

Increased Risk of Renal Malignancy in Patients with Moderate to Severe Atopic Dermatitis

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Database
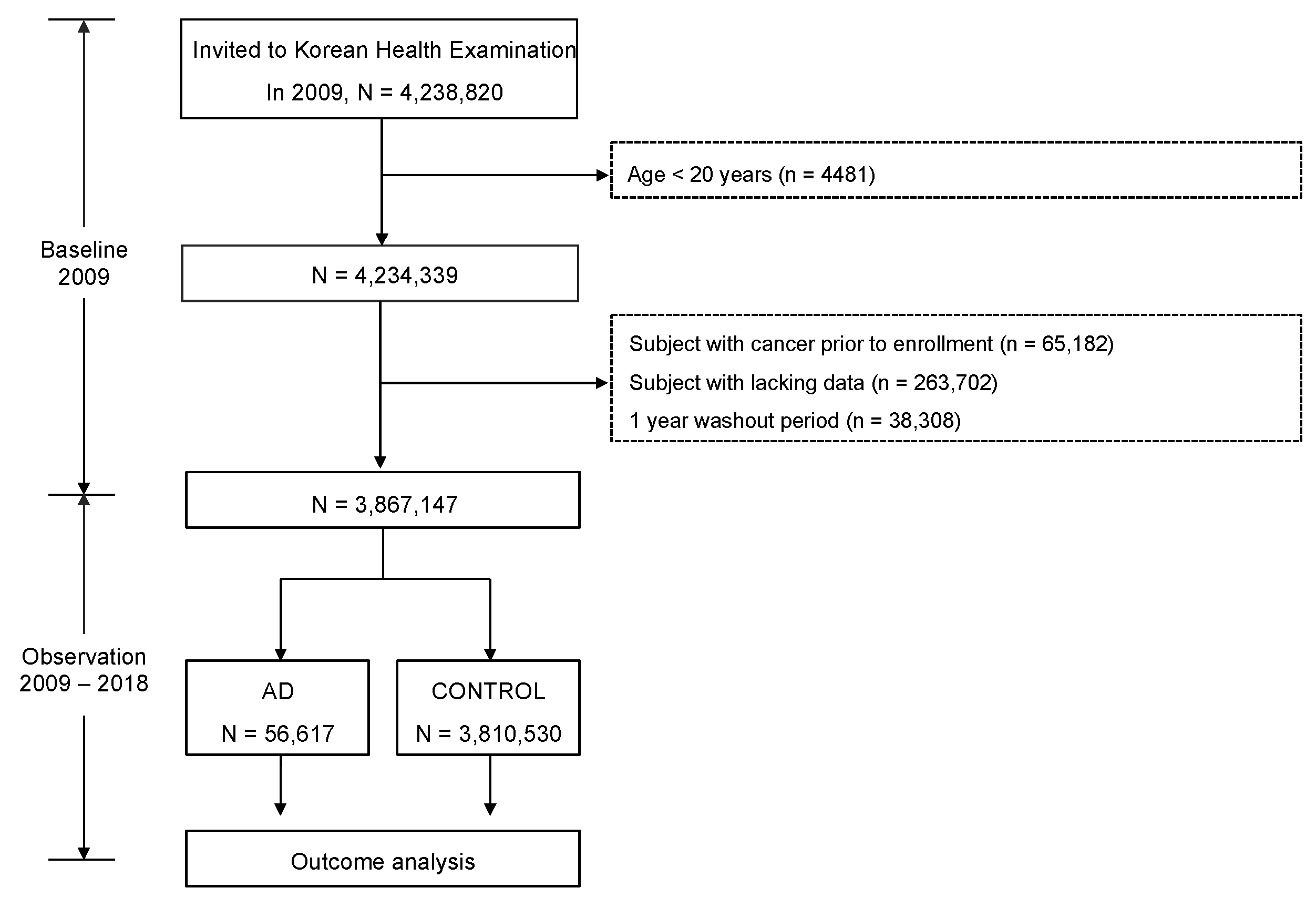
2.2. Study Population
2.3. Inclusion Criteria for AD
2.4. Data Collection
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population by AD Severity
3.2. Incidence Rate and the Risk of Malignancy in the Study Population by AD Severity
3.3. Incidence Rate and Risk of Malignancy in the Study Population by Treatment Modality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Weidinger, S.; Beck, L.A.; Bieber, T.; Kabashima, K.; Irvine, A.D. Atopic dermatitis. Nat. Rev. Dis. Primers 2018, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Silverberg, J.I.; Hanifin, J.M. Adult eczema prevalence and associations with asthma and other health and demographic factors: A us population-based study. J. Allergy Clin. Immunol. 2013, 132, 1132–1138. [Google Scholar] [CrossRef] [PubMed]
- Langan, S.M.; Irvine, A.D.; Weidinger, S. Atopic dermatitis. Lancet 2020, 396, 345–360. [Google Scholar] [CrossRef] [PubMed]
- Stefanovic, N.; Flohr, C.; Irvine, A.D. The exposome in atopic dermatitis. Allergy 2020, 75, 63–74. [Google Scholar] [CrossRef] [PubMed]
- Naghavi, M.; Abajobir, A.A.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abera, S.F.; Aboyans, V.; Adetokunboh, O.; Afshin, A.; Agrawal, A.; et al. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: A systematic analysis for the global burden of disease study 2016. Lancet 2017, 390, 1151–1210. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Rothenbacher, D.; Löw, M.; Stegmaier, C.; Brenner, H.; Diepgen, T.L. Atopic diseases, immunoglobulin e and risk of cancer of the prostate, breast, lung and colorectum. Int. J. Cancer 2006, 119, 695–701. [Google Scholar] [CrossRef] [PubMed]
- Hagströmer, L.; Ye, W.; Nyrén, O.; Emtestam, L. Incidence of cancer among patients with atopic dermatitis. Arch. Dermatol. 2005, 141, 1123–1127. [Google Scholar] [CrossRef]
- Arana, A.; Wentworth, C.E.; Fernández-Vidaurre, C.; Schlienger, R.G.; Conde, E.; Arellano, F.M. Incidence of cancer in the general population and in patients with or without atopic dermatitis in the U.K. Br. J. Dermatol. 2010, 163, 1036–1043. [Google Scholar] [CrossRef]
- Hwang, C.Y.; Chen, Y.J.; Lin, M.W.; Chen, T.J.; Chu, S.Y.; Chen, C.C.; Lee, D.D.; Chang, Y.T.; Wang, W.J.; Liu, H.N. Cancer risk in patients with allergic rhinitis, asthma and atopic dermatitis: A nationwide cohort study in Taiwan. Int. J. Cancer 2012, 130, 1160–1167. [Google Scholar] [CrossRef]
- Mansfield, K.E.; Schmidt, S.A.J.; Darvalics, B.; Mulick, A.; Abuabara, K.; Wong, A.Y.S.; Sørensen, H.T.; Smeeth, L.; Bhaskaran, K.; Dos Santos Silva, I.; et al. Association between atopic eczema and cancer in England and Denmark. JAMA Dermatol. 2020, 156, 1086–1097. [Google Scholar] [CrossRef]
- Wang, L.; Bierbrier, R.; Drucker, A.M.; Chan, A.W. Noncutaneous and cutaneous cancer risk in patients with atopic dermatitis: A systematic review and meta-analysis. JAMA Dermatol. 2020, 156, 158–171. [Google Scholar] [CrossRef] [PubMed]
- Herbert, S.; Haughton, R.; Nava, J.; Ji-Xu, A.; Le, S.T.; Maverakis, E. A review of topical probiotic therapy for atopic dermatitis. Clin. Exp. Dermatol. 2023, 48, 319–324. [Google Scholar] [CrossRef] [PubMed]
- Xie, A.; Chen, A.; Chen, Y.; Luo, Z.; Jiang, S.; Chen, D.; Yu, R. Lactobacillus for the treatment and prevention of atopic dermatitis: Clinical and experimental evidence. Front. Cell. Infect. Microbiol. 2023, 13, 1137275. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.H.; Drucker, A.M.; Lebwohl, M.; Silverberg, J.I. A systematic review of the safety and efficacy of systemic corticosteroids in atopic dermatitis. J. Am. Acad. Dermatol. 2018, 78, 733–740.e11. [Google Scholar] [CrossRef]
- Roekevisch, E.; Spuls, P.I.; Kuester, D.; Limpens, J.; Schmitt, J. Efficacy and safety of systemic treatments for moderate-to-severe atopic dermatitis: A systematic review. J. Allergy Clin. Immunol. 2014, 133, 429–438. [Google Scholar] [CrossRef] [PubMed]
- Sidbury, R.; Davis, D.M.; Cohen, D.E.; Cordoro, K.M.; Berger, T.G.; Bergman, J.N.; Chamlin, S.L.; Cooper, K.D.; Feldman, S.R.; Hanifin, J.M.; et al. Guidelines of care for the management of atopic dermatitis: Section 3. Management and treatment with phototherapy and systemic agents. J. Am. Acad. Dermatol. 2014, 71, 327–349. [Google Scholar] [CrossRef] [PubMed]
- Cheol Seong, S.; Kim, Y.-Y.; Khang, Y.-H.; Heon Park, J.; Kang, H.-J.; Lee, H.; Do, C.-H.; Song, J.-S.; Hyon Bang, J.; Ha, S.; et al. Data resource profile: The national health information database of the national health insurance service in South Korea. Int. J. Epidemiol. 2016, 46, 799–800. [Google Scholar] [CrossRef] [PubMed]
- Margolis, J.S.; Abuabara, K.; Bilker, W.; Hoffstad, O.; Margolis, D.J. Persistence of mild to moderate atopic dermatitis. JAMA Dermatol. 2014, 150, 593–600. [Google Scholar] [CrossRef]
- Drucker, A.M.; Wang, A.R.; Li, W.Q.; Sevetson, E.; Block, J.K.; Qureshi, A.A. The burden of atopic dermatitis: Summary of a report for the national eczema association. J. Investig. Dermatol. 2017, 137, 26–30. [Google Scholar] [CrossRef]
- Ballardini, N.; Östblom, E.; Wahlgren, C.F.; Kull, I. Mild eczema affects self-perceived health among pre-adolescent girls. Acta Derm. Venereol. 2014, 94, 312–316. [Google Scholar] [CrossRef]
- Holm, E.A.; Wulf, H.C.; Stegmann, H.; Jemec, G.B.E. Life quality assessment among patients with atopic eczema. Br. J. Dermatol. 2006, 154, 719–725. [Google Scholar] [CrossRef] [PubMed]
- Bickers, D.R.; Lim, H.W.; Margolis, D.; Weinstock, M.A.; Goodman, C.; Faulkner, E.; Gould, C.; Gemmen, E.; Dall, T. The burden of skin diseases: 2004 a joint project of the American academy of dermatology association and the society for investigative dermatology. J. Am. Acad. Dermatol. 2006, 55, 490–500. [Google Scholar] [CrossRef] [PubMed]
- Mack, T.M.; Yu, M.C.; Hanisch, R.; Henderson, B.E. Pancreas cancer and smoking, beverage consumption, and past medical history. J. Natl. Cancer Inst. 1986, 76, 49–60. [Google Scholar] [PubMed]
- Holly, E.A.; Eberle, C.A.; Bracci, P.M. Prior history of allergies and pancreatic cancer in the San Francisco Bay area. Am. J. Epidemiol. 2003, 158, 432–441. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.; Zens, M.S.; Duell, E.; Perry, A.E.; Chapman, M.S.; Karagas, M.R. History of allergy and atopic dermatitis in relation to squamous cell and basal cell carcinoma of the skin. Cancer Epidemiol. Biomark. Prev. 2015, 24, 749–754. [Google Scholar] [CrossRef] [PubMed]
- Cartwright, R.A.; McKinney, P.A.; O’Brien, C.; Richards, I.D.; Roberts, B.; Lauder, I.; Darwin, C.M.; Bernard, S.M.; Bird, C.C. Non-hodgkin’s lymphoma: Case control epidemiological study in Yorkshire. Leuk. Res. 1988, 12, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Jensen, A.O.; Svaerke, C.; Körmendiné Farkas, D.; Olesen, A.B.; Kragballe, K.; Sørensen, H.T. Atopic dermatitis and risk of skin cancer: A Danish nationwide cohort study (1977–2006). Am. J. Clin. Dermatol. 2012, 13, 29–36. [Google Scholar] [CrossRef]
- Halling-Overgaard, A.S.; Ravnborg, N.; Silverberg, J.I.; Egeberg, A.; Thyssen, J.P. Atopic dermatitis and cancer in solid organs: A systematic review and meta-analysis. J. Eur. Acad. Dermatol. Venereol. 2019, 33, e81–e82. [Google Scholar] [CrossRef]
- Castaing, M.; Youngson, J.; Zaridze, D.; Szeszenia-Dabrowska, N.; Rudnai, P.; Lissowska, J.; Fabiánová, E.; Mates, D.; Bencko, V.; Foretova, L.; et al. Is the risk of lung cancer reduced among eczema patients? Am. J. Epidemiol. 2005, 162, 542–547. [Google Scholar] [CrossRef]
- El-Zein, M.; Parent, M.E.; Kâ, K.; Siemiatycki, J.; St-Pierre, Y.; Rousseau, M.C. History of asthma or eczema and cancer risk among men: A population-based case-control study in Montreal, Quebec, Canada. Ann. Allergy Asthma Immunol. 2010, 104, 378–384. [Google Scholar] [CrossRef]
- Hsieh, J.J.; Purdue, M.P.; Signoretti, S.; Swanton, C.; Albiges, L.; Schmidinger, M.; Heng, D.Y.; Larkin, J.; Ficarra, V. Renal cell carcinoma. Nat. Rev. Dis. Primers 2017, 3, 17009. [Google Scholar] [CrossRef] [PubMed]
- Legendre, L.; Barnetche, T.; Mazereeuw-Hautier, J.; Meyer, N.; Murrell, D.; Paul, C. Risk of lymphoma in patients with atopic dermatitis and the role of topical treatment: A systematic review and meta-analysis. J. Am. Acad. Dermatol. 2015, 72, 992–1002. [Google Scholar] [CrossRef] [PubMed]
- Arellano, F.M.; Wentworth, C.E.; Arana, A.; Fernández, C.; Paul, C.F. Risk of lymphoma following exposure to calcineurin inhibitors and topical steroids in patients with atopic dermatitis. J. Investig. Dermatol. 2007, 127, 808–816. [Google Scholar] [CrossRef] [PubMed]
- Castellsague, J.; Kuiper, J.G.; Pottegård, A.; Anveden Berglind, I.; Dedman, D.; Gutierrez, L.; Calingaert, B.; van Herk-Sukel, M.P.; Hallas, J.; Sundström, A.; et al. A cohort study on the risk of lymphoma and skin cancer in users of topical tacrolimus, pimecrolimus, and corticosteroids (joint European longitudinal lymphoma and skin cancer evaluation—Joelle study). Clin. Epidemiol. 2018, 10, 299–310. [Google Scholar] [CrossRef] [PubMed]
- Kaae, J.; Szecsi, P.B.; Meldgaard, M.; Espersen, M.L.; Stender, S.; Johansen, J.D.; Bandier, J.; Thyssen, J.P.; Menné, T.; Nielsen, S.L.; et al. Individuals with complete filaggrin deficiency may have an increased risk of squamous cell carcinoma. Br. J. Dermatol. 2014, 170, 1380–1381. [Google Scholar] [CrossRef] [PubMed]
- Dotto, G.P.; Rustgi, A.K. Squamous cell cancers: A unified perspective on biology and genetics. Cancer Cell 2016, 29, 622–637. [Google Scholar] [CrossRef] [PubMed]
- Halling-Overgaard, A.S.; Kezic, S.; Jakasa, I.; Engebretsen, K.A.; Maibach, H.; Thyssen, J.P. Skin absorption through atopic dermatitis skin: A systematic review. Br. J. Dermatol. 2017, 177, 84–106. [Google Scholar] [CrossRef] [PubMed]
- Gao, P.S.; Rafaels, N.M.; Hand, T.; Murray, T.; Boguniewicz, M.; Hata, T.; Schneider, L.; Hanifin, J.M.; Gallo, R.L.; Gao, L.; et al. Filaggrin mutations that confer risk of atopic dermatitis confer greater risk for eczema herpeticum. J. Allergy Clin. Immunol. 2009, 124, 507–513.e7. [Google Scholar] [CrossRef]
- Miajlovic, H.; Fallon, P.G.; Irvine, A.D.; Foster, T.J. Effect of filaggrin breakdown products on growth of and protein expression by staphylococcus aureus. J. Allergy Clin. Immunol. 2010, 126, 1184–1190.e1183. [Google Scholar] [CrossRef]
- Beck, L.A.; Boguniewicz, M.; Hata, T.; Schneider, L.C.; Hanifin, J.; Gallo, R.; Paller, A.S.; Lieff, S.; Reese, J.; Zaccaro, D.; et al. Phenotype of atopic dermatitis subjects with a history of eczema herpeticum. J. Allergy Clin. Immunol. 2009, 124, 260–269.e7. [Google Scholar] [CrossRef]
- Langan, S.M.; Abuabara, K.; Henrickson, S.E.; Hoffstad, O.; Margolis, D.J. Increased risk of cutaneous and systemic infections in atopic dermatitis-a cohort study. J. Investig. Dermatol. 2017, 137, 1375–1377. [Google Scholar] [CrossRef] [PubMed]
- Cipolat, S.; Hoste, E.; Natsuga, K.; Quist, S.R.; Watt, F.M. Epidermal barrier defects link atopic dermatitis with altered skin cancer susceptibility. Elife 2014, 3, e01888. [Google Scholar] [CrossRef] [PubMed]
- Arellano, F.M.; Arana, A.; Wentworth, C.E.; Fernández-Vidaurre, C.; Schlienger, R.G.; Conde, E. Lymphoma among patients with atopic dermatitis and/or treated with topical immunosuppressants in the united kingdom. J. Allergy Clin. Immunol. 2009, 123, 1111–1116.e13. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.S.; Karagas, M.R.; Perry, A.E.; Spencer, S.K.; Nelson, H.H. Gene-drug interaction at the glucocorticoid receptor increases risk of squamous cell skin cancer. J. Investig. Dermatol. 2007, 127, 1868–1870. [Google Scholar] [CrossRef] [PubMed]
- Balkwill, F.; Mantovani, A. Inflammation and cancer: Back to virchow? Lancet 2001, 357, 539–545. [Google Scholar] [CrossRef] [PubMed]
- Pompei, R.; Lampis, G.; Ingianni, A.; Nonnis, D.; Ionta, M.T.; Massidda, B. Allergy and tumour outcome after primary cancer therapy. Int. Arch. Allergy Immunol. 2004, 133, 174–178. [Google Scholar] [CrossRef] [PubMed]
- Grivennikov, S.I.; Greten, F.R.; Karin, M. Immunity, inflammation, and cancer. Cell 2010, 140, 883–899. [Google Scholar] [CrossRef]
- De Visser, K.E.; Eichten, A.; Coussens, L.M. Paradoxical roles of the immune system during cancer development. Nat. Rev. Cancer 2006, 6, 24–37. [Google Scholar] [CrossRef]
- Coussens, L.M.; Werb, Z. Inflammation and cancer. Nature 2002, 420, 860–867. [Google Scholar] [CrossRef]
- Mantovani, A.; Allavena, P.; Sica, A.; Balkwill, F. Cancer-related inflammation. Nature 2008, 454, 436–444. [Google Scholar] [CrossRef]
- Allavena, P.; Garlanda, C.; Borrello, M.G.; Sica, A.; Mantovani, A. Pathways connecting inflammation and cancer. Curr. Opin. Genet. Dev. 2008, 18, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Lewandowska, A.M.; Rudzki, M.; Rudzki, S.; Lewandowski, T.; Laskowska, B. Environmental risk factors for cancer—Review paper. Ann. Agric. Environ. Med. 2019, 26, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D. Hallmarks of cancer: New dimensions. Cancer Discov. 2022, 12, 31–46. [Google Scholar] [CrossRef] [PubMed]
- Paller, A.S.; Fölster-Holst, R.; Chen, S.C.; Diepgen, T.L.; Elmets, C.; Margolis, D.J.; Pollock, B.H. No evidence of increased cancer incidence in children using topical tacrolimus for atopic dermatitis. J. Am. Acad. Dermatol. 2020, 83, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, K.; Schned, A.; Fortuny, J.; Heaney, J.; Marsit, C.; Kelsey, K.T.; Karagas, M.R. Glucocorticoid therapy and risk of bladder cancer. Br. J. Cancer 2009, 101, 1316–1320. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, H.T.; Mellemkjaer, L.; Nielsen, G.L.; Baron, J.A.; Olsen, J.H.; Karagas, M.R. Skin cancers and non-hodgkin lymphoma among users of systemic glucocorticoids: A population-based cohort study. J. Natl. Cancer Inst. 2004, 96, 709–711. [Google Scholar] [CrossRef] [PubMed]
- Ostenfeld, E.B.; Erichsen, R.; Thorlacius-Ussing, O.; Riis, A.H.; Sørensen, H.T. Use of systemic glucocorticoids and the risk of colorectal cancer. Aliment. Pharmacol. Ther. 2013, 37, 146–152. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | AD Severity | ||||
|---|---|---|---|---|---|
| No AD | Mild | Moderate to Severe | p-Value | ||
| 3,810,530 | 22,430 | 34,187 | |||
| Age, years | 46.96 ± 13.96 | 48.47 ± 15.21 | 46.46 ± 15.16 | <0.0001 | |
| Age, years (group) | n, (%) | <0.0001 | |||
| <40 | 1,203,545 (31.58) | 6815 (30.38) | 12,085 (35.35) | ||
| 40–64 | 1,826,410 (47.93) | 9556 (42.6) | 14,388 (42.09) | ||
| ≥65 | 780,575 (20.48) | 6059 (27.01) | 7714 (22.56) | ||
| Sex | n, (%) | <0.0001 | |||
| Male | 2,092,135 (54.9) | 10,127 (45.15) | 15,765 (46.11) | ||
| Female | 1,718,395 (45.1) | 12,303 (54.85) | 18,422 (53.89) | ||
| Smoking | n, (%) | <0.0001 | |||
| None | 2,258,682 (59.27) | 15,013 (66.93) | 22,143 (64.77) | ||
| Ex | 543,602 (14.27) | 3240 (14.44) | 4584 (13.41) | ||
| Current | 1,008,246 (26.46) | 4177 (18.62) | 7460 (21.82) | ||
| Drinking | n, (%) | <0.0001 | |||
| None | 1,948,697 (51.14) | 13,117 (58.48) | 18,910 (55.31) | ||
| Mild | 1,554,838 (40.8) | 8006 (35.69) | 13,081 (38.26) | ||
| Heavy | 306,995 (8.06) | 1307 (5.83) | 2196 (6.42) | ||
| Regular exercise | n, (%) | 679,684 (17.84) | 4155 (18.52) | 6020 (17.61) | 0.0148 |
| BMI, kg/m2 (group) | n, (%) | <0.0001 | |||
| <18.5 | 140,957 (3.7) | 933 (4.16) | 1509 (4.41) | ||
| 18.5–23 | 1,485,817 (38.99) | 8924 (39.79) | 14,097 (41.23) | ||
| 23–25 | 937,790 (24.61) | 5269 (23.49) | 8067 (23.6) | ||
| 25–30 | 1,110,011 (29.13) | 6499 (28.97) | 9408 (27.52) | ||
| ≥30 | 135,955 (3.57) | 805 (3.59) | 1106 (3.24) | ||
| BMI, kg/m2 | 23.71 ± 3.47 | 23.62 ± 3.28 | 23.49 ± 3.25 | <0.0001 | |
| Waist circumference, cm | 80.24 ± 9.51 | 79.87 ± 9.64 | 79.39 ± 9.53 | <0.0001 | |
| Diabetes mellitus | n, (%) | 330,158 (8.66) | 2525 (11.26) | 2757 (8.06) | <0.0001 |
| Hypertension | n, (%) | 1,022,277 (26.83) | 7132 (31.8) | 9022 (26.39) | <0.0001 |
| Dyslipidemia | n, (%) | 691,809 (18.16) | 4827 (21.52) | 6752 (19.75) | <0.0001 |
| CKD | n, (%) | 260,196 (6.83) | 1996 (8.9) | 2517 (7.36) | <0.0001 |
| SBP, mmHg | 122.45 ± 15.05 | 121.63 ± 15.12 | 121.25 ± 14.87 | <0.0001 | |
| DBP, mmHg | 76.33 ± 10.07 | 75.62 ± 10 | 75.47 ± 9.91 | <0.0001 | |
| Fasting glucose, mg/dL | 97.29 ± 23.93 | 97.45 ± 24.86 | 95.59 ± 21.84 | <0.0001 | |
| Total cholesterol, mg/dL | 195.37 ± 41.52 | 193.75 ± 44.78 | 195.33 ± 41.43 | <0.0001 | |
| HDL cholesterol, mg/dL | 56.45 ± 32.77 | 57.46 ± 37.24 | 57.74 ± 33.53 | <0.0001 | |
| LDL cholesterol, mg/dL | 121.34 ± 217.11 | 120.54 ± 208.62 | 121.15 ± 211.59 | 0.8456 | |
| TG, mg/dL | 112.86 (112.79–112.92) | 109.56 (108.73–110.4) | 109.52 (108.85–110.2) | <0.0001 | |
| Treatment | |||||
| Topical agents | n, (%) | - | 19,873 (88.6) | 25,626 (74.96) | <0.0001 |
| Systemic agents | n, (%) | ||||
| Steroid | - | - | 33,988 (99.42) | <0.0001 | |
| Azathioprine | - | - | 28 (0.08) | <0.0001 | |
| Cyclosporine | - | - | 430 (1.26) | <0.0001 | |
| Methotrexate | - | - | 64 (0.19) | <0.0001 | |
| Mofetil | - | - | 19 (0.06) | <0.0001 | |
| AD Severity | N | Event | Duration a | Rate b | Model 1 | p-Value | Model 2 | p-Value | Model 3 | p-Value | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Cancer | No AD | 3,810,530 | 201,458 | 30,708,388.67 | 6.56036 | 1 (Ref.) | <0.0001 | 1 (Ref.) | 0.0052 | 1 (Ref.) | 0.0036 |
| Mild | 22,430 | 1384 | 179,514.94 | 7.70966 | 1.175 (1.115, 1.239) | 1.061 (1.007, 1.119) | 1.061 (1.006, 1.118) | ||||
| Moderate to severe | 34,187 | 1899 | 274,374.31 | 6.9212 | 1.055 (1.008, 1.104) | 1.057 (1.01, 1.106) | 1.061 (1.014, 1.11) | ||||
| Renal cancer | No AD | 3,810,530 | 5157 | 31,355,301.55 | 0.16447 | 1 (Ref.) | 0.004 | 1 (Ref.) | 0.0015 | 1 (Ref.) | 0.0017 |
| Mild | 22,430 | 30 | 184,193.3 | 0.16287 | 0.99 (0.692, 1.418) | 0.92 (0.643, 1.318) | 0.897 (0.626, 1.284) | ||||
| Moderate to severe | 34,187 | 69 | 280,439.45 | 0.24604 | 1.496 (1.18, 1.897) | 1.54 (1.215, 1.953) | 1.533 (1.209, 1.944) |
| Treatment | N | Renal Cancer | Duration a | Rate b | HR (95% CI) | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Model 1 | p-Value | Model 2 | p-Value | Model 3 | p-Value | |||||
| No AD | 3,810,530 | 5157 | 31,355,301.55 | 0.16447 | 1 (Ref.) | 0.0035 | 1 (Ref.) | 0.0028 | 1 (Ref.) | 0.0034 |
| Only topical agents | 19,892 | 24 | 163,440.45 | 0.14684 | 0.893 (0.598, 1.334) | 0.847 (0.567, 1.265) | 0.828 (0.555, 1.237) | |||
| Systemic—Steroid | 33,988 | 68 | 278,813.78 | 0.24389 | 1.483 (1.168, 1.884) | 1.527 (1.202, 1.939) | 1.519 (1.196, 1.93) | |||
| Systemic—Others | 2737 | 7 | 22,378.52 | 0.3128 | 1.903 (0.907, 3.993) | 1.554 (0.741, 3.261) | 1.476 (0.703, 3.098) | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, J.; Oh, H.J.; Han, K.-D.; Gee, H.Y.; Lee, J.H. Increased Risk of Renal Malignancy in Patients with Moderate to Severe Atopic Dermatitis. Cancers 2023, 15, 5007. https://doi.org/10.3390/cancers15205007
Oh J, Oh HJ, Han K-D, Gee HY, Lee JH. Increased Risk of Renal Malignancy in Patients with Moderate to Severe Atopic Dermatitis. Cancers. 2023; 15(20):5007. https://doi.org/10.3390/cancers15205007
Chicago/Turabian StyleOh, Jongwook, Hyun Ju Oh, Kyung-Do Han, Heon Yung Gee, and Ji Hyun Lee. 2023. "Increased Risk of Renal Malignancy in Patients with Moderate to Severe Atopic Dermatitis" Cancers 15, no. 20: 5007. https://doi.org/10.3390/cancers15205007
APA StyleOh, J., Oh, H. J., Han, K.-D., Gee, H. Y., & Lee, J. H. (2023). Increased Risk of Renal Malignancy in Patients with Moderate to Severe Atopic Dermatitis. Cancers, 15(20), 5007. https://doi.org/10.3390/cancers15205007