Simple Summary
Hereditary diffuse gastric cancer (HDGC) is caused by germline pathogenic variants in the CDH1 and CTNNA1 genes and is characterized by a high prevalence of diffuse gastric cancer and lobular breast cancer. We aimed to evaluate the contribution of CTNNA1 and CTNND1 germline variants to HDGC, as well as to compare the frequencies of CDH1 and CTNNA1 (and eventually CTNND1) germline variants between patients with diffuse and mixed gastric carcinomas. In this study, we report a deleterious CTNNA1 germline variant and four CDH1 pathogenic variants in patients with criteria for genetic testing. None of the cases with mixed gastric cancer carried pathogenic variants in either the CDH1 or the CTNNA1 genes, so there is no evidence to use this tumor type in testing criteria.
Abstract
The most well-characterized hereditary form of gastric cancer is hereditary diffuse gastric cancer (HDGC), an autosomal dominant syndrome characterized by an increased risk of diffuse gastric and lobular breast cancer. HDGC is predominantly caused by germline pathogenic variants in the CDH1 gene, and more rarely in the CTNNA1 gene. Furthermore, the International Gastric Cancer Linkage Consortium (IGCLC) guidelines do not clarify whether or not mixed gastric cancer (with a diffuse component) should be considered in the HDGC genetic testing criteria. We aimed to evaluate the contribution of CTNNA1 and CTNND1 germline variants to HDGC. Additionally, we also intended to compare the frequencies of CDH1 and CTNNA1 (and eventually CTNND1) germline variants between patients with diffuse and mixed gastric carcinomas to evaluate if genetic testing for these genes should or should not be considered in patients with the latter. We analyzed the CDH1 gene in 67 cases affected with early-onset/familial mixed gastric carcinomas and the CTNNA1 and CTNND1 genes in 208 cases with diffuse or mixed gastric cancer who had tested negative for CDH1 pathogenic germline variants. A deleterious CTNNA1 germline variant was found in 0.7% (1/141) of diffuse gastric cancer patients meeting the 2020 IGCLC criteria, as compared to the rate of 2.8% of CDH1 deleterious variants found by us in this setting. No deleterious variants were found in CTNND1, but six variants of uncertain significance were identified in this gene. We did not find any pathogenic CDH1, CTNNA1 or CTNND1 variant in index patients with early-onset/familial mixed gastric cancer, so there is no evidence that supports including this tumor type in the testing criteria for germline variants in these genes. The role of the CTNND1 gene in inherited gastric cancer predisposition is still unclear.
1. Introduction
Familial clustering is observed in approximately 10% of gastric cancer (GC) cases; however, only 1–3% of GC cases result from a known hereditary syndrome [1]. The most well-characterized hereditary form of GC is hereditary diffuse gastric cancer (HDGC), which is an autosomal dominant syndrome characterized by an increased risk of diffuse gastric cancer (DGC) and lobular breast cancer (LBC) [2]. Until recently, CDH1 was the only known susceptibility gene involved in HDGC, but, in 2013, Majewski and collaborators described a germline variant in the catenin alpha-1 gene (CTNNA1) for the first time in a family that fulfilled the HDGC clinical criteria [3]. Since then, to our knowledge, 13 pathogenic variants in CTNNA1 have been described in 15 families fulfilling the HDGC criteria [3,4,5,6,7,8,9,10,11]. Additionally, loss-of-function variants have been described in families without HDGC clinical criteria [9,11]. Benusiglio and collaborators reported two asymptomatic CTNNA1 pathogenic variant carriers, who displayed DGC foci in the prophylactic gastrectomy and intramucosal focus on esophagogastroduodenoscopy specimens, with loss of catenin alpha-1 expression, suggesting that pathogenic variants in CDH1 and CTNNA1 may have similar implications in DGC risk [1,7]. The penetrance of pathogenic CTNNA1 variants is still unclear, although Coudert and collaborators have recently published the first penetrance estimate for DGC in CTNNA1 families as 49–57% at 80 years [10]. The association of CTNNA1 pathogenic variants with increased LBC risk is also still inconclusive; although some studies have been associating CTNNA1 and breast cancer [9,12,13,14], this association remains to be clarified since the subtype of these cancers was not specified. Therefore, breast cancer surveillance should be considered based on personal and family history [2].
The CDH1 and CTNNA1 genes are members of the cadherin and catenin family, respectively, encoding adherens junction proteins, and they are involved in intercellular cell adhesion [15]. The CDH1 gene encodes the cadherin-1, a transmembrane protein, and its extracellular domain establishes interactions with cadherin-1 proteins on an adjacent cell, whereas its cytoplasmic domain binds to the members of the catenin protein family, such as catenin delta-1 and catenin alpha-1 via catenin beta-1, promoting protein stabilization [16]. The CTNNA1 gene encodes the catenin alpha-1 protein, which forms a complex with catenin beta-1 to bind the cytoplasmic domain of cadherin-1 to the actin cytoskeleton by binding directly to the actin filaments [16,17,18]. This protein is essential for the function of the E-cadherin-catenin complex, and the inactivation of catenin proteins and disruption of cytoplasmic catenin-cadherin binding results in the inability of cadherin-1 to establish cell-to-cell adhesion [17]. The involvement of the catenin delta-1 protein in cell adhesion raises the question of its implication in GC predisposition. The catenin delta-1 protein is encoded by the CTNND1 gene, interacts with the juxtamembrane domain of cadherin-1 and regulates the stability of cell–cell adhesion by controlling the retention of cadherin-1 at the cell surface, being crucial to the maintenance and stability of cell adhesion [16]. A single study has been reported that attempted to identify germline variants in the CTNND1 gene and no pathogenic variants were found in the few families tested [19].
The International Gastric Cancer Linkage Consortium (IGCLC), in 1999, defined clinical criteria to select patients for the screening of CDH1 germline variants [20]. Since then, these criteria have been updated several times [21,22] and, in 2020, the IGCLC published updated and less restrictive testing recommendations [2]. Moreover, according to these new guidelines, CTNNA1 testing should be considered when no CDH1 pathogenic variant has been identified [2]. Despite these updates, the guidelines remain unclear if mixed GC, which harbors the two histological components, intestinal and diffuse, should or should not be considered in the HDGC testing criteria [23,24]. In fact, the IGCLC guidelines are very clear about not considering the intestinal type for CDH1/CTNNA1 testing, as this cancer type is not part of the syndrome [2], but they provide no guidance as regards to mixed GC.
We aimed to evaluate the contribution of CTNNA1 and CTNND1 germline variants to HDGC, as well as to compare the frequencies of CDH1 and CTNNA1 (and eventually CTNND1) germline variants in patients/families with DGC with those with mixed GC to evaluate the pertinence of genetic testing of these genes in the latter.
2. Materials and Methods
2.1. Patients and Samples
This study included 212 index cases; 193 patients who were referred to the Genetics Department of the Portuguese Oncology Institute of Porto (IPO Porto) between 2012 and 2021 and 19 patients from the Portuguese Oncology Institute of Lisbon referred to genetic counseling between 2014 and 2019. Of the 212 families, 145 met the IGCLC 2015 or 2020 clinical criteria for HDGC testing (5 of the index patients had LBC and all the others had DGC); among the 145 patients that met the IGCLC 2020 criteria, 26 patients did not fulfill the IGCLC 2015 criteria. Germline CDH1 testing had been performed in these 145 index patients as part of standard clinical genetic testing. The remaining 67 patients were affected with mixed GC and would have met the IGCLC 2015 or 2020 testing criteria if this histological type had been considered for testing in the same way as DGC.
This study was approved by the Ethics Committee of IPO Porto (reference number CES 351/018) and samples for genetic testing were obtained after genetic counseling and informed consent.
Genomic DNA was extracted from peripheral blood samples according to standard protocols.
2.2. Next Generation Sequencing
CDH1 (NM_004360.5) gene analysis was performed in 67 index cases with mixed GC by next-generation sequencing (NGS), using the TruSight Cancer panel (Illumina, Inc., San Diego, CA, USA), with library preparation performed according to the manufacturer’s protocol, and the sequencing reaction was carried out using a standard flow cell in the MiSeq platform (Illumina, Inc.) in 2 × 150 bp paired-end runs. Sequencing alignment and variant analysis were performed using a bioinformatics pipeline previously validated by our group [25]. In brief, alignment and variant calling were carried out using NextGENe (v2.4, Softgenetics, State College, PA, USA). NGS as described above had been used as part of clinical care for the 145 index cases tested for CDH1.
Sequencing of the CTNNA1 (NM_001903.5) and the CTNND1 (NM_001085458.1) genes was performed in 208 cases (with negative CDH1 testing) using a customized QIASeq Targeted DNA Panel (Qiagen, Antwerp, Belgium). Library preparation was performed according to the manufacturer’s instructions and sequencing was carried out using a micro flow cell in the MiSeq Illumina sequencer (Illumina, Inc.) in a 2 × 150 bp paired-end run. Sequencing alignment and variant calling were performed using QIAGEN’s GeneGlobe data analysis portal (Qiagen). The .vcf files were imported to GeneticistAssistantTM software 1.8 (Softgenetics) for variant annotation. All variants with a variant allele frequency (VAF) less than 10%, minor allele frequency (MAF) greater than 1% and intronic variants at more than 12 bp away from exon–intron boundaries were excluded. For CDH1 analysis, variants with a frequency higher than 5% in our in-house database were also excluded. For MAF filtering, data were obtained from the 1000 Genomes Project (1000 G; Based on Project Phase III Data), Genome Aggregation Database (gnomAD) and Exome Aggregation Consortium (ExAC) databases.
2.3. Immunohistochemistry
Catenin alpha-1 protein expression was evaluated by immunohistochemistry (IHC) in section from a representative formalin-fixed and paraffin-embedded tumor tissue block. Briefly, a mouse monoclonal antibody against catenin alpha-1 (clone EP1793Y, Abcam, Cambridge, UK) was incubated at 1/200 for 20 min, and staining was performed with the Leica Bond-III instrument according to the manufacturer’s instructions. Immunostained slides were evaluated by a pathologist. Diffuse gastric tumors known to be negative for CTNNA1 and CDH1 germline variants were used as controls to assess the specificity of the staining.
3. Results
A total of 212 patients were included in this study; 145 of these patients met IGCLC 2020 clinical criteria for HDGC testing and the remaining 67 patients were diagnosed with mixed GC. The CDH1 gene had been analyzed in the 145 patients that fulfilled the IGCLC criteria as part of standard clinical genetic testing prior to this study and CTNNA1 gene sequencing was performed in all patients who had tested negative for CDH1 pathogenic germline variants (Figure 1). Four families have previously been identified with three pathogenic variants in the CDH1 gene (Table 1). Three of these families were already reported [26,27], two harboring the recurrent splicing variant c.1901C>T, which was identified in two women diagnosed with LBC at 38 and 48 years old, and the third was the c.1565+1G>A variant identified in a man with a cleft lip and diagnosed with DGC at 63 years old. Lastly, the variant c.377del p.(Pro126ArgfsTer89) was identified in a woman diagnosed with DGC at 32 years old (Figure 2a). This variant is classified in ClinVar (ID 406616) as pathogenic and has already been reported in the literature [28].
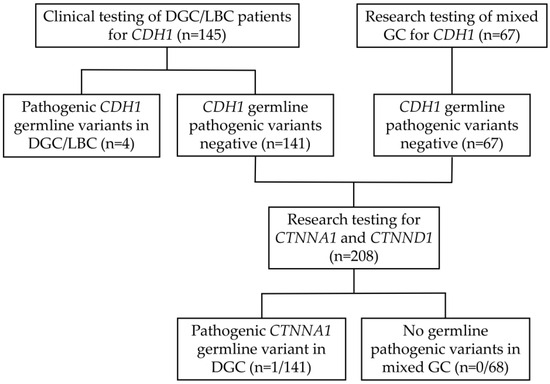
Figure 1.
Flow chart representing patient inclusion and subsequent germline analysis for CDH1, CTNNA1 and CTNND1 genes.

Table 1.
Germline pathogenic variants in the CDH1 and CTNNA1 genes identified in families fulfilling genetic testing criteria.
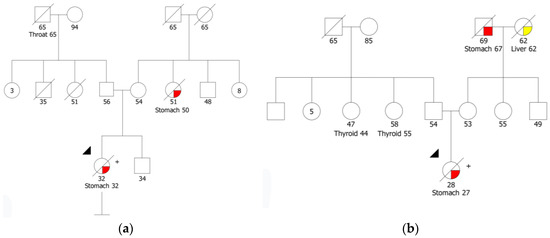
Figure 2.
(a) Pedigree of the HDGC family with the CDH1 variant c.377del p.(Pro126ArgfsTer89); (b) Pedigree of the index patient identified with the CTNNA1 variant c.1426C>T p.(Gln476Ter).
The CTNNA1 germline variant c.1426C>T was found in 1 of 141 (0.7%) patients meeting 2020 IGCLC criteria who had previously tested negative for CDH1 deleterious variants. This is a nonsense variant predicted to lead to premature termination of translation and, consequently, to a truncated protein, p.(Gln476Ter), or to a nonsense-mediated mRNA decay. This variant was identified in a woman diagnosed with a poorly differentiated adenocarcinoma with signet ring cells at age 27 (Figure 2b). There are no CTNNA1 variant classification guidelines; however, Lobo and collaborators classified all variants described in the literature following the CDH1 ACMG/AMP guidelines [29,30]. Following these guidelines, the variant identified in our study is classified as pathogenic, using the criteria PVS1 (nonsense variant), PS4 supporting (one family meeting HDGC criteria) and PM2 (variant absent from population databases). We performed immunohistochemistry (IHC) to assess catenin alpha-1 protein expression in the biopsy sample of the CTNNA1 pathogenic variant carrier. IHC revealed the loss of catenin alpha-1 expression in the gastric adenocarcinoma and preserved catenin alpha-1 expression in the normal epithelial structures (Figure 3d). We also performed IHC in gastric tumors of ten index cases from this series known to be wild-type for the CDH1 and CTNNA1 genes and for whom tumor specimens were available, and catenin alpha-1 expression was retained in both normal and tumor cells (Figure 3b). Regarding family history, the proband’s parents are not affected; the maternal grandfather had stomach cancer at age 67 and the maternal grandmother had liver cancer at 62, both deceased. Two paternal cousins were diagnosed with thyroid cancer at 44 and 55 years old, respectively. To date, it was not possible to perform segregation analysis or test the parents of the proband.
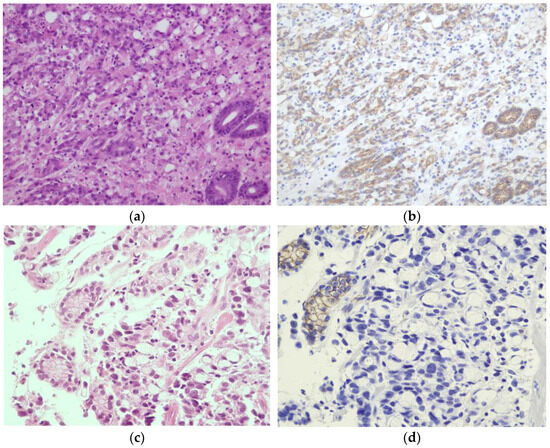
Figure 3.
Microscopic findings showing hematoxylin and eosin (H&E) staining in the left column and immunohistochemistry for catenin alpha-1 in the right column. (a,b) Diffuse gastric cancer in a patient who does not carry CTNNA1 germline variants. Catenin alpha-1 expression is retained in both normal and tumor cells (original magnification, ×200). (c,d) Gastric biopsies of the CTNNA1 c.1426C>T p.(Gln476Ter) variant carrier show signet ring cells infiltrating the mucosa. Catenin alpha-1 was detectable in normal epithelial structures (e.g., the glands of the stomach), but the expression was completely lost in the tumor cells (original magnification, ×400).
None of the 67 cases with mixed GC carried pathogenic variants in either the CDH1 or the CTNNA1 genes. Furthermore, no deleterious CTNND1 variant was detected in the 208 patients without the CDH1 pathogenic germline variants. We identified four missense and two synonymous variants in the CTNND1 gene classified as variants of uncertain significance (VUS) following the ACMG guidelines [29], both in patients with diffuse and mixed gastric cancer subtypes (Table 2).
Table 2.
Variants of uncertain significance identified in the CTNND1 gene.
4. Discussion
Until recently, CDH1 was the only known susceptibility gene associated with HDGC, but, in 2020, the IGCLC recognized CTNNA1 as an HDGC predisposition gene and recommended CTNNA1 testing when no CDH1 pathogenic variant has been identified [2]. On the other hand, the contribution of CTNND1 germline variants for GC predisposition is unknown. Furthermore, the IGCLC still does not clarify if mixed GC with a diffuse component should or should not be considered in the clinical criteria for genetic testing.
Prior to this study and as part of clinical care, the 145 index cases that fulfilled the HDGC testing criteria had been analyzed for CDH1 pathogenic variants, and four families were identified with three pathogenic variants in the CDH1 gene (Table 1). The prevalence of pathogenic CDH1 variants in our patients with HDGC genetic testing criteria is approximately 3% (4/145). The prevalence of CDH1 pathogenic variants in suspected HDGC families varies widely in the literature, which can be mainly explained by the different GC incidences between countries [4]. High-incidence countries, such as Portugal, display a lower frequency of molecularly confirmed HDGC [4,31,32], which can explain the relatively low prevalence of CDH1 deleterious variants we present here. In this study, we analyzed the two candidate genes, CTNNA1 and CTNND1, in the remaining 141 index cases that were negative for CDH1 pathogenic variants. We identified a novel nonsense variant in CTNNA1, c.1426C>T p.(Gln476Ter) in a woman diagnosed with a poorly differentiated adenocarcinoma with signet ring cells at age 27 (Figure 2b). We used the CDH1 ACMG/AMP guidelines to classify this variant as pathogenic, as described by Lobo et al. [29,30]. The IHC showed loss of catenin alpha-1 expression in the tumor cells and preserved catenin alpha-1 expression in the normal gastric epithelium of the CTNNA1 variant carrier. Furthermore, catenin alpha-1 expression was retained in the tumors of ten proband cases, known to be wild-type for CTNNA1 and CDH1 genes, suggesting that catenin alpha-1 expression loss in DGC can be predictive of a CTNNA1 pathogenic variant. Loss or decrease in catenin alpha-1 expression in tumors or biopsy samples of CTNNA1 carriers has also been demonstrated by several authors [3,7,9]. These observations suggest that a second hit inactivating mechanism occurred somatically at the CTNNA1 gene; however, the tumor sample was not available to search for this mechanism. Although the prevalence of CTNNA1 pathogenic variants is not well-established, Lobo et al. suggested that pathogenic variants in CTNNA1 seem to account for less than 2% of the families fulfilling the HDGC testing criteria [11]. The prevalence of pathogenic CTNNA1 variants in our families fulfilling 2020 HDGC testing criteria is approximately 1%, which is similar to the frequency described in the literature [11].
According to the latest HDGC guidelines, CTNNA1 is considered to be a predisposition gene, along with CDH1. Annual endoscopy screening following the Cambridge protocol is recommended in asymptomatic carriers and total gastrectomy should be considered depending on the results of the biopsies and the penetrance of DGC in the family [2]. The risk of GC in carriers of pathogenic CTNNA1 variants is not well defined, but a recent study evaluated DGC risk in CTNNA1 carriers and estimated a cumulative risk of DGC at 80 years of 49–57% [10]. The association of CTNNA1 pathogenic variants with high risk of LBC is also still uncertain; therefore, breast cancer surveillance should be considered based on personal and family history [2].
Beyond HDGC predisposition, the CTNNA1 and CDH1 genes have been associated with macular dystrophy patterned [33,34] and cleft lip/palate and blepharocheilodontic syndrome (BCD) [35,36], respectively. The CTNND1 gene has also been associated with BCD [35,36,37], and the involvement of another cadherin–catenin complex gene in cleft palate and BCD, in addition to its important function in the maintenance and stability of cell adhesion, which makes this gene an ideal candidate for GC predisposition [38]. We therefore analyzed the CTNND1 gene in 208 patients included in this study, but no pathogenic variants were found in the 141 patients with the 2020 IGCLC criteria negative for CDH1 variants. Our negative findings support those of Schuetz et al. [19] in 22 families. However, we identified six VUS in the CTNND1 gene, both in patients with diffuse and mixed gastric cancer subtypes. Here, we report the largest series to date that tested for CTNND1 variants in suspected HDGC patients, but even larger studies will be needed to clarify if the CTNND1 gene has any role in GC predisposition.
A proportion of gastric carcinomas display a mixed phenotype presenting the two histological components, intestinal and diffuse [23,24]. Interestingly, while intestinal-type GC has been completely excluded from the HDGC spectrum [20,21] and the IGCLC guidelines are very clear to not test the patients with this histological type, these guidelines do not indicate whether the mixed type should be considered in the criteria for CDH1 germline variant testing. In this study, we analyzed the CDH1, CTNNA1 and CTNND1 genes in 67 cases affected with mixed GC and did not find any pathogenic CDH1, CTNNA1 or CTNND1 variant. To our knowledge, there are no pathogenic CDH1 variants described in cases with mixed GC in the literature [39,40]. Furthermore, the findings of Machado et al. are in favor of a clonal origin of mixed GC and suggest that an isolated-cell histological component may be originated due to the occurrence of CDH1 somatic variants [41]. Therefore, there is currently no evidence that supports including this tumor type in germline testing of the CDH1 or CTNNA1 genes. However, studies in larger series of mixed GC are necessary to clarify this issue.
5. Conclusions
In this study, a deleterious CTNNA1 germline variant was found in 0.7% (1/141) of patients meeting the 2020 IGCLC criteria, as compared to the rate of 2.8% of CDH1 deleterious variants. Despite the relatively low frequency of HDGC families associated with pathogenic germline variants in CTNNA1, screening for this gene should be conducted for CDH1-negative HDGC families, as recommended in the latest IGCLC guidelines [2]. This will enable the identification of additional CTNNA1 families, allowing more accurate penetrance estimates and a better-defined disease spectrum. The role of CTNND1 variants in inherited gastric cancer predisposition is still unclear.
Author Contributions
Conceptualization, M.R.T. and J.G.; methodology, J.G., C.P., P.P., M.P. (Manuela Pinheiro), C.S., A.P., C.E., A.B., M.P. (Miguel Porto), I.F., P.L., A.R.I. and A.L.C.; formal analysis, J.G., C.P., P.P., M.P. (Manuela Pinheiro), C.S. and A.P.; writing—original draft preparation, J.G.; writing—review and editing, J.G., C.P., P.P., M.P. (Manuela Pinheiro), C.S., A.P., C.E., A.B., M.P. (Miguel Porto), I.F., P.L., A.R.I., A.L.C., C.A., I.C., C.O., J.S. and M.R.T.; supervision, M.R.T.; funding acquisition, M.R.T. All authors have read and agreed to the published version of the manuscript.
Funding
Joana Guerra is a research fellow of the Fundação para a Ciência e Tecnologia (SFRH/BD/138670/2018). Manuela Pinheiro and Miguel Porto are funded by the project “P.CCC: Centro Compreensivo de Cancro do Porto”–NORTE-01-0145-FEDER-072678, supported by the Norte Portugal Regional Operational Programme (NORTE 2020), under the PORTUGAL 2020 Partnership Agreement, through the European Regional Development Fund (ERDF).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Portuguese Oncology Institute of Porto (IPO-Porto) (reference number CES 351/018).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Carneiro, F. Familial and hereditary gastric cancer, an overview. Best Pract. Res. Clin. Gastroenterol. 2022, 58–59, 101800. [Google Scholar] [CrossRef] [PubMed]
- Blair, V.R.; McLeod, M.; Carneiro, F.; Coit, D.G.; D’Addario, J.L.; van Dieren, J.M.; Harris, K.L.; Hoogerbrugge, N.; Oliveira, C.; van der Post, R.S.; et al. Hereditary diffuse gastric cancer: Updated clinical practice guidelines. Lancet Oncol. 2020, 21, e386–e397. [Google Scholar] [CrossRef] [PubMed]
- Majewski, I.J.; Kluijt, I.; Cats, A.; Scerri, T.S.; de Jong, D.; Kluin, R.J.; Hansford, S.; Hogervorst, F.B.; Bosma, A.J.; Hofland, I.; et al. An α-E-catenin (CTNNA1) mutation in hereditary diffuse gastric cancer. J. Pathol. 2013, 229, 621–629. [Google Scholar] [CrossRef] [PubMed]
- Hansford, S.; Kaurah, P.; Li-Chang, H.; Woo, M.; Senz, J.; Pinheiro, H.; Schrader, K.A.; Schaeffer, D.F.; Shumansky, K.; Zogopoulos, G.; et al. Hereditary Diffuse Gastric Cancer Syndrome: CDH1 Mutations and beyond. JAMA Oncol. 2015, 1, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Slavin, T.; Neuhausen, S.L.; Rybak, C.; Solomon, I.; Nehoray, B.; Blazer, K.; Niell-Swiller, M.; Adamson, A.W.; Yuan, Y.C.; Yang, K.; et al. Genetic Gastric Cancer Susceptibility in the International Clinical Cancer Genomics Community Research Network. Cancer Genet. 2017, 216–217, 111–119. [Google Scholar] [CrossRef]
- Weren, R.D.A.; van der Post, R.S.; Vogelaar, I.P.; van Krieken, J.H.; Spruijt, L.; Lubinski, J.; Jakubowska, A.; Teodorczyk, U.; Aalfs, C.M.; van Hest, L.P.; et al. Role of germline aberrations affecting CTNNA1, MAP3K6 and MYD88 in gastric cancer susceptibility. J. Med. Genet. 2018, 55, 669–674. [Google Scholar] [CrossRef] [PubMed]
- Benusiglio, P.R.; Colas, C.; Guillerm, E.; Canard, A.; Delhomelle, H.; Warcoin, M.; Bellanger, J.; Eyries, M.; Zizi, M.; Netter, J.; et al. Clinical implications of CTNNA1 germline mutations in asymptomatic carriers. Gastric Cancer 2019, 22, 899–903. [Google Scholar] [CrossRef]
- Marwitz, T.; Hüneburg, R.; Spier, I.; Lau, J.F.; Kristiansen, G.; Lingohr, P.; Kalff, J.C.; Aretz, S.; Nattermann, J.; Strassburg, C.P. Hereditary Diffuse Gastric Cancer: A Comparative Cohort Study According to Pathogenic Variant Status. Cancers 2020, 12, 3726. [Google Scholar] [CrossRef]
- Clark, D.F.; Michalski, S.T.; Tondon, R.; Nehoray, B.; Ebrahimzadeh, J.; Hughes, S.K.; Soper, E.R.; Domchek, S.M.; Rustgi, A.K.; Pineda-Alvarez, D.; et al. Loss-of-function variants in CTNNA1 detected on multigene panel testing in individuals with gastric or breast cancer. Genet. Med. 2020, 22, 840–846. [Google Scholar] [CrossRef]
- Coudert, M.; Drouet, Y.; Delhomelle, H.; Svrcek, M.; Benusiglio, P.R.; Coulet, F.; Clark, D.F.; Katona, B.W.; van Hest, L.P.; van der Kolk, L.E.; et al. First estimates of diffuse gastric cancer risks for carriers of CTNNA1 germline pathogenic variants. J. Med. Genet. 2022, 59, 1189–1195. [Google Scholar] [CrossRef]
- Lobo, S.; Benusiglio, P.R.; Coulet, F.; Boussemart, L.; Golmard, L.; Spier, I.; Hüneburg, R.; Aretz, S.; Colas, C.; Oliveira, C. Cancer predisposition and germline CTNNA1 variants. Eur. J. Med. Genet. 2021, 64, 104316. [Google Scholar] [CrossRef]
- Felicio, P.S.; Grasel, R.S.; Campacci, N.; de Paula, A.E.; Galvão, H.C.R.; Torrezan, G.T.; Sabato, C.S.; Fernandes, G.C.; Souza, C.P.; Michelli, R.D.; et al. Whole-exome sequencing of non-BRCA1/BRCA2 mutation carrier cases at high-risk for hereditary breast/ovarian cancer. Hum. Mutat. 2021, 42, 290–299. [Google Scholar] [CrossRef]
- Sun, J.; Meng, H.; Yao, L.; Lv, M.; Bai, J.; Zhang, J.; Wang, L.; Ouyang, T.; Li, J.; Wang, T.; et al. Germline Mutations in Cancer Susceptibility Genes in a Large Series of Unselected Breast Cancer Patients. Clin. Cancer Res. 2017, 23, 6113–6119. [Google Scholar] [CrossRef] [PubMed]
- Shirts, B.H.; Casadei, S.; Jacobson, A.L.; Lee, M.K.; Gulsuner, S.; Bennett, R.L.; Miller, M.; Hall, S.A.; Hampel, H.; Hisama, F.M.; et al. Improving performance of multigene panels for genomic analysis of cancer predisposition. Genet. Med. 2016, 18, 974–981. [Google Scholar] [CrossRef]
- van Roy, F. Beyond E-cadherin: Roles of other cadherin superfamily members in cancer. Nat. Rev. Cancer 2014, 14, 121–134. [Google Scholar] [CrossRef] [PubMed]
- Gloushankova, N.A.; Rubtsova, S.N.; Zhitnyak, I.Y. Cadherin-mediated cell-cell interactions in normal and cancer cells. Tissue Barriers 2017, 5, e1356900. [Google Scholar] [CrossRef]
- Kobielak, A.; Fuchs, E. Alpha-catenin: At the junction of intercellular adhesion and actin dynamics. Nat. Rev. Mol. Cell Biol. 2004, 5, 614–625. [Google Scholar] [CrossRef]
- Takeichi, M. Multiple functions of α-catenin beyond cell adhesion regulation. Curr. Opin. Cell Biol. 2018, 54, 24–29. [Google Scholar] [CrossRef]
- Schuetz, J.M.; Leach, S.; Kaurah, P.; Jeyes, J.; Butterfield, Y.; Huntsman, D.; Brooks-Wilson, A.R. Catenin family genes are not commonly mutated in hereditary diffuse gastric cancer. Cancer Epidemiol. Biomark. Prev. 2012, 21, 2272–2274. [Google Scholar] [CrossRef]
- Caldas, C.; Carneiro, F.; Lynch, H.T.; Yokota, J.; Wiesner, G.L.; Powell, S.M.; Lewis, F.R.; Huntsman, D.G.; Pharoah, P.D.; Jankowski, J.A.; et al. Familial gastric cancer: Overview and guidelines for management. J. Med. Genet. 1999, 36, 873–880. [Google Scholar] [PubMed]
- van der Post, R.S.; Vogelaar, I.P.; Carneiro, F.; Guilford, P.; Huntsman, D.; Hoogerbrugge, N.; Caldas, C.; Schreiber, K.E.; Hardwick, R.H.; Ausems, M.G.; et al. Hereditary diffuse gastric cancer: Updated clinical guidelines with an emphasis on germline CDH1 mutation carriers. J. Med. Genet. 2015, 52, 361–374. [Google Scholar] [CrossRef]
- Fitzgerald, R.C.; Hardwick, R.; Huntsman, D.; Carneiro, F.; Guilford, P.; Blair, V.; Chung, D.C.; Norton, J.; Ragunath, K.; Van Krieken, J.H.; et al. Hereditary diffuse gastric cancer: Updated consensus guidelines for clinical management and directions for future research. J. Med. Genet. 2010, 47, 436–444. [Google Scholar] [CrossRef] [PubMed]
- WHO Classification Tumours Editorial Board. (Ed.). WHO Classification of Tumours: Digestive System Tumours, 5th ed.; IARC Press: Lyon, France, 2019. [Google Scholar]
- Lauren, P. The two histological main types of gastric carcinoma: Diffuse and so-called intestinal-type carcinoma. an attempt at a histo-clinical classification. Acta Pathol. Microbiol. Scand. 1965, 64, 31–49. [Google Scholar] [CrossRef] [PubMed]
- Pinto, P.; Paulo, P.; Santos, C.; Rocha, P.; Pinto, C.; Veiga, I.; Pinheiro, M.; Peixoto, A.; Teixeira, M.R. Implementation of next-generation sequencing for molecular diagnosis of hereditary breast and ovarian cancer highlights its genetic heterogeneity. Breast Cancer Res. Treat. 2016, 159, 245–256. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Pelaez, J.; Barbosa-Matos, R.; Lobo, S.; Dias, A.; Garrido, L.; Castedo, S.; Sousa, S.; Pinheiro, H.; Sousa, L.; Monteiro, R.; et al. Genotype-first approach to identify associations between CDH1 germline variants and cancer phenotypes: A multicentre study by the European Reference Network on Genetic Tumour Risk Syndromes. Lancet Oncol. 2023, 24, 91–106. [Google Scholar] [CrossRef]
- Paulo, P.; Pinto, P.; Peixoto, A.; Santos, C.; Pinto, C.; Rocha, P.; Veiga, I.; Soares, G.; Machado, C.; Ramos, F.; et al. Validation of a Next-Generation Sequencing Pipeline for the Molecular Diagnosis of Multiple Inherited Cancer Predisposing Syndromes. J. Mol. Diagn. 2017, 19, 502–513. [Google Scholar] [CrossRef]
- Keller, G.; Vogelsang, H.; Becker, I.; Hutter, J.; Ott, K.; Candidus, S.; Grundei, T.; Becker, K.F.; Mueller, J.; Siewert, J.R.; et al. Diffuse type gastric and lobular breast carcinoma in a familial gastric cancer patient with an E-cadherin germline mutation. Am. J. Pathol. 1999, 155, 337–342. [Google Scholar] [CrossRef]
- Richards, S.; Aziz, N.; Bale, S.; Bick, D.; Das, S.; Gastier-Foster, J.; Grody, W.W.; Hegde, M.; Lyon, E.; Spector, E.; et al. Standards and guidelines for the interpretation of sequence variants: A joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet. Med. 2015, 17, 405–424. [Google Scholar] [CrossRef]
- Lee, K.; Krempely, K.; Roberts, M.E.; Anderson, M.J.; Carneiro, F.; Chao, E.; Dixon, K.; Figueiredo, J.; Ghosh, R.; Huntsman, D.; et al. Specifications of the ACMG/AMP variant curation guidelines for the analysis of germline CDH1 sequence variants. Hum. Mutat. 2018, 39, 1553–1568. [Google Scholar] [CrossRef]
- Corso, G.; Corso, F.; Bellerba, F.; Carneiro, P.; Seixas, S.; Cioffi, A.; La Vecchia, C.; Magnoni, F.; Bonanni, B.; Veronesi, P.; et al. Geographical Distribution of E-cadherin Germline Mutations in the Context of Diffuse Gastric Cancer: A Systematic Review. Cancers 2021, 13, 1269. [Google Scholar] [CrossRef]
- Corso, G.; Marrelli, D.; Pascale, V.; Vindigni, C.; Roviello, F. Frequency of CDH1 germline mutations in gastric carcinoma coming from high- and low-risk areas: Metanalysis and systematic review of the literature. BMC Cancer 2012, 12, 8. [Google Scholar] [CrossRef]
- Saksens, N.T.; Krebs, M.P.; Schoenmaker-Koller, F.E.; Hicks, W.; Yu, M.; Shi, L.; Rowe, L.; Collin, G.B.; Charette, J.R.; Letteboer, S.J.; et al. Mutations in CTNNA1 cause butterfly-shaped pigment dystrophy and perturbed retinal pigment epithelium integrity. Nat. Genet. 2016, 48, 144–151. [Google Scholar] [CrossRef]
- Tanner, A.; Chan, H.W.; Pulido, J.S.; Arno, G.; Ba-Abbad, R.; Jurkute, N.; Robson, A.G.; Egan, C.A.; Knight, H.; Calcagni, A.; et al. Clinical and Genetic Findings in CTNNA1-Associated Macular Pattern Dystrophy. Ophthalmology 2021, 128, 952–955. [Google Scholar] [CrossRef]
- Kievit, A.; Tessadori, F.; Douben, H.; Jordens, I.; Maurice, M.; Hoogeboom, J.; Hennekam, R.; Nampoothiri, S.; Kayserili, H.; Castori, M.; et al. Variants in members of the cadherin-catenin complex, CDH1 and CTNND1, cause blepharocheilodontic syndrome. Eur. J. Hum. Genet. 2018, 26, 210–219. [Google Scholar] [CrossRef] [PubMed]
- Ghoumid, J.; Stichelbout, M.; Jourdain, A.S.; Frenois, F.; Lejeune-Dumoulin, S.; Alex-Cordier, M.P.; Lebrun, M.; Guerreschi, P.; Duquennoy-Martinot, V.; Vinchon, M.; et al. Blepharocheilodontic syndrome is a CDH1 pathway-related disorder due to mutations in CDH1 and CTNND1. Genet. Med. 2017, 19, 1013–1021. [Google Scholar] [CrossRef] [PubMed]
- Cox, L.L.; Cox, T.C.; Moreno Uribe, L.M.; Zhu, Y.; Richter, C.T.; Nidey, N.; Standley, J.M.; Deng, M.; Blue, E.; Chong, J.X.; et al. Mutations in the Epithelial Cadherin-p120-Catenin Complex Cause Mendelian Non-Syndromic Cleft Lip with or without Cleft Palate. Am. J. Hum. Genet. 2018, 102, 1143–1157. [Google Scholar] [CrossRef]
- Benusiglio, P.R. CDH1 germline mutations: Different syndromes, same management? Genet. Med. 2017, 19, 965–966. [Google Scholar] [CrossRef][Green Version]
- Keller, G.; Vogelsang, H.; Becker, I.; Plaschke, S.; Ott, K.; Suriano, G.; Mateus, A.R.; Seruca, R.; Biedermann, K.; Huntsman, D.; et al. Germline mutations of the E-cadherin(CDH1) and TP53 genes, rather than of RUNX3 and HPP1, contribute to genetic predisposition in German gastric cancer patients. J. Med. Genet. 2004, 41, e89. [Google Scholar] [CrossRef] [PubMed]
- van der Post, R.S.; Vogelaar, I.P.; Manders, P.; van der Kolk, L.E.; Cats, A.; van Hest, L.P.; Sijmons, R.; Aalfs, C.M.; Ausems, M.G.; Gómez García, E.B.; et al. Accuracy of Hereditary Diffuse Gastric Cancer Testing Criteria and Outcomes in Patients With a Germline Mutation in CDH1. Gastroenterology 2015, 149, 897–906.e19. [Google Scholar] [CrossRef]
- Machado, J.C.; Soares, P.; Carneiro, F.; Rocha, A.; Beck, S.; Blin, N.; Berx, G.; Sobrinho-Simões, M. E-cadherin gene mutations provide a genetic basis for the phenotypic divergence of mixed gastric carcinomas. Lab. Investig. 1999, 79, 459–465. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).