
Radioisotope-Guided Excision of Mediastinal Lymph Nodes in Patients with Non-Small Cell Lung Carcinoma: Feasibility and Clinical Impact
by
 , , , ,
, , , ,
Cristiano Pini
1,2,‡,
Edoardo Bottoni
3,
Francesco Fiz
4,5,*,
Veronica Maria Giudici
1,3,
Marco Alloisio
3,
Alberto Testori
3, 
Marcello Rodari
2,
Martina Sollini
1,2,
Arturo Chiti
1,§,
Umberto Cariboni
3,† and
Lidija Antunovic
2,†,‖ 1
Department of Biomedical Sciences, Humanitas University, Via Rita Levi Montalcini 4, Pieve Emanuele, 20072 Milan, Italy
2
Diagnostic Imaging Department, IRCCS Humanitas Research Hospital, Rozzano, 20089 Milan, Italy
3
Division of Thoracic Surgery, IRCCS Humanitas Research Hospital, Via Manzoni 56, 20089 Rozzano, Italy
4
Nuclear Medicine Unit, Department of Diagnostic Imaging, Ente Ospedaliero “Ospedali Galliera”, 16128 Genoa, Italy
5
Department of Nuclear Medicine and Clinical Molecular Imaging, University Hospital Tübingen, 72076 Tübingen, Germany
*
Author to whom correspondence should be addressed.
†
These authors contributed equally to this work.
‡
Current address: School of Medicine and Surgery, University of Milano-Bicocca, 20900 Monza, Italy.
§
Current address: Faculty of Medicine, Università Vita-Salute San Raffaele, 20132 Milan, Italy.
‖
Current address: Department of Nuclear Medicine, IRCCS San Raffaele, 20132 Milan, Italy.
Cancers 2023, 15(13), 3320; https://doi.org/10.3390/cancers15133320
Submission received: 21 May 2023
/
Revised: 19 June 2023
/
Accepted: 21 June 2023
/
Published: 24 June 2023
(This article belongs to the Special Issue PET/CT and Conventional Imaging in Cancers)
Simple Summary
We tried to use a small amount of radioactivity, injected around non-small cell lung cancers, to see if this technique can identify the lymph node receiving the flow (and thus potentially the metastases) from the tumour. Our results show that it is possible to do so; this technique could be used to obtain a personalised and potentially safer approach in lung cancer surgery.
Abstract
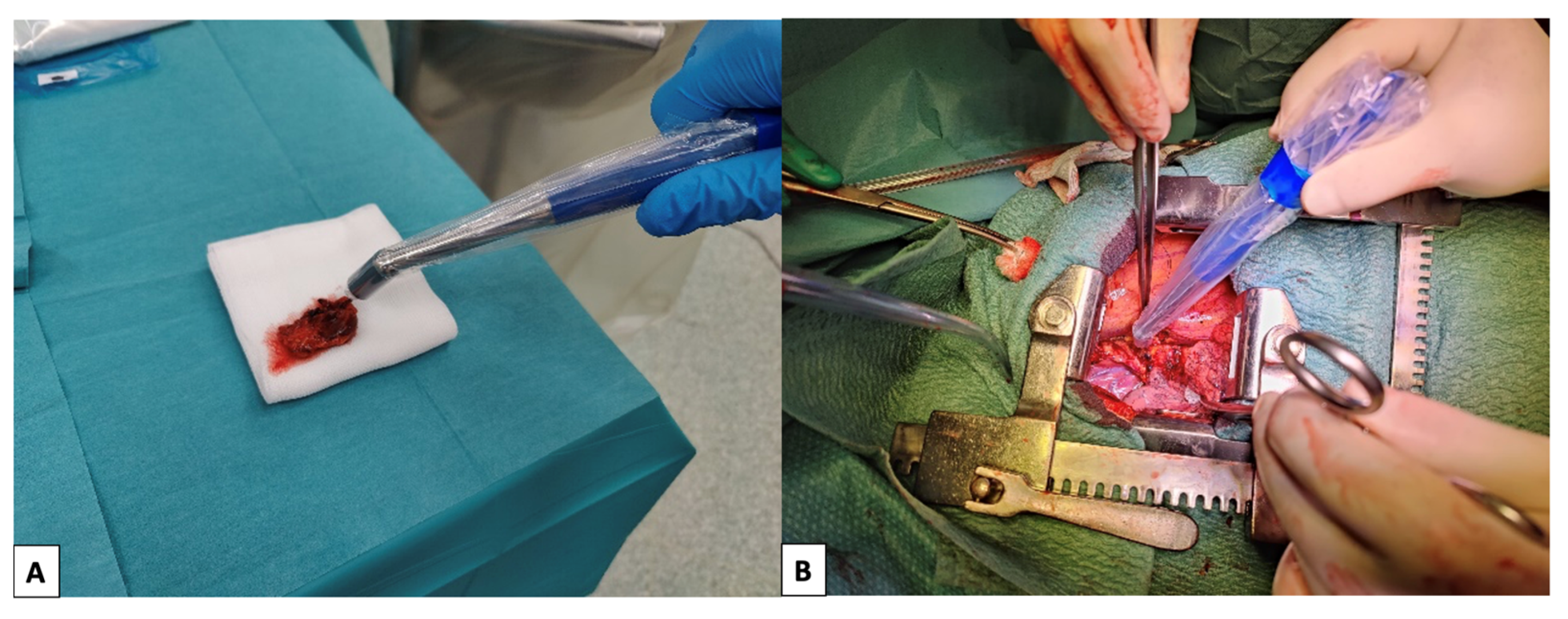
Background: Intraoperative localisation of nodal disease in non-small cell lung cancer (NSCLC) can be challenging. Lymph node localisation via radiopharmaceuticals is used in many conditions; we tested the feasibility of this approach in NSCLC. Methods: NSCLC patients were prospectively recruited. Intraoperative peri-tumoral injections of [99mTc]Tc-albumin nanocolloids were performed, followed by removing the tumour and locoregional lymph nodes. These were examined ex vivo with a gamma probe and labelled sentinel lymph nodes (SLNs) if they showed any activity or non-sentinel lymph nodes (nSLNs) if they did not. Thereafter, the surgical field was scanned with the probe; any further radioactive lymph node was removed and labelled as “extra” SLNs (eSLNs). All specimens were sent to histology, and metastatic status was recorded. Results: 48 patients were enrolled, and 290 nodal stations were identified: 179 SLNs, 87 nSLNs, and 24 eSLNs. A total of 44 nodal metastases were identified in 22 patients, with 36 of them (82%) located within SLNs. Patients with nSLNs metastases had at least a co-existing positive SLN. No metastases were found in eSLNs. Conclusions: The technique shows high sensitivity for intraoperative nodal metastases identification. This information could allow selective lymphadenectomies in low-risk patients or more aggressive approaches in high-risk patients.

{kind=link}
{kind=link}