T.C.; Guo, L.; Lin, H.X. Pan-Immune-Inflammation Value: A New Prognostic Index in Operative Breast Cancer. Front. Oncol. 2022, 12, 830138. [Google Scholar] [CrossRef]
- Susok, L.; Said, S.; Reinert, D.; Mansour, R.; Scheel, C.H.; Becker, J.C.; Gambichler, T. The pan-immune-inflammation value and systemic immune-inflammation index in advanced melanoma patients under immunotherapy. J. Cancer Res. Clin. Oncol. 2022, 148, 3103–3108. [Google Scholar] [CrossRef]
- Topkan, E.; Selek, U.; Kucuk, A.; Pehlivan, B. Low Pre-ChemoradiotherapyPan-Immune-Inflammation Value (PIV) Measures Predict Better Survival Outcomes in Locally Advanced Pancreatic Adenocarcinomas. J. Inflamm. Res. 2022, 15, 5413–5423. [Google Scholar] [CrossRef]
- Zhao, H.; Chen, X.; Zhang, W.; Cheng, D.; Lu, Y.; Wang, C.; Li, J.; You, L.; Yu, J.; Guo, W.; et al. Pan-immune-inflammation value is associated with the clinical stage of colorectal cancer. Front. Surg. 2022, 9, 996844. [Google Scholar] [CrossRef]
- Warnakulasuriya, S. Global epidemiology of oral and oropharyngeal cancer. Oral Oncol. 2009, 45, 309–316. [Google Scholar] [CrossRef]
- Lambert, R.; Sauvaget, C.; de Camargo Cancela, M.; Sankaranarayanan, R. Epidemiology of cancer from the oral cavity and oropharynx. Eur. J. Gastroenterol. Hepatol. 2011, 23, 633–641. [Google Scholar] [CrossRef]
- Liao, C.T.; Wallace, C.G.; Lee, L.Y.; Hsueh, C.; Lin, C.Y.; Fan, K.H.; Wang, H.M.; Ng, S.H.; Lin, C.H.; Tsao, C.K.; et al. Clinical evidence of field cancerization in patients with oral cavity cancer in a betel quid chewing area. Oral Oncol. 2014, 50, 721–731. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Characteristics |
|---|---|
| Age (years) | |
| <65 | 713 (83.6%) |
| ≥65 | 140 (16.4%) |
| Gender | |
| Male | 780 (91.4%) |
| Female | 73 (8.6%) |
| Personal Habits | |
| Alcohol consumption | 583 (68.3%) |
| Betel nut chewing | 699 (81.9%) |
| Cigarettes smoking | 716 (83.9%) |
| Tumor site | |
| Buccal mucosa | 323 (37.9%) |
| Tongue | 310 (36.3%) |
| Others | 220 (25.8%) |
| Overall stage | |
| I | 164 (19.2%) |
| II | 189 (22.2%) |
| III | 129 (15.1%) |
| IV | 371 (43.5%) |
| pT classification | |
| T1 | 194 (22.7%) |
| T2 | 286 (33.5%) |
| T3 | 91 (10.7%) |
| T4 | 282 (33.1%) |
| pN classification | |
| N0 | 547 (64.1%) |
| N1 | 116 (13.6%) |
| N2 | 188 (22.0%) |
| N3 | 2 (0.3%) |
| PNI | 303 (35.6%) |
| ENE | 171 (20.1%) |
| LVI | 64 (7.5%) |
| DOI ≥ 10 mm | 427 (50.1%) |
| Surgical margin | |
| <5 mm | 260 (30.5%) |
| ≥5 mm | 593 (69.5%) |
| Adjuvant therapy | |
| Absent | 366 (42.9%) |
| Radiotherapy | 164 (19.2%) |
| Chemoradiotherapy | 323 (37.9%) |
| Neutrophil (×103 μL−1) § | 5.5 ± 16.5 |
| Platelets (×103 μL−1) § | 258.6 ± 92.0 |
| Monocyte (×103 μL−1) § | 0.5 ± 0.2 |
| Lymphocyte (×103 μL−1) § | 2.0 ± 0.8 |
| PIV § | 410.9 ± 1048.9 |
| PIV | |||
|---|---|---|---|
| Variable | <268 (n = 487) | ≥268 (n = 366) | p-Value |
| Age (years) | |||
| <65 | 400 (82.1%) | 313 (85.5%) | 0.186 |
| ≥65 | 87 (17.9%) | 53 (14.5%) | |
| Gender | |||
| Male | 430 (88.3%) | 350 (95.6%) | <0.001 * |
| Female | 57 (11.7%) | 16 (4.4%) | |
| Alcohol consumption | |||
| No | 173 (35.6%) | 97 (26.6%) | 0.005 * |
| Yes | 313 (64.4%) | 268 (73.4%) | |
| Betel nut chewing | |||
| No | 107 (22.0%) | 47 (12.9%) | <0.001 * |
| Yes | 379 (78.0%) | 318 (87.1%) | |
| Cigarettes smoking | |||
| (−) | 93 (19.1%) | 44 (12.1%) | 0.005 * |
| (+) | 393 (80.9%) | 321 (87.9%) | |
| pT classification | |||
| T1–T2 | 349 (71.7%) | 131 (35.8%) | <0.001 * |
| T3–T4 | 138 (28.3%) | 235 (64.2%) | |
| pN classification | |||
| N0 | 345 (70.8%) | 202 (55.2%) | <0.001 * |
| N1–N3 | 142 (29.2%) | 164 (44.8%) | |
| Overall Stage | |||
| I–II | 268 (55.0%) | 85 (23.2%) | <0.001 * |
| III–IV | 219 (45.0%) | 281 (76.8%) | |
| ENE | |||
| Absent | 421 (86.5%) | 261 (71.3%) | <0.001 * |
| Present | 66 (13.5%) | 105 (28.7%) | |
| Cell differentiation | |||
| W-D/M-D | 443 (91.0%) | 311 (85.0%) | 0.006 * |
| P-D | 44 (9.0%) | 55 (15.0%) | |
| LVI | |||
| Absent | 459 (94.3%) | 330 (90.2%) | 0.024 * |
| Present | 28 (5.7%) | 36 (9.8%) | |
| PNI | |||
| Absent | 351 (72.1%) | 198 (54.3%) | <0.001 * |
| Present | 136 (27.9%) | 167 (45.7%) | |
| DOI | |||
| <10 mm | 312 (64.1%) | 114 (31.2%) | <0.001 * |
| ≥10 mm | 175 (35.9%) | 252 (68.8%) | |
| OS | DFS | LRFS | DMFS | |||||
| Variable | HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value |
| Age (years) | ||||||||
| <65 | Reference | Reference | Reference | Reference | ||||
| ≥65 | 1.622 | <0.001 * | 1.454 | 0.001 * | 1.459 | 0.001 * | 1.597 | <0.001 * |
| (1.275–2.064) | (1.149–1.839) | (1.154–1.846) | (1.254–2.035) | |||||
| Gender | ||||||||
| Female | Reference | Reference | Reference | Reference | ||||
| Male | 0.833 | 0.275 | 0.773 | 0.102 | 0.773 | 0.102 | 0.832 | 0.269 |
| (0.601–1.156) | (0.567–1.053) | (0.567–1.053) | (0.599–1.154) | |||||
| Overall Stage | ||||||||
| I–II | Reference | Reference | Reference | Reference | ||||
| III–IV | 2.614 | <0.001 * | 2.287 | <0.001 * | 2.282 | <0.001 * | 2.610 | <0.001 * |
| (2.084–3.279) | (1.852–2.824) | (1.848–2.818) | (2.080–3.274) | |||||
| Surgical margin | ||||||||
| <5 mm | Reference | Reference | Reference | Reference | ||||
| ≥5 mm | 1.352 | 0.005 * | 1.282 | 0.016 * | 1.279 | 0.017 * | 1.353 | 0.004 * |
| (1.096–1.668) | (1.047–1.571) | (1.045–1.567) | (1.096–1.670) | |||||
| ENE | ||||||||
| Absent | Reference | Reference | Reference | Reference | ||||
| Present | 3.072 | <0.001 * | 2.865 | <0.001 * | 2.853 | <0.001 * | 3.096 | <0.001 * |
| (2.471–3.819) | (2.318–3.540) | (2.309–3.526) | (2.490–3.850) | |||||
| Cell differentiation | ||||||||
| W-D/M-D | Reference | Reference | Reference | Reference | ||||
| P-D | 1.746 | <0.001 * | 1.745 | <0.001 * | 1.751 | <0.001 * | 1.758 | <0.001 * |
| (1.323–2.305) | (1.337–2.277) | (1.341–2.285) | (1.331–2.320) | |||||
| LVI | ||||||||
| Absent | Reference | Reference | Reference | Reference | ||||
| Present | 1.721 | 0.001 * | 1.631 | 0.003 * | 1.608 | 0.004 * | 1.731 | 0.001 * |
| (1.231–2.406) | (1.177–2.260) | (1.161–2.228) | (1.238–2.420) | |||||
| PNI | ||||||||
| Absent | Reference | Reference | Reference | Reference | ||||
| Present | 1.871 | <0.001 * | 1.718 | <0.001 * | 1.716 | <0.001 * | 1.860 | <0.001 * |
| (1.530–2.289) | (1.415–2.084) | (1.414–2.082) | (1.520–2.275) | |||||
| DOI | ||||||||
| <10 mm | Reference | Reference | Reference | Reference | ||||
| ≥10 mm | 2.309 | <0.001 * | 2.047 | <0.001 * | 2.041 | <0.001 * | 2.303 | <0.001 * |
| (1.877–2.841) | (1.682–2.490) | (1.678–2.484) | (1.871–2.834) | |||||
| Adjuvant Tx | ||||||||
| Without | Reference | Reference | Reference | Reference | ||||
| With | 2.326 | <0.001 * | 2.199 | <0.001 * | 2.195 | <0.001 * | 2.321 | <0.001 * |
| (1.868–2.896) | (1.787–2.706) | (1.784–2.701) | (1.864–2.890) | |||||
| PIV | ||||||||
| <268 | Reference | Reference | Reference | Reference | ||||
| ≥268 | 1.723 | <0.001 * | 1.531 | <0.001 * | 1.521 | <0.001 * | 1.717 | <0.001 * |
| (1.410–2.105) | (1.264–1.854) | (1.255–1.842) | (1.405–2.099) | |||||
| OS | DFS | LRFS | DMFS | |||||
|---|---|---|---|---|---|---|---|---|
| Variable | HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value |
| Age (years) | ||||||||
| <65 | Reference | Reference | Reference | Reference | ||||
| ≥65 | 1.023 | <0.001 * | 1.018 | <0.001 * | 1.018 | <0.001 * | 1.022 | <0.001 * |
| (1.014–1.032) | (1.009–1.027) | (1.010–1.027) | (1.013–1.031) | |||||
| Gender | ||||||||
| Female | Reference | Reference | Reference | Reference | ||||
| Male | 0.823 | 0.257 | 0.780 | 0.126 | 0.783 | 0.132 | 0.824 | 0.260 |
| (0.588–1.153) | (0.567–1.073) | (0.569–1.077) | (0.589–1.154) | |||||
| Overall Stage | ||||||||
| I–II | Reference | Reference | Reference | Reference | ||||
| III–IV | 1.460 | 0.025 * | 1.292 | 0.111 | 1.290 | 0.114 | 1.459 | 0.026 * |
| (1.047–2.036) | (0.943–1.770) | (0.941–1.769) | (1.046–2.034) | |||||
| ENE | ||||||||
| Absent | Reference | Reference | Reference | Reference | ||||
| Present | 2.004 | <0.001 * | 1.961 | <0.001 * | 1.963 | <0.001 * | 2.024 | <0.001 * |
| (1.551–2.589) | (1.530–2.514) | (1.531–2.516) | (1.565–2.617) | |||||
| Surgical margin | ||||||||
| <5 mm | Reference | Reference | Reference | Reference | ||||
| ≥5 mm | 1.013$$%(0.816–1.256) | 0.910 | 0.997$$%(0.810–1.227) | 0.975 | 0.994$$%(0.807–1.224) | 0.953 | 1.013$$%(0.816–1.257) | 0.904 |
| DOI | ||||||||
| <10 mm | Reference | Reference | Reference | Reference | ||||
| ≥10 mm | 1.468 | 0.004 * | 1.359 | 0.017 * | 1.370 | 0.014 * | 1.467 | 0.004 * |
| (1.126–1.915) | (1.055–1.750) | (1.064–1.764) | (1.124–1.913) | |||||
| Cell Differentiation | ||||||||
| W-D/M-D | Reference | Reference | Reference | Reference | ||||
| P-D | 1.117 | 0.456 | 1.169 | 0.275 | 1.184 | 0.237 | 1.126 | 0.426 |
| (0.834–1.497) | (0.883–1.546) | (0.895–1.566) | (0.841–1.509) | |||||
| PNI | ||||||||
| Absent | Reference | Reference | Reference | Reference | ||||
| Present | 1.160 | 0.221 | 1.092 | 0.452 | 1.088 | 0.468 | 1.144 | 0.268 |
| (0.914–1.472) | (0.868–1.373) | (0.865–1.369) | (0.901–1.453) | |||||
| LVI | ||||||||
| Absent | Reference | Reference | Reference | Reference | ||||
| Present | 0.873 | 0.458 | 0.893 | 0.525 | 0.881 | 0.477 | 0.880 | 0.485 |
| (0.609–1.251) | (0.630–1.266) | (0.622–1.249) | (0.614–1.261) | |||||
| Adjuvant tx | ||||||||
| Without | Reference | Reference | Reference | Reference | ||||
| With | 1.055 | 0.751 | 1.174 | 0.326 | 1.170 | 0.337 | 1.056 | 0.749 |
| (0.757–1.472) | (0.852–1.617) | (0.849–1.613) | (0.757–1.472) | |||||
| PIV | ||||||||
| <268 | Reference | Reference | Reference | Reference | ||||
| ≥268 | 1.281 | 0.027 * | 1.165 | 0.157 | 1.159 | 0.170 | 1.274 | 0.031 * |
| (1.027–1.596) | (0.943–1.438) | (0.939–1.432) | (1.022–1.588) | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yeh, C.-C.; Kao, H.-K.; Huang, Y.; Tsai, T.-Y.; Young, C.-K.; Hung, S.-Y.; Lu, C.-Y.; Chang, K.-P. Discovering the Clinical and Prognostic Role of Pan-Immune-Inflammation Values on Oral Cavity Squamous Cell Carcinoma. Cancers 2023, 15, 322. https://doi.org/10.3390/cancers15010322
Yeh C-C, Kao H-K, Huang Y, Tsai T-Y, Young C-K, Hung S-Y, Lu C-Y, Chang K-P. Discovering the Clinical and Prognostic Role of Pan-Immune-Inflammation Values on Oral Cavity Squamous Cell Carcinoma. Cancers. 2023; 15(1):322. https://doi.org/10.3390/cancers15010322
Chicago/Turabian StyleYeh, Chia-Chi, Huang-Kai Kao, Yenlin Huang, Tsung-You Tsai, Chi-Kuang Young, Shao-Yu Hung, Chuieng-Yi Lu, and Kai-Ping Chang. 2023. "Discovering the Clinical and Prognostic Role of Pan-Immune-Inflammation Values on Oral Cavity Squamous Cell Carcinoma" Cancers 15, no. 1: 322. https://doi.org/10.3390/cancers15010322
APA StyleYeh, C.-C., Kao, H.-K., Huang, Y., Tsai, T.-Y., Young, C.-K., Hung, S.-Y., Lu, C.-Y., & Chang, K.-P. (2023). Discovering the Clinical and Prognostic Role of Pan-Immune-Inflammation Values on Oral Cavity Squamous Cell Carcinoma. Cancers, 15(1), 322. https://doi.org/10.3390/cancers15010322