
Direct Intra-Patient Comparison of Scaffold Protein-Based Tracers, [99mTc]Tc-ADAPT6 and [99mTc]Tc-(HE)3-G3, for Imaging of HER2-Positive Breast Cancer
 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
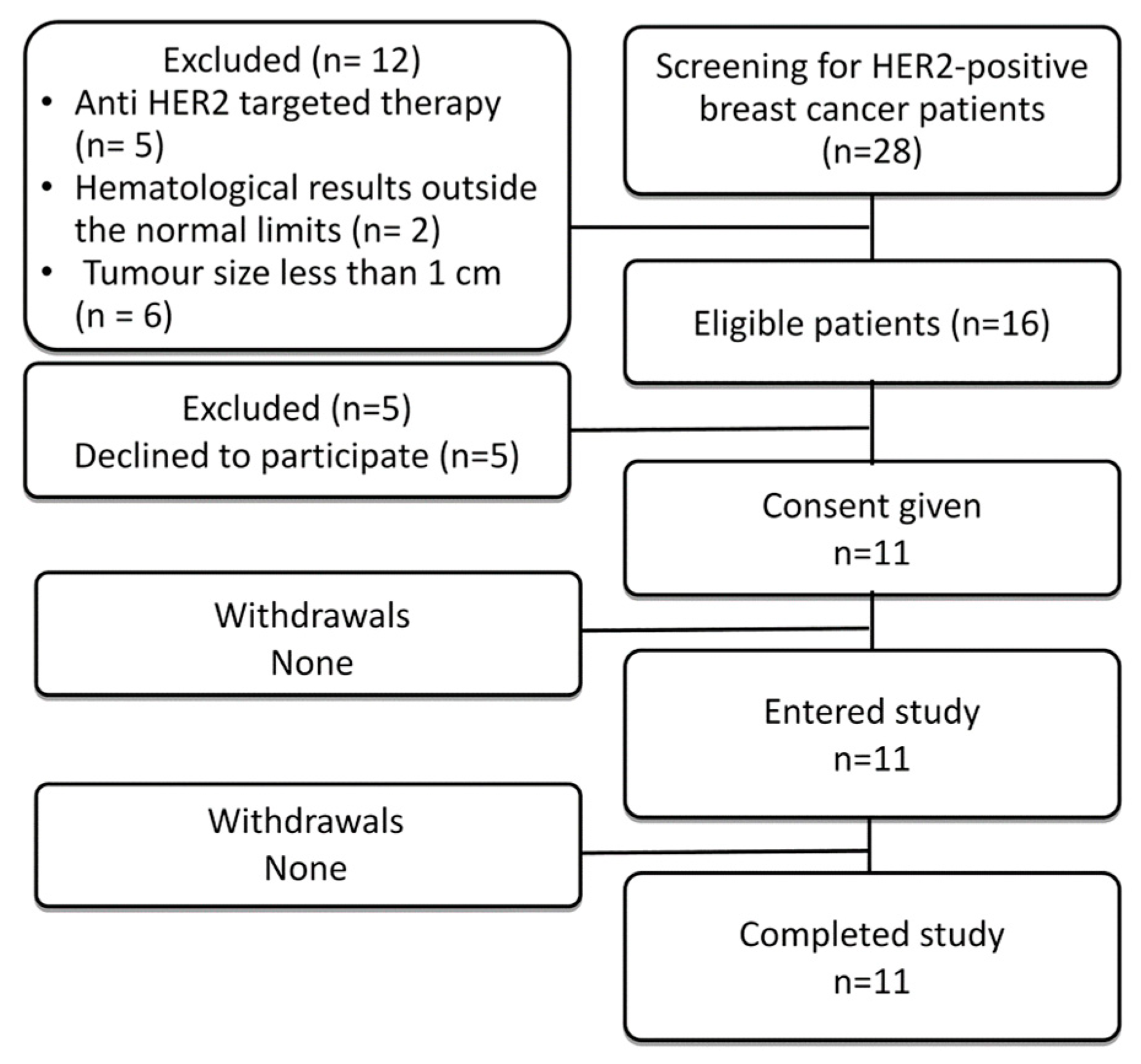
2.1. Patients
2.2. HER2 Immunohistochemistry
2.3. Radiochemistry
2.4. SPECT/CT Protocol
2.5. SPECT Image Quantification
2.6. Statistics
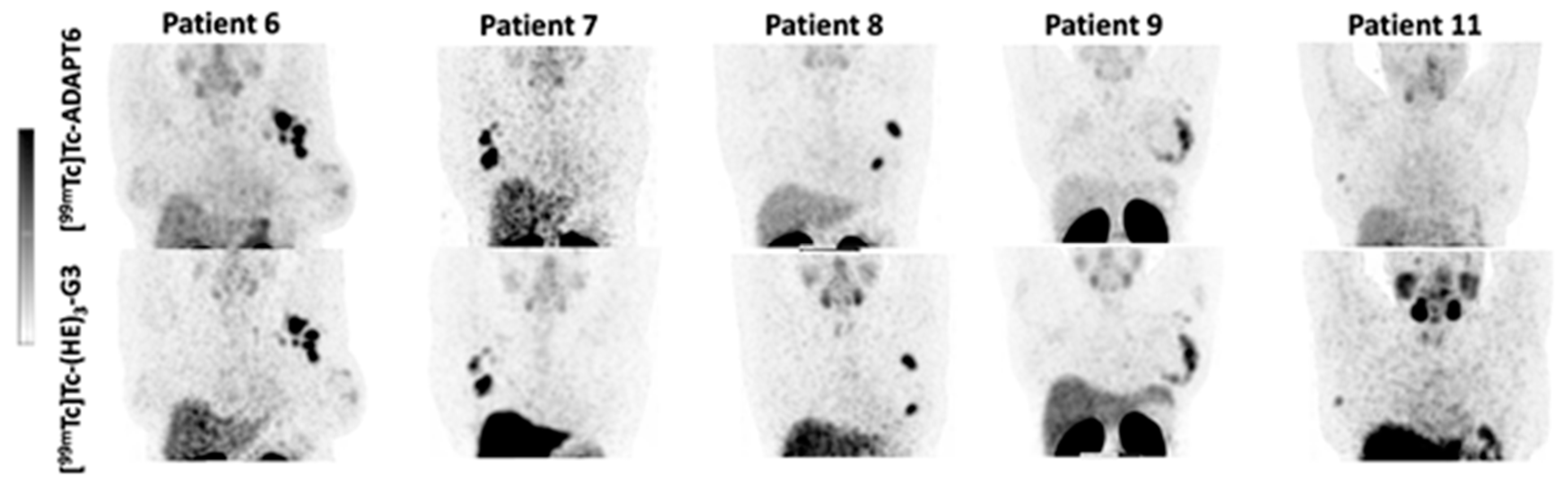
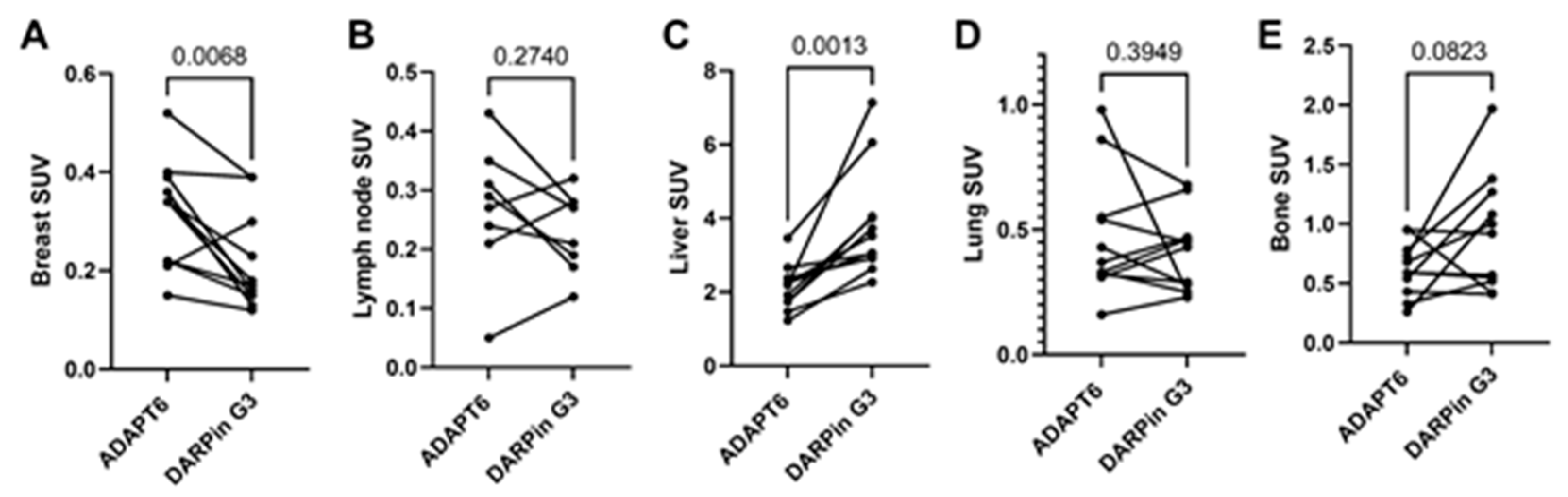
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Duffy, M.; Harbeck, N.; Nap, M.; Molina, R.; Nicolini, A.; Senkus, E.; Cardoso, F. Clinical use of biomarkers in breast cancer: Updated guidelines from the European Group on Tumor Markers (EGTM). Eur. J. Cancer 2017, 75, 284–298. [Google Scholar] [CrossRef] [Green Version]
- Pernas, S.; Tolaney, S.M. HER2-positive breast cancer: New therapeutic frontiers and overcoming resistance. Ther. Adv. Med. Oncol. 2019, 11, 1758835919833519. [Google Scholar] [CrossRef] [Green Version]
- Waks, A.G.; Winer, E.P. Breast Cancer Treatment: A Review. JAMA 2019, 321, 288–300. [Google Scholar] [CrossRef]
- Wolff, A.C.; Hammond, M.E.H.; Allison, K.H.; Harvey, B.E.; Mangu, P.B.; Bartlett, J.M.S.; Bilous, M.; Ellis, I.O.; Fitzgibbons, P.; Hanna, W.; et al. Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Focused Update. J. Clin. Oncol. 2018, 36, 2105–2122. [Google Scholar] [CrossRef] [Green Version]
- Lower, E.E.; Khan, S.; Kennedy, D.; Baughman, R.P. Discordance of the estrogen receptor and HER-2/neu in breast cancer from primary lesion to first and second metastatic site. Breast Cancer 2017, 9, 515–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turner, N.H.; Di Leo, A. HER2 discordance between primary and metastatic breast cancer: Assessing the clinical impact Cancer. Treat Rev. 2013, 39, 947–957. [Google Scholar] [CrossRef] [PubMed]
- Tolmachev, V.; Orlova, A.; Sörensen, J. The emerging role of radionuclide molecular imaging of HER2 expression in breast cancer. Semin. Cancer Biol. 2021, 72, 185–197. [Google Scholar] [CrossRef]
- Henry, K.E.; Ulaner, G.A.; Lewis, J.S. Human Epidermal Growth Factor Receptor 2-Targeted PET/Single- Photon Emission Computed Tomography Imaging of Breast Cancer: Noninvasive Measurement of a Biomarker Integral to Tumor Treatment and Prognosis. PET Clin. 2017, 12, 269–288. [Google Scholar] [CrossRef] [Green Version]
- Bragina, O.; von Witting, E.; Garousi, J.; Zelchan, R.; Sandström, M.; Orlova, A.; Medvedeva, A.; Doroshenko, A.; Vorobyeva, A.; Lindbo, S.; et al. Phase I study of 99mTc-ADAPT6, a scaffold protein-based probe for visualization of HER2 expression in breast cancer. J. Nucl. Med. 2021, 62, 493–499. [Google Scholar] [CrossRef] [PubMed]
- Bragina, O.; Chernov, V.; Schulga, A.; Konovalova, E.; Garbukov, E.; Vorobyeva, A.; Orlova, A.; Tashireva, L.; Sörensen, J.; Zelchan, R.; et al. Phase I Trial of 99mTc-(HE)3-G3, a DARPin-Based Probe for Imaging of HER2 Expression in Breast Cancer. J. Nucl. Med. 2022, 63, 528–535. [Google Scholar] [CrossRef]
- Gebauer, M.; Skerra, A. Engineered Protein Scaffolds as Next-Generation Therapeutics. Annu. Rev. Pharmacol. Toxicol. 2020, 60, 391–415. [Google Scholar] [CrossRef] [PubMed]
- Zahnd, C.; Kawe, M.; Stumpp, M.T.; de Pasquale, C.; Tamaskovic, R.; Nagy-Davidescu, G.; Dreier, B.; Schibli, R.; Binz, H.K.; Waibel, R.; et al. Efficient tumor targeting with high-affinity designed ankyrin repeat proteins: Effects of affinity and molecular size. Cancer Res. 2010, 70, 1595–1605. [Google Scholar] [CrossRef] [Green Version]
- Goldstein, R.; Sosabowski, J.; Livanos, M.; Leyton, J.; Vigor, K.; Bhavsar, G.; Nagy-Davidescu, G.; Rashid, M.; Miranda, E.; Yeung, J.; et al. Development of the designed ankyrin repeat protein (DARPin) G3 for HER2 molecular imaging. Eur. J. Nucl. Med. 2015, 42, 288–301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vorobyeva, A.; Schulga, A.; Konovalova, E.; Güler, R.; Löfblom, J.; Sandström, M.; Garousi, J.; Chernov, V.; Bragina, O.; Orlova, A.; et al. Optimal composition and position of histidine-containing tags improves biodistribution of 99mTc-labeled DARPin G3. Sci. Rep. 2019, 9, 9405. [Google Scholar] [CrossRef] [Green Version]
- Nilvebrant, J.; Estrand, M.; Georgieva-Kotseva, M.; Björnmalm, M.; Löfblom, J.; Hober, S. Engineering of bispecific affinity proteins with high affinity for ERBB2 and adaptable binding to albumin. PLoS ONE 2014, 9, e103094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garousi, J.; Lindbo, S.; Nilvebrant, J.; Åstrand, M.; Buijs, J.; Sandström, M.; Honarvar, H.; Orlova, A.; Tolmachev, V.; Hober, S. ADAPT, a Novel Scaffold Protein-Based Probe for Radionuclide Imaging of Molecular Targets That Are Expressed in Disseminated Cancers. Cancer Res. 2015, 75, 4364–4371. [Google Scholar] [CrossRef] [Green Version]
- Lindbo, S.; Garousi, J.; Åstrand, M.; Honarvar, H.; Orlova, A.; Hober, S.; Tolmachev, V. Influence of Histidine-Containing Tags on the Biodistribution of ADAPT Scaffold Proteins. Bioconjug. Chem. 2016, 27, 716–726. [Google Scholar] [CrossRef]
- Garousi, J.; Orlova, A.; Frejd, F.Y.; Tolmachev, V. Imaging using radiolabelled targeted proteins: Radioimmunodetection and beyond. EJNMMI Radiopharm. Chem. 2020, 5, 1–26. [Google Scholar] [CrossRef]
- Tolmachev, V.; Chernov, V.; Deyev, S. Targeted nuclear medicine. Seek and destroy. Rus. Chem. Rev. 2022, 91, RCR5034. [Google Scholar] [CrossRef]
- Tolmachev, V.; Bodenko, V.; Oroujeni, M.; Deyev, S.; Konovalova, E.; Schulga, A.; Lindbo, S.; Hober, S.; Bragina, O.; Orlova, A.; et al. Direct In Vivo Comparison of 99mTc-Labeled Scaffold Proteins, DARPin G3 and ADAPT6, for Visualization of HER2 Expression and Monitoring of Early Response for Trastuzumab Therapy. Int. J. Mol. Sci. 2022, 23, 15181. [Google Scholar] [CrossRef]
- Bailey, D.L.; Willowson, K.P. Quantitative SPECT/CT: SPECT joins PET as a quantitative imaging modality. Eur. J. Nucl. Med. Mol. Imaging 2014, 41 (Suppl. S1), 17–25. [Google Scholar] [CrossRef]
- Gnesin, S.; Ferreira, P.L.; Malterre, J.; Laub, P.; Prior, J.; Verdun, F.R. Phantom Validation of Tc-99m Absolute Quantification in a SPECT/CT Commercial Device. Comput. Math. Methods Med. 2016, 2016, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Press, D.J.; Miller, M.E.; Liederbach, E.; Yao, K.; Huo, D. De novo metastasis in breast cancer: Occurrence and overall survival stratified by molecular subtype. Clin. Exp. Metastasis 2017, 34, 457–465. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Liu, C.; Xing, Y.; He, J.; O’Doherty, J.; Huang, W.; Zhao, J. Development of a 99mTc-Labeled Single-Domain Antibody for SPECT/CT Assessment of HER2 Expression in Breast Cancer. Mol. Pharm. 2021, 18, 3616–3622. [Google Scholar] [CrossRef]
- Altunay, B.; Goedicke, A.; Winz, O.H.; Hertel, F.; von Mallek, D.; Meszaros, L.K.; Chand, G.; Biersack, H.-J.; Stickeler, E.; Krauss, K.; et al. 99mTc-labeled single-domain antibody for SPECT/CT assessment of HER2 expression in diverse cancer types. Eur. J. Nucl. Med. 2022, 50, 1005–1013. [Google Scholar] [CrossRef]
- Sandström, M.; Lindskog, K.; Velikyan, I.; Wennborg, A.; Feldwisch, J.; Sandberg, D.; Tolmachev, V.; Orlova, A.; Sörensen, J.; Carlsson, J.; et al. Biodistribution and Radiation Dosimetry of the Anti-HER2 Affibody Molecule 68Ga-ABY-025 in Breast Cancer Patients. J. Nucl. Med. 2016, 57, 867–871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’huyvetter, M.; De Vos, J.; Caveliers, V.; Vaneycken, I.; Heemskerk, J.; Duhoux, F.P.; Fontaine, C.; Vanhoeij, M.; Windhorst, A.D.; van der Aa, F.; et al. Phase I Trial of 131I-GMIB-Anti-HER2-VHH1, a New Promising Candidate for HER2-Targeted Radionuclide Therapy in Breast Cancer Patients. J. Nucl. Med. 2021, 62, 1097–1105. [Google Scholar] [CrossRef]
- Sörensen, J.; Sandberg, D.; Sandström, M.; Wennborg, A.; Feldwisch, J.; Tolmachev, V.; Åström, G.; Lubberink, M.; Garske-Román, U.; Carlsson, J.; et al. First-in-human molecular imaging of HER2 expression in breast cancer metastases using the 111In-ABY-025 affibody molecule. J. Nucl. Med. 2014, 55, 730–735. [Google Scholar] [CrossRef] [Green Version]
- Sörensen, J.; Velikyan, I.; Sandberg, D.; Wennborg, A.; Feldwisch, J.; Tolmachev, V.; Orlova, A.; Sandström, M.; Lubberink, M.; Olofsson, H.; et al. Measuring HER2-Receptor Expression In Metastatic Breast Cancer Using [68Ga]ABY-025 Affibody PET/CT. Theranostics 2016, 6, 262–271. [Google Scholar] [CrossRef]
- Keyaerts, M.; Xavier, C.; Heemskerk, J.; Devoogdt, N.; Everaert, H.; Ackaert, C.; Vanhoeij, M.; Duhoux, F.P.; Gevaert, T.; Simon, P.; et al. Phase I Study of 68Ga-HER2-Nanobody for PET/CT Assessment of HER2 Expression in Breast Carcinoma. J. Nucl. Med. 2016, 57, 27–33. [Google Scholar] [CrossRef] [Green Version]
- Qin, X.; Guo, X.; Liu, T.; Li, L.; Zhou, N.; Ma, X.; Meng, X.; Liu, J.; Zhu, H.; Jia, B.; et al. High in-vivo stability in preclinical and first-in-human experiments with [18F]AlF-RESCA-MIRC213: A 18F-labeled nanobody as PET radiotracer for diagnosis of HER2-positive cancers. Eur. J. Nucl. Med. Mol. Imaging 2023, 50, 302–313. [Google Scholar] [CrossRef] [PubMed]
- Jost, C.; Schilling, J.; Tamaskovic, R.; Schwill, M.; Honegger, A.; Plückthun, A. Structural basis for eliciting a cytotoxic effect in HER2-overexpressing cancer cells via binding to the extracellular domain of HER2. Structure 2013, 21, 1979–1991. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tolmachev, V.; Bodenko, V.; Orlova, A.; Schulga, A.; Deyev, S.M.; Vorobyeva, A. Visualization of epithelial cell adhesion molecule-expressing renal cell carcinoma xenografts using designed ankyrin repeat protein Ec1 labelled with 99mTc and 125I. Oncol. Lett. 2022, 25, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Oroujeni, M.; Bezverkhniaia, E.A.; Xu, T.; Liu, Y.; Plotnikov, E.V.; Karlberg, I.; Ryer, E.; Orlova, A.; Tolmachev, V.; Frejd, F.Y. Evaluation of an Affibody-Based Binder for Imaging of Immune Check-Point Molecule B7-H3. Pharmaceutics 2022, 14, 1780. [Google Scholar] [CrossRef]
- Liang, Z.; Hu, X.; Hu, H.; Wang, P.; Cai, J. Novel small 99mTc-labeled affibody molecular probe for PD-L1 receptor imaging. Front Oncol. 2022, 12, 1017737. [Google Scholar] [CrossRef] [PubMed]
- Morath, V.; Brandt, C.; Deuschle, F.-C.; Mendler, C.T.; Blechert, B.; Summer, D.; Barinka, C.; Decristoforo, C.; Weber, W.A.; Schwaiger, M.; et al. Molecular Design of 68Ga- and 89Zr-Labeled Anticalin Radioligands for PET-Imaging of PSMA-Positive Tumors. Mol. Pharm. 2023, 20, 2490–2501. [Google Scholar] [CrossRef]
- Liu, Y.; Yu, S.; Xu, T.; Bodenko, V.; Orlova, A.; Oroujeni, M.; Rinne, S.S.; Tolmachev, V.; Vorobyeva, A.; Gräslund, T. Preclinical Evaluation of a New Format of 68Ga- and 111In-Labeled Affibody Molecule ZIGF-1R:4551 for the Visualization of IGF-1R Expression in Malignant Tumors Using PET and SPECT. Pharmaceutics 2022, 14, 1475. [Google Scholar] [CrossRef]
- Fay, R.; Törő, I.; Schinke, A.-L.; Simic, B.; Schaefer, J.V.; Dreier, B.; Plückthun, A.; Holland, J.P. Sortase-Mediated Site-Specific Conjugation and 89Zr-Radiolabeling of Designed Ankyrin Repeat Proteins for PET. Mol. Pharm. 2022, 19, 3576–3585. [Google Scholar] [CrossRef]
- Sandberg, D.; Tolmachev, V.; Velikyan, I.; Olofsson, H.; Wennborg, A.; Feldwisch, J.; Carlsson, J.; Lindman, H.; Sörensen, J. Intra-image referencing for simplified assessment of HER2-expression in breast cancer metastases using the Affibody molecule ABY-025 with PET and SPECT. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1337–1346. [Google Scholar] [CrossRef] [Green Version]
- Miao, H.; Sun, Y.; Jin, Y.; Hu, X.; Song, S.; Zhang, J. Application of a Novel 68Ga-HER2 Affibody PET/CT Imaging in Breast Cancer Patients. Front. Oncol. 2022, 12, 894767. [Google Scholar] [CrossRef]
- Alhuseinalkhudhur, A.; Lindman, H.; Liss, P.; Sundin, T.; Frejd, F.Y.; Hartman, J.; Iyer, V.; Feldwisch, J.; Lubberink, M.; Rönnlund, C.; et al. HER2-targeting [68Ga]Ga-ABY-025 PET predicts early metabolic response in breast cancer patients—Results from a Phase II study. J. Nucl. Med. 2023; in press. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (y) | HER2 Status in Primary Tumour (IHC a) | Primary Tumour Status (ER/PgR/Ki67) | Primary Tumour Size (mm) | LN Size (mm) | Clinical Stage Before Imaging | |
|---|---|---|---|---|---|---|
| 1 | 61 | 3+ (ICH) | ER+; PgR+; Ki67 40% | 20 | 24 | IV (T4N3M1) |
| 2 | 48 | 3+ (ICH) | ER+; PgR+; Ki67 18% | 37 | 23 | IIB (T2N1M0) |
| 3 | 26 | 3+ (ICH) | ER+; PgR+; Ki67 45% | 49 | 20 | IIB (T2N1M0) |
| 4 | 49 | 3+ (ICH) | ER+; PgR+; Ki67 20% | 15 | none | I (T1N0M0) |
| 5 | 41 | 3+ (ICH) | ER+; PgR+; Ki67 45% | 20 | 24 | IV (T1N1M1) |
| 6 | 65 | 3+ (ICH) | ER+; PgR+; Ki67 60% | 21 | 37 | IIB (T2N1M0) |
| 7 | 59 | 3+ (ICH) | ER−; PgR−; Ki67 55% | 13 | 16 | IIA (T1N1M0) |
| 8 | 55 | 3+ (ICH) | ER−; PgR−; Ki67 18% | 28 | 30 | IIB (T2N1M0) |
| 9 | 38 | 3+ (ICH) | ER+; PgR+; Ki67 25% | 38 | 12 | IIB (T2N1M0) |
| 10 | 65 | 3+ (ICH) | ER−; PgR−; Ki67 18% | 17 | none | I (T1N0M0) |
| 11 | 63 | 3+ (ICH) | ER+; PgR+; Ki67 10% | 20 | none | I (T1N0M0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bragina, O.; Chernov, V.; Schulga, A.; Konovalova, E.; Hober, S.; Deyev, S.; Sörensen, J.; Tolmachev, V. Direct Intra-Patient Comparison of Scaffold Protein-Based Tracers, [99mTc]Tc-ADAPT6 and [99mTc]Tc-(HE)3-G3, for Imaging of HER2-Positive Breast Cancer. Cancers 2023, 15, 3149. https://doi.org/10.3390/cancers15123149
Bragina O, Chernov V, Schulga A, Konovalova E, Hober S, Deyev S, Sörensen J, Tolmachev V. Direct Intra-Patient Comparison of Scaffold Protein-Based Tracers, [99mTc]Tc-ADAPT6 and [99mTc]Tc-(HE)3-G3, for Imaging of HER2-Positive Breast Cancer. Cancers. 2023; 15(12):3149. https://doi.org/10.3390/cancers15123149
Chicago/Turabian StyleBragina, Olga, Vladimir Chernov, Alexey Schulga, Elena Konovalova, Sophia Hober, Sergey Deyev, Jens Sörensen, and Vladimir Tolmachev. 2023. "Direct Intra-Patient Comparison of Scaffold Protein-Based Tracers, [99mTc]Tc-ADAPT6 and [99mTc]Tc-(HE)3-G3, for Imaging of HER2-Positive Breast Cancer" Cancers 15, no. 12: 3149. https://doi.org/10.3390/cancers15123149