
Developing Cardio-Oncology Programs in the New Era: Beyond Ventricular Dysfunction Due to Cancer Treatments

 , , add
Show full author list
, , add
Show full author list
{kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
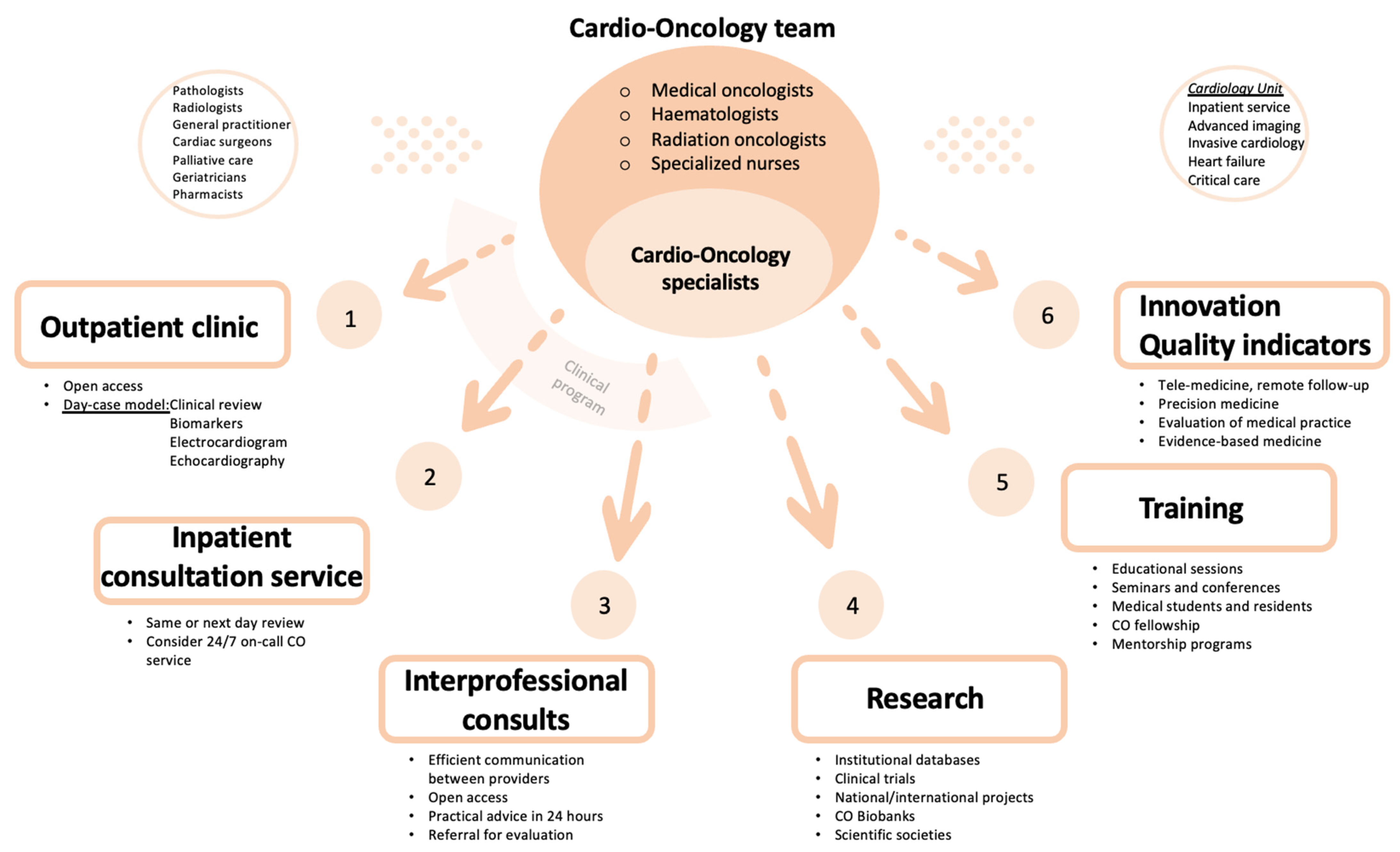
2. Organization of a Cardio-Oncology Unit
2.1. Objective of the Cardio-Oncology Unit
2.2. Components of Cardio-Oncology Team
2.3. Cardio-Oncology Programs
2.3.1. Clinical Program
2.3.2. Research Program
2.3.3. Training Program
2.3.4. Innovation in Cardio-Oncology
2.3.5. Quality Indicators
2.4. Pathway of Care
3. Disease-Specific Clinical Pathways
3.1. Cardiotoxicity and Left Ventricle Dysfunction
3.2. Coronary Artery Disease
3.3. Antithrombotic Treatment in Cancer Patients
3.4. Myocarditis Related to Immune Checkpoint Inhibitors
3.5. Management of Patients with Cardiac Implantable Electronic Devices and Radiotherapy
3.6. Pericardial Effusions
3.7. Direct Cardiac Effects of Extracardiac Neoplasias
4. Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Koene, R.J.; Prizment, A.E.; Blaes, A.; Konety, S.H. Shared Risk Factors in Cardiovascular Disease and Cancer. Circulation 2016, 133, 1104–1114. [Google Scholar] [CrossRef] [PubMed]
- Ameri, P.; Canepa, M.; Anker, M.S.; Belenkov, Y.; Bergler-Klein, J.; Cohen-Solal, A.; Farmakis, D.; López-Fernández, T.; Lainscak, M.; Pudil, R.; et al. Cancer diagnosis in patients with heart failure: Epidemiology, clinical implications and gaps in knowledge. Eur. J. Heart Fail. 2018, 20, 879–887. [Google Scholar] [CrossRef] [PubMed]
- Banke, A.; Schou, M.; Videbaek, L.; Møller, J.E.; Torp-Pedersen, C.; Gustafsson, F.; Dahl, J.S.; Kober, L.; Hildebrandt, P.R.; Gislason, G.H. Incidence of cancer in patients with chronic heart failure: A long-term follow-up study. Eur. J. Heart Fail. 2016, 18, 260–266. [Google Scholar] [CrossRef] [PubMed]
- Moliner, P.; Lupón, J.; de Antonio, M.; Domingo, M.; Santiago-Vacas, E.; Zamora, E.; Cediel, G.; Santesmases, J.; Díez-Quevedo, C.; Isabel, M.; et al. Trends in modes of death in heart failure over the last two decades: Less sudden death but cancer deaths on the rise. Eur. J. Heart Fail. 2019, 21, 1259–1266. [Google Scholar] [CrossRef] [PubMed]
- Nhola, L.F.; Villarraga, H.R. Fundamentos de las unidades de cardio-oncología. Rev. Española Cardiol. 2017, 70, 583–589. [Google Scholar] [CrossRef]
- Ammon, M.; Arenja, N.; Leibundgut, G.; Buechel, R.R.; Kuster, G.M.; Kaufmann, B.A.; Pfister, O. Cardiovascular management of cancer patients with chemotherapy-associated left ventricular systolic dysfunction in real-world clinical practice. J. Card. Fail. 2013, 19, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Parent, S.; Pituskin, E.; Paterson, D.I. The Cardio-oncology Program: A Multidisciplinary Approach to the Care of Cancer Patients With Cardiovascular Disease. Can. J. Cardiol. 2016, 32, 847–851. [Google Scholar] [CrossRef]
- Pareek, N.; Cevallos, J.; Moliner, P.; Shah, M.; Tan, L.L.; Chambers, V.; Baksi, A.J.; Khattar, R.S.; Sharma, R.; Rosen, S.D.; et al. Activity and outcomes of a cardio-oncology service in the United Kingdom-a five-year experience. Eur. J. Heart Fail. 2018, 20, 1721–1731. [Google Scholar] [CrossRef]
- Lancellotti, P.; Suter, T.M.; López-Fernández, T.; Galderisi, M.; Lyon, A.R.; Van der Meer, P.; Cohen, A.; Zamorano, J.L.; Jerusalem, G.; Moonen, M.; et al. Cardio-Oncology Services: Rationale, organization, and implementation. Eur. Heart J. 2019, 40, 1756–1763. [Google Scholar] [CrossRef]
- Barros-Gomes, S.; Herrmann, J.; Mulvagh, S.L.; Lerman, A.; Lin, G.; Villarraga, H.R. Rationale for setting up a cardio-oncology unit: Our experience at Mayo Clinic. Cardiooncology 2016, 2, 5. [Google Scholar] [CrossRef]
- Arjun KGhosh Charlotte Manisty Simon Woldman Tom Crake Mark Westwood, J.M.W. Setting up cardio-oncology services. Br. J. Cardiol. 2017, 24, 1. [Google Scholar]
- Snipelisky, D.; Park, J.Y.; Lerman, A.; Mulvagh, S.; Lin, G.; Pereira, N.; Rodríguez-Porcel, M.; Villarraga, H.R.; Herrmann, J. How to Develop a Cardio-Oncology Clinic. Heart Fail. Clin. 2017, 13, 347–359. [Google Scholar] [CrossRef] [PubMed]
- Okwuosa, T.M.; Barac, A. Burgeoning Cardio-Oncology Programs: Challenges and Opportunities for Early Career Cardiologists/Faculty Directors. J. Am. Coll. Cardiol. 2015, 66, 1193–1197. [Google Scholar] [CrossRef] [PubMed]
- Sadler, D.; Chaulagain, C.; Alvarado, B.; Cubeddu, R.; Stone, E.; Samuel, T.; Bastos, B.; Grossman, D.; Fu, C.L.; Alley, E.; et al. Practical and cost-effective model to build and sustain a cardio-oncology program. Cardiooncology 2020, 6, 9. [Google Scholar] [CrossRef] [PubMed]
- Brown, S.-A.; Rhee, J.-W.; Guha, A.; Rao, V.U. Innovation in Precision Cardio-Oncology during the Coronavirus Pandemic and Into a Post-pandemic World. Front. Cardiovasc. Med. 2020, 7, 145. [Google Scholar] [CrossRef] [PubMed]
- Aktaa, S.; Batra, G.; Wallentin, L.; Baigent, C.; Erlinge, D.; James, S.; Ludman, P.; Maggioni, A.P.; Price, S.; Weston, C.; et al. European Society of Cardiology methodology for the development of quality indicators for the quantification of cardiovascular care and outcomes. Eur. Heart J. Qual. Care Clin. Outcomes 2022, 8, 4–13. [Google Scholar] [CrossRef]
- Lyon, A.R.; López-Fernández, T.; Couch, L.S.; Asteggiano, R.; Aznar, M.C.; Bergler-Klein, J.; Boriani, G.; Cardinale, D.; Córdoba, R.; Cosyns, B.; et al. 2022 ESC Guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur Heart J 2022, 43, 4229–4361. [Google Scholar] [CrossRef]
- Lee, G.A.; Aktaa, S.; Baker, E.; Gale, C.P.; Yaseen, I.F.; Gulati, G.; Asteggiano, R.; Szmit, S.; Cohen-Solal, A.; Abdin, A.; et al. European Society of Cardiology quality indicators for the prevention and management of cancer therapy-related cardiovascular toxicity in cancer treatment. Eur. Heart J. Qual. Care Clin. Outcomes 2022, 9, 1–7. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Zamorano, J.L.; Lancellotti, P.; Rodriguez Muñoz, D.; Aboyans, V.; Asteggiano, R.; Galderisi, M.; Habib, G.; Lenihan, D.J.; Lip, G.Y.; Lyon, A.R.; et al. 2016 ESC Position Paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for Practice Guidelines: The Task Force for cancer treatments and cardiovascular toxicity of the European Society of Cardiology (ESC). Eur. Heart J. 2016, 37, 2768–2801. [Google Scholar] [CrossRef]
- López-Sendón, J.; Álvarez-Ortega, C.; Zamora Auñon, P.; Buño Soto, A.; Lyon, A.R.; Farmakis, D.; Cardinale, D.; Canales, M.; Feliu, J.; Rodríguez, I.; et al. Classification, prevalence, and outcomes of anticancer therapy-induced cardiotoxicity: The CARDIOTOX registry. Eur. Heart J. 2020, 41, 1720–1729. [Google Scholar] [CrossRef] [PubMed]
- Lyon, A.R.; Dent, S.; Stanway, S.; Earl, H.; Brezden-Masley, C.; Cohen-Solal, A.; Tocchetti, C.G.; Moslehi, J.J.; Groarke, J.D.; Bergler-Klein, J.; et al. Baseline cardiovascular risk assessment in cancer patients scheduled to receive cardiotoxic cancer therapies: A position statement and new risk assessment tools from the Cardio-Oncology Study Group of the Heart Failure Association of the European Society of Cardiology in collaboration with the International Cardio-Oncology Society. Eur. J. Heart Fail. 2020, 22, 1945–1960. [Google Scholar] [PubMed]
- Pudil, R.; Mueller, C.; Čelutkienė, J.; Henriksen, P.A.; Lenihan, D.; Dent, S.; Barac, A.; Stanway, S.; Moslehi, J.; Suter, T.M.; et al. Role of serum biomarkers in cancer patients receiving cardiotoxic cancer therapies: A position statement from the Cardio-Oncology Study Group of the Heart Failure Association and the Cardio-Oncology Council of the European Society of Cardiology. Eur. J. Heart Fail. 2020, 22, 1966–1983. [Google Scholar] [CrossRef] [PubMed]
- Plana, J.C.; Galderisi, M.; Barac, A.; Ewer, M.S.; Ky, B.; Scherrer-Crosbie, M.; Ganame, J.; Sebag, I.A.; Agler, D.A.; Badano, L.P.; et al. Expert consensus for multimodality imaging evaluation of adult patients during and after cancer therapy: A report from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2014, 27, 911–939. [Google Scholar] [CrossRef] [PubMed]
- Čelutkienė, J.; Pudil, R.; López-Fernández, T.; Grapsa, J.; Nihoyannopoulos, P.; Bergler-Klein, J.; Cohen-Solal, A.; Farmakis, D.; Tocchetti, C.G.; von Haehling, S.; et al. Role of cardiovascular imaging in cancer patients receiving cardiotoxic therapies: A position statement on behalf of the Heart Failure Association (HFA), the European Association of Cardiovascular Imaging (EACVI) and the Cardio-Oncology Council of the European Society of Cardiology (ESC). Eur. J. Heart Fail. 2020, 22, 1504–1524. [Google Scholar] [PubMed]
- Vejpongsa, P.; Yeh, E.T.H. Prevention of anthracycline-induced cardiotoxicity: Challenges and opportunities. J. Am. Coll. Cardiol. 2014, 64, 938–945. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, N.; Fujii, T.; Aoi, S.; Kozuch, P.S.; Hortobagyi, G.N.; Blum, R.H. Comparison of cardiac events associated with liposomal doxorubicin, epirubicin and doxorubicin in breast cancer: A Bayesian network meta-analysis. Eur. J. Cancer 2015, 51, 2314–2320. [Google Scholar] [CrossRef]
- Neilan, T.G.; Quinaglia, T.; Onoue, T.; Mahmood, S.S.; Drobni, Z.D.; Gilman, H.K.; Smith, A.; Heemelaar, J.C.; Brahmbhatt, P.; Ho, J.S.; et al. Atorvastatin for anthracycline-associated cardiac dysfunction. The STOP-CA randomized clinical trial. JAMA 2023, 330, 528–536. [Google Scholar] [CrossRef]
- Curigliano, G.; Cardinale, D.; Dent, S.; Criscitiello, C.; Aseyev, O.; Lenihan, D.; Cipolla, C.M. Cardiotoxicity of anticancer treatments: Epidemiology, detection, and management. CA Cancer J. Clin. 2016, 66, 309–325. [Google Scholar] [CrossRef]
- Zamorano, J.L.; Gottfridsson, C.; Asteggiano, R.; Atar, D.; Badimon, L.; Bax, J.J.; Cardinale, D.; Cardone, A.; Feijen, E.A.; Ferdinandy, P.; et al. The cancer patient and cardiology. Eur. J. Heart Fail. 2020, 22, 2290–2309. [Google Scholar] [CrossRef]
- Lancellotti, P.; Nkomo, V.T.; Badano, L.P.; Bergler-Klein, J.; Bogaert, J.; Davin, L.; Cosyns, B.; Coucke, P.; Dulgheru, R.; Edvardsen, T.; et al. Expert consensus for multi-modality imaging evaluation of cardiovascular complications of radiotherapy in adults: A report from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 721–740. [Google Scholar] [CrossRef]
- López-Fernández, T.; Martín, A.; Santaballa, A.; Montero, A.; García, R.; Mazón, P.; Velasco, S.; López de Sá, E.; Barreiro-Pérez, M.; Hinojar, R.; et al. Cardio-Onco-Hematology in Clinical Practice. Position Paper and Recommendations. Rev. Esp. Cardiol. 2017, 70, 474–486. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [PubMed]
- Pardo Sanz, A.; Rincón Díaz, L.M.; Tamayo, A.S.; de Lara Delgado, G.; Contreras, H.; Zamorano Gómez, J.L. Current Status of Antithrombotic Therapy in Patients With Breast Cancer and Atrial Fibrillation. Rev. Esp. Cardiol. 2019, 72, 589–591. [Google Scholar] [CrossRef] [PubMed]
- Mosarla, R.C.; Vaduganathan, M.; Qamar, A.; Moslehi, J.; Piazza, G.; Giugliano, R.P. Anticoagulation Strategies in Patients With Cancer: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2019, 73, 1336–1349. [Google Scholar] [CrossRef] [PubMed]
- Khorana, A.A.; Noble, S.; Lee, A.Y.Y.; Soff, G.; Meyer, G.; O’Connell, C.; Carrier, M. Role of direct oral anticoagulants in the treatment of cancer-associated venous thromboembolism: Guidance from the SSC of the ISTH. J. Thromb. Haemost. 2018, 16, 1891–1894. [Google Scholar] [CrossRef] [PubMed]
- Nana, P.; Dakis, K.; Peroulis, M.; Rousas, N.; Spanos, K.; Kouvelos, G.; Arnaoutoglou, E.; Matsagkas, M. The Role of Direct Oral Anticoagulants in Cancer-Associated Thrombosis According to the Current Literature. Medicina 2021, 57, 960. [Google Scholar] [CrossRef]
- Steffel, J.; Verhamme, P.; Potpara, T.S.; Albaladejo, P.; Antz, M.; Desteghe, L.; Haeusler, K.G.; Oldgren, J.; Reinecke, H.; Roldan-Schilling, V.; et al. The 2018 European Heart Rhythm Association Practical Guide on the use of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation. Eur. Heart J. 2018, 39, 1330–1393. [Google Scholar] [CrossRef]
- Mahmood, S.S.; Fradley, M.G.; Cohen, J.V.; Nohria, A.; Reynolds, K.L.; Heinzerling, L.M.; Sullivan, R.J.; Damrongwatanasuk, R.; Chen, C.L.; Gupta, D.; et al. Myocarditis in Patients Treated with Immune Checkpoint Inhibitors. J. Am. Coll. Cardiol. 2018, 71, 1755–1764. [Google Scholar] [CrossRef]
- Salem, J.-E.; Manouchehri, A.; Moey, M.; Lebrun-Vignes, B.; Bastarache, L.; Pariente, A.; Gobert, A.; Spano, J.P.; Balko, J.M.; Bonaca, M.P.; et al. Cardiovascular toxicities associated with immune checkpoint inhibitors: An observational, retrospective, pharmacovigilance study. Lancet Oncol. 2018, 19, 1579–1589. [Google Scholar] [CrossRef]
- Spallarossa, P.; Sarocchi, M.; Tini, G.; Arboscello, E.; Toma, M.; Ameri, P.; Porto, I. How to Monitor Cardiac Complications of Immune Checkpoint Inhibitor Therapy. Front. Pharmacol. 2020, 11, 972. [Google Scholar] [CrossRef] [PubMed]
- Curigliano, G.; Lenihan, D.; Fradley, M.; Ganatra, S.; Barac, A.; Blaes, A.; Herrmann, J.; Porter, C.; Lyon, A.R.; Lancellotti, P.; et al. Management of cardiac disease in cancer patients throughout oncological treatment: ESMO consensus recommendations. Ann. Oncol. 2020, 31, 171–190. [Google Scholar] [CrossRef] [PubMed]
- Fradley, M.G.; Lefebvre, B.; Carver, J.; Cheung, J.W.; Feigenberg, S.J.; Lampert, R.; Liu, J.; Rajagopalan, B.; Lenihan, D.J. How to Manage Patients with Cardiac Implantable Electronic Devices Undergoing Radiation Therapy. JACC Cardio Oncol. 2021, 3, 447–451. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, A.K.; Crake, T.; Manisty, C.; Westwood, M. Pericardial Disease in Cancer Patients. Curr. Treat. Options Cardiovasc. Med. 2018, 20, 60. [Google Scholar] [CrossRef]
- Maleszewski, J.J.; Bois, M.C.; Bois, J.P.; Young, P.M.; Stulak, J.M.; Klarich, K.W. Neoplasia and the Heart: Pathological Review of Effects With Clinical and Radiological Correlation. J. Am. Coll. Cardiol. 2018, 72, 202–227. [Google Scholar] [CrossRef]
- Paredes, A.; Valdebenito, M.; Neira, V.; Castro, P.; Zalaquett, R. Síndrome carcinoide y compromiso valvular cardíaco. Rev. Chil. Cardiol. 2014, 33, 38–43. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pons-Riverola, A.; Morillas, H.; Berdejo, J.; Pernas, S.; Pomares, H.; Asiain, L.; Garay, A.; Fernandez-Ortega, A.; Oliveira, A.C.; Martínez, E.; et al. Developing Cardio-Oncology Programs in the New Era: Beyond Ventricular Dysfunction Due to Cancer Treatments. Cancers 2023, 15, 5885. https://doi.org/10.3390/cancers15245885
Pons-Riverola A, Morillas H, Berdejo J, Pernas S, Pomares H, Asiain L, Garay A, Fernandez-Ortega A, Oliveira AC, Martínez E, et al. Developing Cardio-Oncology Programs in the New Era: Beyond Ventricular Dysfunction Due to Cancer Treatments. Cancers. 2023; 15(24):5885. https://doi.org/10.3390/cancers15245885
Chicago/Turabian StylePons-Riverola, Alexandra, Herminio Morillas, Javier Berdejo, Sonia Pernas, Helena Pomares, Leyre Asiain, Alberto Garay, Adela Fernandez-Ortega, Ana Carla Oliveira, Evelyn Martínez, and et al. 2023. "Developing Cardio-Oncology Programs in the New Era: Beyond Ventricular Dysfunction Due to Cancer Treatments" Cancers 15, no. 24: 5885. https://doi.org/10.3390/cancers15245885
APA StylePons-Riverola, A., Morillas, H., Berdejo, J., Pernas, S., Pomares, H., Asiain, L., Garay, A., Fernandez-Ortega, A., Oliveira, A. C., Martínez, E., Jiménez-Marrero, S., Pina, E., Fort, E., Ramos, R., Alcoberro, L., Hidalgo, E., Antonio-Rebollo, M., Alcober, L., Enjuanes Grau, C., ... Moliner, P. (2023). Developing Cardio-Oncology Programs in the New Era: Beyond Ventricular Dysfunction Due to Cancer Treatments. Cancers, 15(24), 5885. https://doi.org/10.3390/cancers15245885