Simple Summary
Our research focused on understanding how specific patient and clinical factors, present at the diagnosis of advanced renal cell carcinoma (RCC), influence the mortality and recurrence of the disease. We studied patients with advanced RCC from a national Danish database and monitored them over time. Our findings showed that having a positive surgical margin, synchronous metastasis, and poor health status were linked with a higher chance of death and recurrence of the disease. Interestingly, for non-ccRCC patients, having a multidisciplinary team (MDT) discussion during diagnosis was found to lower the risk of death. This suggests that individual clinical details play more significant roles in RCC outcomes than lifestyle factors. Moreover, including MDT discussions in treatment plans may benefit patients.
Abstract
Background: The aim was to investigate whether patient-related or clinical risk factors present at the diagnosis of advanced stage renal cell carcinoma (RCC) had an impact on the overall mortality, cancer-specific mortality, and recurrence risk in a national cohort. Methods: Patients registered with stage III and IV RCC in the Danish Renal Cancer Database (DaRenCa) in 2014–2016 were included in the study and followed up until recurrence or death. We conducted a Cox Proportional Hazard Model to examine the association between several variables and the development of RCC. These variables included BMI, hypertension, smoking status, symptoms at diagnosis, performance status, multidisciplinary team (MDT) discussion, surgical margin, and primary metastasis. Separate analyses were performed for cc-RCC and non-ccRCC patients. Results: In our cohort of 929 patients, 424 individuals died from RCC during the follow-up period, with a median follow-up time of 4.1 (95% CI: 0.8–5.0) years for ccRCC and 2.0 (95% CI: 0.1–5.0) years for non-ccRCC. A multivariate analysis demonstrated that a positive surgical margin (HR 1.53 and 1.43), synchronous metastasis (HR 2.06 and 3.23), and poor performance status (HR 4.73 and 5.27) were significantly associated with a decreased 5-year overall and cancer-specific survival, respectively. Furthermore, a positive surgical margin was associated with a higher risk of recurrence in ccRCC. MDT discussion was found to reduce mortality risk in non-ccRCC. Conclusion: Clinical- and disease-related variables have a greater impact on RCC mortality and recurrence than the selected lifestyle-related factors. The inclusion of MDT discussion in the diagnosis and management of advanced RCC should be further evaluated for its potential to improve patient outcomes.
1. Background
The incidence of renal cell carcinoma (RCC) has increased in recent years, particularly in Western countries, due to the aging population and increasing detection of incidental findings [1,2]. While patients diagnosed with early-stage RCC (stages I and II) have a favourable prognosis, those with advanced RCC (stages III and IV), approximately 15% of which present with metastasis at diagnosis, face a considerably worse outcome [3]. Clinical and pathological factors, such as TNM stage, Fuhrman grade, tumour size, tumour necrosis, and sarcomatoid differentiation, are known to play roles in prognosis and have been used to develop predictive models for survival and recurrence [4].
However, the impact of patient-related factors, such as lifestyle and general health, on prognosis has received less attention. Nevertheless, evidence suggests that factors such as hypertension [5], a poor performance status [6], and the presence of symptoms at diagnosis [5,6] may also play roles in survival. Despite the absence of metastasis at diagnosis, 20–30% of patients still develop recurrence within three years, highlighting the potential role of non-clinical factors in determining risk [3].
This study aims to examine the effect of patient-related and clinical factors on overall and cancer-specific mortality (RQ1) and recurrence (RQ2). Additionally, we will investigate the impact of time to recurrence and the treatment of recurrences on overall and cancer-specific mortality (RQ3).
2. Methods
Data were collected from the Danish Renal Cancer Database (DaRenCa) and medical records for patients diagnosed with stage III and IV renal cell carcinoma between 1 January 2014 and 31 December 2016. Approval and permissions were obtained from the Danish Patient Safety Authority (3-3013-2902/1) and the study is in accordance with the regulations set by the Danish Data Protection Agency (REG-041-2021). The data collection was performed between May 2020 and December 2021.
In addition to the information obtained from DaRenCa, we also utilized data from several other relevant national registries, including the Civil Registration System, the Danish National Patient Registry, the Danish National Pathology Registry, and the Danish Pathology Data Bank [7,8,9,10,11].
2.1. Exposures
Patient-Related Factors
Based on the information from the medical records, we defined the following patient-related factors as body mass index (BMI kg/m2) at diagnosis; hypertension (indicated by one or more active prescriptions for antihypertensive medication); smoking status as current, former, or never smoker; the presence of symptoms at diagnosis (pain, haematuria, weight loss, or other); and performance status categorized as 0, 1–2, or 3–4 using the Eastern Cooperative Oncology Group Performance status.
2.2. Clinical Characteristics and Treatment
The histology of RCC was categorized as clear cell or non-clear cell, T-stage was assigned according to the 2009 TNM classification [12], N-stage was assigned based on malignant lymph nodes in a histological examination, and M-stage was assigned based on pathological or radiological evidence of metastasis at diagnosis or within 120 days of diagnosis. We then defined stage III or IV based on T-stage, N-stage, and M-stage. The Leibovich score was calculated according to the Leibovich score 2003 [13], and a positive surgical margin was defined based on the final histological report. For treatment, we defined interaction with a multidisciplinary team (MDT) before surgery (yes/no), cytoreductive nephrectomy, and lymphadenectomy (yes/no), and the treatment of recurrence was categorized as surgical, oncological, combined, or none.
2.3. Outcomes
We defined the following events as outcomes: death of all causes, cancer-specific death, recurrence based on the information from medical records and computerized tomography scan reports, and death after recurrence.
2.4. Statistical Methods
Risk time was defined from the date of diagnosis until an event of interest or the last follow-up on 31 December 2021. The relationship between exposures of interest and outcomes of interest was evaluated using univariate and multivariate regression models. The Cox proportional hazards model was used to assess the effect of each exposure on overall death and cancer-specific death after one year and five years, as well as the effect of each exposure on recurrence. The models were adjusted for relevant covariates, including demographic information, clinical characteristics, patient health status, and treatment factors. The assumption of proportional hazards was tested using Schoenfeld residuals and the assumption of linearity of the continuous variables was tested by including squared and cubic variables in the Cox proportional hazard model. We took steps to mitigate the risk of immortal time bias by utilizing a time-dependent covariate analysis in the Cox Proportional Hazards Model.
The relationship between time to recurrence and death was evaluated using univariate and multivariate regression models. The Cox proportional hazards model was used to assess the effect of time to recurrence on overall death and cancer-specific death. The models were adjusted for relevant covariates, including demographic information, clinical characteristics, patient health status, and treatment factors. The assumption of proportional hazards was tested using Schoenfeld residuals and the assumption of linearity of the continuous variables was tested by including squared and cubic variables in the Cox model.
Multiple imputations were performed to handle missing data, which accounted for 13% (127 out of 929) of the study population. The method used for imputation was fully conditional specification, which was performed separately for clear cell RCC (ccRCC) and non-clear cell RCC (non-ccRCC) [14]. Body mass index (BMI), Fuhrman grade (only for ccRCC), T-stage, tumour size, smoking status, and performance status were imputed. These variables were imputed in their uncategorized form and later categorized after the imputation. The Leibovich score was calculated after the imputation and before the Cox proportional hazards model. All the variables included in the analysis, as well as the variables of operation status (yes/no), operation type, outcome, and follow-up time, were included in the imputation. In total, 50 imputations were calculated with 500 iterations. The results were combined using Rubin’s rules and reported as hazard ratios (HR) with 95% confidence intervals (CI).
The complete-case Cox proportional hazards model results can be found in the Supplementary Tables S1–S8. The statistical analysis was performed using Stata version 16.1. Figure 1 and Figure 2 display the Kaplan–Meier curves created using R version 4.1.2 and the packages “ggplot2”, “patchwork”, and “prodlim”. Meanwhile, Figure 3, Figure 4, Figure 5 and Figure 6 show other graphical presentations.
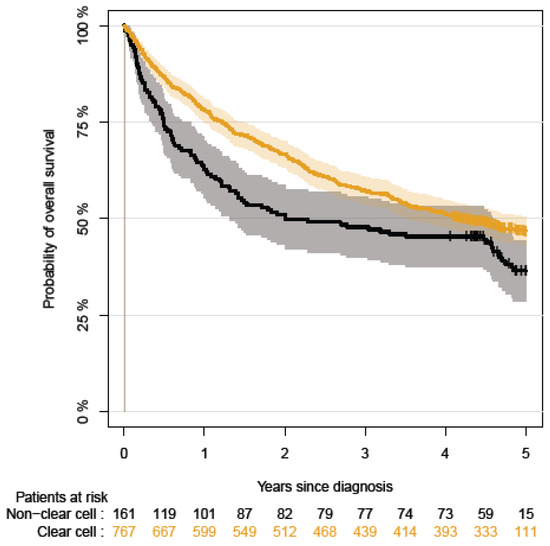
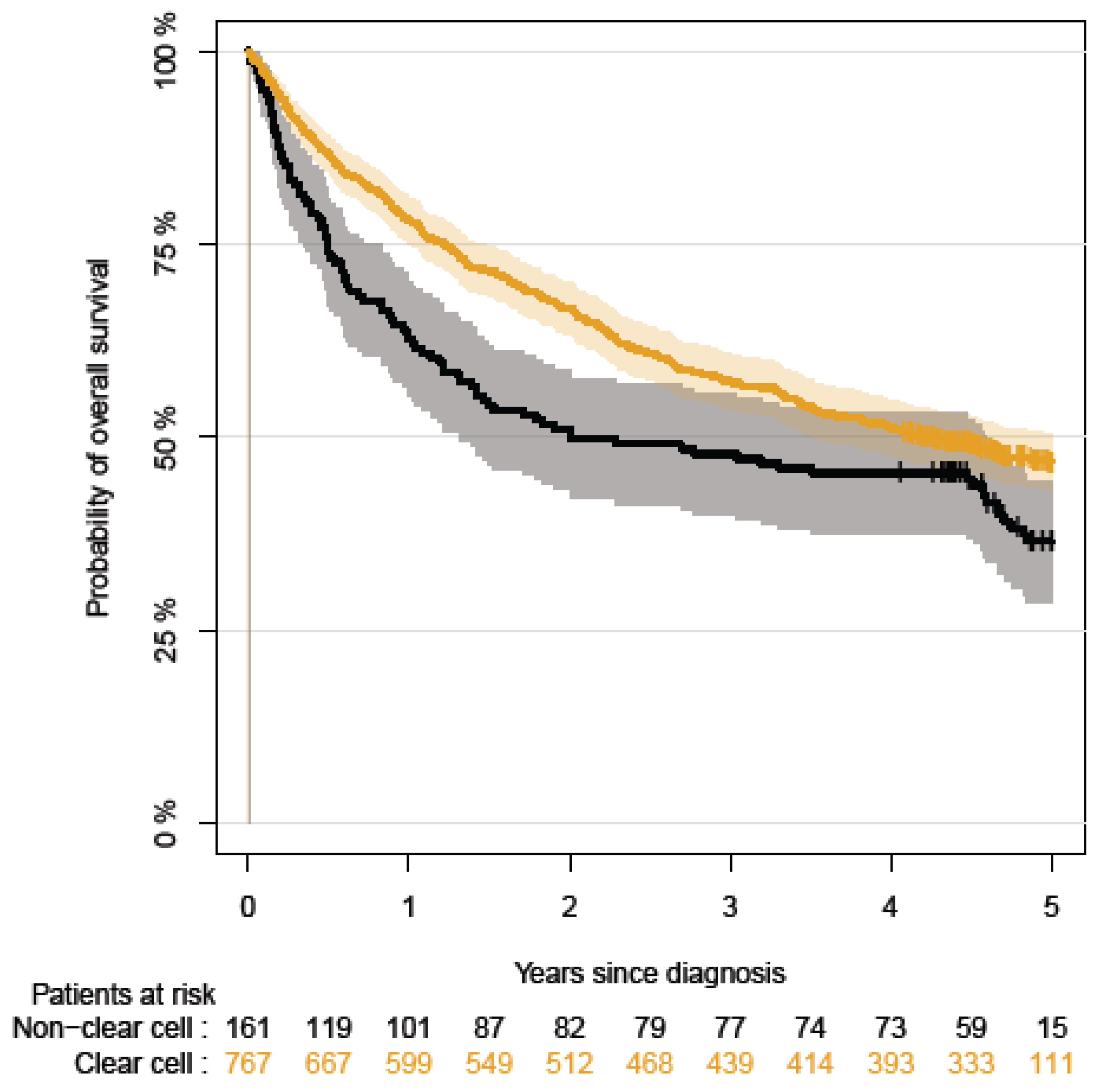
Figure 1.
The five-year overall survival rates for patients with stage III and IV for non-ccRCC.
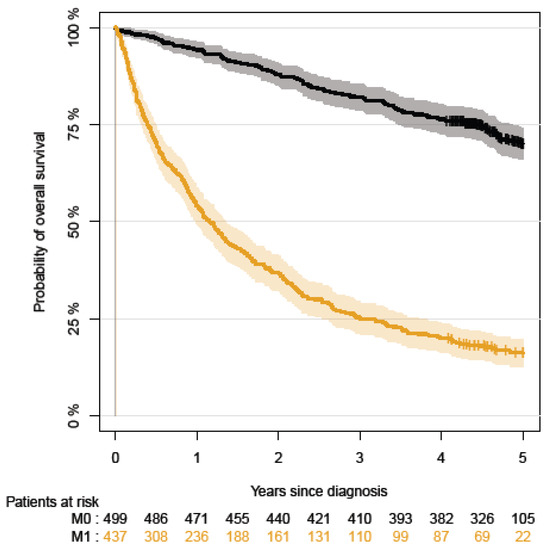
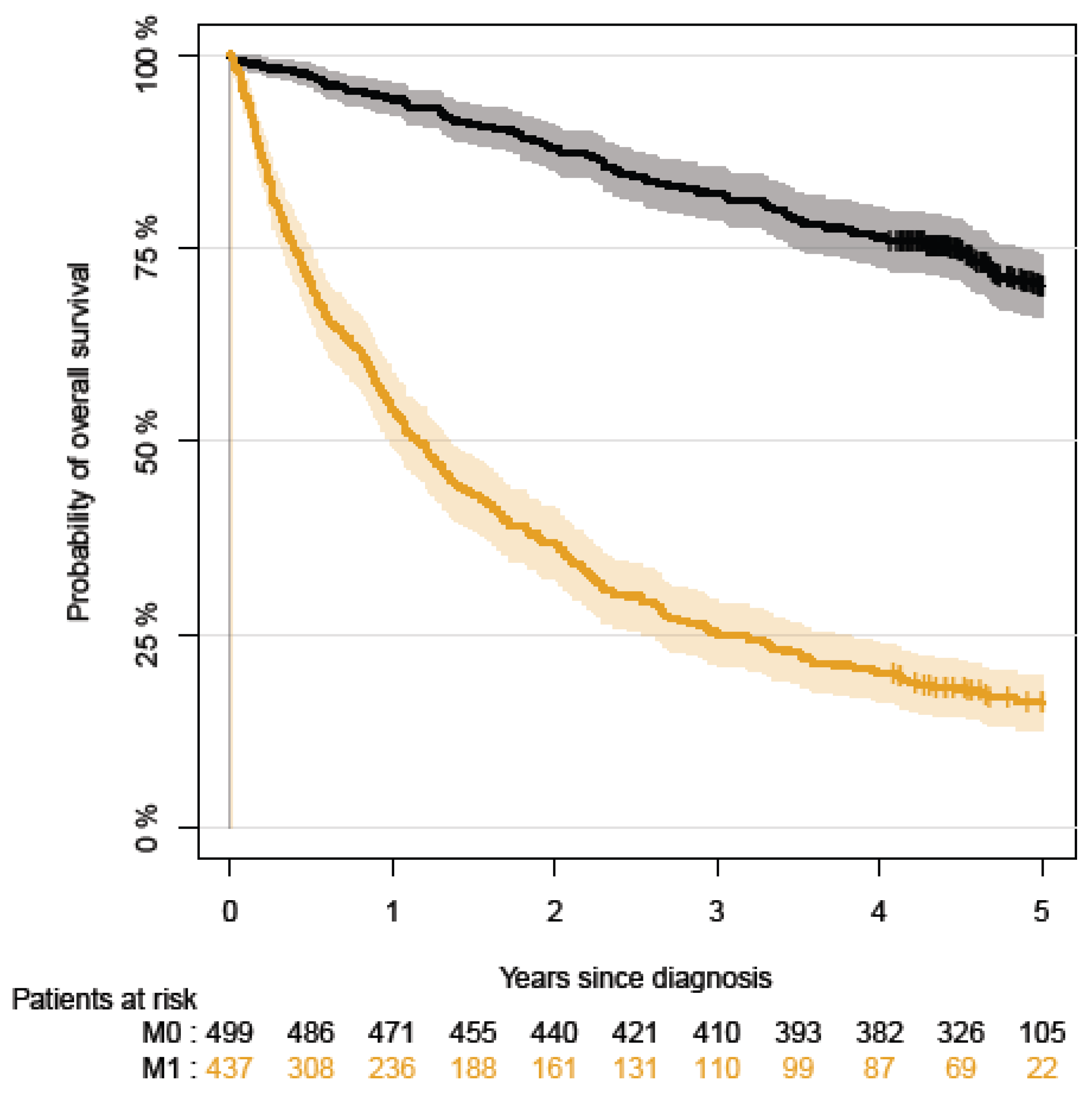
Figure 2.
The five-year overall survival rates for patients with primary metastatic disease versus non-metastatic RCC.
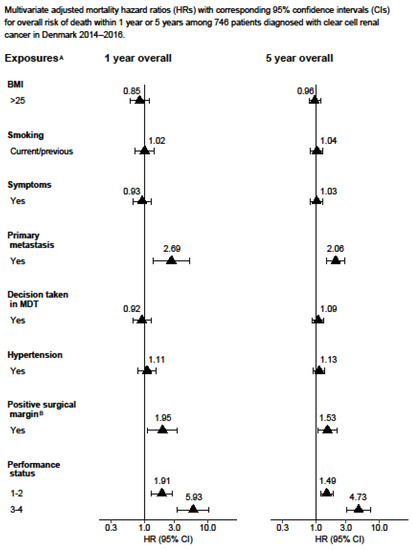
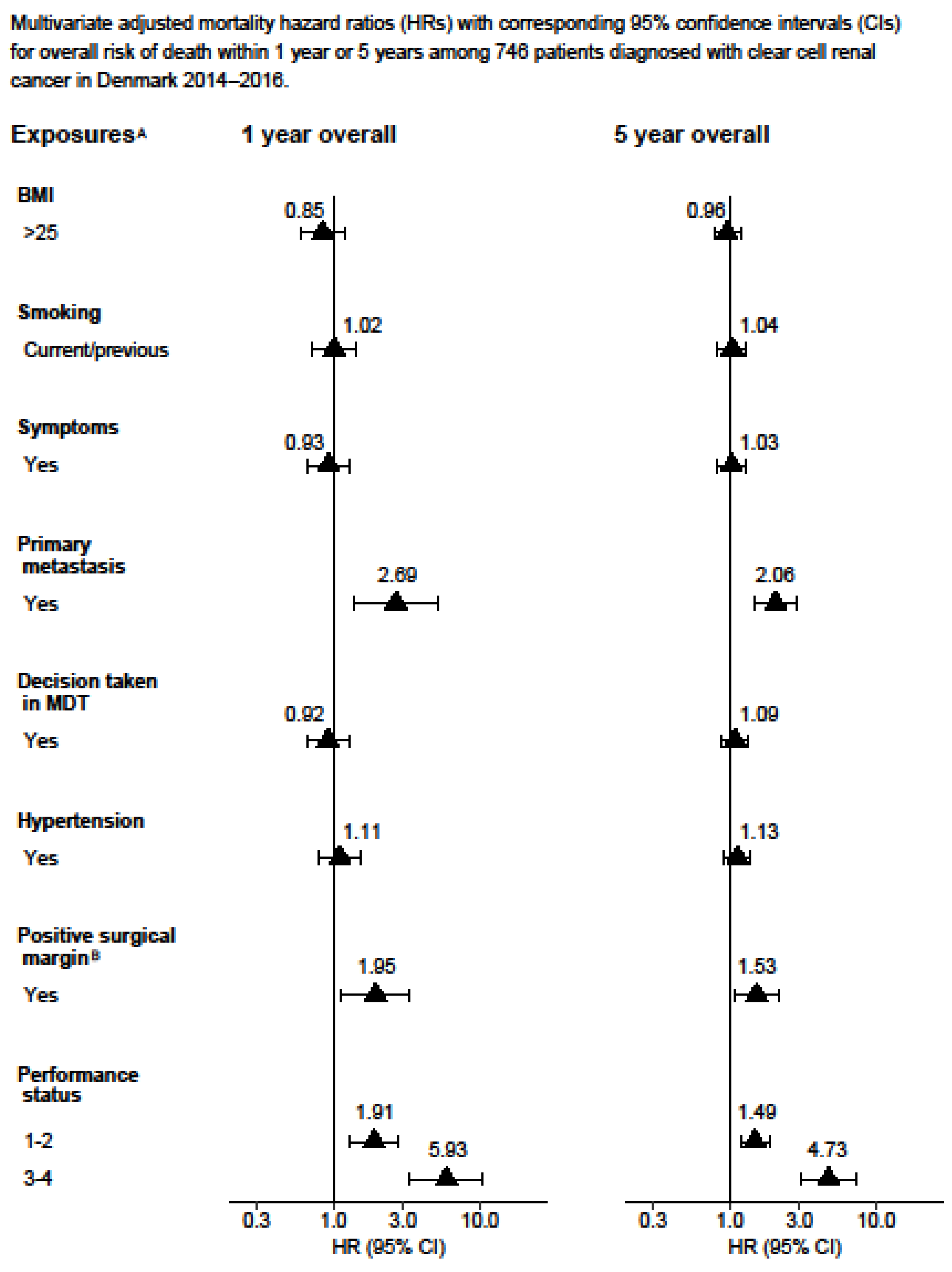
Figure 3.
Multivariate adjusted mortality hazard ratios (HRs) with corresponding 95% confidence intervals (CIs) for overall risk of death within 1 year or 5 years among 746 patients diagnosed with clear cell renal cancer in Denmark 2014–2016. A Adjusted for age, gender, Leibovich score, sarcomatoid, smoking, hypertension, performance status, decision taken in MDT, debulking, and lymphadenectomy. B Also adjusted for partial or radical nephrectomy in model 1.
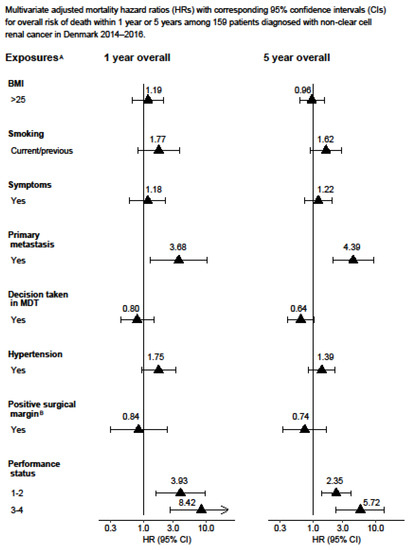
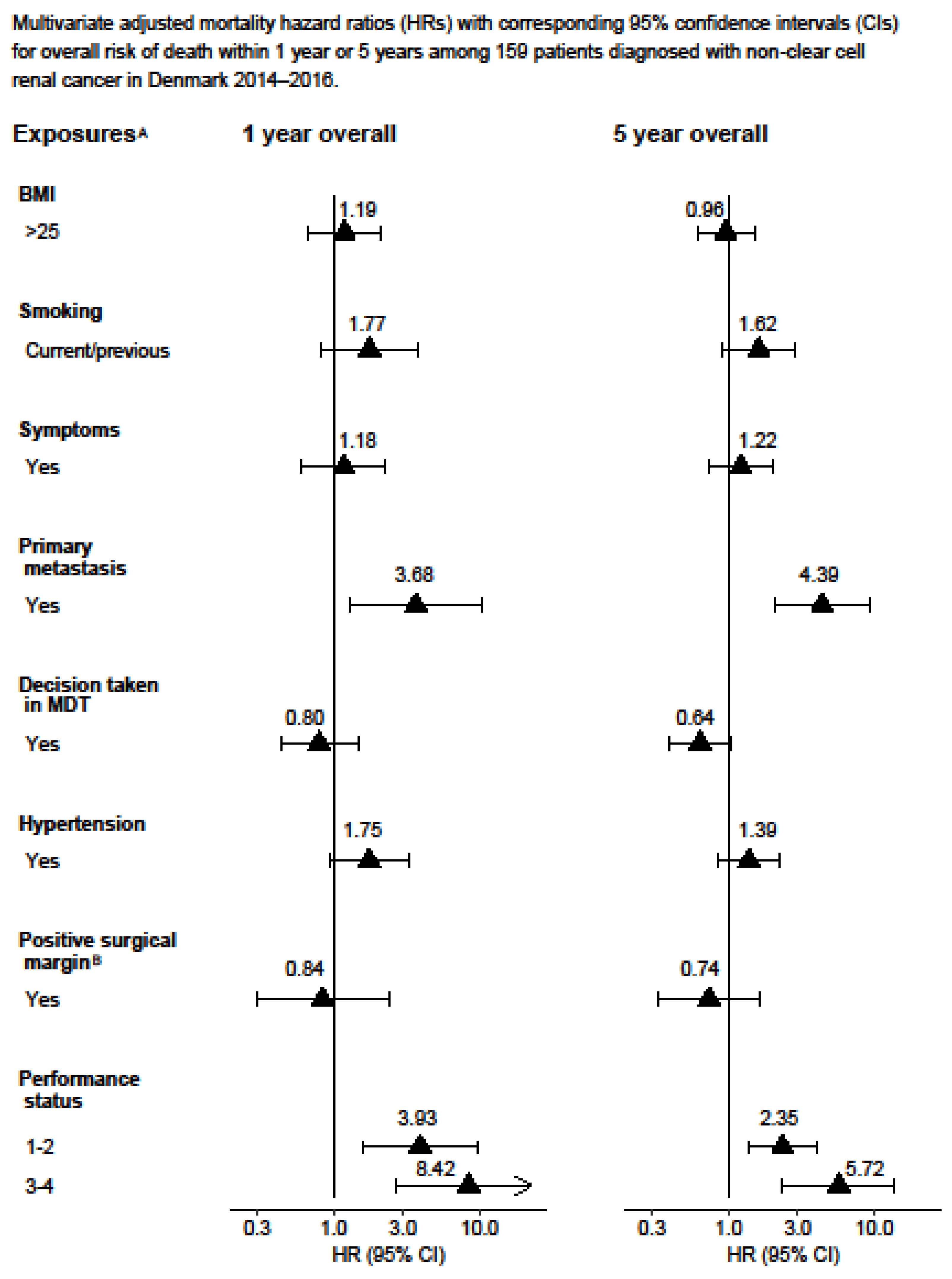
Figure 4.
Multivariate adjusted mortality hazard ratios (HRs) with corresponding 95% confidence intervals (CIs) for overall risk of death within 1 year or 5 years among 159 patients diagnosed with non-clear cell renal cancer in Denmark 2014–2016. A Adjusted for age, T-stage, N-stage, M-stage, size of tumour, hypertension, performance status, and debulking. B Also adjusted for partial or radical nephrectomy.
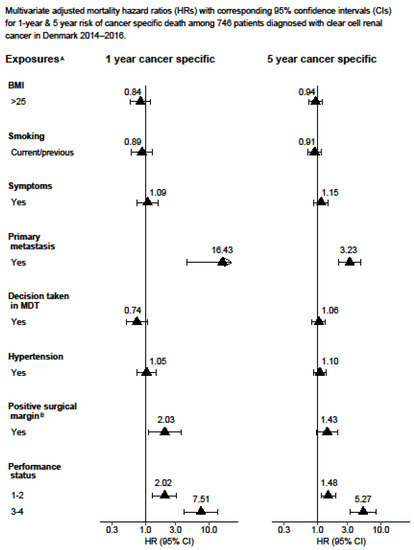
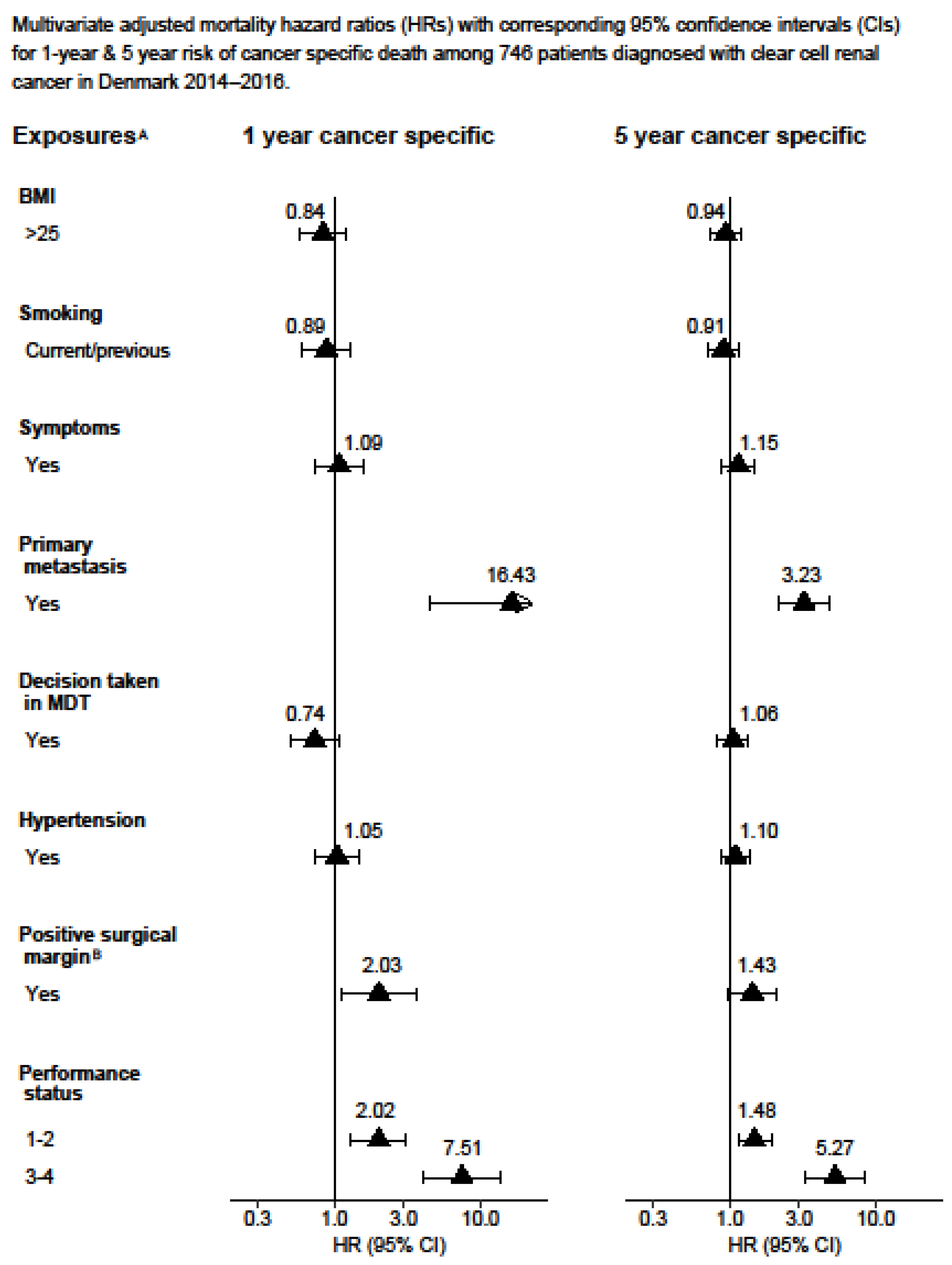
Figure 5.
Multivariate adjusted mortality hazard ratios (HRs) with corresponding 95% confidence intervals (CIs) for 1-year and 5-year risk of cancer-specific death among 746 patients diagnosed with clear cell renal cancer in Denmark 2014–2016. A Model 3: Adjusted for age, gender, Leibovich score, sarcomatoid, smoking, hypertension, performance status, decision taken in MDT, debulking, and lymphadenectomy. B Also adjusted for partial or radical nephrectomy.
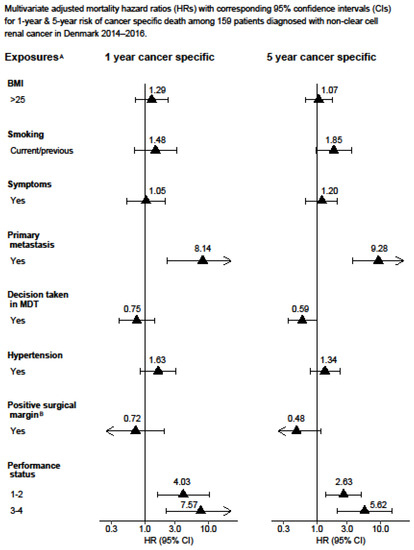
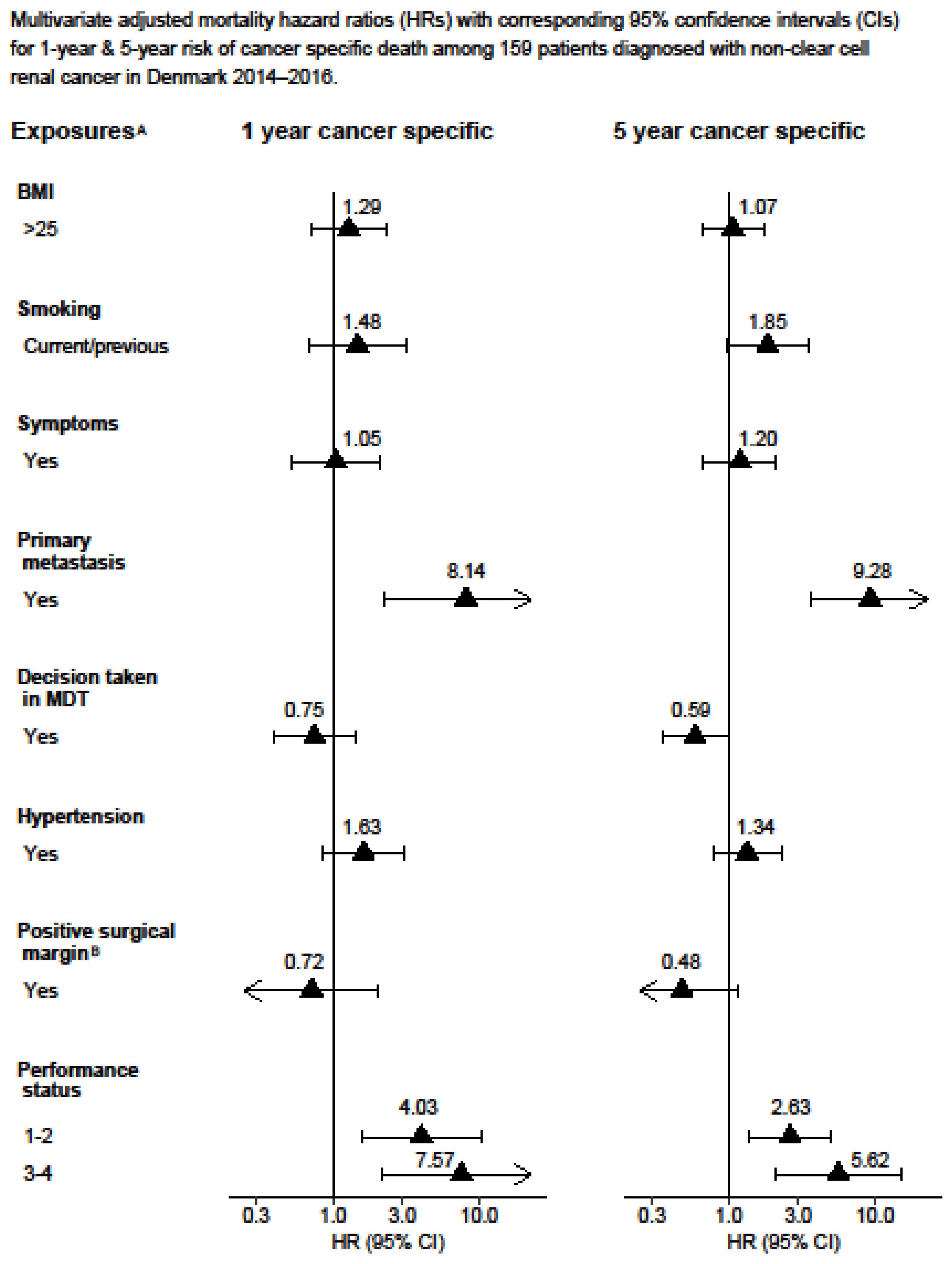
Figure 6.
Multivariate adjusted mortality hazard ratios (HRs) with corresponding 95% confidence intervals (CIs)for 1-year and 5-year risk of cancer-specific death among 159 patients diagnosed with non-clear cell renal cancer in Denmark 2014–2016. A Adjusted for age, T-stage, N-stage, M-stage, size of tumour, sarcomatoid, hypertension, performance status, and debulking. B Adjusted for partial or radical nephrectomy.
3. Results
3.1. Study Population Characteristics
A total of 929 patients diagnosed with stage III (53%) or stage IV (47%) renal cell carcinoma were included in the study. Table 1 displays the demographic and lifestyle characteristics of the study population. Out of the 929 patients, 525 (55%) died from any cause and, among these, 424 (45%) died from renal cell carcinoma. In total, 610 (66%) patients underwent radical nephrectomy and 73 (8%) underwent partial nephrectomy, with 81 (13%) and 13 (18%) patients having a positive surgical margin, respectively. At the time of diagnosis, 517 (56%) patients had hypertension. Some 296 (32%) patients underwent cytoreductive nephrectomy. During the follow-up, 170/494 patients (34%) experienced a recurrence of RCC, for which 31 of these patients (18%) received surgical treatment. The results obtained from the multiple imputations are presented in Figure 3, Figure 4, Figure 5 and Figure 6, whereas the results from the complete-case analysis can be found in Supplementary Tables S1, S2, and S4. In the complete-case analysis, smoking demonstrated a negative effect on clear cell renal cell carcinoma (ccRCC). In contrast, hypertension was associated with higher mortality rates for both ccRCC and non-ccRCC, although this association was not observed in the multiple imputation analysis. Furthermore, a body mass index (BMI) greater than 25 kg/m2 was found to significantly reduce overall and cancer-specific mortality in the univariate analysis for ccRCC, but not for non-ccRCC. There was no discernible difference in mortality between current and former smokers.

Table 1.
Baseline characteristics of 929 patients diagnosed with stage III or IV renal cancer in Denmark 2014–2016.
3.2. Overall Mortality
The median follow-up time until overall death for ccRCC was 4.13 (95% CI: 0.8–5.0) years and 2.00 (95% CI: 0.1–5.0) years for non-ccRCC. The five-year overall survival rates for patients with stage III and IV were 47% for ccRCC and 36% for non-ccRCC (Figure 1).
The five-year overall survival rates for patients with primary metastatic disease versus non-metastatic RCC were 16% and 70%, respectively (Figure 2).
In the fully adjusted model, the presence of primary metastasis (HR 2.69 and 2.06), a positive surgical margin (HR 1.95 and 1.53), and a poor performance status (HR 5.93 and 4.73) significantly increased the one-year and five-year overall mortality for ccRCC, respectively (Figure 3).
Similarly, a poor performance status and primary metastasis were associated with an increased risk of death of all causes in patients with non-ccRCC after one year and five years (Figure 4).
3.3. Cancer-Specific Mortality
In the fully adjusted model, primary metastasis (HR 16.43 and 3.23), a positive surgical margin (HR 2.03 and 1.43) (with marginal significance for five-year risk of death), and a poor performance status (HR 7.51 and 5.27) significantly increased the one-year and five-year ccRCC-specific mortality, respectively (Figure 5).
Additionally, the presence of primary metastasis and a poor performance status increased non-ccRCC-specific mortality. Meanwhile, the decision taken by the multidisciplinary team was associated with a lower five-year non-ccRCC-specific mortality (Figure 6).
3.4. Recurrence
A total of 170 (18%) patients, comprising 147 with ccRCC and 23 with non-ccRCC, experienced recurrence. The median time to recurrence was 2.66 years for ccRCC and 1.44 years for non-ccRCC. In the multivariate analysis, a positive surgical margin was found to significantly increase the risk of recurrence in ccRCC patients, with a hazard ratio of 2.40 (95% confidence interval 1.45–3.94) (Table 2).
Table 2.
Multivariate adjusted hazard ratios (HRs) with corresponding 95% confidence intervals (CIs) for risk of recurrence among 386 clear cell patients diagnosed with clear cell renal cancer without primary metastasis in Denmark 2014–2016.
3.5. Mortality after Recurrence
Out of the 147 ccRCC patients who experienced recurrence, 71 died. The median time to death after recurrence was 2.2 years. The results showed that patients who experienced recurrence more than one year after the initial diagnosis had a lower risk of both overall and cancer-specific mortality compared to patients who experienced recurrence within the first year. Patients who experienced recurrence between 2 and 3 years after the initial diagnosis had the lowest risk of both cancer-specific (HR 0.22; 95% CI: 0.09–0.57) and all-cause mortality (HR 0.22; 95% CI: 0.09–0.54) in comparison to patients who experienced recurrence within the first year after diagnosis (Table 3). On the other hand, patients who received only oncological treatment for recurrent RCC had a higher risk of both overall (HR 5.93; 95% CI: 1.78–19.81) and cancer-specific (HR 8.76; 95% CI: 2.05–37.51) mortality compared to those who received surgical treatment for recurrent RCC.
Table 3.
Multivariate adjusted overall mortality and cancer-specific hazard ratios (HRs) with corresponding 95% confidence intervals (CIs) among 141 patients diagnosed with recurrent clear cell renal cancer in Denmark 2014–2016.
4. Discussion
In this nationwide cohort of Danish stage III and IV RCC patients, we did not find any significant associations between lifestyle factors and worse outcomes. These findings raise the question of the broader implications of lifestyle factors in RCC and whether they may play more nuanced roles than what is reflected in clinical outcomes. However, our study trended towards smoking having a negative effect on ccRCC, although this result was not statistically significant. This is consistent with the wider understanding of smoking’s potential role in carcinogenesis and disease progression in various other cancers [15,16]. Future research might consider larger cohorts or meta-analyses to reach a more definitive conclusion on this. Hypertension was associated with a greater mortality for ccRCC and non-ccRCC in the complete-case analysis, but this relationship was not significant in the multiple imputation (MI) analysis. The effect of hypertension on mortality in RCC has been inconsistent in the literature [5,17]. A BMI greater than 25 kg/m2 was associated with a significant reduction in overall and cancer-specific mortality in our univariate analysis for ccRCC, but not in that for non-ccRCC.
Our nationwide Danish cohort contrasts with the Brazilian Oncology Group study [18], which explored obesity and its association with immune checkpoint inhibitors’ (ICI) efficacy. While they found no significant improvement in overall survival among high-BMI patients treated with ICI, our findings demonstrated a significant reduction in overall and cancer-specific mortality in ccRCC patients with a BMI greater than 25 kg/m2. Both studies, however, indicate the complexity surrounding the role of BMI in cancer outcomes. Additionally, the inconsistent effects of hypertension on RCC mortality, as observed in our study, highlight the disparities and nuances in patient populations and the need for further investigation.
Consistent with previous research, our study found that a worse performance status was significantly associated with higher cancer-specific and overall mortality in both ccRCC and non-ccRCC patients [19]. However, we did not find a significant association between the presence of symptoms at diagnosis and mortality.
Primary metastasis was strongly associated with an increased mortality, particularly in non-ccRCC, where an eight-fold increase in risk was observed. Patients with primary metastatic non-ccRCC have previously been found to have a significantly shorter time-to-treatment-failure and lower overall survival compared to patients with ccRCC [20].
In this study, the presence of primary metastasis and a poor performance status increased the cancer-specific mortality for both ccRCC and non-ccRCC. When the treatment decision was taken by the MDT, it was associated with a lower five-year cancer-specific mortality in non-ccRCC, but not ccRCC. The relationship between MDT discussion and mortality in cancer patients has been debated, with one study showing no positive benefit for metastatic RCC after an adjustment for clinical factors, and other studies showing no significant relationship for other cancer types [21,22].
Regarding mortality after recurrence, Brookman-May and colleagues found that a recurrence occurring more than a year after primary surgery conferred a 21% lower risk of cancer-specific mortality, similar to our findings [23]. Our results confirmed that receiving both oncological treatment and surgery was associated with a lower mortality risk compared to only receiving oncological treatment, even after an adjustment for factors such as Leibovich score, age, number of metastasis sites, and performance status [24].
Strengths and Limitations
This study has several strengths, including its nationwide, multicentre design and that the data were extracted from both medical records and registries, enabling the analysis of several important variables. The application of multiple imputations (MI) with a high number of imputations allowed for the efficient use of the cohort. Some differences were noted between the MI and complete-case analysis, but we can assume that values were missing at random (MAR), which makes the MI less biased than the complete-case analysis [25].
Our study, though comprehensive in its approach, does come with some inherent limitations that should be acknowledged when interpreting the results. The retrospective nature of the design, while valuable for understanding historical data patterns, can introduce potential biases, particularly in terms of patient selection and data recording. Consequently, causality cannot be ascertained from our findings. The omission of an adjustment for socioeconomic position might limit the granularity of our results. Socioeconomic factors are known to influence health outcomes, access to care, and adherence to treatments. Thus, not adjusting for them might have potentially masked or skewed some associations. The absence of adjustments for immune checkpoint inhibitor treatments also stands as a significant limitation. Given the rising prominence of these treatments in modern oncology, they can play a pivotal role in determining patient outcomes. Without accounting for them, there could be an inadvertent oversight in understanding the therapeutic implications. Our dataset contained fewer patients with non-ccRCC. This imbalance might lead to the potential of over-adjustment, making some of the analyses less generalizable to the broader non-ccRCC patient population. Lastly, the non-availability of specific biomarkers poses a limitation. In the era of precision medicine, biomarkers can provide in-depth insights into disease prognoses, therapeutic response, and patient outcomes. Their absence in our study might hinder the comprehensive understanding of RCC in the context of the examined lifestyle factors.
5. Conclusions
The results of this study suggest that patient-related factors, such as lifestyle, play a less significant role in determining the outcomes of advanced RCC compared to clinical- and disease-related variables. The results also highlight the potential benefits of considering the involvement of multidisciplinary teams during the diagnostic process. Further research is needed to better understand the impact of lifestyle factors on RCC outcomes and explore the differential effects of these factors in terms of cancer stage, particularly in non-clear cell RCC.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/cancers15184488/s1, Table S1: Complete-case analysis of multivariate adjusted mortality hazard ratios (HRs) with corresponding 95% confidence intervals (CIs) for overall risk of death within 1 year or 5 years among 646 patients diagnosed with clear cell renal cancer in Denmark 2014–2016.; Table S2: Complete-case analysis of multivariate adjusted mortality hazard ratios (HRs) with corresponding 95% confidence intervals (CIs) for overall risk of death within 1 year or 5 years among 141 patients diagnosed with non-clear cell renal cancer in Denmark 2014–2016. Table S3: Complete-case analysis of multivariate adjusted mortality hazard ratios (HRs) with corresponding 95% confidence intervals (CIs) for 1-year and 5-year risk of cancer specific death among 661 patients diagnosed with clear cell renal cancer in Denmark 2014–2016. Table S4: Complete-case analysis of multivariate adjusted mortality hazard ratios (HRs) with corresponding 95% confidence intervals (CIs) for 1-year and 5-year risk of cancer specific death among 141 patients diagnosed with non-clear cell renal cancer in Denmark 2014–2016. Table S5: MI analysis of multivariate adjusted mortality hazard ratios (HRs) with corresponding 95% confidence intervals (CIs) for overall risk of death within 1 year or 5 years among 746 patients diagnosed with clear cell renal cancer in Denmark 2014–2016. Table S6: MI analysis of multivariate adjusted mortality hazard ratios (HRs) with corresponding 95% confidence intervals (CIs) for overall risk of death within 1 year or 5 years among 159 patients diagnosed with non-clear cell renal cancer in Denmark 2014–2016. Table S7: MI analysis of multivariate adjusted mortality hazard ratios (HRs) with corresponding 95% confidence intervals (CIs) for 1-year and 5-year risk of cancer specific death among 746 patients diagnosed with clear cell renal cancer in Denmark 2014–2016. Table S8: MI analysis of multivariate adjusted mortality hazard ratios (HRs) with corresponding 95% confidence intervals (CIs) for 1-year and 5-year risk of cancer specific death among 159 patients diagnosed with non-clear cell renal cancer in Denmark 2014–2016.
Author Contributions
Conceptualization, N.A., F.E.E., N.V.J., N.F., L.L., F.D. and S.O.D.; methodology, N.A., F.E.E., J.C., N.V.J., N.F., L.L. and F.D.; formal analysis, N.A. and J.C.; investigation, F.E.E.; data curation, N.A., F.E.E., N.N., K.S.S.M., S.S.A., L.G. and J.C.; writing—original draft preparation, N.A. and S.O.D.; writing—review and editing, N.A., F.E.E., N.N., K.S.S.M., S.S.A., L.G., J.C., N.V.J., N.F., L.L., F.D. and S.O.D.; supervision, N.V.J., N.F., L.L. and F.D. All authors have read and agreed to the published version of the manuscript.
Funding
This study received financial support from the Danish Cancer Society.
Institutional Review Board Statement
All methods were carried out in accordance with relevant guidelines and regulations. The study was approved by the Danish Patients Data Authority (3-3013-2056/1) and the Data Protection Agency (EMN-2021-03452). The need for informed consent was waived by the ethics committee/Institutional Review Board of Danish Patients Data Authority (3-3013-2056/1).
Informed Consent Statement
Not Applicable.
Data Availability Statement
All data generated or analysed during this study are included in this published article and its supplementary tables.
Conflicts of Interest
The authors have stated that they have no conflict of interest associated with this study.
Abbreviations
| Renal cell carcinoma | RCC |
| Examine the effect of patient-related and clinical factors on overall and cancer-specific mortality | RQ1 |
| Examine the effect of patient-related and clinical factors on recurrence | RQ2 |
| Investigate the impact of time to recurrence and the treatment of recurrences on overall and cancer-specific mortality | RQ3 |
| Danish Renal Cancer Database | DaRenCa |
| Body Mass Index | BMI |
| Multidisciplinary team | MDT |
| Clear cell RCC | ccRCC |
| Non-clear cell RCC | non-ccRCC |
| Hazard ratios | HR |
| Confidence intervals | CI |
| Multiple imputations | MI |
| Missing at random | MAR |
References
- Capitanio, U.; Montorsi, F. Renal cancer. Lancet 2016, 387, 894–906. [Google Scholar] [CrossRef]
- Næraa, S.H.; Bersang, A.B.; Dahl, C.; Subhi, Y.; Azawi, N. Burden of renal cancer in Nordic countries. Scand. J. Urol. 2019, 53, 177–184. [Google Scholar] [CrossRef]
- Petersen, A.; Søgaard, M.; Mehnert, F.; Larsen, E.H.; Donskov, F.; Azawi, N.; Kromann-Andersen, B. The database of the Danish Renal Cancer Group. Clin. Epidemiol. 2016, 8, 725–729. [Google Scholar] [CrossRef]
- Volpe, A.; Patard, J.J. Prognostic factors in renal cell carcinoma. World J. Urol. 2010, 28, 319–327. [Google Scholar] [CrossRef]
- Kocher, N.J.; Rjepaj, C.; Robyak, H.; Lehman, E.; Raman, J.D. Hypertension is the primary component of metabolic syndrome associated with pathologic features of kidney cancer. World J. Urol. 2017, 35, 67–72. [Google Scholar] [CrossRef]
- Zisman, A.; Pantuck, A.J.; Dorey, F.; Said, J.W.; Shvarts, O.; Quintana, D.; Gitlitz, B.J.; deKernion, J.B.; Figlin, R.A.; Belldegrun, A.S. Improved prognostication of renal cell carcinoma using an integrated staging system. J. Clin. Oncol. 2001, 19, 1649–1657. [Google Scholar] [CrossRef]
- Schmidt, M.; Pedersen, L.; Sørensen, H.T. The Danish Civil Registration System as a tool in epidemiology. Eur. J. Epidemiol. 2014, 29, 541–549. [Google Scholar] [CrossRef]
- Schmidt, M.; Schmidt, S.A.J.; Sandegaard, J.L.; Ehrenstein, V.; Pedersen, L.; Sørensen, H.T. The Danish National Patient Registry: A review of content, data quality, and research potential. Clin. Epidemiol. 2015, 7, 449–490. [Google Scholar] [CrossRef]
- Erichsen, R.; Lash, T.L.; Hamilton-Dutoit, S.J.; Bjerregaard, B.; Vyberg, M.; Pedersen, L. Existing data sources for clinical epidemiology: The Danish National Pathology Registry and Data Bank. Clin. Epidemiol. 2010, 2, 51–56. [Google Scholar] [CrossRef]
- Gjerstorff, M.L. The Danish Cancer Registry. Scand. J. Public Health 2011, 39, 42–45. [Google Scholar] [CrossRef]
- Helweg-Larsen, K. The Danish Register of Causes of Death. Scand. J. Public Health 2011, 39, 26–29. [Google Scholar] [CrossRef]
- Moch, H.; Artibani, W.; Delahunt, B.; Ficarra, V.; Knuechel, R.; Montorsi, F.; Patard, J.-J.; Stief, C.G.; Sulser, T.; Wild, P.J. Reassessing the current UICC/AJCC TNM staging for renal cell carcinoma. Eur. Urol. 2009, 56, 636–643. [Google Scholar] [CrossRef]
- Leibovich, B.C.; Blute, M.L.; Cheville, J.C.; Lohse, C.M.; Frank, I.; Kwon, E.D.; Weaver, A.L.; Parker, A.S.; Zincke, H. Prediction of progression after radical nephrectomy for patients with clear cell renal cell carcinoma. Cancer 2003, 97, 1663–1671. [Google Scholar] [CrossRef]
- White, I.R.; Royston, P.; Wood, A.M. Multiple imputation using chained equations: Issues and guidance for practice. Stat. Med. 2011, 30, 377–399. [Google Scholar] [CrossRef]
- Eckel-Passow, J.E.; Serie, D.J.; Bot, B.M.; Joseph, R.W.; Cheville, J.C.; Parker, A.S. ANKS1B is a smoking-related molecular alteration in clear cell renal cell carcinoma. BMC Urol. 2014, 14, 14. [Google Scholar] [CrossRef]
- Kumar, R.; Matulewicz, R.; Mari, A.; Moschini, M.; Ghodoussipour, S.; Pradere, B.; Rink, M.; Autorino, R.; Desai, M.M.; Gill, I.; et al. Impact of smoking on urologic cancers: A snapshot of current evidence. World J. Urol. 2023, 41, 1473–1479. [Google Scholar] [CrossRef]
- Eskelinen, T.J.; Kotsar, A.; Tammela, T.L.J.; Murtola, T.J. Components of metabolic syndrome and prognosis of renal cell cancer. Scand. J. Urol. 2017, 51, 435–441. [Google Scholar] [CrossRef]
- Moreira, R.B.; Fernandes, M.; Monteiro, M.R.; Luiz, F.M.A.; Silva, E.S.; de Mello Andrade, P.; Pinto, M.B.; Lima, L.; Silva, A.; Nunez, J.; et al. Body mass index and immune checkpoint inhibitor efficacy in metastatic cancer patients: A Brazilian retrospective study. Front. Urol. 2022, 2, 1069045. [Google Scholar] [CrossRef]
- Choueiri, T.K.; Rini, B.I.; Garcia, J.A.; Baz, R.C.; Abou-Jawde, R.M.; Thakkar, S.G.; Elson, P.; Mekhail, T.M.; Zhou, M.; Bukowski, R.M. Prognostic factors associated with long-term survival in previously untreated metastatic renal cell carcinoma. Ann. Oncol. 2007, 18, 249–255. [Google Scholar] [CrossRef]
- Kroeger, N.; Xie, W.; Lee, J.-L.; Bjarnason, G.A.; Knox, J.J.; MacKenzie, M.J.; Wood, L.; Srinivas, S.; Vaishamayan, U.N.; Rha, S.-Y.; et al. Metastatic non-clear cell renal cell carcinoma treated with targeted therapy agents: Characterization of survival outcome and application of the International mRCC Database Consortium criteria: Outcome and Prognostication in nccRCC. Cancer 2013, 119, 2999–3006. [Google Scholar] [CrossRef]
- Liu, W.K.; Lam, J.M.; Butters, T.; Grant, M.; Jackson-Spence, F.; Bex, A.; Powles, T.; Szabados, B. Cytoreductive nephrectomy in metastatic renal cell carcinoma: Outcome of patients treated with a multidisciplinary, algorithm-driven approach. World J. Urol. 2020, 38, 3199–3205. [Google Scholar] [CrossRef] [PubMed]
- Pillay, B.; Wootten, A.C.; Crowe, H.; Corcoran, N.; Tran, B.; Bowden, P.; Crowe, J.; Costello, A.J. The impact of multidisciplinary team meetings on patient assessment, management and outcomes in oncology settings: A systematic review of the literature. Cancer Treat. Rev. 2016, 42, 56–72. [Google Scholar] [CrossRef]
- Brookman-May, S.D.; May, M.; Shariat, S.F.; Novara, G.; Zigeuner, R.; Cindolo, L.; De Cobelli, O.; De Nunzio, C.; Pahernik, S.; Wirth, M.P.; et al. Time to recurrence is a significant predictor of cancer-specific survival after recurrence in patients with recurrent renal cell carcinoma—Results from a comprehensive multi-centre database (CORONA/SATURN-Project): Time to recurrence as predictor for CSS after recurrence in patients with RCC. BJU Int. 2013, 112, 909–916. [Google Scholar] [CrossRef]
- Lam, J.S.; Shvarts, O.; Leppert, J.T.; Pantuck, A.J.; Figlin, R.A.; Belldegrun, A.S. Postoperative surveillance protocol for patients with localized and locally advanced renal cell carcinoma based on a validated prognostic nomogram and risk group stratification system. J. Urol. 2005, 174, 466–472. [Google Scholar] [CrossRef] [PubMed]
- Hughes, R.A.; Heron, J.; Sterne, J.A.C.; Tilling, K. Accounting for missing data in statistical analyses: Multiple imputation is not always the answer. Int. J. Epidemiol. 2019, 48, 1294–1304. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).