Simple Summary
Hepatocellular carcinoma (HCC) is a prevalent and fatal type of liver cancer with various risk factors. This study examines the connection between a specific genetic variant, STAT4 rs7574865, and HCC risk in Latin American and European populations. The results reveal no general association between this genetic variant and HCC in the studied groups. This study underscores the significance of researching diverse populations to gain a better understanding of the broader influence of genetic factors on HCC risk, which may aid in developing more effective strategies for identifying and managing high-risk individuals.
Abstract
Hepatocellular carcinoma (HCC) is the third leading cause of cancer death worldwide. The STAT4 rs7574865 genetic variant has been associated with an increased risk of developing HCC in Asian populations. However, this association has not been studied in Latin America and is poorly assessed in European populations. This case-control study investigated the association between STAT4 rs7574865 and HCC risk in these populations. We evaluated DNA samples from seven medical institutions across six Latin American countries and one Dutch institution in 1060 individuals (344 HCC and 716 controls). STAT4 rs7574865 SNP was genotyped using TaqMan-genotyping assay and analyzed using logistic regression. We found no significant association between the homozygous risk allele (G) of STAT4 and HCC development in either population, with odds ratios (OR) for GG versus TT of 0.85 (CI: 0.48–1.52, p = 0.58) and 0.81 (CI: 0.34–1.93, p = 0.67) for Latin Americans and Europeans respectively. No correlation was found between the risk allele and HCC based on underlying liver disease. However, we found that Latin Americans of European ancestry were more likely to carry the risk allele. Our results suggest that the STAT4 SNP rs7574865 does not influence the risk of developing HCC in Latin American or European populations, highlighting the importance of evaluating genetic risk factors in various ethnic groups and understanding the possible influence of ancestry on the genetic basis of disease.
1. Introduction
Hepatocellular carcinoma (HCC) is the most common cause of primary liver cancer and the third leading cause of cancer death globally [1]. The significant risk factors for HCC include infections with hepatitis B virus (HBV) and hepatitis C virus (HCV), as well as alcohol-associated cirrhosis and metabolic dysfunction-associated steatotic liver disease (MASLD) [2]. Both MASLD and HBV are particularly important in Latin America. The impact of MASLD has been steadily growing worldwide, given the obesity epidemic, with a particular emphasis in Latin America [3,4,5]. Current trends show that by 2040, liver cancer deaths related to MASLD among Latin Americans will increase by 85% compared to the global 59%, and recent data have shown a high rate of advanced-stage HCC diagnosis in Latin America, despite current developments in diagnostics and surveillance [6,7,8,9].
Regarding HBV, a previous study by our group in Latin America showed a significant proportion of early HCC and high mortality related to HBV infection, suggesting that HBV is an underreported cause of early HCC in the region [10]. The stage of HCC diagnosis is highly predictive of mortality, with high mortality rates associated with diagnosis of HCC in the later stages of the disease [11]. Therefore, successful identification and determination of high-risk individuals can play a crucial role in the earlier diagnosis of HCC.
HCC risk assessment proposed by genetic determination is an attractive and applicable path. HCC has a considerable genetic component, and a family history doubles the risk for HCC development [12]. Single nucleotide polymorphisms (SNPs) are common genetic variations that can significantly influence an individual’s susceptibility to various diseases [13]. Among those variations, an SNP on the gene STAT4 rs7574865 has been increasingly implicated in the development of HCC, mainly in Asian populations. This SNP consists of two alleles, G and T, with the G allele being associated with an increased risk of developing HCC [14]. This SNP has been previously associated with autoimmune diseases such as autoimmune thyroid disease, ulcerative colitis, and malignancies such as HCC [15,16]. STAT4 expression has also been associated with numerous malignancies, such as ovarian and lung cancer [17,18]. It has been theorized that reduced STAT4 expression, induced by the SNP, could potentially weaken the anti-tumor response by affecting STAT4 modulation of interleukin 12 in NK cells [19].
Building on this mechanistic understanding, numerous studies have assessed its clinical relevance, confirming a notable association between this SNP in STAT4 and HCC in different populations. Jiang et al. found an association between STAT4 and HCC among patients with HBV-related HCC in a genome-wide association study (GWAS) performed in China [14]. While other studies, such as the replication study by Chen et al., failed to repeat the same findings [20]. However, these studies have been performed in Asian and Caucasian populations with no representation of other ethnic groups [14,20,21,22,23]. Supplementary Table S1 describes all previous studies on STAT4 and HCC and their methodologies. To our knowledge, no evaluations of the genetic association between STAT4 and HCC have been conducted in Latin Americans. The current study addresses this knowledge gap by focusing on a Latin American cohort. Specifically, we hypothesized that a different risk allele frequency would be found in this population due to differential genetic background.
2. Methods
2.1. Samples and Study Subjects
This is a cross-sectional study focusing on patients who were incorporated into the ESCALON network (www.escalon.eu, accessed on 1 August 2023). For this study, we included samples from seven medical institutions in six Latin American countries (Argentina, Ecuador, Brazil, Chile, Peru and Colombia) alongside a single Dutch institution that served as the source of the European subjects. Participants were chosen for the study as per continuous participation in the ESCALON study (prospective follow-up for HCC biomarkers) rather than randomly [24,25].
At each participating medical center, patient data and blood samples were gathered and recorded in a Research Electronic Data Capture (REDCap) registry. To uphold ethical standards, all patient data was anonymized, and the provision of previous informed consent (in the patient’s respective language) and ethics approval from all participating institutions was mandatory. Upon inclusion in the study, control participants are followed every six months in their respective clinics with clinical, ultrasound and laboratory evaluations. This allows the investigators to determine the lack of HCC development for the duration of the study. Participants do not receive remuneration or simile for participation as it is part of their recommended care by being at risk for HCC.
Patients were classified as having HCC if they met the American Association for the Study of Liver Disease’s prescribed biopsy or imaging standards [26]. The diagnostic process involved two main avenues: histological confirmation and imaging studies. A liver biopsy was performed for histological confirmation, which involved extracting tissue samples from the liver lesion for microscopic examination. This method was primarily reserved for cases where imaging studies yielded inconclusive results, or additional histopathological information was deemed clinically necessary. For imaging-based diagnosis, a multiphasic computed tomography (CT) or magnetic resonance imaging (MRI) was utilized. Specific criteria, such as arterial phase hyper-enhancement followed by venous phase washout, had to be met to confirm an HCC diagnosis solely on imaging grounds. Dual-phase or triple-phase techniques were employed, capturing images at multiple time intervals post-contrast administration to assess the vascular behavior of the lesion.
Patients were classified as having alcohol-related liver disease if they had persistent steatohepatitis in the setting of prolonged ethanol intake, defined as 30 g/day for women and 40 g/day for men over ten years. The diagnosis of MASLD was determined by the managing hepatologist or by evidence of hepatic steatosis on pathology or imaging in the absence of other clear reasons for hepatic steatosis. Individuals without viral hepatitis, MASLD or alcohol-related liver disease were categorized as “other” etiology, which encompassed both known causes and unknown causes. If patients were identified with a mixed etiology—having any combination of HBV, HCV, MASLD, and alcohol-related liver disease—they were excluded from the subgroup analysis.
To ensure accuracy and integrity, all collected data underwent regular audits and was independently verified by the overseeing institution before initiating data analysis.
2.2. Genotypic Analysis
To assess single nucleotide polymorphisms, genomic DNA was obtained from whole blood samples utilizing Gentra Puregene (Minneapolis, MN, USA), following the steps outlined in the manufacturer’s instructions. The STAT4 SNP rs7574865 G > T was specifically genotyped using pre-configured TaqMan probe SNP genotyping assays from Thermo Fisher (cat. nr. 4351376). The context sequence of the probes is TATGAAAAGTTGGTGACCAAAATGT[G/T]AATAGTGGTTATCTTATTTCAGTGG, with the variation G versus T as indicated. The TaqMan SNP genotyping assay aims to determine genetic variations within genomic DNA by identifying a single nucleotide difference within a specific gene locus. Each TaqMan SNP Genotyping Assay includes two differentially labeled, allele-specific TaqMan MGB probes and a PCR primer pair that uniquely amplify and provide unmatched specificity for the allele of interest. Upon amplification by real-time PCR, the fluorescent signal of the probes is registered and visualized in allelic discrimination plots. The genotyping was carried out with the StepOne-Plus Real-Time PCR System, in combination with a Custom TaqMan SNP Genotyping Assay (Applied Biosystems, Waltham, MA, USA). Each quantitative PCR reaction had a 10 µL volume, comprising 4 µL of genomic DNA and a 6 µL genotyping master mix inclusive of the probe.
2.3. Statistical Analysis
The comparison of demographic and clinical traits across various subjects involved presenting continuous variables as means and standard deviations, while categorical variables were depicted as proportions. Chi-squared, Fisher’s Exact test and multiple logistic regression were performed to evaluate the association between this SNP and HCC. The odds ratios (OR) and 95% confidence intervals (CI) for each variable were determined. JASP (Version 0.17.1) [Computer software] was utilized for performing these statistical calculations. JASP software was chosen for our statistical analysis due to its user-friendly interface, versatile range of statistical tests, including chi-square tests and logistic regression models, and its robust performance in handling large data sets, making it particularly suitable for the study’s requirements.
2.4. Ethics
Each institution involved in the study provided ethical approval for the research as required for ESCALON. Before their involvement in the ESCALON study, all participants provided written informed consent in their native language.
3. Results
3.1. Patient Characteristics
We included 1060 individuals: 344 patients with HCC (155 Latin Americans, 189 Europeans) and 716 controls (454 Latin Americans, 262 Europeans). The controls consisted of patients who had liver disease but no HCC. Of the Latin American controls, 80% had cirrhosis, while 60% of the European controls had cirrhosis. The median age for Latin Americans with HCC and controls was 68 (IQR 62–73) and 63 (IQR 57–69) years, respectively, while for the European cohort, it was 67 (IQR 61–71) and 58 (IQR 46–66) years, respectively. Males represented 64% of the Latin American HCC cohort and 77% of the European HCC cohort.
The most common causes of underlying liver disease in Latin Americans were MASLD, 46% and 59% in the study group and controls, respectively, followed by alcohol use disorder (AUD), 25% and 15%, respectively. In the European cohort, AUD and MASLD predominated in the HCC group (35% and 19%, respectively), with HBV and HCV being more common among controls (31% and 29%). All patient characteristics are summarized in Table 1.

Table 1.
Basic patient characteristics.
3.2. STAT4 HCC Risk Assessment
Latin Americans with HCC presented with lower frequencies of the risk-associated GG genotype compared to their counterparts without HCC (37% vs. 42%, respectively, Figure 1). However, this difference was not statistically significant (p = 0.46). Similarly, a non-significant lower frequency of the GG genotype was observed in Europeans with HCC (58%) compared to those without HCC (62%, p = 1). There was no significant statistical difference in the frequencies of the TT genotype and GT genotype between participants with and without HCC in either cohort (Table 2). Overall, the G allele (risk allele) did not determine risk for HCC in either cohort yet showed a trend towards a non-statistically significant reduction in risk in both groups with odds ratios (OR) for GG versus TT of 0.85 (CI: 0.47–1.52) and 0.81 (CI: 0.34–1.93) for Latin Americans and Europeans respectively. We later performed a risk assessment of the G allele between cirrhotic and non-cirrhotic patients but found no correlation among both groups in either cohort (Supplementary Table S2). Risk allele frequency was also evaluated using the gnomAD database, a genomic data aggregation platform incorporating 17,720 sequences related to Latin Americans (https://gnomad.broadinstitute.org/, accessed on 5 June 2023) [27]. The risk allele frequency within the gnomAD database registered at 64.8% for Latin Americans; in our Latin Americans HCC cohort, it was found to be 60.52%. Importantly, this did not differ significantly from the risk allele frequency in our cohort of Latin Americans with cirrhosis but without HCC (OR = 0.92, 95% CI: 0.70–1.20, p = 0.53).
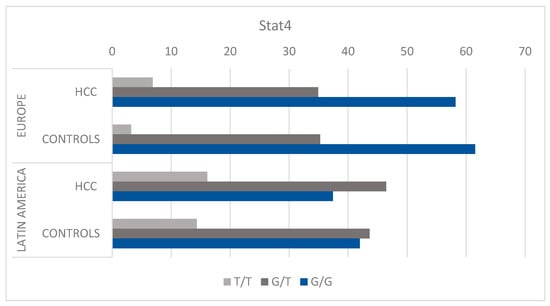
Figure 1.
Distribution of genotypes. The genotype frequency distribution of the STAT4 rs7574865 G > T single nucleotide polymorphism in patients with hepatocellular carcinoma compared to controls without hepatocellular carcinoma with liver disease. Genotype frequency is stratified by geographic patient location in two separate cohorts, Europeans and Latin Americans. Percentage of each genotype among the European HCC and control groups, respectively: GG (58.2%, 61.54%), GT (34.93%, 35.26%), TT (6.88%, 3.21%). Percentage of each genotype among the Latin American HCC and control groups, respectively: GG (37.42%, 41.99%), GT (46.45%, 43.65%), TT (16.13%, 14.36%). Abbreviations: HCC, hepatocellular carcinoma.
Table 2.
Odds of HCC divided by cause of liver disease and ethnicity.
3.3. STAT4 HCC Risk Assessment Based on Underlying Liver Disease
We performed subgroup analyses focused on underlying liver disease, but no association was found between the GG genotype and HCC in Latin Americans diagnosed with MASLD (GG vs. GT and TT OR = 0.78, 95% CI: 0.43–1.38, p = 0.414). We also did not find significant correlations between the GG genotype and HCC in Latin Americans with viral hepatitis or alcohol-related liver disease (Table 3). A specific assessment was performed on those with HBV. However, the number of HBV samples was too low to perform a reasonable analysis (Table 3). Similarly, for the European cohort, no correlation was observed between the GG genotype and HCC in subgroup analyses based on the type of underlying liver disease (Table 3).
Table 3.
Odds of HCC stratified by STAT4 risk allele.
3.4. Effect of Ancestry in HCC Risk Related to STAT4
Most (87%) Latin Americans diagnosed with HCC or cirrhosis examined in this study had non-European ancestry. The risk allele frequency for Latin Americans of non-European descent was 60.9%, whereas it was 69.38% for European descent (p = 0.04). This suggests that Latin Americans of European ancestry are more likely to carry the G allele (OR = 1.46, 95% CI: 1.02–2.08, Figure 2A). Crucially, there was no significant difference in risk allele frequency between Europeans and Latin Americans of European ancestry (p = 0.07). The same applied when comparing Europeans with HCC to Latin Americans of European ancestry with HCC (p = 0.76) (Figure 2B). Another analysis showed that Latin Americans with HCC are significantly less likely to carry the GG genotype than Europeans with HCC (OR = 0.424, 95% CI: 0.27–0.66, p < 0.001). However, this significance was not seen when observing patients of European descent (OR = 1.4, 95% CI:0.46–4.29, p = 0.78) (Figure 3).
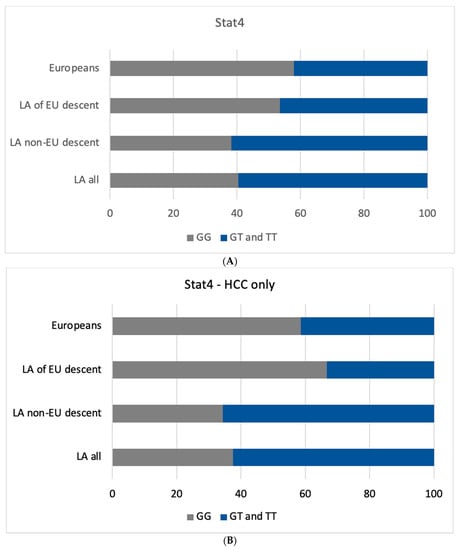
Figure 2.
(A) Genotype Frequency Distribution of STAT4 rs7574865 G > T SNP Across Different Geographic and Ethnic Cohorts. The genotype frequency distribution of the STAT4 rs7574865 G > T single nucleotide polymorphism in all patients. Frequencies are compared between patients of different current geographic locations and descent with a European cohort, a Latin American cohort of European descent and a Latin American cohort of non-European descent. This figure shows the similarities in the distribution of the GG genotype between Europeans and Latin Americans of European descent. (B) Genotype Frequency Distribution of STAT4 rs7574865 G > T SNP in HCC patients. The genotype frequency distribution of the STAT4 rs7574865 G > T single nucleotide polymorphism in HCC patients. Frequencies are compared between patients of different current geographic locations and descent with a European cohort, a Latin American cohort of European descent and a Latin American cohort of non-European descent. This figure shows the differences in the distribution of the GG genotype between different cohorts. The x-axis indicates the frequency of each genotype measured in percentages, while the y-axis represents different patient cohorts. Each bar is color-coded to differentiate between the GG, GT, and TT genotypes. Abbreviations: LA, Latin Americans; EU, European.
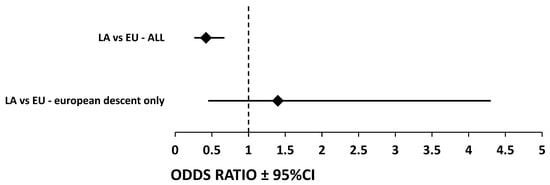
Figure 3.
Differences in GG Genotype Prevalence Between Latin American and European Cohorts: Odds Ratios and 95% Confidence Intervals. Illustrating the Difference in GG Genotype Prevalence between Patient Cohorts. This figure visualizes the odds ratios (OR) and 95% confidence intervals (CI) for the prevalence of the GG genotype in STAT4 rs7574865 G > T SNP across different patient groups. The y-axis delineates two key comparisons: the first line represents the comparison between Latin Americans and Europeans, while the second line compares Latin Americans of European descent with Europeans of European descent. The x-axis shows the OR values along with the corresponding 95% CIs. For the comparison between Latin Americans and Europeans, the OR is 0.424 with a 95% CI of 0.27–0.66, indicating a significant difference. Conversely, the analysis comparing Latin Americans of European descent and Europeans yielded an OR of 1.4 with a 95% CI of 0.46–4.29, suggesting a lack of significant difference. Each OR is represented by a square, and the horizontal lines extending from it illustrate the range of the 95% CI—abbreviations: LA, Latin Americans; EU, Europeans; CI, Confidence interval.
4. Discussion
Our analysis found no statistically significant association between the STAT4 rs7574865 G > T SNP and HCC in a Latin American population. To our knowledge, this is the first study on the effect of the STAT4 SNP on HCC development in patients from Latin America. In addition, we evaluated a cohort from Europe for comparative purposes, and consistent with other prior findings, we discerned no correlation between the SNP and the progression of HCC in patients with liver disease [20,28,29,30]. This study emphasizes the need to entertain population background in the clinic when addressing genetic risk for HCC. Moreover, it suggests that future research should focus on multiple and broad backgrounds when assessing a specific biomarker (be genetic, immune, or other) to risk-stratify the approach to HCC.
STAT4 functions as a mediator of immunity and tumor growth as an important member of the JAK-STAT pathway. It has been associated with autoimmune diseases [31,32] and malignancies such as lung, colon, and breast cancer [22,23,33,34,35,36,37].
A mechanism proposed by El Sharkawy et al. suggested that the G risk allele is linked with reduced STAT4 mRNA expression, subsequently impairing interleukin 12 signaling in NK cells, thereby weakening their anti-tumor efficacy [22]. However, our study found no differences between cirrhotic and non-cirrhotic populations in terms of STAT4 risk allele. Our study found that STAT4 mutation does not seem to be associated with HCC in our populations (both Latin American and European). However, future studies demonstrating the functional consequences of the SNP are needed to determine whether the polymorphism affects the expression levels of STAT4 in selected immune cells and whether the phosphorylation of STAT4 is affected upon stimulation of these cells with known stimulators such as interleukin-12.
The discrepancy in our results compared to existing literature may not only stem from the ethnic diversity of our cohort compared to the vastly homogenous Chinese population but also the underlying pathophysiological mechanisms of HCC development [38,39,40,41,42,43]. For instance, the role of STAT4 in HCC development may differ depending on the etiology of liver disease. While hepatitis B virus (HBV) is the primary cause of HCC in Chinese populations [42], only 9% of HCC cases in our study were HBV-related, potentially affecting the impact of STAT4 polymorphisms on disease progression. Indeed, Zhong et al. had 74% of HBV-related HCC, and Chen et al. had 82% of HBV-related HCC in their studies [44,45]. This difference in the underlying cause of HCC reflects the different mechanisms of HCC development and the role of STAT4 in its occurrence in different etiologies of liver disease. Due to a low number of samples, we could not assess the impact of the STAT4 SNP in those exclusively with HBV-related HCC.
El Sharkawy et al. have recently confirmed that a risk STAT4 SNP in a Caucasian population is associated with a greater rate of fibrosis and inflammation in HBV patients [22]. The same effects have been described in Asian populations [23,34,36,37]. It is also possible that inflammatory mechanisms leading to different immune active mechanisms related to STAT activation or inactivation are present in certain populations compared to others, affecting HCC risk [20,46,47]. This could be associated with a multiple-hit development with environmental exposures (such as aflatoxins) and specific SNPs, eventually leading to HCC development [44].
Importantly, our study also evaluated self-reported heritage background. Latin Americans of European descent showed a similar distribution of the risk allele compared to the European cohort in the overall population (partially supporting self-reported heritage as a reasonable factor when full genome analysis is unavailable) and no difference in SNP prevalence among HCC or controls. It is important to note that our study relied on self-reported heritage background without any genetic analysis, which could introduce bias. Although this approach enhances the data and provides preliminary findings related to ancestry, this association should be confirmed in the setting of admixture studies [41]. Furthermore, the sample size in our study was relatively small, limiting the generalizability of our findings. Therefore, larger studies are needed to confirm and further investigate these associations.
The current findings do not yet inform clinical practice in terms of better diagnosis or treatment of HCC. However, understanding the value of STAT4 for risk-stratification in HCC could potentially guide future strategies. Moreover, our study warns against extrapolating the risk profile of SNPs from different populations.
5. Conclusions
This study provides novel evidence regarding the association of the STAT4 rs7574865 G > T single nucleotide polymorphism and hepatocellular carcinoma (HCC) within Latin American populations. Our results indicate no significant association between this SNP and the occurrence of HCC in the studied Latin American cohorts compared to a European control group. Future research should aim to include larger sample sizes and more diverse ethnic groups to validate these findings.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/cancers15184530/s1, Table S1: Table with previous studies on STAT4 rs7574865 and liver pathology; Table S2: Comparing G allele frequency of cirrhotic patients to patients without cirrhosis and divided for Latin Americans (LA), and Europeans (EU). References [48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64] are cited in the Supplementary Materials.
Author Contributions
A.A. and C.M.A. analysis and interpretation of data, drafting of the manuscript. J.P., D.B., J.D.F., A.Z.M., M.A., E.C., Z.M.A.G. and J.O. acquisition of data, data analysis, revision of the manuscript. J.D.D. and A.B. study design, interpretation of data, critical editing of the manuscript, and study supervision. All authors have read and agreed to the published version of the manuscript.
Funding
European-Latin American ESCALON consortium, funded by the EU Horizon 2020 program, project number 825510, AIRP UMN and NIH-R21TW012390-01A1.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Erasmus MC (MEC-2019-0137).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author (JD).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Hyuna, S.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Kulik, L.; El-Serag, H.B. Epidemiology and Management of Hepatocellular Carcinoma. Gastroenterology 2019, 156, 477–491. [Google Scholar] [CrossRef]
- Mcglynn, K.A.; Petrick, J.L.; El-Serag, H.B. Epidemiology of Hepatocellular Carcinoma. Hepatology 2021, 73, 4–13. [Google Scholar] [CrossRef] [PubMed]
- Caines, A.; Selim, R.; Salgia, R. The Changing Global Epidemiology of Hepatocellular Carcinoma. Clin. Liver Dis. 2020, 24, 535–547. [Google Scholar] [CrossRef] [PubMed]
- Pinto, C.; Souza De Oliveira, M.; Cotrim, H.P.; Arrese, M. Nonalcoholic Fatty Liver Disease Risk Factors in Latin American Populations: Current Scenario and Perspectives. Clin. Liver Dis. 2019, 13, 39–42. [Google Scholar] [CrossRef]
- Jose Carrilho, F.; Cerqueira Paranaguá-Vezozzo, D.; Lopes Chagas, A.; Saraiva de Souza Melo Alencar, R.; Gomes da Fonseca, L.; Carrilho, J.; Paulo, S. Epidemiology of Liver Cancer in Latin America: Current and Future Trends. Liver Dis. 2020, 40, 101–110. [Google Scholar] [CrossRef]
- Farah, M.; Anugwom, C.; Ferrer, J.D.; Baca, E.L.; Mattos, A.Z.; Possebon, J.P.P.; Arrese, M.; Prieto, J.; Balderramo, D.; Carrera, E.; et al. Changing Epidemiology of Hepatocellular Carcinoma in South America: A Report from the South American Liver Research Network. Ann. Hepatol. 2023, 28, 100876. [Google Scholar] [CrossRef]
- Ferlay, J.; LMEMLFCMMLPMZASIBF. Global Cancer Observatory: Cancer Tomorrow. Lyon, France: International Agency for Research on Cancer. Available online: https://gco.iarc.fr/Tomorrow (accessed on 5 December 2022).
- Akambase, J.A.; Prieto, J.E.; Mattos, A.Z.; Mattos, A.A.; Carrera, E.; Díaz-Ferrer, J.; Gallardo, P.; Curia, A.; Ballerga, E.G.; Tovo, C.V.; et al. Epidemiology and Risk Factors for Histopathologic Characteristics of Non-Alcoholic Fatty Liver Disease in South America. Aliment. Pharmacol. Ther. 2023. [Google Scholar] [CrossRef]
- Debes, J.D.; Chan, A.J.; Balderramo, D.; Kikuchi, L.; Gonzalez Ballerga, E.; Prieto, J.E.; Tapias, M.; Idrovo, V.; Davalos, M.B.; Cairo, F.; et al. Hepatocellular Carcinoma in South America: Evaluation of Risk Factors, Demographics and Therapy. Liver Int. 2018, 38, 136–143. [Google Scholar] [CrossRef]
- Galle, P.R.; Forner, A.; Llovet, J.M.; Mazzaferro, V.; Piscaglia, F.; Raoul, J.L.; Schirmacher, P.; Vilgrain, V. EASL Clinical Practice Guidelines: Management of Hepatocellular Carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef]
- Mezina, A.; Philips, N.; Bogus, Z.; Erez, N.; Xiao, R.; Fan, R.; Olthoff, K.M.; Reddy, K.R.; Samadder, N.J.; Nielsen, S.M.; et al. Multigene Panel Testing in Individuals With Hepatocellular Carcinoma Identifies Pathogenic Germline Variants. JCO Precis. Oncol. 2021, 5, 988–1000. [Google Scholar] [CrossRef]
- Shastry, B.S. SNPs: Impact on Gene Function and Phenotype. Methods Mol. Biol. 2009, 578, 3–22. [Google Scholar] [CrossRef]
- Jiang, D.-K.; Sun, J.; Cao, G.; Liu, Y.; Lin, D.; Gao, Y.-Z.; Ren, W.-H.; Long, X.-D.; Zhang, H.; Ma, X.-P.; et al. Genetic Variants in STAT4 and HLA-DQ Genes Confer Risk of Hepatitis B Virus–Related Hepatocellular Carcinoma. Nat. Genet. 2013, 45, 72–75. [Google Scholar] [CrossRef]
- Michael Morton, N.; James Simmonds, M.; Monzani, F.; Yu, Y.; Gao, X.; Wang, J. The Association Between STAT4 Rs7574865 Polymorphism and the Susceptibility of Autoimmune Thyroid Disease: A Meta-Analysis. Front. Genet. 2019. [Google Scholar] [CrossRef]
- Xu, L.; Dai, W.Q.; Wang, F.; He, L.; Zhou, Y.Q.; Lu, J.; Xu, X.F.; Guo, C.Y. Association of STAT4 Gene Rs7574865G > T Polymorphism with Ulcerative Colitis Risk: Evidence from 1532 Cases and 3786 Controls. Arch. Med. Sci. 2014, 10, 419. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Ji, G.; Le, X.; Luo, Z.; Wang, C.; Feng, M.; Xu, L.; Zhang, Y.; Lau, W.B.; Lau, B.; et al. An Integrated Analysis Identifies STAT4 as a Key Regulator of Ovarian Cancer Metastasis. Oncogene 2017, 36, 3384–3396. [Google Scholar] [CrossRef] [PubMed]
- Yoon, Y.H.; Hwang, H.J.; Sung, H.J.; Heo, S.H.; Kim, D.S.; Hong, S.H.; Lee, K.H.; Cho, J.Y. Upregulation of Complement Factor H by SOCS-1/3–STAT4 in Lung Cancer. Cancers 2019, 11, 471. [Google Scholar] [CrossRef] [PubMed]
- El Sharkawy, R.; George, J.; Eslam, M. Editorial: STAT-4 Polymorphism—A Tool to Personalise Clinical Practice in Chronic HBV Infection. Authors’ Reply. Aliment. Pharmacol. The.r 2018, 48, 769–770. [Google Scholar] [CrossRef]
- Chen, K.; Shi, W.; Xin, Z.; Wang, H.; Zhu, X.; Wu, X.; Li, Z.; Li, H.; Liu, Y. Replication of Genome-Wide Association Studies on Hepatocellular Carcinoma Susceptibility Loci in a Chinese Population. PLoS ONE 2013, 8, e77315. [Google Scholar] [CrossRef]
- Yang, C.; Chen, H.; Zhou, B.; Yin, J.; Cao, G.; Hou, J.; Jiang, D. The Effects of the Interactions of STAT4 Rs7574865 with HBV Mutations on the Risk of Hepatocellular Carcinoma. Mol. Carcinog. 2022. [Google Scholar] [CrossRef]
- El Sharkawy, R.; Thabet, K.; Lampertico, P.; Petta, S.; Mangia, A.; Berg, T.; Metwally, M.; Bayoumi, A.; Boonstra, A.; Brouwer, W.P.; et al. A STAT4 Variant Increases Liver Fibrosis Risk in Caucasian Patients with Chronic Hepatitis B. Aliment. Pharmacol. Ther. 2018, 48, 564–573. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Gao, N.; Yang, L.; Guo, Y.; Fang, Y.; Wang, T.; Xu, C.; Li, G.F.; Zhou, J.; Zhang, Y.; et al. Stat4 Rs7574865 Polymorphism Promotes the Occurrence and Progression of Hepatocellular Carcinoma via the Stat4/CYP2E1/FGL2 Pathway. Cell Death Dis. 2022, 13, 130. [Google Scholar] [CrossRef] [PubMed]
- Debes, J.D.; Carrera, E.; Mattos, A.Z.; Prieto, J.E.; Boonstra, A. Hepatocellular Carcinoma, a Unique Tumor with a Lack of Biomarkers. Ann. Hepatol. 2019, 18, 786–787. [Google Scholar] [CrossRef] [PubMed]
- Debes, J.D.; Boonstra, A.; Balderramo, D.; Mattos, A.Z.; Arrese, M. Hepatobiliary Cancers in South America: Disparity Strikes. Lancet. Gastroenterol. Hepatol. 2019, 4, 581. [Google Scholar] [CrossRef]
- Amit Singal, C.G.; Llovet, J.M.; Yarchoan, M.; Mehta, N.; Heimbach, J.K.; Dawson, L.A.; Jou, J.H.; Kulik, L.M.; Agopian, V.G.; Marrero, J.A.; et al. AASLD Practice Guidance on Prevention, Diagnosis, and Treatment of Hepatocellular. Hepatology 2023. ahead of print. [Google Scholar] [CrossRef]
- Chen, S.; Francioli, L.C.; Goodrich, J.K.; Collins, R.L.; Wang, Q.; Alföldi, J.; Watts, N.A.; Vittal, C.; Gauthier, L.D.; Poterba, T.; et al. A Genome-Wide Mutational Constraint Map Quantified from Variation in 76,156 Human Genomes. bioRxiv 2022. [Google Scholar] [CrossRef]
- Chao, X.; Wu, J.; Zhang, W.; Feng, X.; Zhao, L.; Huang, F.; Jiang, C. A New Discovery of STAT4 Single Nucleotide Polymorphisms Associated with Hepatocellular Carcinoma Risk in Chinese Han Population: A Case-Control Study. Biosci. Rep. 2021, 41, BSR20210124. [Google Scholar] [CrossRef]
- Kim, L.H.; Cheong, H.S.; Namgoong, S.; Kim, J.O.; Kim, J.H.; Park, B.L.; Cho, S.W.; Park, N.H.; Cheong, J.Y.; Koh, I.S.; et al. Replication of Genome-Wide Association Studies on Hepatocellular Carcinoma Susceptibility Loci of STAT4 and HLA-DQ in a Korean Population. Infect. Genet. Evol. 2015, 33, 72–76. [Google Scholar] [CrossRef]
- Clark, A.; Gerlach, F.; van Tong, H.; Hoan, N.X.; Song, L.H.; Toan, N.L.; Bock, C.-T.; Kremsner, P.G.; Velavan, T.P. A Trivial Role of STAT4 Variant in Chronic Hepatitis B Induced Hepatocellular Carcinoma. Infect. Genet. Evol. 2013, 18, 257–261. [Google Scholar] [CrossRef]
- Han, J.W.; Zheng, H.F.; Cui, Y.; Sun, L.D.; Ye, D.Q.; Hu, Z.; Xu, J.H.; Cai, Z.M.; Huang, W.; Zhao, G.P.; et al. Genome-Wide Association Study in a Chinese Han Population Identifies Nine New Susceptibility Loci for Systemic Lupus Erythematosus. Nat. Genet 2009, 41, 1234–1237. [Google Scholar] [CrossRef]
- Remmers, E.F.; Plenge, R.M.; Lee, A.T.; Graham, R.R.; Hom, G.; Behrens, T.W.; de Bakker, P.I.W.; Le, J.M.; Lee, H.-S.; Batliwalla, F.; et al. STAT4 and the Risk of Rheumatoid Arthritis and Systemic Lupus Erythematosus. N. Engl. J. Med. 2007, 357, 977. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Wang, F.; Luo, F. The Role of JAK/STAT Pathway in Fibrotic Diseases: Molecular and Cellular Mechanisms. Biomolecules 2023, 13, 119. [Google Scholar] [CrossRef]
- Li, J.; Liang, L.; Liu, Y.; Luo, Y.; Liang, X.; Luo, D.; Feng, Z.; Dang, Y.; Yang, L.; Chen, G. Clinicopathological Significance of STAT4 in Hepatocellular Carcinoma and Its Effect on Cell Growth and Apoptosis. Onco. Targets Ther. 2016, 9, 1721. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Qu, A.; Qu, A. Signal Transducer and Activator of Transcription 4 in Liver Diseases. Int. J. Biol. Sci. 2015, 11, 448. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Chen, J.H.; Qiang, Y.; Wang, D.Z.; Chen, Z. Decreased STAT4 Indicates Poor Prognosis and Enhanced Cell Proliferation in Hepatocellular Carcinoma. World J. Gastroenterol. 2015, 21, 3983. [Google Scholar] [CrossRef]
- Wubetu, G.Y.; Utsunomiya, T.; Ishikawa, D.; Yamada, S.; Ikemoto, T.; Morine, Y.; Iwahashi, S.; Saito, Y.; Arakawa, Y.; Imura, S.; et al. High STAT4 Expression Is a Better Prognostic Indicator in Patients with Hepatocellular Carcinoma after Hepatectomy. Ann. Surg. Oncol. 2014, 21, 721–728. [Google Scholar] [CrossRef]
- Main Data of the Seventh National Population Census. Available online: http://www.stats.gov.cn/english/PressRelease/202105/t20210510_1817185.html (accessed on 19 February 2023).
- Lamarca, A.; Mendiola, M.; Barriuso, J. Hepatocellular Carcinoma: Exploring the Impact of Ethnicity on Molecular Biology. Crit. Rev. Oncol. Hematol. 2016, 105, 65–72. [Google Scholar] [CrossRef]
- Zhang, X.; El-Serag, H.B.; Thrift, A.P. Sex and Race Disparities in the Incidence of Hepatocellular Carcinoma in the United States Examined through Age-Period-Cohort Analysis. Cancer Epidemiol. Biomark. Prev. 2020, 29, 88–94. [Google Scholar] [CrossRef]
- Lakeman, P.; Henneman, L.; Bezemer, P.D.; Cornel, M.C.; Kate, L.P. Ten Developing and Optimizing a Decisional Instrument Using Self-Reported Ancestry for Carrier Screening in a Multi-Ethnic Society. Genet. Med. 2006, 8, 502–509. [Google Scholar] [CrossRef][Green Version]
- Zhu, R.X.; Seto, W.K.; Lai, C.L.; Yuen, M.F. Epidemiology of Hepatocellular Carcinoma in the Asia-Pacific Region. Gut Liver 2016, 10, 332–339. [Google Scholar] [CrossRef]
- Jalil, I.; Arshad, M.; Khan, S.; Dasti, J.I. The STAT4 and Not the IFNL3 Variant Is Associated with Hepatitis B Virus Clearance in a Population from the Khyber Pakhtunkhwa Region of Pakistan. Arab J. Gastroenterol. 2020, 21, 91–94. [Google Scholar] [CrossRef] [PubMed]
- Zhong, X.; Luo, M.; Wu, Y.; Zhou, X.; Yu, X.; Liu, L.; Chen, S. Genetic Variants in STAT4 and Their Interactions with Environmental Factors for the Incidence of Hepatocellular Carcinoma. Cancer Biomark. 2021, 32, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Wang, M.; Zhang, Z.; Tang, H.; Zuo, X.; Meng, X.; Xiong, M.; Zhou, F.; Liang, B.; Dai, F.; et al. Replication the Association of 2q32.2-Q32.3 and 14q32.11 with Hepatocellular Carcinoma. Gene 2015, 561, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Dong, M.; Li, J.; Tang, R.; Zhu, P.; Qiu, F.; Wang, C.; Qiu, J.; Wang, L.; Dai, Y.; Xu, P.; et al. Multiple Genetic Variants Associated with Primary Biliary Cirrhosis in a Han Chinese Population. Clin. Rev. Allergy Immunol. 2015, 48, 316–321. [Google Scholar] [CrossRef]
- Aiba, Y.; Yamazaki, K.; Nishida, N.; Kawashima, M.; Hitomi, Y.; Nakamura, H.; Komori, A.; Fuyuno, Y.; Takahashi, A.; Kawaguchi, T.; et al. Disease Susceptibility Genes Shared by Primary Biliary Cirrhosis and Crohn’s Disease in the Japanese Population. J. Hum. Genet. 2015, 60, 525–531. [Google Scholar] [CrossRef]
- Qi, X.; Li, F.; Zhang, Y.; Zhu, H.; Yang, F.; Li, X.; Jiang, X.; Chen, L.; Huang, Y.; Zhang, J. STAT4 Genetic Polymorphism Significantly Affected HBeAg Seroconversion in HBeAg-Positive Chronic Hepatitis B Patients Receiving Peginterferon-α Therapy: A Prospective Cohort Study in China. J. Med. Virol. 2022, 94, 4449–4458. [Google Scholar] [CrossRef] [PubMed]
- Limothai, U.; Chuaypen, N.; Poovorawan, K.; Poovorawan, Y.; Tangkijvanich, P. Genetic Variation in STAT4 Is Associated with Treatment Response to Pegylated Interferon in Patients with Chronic Hepatitis B. Asian Pac. J. Allergy Immunol. 2022, 40, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Sun, J.; Zhou, B.; Peng, J.; Xie, Q.; Liang, X.; Fan, R.; Conran, C.; Xu, J.; Ji, Y.; et al. A Missense Variant in Complement Factor B (CFB) Is a Potential Predictor of 24-Week off-Treatment Response to PegIFNα Therapy in Chinese HBeAg-Positive Chronic Hepatitis B Patients. Aliment Pharmacol. Ther. 2020, 51, 469–478. [Google Scholar] [CrossRef]
- Chen, H.; Sun, J.; Zhou, B.; Xie, Q.; Liang, X.; Fan, R.; Conran, C.; Xu, J.; Ji, Y.; Zhang, X.; et al. Variants in STAT4 Associated with Cure of Chronic HBV Infection in HBeAg-Positive Patients Treated with Pegylated Interferon-Alpha. Clin. Gastroenterol. Hepatol. 2020, 18, 196–204.e8. [Google Scholar] [CrossRef]
- Jiang, D.K.; Wu, X.; Qian, J.; Ma, X.P.; Yang, J.; Li, Z.; Wang, R.; Sun, L.; Liu, F.; Zhang, P.; et al. Genetic Variation in STAT4 Predicts Response to Interferon-α Therapy for Hepatitis B e Antigen-Positive Chronic Hepatitis B. Hepatology 2016, 63, 1102–1111. [Google Scholar] [CrossRef]
- Lu, Y.; Zhu, Y.; Peng, J.; Wang, X.; Wang, F.; Sun, Z. STAT4 Genetic Polymorphisms Association with Spontaneous Clearance of Hepatitis B Virus Infection. Immunol. Res. 2015, 62, 146–152. [Google Scholar] [CrossRef]
- Jiang, D.K.; Ma, X.P.; Wu, X.; Peng, L.; Yin, J.; Dan, Y.; Huang, H.X.; Ding, D.L.; Zhang, L.Y.; Shi, Z.; et al. Genetic Variations in STAT4,C2,HLA-DRB1 and HLA-DQ Associated with Risk of Hepatitis B Virus-Related Liver Cirrhosis. Sci. Rep. 2015, 5, 16278. [Google Scholar] [CrossRef]
- Liao, Y.; Cai, B.; Li, Y.; Chen, J.; Ying, B.; Tao, C.; Zhao, M.; Ba, Z.; Zhang, Z.; Wang, L. Association of HLA-DP/DQ, STAT4 and IL-28B Variants with HBV Viral Clearance in Tibetans and Uygurs in China. Liver Int. 2015, 35, 886–896. [Google Scholar] [CrossRef]
- Ali, N.A.; Hamdy, N.M.; Gibriel, A.A.; EL Mesallamy, H.O. Investigation of the Relationship between CTLA4 and the Tumor Suppressor RASSF1A and the Possible Mediating Role of STAT4 in a Cohort of Egyptian Patients Infected with Hepatitis C Virus with and without Hepatocellular Carcinoma. Arch. Virol. 2021, 166, 1643–1651. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Trépo, E.; Nahon, P.; Cao, Q.; Moreno, C.; Letouzé, E.; Imbeaud, S.; Gustot, T.; Deviere, J.; Debette, S.; et al. PNPLA3 and TM6SF2 Variants as Risk Factors of Hepatocellular Carcinoma across Various Etiologies and Severity of Underlying Liver Diseases. Int. J. Cancer 2019, 144, 533–544. [Google Scholar] [CrossRef] [PubMed]
- Chanthra, N.; Payungporn, S.; Chuaypen, N.; Piratanantatavorn, K.; Pinjaroen, N.; Poovorawan, Y.; Tangkijvanich, P. Single Nucleotide Polymorphisms in STAT3 and STAT4 and Risk of Hepatocellular Carcinoma in Thai Patients with Chronic Hepatitis B. Asian Pac. J. Cancer Prev. 2016, 16, 8405–8410. [Google Scholar] [CrossRef] [PubMed]
- Shi, H.; He, H.; Ojha, S.C.; Sun, C.; Fu, J.; Yan, M.; Deng, C.; Sheng, Y. Association of STAT3 and STAT4 Polymorphisms with Susceptibility to Chronic Hepatitis B Virus Infection and Risk of Hepatocellular Carcinoma: A Meta-Analysis. Biosci. Rep. 2019, 39, 20190783. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Y.; Liu, G.; Gong, L. Systematic Review and Meta-Analysis on the Association between Polymorphisms in Genes of IL-12 Signaling Pathway and Hepatocellular Carcinoma Risk. J. Cancer 2018, 9, 3583–3592. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Xu, K.; Liu, C.; Chen, J. Meta-Analysis Reveals an Association between Signal Transducer and Activator of Transcription-4 Polymorphism and Hepatocellular Carcinoma Risk. Hepatol. Res. 2017, 47, 303–311. [Google Scholar] [CrossRef]
- Jiang, X.; Su, K.; Tao, J.; Fan, R.; Xu, Y.; Han, H.; Li, L.; Li, M.D. Association of STAT4 Polymorphisms with Hepatitis B Virus Infection and Clearance in Chinese Han Population. Amino Acids 2016, 48, 2589–2598. [Google Scholar] [CrossRef]
- Zhao, X.; Jiang, K.; Liang, B.; Huang, X. STAT4 Gene Polymorphism and Risk of Chronic Hepatitis B-Induced Hepatocellular Carcinoma. Cell Biochem. Biophys. 2015, 71, 353–357. [Google Scholar] [CrossRef]
- Liao, Y.; Cai, B.; Li, Y.; Chen, J.; Tao, C.; Huang, H.; Wang, L. Association of HLA-DP/DQ and STAT4 Polymorphisms with HBV Infection Outcomes and a Mini Meta-Analysis. PLoS ONE 2014, 9, e111677. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).