
Telemedicine in Care of Sarcoma Patients beyond the COVID-19 Pandemic: Challenges and Opportunities




Abstract
:Simple Summary
Abstract
1. Introduction
1.1. History of Telemedicine in Oncology
1.2. Telehealth and COVID-19
1.3. Telehealth in Sarcoma Care
1.4. Aim
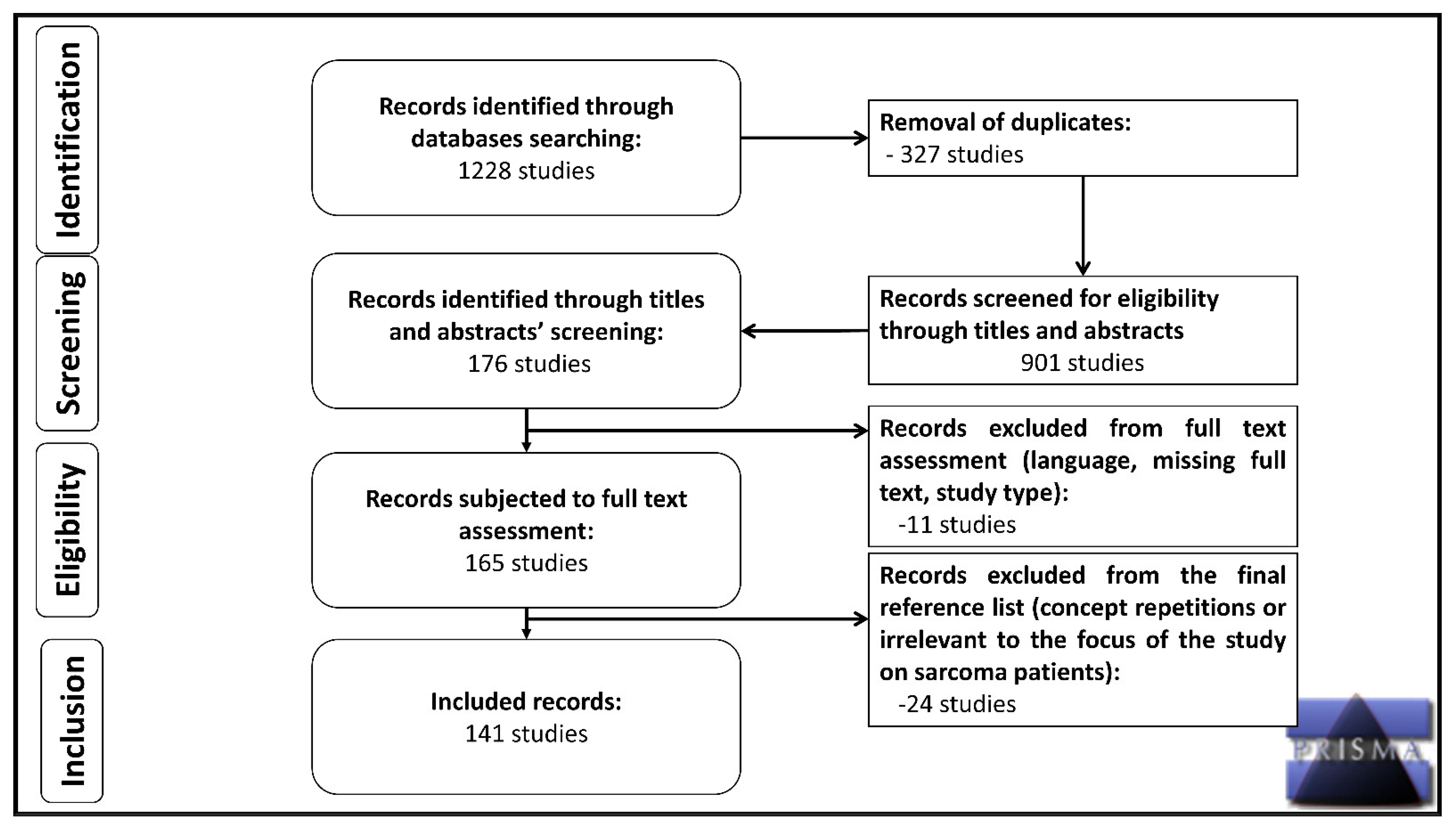
2. Materials and Methods
3. Results
3.1. Qualitative and Quantitative Data Presentation
3.1.1. Telemedicine and Sarcoma Diagnosis
3.1.2. Telemedicine and Surgery
3.1.3. Tele-Oncology for Sarcoma Patients
3.1.4. Telerehabilitation for Sarcoma Patients
3.1.5. Telemedicine and Mental Health during COVID-19
3.1.6. Compliance and Satisfaction with Telemedicine
3.2. Telemedicine Guidelines, Practice and Policy
4. Discussion
4.1. Benefits of Telemedicine in Cancer Care
4.2. Challenges of Telemedicine
4.3. Opportunities and Future Perspectives
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Nesbitt, T. The Evolution of Telehealth: Where Have We Been and Where Are We Going? In The Role of Telehealth in an Evolving Health Care Environment: Workshop Summary; Board on Health Care Services Institute of Medicine; National Academies Press: Washington, DC, USA, 2012. [Google Scholar]
- Tsagkaris, C. A short history of surgery and anesthesiology in Space. JSS 2019, 6, 101–102. [Google Scholar] [CrossRef] [Green Version]
- Sirintrapun, S.J.; Lopez, A.M. Telemedicine in Cancer Care. Am. Soc. Clin. Oncol. Educ. Book 2018, 38, 540–545. [Google Scholar] [CrossRef] [PubMed]
- Aunon-Chancellor, S.M.; Pattarini, J.M.; Moll, S.; Sargsyan, A. Venous Thrombosis during Spaceflight. N. Engl. J. Med. 2020, 382, 89–90. [Google Scholar] [CrossRef] [PubMed]
- Barney, A.; Buckelew, S.; Mesheriakova, V.; Raymond-Flesch, M. The COVID-19 Pandemic and Rapid Implementation of Adolescent and Young Adult Telemedicine: Challenges and Opportunities for Innovation. J. Adolesc. Health 2020, 67, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Liu, R.; Zhou, Q.; Wang, X.; Huang, L.; Shi, Q.; Wang, Z.; Lu, S.; Li, W.; Ma, Y.; et al. Application of telemedicine during the coronavirus disease epidemics: A rapid review and meta-analysis. Ann. Transl. Med. 2020, 8, 626. [Google Scholar] [CrossRef]
- Sabesan, S.; Larkins, S.; Evans, R.; Varma, S.; Andrews, A.; Beuttner, P.; Brennan, S.; Young, M. Telemedicine for rural cancer care in North Queensland: Bringing cancer care home. Aust. J. Rural Health 2012, 20, 259–264. [Google Scholar] [CrossRef]
- Arem, H.; Moses, J.; Cisneros, C.; Blondeau, B.; Nekhlyudov, L.; Killackey, M.; Pratt-Chapman, M.L. Cancer Provider and Survivor Experiences with Telehealth during the COVID-19 Pandemic. JCO Oncol. Pract. 2022, 18, e452–e461. [Google Scholar] [CrossRef]
- Burningham, Z.; Hashibe, M.; Spector, L.; Schiffman, J.D. The epidemiology of sarcoma. Clin. Sarcoma Res. 2012, 2, 14. [Google Scholar] [CrossRef] [Green Version]
- Hoang, N.T.; Acevedo, L.A.; Mann, M.J.; Tolani, B. A review of soft-tissue sarcomas: Translation of biological advances into treatment measures. Cancer Manag. Res. 2018, 10, 1089–1114. [Google Scholar] [CrossRef] [Green Version]
- McCabe, H.M.; Smrke, A.; Cowie, F.; White, J.; Chong, P.; Lo, S.; Mahendra, A.; Gupta, S.; Ferguson, M.; Boddie, D.; et al. What Matters to Us: Impact of Telemedicine during the Pandemic in the Care of Patients with Sarcoma Across Scotland. JCO Glob. Oncol. 2021, 7, 1067–1073. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Olshinka, N.; Mottard, S. Musculoskeletal oncology: Patient triage and management during the COVID-19 pandemic. Curr. Oncol. 2020, 27, e512–e515. [Google Scholar] [CrossRef]
- Younger, E.; Smrke, A.; Lidington, E.; Farag, S.; Ingley, K.; Chopra, N.; Maleddu, A.; Augustin, Y.; Merry, E.; Wilson, R.; et al. Health-Related Quality of Life and Experiences of Sarcoma Patients during the COVID-19 Pandemic. Cancers 2020, 12, 2288. [Google Scholar] [CrossRef]
- Smrke, A.; Younger, E.; Wilson, R.; Husson, O.; Farag, S.; Merry, E.; Macklin-Doherty, A.; Cojocaru, E.; Arthur, A.; Benson, C.; et al. Telemedicine during the COVID-19 Pandemic: Impact on Care for Rare Cancers. JCO Glob. Oncol. 2020, 6, 1046–1051. [Google Scholar] [CrossRef]
- Lidington, E.K.; Smrke, A.; Ingley, K.M.; Strauss, S.J.; Husson, O.; Younger, E. Cancer care and well-being in adolescents and young adults during the coronavirus disease 2019 pandemic: A UK sarcoma perspective. Cancer 2020, 126, 5359–5360. [Google Scholar] [CrossRef]
- Buonaguro, F.M.; Botti, G.; Ascierto, P.A.; Pignata, S.; Ionna, F.; Delrio, P.; Petrillo, A.; Cavalcanti, E.; Di Bonito, M.; Perdona, S.; et al. The clinical and translational research activities at the INT—IRCCS “Fondazione Pascale” cancer center (Naples, Italy) during the COVID-19 pandemic. Infect. Agents Cancer 2020, 15, 69. [Google Scholar] [CrossRef]
- Martinez, D.; Sarria, G.J.; Wakefield, D.; Flores, C.; Malhotra, S.; Li, B.; Ehmann, M.; Schwartz, D.L.; Sarria, G.R. COVID’s Impact on Radiation Oncology: A Latin American Survey Study. Int. J. Radiat. Oncol. Biol. Phys. 2020, 108, 374–378. [Google Scholar] [CrossRef]
- de Joode, K.; Dumoulin, D.W.; Engelen, V.; Bloemendal, H.J.; Verheij, M.; van Laarhoven, H.W.M.; Dingemans, I.H.; Dingemans, A.C.; van der Veldt, A.A.M. Impact of the coronavirus disease 2019 pandemic on cancer treatment: The patients’ perspective. Eur. J. Cancer 2020, 136, 132–139. [Google Scholar] [CrossRef]
- Kosir, U.; Loades, M.; Wild, J.; Wiedemann, M.; Krajnc, A.; Roskar, S.; Bowes, L. The impact of COVID-19 on the cancer care of adolescents and young adults and their well-being: Results from an online survey conducted in the early stages of the pandemic. Cancer 2020, 126, 4414–4422. [Google Scholar] [CrossRef]
- Folsom, S.; Christie, A.J.; Cohen, L.; Lopez, G. Implementing Telehealth Music Therapy Services in an Integrative Oncology Setting: A Case Series. Integr. Cancer Ther. 2021, 20, 15347354211053647. [Google Scholar] [CrossRef]
- Hassan, H.; Elazar, A.; Takabe, K.; Datta, R.; Takahashi, H.; Seitelman, E. Scalp Leiomyosarcoma: Diagnosis and Treatment during a Global Pandemic with COVID-19. World J. Oncol. 2021, 12, 132–136. [Google Scholar] [CrossRef] [PubMed]
- Lawrenz, J.M.; Krout, J.C.; Moran, C.P.; Ready, A.K.; Schafer, E.A.; Higgins, R.T.; Halpern, J.L.; Schwartz, H.S.; Holt, G.E. Telemedicine in Orthopedic Oncology During COVID-19: Patient Satisfaction, Reimbursement, and Physical Examination Competency. Orthopedics 2021, 44, 274–279. [Google Scholar] [CrossRef] [PubMed]
- Yeshayahu, Y. Delayed Presentation of Children to Healthcare Facilities due to COVID-19 Lockdown, Leading to Severe Complications. Rambam Maimonides Med. J. 2021, 12, e0017. [Google Scholar] [CrossRef] [PubMed]
- Rajasekaran, R.B.; Whitwell, D.; Cosker, T.D.A.; Gibbons, C.; Carr, A. Will virtual multidisciplinary team meetings become the norm for musculoskeletal oncology care following the COVID-19 pandemic?—Experience from a tertiary sarcoma centre. BMC Musculoskelet. Disord. 2021, 22, 18. [Google Scholar] [CrossRef] [PubMed]
- Natesan, D.; Koontz, B.F.; Blitzblau, R.C. Radiation Oncology Provider Telehealth Satisfaction: Survey Results from a Single NCI-Designated Institution. Int. J. Radiat. Oncol. Biol. Phys. 2021, 111, e356. [Google Scholar] [CrossRef]
- Global Health Research Group on Children’s Non-Communicable Diseases Collaborative. Impact of the COVID-19 pandemic on patients with paediatric cancer in low-income, middle-income and high-income countries: A multicentre, international, observational cohort study. BMJ Open 2022, 12, e054690. [Google Scholar] [CrossRef]
- Onesti, C.E.; Vari, S.; Nardozza, F.; Maggi, G.; Minghelli, D.; Rossi, B.; Sperati, F.; Checcucci, E.; Faltyn, W.; Cercato, M.C.; et al. The impact of the COVID-19 pandemic on diagnosis and treatment of patients with soft tissue and bone sarcomas or aggressive benign musculoskeletal diseases: A single-center retrospective study (SarCorD study). Front. Oncol. 2022, 12, 1000056. [Google Scholar] [CrossRef]
- Sarfraz, S.; Saeed, H. Feasibility and safety of outpatient administration of ifosfamide and etoposide for pediatric patients with Ewing sarcoma in a resource-limited setting amid the COVID-19 pandemic. Pediatr. Blood Cancer 2022, 69, e29595. [Google Scholar] [CrossRef]
- van Erkel, F.M.; Pet, M.J.; Bossink, E.H.; van de Graaf, C.F.M.; Hodes, M.T.J.; van Ogtrop, S.N.; Mourits, M.J.E.; Welker, G.A.; Halmos, G.B.; van Leeuwen, B.; et al. Experiences of patients and health care professionals on the quality of telephone follow-up care during the COVID-19 pandemic: A large qualitative study in a multidisciplinary academic setting. BMJ Open 2022, 12, e058361. [Google Scholar] [CrossRef]
- Kotrych, D.; Ciechanowicz, D.; Pawlik, J.; Szyjkowska, M.; Kwapisz, B.; Madry, M. Delay in Diagnosis and Treatment of Primary Bone Tumors during COVID-19 Pandemic in Poland. Cancers 2022, 14, 6037. [Google Scholar] [CrossRef]
- Wagner, M.J.; Hennessy, C.; Beeghly, A.; French, B.; Shah, D.P.; Croessmann, S.; Vilar-Compte, D.; Ruiz-Garcia, E.; Ingham, M.; Schwartz, G.K.; et al. Demographics, Outcomes, and Risk Factors for Patients with Sarcoma and COVID-19: A CCC19-Registry Based Retrospective Cohort Study. Cancers 2022, 14, 4334. [Google Scholar] [CrossRef]
- Ryu, J.H.; Rahman, J.; Deo, S.; Flint, M. Effects of time to treatment initiation on outcomes for soft tissue sarcomas. J. Surg. Oncol. 2023, 127, 1174–1186. [Google Scholar] [CrossRef]
- Naidich, J.J.; Boltyenkov, A.; Wang, J.J.; Chusid, J.; Hughes, D.; Sanelli, P.C. Impact of the Coronavirus Disease 2019 (COVID-19) Pandemic on Imaging Case Volumes. J. Am. Coll. Radiol. 2020, 17, 865–872. [Google Scholar] [CrossRef]
- Baldwin-Medsker, A.; Skwira-Brown, A. The COVID-19 Pandemic and Transition to Digital Health in Clinical Oncology Care. Clin. J. Oncol. Nurs. 2022, 26, 374–382. [Google Scholar] [CrossRef]
- Chazan, G.; Franchini, F.; Alexander, M.; Banerjee, S.; Mileshkin, L.; Blinman, P.; Zielinski, R.; Karikios, D.; Pavlakis, N.; Peters, S.; et al. Impact of COVID-19 on cancer service delivery: A follow-up international survey of oncology clinicians. ESMO Open 2021, 6, 100224. [Google Scholar] [CrossRef]
- COVIDSurg Collaborative. Effect of COVID-19 pandemic lockdowns on planned cancer surgery for 15 tumour types in 61 countries: An international, prospective, cohort study. Lancet Oncol. 2021, 22, 1507–1517. [Google Scholar] [CrossRef]
- COVIDSurg Collaborative. Elective surgery cancellations due to the COVID-19 pandemic: Global predictive modelling to inform surgical recovery plans. Br. J. Surg. 2020, 107, 1440–1449. [Google Scholar] [CrossRef]
- Putro, Y.A.P.; Magetsari, R.; Mahyudin, F.; Basuki, M.H.; Saraswati, P.A.; Huwaidi, A.F. Impact of the COVID-19 on the surgical management of bone and soft tissue sarcoma: A systematic review. J. Orthop. 2023, 38, 1–6. [Google Scholar] [CrossRef]
- Callegaro, D.; Raut, C.P.; Keung, E.Z.; Kim, T.; Le Pechoux, C.; Martin-Broto, J.; Gronchi, A.; Swallow, C.; Gladdy, R. Strategies for care of patients with gastrointestinal stromal tumor or soft tissue sarcoma during COVID-19 pandemic: A guide for surgical oncologists. J. Surg. Oncol. 2021, 123, 12–23. [Google Scholar] [CrossRef]
- Tiwari, V.; Sharma, P.K.; Sampath Kumar, V.; Poudel, R.R.; Meena, S.; Banjara, R. Changes in the Management of Malignant Bone Tumors in the COVID-19 Pandemic in Developing Countries. Cureus 2022, 14, e25245. [Google Scholar] [CrossRef]
- Vordermark, D. Shift in indications for radiotherapy during the COVID-19 pandemic? A review of organ-specific cancer management recommendations from multidisciplinary and surgical expert groups. Radiat. Oncol. 2020, 15, 140. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, C.F.; Palmer Kelly, E.; Paro, A.; Cloyd, J.; Ejaz, A.; Beal, E.W.; Pawlik, T.M. Burnout Assessment among Surgeons and Surgical Trainees during the COVID-19 Pandemic: A Systematic Review. J. Surg. Educ. 2022, 79, 1206–1220. [Google Scholar] [CrossRef] [PubMed]
- Thaler, M.; Khosravi, I.; Leithner, A.; Papagelopoulos, P.J.; Ruggieri, P. Impact of the COVID-19 pandemic on patients suffering from musculoskeletal tumours. Int. Orthop. 2020, 44, 1503–1509. [Google Scholar] [CrossRef] [PubMed]
- Marrari, A.; Gennaro, N.; Cariboni, U.; Quagliuolo, V.L.; D’Orazio, F.; Cananzi, F.; Santoro, A.; Bertuzzi, A.F. It was hard enough: The spectre of COVID-19 on the management of sarcoma patients. Eur. J. Cancer Prev. 2023, 32, 69–70. [Google Scholar] [CrossRef]
- Hazin, R.; Qaddoumi, I. Teleoncology: Current and future applications for improving cancer care globally. Lancet Oncol. 2010, 11, 204–210. [Google Scholar] [CrossRef] [Green Version]
- Sabesan, S.; Kelly, J. Are teleoncology models merely about avoiding long distance travel for patients? Eur. J. Cancer Care 2014, 23, 745–749. [Google Scholar] [CrossRef]
- Sabesan, S. Medical models of teleoncology: Current status and future directions. Asia-Pac. J. Clin. Oncol. 2014, 10, 200–204. [Google Scholar] [CrossRef] [Green Version]
- Sabesan, S.; Simcox, K.; Marr, I. Medical oncology clinics through videoconferencing: An acceptable telehealth model for rural patients and health workers. Intern. Med. J. 2012, 42, 780–785. [Google Scholar] [CrossRef]
- Monaghesh, E.; Hajizadeh, A. The role of telehealth during COVID-19 outbreak: A systematic review based on current evidence. BMC Public Health 2020, 20, 1193. [Google Scholar] [CrossRef]
- Onesti, C.E.; Rugo, H.S.; Generali, D.; Peeters, M.; Zaman, K.; Wildiers, H.; Harbeck, N.; Martin, M.; Cristofanilli, M.; Cortes, J.; et al. Oncological care organisation during COVID-19 outbreak. ESMO Open 2020, 5, e000853. [Google Scholar] [CrossRef]
- Orazem, M.; Oblak, I.; Spanic, T.; Ratosa, I. Telemedicine in Radiation Oncology Post-COVID-19 Pandemic: There Is No Turning Back. Int. J. Radiat. Oncol. Biol. Phys. 2020, 108, 411–415. [Google Scholar] [CrossRef]
- McGrowder, D.A.; Miller, F.G.; Vaz, K.; Anderson Cross, M.; Anderson-Jackson, L.; Bryan, S.; Latore, L.; Thompson, R.; Lowe, D.; McFarlane, S.R.; et al. The Utilization and Benefits of Telehealth Services by Health Care Professionals Managing Breast Cancer Patients during the COVID-19 Pandemic. Healthcare 2021, 9, 1401. [Google Scholar] [CrossRef]
- Curigliano, G.; Banerjee, S.; Cervantes, A.; Garassino, M.C.; Garrido, P.; Girard, N.; Haanen, J.; Jordan, K.; Lordick, F.; Machiels, J.P.; et al. Managing cancer patients during the COVID-19 pandemic: An ESMO multidisciplinary expert consensus. Ann. Oncol. 2020, 31, 1320–1335. [Google Scholar] [CrossRef]
- Catanese, S.; Pentheroudakis, G.; Douillard, J.Y.; Lordick, F. ESMO Management and treatment adapted recommendations in the COVID-19 era: Pancreatic Cancer. ESMO Open 2020, 5, e000804. [Google Scholar] [CrossRef]
- Vecchione, L.; Stintzing, S.; Pentheroudakis, G.; Douillard, J.Y.; Lordick, F. ESMO management and treatment adapted recommendations in the COVID-19 era: Colorectal cancer. ESMO Open 2020, 5, e000826. [Google Scholar] [CrossRef]
- Khairat, S.; Meng, C.; Xu, Y.; Edson, B.; Gianforcaro, R. Interpreting COVID-19 and Virtual Care Trends: Cohort Study. JMIR Public Health Surveill. 2020, 6, e18811. [Google Scholar] [CrossRef] [Green Version]
- Berlin, A.; Lovas, M.; Truong, T.; Melwani, S.; Liu, J.; Liu, Z.A.; Badzynski, A.; Carpenter, M.B.; Virtanen, C.; Morley, L.; et al. Implementation and Outcomes of Virtual Care across a Tertiary Cancer Center during COVID-19. JAMA Oncol. 2021, 7, 597–602. [Google Scholar] [CrossRef]
- Loree, J.M.; Dau, H.; Rebic, N.; Howren, A.; Gastonguay, L.; McTaggart-Cowan, H.; Gill, S.; Raghav, K.; De Vera, M.A. Virtual Oncology Appointments during the Initial Wave of the COVID-19 Pandemic: An International Survey of Patient Perspectives. Curr. Oncol. 2021, 28, 671–677. [Google Scholar] [CrossRef]
- Narayanan, S.; Lopez, G.; Powers-James, C.; Fellman, B.M.; Chunduru, A.; Li, Y.; Bruera, E.; Cohen, L. Integrative Oncology Consultations Delivered via Telehealth in 2020 and In-Person in 2019: Paradigm Shift during the COVID-19 World Pandemic. Integr. Cancer Ther. 2021, 20, 1534735421999101. [Google Scholar] [CrossRef]
- Kasper, B.; Lecointe-Artzner, E.; Wait, S.; Boldon, S.; Wilson, R.; Gronchi, A.; Valverde, C.; Eriksson, M.; Dumont, S.; Drove, N.; et al. Working to improve the management of sarcoma patients across Europe: A policy checklist. BMC Cancer 2018, 18, 424. [Google Scholar] [CrossRef] [Green Version]
- van der Graaf, W.T.; Blay, J.Y.; Chawla, S.P.; Kim, D.W.; Bui-Nguyen, B.; Casali, P.G.; Schoffski, P.; Aglietta, M.; Staddon, A.P.; Beppu, Y.; et al. Pazopanib for metastatic soft-tissue sarcoma (PALETTE): A randomised, double-blind, placebo-controlled phase 3 trial. Lancet 2012, 379, 1879–1886. [Google Scholar] [CrossRef] [PubMed]
- Wagner, A.J.; Malinowska-Kolodziej, I.; Morgan, J.A.; Qin, W.; Fletcher, C.D.; Vena, N.; Ligon, A.H.; Antonescu, C.R.; Ramaiya, N.H.; Demetri, G.D.; et al. Clinical activity of mTOR inhibition with sirolimus in malignant perivascular epithelioid cell tumors: Targeting the pathogenic activation of mTORC1 in tumors. J. Clin. Oncol. 2010, 28, 835–840. [Google Scholar] [CrossRef] [PubMed]
- Rutkowski, P.; Van Glabbeke, M.; Rankin, C.J.; Ruka, W.; Rubin, B.P.; Debiec-Rychter, M.; Lazar, A.; Gelderblom, H.; Sciot, R.; Lopez-Terrada, D.; et al. Imatinib mesylate in advanced dermatofibrosarcoma protuberans: Pooled analysis of two phase II clinical trials. J. Clin. Oncol. 2010, 28, 1772–1779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cassier, P.A.; Gelderblom, H.; Stacchiotti, S.; Thomas, D.; Maki, R.G.; Kroep, J.R.; van der Graaf, W.T.; Italiano, A.; Seddon, B.; Domont, J.; et al. Efficacy of imatinib mesylate for the treatment of locally advanced and/or metastatic tenosynovial giant cell tumor/pigmented villonodular synovitis. Cancer 2012, 118, 1649–1655. [Google Scholar] [CrossRef]
- Drilon, A.; Laetsch, T.W.; Kummar, S.; DuBois, S.G.; Lassen, U.N.; Demetri, G.D.; Nathenson, M.; Doebele, R.C.; Farago, A.F.; Pappo, A.S.; et al. Efficacy of Larotrectinib in TRK Fusion-Positive Cancers in Adults and Children. N. Engl. J. Med. 2018, 378, 731–739. [Google Scholar] [CrossRef]
- Duffaud, F.; Mir, O.; Boudou-Rouquette, P.; Piperno-Neumann, S.; Penel, N.; Bompas, E.; Delcambre, C.; Kalbacher, E.; Italiano, A.; Collard, O.; et al. Efficacy and safety of regorafenib in adult patients with metastatic osteosarcoma: A non-comparative, randomised, double-blind, placebo-controlled, phase 2 study. Lancet Oncol. 2019, 20, 120–133. [Google Scholar] [CrossRef]
- Lostes-Bardaji, M.J.; Garcia-Illescas, D.; Valverde, C.; Serrano, C. Ripretinib in gastrointestinal stromal tumor: The long-awaited step forward. Ther. Adv. Med. Oncol. 2021, 13, 1758835920986498. [Google Scholar] [CrossRef]
- Blanke, C.D.; Rankin, C.; Demetri, G.D.; Ryan, C.W.; von Mehren, M.; Benjamin, R.S.; Raymond, A.K.; Bramwell, V.H.; Baker, L.H.; Maki, R.G.; et al. Phase III randomized, intergroup trial assessing imatinib mesylate at two dose levels in patients with unresectable or metastatic gastrointestinal stromal tumors expressing the kit receptor tyrosine kinase: S0033. J. Clin. Oncol. 2008, 26, 626–632. [Google Scholar] [CrossRef]
- Demetri, G.D.; Garrett, C.R.; Schoffski, P.; Shah, M.H.; Verweij, J.; Leyvraz, S.; Hurwitz, H.I.; Pousa, A.L.; Le Cesne, A.; Goldstein, D.; et al. Complete longitudinal analyses of the randomized, placebo-controlled, phase III trial of sunitinib in patients with gastrointestinal stromal tumor following imatinib failure. Clin. Cancer Res. 2012, 18, 3170–3179. [Google Scholar] [CrossRef] [Green Version]
- Demetri, G.D.; Reichardt, P.; Kang, Y.K.; Blay, J.Y.; Rutkowski, P.; Gelderblom, H.; Hohenberger, P.; Leahy, M.; von Mehren, M.; Joensuu, H.; et al. Efficacy and safety of regorafenib for advanced gastrointestinal stromal tumours after failure of imatinib and sunitinib (GRID): An international, multicentre, randomised, placebo-controlled, phase 3 trial. Lancet 2013, 381, 295–302. [Google Scholar] [CrossRef] [Green Version]
- George, S.; Jones, R.L.; Bauer, S.; Kang, Y.K.; Schoffski, P.; Eskens, F.; Mir, O.; Cassier, P.A.; Serrano, C.; Tap, W.D.; et al. Avapritinib in Patients with Advanced Gastrointestinal Stromal Tumors following at Least Three Prior Lines of Therapy. Oncologist 2021, 26, e639–e649. [Google Scholar] [CrossRef]
- Schoffski, P.; Mir, O.; Kasper, B.; Papai, Z.; Blay, J.Y.; Italiano, A.; Benson, C.; Kopeckova, K.; Ali, N.; Dileo, P.; et al. Activity and safety of the multi-target tyrosine kinase inhibitor cabozantinib in patients with metastatic gastrointestinal stromal tumour after treatment with imatinib and sunitinib: European Organisation for Research and Treatment of Cancer phase II trial 1317 ‘CaboGIST’. Eur. J. Cancer 2020, 134, 62–74. [Google Scholar] [CrossRef]
- Maccaroni, E.; Lunerti, V.; Agostinelli, V.; Giampieri, R.; Zepponi, L.; Pagliacci, A.; Berardi, R. New Insights into Hormonal Therapies in Uterine Sarcomas. Cancers 2022, 14, 921. [Google Scholar] [CrossRef]
- Malliaras, P.; Cridland, K.; Hopmans, R.; Ashton, S.; Littlewood, C.; Page, R.; Harris, I.; Skouteris, H.; Haines, T. Internet and Telerehabilitation-Delivered Management of Rotator Cuff-Related Shoulder Pain (INTEL Trial): Randomized Controlled Pilot and Feasibility Trial. JMIR Mhealth Uhealth 2020, 8, e24311. [Google Scholar] [CrossRef]
- Chang, P.; Zheng, J. Updates in Cancer Rehabilitation Telehealth. Curr. Phys. Med. Rehabil. Rep. 2022, 10, 332–338. [Google Scholar] [CrossRef]
- Lopez, C.J.; Edwards, B.; Langelier, D.M.; Chang, E.K.; Chafranskaia, A.; Jones, J.M. Delivering Virtual Cancer Rehabilitation Programming during the First 90 Days of the COVID-19 Pandemic: A Multimethod Study. Arch. Phys. Med. Rehabil. 2021, 102, 1283–1293. [Google Scholar] [CrossRef]
- Campbell, K.L.; Winters-Stone, K.M.; Wiskemann, J.; May, A.M.; Schwartz, A.L.; Courneya, K.S.; Zucker, D.S.; Matthews, C.E.; Ligibel, J.A.; Gerber, L.H.; et al. Exercise Guidelines for Cancer Survivors: Consensus Statement from International Multidisciplinary Roundtable. Med. Sci. Sports Exerc. 2019, 51, 2375–2390. [Google Scholar] [CrossRef]
- Bland, K.A.; Bigaran, A.; Campbell, K.L.; Trevaskis, M.; Zopf, E.M. Exercising in Isolation? The Role of Telehealth in Exercise Oncology during the COVID-19 Pandemic and Beyond. Phys. Ther. 2020, 100, 1713–1716. [Google Scholar] [CrossRef]
- Galiano-Castillo, N.; Cantarero-Villanueva, I.; Fernandez-Lao, C.; Ariza-Garcia, A.; Diaz-Rodriguez, L.; Del-Moral-Avila, R.; Arroyo-Morales, M. Telehealth system: A randomized controlled trial evaluating the impact of an internet-based exercise intervention on quality of life, pain, muscle strength, and fatigue in breast cancer survivors. Cancer 2016, 122, 3166–3174. [Google Scholar] [CrossRef]
- Neil-Sztramko, S.E.; Winters-Stone, K.M.; Bland, K.A.; Campbell, K.L. Updated systematic review of exercise studies in breast cancer survivors: Attention to the principles of exercise training. Br. J. Sports Med. 2019, 53, 504–512. [Google Scholar] [CrossRef] [Green Version]
- Morrison, K.S.; Paterson, C.; Toohey, K. The Feasibility of Exercise Interventions Delivered via Telehealth for People Affected by Cancer: A Rapid Review of the Literature. Semin. Oncol. Nurs. 2020, 36, 151092. [Google Scholar] [CrossRef] [PubMed]
- Chirico, A.; Lucidi, F.; De Laurentiis, M.; Milanese, C.; Napoli, A.; Giordano, A. Virtual Reality in Health System: Beyond Entertainment. A Mini-Review on the Efficacy of VR During Cancer Treatment. J. Cell. Physiol. 2016, 231, 275–287. [Google Scholar] [CrossRef] [PubMed]
- Schade, E.C.; Elkaddoum, R.; Kourie, H.R. The psychological challenges for oncological patients in times of COVID-19 pandemic: Telemedicine, a solution? Future Oncol. 2020, 16, 2265–2268. [Google Scholar] [CrossRef]
- Koc, Z.; Kaplan, E.; Tanriverdi, D. The effectiveness of telehealth programs on the mental health of women with breast cancer: A systematic review. J. Telemed. Telecare 2022, 1357633X211069663. [Google Scholar] [CrossRef]
- Sansom-Daly, U.M.; Wakefield, C.E.; Ellis, S.J.; McGill, B.C.; Donoghoe, M.W.; Butow, P.; Bryant, R.A.; Sawyer, S.M.; Patterson, P.; Anazodo, A.; et al. Online, Group-Based Psychological Support for Adolescent and Young Adult Cancer Survivors: Results from the Recapture Life Randomized Trial. Cancers 2021, 13, 2460. [Google Scholar] [CrossRef] [PubMed]
- Melton, L.; Brewer, B.; Kolva, E.; Joshi, T.; Bunch, M. Increasing access to care for young adults with cancer: Results of a quality-improvement project using a novel telemedicine approach to supportive group psychotherapy. Palliat. Support. Care 2017, 15, 176–180. [Google Scholar] [CrossRef]
- Larson, J.L.; Rosen, A.B.; Wilson, F.A. The Effect of Telehealth Interventions on Quality of Life of Cancer Patients: A Systematic Review and Meta-Analysis. Telemed. J. e-Health 2018, 24, 397–405. [Google Scholar] [CrossRef]
- Basch, E.; Schrag, D.; Henson, S.; Jansen, J.; Ginos, B.; Stover, A.M.; Carr, P.; Spears, P.A.; Jonsson, M.; Deal, A.M.; et al. Effect of Electronic Symptom Monitoring on Patient-Reported Outcomes among Patients with Metastatic Cancer: A Randomized Clinical Trial. JAMA 2022, 327, 2413–2422. [Google Scholar] [CrossRef]
- Reynolds, L.M.; Cavadino, A.; Chin, S.; Little, Z.; Akroyd, A.; Tennant, G.; Dobson, R.; Broom, R.; Gautier, A. The benefits and acceptability of virtual reality interventions for women with metastatic breast cancer in their homes; a pilot randomised trial. BMC Cancer 2022, 22, 360. [Google Scholar] [CrossRef]
- Hoffman, A.J.; Brintnall, R.A.; Brown, J.K.; von Eye, A.; Jones, L.W.; Alderink, G.; Ritz-Holland, D.; Enter, M.; Patzelt, L.H.; VanOtteren, G.M. Virtual reality bringing a new reality to postthoracotomy lung cancer patients via a home-based exercise intervention targeting fatigue while undergoing adjuvant treatment. Cancer Nurs. 2014, 37, 23–33. [Google Scholar] [CrossRef]
- Melillo, A.; Chirico, A.; De Pietro, G.; Gallo, L.; Caggianese, G.; Barone, D.; De Laurentiis, M.; Giordano, A. Virtual Reality Rehabilitation Systems for Cancer Survivors: A Narrative Review of the Literature. Cancers 2022, 14, 3163. [Google Scholar] [CrossRef]
- Steindal, S.A.; Nes, A.A.G.; Godskesen, T.E.; Dihle, A.; Lind, S.; Winger, A.; Klarare, A. Patients’ Experiences of Telehealth in Palliative Home Care: Scoping Review. J. Med. Internet Res. 2020, 22, e16218. [Google Scholar] [CrossRef]
- Dubey, S.; Biswas, P.; Ghosh, R.; Chatterjee, S.; Dubey, M.J.; Chatterjee, S.; Lahiri, D.; Lavie, C.J. Psychosocial impact of COVID-19. Diabetes Metab. Syndr. 2020, 14, 779–788. [Google Scholar] [CrossRef]
- Rivest, J.; Caron, D.; Desbeaumes Jodoin, V. COVID-19 pandemic: Will telemedicine be a new standard for mental health in cancer care? J. Psychosoc. Oncol. 2021, 39, 333–336. [Google Scholar] [CrossRef]
- Singleton, A.C.; Raeside, R.; Hyun, K.K.; Partridge, S.R.; Di Tanna, G.L.; Hafiz, N.; Tu, Q.; Tat-Ko, J.; Sum, S.C.M.; Sherman, K.A.; et al. Electronic Health Interventions for Patients with Breast Cancer: Systematic Review and Meta-Analyses. J. Clin. Oncol. 2022, 40, 2257–2270. [Google Scholar] [CrossRef]
- Orlando, J.F.; Beard, M.; Kumar, S. Systematic review of patient and caregivers’ satisfaction with telehealth videoconferencing as a mode of service delivery in managing patients’ health. PLoS ONE 2019, 14, e0221848. [Google Scholar] [CrossRef] [Green Version]
- Marzorati, C.; Renzi, C.; Russell-Edu, S.W.; Pravettoni, G. Telemedicine Use Among Caregivers of Cancer Patients: Systematic Review. J. Med. Internet Res. 2018, 20, e223. [Google Scholar] [CrossRef]
- Turner, K.; Bobonis Babilonia, M.; Naso, C.; Nguyen, O.; Gonzalez, B.D.; Oswald, L.B.; Robinson, E.; Elston Lafata, J.; Ferguson, R.J.; Alishahi Tabriz, A.; et al. Health Care Providers’ and Professionals’ Experiences with Telehealth Oncology Implementation During the COVID-19 Pandemic: A Qualitative Study. J. Med. Internet Res. 2022, 24, e29635. [Google Scholar] [CrossRef]
- Jimenez-Rodriguez, D.; Santillan Garcia, A.; Montoro Robles, J.; Rodriguez Salvador, M.D.M.; Munoz Ronda, F.J.; Arrogante, O. Increase in Video Consultations During the COVID-19 Pandemic: Healthcare Professionals’ Perceptions about Their Implementation and Adequate Management. Int. J. Environ. Res. Public Health 2020, 17, 5112. [Google Scholar] [CrossRef]
- Johnston, B.; Kidd, L.; Wengstrom, Y.; Kearney, N. An evaluation of the use of Telehealth within palliative care settings across Scotland. Palliat. Med. 2012, 26, 152–161. [Google Scholar] [CrossRef]
- Isautier, J.M.; Copp, T.; Ayre, J.; Cvejic, E.; Meyerowitz-Katz, G.; Batcup, C.; Bonner, C.; Dodd, R.; Nickel, B.; Pickles, K.; et al. People’s Experiences and Satisfaction with Telehealth During the COVID-19 Pandemic in Australia: Cross-Sectional Survey Study. J. Med. Internet Res. 2020, 22, e24531. [Google Scholar] [CrossRef] [PubMed]
- Society of Surgical Oncology (SSO). Resource for Management Options of Sarcoma during COVID-19. Available online: https://www.surgonc.org/wp-content/uploads/2020/03/Sarcoma-Resource-during-COVID-19-3.30.20.pdf (accessed on 30 March 2020).
- ASCO. Special Report: A Guide to Cancer Care Delivery during the COVID-19 Pandemic. ASCO.org. Available online: https://www.asco.org/sites/new-www.asco.org/files/content-files/2020-ASCO-Guide-Cancer-COVID19.pdf (accessed on 13 July 2021).
- Cavaliere, D.; Parini, D.; Marano, L.; Cipriani, F.; Di Marzo, F.; Macri, A.; D’Ugo, D.; Roviello, F.; Gronchi, A.; SICO. Surgical management of oncologic patient during and after the COVID-19 outbreak: Practical recommendations from the Italian society of Surgical Oncology. Updates Surg. 2021, 73, 321–329. [Google Scholar] [CrossRef] [PubMed]
- Martin-Broto, J.; Hindi, N.; Aguiar, S., Jr.; Badilla-Gonzalez, R.; Castro-Oliden, V.; Chacon, M.; Correa-Generoso, R.; de Alava, E.; Donati, D.M.; Eriksson, M.; et al. Sarcoma European and Latin American Network (SELNET) Recommendations on Prioritization in Sarcoma Care during the COVID-19 Pandemic. Oncologist 2020, 25, e1562–e1573. [Google Scholar] [CrossRef] [PubMed]
- Burki, T.K. Cancer guidelines during the COVID-19 pandemic. Lancet Oncol. 2020, 21, 629–630. [Google Scholar] [CrossRef]
- Casali, P.G.; Blay, J.Y.; Abecassis, N.; Bajpai, J.; Bauer, S.; Biagini, R.; Bielack, S.; Bonvalot, S.; Boukovinas, I.; Bovee, J.; et al. Gastrointestinal stromal tumours: ESMO-EURACAN-GENTURIS Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2022, 33, 20–33. [Google Scholar] [CrossRef]
- Strauss, S.J.; Frezza, A.M.; Abecassis, N.; Bajpai, J.; Bauer, S.; Biagini, R.; Bielack, S.; Blay, J.Y.; Bolle, S.; Bonvalot, S.; et al. Bone sarcomas: ESMO-EURACAN-GENTURIS-ERN PaedCan Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. 2021, 32, 1520–1536. [Google Scholar] [CrossRef]
- Rossi, B.; Zoccali, C.; Baldi, J.; Scotto di Uccio, A.; Biagini, R.; De Luca, A.; Petrongari, M.G.; Ferraresi, V. Reorganization Tips from a Sarcoma Unit at Time of the COVID-19 Pandemic in Italy: Early Experience from a Regional Referral Oncologic Center. J. Clin. Med. 2020, 9, 1868. [Google Scholar] [CrossRef]
- Janssens, G.O.; Mandeville, H.C.; Timmermann, B.; Maduro, J.H.; Alapetite, C.; Padovani, L.; Horan, G.; Lassen-Ramshad, Y.; Dieckmann, K.; Ruebe, C.; et al. A rapid review of evidence and recommendations from the SIOPE radiation oncology working group to help mitigate for reduced paediatric radiotherapy capacity during the COVID-19 pandemic or other crises. Radiother. Oncol. 2020, 148, 216–222. [Google Scholar] [CrossRef]
- Siavashpour, Z.; Goharpey, N.; Mobasheri, M. Radiotherapy based management during COVID-19 pandemic—A systematic review of presented consensus and guidelines. Crit. Rev. Oncol. Hematol. 2021, 164, 103402. [Google Scholar] [CrossRef]
- Lenihan, D.; Carver, J.; Porter, C.; Liu, J.E.; Dent, S.; Thavendiranathan, P.; Mitchell, J.D.; Nohria, A.; Fradley, M.G.; Pusic, I.; et al. Cardio-oncology care in the era of the coronavirus disease 2019 (COVID-19) pandemic: An International Cardio-Oncology Society (ICOS) statement. CA Cancer J. Clin. 2020, 70, 480–504. [Google Scholar] [CrossRef]
- Ben-Arye, E.; Paller, C.J.; Lopez, A.M.; White, S.; Pendleton, E.; Kienle, G.S.; Samuels, N.; Abbawaajii, N.; Balneaves, L.G. The Society for Integrative Oncology Practice Recommendations for online consultation and treatment during the COVID-19 pandemic. Support. Care Cancer 2021, 29, 6155–6165. [Google Scholar] [CrossRef]
- Lloyd, J.; Lee, C.J. Use of Telemedicine in Care of Hematologic Malignancy Patients: Challenges and Opportunities. Curr. Hematol. Malig. Rep. 2022, 17, 25–30. [Google Scholar] [CrossRef]
- Shen, Y.T.; Chen, L.; Yue, W.W.; Xu, H.X. Digital Technology-Based Telemedicine for the COVID-19 Pandemic. Front. Med. 2021, 8, 646506. [Google Scholar] [CrossRef]
- Lieneck, C.; Garvey, J.; Collins, C.; Graham, D.; Loving, C.; Pearson, R. Rapid Telehealth Implementation during the COVID-19 Global Pandemic: A Rapid Review. Healthcare 2020, 8, 517. [Google Scholar] [CrossRef]
- Khera, N.; Martin, P.; Edsall, K.; Bonagura, A.; Burns, L.J.; Juckett, M.; King, O.; LeMaistre, C.F.; Majhail, N.S. Patient-centered care coordination in hematopoietic cell transplantation. Blood Adv. 2017, 1, 1617–1627. [Google Scholar] [CrossRef] [Green Version]
- Sahin, U.; Toprak, S.K.; Atilla, P.A.; Atilla, E.; Demirer, T. An overview of infectious complications after allogeneic hematopoietic stem cell transplantation. J. Infect. Chemother. 2016, 22, 505–514. [Google Scholar] [CrossRef] [Green Version]
- Williams, A.M.; Bhatti, U.F.; Alam, H.B.; Nikolian, V.C. The role of telemedicine in postoperative care. Mhealth 2018, 4, 11. [Google Scholar] [CrossRef]
- Laughlin, A.I.; Begley, M.; Delaney, T.; Zinck, L.; Schuchter, L.M.; Doyle, J.; Mehta, S.; Bekelman, J.E.; Scott, C.A. Accelerating the delivery of cancer care at home during the COVID-19 pandemic. NEJM Catal. 2020, 1. [Google Scholar]
- Paterson, C.; Bacon, R.; Dwyer, R.; Morrison, K.S.; Toohey, K.; O’Dea, A.; Slade, J.; Mortazavi, R.; Roberts, C.; Pranavan, G.; et al. The Role of Telehealth during the COVID-19 Pandemic across the Interdisciplinary Cancer Team: Implications for Practice. Semin. Oncol. Nurs. 2020, 36, 151090. [Google Scholar] [CrossRef]
- McCue, M.; Fairman, A.; Pramuka, M. Enhancing quality of life through telerehabilitation. Phys. Med. Rehabil. Clin. N. Am. 2010, 21, 195–205. [Google Scholar] [CrossRef]
- Tarasenko, Y.N.; Linder, D.F.; Miller, E.A. Muscle-strengthening and aerobic activities and mortality among 3+ year cancer survivors in the U.S. Cancer Causes Control 2018, 29, 475–484. [Google Scholar] [CrossRef] [PubMed]
- Ftouni, R.; AlJardali, B.; Hamdanieh, M.; Ftouni, L.; Salem, N. Challenges of Telemedicine during the COVID-19 pandemic: A systematic review. BMC Med. Inform. Decis. Mak. 2022, 22, 207. [Google Scholar] [CrossRef] [PubMed]
- Lopez, A.M.; Lam, K.; Thota, R. Barriers and Facilitators to Telemedicine: Can You Hear Me Now? Am. Soc. Clin. Oncol. Educ. Book 2021, 41, 25–36. [Google Scholar] [CrossRef]
- Shao, C.C.; McLeod, M.C.; Gleason, L.T.; Dos Santos Marques, I.C.; Chu, D.I.; Wallace, E.L.; Fouad, M.N.; Reddy, S. Inequity in Telemedicine Use among Patients with Cancer in the Deep South during the COVID-19 Pandemic. Oncologist 2022, 27, 555–564. [Google Scholar] [CrossRef] [PubMed]
- Saeed, S.A.; Masters, R.M. Disparities in Health Care and the Digital Divide. Curr. Psychiatry Rep. 2021, 23, 61. [Google Scholar] [CrossRef]
- Chan, R.J.; Crichton, M.; Crawford-Williams, F.; Agbejule, O.A.; Yu, K.; Hart, N.H.; de Abreu Alves, F.; Ashbury, F.D.; Eng, L.; Fitch, M.; et al. The efficacy, challenges, and facilitators of telemedicine in post-treatment cancer survivorship care: An overview of systematic reviews. Ann. Oncol. 2021, 32, 1552–1570. [Google Scholar] [CrossRef]
- Kronenfeld, J.P.; Penedo, F.J. Novel Coronavirus (COVID-19): Telemedicine and remote care delivery in a time of medical crisis, implementation, and challenges. Transl. Behav. Med. 2021, 11, 659–663. [Google Scholar] [CrossRef]
- Gerke, S.; Shachar, C.; Chai, P.R.; Cohen, I.G. Regulatory, safety, and privacy concerns of home monitoring technologies during COVID-19. Nat. Med. 2020, 26, 1176–1182. [Google Scholar] [CrossRef]
- Bassan, S. Data privacy considerations for telehealth consumers amid COVID-19. J. Law Biosci. 2020, 7, lsaa075. [Google Scholar] [CrossRef]
- Murphy, A.; Kirby, A.; Lawlor, A.; Drummond, F.J.; Heavin, C. Mitigating the Impact of the COVID-19 Pandemic on Adult Cancer Patients through Telehealth Adoption: A Systematic Review. Sensors 2022, 22, 3598. [Google Scholar] [CrossRef]
- Lenharo, M. WHO declares end to COVID-19′s emergency phase. Nature 2023, 882. [Google Scholar] [CrossRef]
- Damico, N.J.; Deshane, A.; Kharouta, M.; Wu, A.; Wang, G.M.; Machtay, M.X.; Kumar, A.; Choi, S.; Bhatt, A.D. Telemedicine Use and Satisfaction among Radiation Oncologists during the COVID-19 Pandemic: Evaluation of Current Trends and Future Opportunities. Adv. Radiat. Oncol. 2022, 7, 100835. [Google Scholar] [CrossRef]
- Fisher, J.A.; McManus, L.; Kalbaugh, J.M.; Walker, R.L. Phase I trial compensation: How much do healthy volunteers actually earn from clinical trial enrollment? Clin. Trials 2021, 18, 477–487. [Google Scholar] [CrossRef]
- Jagsi, R.; Griffith, K.A.; Stewart, A.; Sambuco, D.; DeCastro, R.; Ubel, P.A. Gender differences in salary in a recent cohort of early-career physician-researchers. Acad. Med. 2013, 88, 1689–1699. [Google Scholar] [CrossRef]
- Panteli, D.; Maier, C.B. Regulating the health workforce in Europe: Implications of the COVID-19 pandemic. Human Resour. Health 2021, 19, 80. [Google Scholar] [CrossRef]
- Gordiichuk, P.; Kliusov, O.; Gordiichuk, M.; Kondratenko, A.; Ponomarova, O.; Grushynska, T.; Kliusov, A.; Chervynskyy, I. A view on the problem of providing oncological aid during the war in Ukraine. Contemp. Oncol. 2022, 26, 191–195. [Google Scholar] [CrossRef]
- Tsagkaris, C.; Laubsher, L.; Matiashova, L.; Lin, L.C.; Isayeva, A. The impact of energy shortages on health and healthcare in Europe. Health Sci. Rep. 2023, 6, e1075. [Google Scholar] [CrossRef] [PubMed]
- Purohit, A.; Smith, J.; Hibble, A. Does telemedicine reduce the carbon footprint of healthcare? A systematic review. Future Healthc. J. 2021, 8, e85–e91. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| First Author (Study) | Date | Study Type | Cancer Type | Sample | Type of Telemedical Intervention | Phase of Cancer Care | Categorization |
|---|---|---|---|---|---|---|---|
| Olshinka et al. [13] | 2020 | Retrospective observational study | Sarcoma | 155 FUs, 96 new referrals | Email-fax-telephone | New referrals, FU | Surgery, TO |
| Younger et al. [14] | 2020 | Cross-sectional questionnaire-based survey | Sarcoma | 350 patients | N/A | Under treatment | Mental health, Satisfaction |
| Smrke et al. [15] | 2020 | Observational, questionnaire-based survey | Sarcoma | 316 patients (379 appointments), 18 providers and 108 patients completed the survey | Telephone | New referrals, under treatment, FU | Satisfaction, TO |
| Lidington et al. [16] | 2020 | Retrospective, observational study | Sarcoma | 350 patients | N/A | Under treatment | TR, TO |
| Buonaguro et al. [17] | 2020 | Retrospective, observational study | Various types including sarcoma | N/A | Telephone, e-mail, a home healthcare platform, intensive healthcare platform | Under treatment, FU | TH in oncology and COVID-19, TO |
| Martinez et al. [18] American Society for Radiation Oncology | 2020 | Questionnaire-based survey | Various types including sarcoma | 115 responses | N/A | Under treatment, FU | Teleradiology (TO) |
| De Joode et al. [19] | 2020 | Survey-based analysis | Various types including sarcoma | 5302 patients | Telephone, video | Under treatment, FU | Satisfaction, mental health |
| Košir et al. [20] | 2020 | Cross-sectional study | Various types (AΥA) | 177 individuals | N/A | Under treatment | TO, Mental health |
| McCabe et al. [11] | 2021 | Comparative questionnaire-based observational survey, | Sarcoma | 74 patients, 26 providers | Telephone or video consultation | Under treatment, FU | TR, TO |
| Folsom et al. [21] | 2021 | Case series | Various types including sarcoma | 2 patients | videocall (zoom) | Under treatment, FU | Satisfaction, mental health |
| Hassan et al. [22] | 2021 | Case report- observational | Leiomyosarcoma | 1 patient | N/A | Diagnosis | Diagnosis, TO |
| Lawrenz et al. [23] | 2021 | Cohort-telephone survey | Sarcoma | 64 patients | Telephone | FU | Satisfaction, TO |
| Yeshayahet al. [24] | 2021 | Case series | Ewing Sarcoma | 4 patients | Telephone consultation before ER | New referrals | Diagnosis |
| Rajasekaran et al. [25] | 2021 | Questionnaire-based survey | Sarcoma | 36/39 responses | Videoconferencing platforms | MDT | Satisfaction, TO |
| Natesan et al. [26] | 2021 | Questionnaire-based survey | Various types including sarcoma | 18 radiation oncology providers | Telephone or video | Under treatment | Satisfaction, teleradiology (TO) |
| Global Health Research Group on Children’s Non-Communicable Diseases Collaborative [27] | 2022 | Retrospective observational cohort study | Various pediatric tumors including sarcoma | 1660 patients (91 hospitals and cancer centers in 39 countries) | N/A | New referrals, under treatment | TO |
| Onesti et al. [28] | 2022 | Retrospective study | STS and bone sarcoma | 372 patients | N/A | Diagnosis | TR, TO |
| Sarfraz et al. [29] | 2022 | Retrospective study | Ewing sarcoma | 20 patients | N/A | Under treatment | TO |
| M van Erkel et al. [30] | 2022 | Qualitative study using semi-structured interviews and reflexive thematic analysis | Various types including sarcoma | 82 patients and 58 providers | Telephone consultation before ER | FU | Satisfaction, TO |
| Kotrych et al. [31] | 2022 | Retrospective study | Bone sarcoma | 87 patients | N/A | New referrals | Diagnosis |
| Wagner et al. [32] | 2022 | CCC19-Registry Based Retrospective Cohort Study | Sarcoma | 281 patients | N/A | N/A | TO, sarcoma and COVID-19 |
| Hong Ryu et al. [33] | 2023 | Retrospective trial | Sarcoma | 5927 (223 eligible patients) | N/A | New referrals | TO |
| First Author (Study) | Date | Study Type | Cancer Type | Remarks |
|---|---|---|---|---|
| Curigliano et al. [54] | 2020 | Review (ESMO practice guidelines for diagnosis, treatment and FU) | Various types |
|
| SSO [103] | 2020 | Resource for management options of sarcoma during COVID-19 | Sarcoma |
|
| Lenihan et al. (ICOS) [113] | 2020 | Review (guidelines) | Various types |
Baseline ECG and QTc, as well as periodic assessment of cardiac biomarkers (TnI/TnT and NPs every 3– 6 weeks) in patients undergoing potentially cardiotoxic CT, such as anthracyclines; Routine home blood pressure monitoring in patients receiving TKIs; Prior RT: reduced cardiopulmonary reserve and increased susceptibility to a complicated COVID-19 infection; Antithrombotic prophylaxis in immobilized cardio-oncology patients with COVID-19; LMWHs constitute the first-choice antithrombotic therapy for this population. |
| Martin-Broto et al. (SELNET) [106] | 2020 | Review (guidelines) | Sarcoma |
|
| Burki et al. [107] | 2020 | Commentary | Sarcoma | The risk-benefit calculus remains challenging despite the patients’ categorization into priority groups based on their primary disease and the burden of their disease. |
| Janssens et al. (SIOPE radiation oncology group) [111] | 2020 | Review (guidelines) | Various pediatric tumors including sarcoma |
|
| Cavaliere et al. (SICO) [105] | 2021 | Review (guidelines) | Various types including STS |
|
| Siavashpour et al. [112] | 2021 | Systematic review (guidelines) regarding RT | Various types including sarcoma |
|
| Ben-Arye et al. (SIO) [114] | 2021 | Review, questionnaire, (online practice guidelines) | Various types |
|
| ASCO [104] | 2021 | ASCO special report: A guide to cancer care delivery during the COVID-19 pandemic | Various types |
|
| Strauss et al. [109] | 2021 | Review (ESMO practice guidelines for diagnosis, treatment and FU) | Bone sarcomas |
|
| Casali et al. [108] | 2022 | Review (ESMO practice guidelines for diagnosis, treatment and FU) | GIST |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsagkaris, C.; Trygonis, N.; Spyrou, V.; Koulouris, A. Telemedicine in Care of Sarcoma Patients beyond the COVID-19 Pandemic: Challenges and Opportunities. Cancers 2023, 15, 3700. https://doi.org/10.3390/cancers15143700
Tsagkaris C, Trygonis N, Spyrou V, Koulouris A. Telemedicine in Care of Sarcoma Patients beyond the COVID-19 Pandemic: Challenges and Opportunities. Cancers. 2023; 15(14):3700. https://doi.org/10.3390/cancers15143700
Chicago/Turabian StyleTsagkaris, Christos, Nikolaos Trygonis, Vasiliki Spyrou, and Andreas Koulouris. 2023. "Telemedicine in Care of Sarcoma Patients beyond the COVID-19 Pandemic: Challenges and Opportunities" Cancers 15, no. 14: 3700. https://doi.org/10.3390/cancers15143700
APA StyleTsagkaris, C., Trygonis, N., Spyrou, V., & Koulouris, A. (2023). Telemedicine in Care of Sarcoma Patients beyond the COVID-19 Pandemic: Challenges and Opportunities. Cancers, 15(14), 3700. https://doi.org/10.3390/cancers15143700