
Salvage Perioperative Interstitial High-Dose-Rate Interventional Radiotherapy (Brachytherapy) for Local Recurrences of the Chest Wall Following Mastectomy and Previous External Irradiation


Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Patients
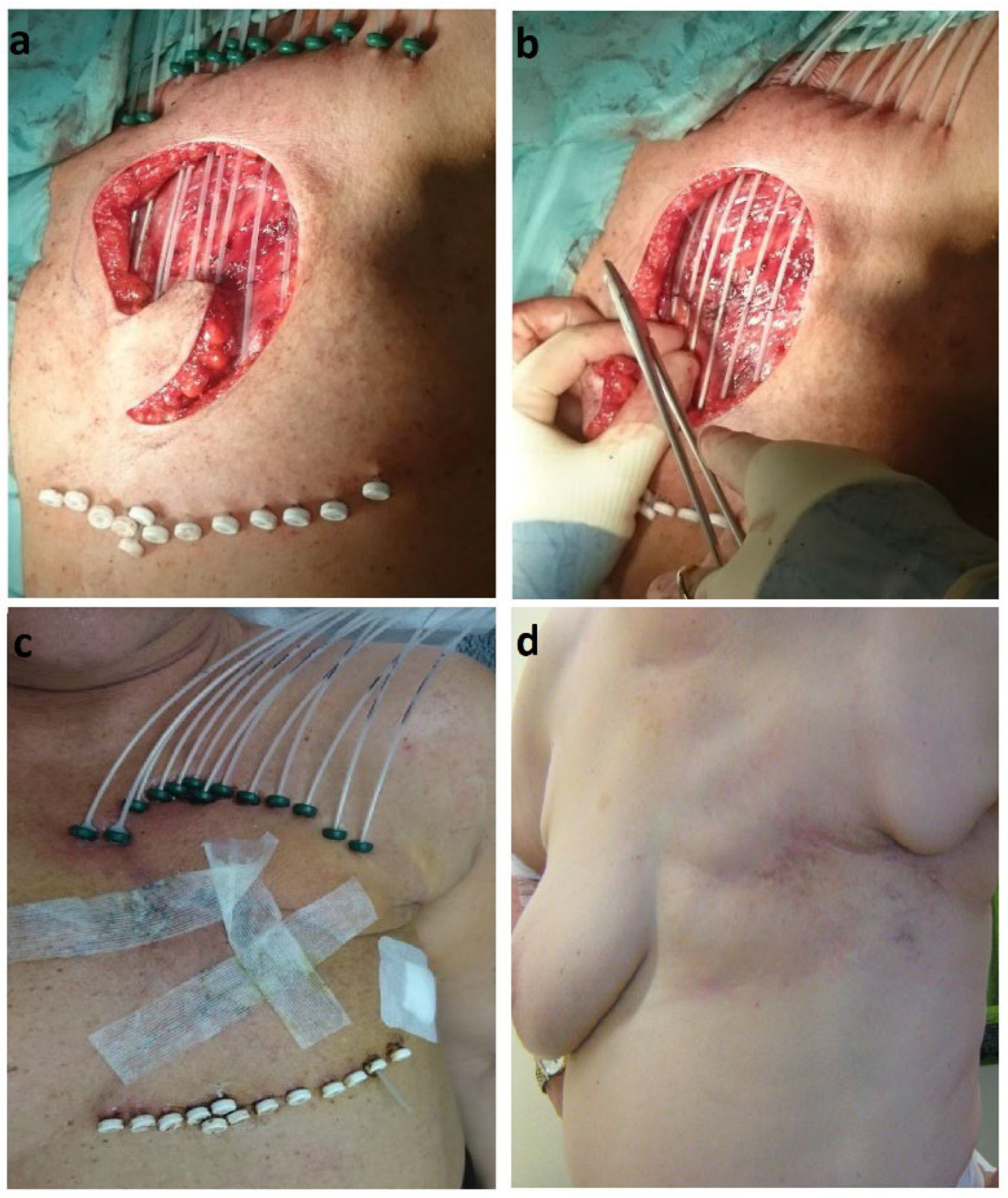
2.2. Interventional Radiotherapy (Brachytherapy)
2.3. Follow-up
2.4. Statistical Analysis
3. Results
3.1. Patient and Tumor Characteristics
3.2. HDR-IRT Treatment Characteristics
3.3. Treatment Outcome and Related Toxicities
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bedwinek, J. Natural History and Management of Isolated Local-Regional Recurrence Following Mastectomy. Semin. Radiat. Oncol. 1994, 4, 260–269. [Google Scholar] [CrossRef] [PubMed]
- Buchanan, C.L.; Dorn, P.L.; Fey, J.; Giron, G.; Naik, A.; Mendez, J.; Murphy, C.; Sclafani, L.M. Locoregional Recurrence after Mastectomy: Incidence and Outcomes. J. Am. Coll. Surg. 2006, 203, 469–474. [Google Scholar] [CrossRef] [PubMed]
- McGale, P.; Taylor, C.; Correa, C.; Cutter, D.; Duane, F.; Ewertz, M.; Gray, R.; Mannu, G.; Peto, R.; Whelan, T.; et al. Effect of Radiotherapy after Mastectomy and Axillary Surgery on 10-Year Recurrence and 20-Year Breast Cancer Mortality: Meta-Analysis of Individual Patient Data for 8135 Women in 22 Randomised Trials. Lancet 2014, 383, 2127–2135. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, H.M.; Overgaard, M.; Grau, C.; Jensen, A.R.; Overgaard, J. Study of Failure Pattern among High-Risk Breast Cancer Patients with or without Postmastectomy Radiotherapy in Addition to Adjuvant Systemic Therapy: Long-Term Results from the Danish Breast Cancer Cooperative Group DBCG 82 b and c Randomized Studies. J. Clin. Oncol. 2006, 24, 2268–2275. [Google Scholar] [CrossRef] [Green Version]
- Fattahi, S.; Ahmed, S.K.; Park, S.S.; Petersen, I.A.; Shumway, D.A.; Stish, B.J.; Yan, E.S.; Remmes, N.B.; Mutter, R.W.; Corbin, K.S. Reirradiation for Locoregional Recurrent Breast Cancer. Adv. Radiat. Oncol. 2020, 6, 100640. [Google Scholar] [CrossRef]
- Marta, G.N.; Hijal, T.; de Andrade Carvalho, H. Reirradiation for Locally Recurrent Breast Cancer. Breast 2017, 33, 159–165. [Google Scholar] [CrossRef]
- Harms, W.; Krempien, R.; Grehn, C.; Hensley, F.; Berns, C.; Wannenmacher, M.; Debus, J. Reirradiation of Chest Wall Local Recurrences from Breast Cancer. Zentralbl. Gynakol. 2004, 126, 19–23. [Google Scholar] [CrossRef]
- De-Colle, C.; Weidner, N.; Heinrich, V.; Brucker, S.; Hahn, M.; MacMillan, K.; Lamprecht, U.; Gaupp, S.; Voigt, O.; Zips, D. Hyperthermic Chest Wall Re-Irradiation in Recurrent Breast Cancer: A Prospective Observational Study. Strahlenther. Onkol. 2019, 195, 318–326. [Google Scholar] [CrossRef]
- Oldenborg, S.; Rasch, C.R.N.; van Os, R.; Kusumanto, Y.H.; Oei, B.S.; Venselaar, J.L.; Heymans, M.W.; zum Vörde Sive Vörding, P.J.; Crezee, H.; van Tienhoven, G. Reirradiation + Hyperthermia for Recurrent Breast Cancer En Cuirasse. Strahlenther. Onkol. 2018, 194, 206–214. [Google Scholar] [CrossRef] [Green Version]
- Besson, N.; Hennequin, C.; Guillerm, S.; Fumagalli, I.; Martin, V.; Michaud, S.; Texeira, L.; Quero, L. Plesiobrachytherapy for Chest Wall Recurrences of Breast Cancer after Mastectomy and Radiotherapy for Breast Cancer. Brachytherapy 2018, 17, 425–431. [Google Scholar] [CrossRef]
- Auoragh, A.; Strnad, V.; Ott, O.J.; Beckmann, M.W.; Fietkau, R. Re-Irradiation of the Chest Wall for Local Breast Cancer Recurrence: Results of Salvage Brachytherapy with Hyperthermia. Strahlenther. Onkol. 2016, 192, 617–623. [Google Scholar] [CrossRef] [PubMed]
- Harms, W.; Krempien, R.; Hensley, F.W.; Berns, C.; Wannenmacher, M.; Fritz, P. Results of Chest Wall Reirradiation Using Pulsed-Dose-Rate (PDR) Brachytherapy Molds for Breast Cancer Local Recurrences. Int. J. Radiat. Oncol. Biol. Phys. 2001, 49, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Mayer, Á.; Naszály, A.; Patyánik, M.; Zaránd, P.; Polgár, I.; Klinkó, T. Perioperative Brachytherapy for Pretreated Chest Wall Recurrence of Breast Cancer. Strahlenther. Onkol. 2002, 178, 633–636. [Google Scholar] [CrossRef] [PubMed]
- Niehoff, P.; Dietrich, J.; Ostertag, H.; Schmid, A.; Kohr, P.; Kimmig, B.; Kovács, G. High-Dose-Rate (HDR) or Pulsed-Dose-Rate (PDR) Perioperative Interstitial Intensity-Modulated Brachytherapy (IMBT) for Local Recurrences of Previously Irradiated Breast or Thoracic Wall Following Breast Cancer. Strahlenther. Onkol. 2006, 182, 102–107. [Google Scholar] [CrossRef] [PubMed]
- Khan, N.; Clemens, M.; Liu, J.; Garden, A.S.; Lawyer, A.; Weber, R.; Gunn, G.B.; Morrison, W.H.; Kupferman, M.E. The Role of Salvage Surgery with Interstitial Brachytherapy for the Management of Regionally Recurrent Head and Neck Cancers. Cancers Head Neck 2019, 4, 4. [Google Scholar] [CrossRef]
- Soror, T.; Kovács, G.; Fürschke, V.; Ismail, M.; Badakhshi, H. Salvage Treatment with Sole High-Dose-Rate Endobronchial Interventional Radiotherapy (Brachytherapy) for Isolated Endobronchial Tumor Recurrence in Non-Small-Cell Lung Cancer Patients: A 20-Year Experience. Brachytherapy 2019, 18, 727–732. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.P.; Weinberg, V.; Shinohara, K.; Roach, M.; Nash, M.; Gottschalk, A.; Chang, A.J.; Hsu, I.C. Salvage HDR Brachytherapy for Recurrent Prostate Cancer After Previous Definitive Radiation Therapy: 5-Year Outcomes. Int. J. Radiat. Oncol. Biol. Phys. 2013, 86, 324–329. [Google Scholar] [CrossRef]
- Chest Wall Resection in the Treatment of Locally Recurrent Breast Carcinoma: Indications and Outcome for 44 Patients. Available online: https://pubmed.ncbi.nlm.nih.gov/9307188/ (accessed on 25 November 2022).
- van der Pol, C.C.; van Geel, A.N.; Menke-Pluymers, M.B.E.; Schmitz, P.I.M.; Lans, T.E. Prognostic Factors in 77 Curative Chest Wall Resections for Isolated Breast Cancer Recurrence. Ann. Surg. Oncol. 2009, 16, 3414–3421. [Google Scholar] [CrossRef] [Green Version]
- Wahl, A.O.; Rademaker, A.; Kiel, K.D.; Jones, E.L.; Marks, L.B.; Croog, V.; McCormick, B.M.; Hirsch, A.; Karkar, A.; Motwani, S.B.; et al. Multi-Institutional Review of Repeat Irradiation of Chest Wall and Breast for Recurrent Breast Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 477–484. [Google Scholar] [CrossRef]
- Oldenborg, S.; Griesdoorn, V.; van Os, R.; Kusumanto, Y.H.; Oei, B.S.; Venselaar, J.L.; zum Vörde Sive Vörding, P.J.; Heymans, M.W.; Kolff, M.W.; Rasch, C.R.N.; et al. Reirradiation and Hyperthermia for Irresectable Locoregional Recurrent Breast Cancer in Previously Irradiated Area: Size Matters. Radiother. Oncol. 2015, 117, 223–228. [Google Scholar] [CrossRef]
- Marples, B.; Collis, S.J. Low-Dose Hyper-Radiosensitivity: Past, Present, and Future. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 1310–1318. [Google Scholar] [CrossRef] [PubMed]
- Burr, A.R.; Robins, H.I.; Bayliss, R.A.; Howard, S.P. Pulsed Reduced Dose Rate for Reirradiation of Recurrent Breast Cancer. Pract. Radiat. Oncol. 2020, 10, e61–e70. [Google Scholar] [CrossRef] [PubMed]
- LaRiviere, M.J.; Dreyfuss, A.; Taunk, N.K.; Freedman, G.M. Proton Reirradiation for Locoregionally Recurrent Breast Cancer. Adv. Radiat. Oncol. 2021, 6, 100710. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.I.; Khan, A.J.; Powell, S.N.; McCormick, B.; Lozano, A.J.; del Rosario, G.; Mamary, J.; Liu, H.; Fox, P.; Gillespie, E.; et al. Proton Reirradiation for Recurrent or New Primary Breast Cancer in the Setting of Prior Breast Irradiation. Radiother. Oncol. 2021, 165, 142–151. [Google Scholar] [CrossRef]
- Harms, W.; Budach, W.; Dunst, J.; Feyer, P.; Fietkau, R.; Haase, W.; Krug, D.; Piroth, M.D.; Sautter-Bihl, M.L.; Sedlmayer, F.; et al. DEGRO Practical Guidelines for Radiotherapy of Breast Cancer VI: Therapy of Locoregional Breast Cancer Recurrences. Strahlenther. Onkol. 2016, 192, 199–208. [Google Scholar] [CrossRef] [Green Version]
- Smanykó, V.; Mészáros, N.; Újhelyi, M.; Fröhlich, G.; Stelczer, G.; Major, T.; Mátrai, Z.; Polgár, C. Second Breast-Conserving Surgery and Interstitial Brachytherapy vs. Salvage Mastectomy for the Treatment of Local Recurrences: 5-Year Results. Brachytherapy 2019, 18, 411–419. [Google Scholar] [CrossRef]
- Teudt, I.U.; Kovàcs, G.; Ritter, M.; Melchert, C.; Soror, T.; Wollenberg, B.; Meyer, J.E. Intensity Modulated Perioperative HDR Brachytherapy for Recurrent and/or Advanced Head and Neck Metastases. Eur. Arch. Otorhinolaryngol. 2016, 273, 2707–2715. [Google Scholar] [CrossRef]
- Quivrin, M.; Peignaux-Casasnovas, K.; Martin; Rouffiac, M.; Thibouw, D.; Chevalier, C.; Vulquin, N.; Aubignac, L.; Truc, G.; Créhange, G. Salvage Brachytherapy as a Modern Reirradiation Technique for Local Cancer Failure: The Phoenix Is Reborn from Its Ashes. Cancer Radiother. 2018, 22, 372–381. [Google Scholar] [CrossRef]
- Hannoun-Levi, J.M.; Gal, J.; van Limbergen, E.; Chand, M.E.; Schiappa, R.; Smanyko, V.; Kauer-Domer, D.; Pasquier, D.; Lemanski, C.; Racadot, S.; et al. Salvage Mastectomy Versus Second Conservative Treatment for Second Ipsilateral Breast Tumor Event: A Propensity Score-Matched Cohort Analysis of the GEC-ESTRO Breast Cancer Working Group Database. Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 452–461. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Characteristic | Value | Number (%) |
|---|---|---|
| Initial T stage | T0 T1 T2 T3 T4 Unknown | 1 (1.8%) 11 (19.6%) 22 (39.3%) 4 (7.1%) 6 (10.7%) 12 (21.4%) |
| T stage at salvage treatment | T1 T2 T3 T4 | 19 (33.9%) 32 (57.1%) 3 (5.4%) 2 (3.6%) |
| Initial lymph node status | Negative Positive Unknown | 20 (35.7%) 24 (42.9%) 12 (21.4%) |
| Histology type | Ductal carcinoma in situ Non-special type Lobular carcinoma Other | 1 (1.8%) 39 (69.6%) 9 (16.1%) 7 (12.5%) |
| Initial histologic grade | Grade 1 Grade 2 Grade 3 Unknown | 3 (5.4%) 21 (37.5%) 17 (30.4%) 15 (26.7%) |
| Histologic grade at salvage treatment | Grade 1 Grade 2 Grade 3 | 3 (5.4%) 27 (48.2%) 26 (46.4%) |
| Initial surgical margin status | Negative Positive | 56 (100%) 0 (0%) |
| Surgical margin status at salvage treatment | Negative Positive | 51 (47.1%) 5 (8.9) |
| Estrogen/progesterone receptor status | Positive Negative Unknown | 39 (69.6%) 12 (21.4%) 5 (8.9%) |
| HER2-status | Positive Negative Unknown | 22 (39.3%) 28 (50%) 6 (10.7%) |
| Primary surgical operation | Mastectomy Breast conserving surgery | 43 (75.4%) 14 (24.6%) |
| Previous hormonal treatment | 39 (69.6%) | |
| Previous chemotherapy | 43 (76.8%) |
| Parameter | Median (Range) |
|---|---|
| HDR-IRT dose Total dose Dose per fraction Number of fractions | 30 Gy (25–36) 2.5 Gy (2.5–4) 10 (8–12) |
| Clinical target volume (CTV) | |
| Volume D90% V100% V150% | 25.5 cc (16–46) 93.8% (89.5–102) 87.2% (84.3–92.8) 37.2% (33.1–42.2) |
| Ipsilateral lung mean dose | 3.2% (2.7–3.8) |
| Heart mean dose (in left-sided tumors) | 2.8% (2.2–3.3) |
| Encountered Toxicity | Number (%) | Severity |
|---|---|---|
| Acute radiation dermatitis | 22 (39.3%) | Grade 1–2 |
| Late skin toxicities | 19 (33.9%) | Grade 1–2 |
| Fibrosis | 14 (25%) 3 (5.4%) | Grade 1–2 Grade ≥3 |
| Chronic wound complications | 1 (1.8%) | Grade ≥3 |
| Necrosis | 1 (1.8%) | Grade ≥3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soror, T.; Banys-Paluchowski, M.; Melchert, C.; Rades, D.; Rody, A.; Muras, K.; Xie, M.; Kovács, G. Salvage Perioperative Interstitial High-Dose-Rate Interventional Radiotherapy (Brachytherapy) for Local Recurrences of the Chest Wall Following Mastectomy and Previous External Irradiation. Cancers 2023, 15, 614. https://doi.org/10.3390/cancers15030614
Soror T, Banys-Paluchowski M, Melchert C, Rades D, Rody A, Muras K, Xie M, Kovács G. Salvage Perioperative Interstitial High-Dose-Rate Interventional Radiotherapy (Brachytherapy) for Local Recurrences of the Chest Wall Following Mastectomy and Previous External Irradiation. Cancers. 2023; 15(3):614. https://doi.org/10.3390/cancers15030614
Chicago/Turabian StyleSoror, Tamer, Maggie Banys-Paluchowski, Corinna Melchert, Dirk Rades, Achim Rody, Kerstin Muras, Meiting Xie, and György Kovács. 2023. "Salvage Perioperative Interstitial High-Dose-Rate Interventional Radiotherapy (Brachytherapy) for Local Recurrences of the Chest Wall Following Mastectomy and Previous External Irradiation" Cancers 15, no. 3: 614. https://doi.org/10.3390/cancers15030614