

Nectin-4 as a Predictive Marker for Poor Prognosis of Endometrial Cancer with Mismatch Repair Impairment

 , , , ,
, , , ,  and
and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Tissue Specimens
2.2. Tissue Microarray Construction and Immunohistochemistry
2.3. Public Databases
2.4. Statistical Analysis
3. Results
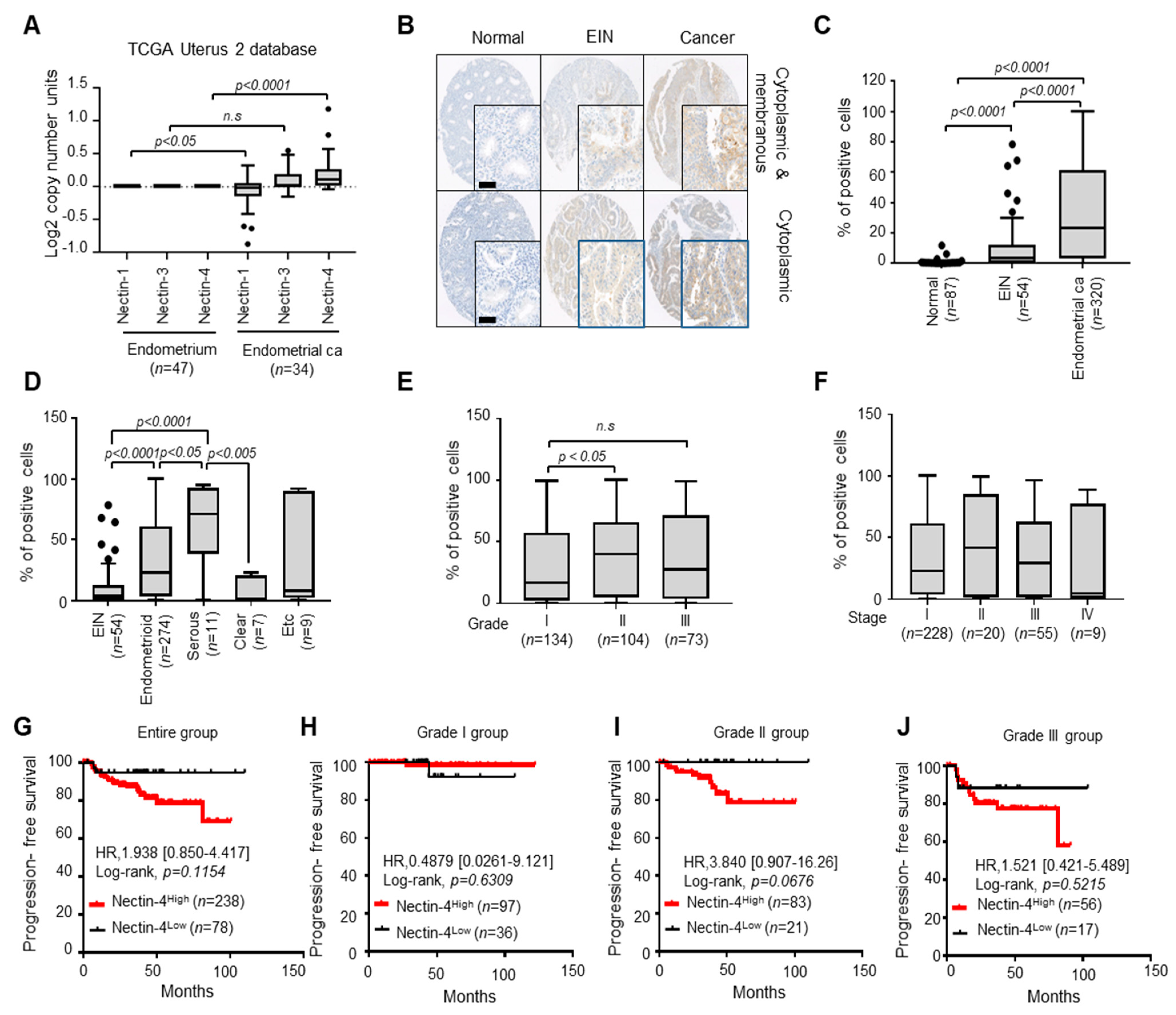
3.1. Nectin-4 Is Overexpressed in EC Tissues Compared with Normal Endometrial and EIN Tissues
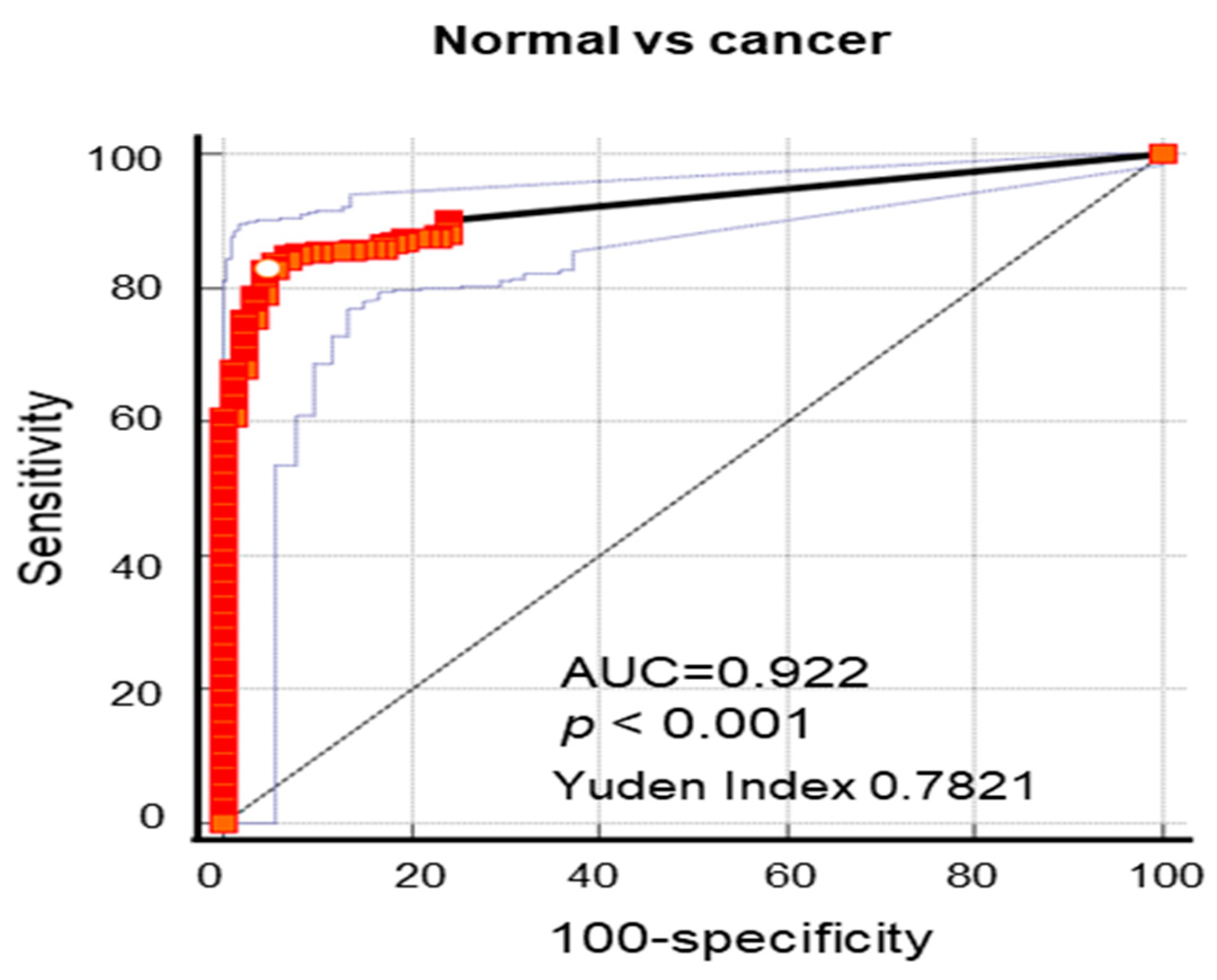
3.2. Nectin-4 Is a Powerful Diagnostic Marker of EC
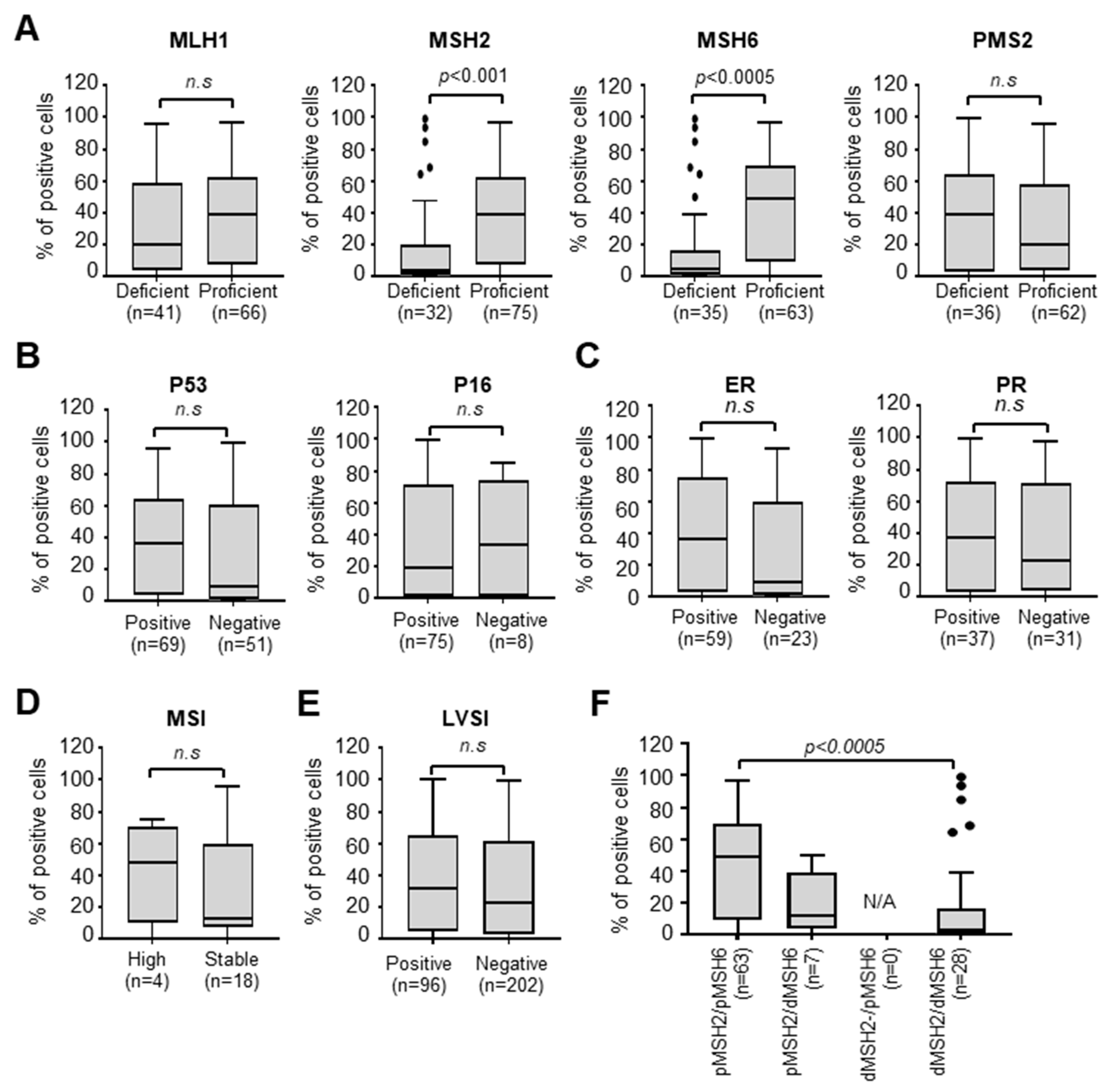
3.3. Nectin-4 Is Associated with MMR Deficiency
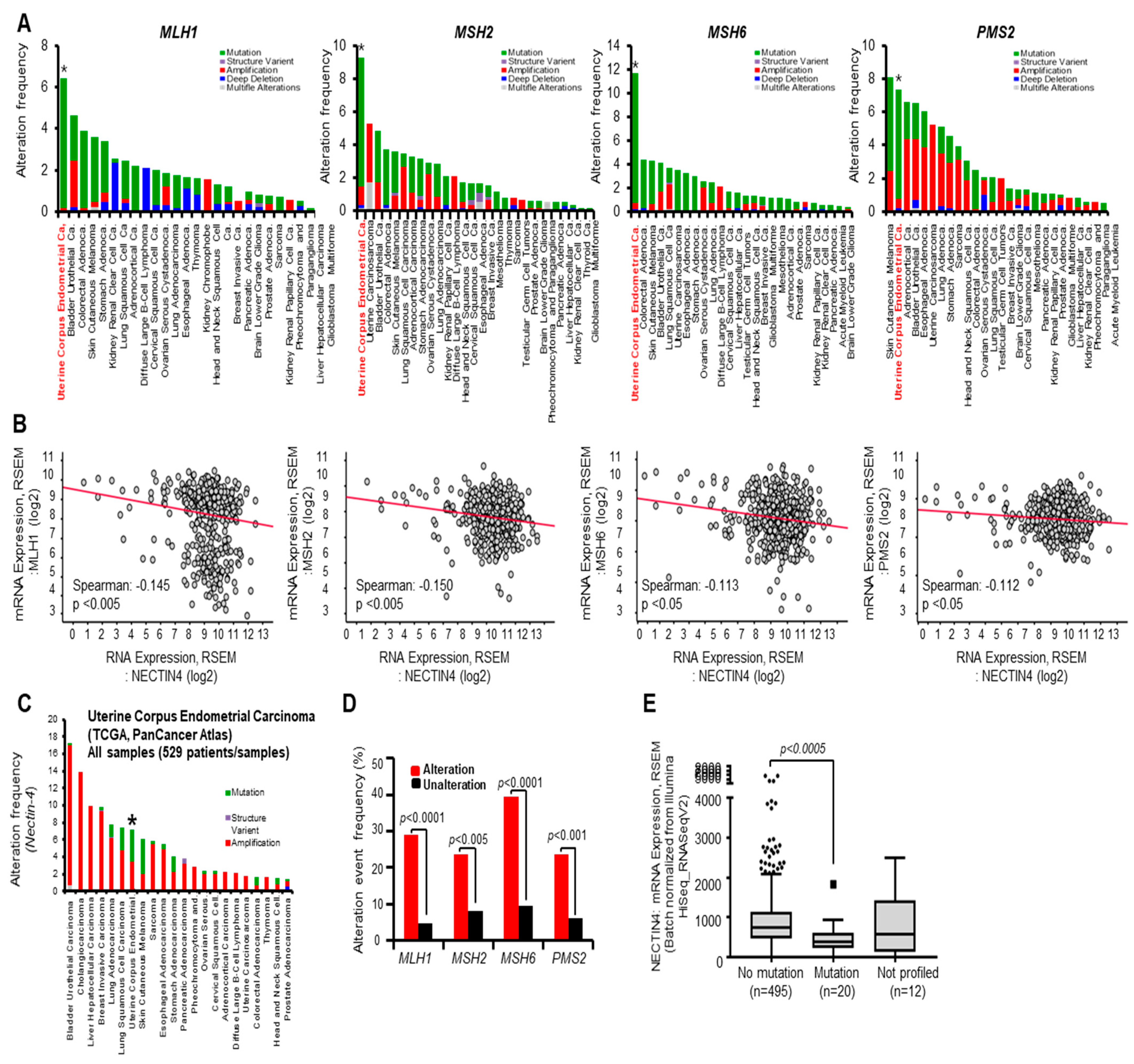
3.4. Alteration Frequency of MMR Is Associated with Nectin-4 Expression in EC
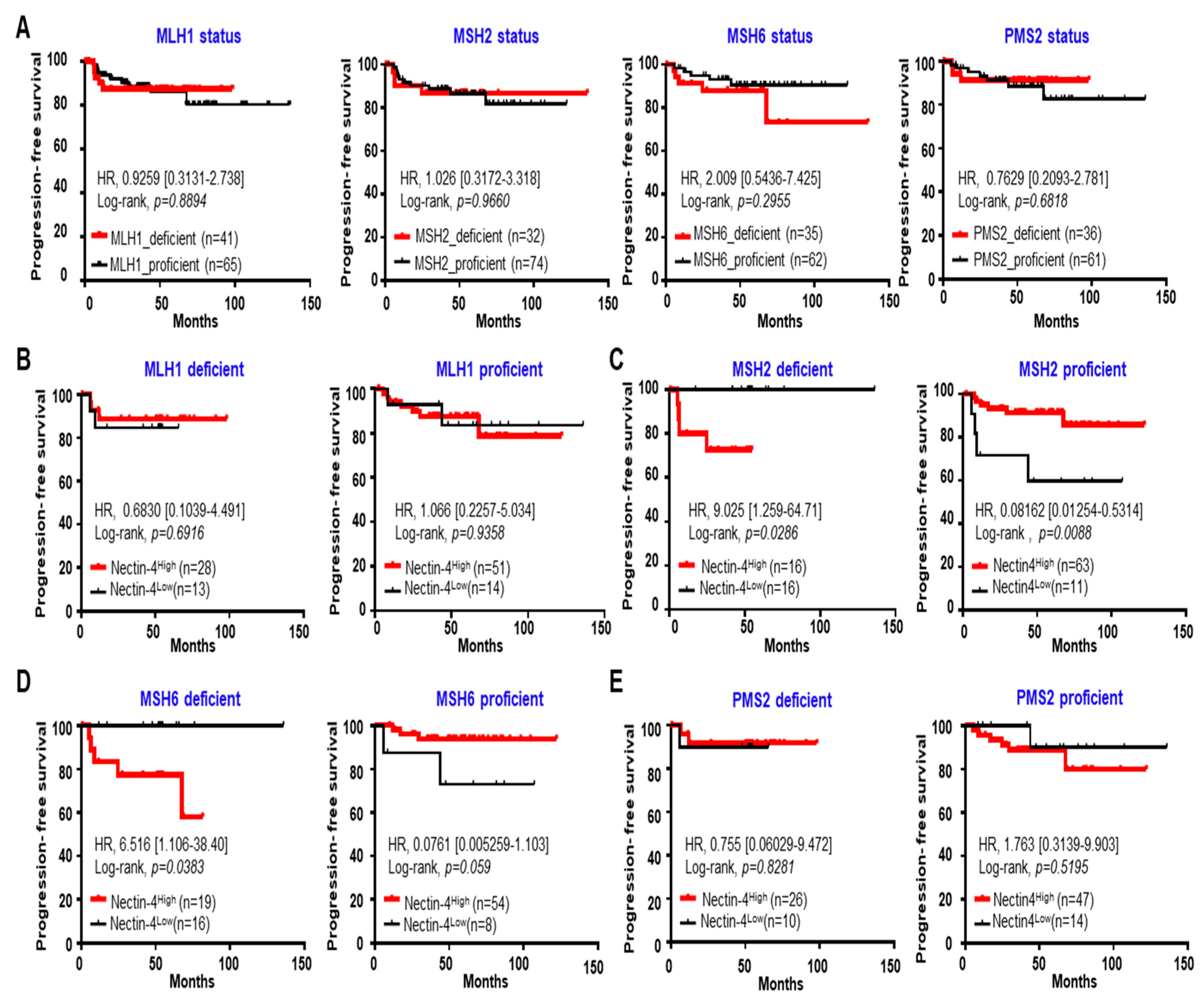
3.5. High Expression of Nectin-4 in MSH2 Deficiency Caused a Short PFS in EC
3.6. Increase in LVSI-Positive Patients in the MSH2-Deficient/Nectin-4High Group
3.7. Decrease in CD8-Positive Patients in the MSH2-Deficient/Nectin-4High Group
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Parkin, D.M.; Pisani, P.; Ferlay, J. Estimates of the worldwide incidence of 25 major cancers in 1990. Int. J. Cancer 1999, 80, 827–841. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Masuda, K.; Banno, K.; Yanokura, M.; Kobayashi, Y.; Kisu, I.; Ueki, A.; Ono, A.; Asahara, N.; Nomura, H.; Hirasawa, A.; et al. Relationship between DNA Mismatch Repair Deficiency and Endometrial Cancer. Mol. Biol. Int. 2011, 2011, 256063. [Google Scholar] [CrossRef]
- Aarnio, M.; Sankila, R.; Pukkala, E.; Salovaara, R.; Aaltonen, L.A.; de la Chapelle, A.; Peltomäki, P.; Mecklin, J.P.; Järvinen, H.J. Cancer risk in mutation carriers of DNA-mismatch-repair genes. Int. J. Cancer 1999, 81, 214–218. [Google Scholar] [CrossRef]
- MacDonald, N.D.; Salvesen, H.B.; Ryan, A.; Iversen, O.E.; Akslen, L.A.; Jacobs, I.J. Frequency and prognostic impact of microsatellite instability in a large population-based study of endometrial carcinomas. Cancer Res. 2000, 60, 1750–1752. [Google Scholar]
- Bell, D.W.; Ellenson, L.H. Molecular genetics of endometrial carcinoma. Annu. Rev. Pathol. 2019, 14, 339–367. [Google Scholar] [CrossRef]
- Reitsam, N.G.; Märkl, B.; Dintner, S.; Waidhauser, J.; Vlasenko, D.; Grosser, B. Concurrent loss of MLH1, PMS2 and MSH6 immunoexpression in digestive system cancers indicating a widespread dysregulation in DNA repair processes. Front. Oncol. 2022, 12, 1019798. [Google Scholar] [CrossRef]
- McCoy, P.; Mangiola, S.; Macintyre, G.; Hutchinson, R.; Tran, B.; Pope, B.; Georgeson, P.; Hong, M.K.H.; Kurganovs, N.; Lunke, S.; et al. MSH2-deficient prostate tumours have a distinct immune response and clinical outcome compared to MSH2-deficient colorectal or endometrial cancer. Prostate Cancer Prostatic. Dis. 2021, 24, 1167–1180. [Google Scholar] [CrossRef]
- McMeekin, D.S.; Tritchler, D.L.; Cohn, D.E.; Mutch, D.G.; Lankes, H.A.; Geller, M.A.; Powell, M.A.; Backes, F.J.; Landrum, L.M.; Zaino, R.; et al. Clinicopathologic Significance of Mismatch Repair Defects in Endometrial Cancer: An NRG Oncology/Gynecologic Oncology Group Study. J. Clin. Oncol. 2016, 34, 3062–3068. [Google Scholar] [CrossRef]
- Shikama, A.; Minaguchi, T.; Matsumoto, K.; Akiyama-Abe, A.; Nakamura, Y.; Michikami, H.; Nakao, S.; Sakurai, M.; Ochi, H.; Onuki, M.; et al. Clinicopathologic implications of DNA mismatch repair status in endometrial carcinomas. Gynecol. Oncol. 2016, 140, 226–233. [Google Scholar] [CrossRef]
- Cosgrove, C.M.; Cohn, D.E.; Hampel, H.; Frankel, W.L.; Jones, D.; McElroy, J.P.; Suarez, A.A.; Zhao, W.; Chen, W.; Salani, R.; et al. Epigenetic silencing of MLH1 in endometrial cancers is associated with larger tumor volume, increased rate of lymph node positivity and reduced recurrence-free survival. Gynecol. Oncol. 2017, 146, 588–595. [Google Scholar] [CrossRef]
- Carr, C.; Son, J.; Yao, M.; Priyadarshini, A.; Marquard, J.; Vargas, R.; Michener, C.; AlHilli, M.M. Clinicopathologic characteristics and outcomes of endometrial Cancer patients with mismatch repair deficiency in the era of universal Lynch syndrome screening. Gynecol. Oncol. 2020, 159, 712–720. [Google Scholar] [CrossRef]
- Pasanen, A.; Loukovaara, M.; Bützow, R. Clinicopathological significance of deficient DNA mismatch repair and MLH1 promoter methylation in endometrioid endometrial carcinoma. Mod. Pathol. 2020, 33, 1443–1452. [Google Scholar] [CrossRef]
- Kim, S.R.; Tone, A.; Kim, R.H.; Cesari, M.; Clarke, B.A.; Eiriksson, L.; Hart, T.; Aronson, M.; Holter, S.; Lytwyn, A.; et al. Understanding the clinical implication of mismatch repair deficiency in endometrioid endometrial cancer through a prospective study. Gynecol. Oncol. 2021, 161, 221–227. [Google Scholar] [CrossRef]
- Diaz-Padilla, I.; Romero, N.; Amir, E.; Matias-Guiu, X.; Vilar, E.; Muggia, F.; Garcia-Donas, J. Mismatch repair status and clinical outcome in endometrial cancer: A systematic review and meta-analysis. Crit. Rev. Oncol. Hematol. 2013, 88, 154–167. [Google Scholar] [CrossRef]
- Nagle, C.M.; O’Mara, T.A.; Tan, Y.; Buchanan, D.D.; Obermair, A.; Blomfield, P.; Quinn, M.A.; Webb, P.M.; Spurdle, A.B. Australian Endometrial Cancer Study Group. Endometrial cancer risk and survival by tumor MMR status. J. Gynecol. Oncol. 2018, 29, e39. [Google Scholar] [CrossRef]
- Noyce, R.S.; Richardson, C.D. Nectin 4 is the epithelial cell receptor for measles virus. Trends Microbiol. 2012, 20, 429–439. [Google Scholar] [CrossRef]
- Mühlebach, M.D.; Mateo, M.; Sinn, P.L.; Prüfer, S.; Uhlig, K.M.; Leonard, V.H.; Navaratnarajah, C.K.; Frenzke, M.; Wong, X.X.; Sawatsky, B.; et al. Adherens junction protein nectin-4 is the epithelial receptor for measles virus. Nature 2011, 480, 530–533. [Google Scholar] [CrossRef]
- Bouleftour, W.; Guillot, A.; Magne, N. The Anti-Nectin 4: A Promising Tumor Cells Target. A Systematic Review. Mol. Cancer Ther. 2022, 21, 493–501. [Google Scholar] [CrossRef]
- Tomiyama, E.; Fujita, K.; Rodriguez Pena, M.D.C.; Taheri, D.; Banno, E.; Kato, T.; Hatano, K.; Kawashima, A.; Ujike, T.; Uemura, M.; et al. Expression of Nectin-4 and PD-L1 in Upper Tract Urothelial Carcinoma. Int. J. Mol. Sci. 2020, 21, 5390. [Google Scholar] [CrossRef]
- Takano, A.; Ishikawa, N.; Nishino, R.; Masuda, K.; Yasui, W.; Inai, K.; Nishimura, H.; Ito, H.; Nakayama, H.; Miyagi, Y.; et al. Identification of nectin-4 oncoprotein as a diagnostic and therapeutic target for lung cancer. Cancer Res. 2009, 69, 6694–6703. [Google Scholar] [CrossRef]
- Derycke, M.S.; Pambuccian, S.E.; Gilks, C.B.; Kalloger, S.E.; Ghidouche, A.; Lopez, M.; Bliss, R.L.; Geller, M.A.; Argenta, P.A.; Harrington, K.M.; et al. Nectin 4 overexpression in ovarian cancer tissues and serum: Potential role as a serum biomarker. Am. J. Clin. Pathol. 2010, 134, 835–845. [Google Scholar] [CrossRef]
- Nishiwada, S.; Sho, M.; Yasuda, S.; Shimada, K.; Yamato, I.; Akahori, T.; Kinoshita, S.; Nagai, M.; Konishi, N.; Nakajima, Y. Nectin-4 expression contributes to tumor proliferation, angiogenesis and patient prognosis in human pancreatic cancer. J. Exp. Clin. Cancer Res. 2015, 34, 30. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhang, J.; Shen, Q.; Yin, W.; Huang, H.; Liu, Y.; Ni, Q. High expression of Nectin-4 is associated with unfavorable prognosis in gastric cancer. Oncol. Lett. 2018, 15, 8789–8795. [Google Scholar] [CrossRef]
- Zhang, Y.; Liu, S.; Wang, L.; Wu, Y.; Hao, J.; Wang, Z.; Lu, W.; Wang, X.A.; Zhang, F.; Cao, Y.; et al. A novel PI3K/AKT signaling axis mediates Nectin-4-induced gallbladder cancer cell proliferation, metastasis and tumor growth. Cancer Lett. 2016, 375, 179–189. [Google Scholar] [CrossRef]
- Pavlova, N.N.; Pallasch, C.; Elia, A.E.; Braun, C.J.; Westbrook, T.F.; Hemann, M.; Elledge, S.J. A role for PVRL4-driven cell-cell interactions in tumorigenesis. eLife 2013, 2, e00358. [Google Scholar] [CrossRef]
- Siddharth, S.; Goutam, K.; Das, S.; Nayak, A.; Nayak, D.; Sethy, C.; Wyatt, M.D.; Kundu, C.N. Nectin-4 is a breast cancer stem cell marker that induces WNT/β-catenin signaling via Pi3k/Akt axis. Int. J. Biochem. Cell Biol. 2017, 89, 85–94. [Google Scholar] [CrossRef]
- Zhang, Y.; Chen, P.; Yin, W.; Ji, Y.; Shen, Q.; Ni, Q. Nectin-4 promotes gastric cancer progression via the PI3K/AKT signaling pathway. Hum. Pathol. 2018, 72, 107–116. [Google Scholar] [CrossRef]
- Heath, E.I.; Rosenberg, J.E. The biology and rationale of targeting nectin-4 in urothelial carcinoma. Nat. Rev. Urol. 2021, 18, 93–103. [Google Scholar] [CrossRef]
- Fabre-Lafay, S.; Monville, F.; Garrido-Urbani, S.; Berruyer-Pouyet, C.; Ginestier, C.; Reymond, N.; Finetti, P.; Sauvan, R.; Adélaïde, J.; Geneix, J.; et al. Nectin-4 is a new histological and serological tumor associated marker for breast cancer. BMC Cancer 2007, 7, 73. [Google Scholar] [CrossRef]
- Challita-Eid, P.M.; Satpayev, D.; Yang, P.; An, Z.; Morrison, K.; Shostak, Y.; Raitano, A.; Nadell, R.; Liu, W.; Lortie, D.R.; et al. Enfortumab Vedotin Antibody-Drug Conjugate Targeting Nectin-4 Is a Highly Potent Therapeutic Agent in Multiple Preclinical Cancer Models. Cancer Res. 2016, 76, 3003–3013. [Google Scholar] [CrossRef]
- Siegel, R.; Ma, J.; Zou, Z.; Jemal, A. Cancer statistics, 2014. CA Cancer J. Clin. 2014, 64, 9–29. [Google Scholar] [CrossRef]
- Moore, M.J.; Goldstein, D.; Hamm, J.; Figer, A.; Hecht, J.R.; Gallinger, S.; Au, H.J.; Murawa, P.; Walde, D.; Wolff, R.A.; et al. Erlotinib plus gemcitabine compared with gemcitabine alone in patients with advanced pancreatic cancer: A phase III trial of the National Cancer Institute of Canada Clinical Trials Group. J. Clin. Oncol. 2007, 25, 1960–1966. [Google Scholar] [CrossRef]
- Rajc, J.; Gugić, D.; Fröhlich, I.; Marjanović, K.; Dumenčić, B. Prognostic role of Nectin-4 expression in luminal B (HER2 negative) breast cancer. Pathol. Res. Pract. 2017, 213, 1102–1108. [Google Scholar] [CrossRef]
- Siddharth, S.; Nayak, A.; Das, S.; Nayak, D.; Panda, J.; Wyatt, M.D.; Kundu, C.N. The soluble nectin-4 ecto-domain promotes breast cancer induced angiogenesis via endothelial Integrin-β4. Int. J. Biochem. Cell Biol. 2018, 102, 151–160. [Google Scholar] [CrossRef]
- Zeindler, J.; Soysal, S.D.; Piscuoglio, S.; Ng, C.K.Y.; Mechera, R.; Isaak, A.; Weber, W.P.; Muenst, S.; Kurzeder, C. Nectin-4 Expression Is an Independent Prognostic Biomarker and Associated with Better Survival in Triple-Negative Breast Cancer. Front. Med. 2019, 6, 200. [Google Scholar] [CrossRef]
- Liu, Y.; Li, G.; Zhang, Y.; Li, L.; Zhang, Y.; Huang, X.; Wei, X.; Zhou, P.; Liu, M.; Zhao, G.; et al. Nectin-4 promotes osteosarcoma progression and metastasis through activating PI3K/AKT/NF-κB signaling by down-regulation of miR-520c-3p. Cancer Cell Int. 2022, 22, 252. [Google Scholar] [CrossRef]
- Hashimoto, H.; Tanaka, Y.; Murata, M.; Ito, T. Nectin-4: A Novel Therapeutic Target for Skin Cancers. Curr. Treat Options Oncol. 2022, 23, 578–593. [Google Scholar] [CrossRef]
- Kedashiro, S.; Kameyama, T.; Mizutani, K.; Takai, Y. Nectin-4 and p95-ErbB2 cooperatively regulate Hippo signaling-dependent SOX2 gene expression, enhancing anchorage-independent T47D cell proliferation. Sci. Rep. 2021, 11, 7344. [Google Scholar] [CrossRef]
- Sethy, C.; Goutam, K.; Das, B.; Dash, S.R.; Kundu, C.N. Nectin-4 promotes lymphangiogenesis and lymphatic metastasis in breast cancer by regulating CXCR4-LYVE-1 axis. Vascul. Pharmacol. 2021, 140, 106865. [Google Scholar] [CrossRef]
- Murali, R.; Soslow, R.A.; Weigelt, B. Classification of endometrial carcinoma: More than two types. Lancet Oncol. 2014, 15, e268–e278. [Google Scholar] [CrossRef]
- Alexa, M.; Hasenburg, A.; Battista, M.J. The TCGA Molecular Classification of Endometrial Cancer and Its Possible Impact on Adjuvant Treatment Decisions. Cancers 2021, 13, 1478. [Google Scholar] [CrossRef]
- Talhouk, A.; McConechy, M.K.; Leung, S.; Yang, W.; Lum, A.; Senz, J.; Boyd, N.; Pike, J.; Anglesio, M.; Kwon, J.S.; et al. Confirmation of ProMisE: A simple, genomics-based clinical classifier for endometrial cancer. Cancer 2017, 123, 802–813. [Google Scholar] [CrossRef]
- Li, K.; Luo, H.; Huang, L.; Luo, H.; Zhu, X. Microsatellite instability: A review of what the oncologist should know. Cancer Cell Int. 2020, 20, 16. [Google Scholar] [CrossRef]
- Kurnit, K.C.; Westin, S.N.; Coleman, R.L. Microsatellite instability in endometrial cancer: New purpose for an old test. Cancer 2019, 125, 2154–2163. [Google Scholar] [CrossRef]
- Zhang, X.; Wu, T.; Cai, X.; Dong, J.; Xia, C.; Zhou, Y.; Ding, R.; Yang, R.; Tan, J.; Zhang, L.; et al. Neoadjuvant Immunotherapy for MSI-H/dMMR Locally Advanced Colorectal Cancer: New Strategies and Unveiled Opportunities. Front. Immunol. 2022, 13, 795972. [Google Scholar] [CrossRef]
- Di Dio, C.; Bogani, G.; Di Donato, V.; Cuccu, I.; Muzii, L.; Musacchio, L.; Scambia, G.; Lorusso, D. The role of immunotherapy in advanced and recurrent MMR deficient and proficient endometrial carcinoma. Gynecol. Oncol. 2023, 169, 27–33. [Google Scholar] [CrossRef]
- Gelsomino, F.; Barbolini, M.; Spallanzani, A.; Pugliese, G.; Cascinu, S. The evolving role of microsatellite instability in colorectal cancer: A review. Cancer Treat Rev. 2016, 51, 19–26. [Google Scholar] [CrossRef]
- Wang, L.; Yang, M.; Guo, X.; Yang, Z.; Liu, S.; Ji, Y.; Jin, H. Estrogen-related receptor-α promotes gallbladder cancer development by enhancing the transcription of Nectin-4. Cancer Sci. 2020, 111, 1514–1527. [Google Scholar] [CrossRef]
- Chen, J.; Bhandari, A.; Hirachan, S.; Lv, S.; Mainali, S.; Zheng, C.; Hao, R. A Specificity Protein 1 assists the progression of the papillary thyroid cell line by initiating NECTIN4. Endocr. Metab. Immune Disord. Drug Targets 2023. [Google Scholar] [CrossRef]
- Mandai, K.; Rikitake, Y.; Mori, M.; Takai, Y. Nectins and nectin-like molecules in development and disease. Curr. Top. Dev. Biol. 2015, 112, 197–231. [Google Scholar]
- Mizutani, K.; Kedashiro, S.; Maruoka, M.; Ueda, Y.; Takai, Y. Nectin-like molecule-4/cell adhesion molecule 4 inhibits the ligand-induced dimerization of ErbB3 with ErbB2. Sci. Rep. 2017, 7, 11375. [Google Scholar] [CrossRef]
- Maruoka, M.; Kedashiro, S.; Ueda, Y.; Mizutani, K.; Takai, Y. Nectin-4 co-stimulates the prolactin receptor by interacting with SOCS1 and inhibiting its activity on the JAK2-STAT5a signaling pathway. J. Biol. Chem. 2017, 292, 6895–6909. [Google Scholar] [CrossRef]
- Sakamoto, Y.; Ogita, H.; Hirota, T.; Kawakatsu, T.; Fukuyama, T.; Yasumi, M.; Kanzaki, N.; Ozaki, M.; Takai, Y. Interaction of integrin alpha(v)beta3 with nectin. Implication in cross-talk between cell-matrix and cell-cell junctions. J. Biol. Chem. 2006, 281, 19631–19644. [Google Scholar] [CrossRef]
- Kedashiro, S.; Sugiura, A.; Mizutani, K.; Takai, Y. Nectin-4 cis-interacts with ErbB2 and its trastuzumab-resistant splice variants, enhancing their activation and DNA synthesis. Sci. Rep. 2019, 9, 18997. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Nectin-4 Expression | ||
|---|---|---|---|
| Nectin-4High | Nectin-4Low | p-Value | |
| n (%) | n (%) | ||
| Diagnosis | 0.000 * | ||
| Nonadjacent normal tissue | 2 (2.3%) | 85 (97.7%) | |
| EIN | 28 (51.9%) | 26 (48.1%) | |
| Cancer | 240 (75.0%) | 80 (25.0%) | |
| Age | 0.098 | ||
| ≥50 | 179 (74.6%) | 52 (65.0%) | |
| 50< | 61 (25.4%) | 28 (35.0%) | |
| FIGO stage | 0.900 | ||
| I | 173 (72.1%) | 55 (68.8%) | |
| II | 14 (5.8%) | 6 (7.5%) | |
| III | 40 (16.7%) | 15 (18.8%) | |
| IV | 6 (2.5%) | 3 (3.8%) | |
| Recurrence | 6 (2.5%) | 1 (1.3%) | |
| Unclassified | 1 (0.4%) | 0 (0%) | |
| Differentiation | 0.059 | ||
| Grade I | 97 (40.4%) | 37 (46.3%) | |
| Grade II | 83 (34.6%) | 21 (26.3%) | |
| Grade III | 56 (23.3%) | 17 (21.3%) | |
| Mix | 0 (0%) | 2 (2.5%) | |
| Unclassified | 4 (1.7%) | 3 (3.8%) | |
| Histology | 0.076 | ||
| Endometrioid | 206 (85.8%) | 68 (85.0%) | |
| Serous | 10 (4.2%) | 1 (1.3%) | |
| Clear | 2 (0.8%) | 5 (6.3%) | |
| Mix | 14 (5.8%) | 4 (5.0%) | |
| ETS | 7 (2.9%) | 2 (2.5%) | |
| Unclassified | 1 (0.4%) | 0 (0.0%) | |
| CA125 (U/mL) | 0.559 | ||
| ≥35 | 167 (69.6%) | 58 (72.5%) | |
| 35< | 60 (25.0%) | 20 (25.0%) | |
| Unclassified | 13 (5.4%) | 2 (2.5%) | |
| MSH2 status | 0.001 * | ||
| Deficient | 16 (6.7%) | 16 (20.0%) | |
| Proficient | 63 (26.3%) | 12 (15.0%) | |
| Unclassified | 161 (67.1%) | 52 (65.0%) | |
| MSH6 status | 0.003 * | ||
| Deficient | 19 (7.90%) | 16 (20.0%) | |
| Proficient | 54 (22.5%) | 9 (11.3%) | |
| Unclassified | 167 (69.6%) | 55 (68.8%) | |
| Group | Youden Index J | ROC–AUC (95%CI) | Sensitivity (95%CI) | Specificity (95%CI) | PPV (95%CI) | NPV (95%CI) |
|---|---|---|---|---|---|---|
| Nectin-4 | 0.7821 | 0.922 (0.892–0.946) | 82.81 (78.2–86.8) | 95.40 (88.6–98.7) | 98.5 (96.2–99.4) | 60.1 (54.2–65.8) |
| Group | Odds Ratio | (95% CI) | p-Value |
|---|---|---|---|
| Nectin-4 > 0.7821% | 79.01 | (30.60–203.99) | <0.0001 |
| Gene | Altered Group | Unaltered Group | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Max. | 75% | Median | 25% | Min. | Max. | 75% | Median | 25% | Min. | p-Value | ||
| Nectin-4 | Tumor mutation burden (nonsynonymous) | 748.4 | 300.6 | 15.4 | 2.1 | 0.9 | 38.7 | 16.4 | 2.4 | 1.5 | 0 | <0.0001 |
| MSIsensor Score | 23.17 | 9.49 | 0.97 | 0.37 | 0 | 26.4 | 10.65 | 0.41 | 0.09 | 0 | 0.0431 | |
| MSH2 | Tumor mutation burden (nonsynonymous) | 758.8 | 325.1 | 166.9 | 36.1 | 1.1 | 33.0 | 14.1 | 2.3 | 1.5 | 0 | <0.0001 |
| MSIsensor Score | 35.7 | 16.0 | 2.1 | 0.35 | 0.0 | 24.4 | 9.83 | 0.4 | 0.09 | 0 | <0.0001 | |
| MSH6 | Tumor mutation burden (nonsynonymous) | 763.9 | 325.1 | 192.3 | 32.6 | 1.1 | 27.1 | 11.7 | 2.2 | 1.5 | 0 | <0.0001 |
| MSIsensor Score | 34.8 | 14.3 | 2.6 | 0.7 | 0 | 22.8 | 9.1 | 0.3 | 0.0 | 0 | <0.0001 | |
| Clinicopathologic Variables | MSH2 Status | MSH6 Status | ||||
|---|---|---|---|---|---|---|
| Deficiency | Proficiency | p-Value | Deficiency | Proficiency | p-Value | |
| n = 32 | n = 75 | n = 35 | n = 63 | |||
| Age | 0.091 | 0.604 | ||||
| ≥50 | 20 (62.5%) | 58 (77.3%) | 25 (71.4%) | 48 (76.2%) | ||
| <50 | 12 (37.5%) | 17 (22.7%) | 10 (28.6%) | 15 (23.8%) | ||
| FIGO stage | 0.077 | 0.317 | ||||
| I/II | 23 (71.9%) | 54 (72.0%) | 23 (65.7%) | 50 (79.4%) | ||
| III/IV | 9 (28.1%) | 14 (18.7%) | 10 (28.6%) | 9 (14.3%) | ||
| Recurrence | 0 (0%) | 6 (8.0%) | 2 (5.7%) | 3 (4.8 %) | ||
| Unclassified | 0 (0%) | 1 (1.3 %) | 0 (0 %) | 1 (1.6%) | ||
| Differentiation | 0.580 | 0.335 | ||||
| Grade I | 10 (31.3%) | 28 (37.3%) | 11(31.4%) | 27 (42.9%) | ||
| Grade II/III | 21 (65.6%) | 42 (56.0%) | 21 (60.0 %) | 34 (54.0%) | ||
| Unclassified | 1 (3.1 %) | 5 (6.7%) | 3 (8.6 %) | 2 (3.2%) | ||
| CA125 (U/mL) | 0.493 | 0.739 | ||||
| ≥35 | 11 (34.4%) | 27 (36.0%) | 13 (37.1 %) | 20 (31.7%) | ||
| <35 | 20 (62.5%) | 41 (54.7%) | 20 (57.1%) | 37 (58.7%) | ||
| Unclassified | 1 (3.1%) | 7 (9.3%) | 2 (5.7%) | 6 (9.5%) | ||
| Lymphovascular invasion | 0.089 | 0.129 | ||||
| Absent | 19 (59.4%) | 41 (54.7%) | 20 (57.1%) | 37 (58.7%) | ||
| Present | 13 (40.6 %) | 24 (32.0 %) | 14 (40.0%) | 17 (27.0%) | ||
| Unclassified | 0 (0%) | 10 (13.3%) | 1 (2.9%) | 9 (14.3%) | ||
| Nectin-4 expression | 0.000 * | 0.001 * | ||||
| High | 16 (50%) | 63 (84.0%) | 19 (54.3%) | 54 (85.7%) | ||
| Low | 16 (50%) | 12 (16.0%) | 16 (45.7%) | 9 (14.3%) | ||
| Groups | LVSI-Positive % | LVSI-Negative % | Total | p-Value | |
|---|---|---|---|---|---|
| MSH2_deficient | Nectin-4High | 56.3% (9/16) | 43.8% (7/16) | 16 | 0.072 |
| Nectin-4Low | 25% (4/16) | 75% (12/16) | 16 | ||
| MSH2_proficient | Nectin-4High | 40.7% (22/54) | 59.3% (32/54) | 54 | 0.158 |
| Nectin-4Low | 18.2% (2/11) | 81.8% (9/11) | 11 | ||
| MSH6_deficient | Nectin-4High | 52.6% (10/19) | 47.4% (9/19) | 19 | 0.203 |
| Nectin-4Low | 31.3% (5/16) | 68.8% (11/16) | 16 | ||
| MSH6_proficient | Nectin-4High | 35.6% (16/45) | 64.4% (29/45) | 45 | 0.149 |
| Nectin-4Low | 11.1% (1/9) | 88.9% (8/9) | 9 | ||
| Clinicopathologic Variables | MSH2 Deficient | MSH2 Proficient | ||||
|---|---|---|---|---|---|---|
| Nectin-4High | Nectin-4Low | p-Value | Nectin-4High | Nectin-4Low | p-Value | |
| n = 16 | n = 16 | n = 57 | n = 11 | |||
| FIGO stage | 0.694 | 0.158 | ||||
| I/II | 11 (68.8%) | 12 (75.0%) | 47 (82.5%) | 7 (63.6%) | ||
| III/IV | 5 (31.3%) | 4 (25.0%) | 10 (17.5%) | 4 (36.4%) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, H.K.; Park, Y.H.; Choi, J.-A.; Kim, J.W.; Kim, J.; Kim, H.S.; Lee, H.N.; Cho, H.; Chung, J.-Y.; Kim, J.-H. Nectin-4 as a Predictive Marker for Poor Prognosis of Endometrial Cancer with Mismatch Repair Impairment. Cancers 2023, 15, 2865. https://doi.org/10.3390/cancers15102865
Chang HK, Park YH, Choi J-A, Kim JW, Kim J, Kim HS, Lee HN, Cho H, Chung J-Y, Kim J-H. Nectin-4 as a Predictive Marker for Poor Prognosis of Endometrial Cancer with Mismatch Repair Impairment. Cancers. 2023; 15(10):2865. https://doi.org/10.3390/cancers15102865
Chicago/Turabian StyleChang, Ha Kyun, Young Hoon Park, Jung-A Choi, Jeong Won Kim, Jisup Kim, Hyo Sun Kim, Hae Nam Lee, Hanbyoul Cho, Joon-Yong Chung, and Jae-Hoon Kim. 2023. "Nectin-4 as a Predictive Marker for Poor Prognosis of Endometrial Cancer with Mismatch Repair Impairment" Cancers 15, no. 10: 2865. https://doi.org/10.3390/cancers15102865
APA StyleChang, H. K., Park, Y. H., Choi, J.-A., Kim, J. W., Kim, J., Kim, H. S., Lee, H. N., Cho, H., Chung, J.-Y., & Kim, J.-H. (2023). Nectin-4 as a Predictive Marker for Poor Prognosis of Endometrial Cancer with Mismatch Repair Impairment. Cancers, 15(10), 2865. https://doi.org/10.3390/cancers15102865