

Development and External Validation of Partial Proportional Odds Risk Prediction Models for Cancer Stage at Diagnosis among Males and Females in Canada

 , , , , and
, , , , and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
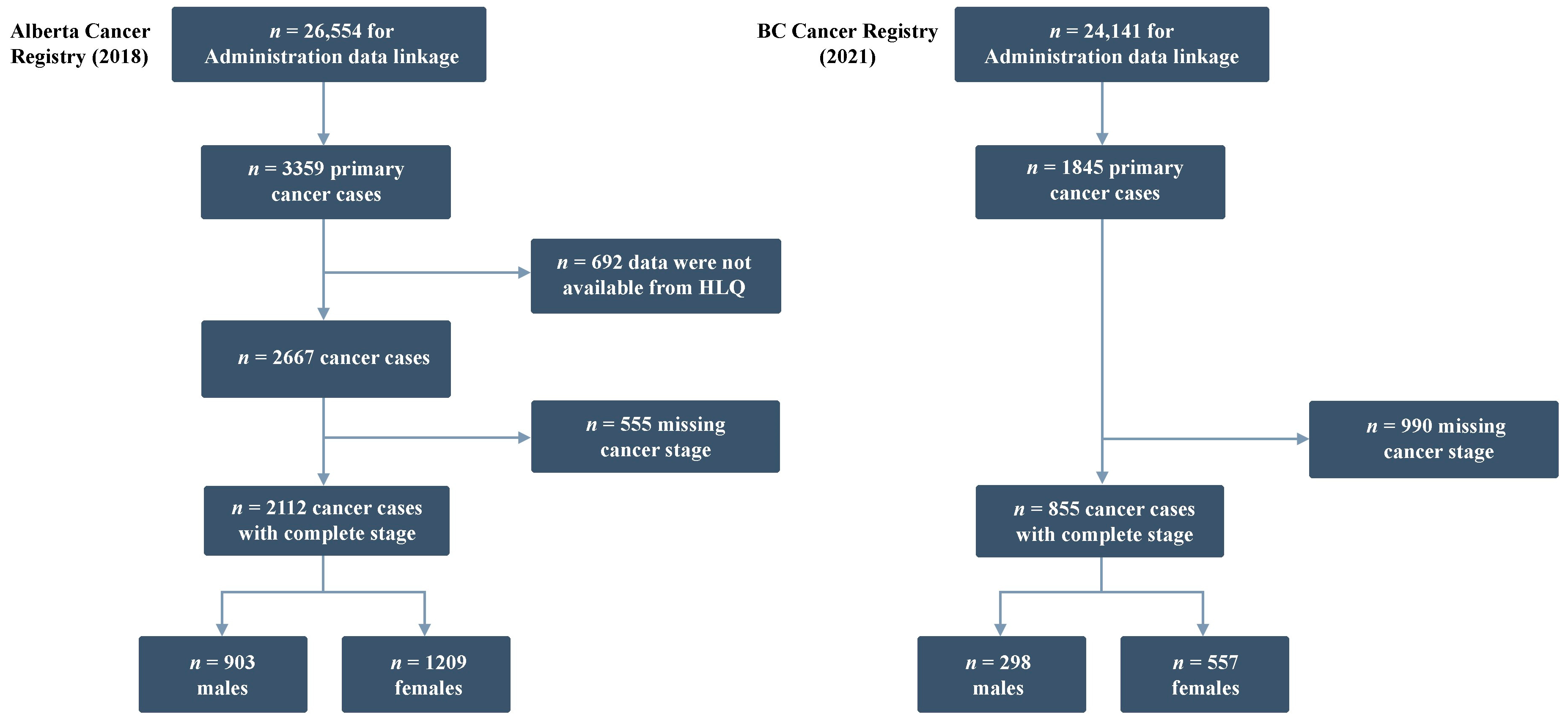
2.1. Data Sources
2.2. Outcome
2.3. Predictors
2.4. Model Development
2.5. Model Performance and External Validation
3. Results
3.1. Model Development
3.1.1. ATP Cohort Characteristics
3.1.2. Predictors of Cancer Stage at Diagnosis in the ATP Cohort
3.2. External Validation
3.2.1. BCGP Cohort Characteristics
3.2.2. Model Performance in the BCGP Cohort
4. Discussion
4.1. Strengths
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics 2021; Canadian Cancer Society: Toronto, ON, Canada, 2021. [Google Scholar]
- Cancer Care Alberta. The 2021 Report on Cancer Statistics in Alberta-ROCSIA 2021-Top 10 Most Common Cancers Incidence and Mortality. Available online: https://public.tableau.com/app/profile/cancercontrol.ab/viz/The2021ReportonCancerStatisticsinAlberta/Highlights (accessed on 21 August 2021).
- Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics 2018; Canadian Cancer Society: Toronto, ON, Canada, 2018. [Google Scholar]
- Canadian Partnership against Cancer. Eight Priorities for Canada’s Cancer System. Available online: https://www.partnershipagainstcancer.ca/cancer-strategy/strategic-priorities/ (accessed on 22 November 2022).
- World Health Organization. Guide to Cancer Early Diagnosis. Available online: https://www.who.int/publications/i/item/9789241511940 (accessed on 22 November 2022).
- Chaput, G.; Giudice, E.D.; Kucharski, E. Cancer screening in Canada. Can. Fam. Physician 2021, 67, 27–29. [Google Scholar] [CrossRef]
- Aktary, M.L.; Ghebrial, M.; Wang, Q.; Shack, L.; Robson, P.J.; Kopciuk, K.A. Health-Related and Behavioral Factors Associated With Lung Cancer Stage at Diagnosis: Observations From Alberta’s Tomorrow Project. Cancer Control 2022, 29, 10732748221091678. [Google Scholar] [CrossRef]
- Ghebrial, M.; Aktary, M.L.; Wang, Q.; Spinelli, J.J.; Shack, L.; Robson, P.J.; Kopciuk, K.A. Predictors of CRC Stage at Diagnosis among Male and Female Adults Participating in a Prospective Cohort Study: Findings from Alberta’s Tomorrow Project. Curr. Oncol. 2021, 28, 4938–4952. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Aktary, M.L.; Spinelli, J.J.; Shack, L.; Robson, P.J.; Kopciuk, K.A. Pre-diagnosis lifestyle, health history and psychosocial factors associated with stage at breast cancer diagnosis—Potential targets to shift stage earlier. Cancer Epidemiol. 2022, 78, 102152. [Google Scholar] [CrossRef] [PubMed]
- Slatore, C.G.; Gould, M.K.; Au, D.H.; Deffebach, M.E.; White, E. Lung cancer stage at diagnosis: Individual associations in the prospective VITamins and lifestyle (VITAL) cohort. BMC Cancer 2011, 11, 228. [Google Scholar] [CrossRef] [Green Version]
- Blair, A.; Datta, G.D. Associations between area-level deprivation, rural residence, physician density, screening policy and late-stage colorectal cancer in Canada. Cancer Epidemiol. 2020, 64, 101654. [Google Scholar] [CrossRef] [PubMed]
- Andrew, A.S.; Parker, S.; Anderson, J.C.; Rees, J.R.; Robinson, C.; Riddle, B.; Butterly, L.F. Risk Factors for Diagnosis of Colorectal Cancer at a Late Stage: A Population-Based Study. J. Gen. Intern. Med. 2018, 33, 2100–2105. [Google Scholar] [CrossRef] [Green Version]
- Moore, K.J.; Sussman, D.A.; Koru-Sengul, T. Age-Specific Risk Factors for Advanced Stage Colorectal Cancer, 1981–2013. Prev. Chronic Dis. 2018, 15, E106. [Google Scholar] [CrossRef] [Green Version]
- Patel, A.; Gantz, O.; Zagadailov, P.; Merchant, A.M. The role of socioeconomic disparity in colorectal cancer stage at presentation. Updates Surg. 2019, 71, 523–531. [Google Scholar] [CrossRef]
- White, A.; Ironmonger, L.; Steele, R.J.C.; Ormiston-Smith, N.; Crawford, C.; Seims, A. A review of sex-related differences in colorectal cancer incidence, screening uptake, routes to diagnosis, cancer stage and survival in the UK. BMC Cancer 2018, 18, 906. [Google Scholar] [CrossRef] [Green Version]
- Perdue, D.G.; Haverkamp, D.; Perkins, C.; Daley, C.M.; Provost, E. Geographic variation in colorectal cancer incidence and mortality, age of onset, and stage at diagnosis among American Indian and Alaska Native people, 1990–2009. Am. J. Public Health 2014, 104, S404–S414. [Google Scholar] [CrossRef]
- Van Calster, B.; McLernon, D.J.; van Smeden, M.; Wynants, L.; Steyerberg, E.W. Calibration: The Achilles heel of predictive analytics. BMC Med. 2019, 17, 230. [Google Scholar] [CrossRef] [Green Version]
- Chen, Q.; Cherry, D.R.; Nalawade, V.; Qiao, E.M.; Kumar, A.; Lowy, A.M.; Simpson, D.R.; Murphy, J.D. Clinical Data Prediction Model to Identify Patients With Early-Stage Pancreatic Cancer. JCO Clin. Cancer Inform. 2021, 5, 279–287. [Google Scholar] [CrossRef]
- He, B.; Chen, W.; Liu, L.; Hou, Z.; Zhu, H.; Cheng, H.; Zhang, Y.; Zhan, S.; Wang, S. Prediction Models for Prognosis of Cervical Cancer: Systematic Review and Critical Appraisal. Front. Public Health 2021, 9, 654454. [Google Scholar] [CrossRef]
- Usher-Smith, J.A.; Walter, F.M.; Emery, J.D.; Win, A.K.; Griffin, S.J. Risk Prediction Models for Colorectal Cancer: A Systematic Review. Cancer Prev. Res. 2016, 9, 13–26. [Google Scholar] [CrossRef] [Green Version]
- Usher-Smith, J.A.; Sharp, S.J.; Luben, R.; Griffin, S.J. Development and Validation of Lifestyle-Based Models to Predict Incidence of the Most Common Potentially Preventable Cancers. Cancer Epidemiol. Biomark. Prev. 2019, 28, 67–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jarbol, D.E.; Hyldig, N.; Moller, S.; Wehberg, S.; Rasmussen, S.; Balasubramaniam, K.; Haastrup, P.F.; Sondergaard, J.; Rubin, K.H. Can National Registries Contribute to Predict the Risk of Cancer? The Cancer Risk Assessment Model (CRAM). Cancers 2022, 14, 3823. [Google Scholar] [CrossRef]
- Van Calster, B.; Valentin, L.; Van Holsbeke, C.; Testa, A.C.; Bourne, T.; Van Huffel, S.; Timmerman, D. Polytomous diagnosis of ovarian tumors as benign, borderline, primary invasive or metastatic- development and validation of standard and kernel-based risk prediction models. BMC Med. Res. Methodol. 2010, 10, 1–12. [Google Scholar] [CrossRef]
- Van Calster, B.; Van Hoorde, K.; Valentin, L.; Testa, A.C.; Fischerova, D.; Van Holsbeke, C.; Savelli, L.; Franchi, D.; Epstein, E.; Kaijser, J.; et al. Evaluating the risk of ovarian cancer before surgery using the ADNEX model to differentiate between benign, borderline, early and advanced stage invasive, and secondary metastatic tumours: Prospective multicentre diagnostic study. BMJ 2014, 349, g5920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, P.; Wang, J.J.; Duan, W.; Song, C.; Yang, Y.; Wu, Q.Q. Estimating the risk of malignancy of adnexal masses: Validation of the ADNEX model in the hands of nonexpert ultrasonographers in a gynaecological oncology centre in China. J. Ovarian Res. 2021, 14, 169. [Google Scholar] [CrossRef] [PubMed]
- Sayasneh, A.; Ferrara, L.; De Cock, B.; Saso, S.; Al-Memar, M.; Johnson, S.; Kaijser, J.; Carvalho, J.; Husicka, R.; Smith, A.; et al. Evaluating the risk of ovarian cancer before surgery using the ADNEX model: A multicentre external validation study. Br. J. Cancer 2016, 115, 542–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yue, X.; Zhong, L.; Wang, Y.; Zhang, C.; Chen, X.; Wang, S.; Hu, J.; Hu, J.; Wang, C.; Liu, X. Value of Assessment of Different Neoplasias in the Adnexa in the Differential Diagnosis of Malignant Ovarian Tumor and Benign Ovarian Tumor: A Meta-analysis. Ultrasound Med. Biol. 2022, 48, 730–742. [Google Scholar] [CrossRef] [PubMed]
- Tug, N.; Yassa, M.; Sargın, M.A.; Taymur, B.D.; Sandal, K.; Meg, E. Preoperative discriminating performance of the IOTA-ADNEX model and comparison with Risk of Malignancy Index: An external validation in a non-gynecologic oncology tertiary center. Eur. J. Gynaecol. Oncol. 2020, 41, 200–207. [Google Scholar] [CrossRef] [Green Version]
- Danaei, G.; Vander Hoorn, S.; Lopez, A.D.; Murray, C.J.; Ezzati, M.; The Comparative Risk Assessment Collaborating Group (Cancers). Causes of cancer in the world: Comparative risk assessment of nine behavioural and environmental risk factors. Lancet 2005, 366, 1784–1793. [Google Scholar] [CrossRef] [Green Version]
- Green, T.; Atkin, K.; Macleod, U. Cancer detection in primary care: Insights from general practitioners. Br. J. Cancer 2015, 112 (Suppl. S1), S41–S49. [Google Scholar] [CrossRef]
- Canadian Partnership for Tomorrow’s Health. Partnering across Canada. Available online: https://canpath.ca/ (accessed on 11 November 2022).
- Robson, P.J.; Solbak, N.M.; Haig, T.R.; Whelan, H.K.; Vena, J.E.; Akawung, A.K.; Rosner, W.K.; Brenner, D.R.; Cook, L.S.; Csizmadi, I.; et al. Design, methods and demographics from phase I of Alberta’s Tomorrow Project cohort: A prospective cohort profile. CMAJ Open 2016, 4, E515–E527. [Google Scholar] [CrossRef] [Green Version]
- Ye, M.; Robson, P.J.; Eurich, D.T.; Vena, J.E.; Xu, J.Y.; Johnson, J.A. Cohort Profile: Alberta’s Tomorrow Project. Int. J. Epidemiol. 2017, 46, 1097–1098l. [Google Scholar] [CrossRef] [Green Version]
- Alberta’s Tomorrow Project. Survey Questions Asked. Available online: https://myatpresearch.ca/survey-questions/ (accessed on 12 May 2021).
- Csizmadi, I.; Kahle, L.; Ullman, R.; Dawe, U.; Zimmerman, T.P.; Friedenreich, C.M.; Bryant, H.; Subar, A.F. Adaptation and evaluation of the National Cancer Institute’s Diet History Questionnaire and nutrient database for Canadian populations. Public Health Nutr. 2007, 10, 88–96. [Google Scholar] [CrossRef] [Green Version]
- Friedenreich, C.M.; Courneya, K.S.; Neilson, H.K.; Matthews, C.E.; Willis, G.; Irwin, M.; Troiano, R.; Ballard-Barbash, R. Reliability and validity of the Past Year Total Physical Activity Questionnaire. Am. J. Epidemiol. 2006, 163, 959–970. [Google Scholar] [CrossRef]
- Dhalla, A.; McDonald, T.E.; Gallagher, R.P.; Spinelli, J.J.; Brooks-Wilson, A.R.; Lee, T.K.; Lai, C.; Borugian, M.J.; Woods, R.R.; Le, N.D.; et al. Cohort Profile: The British Columbia Generations Project (BCGP). Int. J. Epidemiol. 2019, 48, 377–378k. [Google Scholar] [CrossRef]
- BC Generations Project. Health and Lifestyle Core Questionnaire for Women and Men. Available online: https://www.bcgenerationsproject.ca/wp-content/uploads/2015/06/TELF-Q.pdf (accessed on 19 November 2022).
- Van Calster, B.; Van Belle, V.; Vergouwe, Y.; Steyerberg, E.W. Discrimination ability of prediction models for ordinal outcomes: Relationships between existing measures and a new measure. Biom. J. 2012, 54, 674–685. [Google Scholar] [CrossRef] [PubMed]
- Van Hoorde, K.; Vergouwe, Y.; Timmerman, D.; Van Huffel, S.; Steyerberg, E.W.; Van Calster, B. Assessing calibration of multinomial risk prediction models. Stat. Med. 2014, 33, 2585–2596. [Google Scholar] [CrossRef]
- Van Calster, B.; Nieboer, D.; Vergouwe, Y.; De Cock, B.; Pencina, M.J.; Steyerberg, E.W. A calibration hierarchy for risk models was defined: From utopia to empirical data. J. Clin. Epidemiol. 2016, 74, 167–176. [Google Scholar] [CrossRef]
- Edlinger, M.; van Smeden, M.; Alber, H.F.; Wanitschek, M.; Van Calster, B. Risk prediction models for discrete ordinal outcomes: Calibration and the impact of the proportional odds assumption. Stat. Med. 2022, 41, 1334–1360. [Google Scholar] [CrossRef] [PubMed]
- Lyratzopoulos, G.; Abel, G.A.; Barbiere, J.M.; Brown, C.H.; Rous, B.A.; Greenberg, D.C. Variation in advanced stage at diagnosis of lung and female breast cancer in an English region 2006–2009. Br. J. Cancer 2012, 106, 1068–1075. [Google Scholar] [CrossRef] [Green Version]
- Rendon, R.A.; Mason, R.J.; Marzouk, K.; Finelli, A.; Saad, F.; So, A.; Violette, P.; Breau, R.H. Canadian Urological Association recommendations on prostate cancer screening and early diagnosis. Can. Urol. Assoc. J. 2017, 11, 298–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, G.; Zhang, Y.; Wang, L.; Huang, Y.; Yu, Q.; Guo, P.; Li, K. Risk of colorectal cancer with hysterectomy and oophorectomy: A systematic review and meta-analysis. Int. J. Surg. 2016, 34, 88–95. [Google Scholar] [CrossRef]
- Collins, G.S.; de Groot, J.A.; Dutton, S.; Omar, O.; Shanyinde, M.; Tajar, A.; Voysey, M.; Wharton, R.; Yu, L.M.; Moons, K.G.; et al. External validation of multivariable prediction models: A systematic review of methodological conduct and reporting. BMC Med. Res. Methodol. 2014, 14, 40. [Google Scholar] [CrossRef] [Green Version]
- Van Calster, B.; Vickers, A.J. Calibration of risk prediction models: Impact on decision-analytic performance. Med. Decis. Making 2015, 35, 162–169. [Google Scholar] [CrossRef]
- Birkenbihl, C.; Emon, M.A.; Vrooman, H.; Westwood, S.; Lovestone, S.; AddNeuroMed, C.; Hofmann-Apitius, M.; Frohlich, H.; Alzheimer’s Disease Neuroimaging Initiative. Differences in cohort study data affect external validation of artificial intelligence models for predictive diagnostics of dementia—Lessons for translation into clinical practice. EPMA J. 2020, 11, 367–376. [Google Scholar] [CrossRef]
- Gravesteijn, B.Y.; Sewalt, C.A.; Venema, E.; Nieboer, D.; Steyerberg, E.W.; Collaborators, C.-T. Missing Data in Prediction Research: A Five-Step Approach for Multiple Imputation, Illustrated in the CENTER-TBI Study. J. Neurotrauma 2021, 38, 1842–1857. [Google Scholar] [CrossRef] [PubMed]
- Binuya, M.A.E.; Engelhardt, E.G.; Schats, W.; Schmidt, M.K.; Steyerberg, E.W. Methodological guidance for the evaluation and updating of clinical prediction models: A systematic review. BMC Med. Res. Methodol. 2022, 22, 316. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| ATP | BCGP | |||||
|---|---|---|---|---|---|---|
| Cancer Cases from the Alberta Cancer Registry (n) | Cancer Staging Available (n) | Missing Cancer Staging (%) | Cancer Cases from the BC Cancer Registry (n) | Cancer Staging Available (n) | Missing Cancer Staging (%) | |
| Male | ||||||
| Breast cancer | ||||||
| Lung cancer | 95 | 88 | 7% | 27 | 21 | 22% |
| Colorectal cancer | 135 | 128 | 5% | 36 | 24 | 33% |
| Prostate cancer | 461 | 410 | 11% | 228 | 171 | 25% |
| Other cancers | 484 | 277 | 43% | 444 | 82 | 82% |
| Total | 1175 | 903 | 23% | 735 | 298 | 59% |
| Female | ||||||
| Breast cancer | 530 | 526 | 1% | 358 | 293 | 18% |
| Lung cancer | 149 | 133 | 11% | 61 | 47 | 23% |
| Colorectal cancer | 144 | 139 | 3% | 61 | 47 | 23% |
| Prostate cancer | ||||||
| Other cancers | 669 | 411 | 39% | 630 | 170 | 73% |
| Total | 1492 | 1209 | 19% | 1110 | 557 | 50% |
| Cancer Stage (PPO) | OR (95% CI) | p Value | |
|---|---|---|---|
| Age at diagnosis (10 years) | 0.84 (0.72, 0.99) | 0.04 | |
| Employed full- or part-time | |||
| Yes vs. No | IV vs. I and II and III | 0.49 (0.34, 0.70) | <0.001 |
| III and IV vs. I and II | 0.72 (0.53, 0.99) | 0.04 | |
| II and III and IV vs. I | 0.77 (0.53, 1.10) | 0.15 | |
| Heart attack family history | |||
| Yes vs. No | 1.26 (0.98, 1.63) | 0.07 | |
| History of PSA blood test | |||
| Yes vs. No | IV vs. I and II and III | 0.68 (0.48, 0.96) | 0.03 |
| III and IV vs. I and II | 0.69 (0.51, 0.92) | 0.01 | |
| II and III and IV vs. I | 1.01 (0.73, 1.40) | 0.96 | |
| Smoking status | |||
| Never smoker | 1.0 | ||
| Past smoker | 1.44 (1.10, 1.90) | 0.01 | |
| Current smoker | 2.34 (1.66, 3.29) | <0.001 |
| Cancer Stage (PPO) | ORs (95% CI) | p Value | |
|---|---|---|---|
| Age at diagnosis (10 years) | III/IV vs. I and II | 1.40 (1.21, 1.61) | <0.001 |
| II and III/IV vs. I | 1.09 (0.96, 1.25) | 0.19 | |
| Number of pregnancies | 1.08 (1.01, 1.14) | 0.02 | |
| History of sigmoidoscopy or colonoscopy | |||
| Yes vs. No | 0.74 (0.58, 0.95) | 0.02 | |
| History of mammogram | |||
| Yes vs. No | 0.69 (0.50, 0.95) | 0.02 | |
| History of hysterectomy | |||
| Yes vs. No | 1.32 (1.03, 1.70) | 0.03 |
| Calibration Intercepts (95% CI) per Outcome Dichotomy | |||||
|---|---|---|---|---|---|
| Model | ECI | ORC | |||
| Male PPO | 0.11 (−0.17, 0.37) | −0.19 (−0.42, 0.05) | 0.08 (−0.21, 0.39) | 1.11 | 0.58 |
| Female PPO | 0.06 (−0.11, 0.22) | −0.04 (−0.22, 0.15) | 0.32 | 0.53 | |
| Calibration slopes (95% CI) Per outcome dichotomy | |||||
| Male PPO | 0.67 (−0.30, 1.69) | 1.43 (0.68, 2.23) | 0.86 (0.15, 1.59) | ||
| Female PPO | 0.62 (−0.08, 1.33) | 0.53 (−0.01, 1.08) | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Biziaev, T.; Aktary, M.L.; Wang, Q.; Chekouo, T.; Bhatti, P.; Shack, L.; Robson, P.J.; Kopciuk, K.A. Development and External Validation of Partial Proportional Odds Risk Prediction Models for Cancer Stage at Diagnosis among Males and Females in Canada. Cancers 2023, 15, 3545. https://doi.org/10.3390/cancers15143545
Biziaev T, Aktary ML, Wang Q, Chekouo T, Bhatti P, Shack L, Robson PJ, Kopciuk KA. Development and External Validation of Partial Proportional Odds Risk Prediction Models for Cancer Stage at Diagnosis among Males and Females in Canada. Cancers. 2023; 15(14):3545. https://doi.org/10.3390/cancers15143545
Chicago/Turabian StyleBiziaev, Timofei, Michelle L. Aktary, Qinggang Wang, Thierry Chekouo, Parveen Bhatti, Lorraine Shack, Paula J. Robson, and Karen A. Kopciuk. 2023. "Development and External Validation of Partial Proportional Odds Risk Prediction Models for Cancer Stage at Diagnosis among Males and Females in Canada" Cancers 15, no. 14: 3545. https://doi.org/10.3390/cancers15143545
APA StyleBiziaev, T., Aktary, M. L., Wang, Q., Chekouo, T., Bhatti, P., Shack, L., Robson, P. J., & Kopciuk, K. A. (2023). Development and External Validation of Partial Proportional Odds Risk Prediction Models for Cancer Stage at Diagnosis among Males and Females in Canada. Cancers, 15(14), 3545. https://doi.org/10.3390/cancers15143545