
Gastric Cancer: Molecular Mechanisms, Novel Targets, and Immunotherapies: From Bench to Clinical Therapeutics

Abstract
:Simple Summary
Abstract
1. Introduction
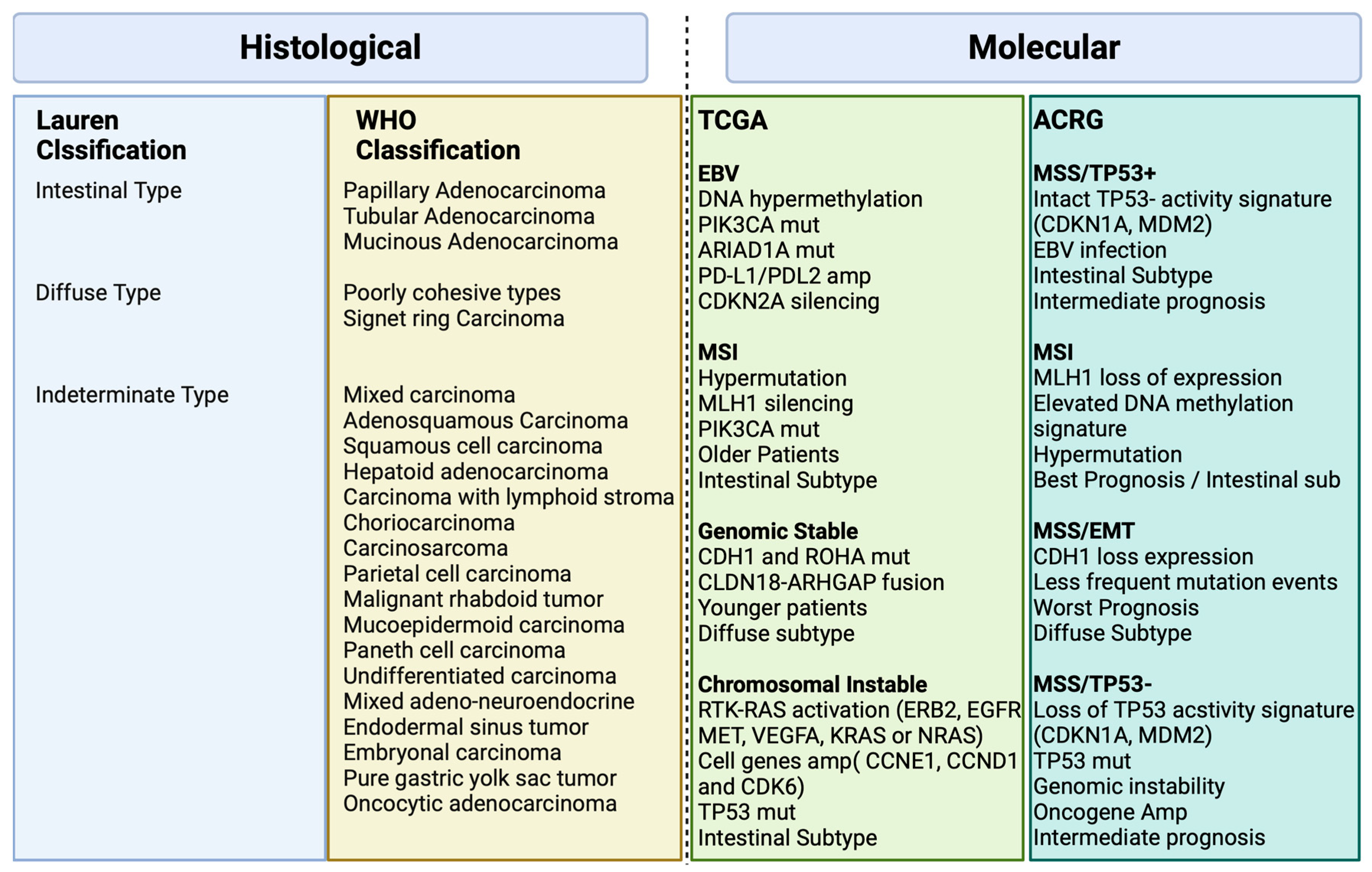
2. Histological and Molecular Classification
3. Risk Factors and Molecular Mechanisms
4. Molecular Mechanisms and Signaling Pathways in Gastric Cancer
4.1. MAPK Signaling Pathway
4.2. HER2 Signaling Pathway
4.3. PI3K/AKT/mTOR Signaling Pathway
4.4. HGF/c-MET Signaling Pathway
4.5. Wnt/β-Catenin Signaling Pathway
4.6. FGF/FGFR Signaling Pathway
4.7. HIF-1α Signaling Pathway
4.8. Claudin 18.2 Signaling Pathway
4.9. NF-κB Signaling Pathway
4.10. TGF-β Signaling Pathway
4.11. P53 Signaling Pathway
4.12. STAT3 Signaling Pathway
4.13. PDL-1/PD-1/CTLA-4
4.14. MSI High
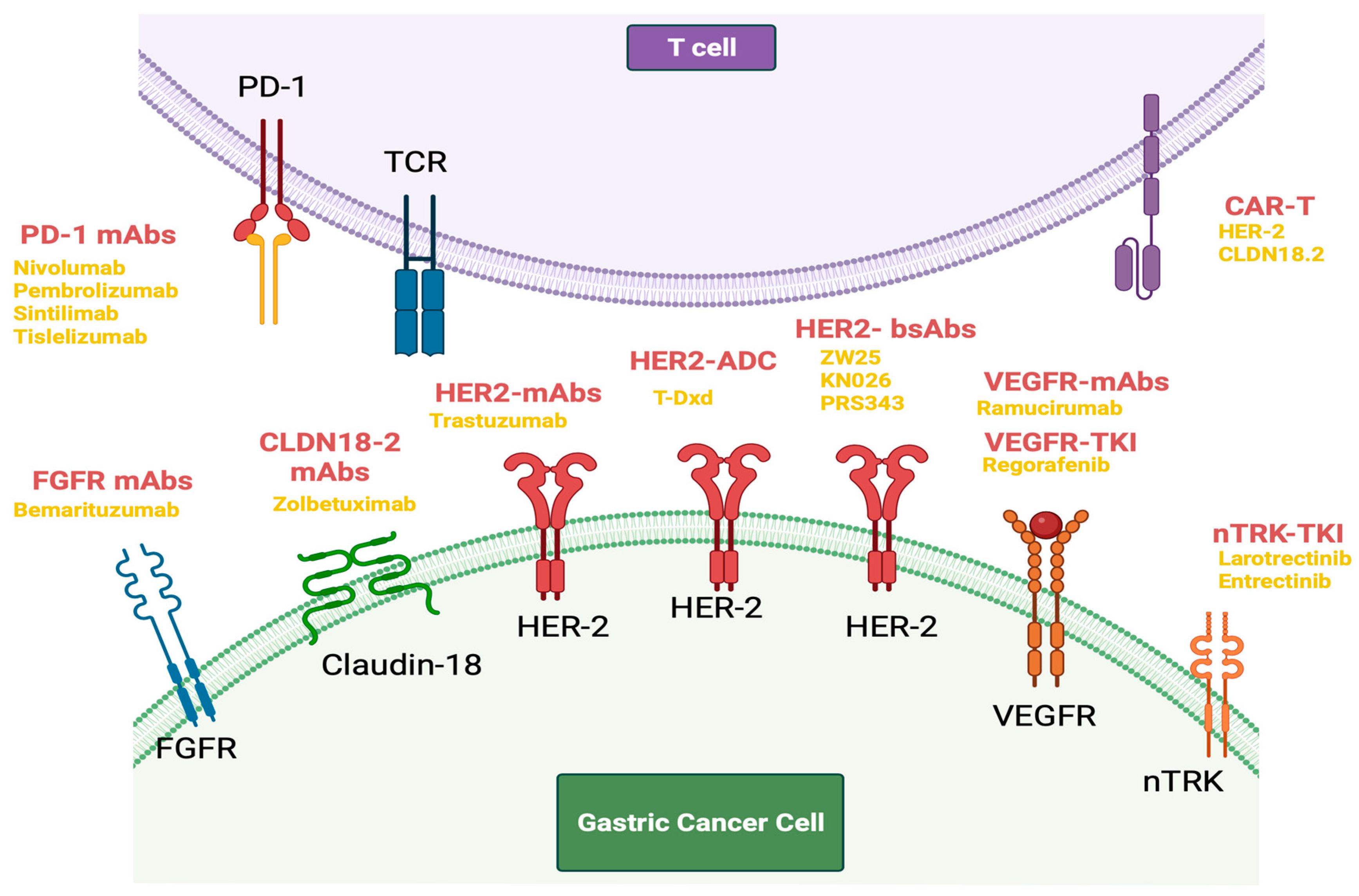
5. Novel Targeted Treatments in Gastric Cancer
5.1. HER-2-Directed Therapy
5.2. FGFR Agents
5.3. VEGF Agents
5.4. NTRK Agents
5.5. Claudin 18 Agents
6. Immune Checkpoint-Targeted Therapies and Other Immunotherapies
6.1. Immune Checkpoint Inhibitors in Metastatic/Advanced Gastric Cancer
6.2. Immune Checkpoint Inhibitors in Locally Advanced Gastric Cancer
6.3. Immune Checkpoint Combined with Target Therapies
6.4. Immune Checkpoint Inhibitors in Microsatellite Instability-High (MSI-H) Gastric Cancer
7. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Chia, N.; Tan, P. Molecular classification of gastric cancer. Ann. Oncol. 2016, 27, 763–769. [Google Scholar] [CrossRef] [PubMed]
- Reddavid, R.; Dagatti, S.; Franco, C.; Puca, L.; Tomatis, M.; Corso, S.; Giordano, S.; Degiuli, M. Molecularly targeted therapies for gastric cancer. state of the art. Cancers 2021, 13, 4094. [Google Scholar] [CrossRef] [PubMed]
- Bass, A.J.; Thorsson, V.; Shmulevich, I.; Reynolds, S.M.; Miller, M.; Bernard, B.; Hinoue, T.; Laird, P.W.; Curtis, C.; Shen, H.; et al. Comprehensive molecular characterization of gastric adenocarcinoma. Nature 2014, 513, 202–209. [Google Scholar] [CrossRef]
- Cristescu, R.; Lee, J.; Nebozhyn, M.; Kim, K.; Ting, J.C.; Wong, S.N.; Liu, J.; Yue, Y.; Wang, J.; Yu, K.; et al. Molecular analysis of gastric cancer identifies subtypes associated with distinct clinical outcomes. Nat. Med. 2015, 21, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Laurén, P. The two histological main types of gastric carcinoma: Diffuse and so-called intestinal-type carcinoma. Acta Pathol. Microbiol. Scand. 1965, 64, 31–49. [Google Scholar] [CrossRef]
- World Health Organization. WHO Classification of Tumours: Digestive System Tumours; Report No. 9283244990; World Health Organization (WHO): Geneva, Switzerland, 2019. [Google Scholar]
- Hansford, S.; Kaurah, P.; Li-Chang, H.; Woo, M.; Senz, J.; Pinheiro, H.; Schrader, K.A.; Schaeffer, D.F.; Shumansky, K.; Zogopoulos, G.; et al. Hereditary Diffuse Gastric cancer syndrome. JAMA Oncol. 2015, 1, 23. [Google Scholar] [CrossRef]
- Uemura, N.; Okamoto, S.; Yamamoto, S.; Matsumura, N.; Yamaguchi, S.; Yamakido, M.; Taniyama, K.; Sasaki, N.; Schlemper, R.J. Helicobacter pylori Infection and the Development of Gastric Cancer. N. Engl. J. Med. 2001, 345, 784–789. [Google Scholar] [CrossRef]
- Mukaisho, K.; Nakayama, T.; Hagiwara, T.; Hattori, T.; Sugihara, H. Two distinct etiologies of gastric cardia adenocarcinoma: Interactions among pH, Helicobacter pylori, and bile acids. Front. Microbiol. 2015, 6, 412. [Google Scholar] [CrossRef]
- Yao, X.; Zhang, X.; Luo, Q.; Gan, H.; Liu, Y.; Shao, S.; Mao, X. Helicobacter pylori regulates stomach diseases by activating cell pathways and DNA methylation of host cells. Front. Cell Dev. Biol. 2023, 11, 1187638. [Google Scholar] [CrossRef]
- Karimi, P.; Islami, F.; Anandasabapathy, S.; Freedman, N.D.; Kamangar, F. Gastric Cancer: Descriptive Epidemiology, risk factors, screening, and Prevention. Cancer Epidemiol. Biomark. Prev. 2014, 23, 700–713. [Google Scholar] [CrossRef] [PubMed]
- Naseem, M.; Barzi, A.; Brezden-Masley, C.; Puccini, A.; Berger, M.D.; Tokunaga, R.; Battaglin, F.; Soni, S.; McSkane, M.; Zhang, W.; et al. Outlooks on Epstein-Barr virus associated gastric cancer. Cancer Treat. Rev. 2018, 66, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Lima, Á.; Sousa, H.; Medeiros, R.; Nobre, A.M.D.; Machado, M. PD-L1 expression in EBV associated gastric cancer: A systematic review and meta-analysis. Discov. Oncol. 2022, 13, 19. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Huang, C. Mitogen-activated protein kinase signaling pathway and invasion and metastasis of gastric cancer. World J. Gastroenterol. 2015, 21, 11673. [Google Scholar] [CrossRef] [PubMed]
- Shen, B.; Li, M.; Wang, H.; Xin, L.; Xie, J. Expression and clinical significance of the RAS/RAF/MAPK cell signaling pathway in gastric cancer. Int. J. Clin. Exp. Med. 2018, 11, 11682–11689. [Google Scholar]
- Weston, C.R.; Davis, R.J. The JNK signal transduction pathway. Curr. Opin. Cell Biol. 2007, 19, 142–149. [Google Scholar] [CrossRef]
- Shibata, W.; Maeda, S.; Hikiba, Y.; Yanai, A.; Sakamoto, K.; Nakagawa, H.; Ogura, K.; Karin, M.; Omata, M. C-Jun NH2-Terminal kinase 1 is a critical regulator for the development of gastric cancer in mice. Cancer Res. 2008, 68, 5031–5039. [Google Scholar] [CrossRef]
- Guo, X.; Ma, N.; Wang, J.; Song, J.; Bu, X.; Cheng, Y.; Sun, K.; Xiong, H.; Jiang, G.; Zhang, B.; et al. Increased p38-MAPK is responsible for chemotherapy resistance in human gastric cancer cells. BMC Cancer 2008, 8, 375. [Google Scholar] [CrossRef]
- Kipkeeva, F.; Музаффарoва, Т.А.; Korotaeva, A.; Nikulin, M.P.; Гришина, К.А.; Mansorunov, D.; Apanovich, P.; Карпухин, А.В. MicroRNA in gastric cancer development: Mechanisms and biomarkers. Diagnostics 2020, 10, 891. [Google Scholar] [CrossRef]
- Rajadurai, P.; Fatt, H.K.; Ching, F.Y. Prevalence of HER2 positivity and its clinicopathological correlation in locally Advanced/Metastatic Gastric Cancer patients in Malaysia. J. Gastrointest. Cancer 2017, 49, 150–157. [Google Scholar] [CrossRef]
- Vaught, D.; Stanford, J.C.; Young, C.D.; Hicks, D.J.; Wheeler, F.; Rinehart, C.; Sanchez, V.; Koland, J.G.; Muller, W.J.; Arteaga, C.L.; et al. HER3 is required for HER2-Induced preneoplastic changes to the breast epithelium and tumor formation. Cancer Res. 2012, 72, 2672–2682. [Google Scholar] [CrossRef] [PubMed]
- Bang, Y.J.; Van Cutsem, E.; Feyereislova, A.; Chung, S.L.; Sawaki, A.; Lordick, F.; Ohtsu, A.; Omuro, Y.; Satoh, T.; Aprile, G.; et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): A phase 3, open-label, randomised controlled trial. Lancet 2010, 376, 687–697. [Google Scholar] [CrossRef]
- Matsuoka, T.; Yashiro, M. The role of PI3K/AKT/MTOR signaling in gastric carcinoma. Cancers 2014, 6, 1441–1463. [Google Scholar] [CrossRef]
- Karakas, B.; Bachman, K.E.; Park, B.H. Mutation of the PIK3CA oncogene in human cancers. Br. J. Cancer 2006, 94, 455–459. [Google Scholar] [CrossRef]
- Tapia, O.; Riquelme, I.; Leal, P.; Sandoval, A.; Aedo, S.; Weber, H.; Letelier, P.; Bellolio, E.; Villaseca, M.; García, P.; et al. The PI3K/AKT/mTOR pathway is activated in gastric cancer with potential prognostic and predictive significance. Virchows Arch. 2014, 465, 25–33. [Google Scholar] [CrossRef]
- Shi, J.; Yao, D.; Liu, W.; Wang, N.; Lv, H.; Zhang, G.; Ji, M.; Xu, L.; He, N.; Shi, B.; et al. Highly frequent PIK3CA amplification is associated with poor prognosis in gastric cancer. BMC Cancer 2012, 12, 50. [Google Scholar] [CrossRef] [PubMed]
- Vara, J.Á.F.; Casado, E.; De Castro, J.; Cejas, P.; Belda-Iniesta, C.; González-Barón, M. PI3K/Akt signalling pathway and cancer. Cancer Treat. Rev. 2004, 30, 193–204. [Google Scholar] [CrossRef] [PubMed]
- Baselga, J.; Phillips, G.D.L.; Verma, S.; Ro, J.; Huober, J.; Guardino, A.E.; Samant, M.; Olsen, S.; Haas, S.; Pegram, M.D. Relationship between Tumor Biomarkers and Efficacy in EMILIA, a Phase III Study of Trastuzumab Emtansine in HER2-Positive Metastatic Breast Cancer. Clin. Cancer Res. 2016, 22, 3755–3763. [Google Scholar] [CrossRef] [PubMed]
- Fu, J.; Su, X.; Li, Z.; Deng, L.; Liu, X.; Feng, X.; Peng, J. HGF/c-MET pathway in cancer: From molecular characterization to clinical evidence. Oncogene 2021, 40, 4625–4651. [Google Scholar] [CrossRef]
- Faiella, A.; Riccardi, F.; Cartenì, G.; Chiurazzi, M.; Onofrio, L. The emerging role of C-MET in carcinogenesis and clinical implications as a possible therapeutic target. J. Oncol. 2022, 2022, 5179182. [Google Scholar] [CrossRef]
- Marano, L.; Chiari, R.; Fabozzi, A.; De Vita, F.; Boccardi, V.; Roviello, G.; Petrioli, R.; Marrelli, D.; Roviello, F.; Patriti, A. c-Met targeting in advanced gastric cancer: An open challenge. Cancer Lett. 2015, 365, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.; Yu, Y.; Zhao, N.; Cui, J.; Li, W.; Liu, T. C-Met as a Prognostic marker in Gastric Cancer: A Systematic Review and Meta-Analysis. PLoS ONE 2013, 8, e79137. [Google Scholar] [CrossRef] [PubMed]
- Darsa, H.E.; Sayed, R.E.; Abdel-Rahman, O. MET Inhibitors for the Treatment of Gastric Cancer: What’s Their Potential? J. Exp. Pharmacol. 2020, 12, 349–361. [Google Scholar] [CrossRef]
- Li, Y.; Zhao, Y.; Li, Y.; Zhang, X.; Li, C.; Long, N.; Chen, X.; Bao, L.; Zhou, J.; Xie, Y. Gastrin-17 induces gastric cancer cell epithelial-mesenchymal transition via the Wnt/β-catenin signaling pathway. J. Physiol. Biochem. 2021, 77, 93–104. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Hu, G.; Wu, R.; Gong, N. High expression of miR-135b predicts malignant transformation and poor prognosis of gastric cancer. Life Sci. 2020, 257, 118133. [Google Scholar] [CrossRef]
- Ren, Y.; Guo, T.; Xu, J.; Liu, Y.; Huang, J. The novel target of esophageal squamous cell carcinoma: lncRNA GASL1 regulates cell migration, invasion and cell cycle stagnation by inactivating the Wnt3a/β-catenin signaling. Pathol. Res. Pract. 2021, 217, 153289. [Google Scholar] [CrossRef]
- Yu, Z.; Jiang, X.; Qin, L.; Deng, H.; Wang, J.; Ren, W.X.; Li, H.; Zhao, L.; Liu, H.; Hong, Y.; et al. A novel UBE2T inhibitor suppresses Wnt/β-catenin signaling hyperactivation and gastric cancer progression by blocking RACK1 ubiquitination. Oncogene 2020, 40, 1027–1042. [Google Scholar] [CrossRef]
- Ji, L.; Qian, W.; Gui, L.; Ji, Z.; Yin, P.; Lin, G.N.; Wang, Y.; Ma, B.; Gao, W. Blockade of Β-Catenin–Induced CCL28 suppresses gastric cancer progression via inhibition of treg cell infiltration. Cancer Res. 2020, 80, 2004–2016. [Google Scholar] [CrossRef]
- Takahashi, N.; Yamada, Y.; Taniguchi, H.; Fukahori, M.; Sasaki, Y.; Shoji, H.; Honma, Y.; Iwasa, S.; Takashima, A.; Kato, K.; et al. Clinicopathological features and prognostic roles of KRAS, BRAF, PIK3CA and NRAS mutations in advanced gastric cancer. BMC Res. Notes 2014, 7, 271. [Google Scholar] [CrossRef]
- Helsten, T.; Schwaederle, M.; Kurzrock, R. Fibroblast growth factor receptor signaling in hereditary and neoplastic disease: Biologic and clinical implications. Cancer Metastasis Rev. 2015, 34, 479–496. [Google Scholar] [CrossRef]
- Lengyel, C.G.; Hussain, S.; Seeber, A.; Nidhamalddin, S.J.; Trapani, D.; Habeeb, B.S.; Elfaham, E.; Mazher, S.; Seid, F.; Khan, S.Z.; et al. FGFR pathway inhibition in gastric cancer: The golden era of an old target? Life 2022, 12, 81. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Gao, L.; Zhu, W.; He, Q.; Liu, Y.; Chen, X.; Liu, J.; Lin, J.; Han-Zhang, H.; Yang, Z.; et al. A comprehensive pan-cancer study of fibroblast growth factor receptor aberrations in Chinese cancer patients. Ann. Transl. Med. 2020, 8, 1290. [Google Scholar] [CrossRef]
- Matsumoto, K.; Arao, T.; Hamaguchi, T.; Shimada, Y.; Kato, K.; Oda, I.; Taniguchi, H.; Koizumi, F.; Yanagihara, K.; Sasaki, H.; et al. FGFR2 gene amplification and clinicopathological features in gastric cancer. Br. J. Cancer 2012, 106, 727–732. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Wong, C.C.; Leung, K.T.; Wu, F.; Zhou, Y.; Tong, J.H.; Chan, R.L.; Li, H.; Wang, Y.; Yan, H.; et al. FGF18–FGFR2 signaling triggers the activation of c-Jun–YAP1 axis to promote carcinogenesis in a subgroup of gastric cancer patients and indicates translational potential. Oncogene 2020, 39, 6647–6663. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zhou, Y.; Huang, T.; Wu, F.; Pan, Y.; Dong, Y.; Wang, Y.; Chan, A.K.; Liu, L.; Kwan, J.S.H.; et al. FGF18, a prominent player in FGF signaling, promotes gastric tumorigenesis through autocrine manner and is negatively regulated by miR-590-5p. Oncogene 2018, 38, 33–46. [Google Scholar] [CrossRef]
- Wainberg, Z.A.; Enzinger, P.C.; Kang, Y.K.; Qin, S.; Yamaguchi, K.; Kim, I.H.; Saeed, A.; Oh, S.C.; Li, J.; Turk, H.M.; et al. Bemarituzumab in patients with FGFR2b-selected gastric or gastro-oesophageal junction adenocarcinoma (FIGHT): A randomised, double-blind, placebo-controlled, phase 2 study. Lancet Oncol. 2022, 23, 1430–1440. [Google Scholar] [CrossRef] [PubMed]
- Van Cutsem, E.; Bang, Y.; Mansoor, W.; Petty, R.; Chao, Y.; Cunningham, D.; Ferry, D.; Smith, N.R.; Frewer, P.; Ratnayake, J.; et al. A randomized, open-label study of the efficacy and safety of AZD4547 monotherapy versus paclitaxel for the treatment of advanced gastric adenocarcinoma with FGFR2 polysomy or gene amplification. Ann. Oncol. 2017, 28, 1316–1324. [Google Scholar] [CrossRef]
- Akanji, M.A.; Rotimi, D.; Adeyemi, O.S. Hypoxia-Inducible factors as an alternative source of treatment strategy for cancer. Oxid. Med. Cell. Longev. 2019, 2019, 8547846. [Google Scholar] [CrossRef]
- Zhu, C.; Huang, Q.; Liu, C.; Lin, X.; Xie, F. Prognostic value of HIF-1α expression in patients with gastric cancer. Mol. Biol. Rep. 2013, 40, 6055–6062. [Google Scholar] [CrossRef]
- Yukitoshi, S.; Oue, N.; Mitani, Y.; Yoshida, K.; Nakayama, H.; Yasui, W. Down-regulation of the claudin-18 gene, identified through serial analysis of gene expression data analysis, in gastric cancer with an intestinal phenotype. J. Pathol. 2006, 208, 633–642. [Google Scholar] [CrossRef]
- Türeci, Ö.; Mitnacht-Kraus, R.; Wöll, S.; Yamada, T.; Sahin, U. Characterization of zolbetuximab in pancreatic cancer models. OncoImmunology 2018, 8, e1523096. [Google Scholar] [CrossRef] [PubMed]
- Cao, W.; Xing, H.; Li, Y.; Tian, W.; Song, Y.; Jiang, Z.; Yu, J. Claudin18.2 is a novel molecular biomarker for tumor-targeted immunotherapy. Biomark. Res. 2022, 10, 38. [Google Scholar] [CrossRef] [PubMed]
- Ungureanu, B.S.; Lungulescu, C.; Pirici, D.; Turcu-Stiolica, A.; Gheonea, D.I.; Sacerdotianu, V.M.; Liliac, I.M.; Moraru, E.; Bende, F.; Saftoiu, A. Clinicopathologic Relevance of Claudin 18.2 Expression in Gastric Cancer: A Meta-Analysis. Front. Oncol. 2021, 11, 50. [Google Scholar] [CrossRef] [PubMed]
- Neumann, M.; Naumann, M. Beyond IκBs: Alternative regulation of NF-KB activity. FASEB J. 2007, 21, 2642–2654. [Google Scholar] [CrossRef]
- Takaya, S. Upregulation of Immune Checkpoint Molecules, PD-1 and LAG-3, on CD4+ and CD8+ T Cells after Gastric Cancer Surgery. PubMed Central (PMC). 1 March 2015. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4502424/ (accessed on 12 September 2023).
- Sokolova, O.; Naumann, M. NF-ΚB signaling in gastric cancer. Toxins 2017, 9, 119. [Google Scholar] [CrossRef]
- Morikawa, M.; Derynck, R.; Miyazono, K. TGF-Β and the TGF-Β family: Context-Dependent Roles in Cell and Tissue Physiology. Cold Spring Harb. Perspect. Biol. 2016, 8, a021873. [Google Scholar] [CrossRef]
- Klass, B.; Grobbelaar, A.O.; Rolfe, K. Transforming growth factor β1 signalling, wound healing and repair: A multifunctional cytokine with clinical implications for wound repair, a delicate balance. Postgrad. Med. J. 2009, 85, 9–14. [Google Scholar] [CrossRef]
- Hata, A.; Chen, Y. TGF-β Signaling from Receptors to Smads. Cold Spring Harb. Perspect. Biol. 2016, 8, a022061. [Google Scholar] [CrossRef]
- Ingaramo, M.; Sánchez, J.R.T.; Dekanty, A. Regulation and function of p53: A perspective from Drosophila studies. Mech. Dev. 2018, 154, 82–90. [Google Scholar] [CrossRef]
- Bockerstett, K.A.; Lewis, S.A.; Noto, C.; Ford, E.; Sáenz, J.B.; Jackson, N.; Ahn, T.; Mills, J.C.; DiPaolo, R.J. Single-Cell transcriptional analyses identify Lineage-Specific epithelial responses to inflammation and metaplastic development in the gastric corpus. Gastroenterology 2020, 159, 2116–2129.e4. [Google Scholar] [CrossRef]
- Wada, Y.; Takemura, K.; Tummala, P.; Uchida, K.; Kitagaki, K.; Furukawa, A.; Ishige, Y.; Ito, T.; Hara, Y.; Suzuki, T.; et al. Helicobacter pylori induces somatic mutations in TP 53 via overexpression of CHAC 1 in infected gastric epithelial cells. FEBS Open Bio. 2018, 8, 671–679. [Google Scholar] [CrossRef] [PubMed]
- Siveen, K.S.; Sikka, S.; Surana, R.; Dai, X.; Zhang, J.; Kumar, A.P.; Tan, B.K.; Sethi, G.; Bishayee, A. Targeting the STAT3 signaling pathway in cancer: Role of synthetic and natural inhibitors. Biochim. Biophys. Acta-Rev. Cancer 2014, 1845, 136–154. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Lv, X.; Guo, X.; Dong, Y.; Peng, P.; Huang, F.; Wang, P.; Zhang, H.; Zhou, J.; Wang, Y.; et al. Feedback activation of STAT3 limits the response to PI3K/AKT/mTOR inhibitors in PTEN-deficient cancer cells. Oncogenesis 2021, 10, 8. [Google Scholar] [CrossRef]
- Pandey, A.; Tripathi, S.C.; Shukla, S.; Mahata, S.; Vishnoi, K.; Misra, S.P.; Misra, V.; Mitra, S.; Dwivedi, M.; Bharti, A.C. Differentially localized survivin and STAT3 as markers of gastric cancer progression: Association with Helicobacter pylori. Cancer Rep. 2018, 1, e1004. [Google Scholar] [CrossRef] [PubMed]
- Yan, X.; Luo, Q.; Zhou, S.; Pan, W.; Zhang, L.; Yang, D. MicroRNA-375 reverses the expression of PD-L1 by inactivating the JAK2/STAT3 signaling pathways in gastric cancer. Clin. Res. Hepatol. Gastroenterol. 2021, 45, 101574. [Google Scholar] [CrossRef] [PubMed]
- Vogel, I.; Kasran, A.; Cremer, J.; Kim, Y.; Boon, L.; Van Gool, S.W.; Ceuppens, J.L. CD28/CTLA-4/B7 costimulatory pathway blockade affects regulatory T-cell function in autoimmunity. Eur. J. Immunol. 2015, 45, 1832–1841. [Google Scholar] [CrossRef]
- Carreno, B.M.; Carter, L.; Collins, M. Therapeutic opportunities in the B7/CD28 family of ligands and receptors. Curr. Opin. Pharmacol. 2005, 5, 424–430. [Google Scholar] [CrossRef]
- Wang, D.; Yanmei, G.; Yan, X.; Huo, C.; Wang, G.; Zhao, Y.; Teng, M.; Li, Y. Role of CD155/TIGIT in Digestive cancers: Promising cancer target for immunotherapy. Front. Oncol. 2022, 12, 844260. [Google Scholar] [CrossRef]
- Li, G.M. Mechanisms and functions of DNA mismatch repair. Cell Res. 2007, 18, 85–98. [Google Scholar] [CrossRef]
- Puliga, E.; Corso, S.; Pietrantonio, F.; Giordano, S. Microsatellite instability in Gastric Cancer: Between lights and shadows. Cancer Treat. Rev. 2021, 95, 102175. [Google Scholar] [CrossRef]
- Capelle, L.; Van Grieken, N.C.; Lingsma, H.F.; Steyerberg, E.W.; Klokman, W.J.; Bruno, M.J.; Vasen, H.F.A.; Kuipers, E.J. Risk and Epidemiological Time Trends of Gastric Cancer in Lynch Syndrome Carriers in The Netherlands. Gastroenterology 2010, 138, 487–492. [Google Scholar] [CrossRef]
- Corso, G.; Velho, S.; Paredes, J.; Pedrazzani, C.; Martins, D.; Milanezi, F.; Pascale, V.; Vindigni, C.; Pinheiro, H.; Leite, M.C.; et al. Oncogenic mutations in gastric cancer with microsatellite instability. Eur. J. Cancer 2011, 47, 443–451. [Google Scholar] [CrossRef] [PubMed]
- Grávalos, C.; Jimeno, A. HER2 in gastric cancer: A new prognostic factor and a novel therapeutic target. Ann. Oncol. 2008, 19, 1523–1529. [Google Scholar] [CrossRef] [PubMed]
- Roviello, G.; Generali, D. Pertuzumab therapy for HER2-positive metastatic gastric or gastro-oesophageal junction cancer. Lancet Oncol. 2018, 19, 1270–1272. [Google Scholar] [CrossRef] [PubMed]
- Swain, S.M.; Baselga, J.; Kim, S.; Ro, J.; Semiglazov, V.; Campone, M.; Ciruelos, E.; Ferrero, J.; Schneeweiss, A.; Heeson, S.; et al. Pertuzumab, trastuzumab, and docetaxel in HER2-Positive metastatic breast cancer. N. Engl. J. Med. 2015, 372, 724–734. [Google Scholar] [CrossRef]
- Tabernero, J.; Hoff, P.M.; Shen, L.; Ohtsu, A.; Shah, M.A.; Cheng, K.; Song, C.; Wu, H.; Eng-Wong, J.; Kim, K.; et al. Pertuzumab plus trastuzumab and chemotherapy for HER2-positive metastatic gastric or gastro-oesophageal junction cancer (JACOB): Final analysis of a double-blind, randomised, placebo-controlled phase 3 study. Lancet Oncol. 2018, 19, 1372–1384. [Google Scholar] [CrossRef] [PubMed]
- Satoh, T.; Xu, R.; Chung, H.C.; Sun, G.; Doi, T.; Xu, J.; Tsuji, A.; Omuro, Y.; Li, J.; Wang, J.; et al. Lapatinib Plus Paclitaxel Versus Paclitaxel Alone in the Second-Line Treatment of HER2-Amplified Advanced Gastric Cancer in Asian Populations: TyTAN—A Randomized, Phase III Study. J. Clin. Oncol. 2014, 32, 2039–2049. [Google Scholar] [CrossRef] [PubMed]
- Hecht, J.R.; Bang, Y.J.; Qin, S.; Chung, X.J.; Park, J.O.; Jeziorski, K.; Shparyk, Y.; Hoff, P.M.; Sobrero, A.; Salman, D.; et al. Lapatinib in combination with capecitabine plus oxaliplatin in human epidermal growth factor receptor 2–Positive advanced or metastatic gastric, esophageal, or gastroesophageal adenocarcinoma: TRIO-013/LOGIC—A randomized phase III trial. J. Clin. Oncol. 2016, 34, 443–451. [Google Scholar] [CrossRef]
- Meric-Bernstam, F.; Beeram, M.; Hamilton, E.; Oh, D.Y.; Hanna, D.L.; Kang, Y.K.; Elimova, E.; Chaves, J.; Goodwin, R.; Lee, J.; et al. Zanidatamab, a novel bispecific antibody, for the treatment of locally advanced or metastatic HER2-expressing or HER2-amplified cancers: A phase 1, dose-escalation and expansion study. Lancet Oncol. 2022, 23, 1558–1570. [Google Scholar] [CrossRef]
- Ku, G.; Elena, E.; Denlinger, C.S.; Mehta, R.; Lee, K.-W.; Iqbal, S.; Kang, Y.-K.; Oh, D.-Y.; Rha, S.Y.; Kim, Y.H.; et al. 1380P Phase (Ph) II study of zanidatamab + chemotherapy (chemo) in first-line (1L) HER2 expressing gastroesophageal adenocarcinoma (GEA). Ann. Oncol. 2021, 32, S1044–5. [Google Scholar] [CrossRef]
- Elimova, E.; Ajani, J.A.; Howard, A.B., III; Denlinger, C.S.; Iqbal, S.; Kang, Y.-K.; Hong, Y.; Kim, H.; Lee, K.-W.; Lin, B.; et al. T Zanidatamab + chemotherapy as first-line treatment for HER2-expressing metastatic gastroesophageal adenocarcinoma (mGEA). J. Clin. Oncol. 2023, 41 (Suppl. 4), 347–347. [Google Scholar] [CrossRef]
- Xu, J.; Ying, J.; Liu, R.; Wu, J.; Ye, F.; Xu, N.; Zhang, Y.; Zhao, R.; Xiang, X.; Wang, J.; et al. KN026 (anti-HER2 bispecific antibody) in patients with previously treated, advanced HER2-expressing gastric or gastroesophageal junction cancer. Eur. J. Cancer 2023, 178, 1–12. [Google Scholar] [CrossRef]
- Piha-Paul, S.; Bendell, J.; Tolcher, A.; Hurvitz, S.; Patnaik, A.; Shroff, R.; Pohlmann, P.; Zettl, M.; Hahn, N.; Krishnamurthy, A.; et al. O82 A phase 1 dose escalation study of PRS-343, a HER2/4–1BB bispecific molecule, in patients with HER2-positive malignancies. J. Immunother. Cancer 2020, 8 (Suppl. 1), A1–A2. [Google Scholar]
- Phillips, G.D.L.; Li, G.; Dugger, D.L.; Crocker, L.; Parsons, K.L.; Mai, E.; Blättler, W.A.; Lambert, J.M.; Chari, R.; Lutz, R.J.; et al. Targeting HER2-Positive Breast Cancer with Trastuzumab-DM1, an Antibody–Cytotoxic Drug Conjugate. Cancer Res. 2008, 68, 9280–9290. [Google Scholar] [CrossRef] [PubMed]
- Thuss-Patience, P.; Shah, M.A.; Ohtsu, A.; Van Cutsem, E.; Ajani, J.A.; Castro, H.R.; Mansoor, W.; Chung, B.G.; Shitara, K.; Phillips, G.D.L.; et al. Trastuzumab emtansine versus taxane use for previously treated HER2-positive locally advanced or metastatic gastric or gastro-oesophageal junction adenocarcinoma (GATSBY): An international randomised, open-label, adaptive, phase 2/3 study. Lancet Oncol. 2017, 18, 640–653. [Google Scholar] [CrossRef]
- Cortés, J.; Kim, S.; Chung, W.K.; Im, S.; Park, Y.H.; Hegg, R.; Kim, M.H.; Tseng, L.; Petry, V.; Chung, C.; et al. Trastuzumab Deruxtecan versus Trastuzumab Emtansine for Breast Cancer. N. Engl. J. Med. 2022, 386, 1143–1154. [Google Scholar] [CrossRef]
- Shitara, K.; Bang, Y.; Iwasa, S.; Sugimoto, N.; Ryu, M.; Sakai, D.; Chung, H.C.; Kawakami, H.; Yabusaki, H.; Lee, J.; et al. Trastuzumab deruxtecan in previously treated HER2-Positive gastric cancer. N. Engl. J. Med. 2020, 382, 2419–2430. [Google Scholar] [CrossRef]
- Yamaguchi, K.; Bang, Y.; Iwasa, S.; Sugimoto, N.; Ryu, M.; Sakai, D.; Chung, H.C.; Kawakami, H.; Yabusaki, H.; Lee, J.; et al. Trastuzumab deruxtecan in Anti–Human Epidermal Growth Factor receptor 2 Treatment–Naive patients with human epidermal growth factor receptor 2–Low gastric or gastroesophageal junction adenocarcinoma: Exploratory cohort results in a phase II trial. J. Clin. Oncol. 2023, 41, 816–825. [Google Scholar] [CrossRef]
- Pietrantonio, F.; Caporale, M.; Morano, F.; Scartozzi, M.; Gloghini, A.; De Vita, F.; Giommoni, E.; Fornaro, L.; Aprile, G.; Melisi, D.; et al. HER2 loss in HER2-positive gastric or gastroesophageal cancer after trastuzumab therapy: Implication for further clinical research. Int. J. Cancer 2016, 139, 2859–2864. [Google Scholar] [CrossRef]
- Van Cutsem, E.; Di Bartolomeo, M.; Smyth, E.; Chau, I.; Park, H.; Siena, S.; Lonardi, S.; Wainberg, Z.A.; Ajani, J.A.; Chao, J.; et al. Trastuzumab deruxtecan in patients in the USA and Europe with HER2-positive advanced gastric or gastroesophageal junction cancer with disease progression on or after a trastuzumab-containing regimen (DESTINY-Gastric02): Primary and updated analyses from a single-arm, phase 2 study. Lancet Oncol. 2023, 24, 744–756. [Google Scholar] [CrossRef]
- Sun, J.; Li, X.; Chen, P.; Gao, Y. From Anti-HER-2 to Anti-HER-2-CAR-T cells: An evolutionary immunotherapy approach for gastric cancer. J. Inflamm. Res. 2022, 15, 4061–4085. [Google Scholar] [CrossRef] [PubMed]
- Smyth, E.; Chao, J.; Muro, K.; Yen, P.; Yanes, R.E.; Zahlten-Kumeli, A.; Rha, S.Y. Trial in progress: Phase 3 study of bemarituzumab + mFOLFOX6 versus placebo + mFOLFOX6 in previously untreated advanced gastric or gastroesophageal junction (GEJ) cancer with FGFR2b overexpression (FORTITUDE-101). J. Clin. Oncol. 2022, 40 (Suppl. 16), TPS4164. [Google Scholar] [CrossRef]
- Young, K.; Smyth, E.; Chau, I. Ramucirumab for advanced gastric cancer or gastro-oesophageal junction adenocarcinoma. Ther. Adv. Gastroenterol. 2015, 8, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, C.S.; Tomášek, J.; Yong, C.J.; Dumitru, F.; Passalacqua, R.; Goswami, C.; Safran, H.; Santos, L.V.D.; Aprile, G.; Ferry, D.; et al. Ramucirumab monotherapy for previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (REGARD): An international, randomised, multicentre, placebo-controlled, phase 3 trial. Lancet 2014, 383, 31–39. [Google Scholar] [CrossRef]
- Wilke, H.; Muro, K.; Van Cutsem, E.; Oh, S.C.; Bodoky, G.; Shimada, Y.; Hironaka, S.; Sugimoto, N.; Lipatov, O.; Kim, T.Y.; et al. Ramucirumab plus paclitaxel versus placebo plus paclitaxel in patients with previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (RAINBOW): A double-blind, randomised phase 3 trial. Lancet Oncol. 2014, 15, 1224–1235. [Google Scholar] [CrossRef]
- Pavlakis, N.; Sjoquist, K.M.; Martin, A.J.; Tsobanis, E.; Yip, S.; Kang, Y.K.; Bang, Y.J.; Alcindor, T.; O’Callaghan, C.J.; Burnell, M.J.; et al. Regorafenib for the Treatment of Advanced Gastric Cancer (INTEGRATE): A Multinational Placebo-Controlled Phase II Trial. J. Clin. Oncol. 2016, 34, 2728–2735. [Google Scholar] [CrossRef]
- Lam, L.L.; Pavlakis, N.; Shitara, K.; Sjoquist, K.M.; Martin, A.; Yip, S.; Kang, Y.; Bang, Y.; Chen, L.; Moehler, M.; et al. INTEGRATE II: Randomised phase III controlled trials of regorafenib containing regimens versus standard of care in refractory Advanced Gastro-Oesophageal Cancer (AGOC): A study by the Australasian Gastro-Intestinal Trials Group (AGITG). BMC Cancer 2023, 23, 180. [Google Scholar] [CrossRef]
- Li, J.; Qin, S.; Xu, J.; Xiong, J.; Wu, C.; Bai, Y.; Liu, W.; Tong, J.; Liu, Y.; Xu, R.; et al. Randomized, Double-Blind, Placebo-Controlled phase III trial of Apatinib in patients with Chemotherapy-Refractory advanced or metastatic adenocarcinoma of the stomach or gastroesophageal junction. J. Clin. Oncol. 2016, 34, 1448–1454. [Google Scholar] [CrossRef]
- Drilon, A.; Laetsch, T.W.; Kummar, S.; DuBois, S.G.; Lassen, U.; Demetri, G.D.; Nathenson, M.J.; Doebele, R.C.; Farago, A.F.; Pappo, A.S.; et al. Efficacy of Larotrectinib inTRKFusion–Positive Cancers in Adults and Children. N. Engl. J. Med. 2018, 378, 731–739. [Google Scholar] [CrossRef]
- Doebele, R.C.; Drilon, A.; Paz-Ares, L.; Siena, S.; Shaw, A.T.; Farago, A.F.; Blakely, C.M.; Seto, T.; Cho, B.C.; Tosi, D.; et al. Entrectinib in patients with advanced or metastatic NTRK fusion-positive solid tumours: Integrated analysis of three phase 1–2 trials. Lancet Oncol. 2020, 21, 271–282. [Google Scholar] [CrossRef]
- Shitara, K.; Lordick, F.; Bang, Y.; Enzinger, P.C.; Ilson, D.H.; Shah, M.A.; Van Cutsem, E.; Xu, R.; Aprile, G.; Xu, J.; et al. Zolbetuximab plus mFOLFOX6 in patients with CLDN18.2-positive, HER2-negative, untreated, locally advanced unresectable or metastatic gastric or gastro-oesophageal junction adenocarcinoma (SPOTLIGHT): A multicentre, randomised, double-blind, phase 3 trial. Lancet 2023, 401, 1655–1668. [Google Scholar] [CrossRef] [PubMed]
- Xu, R.; Shitara, K.; Ajani, J.A.; Bang, Y.; Enzinger, P.C.; Ilson, D.H.; Lordick, F.; Van Cutsem, E.; Plazas, J.G.; Huang, J.; et al. Zolbetuximab + CAPOX in 1L claudin-18.2+ (CLDN18.2+)/HER2− locally advanced (LA) or metastatic gastric or gastroesophageal junction (mG/GEJ) adenocarcinoma: Primary phase 3 results from GLOW. J. Clin. Oncol. 2023, 41 (Suppl. 36), 405736. [Google Scholar] [CrossRef]
- Xu, R.; Wei, X.; Zhang, D.; Qiu, M.; Zhang, Y.; Zhao, H.; Chen, B.; Yan, J. A phase 1a dose-escalation, multicenter trial of anti-claudin 18.2 antibody drug conjugate CMG901 in patients with resistant/refractory solid tumors. J. Clin. Oncol. 2023, 41 (Suppl. 4), 352. [Google Scholar] [CrossRef]
- Wang, Y.; Gong, J.; Lin, R.; Zhao, S.; Wang, J.; Wang, Q.; Zhang, Y.; Su, D.; Zhang, J.; Dong, Q.; et al. First-in-human dose escalation and expansion study of SYSA1801, an antibody-drug conjugate targeting claudin 18.2 in patients with resistant/refractory solid tumors. J. Clin. Oncol. 2023, 41 (Suppl. 16), 3016. [Google Scholar] [CrossRef]
- Brar, G.; Shah, M.A. The role of pembrolizumab in the treatment of PD-L1 expressing gastric and gastroesophageal junction adenocarcinoma. Ther. Adv. Gastroenterol. 2019, 12, 175628481986976. [Google Scholar] [CrossRef]
- Bang, Y.J.; Kang, Y.K.; Catenacci, D.V.; Muro, K.; Fuchs, C.S.; Geva, R.; Hara, H.; Golan, T.; Garrido, M.; Jalal, S.I.; et al. Pembrolizumab alone or in combination with chemotherapy as first-line therapy for patients with advanced gastric or gastroesophageal junction adenocarcinoma: Results from the phase II nonrandomized KEYNOTE-059 study. Gastric Cancer 2019, 22, 828–837. [Google Scholar] [CrossRef]
- Shitara, K.; Van Cutsem, E.; Bang, Y.J.; Fuchs, C.S.; Wyrwicz, L.; Lee, M.H.; Kudaba, I.; Garrido, M.; Chung, L.J.; Castro, H.R.; et al. Efficacy and Safety of Pembrolizumab or Pembrolizumab Plus Chemotherapy vs. Chemotherapy Alone for Patients With First-line, Advanced Gastric Cancer. JAMA Oncol. 2020, 6, 1571. [Google Scholar] [CrossRef]
- Rha, S.; Wyrwicz, L.; Weber, P.Y.; Bai, Y.; Ryu, M.; Lee, J.; Rivera, F.; Alves, G.; Garrido, M.; Shiu, K.K.; et al. VP1-2023: Pembrolizumab (pembro) plus chemotherapy (chemo) as first-line therapy for advanced HER2-negative gastric or gastroesophageal junction (G/GEJ) cancer: Phase III KEYNOTE-859 study. Ann. Oncol. 2023, 34, 319–320. [Google Scholar] [CrossRef]
- Kang, Y.; Chen, L.; Ryu, M.; Oh, D.; Oh, S.C.; Chung, H.C.; Lee, K.; Omori, T.; Shitara, K.; Sakuramoto, S.; et al. Nivolumab plus chemotherapy versus placebo plus chemotherapy in patients with HER2-negative, untreated, unresectable advanced or recurrent gastric or gastro-oesophageal junction cancer (ATTRACTION-4): A randomised, multicentre, double-blind, placebo-controlled, phase 3 trial. Lancet 2022, 23, 234–247. [Google Scholar] [CrossRef]
- Janjigian, Y.Y.; Shitara, K.; Moehler, M.; Garrido, M.; Salman, P.; Shen, L.; Wyrwicz, L.; Yamaguchi, K.; Skoczylas, T.; Bragagnoli, A.C.; et al. First-line nivolumab plus chemotherapy versus chemotherapy alone for advanced gastric, gastro-oesophageal junction, and oesophageal adenocarcinoma (CheckMate 649): A randomised, open-label, phase 3 trial. Lancet 2021, 398, 27–40. [Google Scholar] [CrossRef]
- Xu, J.; Jiang, H.; Pan, Y.; Gu, K.; Cang, S.; Han, L.; Shu, Y.; Li, J.; Zhao, J.; Pan, H.; et al. LBA53 Sintilimab plus chemotherapy (chemo) versus chemo as first-line treatment for advanced gastric or gastroesophageal junction (G/GEJ) adenocarcinoma (ORIENT-16): First results of a randomized, double-blind, phase III study. Ann. Oncol. 2021, 32, S1331. [Google Scholar] [CrossRef]
- Li, S.; Yu, W.; Xie, F.; Luo, H.; Liu, Z.; Lv, W.; Shi, D.; Yu, D.; Gao, P.; Chen, C.; et al. Neoadjuvant therapy with immune checkpoint blockade, antiangiogenesis, and chemotherapy for locally advanced gastric cancer. Nat. Commun. 2023, 14, 8. [Google Scholar] [CrossRef] [PubMed]
- André, T.; Tougeron, D.; Piessen, G.; De La Fouchardière, C.; Louvet, C.; Adenis, A.; Jary, M.; Tournigand, C.; Aparicio, T.; Desramé, J.; et al. Neoadjuvant nivolumab plus ipilimumab and adjuvant nivolumab in localized deficient mismatch Repair/Microsatellite Instability–High gastric or esophagogastric junction adenocarcinoma: The GERCOR NEONIPIGA Phase II study. J. Clin. Oncol. 2023, 41, 255–265. [Google Scholar] [CrossRef]
- Kelly, R.J.; Ajani, J.A.; Kużdżał, J.; Zander, T.; Van Cutsem, E.; Piessen, G.; Mendez, G.; Feliciano, J.; Motoyama, S.; Lièvre, A.; et al. Adjuvant nivolumab in resected esophageal or gastroesophageal junction cancer. N. Engl. J. Med. 2021, 384, 1191–1203. [Google Scholar] [CrossRef]
- Al-Batran, S.; Lorenzen, S.; Thuss-Patience, P.; Homann, N.; Schenk, M.; Lindig, U.; Heuer, V.; Kretzschmar, A.; Goekkurt, E.; Haag, G.M.; et al. Surgical and pathological outcome, and pathological regression, in patients receiving perioperative atezolizumab in combination with FLOT chemotherapy versus FLOT alone for resectable esophagogastric adenocarcinoma: Interim results from DANTE, a randomized, multicenter, phase IIb trial of the FLOT-AIO German Gastric Cancer Group and Swiss SAKK. J. Clin. Oncol. 2022, 40 (Suppl. 16), 4003. [Google Scholar] [CrossRef]
- Janjigian, Y.Y.; Van Cutsem, E.; Muro, K.; Wainberg, Z.A.; Al-Batran, S.; Hyung, W.J.; Molena, D.; Evans, B.; Ruscica, D.; Robbins, S.H.; et al. MATTERHORN: Efficacy and safety of neoadjuvant-adjuvant durvalumab and FLOT chemotherapy in resectable gastric and gastroesophageal junction cancer—A randomized, double-blind, placebo-controlled, phase 3 study. J. Clin. Oncol. 2021, 39 (Suppl. 15), TPS4151. [Google Scholar] [CrossRef]
- Terashima, M.; Kang, Y.; Kim, Y.; Boku, N.; Chung, H.C.C.; Chen, J.; Ji, J.; Yeh, T.; Chen, L.; Ryu, M.; et al. ATTRACTION-5: A phase 3 study of nivolumab plus chemotherapy as postoperative adjuvant treatment for pathological stage III (pStage III) gastric or gastroesophageal junction (G/GEJ) cancer. J. Clin. Oncol. 2023, 41 (Suppl. 16), 4000. [Google Scholar] [CrossRef]
- Bang, Y.J.; Van Cutsem, E.; Fuchs, C.S.; Ohtsu, A.; Tabernero, J.; Ilson, D.H.; Hyung, W.J.; Strong, V.E.; Goetze, T.O.; Yoshikawa, T.; et al. KEYNOTE-585: Phase III study of perioperative chemotherapy with or without pembrolizumab for gastric cancer. Future Oncol. 2019, 15, 943–952. [Google Scholar] [CrossRef]
- Merck Provides Update on Phase 3 KEYNOTE-585 Trial in Locally Advanced Resectable Gastric and Gastroesophageal Junction (GEJ) Adenocarcinoma-June 2023. Available online: https://www.merck.com/news/merck-provides-update-on-phase-3-keynote-585-trial-in-locally-advanced-resectable-gastric-and-gastroesophageal-junction-gej-adenocarcinoma/ (accessed on 12 September 2023).
- Müller, P.; Kreuzaler, M.; Khan, T.A.; Thommen, D.S.; Martin, K.; Glatz, K.; Savic, S.; Harbeck, N.; Nitz, U.; Gluz, O.; et al. Trastuzumab emtansine (T-DM1) renders HER2 + breast cancer highly susceptible to CTLA-4/PD-1 blockade. Sci. Transl. Med. 2015, 7, 315ra188. [Google Scholar] [CrossRef]
- Janjigian, Y.Y.; Maron, S.B.; Chatila, W.K.; Millang, B.M.; Chavan, S.S.; Alterman, C.; Chou, J.F.; Segal, M.; Simmons, M.Z.; Momtaz, P.; et al. First-line pembrolizumab and trastuzumab in HER2-positive oesophageal, gastric, or gastro-oesophageal junction cancer: An open-label, single-arm, phase 2 trial. Lancet Oncol. 2020, 21, 821–831. [Google Scholar] [CrossRef]
- Janjigian, Y.Y.; Kawazoe, A.; Yañez, P.; Li, N.; Lonardi, S.; Kolesnik, O.; Barajas, O.; Bai, Y.; Shen, L.; Tang, Y.; et al. The KEYNOTE-811 trial of dual PD-1 and HER2 blockade in HER2-positive gastric cancer. Nature 2021, 600, 727–730. [Google Scholar] [CrossRef] [PubMed]
- Tabernero, J.; Elimova, E.; Ku, G.Y.; Shitara, K.; Shen, L.; Liu, T.; Lin, X.; Boyken, L.; Li, H.; Grim, J.E.; et al. P-26 HERIZON-GEA-01: A phase 3 study of zanidatamab in combination with chemotherapy with or without tislelizumab in first-line human epidermal growth factor receptor 2 positive (HER2+) advanced/metastatic gastroesophageal adenocarcinoma (GEA). Ann. Oncol. 2022, 33, S256. [Google Scholar] [CrossRef]
- Bonneville, R.; Krook, M.A.; Kautto, E.A.; Miya, J.; Wing, M.R.; Chen, H.; Reeser, J.W.; Yu, L.; Roychowdhury, S. Landscape of microsatellite instability across 39 cancer types. JCO Precis. Oncol. 2017, 1, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Vrána, D.; Matzenauer, M.; Neoral, C.; Aujeský, R.; Vrba, R.; Melichar, B.; Rušarová, N.; Bartoušková, M.; Jankowski, J.A. From tumor immunology to immunotherapy in gastric and esophageal cancer. Int. J. Mol. Sci. 2018, 20, 13. [Google Scholar] [CrossRef]
- Janjigian, Y.Y.; Shitara, K.; Moehler, M.; Garrido, M.; Gallardo, C.; Shen, L.; Yamaguchi, K.; Wyrwicz, L.; Skoczylas, T.; Bragagnoli, A.S.C.; et al. Nivolumab (NIVO) plus chemotherapy (chemo) vs chemo as first-line (1L) treatment for advanced gastric cancer/gastroesophageal junction cancer/esophageal adenocarcinoma (GC/GEJC/EAC): 3-year follow-up from CheckMate 649. J. Clin. Oncol. 2023, 41 (Suppl. 4), 291. [Google Scholar] [CrossRef]
- Pietrantonio, F.; Raimondi, A.; Lonardi, S.; Murgioni, S.; Cardellino, G.G.; Tamberi, S.; Strippoli, A.; Palermo, F.; Prisciandaro, M.; Randon, G.; et al. INFINITY: A multicentre, single-arm, multi-cohort, phase II trial of tremelimumab and durvalumab as neoadjuvant treatment of patients with microsatellite instability-high (MSI) resectable gastric or gastroesophageal junction adenocarcinoma (GAC/GEJAC). J. Clin. Oncol. 2023, 41 (Suppl. 4), 358. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Molecular Alteration | Trial | Phase | Patient Population | Treatment | Median PFS (Months) | Median OS (Months) |
|---|---|---|---|---|---|---|
| HER 2 Amplification | ToGA | III | Treatment-naive | Capecitabine or 5FU + Ciplastin | 5.5 | 11.1 |
| Capecitabine/5FU + Cisplatin + Trastuzumab | 6.7 | 13.8 | ||||
| DESTINY GASTRIC 01 | II | Pretreated (3rd line or later) | Trastuzumab deruxtecan | 5.6 | 12.5 | |
| Chemotherapy (Irinotecan or Paclitaxel) | 3.5 | 8.4 | ||||
| DESTINY-GASTRIC 02 | II | Pretreated (2nd Line) | Trastuzumab deruxtecan | 4.1 | 7.9 | |
| (NCT03929666) ZW-25 | II | Treatment-naive | ZW25 + Chemotherapy | 12.5 | NR | |
| FGFRmutations | FIGHT | II | Treatment-naive | Bemarituzumab + mFOLFOX6 | 9.5 | NR |
| Placebo + mFOLFOX6 | 7.4 | 12.9 | ||||
| CLDN18.2 | SPOTLIGHT | III | Treatment-naive | Zolbetuximab mFOLFOX6 | 10.6 | 18.2 |
| Placebo + mFOLFOX6 | 8.6 | 15.5 | ||||
| VEGF/ VEGFR | RAINBOW | III | Pretreated (2nd Line) | Paclitaxel | 2.86 | 7.4 |
| Paclitaxel + Ramucirumab | 4.4 | 9.6 | ||||
| REGARD | III | Pretreated (2nd Line) | Ramucirumab | 2.1 | 5.2 | |
| Placebo | 1.3 | 3.8 | ||||
| INTEGRATE | II | Pretreated | Regorafenib | 2.6 | 5.8 | |
| Placebo | 0.9 | 3.4 |
| Molecular Alteration | Trial | Phase | Patient Population | Treatment | Median PFS (Months) | Median OS (Months) |
|---|---|---|---|---|---|---|
| PD-1 | KEYNOTE-062 | III | Treatment-naïve G/GEJ | Pembrolizumab Pembrolizumab/chemotherapy Chemotherapy | 6.2 6.9 6.4 | 10.6 12.5 11.1 |
| ATTRACTION-04 | II/III | Treatment-naïve G/GEJ | Nivolumab/chemotherapy Chemotherapy | 10.5 8.3 | 17.5 17.2 | |
| CHECKMATE-649 | III | Treatment-naïve G/GEJ | Nivolumab/chemotherapy Nivolumab/ipilimumab Chemotherapy | 7.7 NA 6 | 14.4 NA 11.1 | |
| ORIENT-16 | III | Treatment-naïve G/GEJ | Sintilimab/chemotherapy Chemotherapy | NA | 15.2 12.3 | |
| MSI-H | KEYNOTE-158 | II | Non-colorectal, MSI-H, after fist-line | Pembrolizumab | 4.1 | 23.5 |
| PD-1 HER 2 | KEYNOTE-811 | III | Treatment-naïve G/GEJ HER2+ | Pembrolizumab/Trastuzumab/Chemotherapy Trastuzumab/Chemotherapy | To be released | Negative in ITT |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baccili Cury Megid, T.; Farooq, A.R.; Wang, X.; Elimova, E. Gastric Cancer: Molecular Mechanisms, Novel Targets, and Immunotherapies: From Bench to Clinical Therapeutics. Cancers 2023, 15, 5075. https://doi.org/10.3390/cancers15205075
Baccili Cury Megid T, Farooq AR, Wang X, Elimova E. Gastric Cancer: Molecular Mechanisms, Novel Targets, and Immunotherapies: From Bench to Clinical Therapeutics. Cancers. 2023; 15(20):5075. https://doi.org/10.3390/cancers15205075
Chicago/Turabian StyleBaccili Cury Megid, Thais, Abdul Rehman Farooq, Xin Wang, and Elena Elimova. 2023. "Gastric Cancer: Molecular Mechanisms, Novel Targets, and Immunotherapies: From Bench to Clinical Therapeutics" Cancers 15, no. 20: 5075. https://doi.org/10.3390/cancers15205075