
Combining TNFR2-Expressing Tregs and IL-6 as Superior Diagnostic Biomarkers for High-Grade Serous Ovarian Cancer Masses

 ,
, 
 , , ,
, , , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Trial Design and Patient Details
2.2. Serum Isolation
2.3. Ascites Supernatant Isolation
2.4. Isolation of Peripheral Blood Mononuclear Cells
2.5. Multiplex Bead Immunoassays
2.6. In-Vitro Conditioning with Ascites
2.7. In Vitro Blockade of Cytokines within Ascites with Monoclonal Antibodies
2.8. Flow Cytometric Analysis
2.9. Statistical Analysis of Data
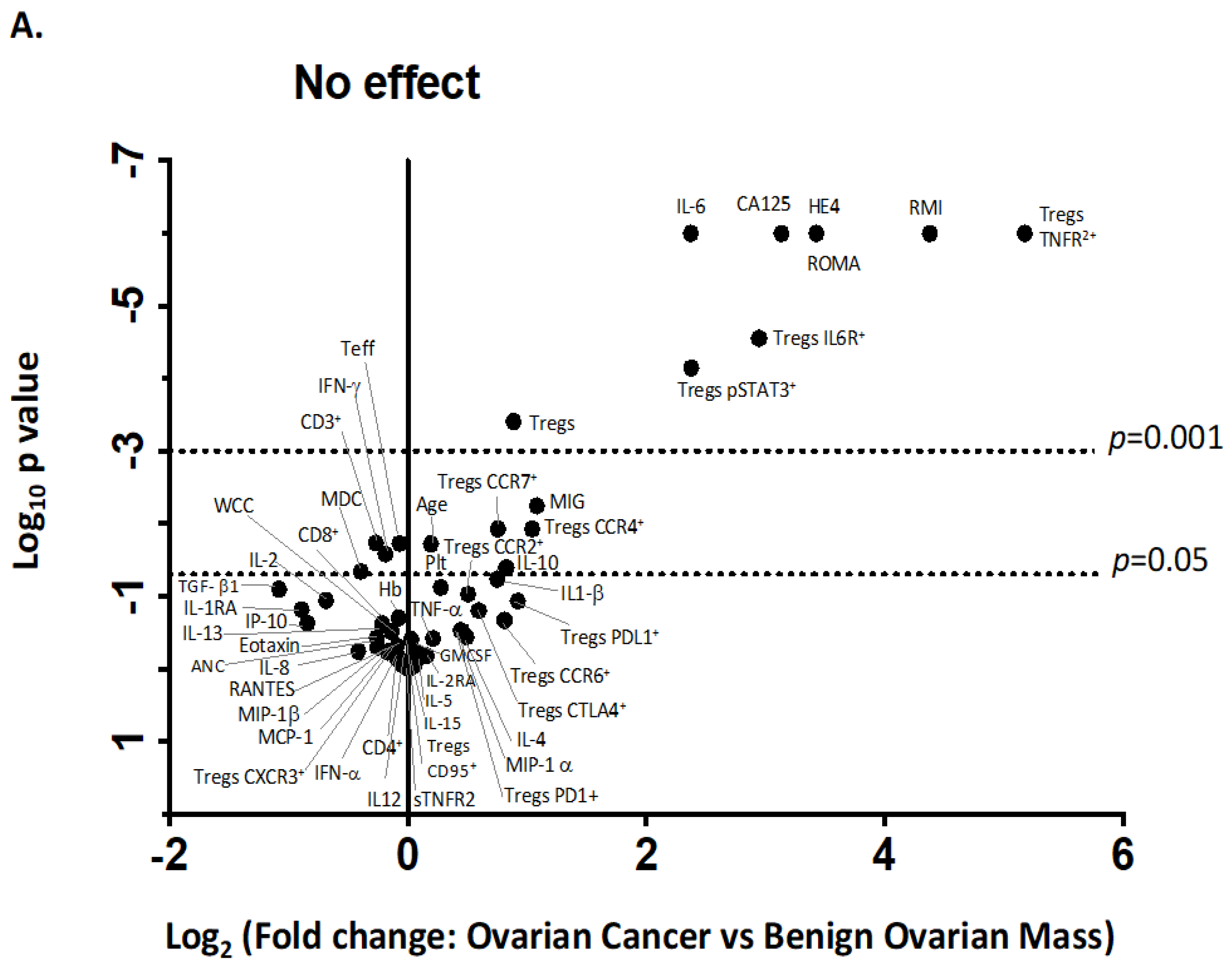
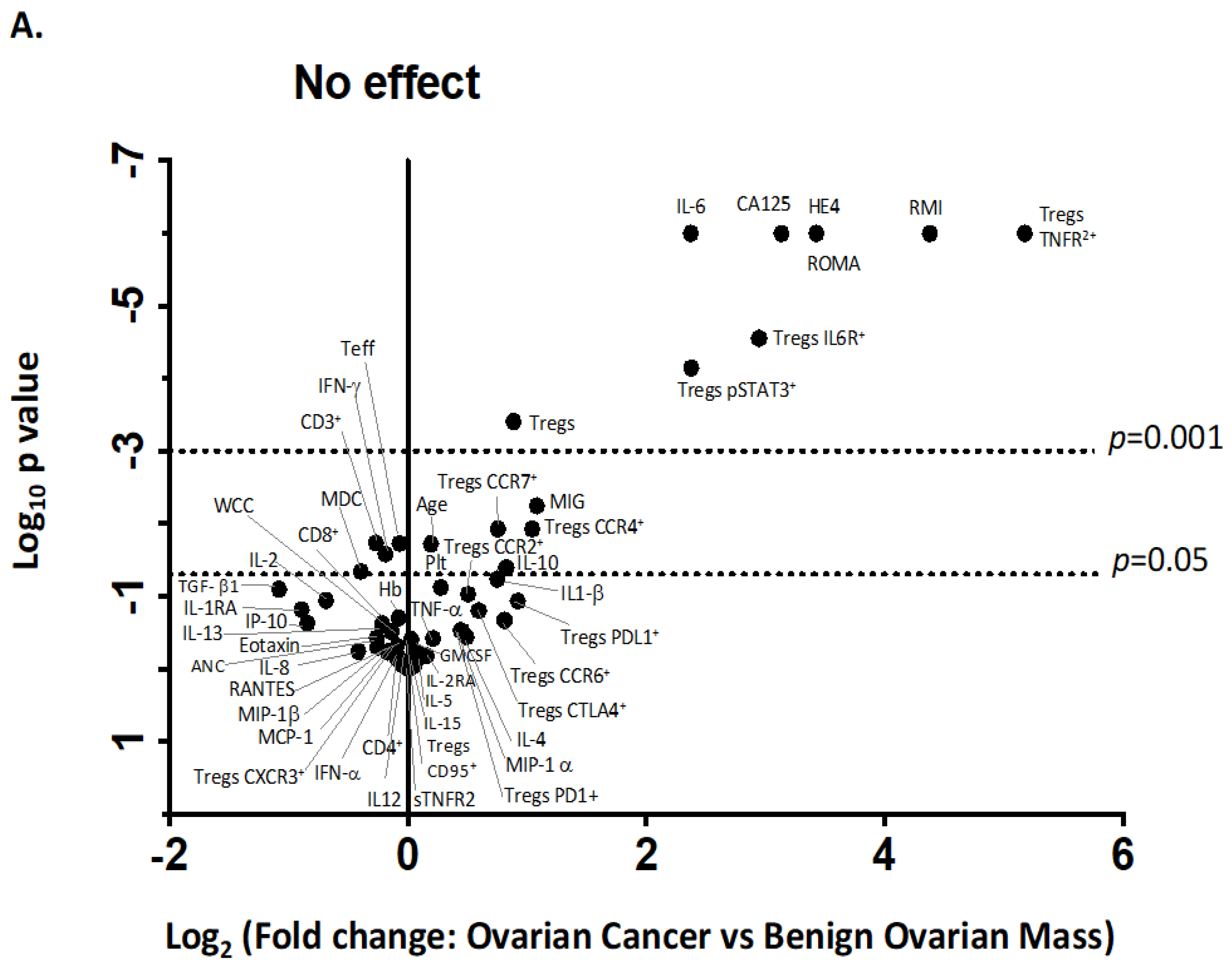
2.9.1. Volcano Plot
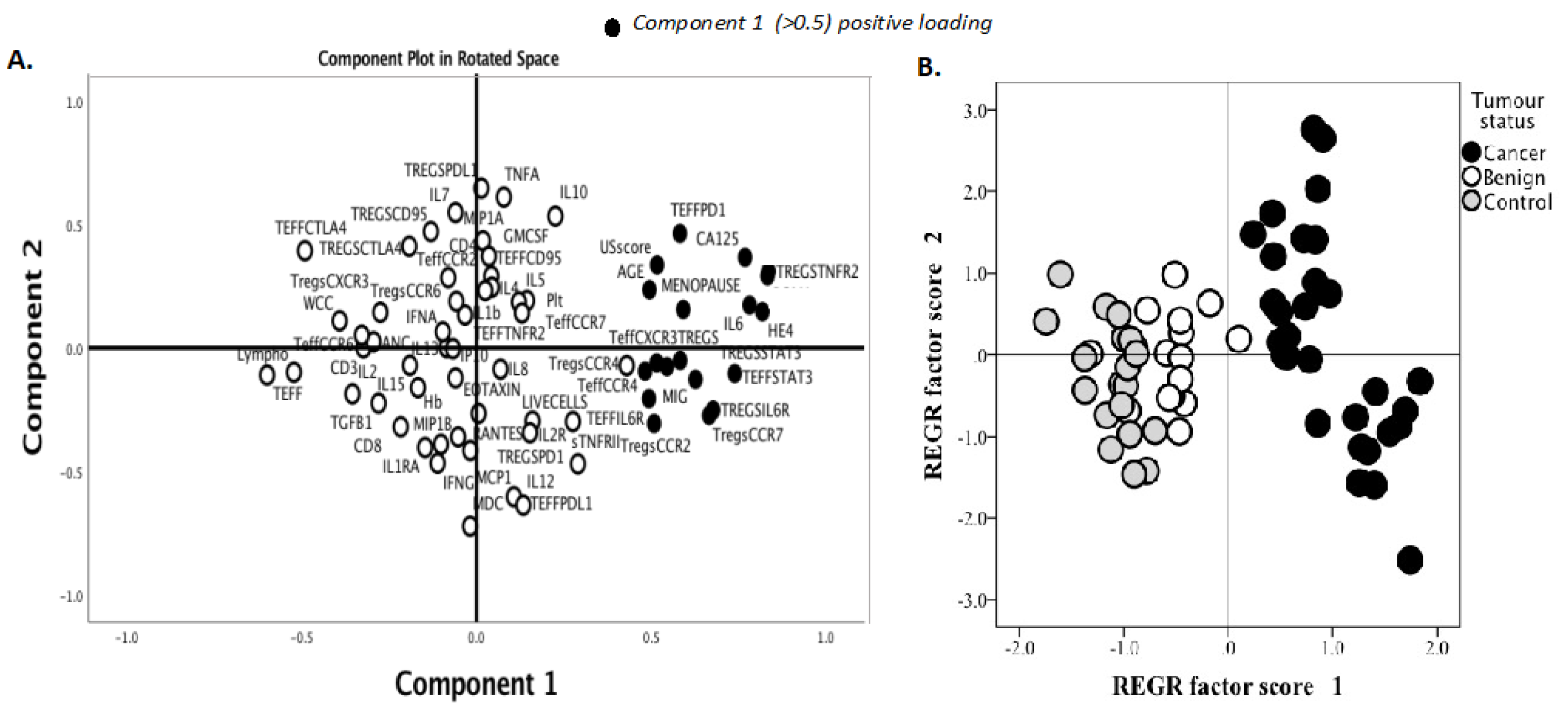
2.9.2. Principal Component Analysis (PCA)
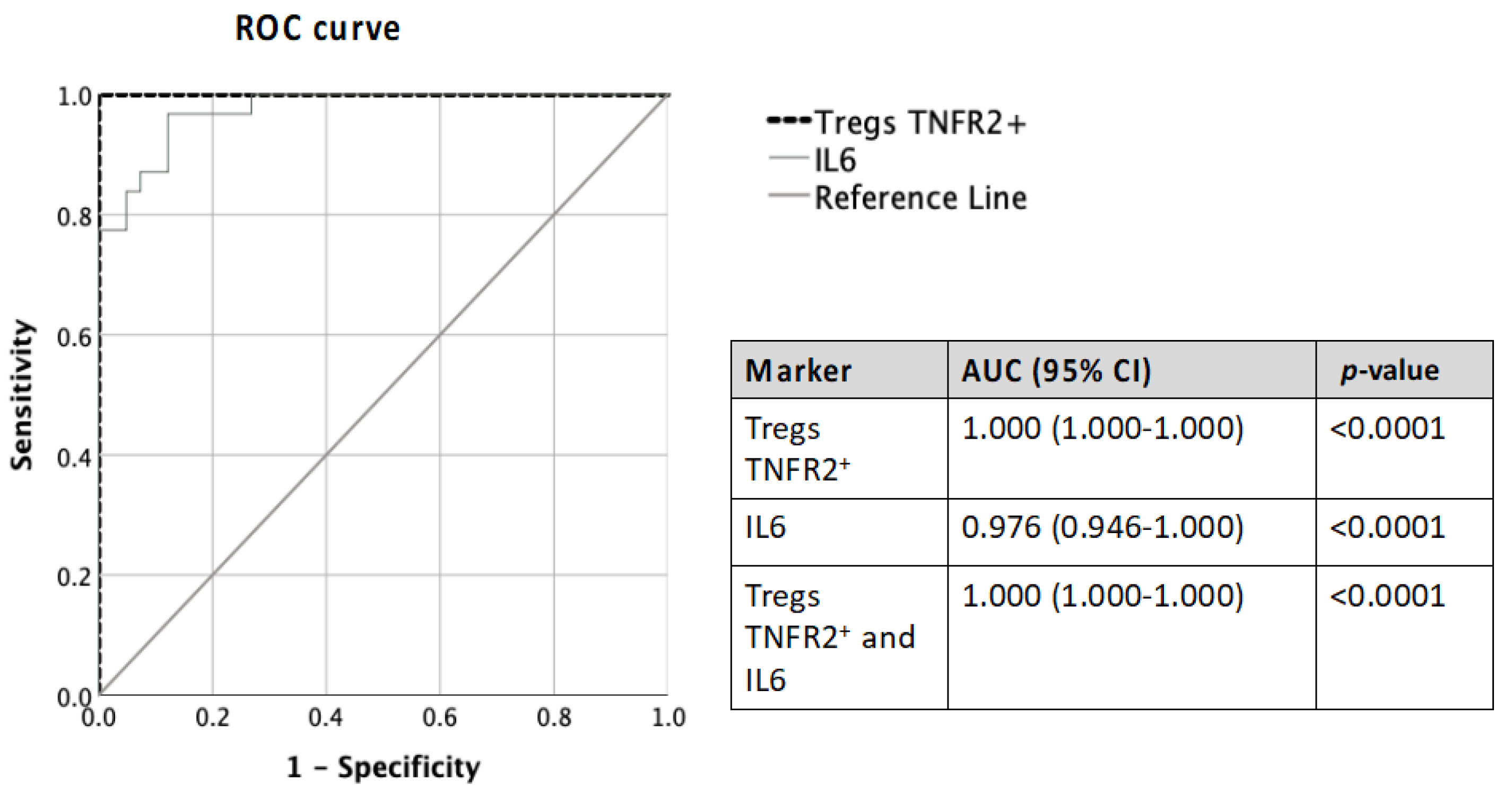
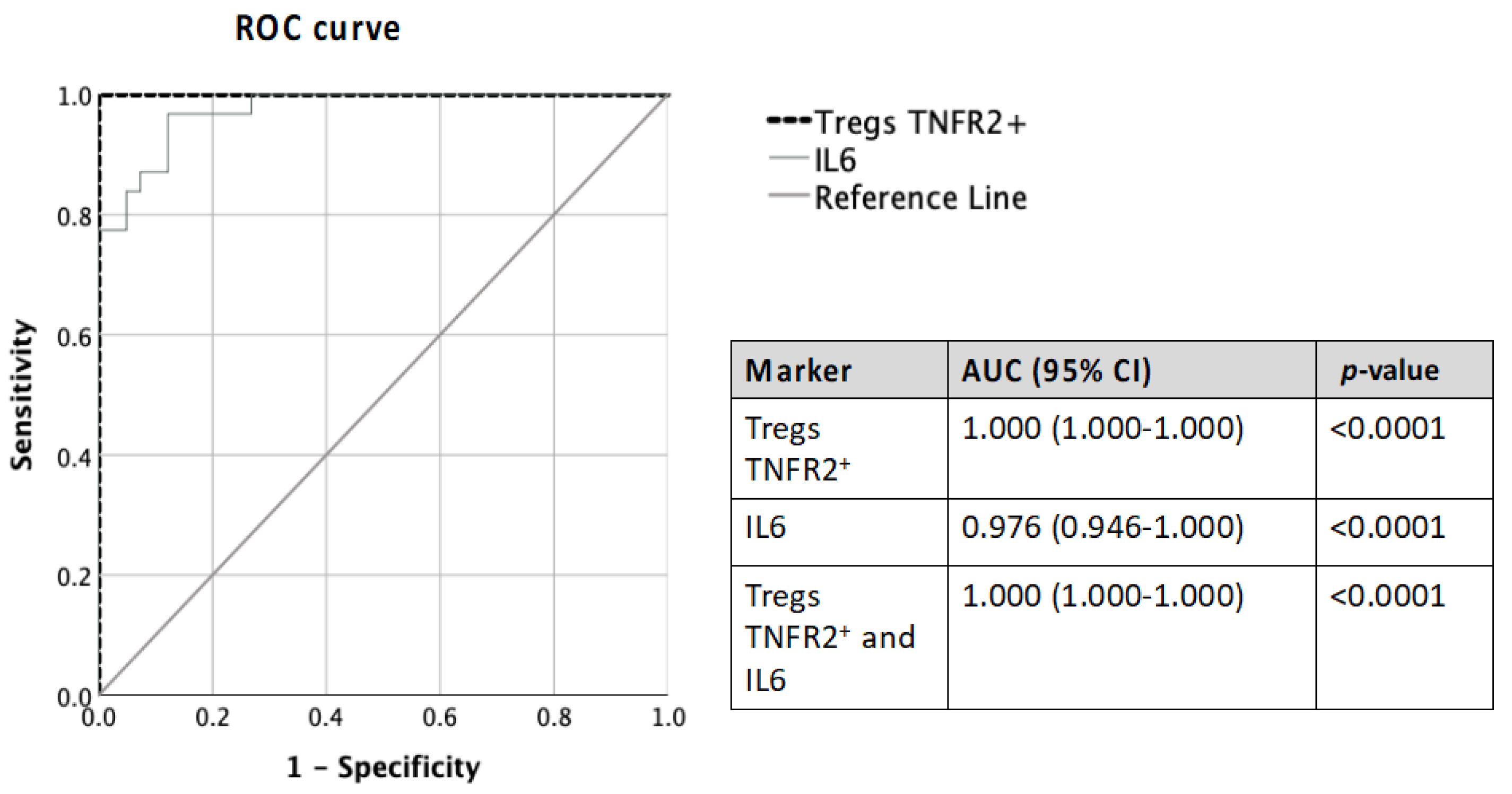
2.9.3. Receiver Operator Characteristic (ROC)
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bowtell, D.D.; Böhm, S.; Ahmed, A.; Aspuria, P.-J.; Bast, R.; Beral, V., Jr.; Berek, J.; Birrer, M.; Blagden, S.; Bookman, M. Rethinking ovarian cancer II: Reducing mortality from high-grade serous ovarian cancer. Nat. Rev. Cancer 2015, 15, 668–679. [Google Scholar] [CrossRef] [Green Version]
- Lheureux, S.; Braunstein, M.; Oza, A.M. Epithelial ovarian cancer: Evolution of management in the era of precision medicine. CA A Cancer J. Clin. 2019, 69, 280–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, J.; Wu, S.; Wang, J.; Sun, J.; He, Z.; Jin, X.; Zhang, W. The Effect of Histological Subtypes on Outcomes of Stage IV Epithelial Ovarian Cancer. Front. Oncol. 2018, 8, 577. [Google Scholar] [CrossRef]
- Cancer Data in Australia: Improving the Understanding of Ovarian Cancer Statistics. Available online: https://www.canceraustralia.gov.au/cancer-types/ovarian-cancer/statistics (accessed on 1 December 2022).
- Engelen, M.J.; Kos, H.E.; Willemse, P.H.; Aalders, J.G.; de Vries, E.G.; Schaapveld, M.; Otter, R.; van der Zee, A.G. Surgery by consultant gynecologic oncologists improves survival in patients with ovarian carcinoma. Cancer 2006, 106, 589–598. [Google Scholar] [CrossRef] [PubMed]
- Kontoninas, Z.; Kaiafa, G.D.; Saouli, Z.; Savopoulos, C.G.; Triantafyllos, D.; Anagnostopoulos, A.; Hatzitolios, A.I.; Papadopoulos, A. Tumor Markers in Diagnosis and Follow up of Haematologic Malignancies. Am. Soc. Hematol. 2016, 128, 5337. [Google Scholar] [CrossRef]
- Giamougiannis, P.; Martin-Hirsch, P.L.; Martin, F.L. The evolving role of MUC16 (CA125) in the transformation of ovarian cells and the progression of neoplasia. Carcinogenesis 2021, 42, 327–343. [Google Scholar] [CrossRef]
- Jacobs, I.; Bast, R.C., Jr. The CA 125 tumour-associated antigen: A review of the literature. Hum. Reprod. 1989, 4, 1–12. [Google Scholar] [CrossRef]
- Wang, Y.-S.; Ren, S.-F.; Jiang, W.; Lu, J.-Q.; Zhang, X.-Y.; Li, X.-P.; Cao, R.; Xu, C.-J. CA125-Tn ELISA assay improves specificity of pre-operative diagnosis of ovarian cancer among patients with elevated serum CA125 levels. Ann. Transl. Med. 2021, 9, 788. [Google Scholar] [CrossRef]
- Kang, K.N.; Koh, E.Y.; Jang, J.Y.; Kim, C.W. Multiple biomarkers are more accurate than a combination of carbohydrate antigen 125 and human epididymis protein 4 for ovarian cancer screening. Obstet. Gynecol. Sci. 2022, 65, 346–354. [Google Scholar] [CrossRef]
- Myers, E.; Bastian, B.; Havrilesky, L.; Kulasingam, S.; Terplan, M.; Cline, K.; Gray, R.; McCrory, D. Management of Adnexal Mass. In Evidence Report/Technology Assessment No. 130 (Prepared by the Duke Evidence-Based Practice Center under Contract No. 290-02-0025); Agency for Healthcare Research and Quality: Rockville, MD, USA, 2006. [Google Scholar]
- Engelen, M.J.A.; Bongaerts, A.H.H.; Sluiter, W.J.; de Haan, H.H.; Bogchelman, D.H.; TenVergert, E.M.; Willemse, P.H.B.; van der Zee, A.G.J. Distinguishing benign and malignant pelvic masses: The value of different diagnostic methods in everyday clinical practice. Eur. J. Obstet. Gynecol. Reprod. Biol. 2008, 136, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Anastasi, E.; Marchei, G.G.; Viggiani, V.; Gennarini, G.; Frati, L.; Reale, M.G. HE4: A new potential early biomarker for the recurrence of ovarian cancer. Tumor Biol. 2010, 31, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Van Gorp, T.; Cadron, I.; Despierre, E.; Daemen, A.; Leunen, K.; Amant, F.; Timmerman, D.; De Moor, B.; Vergote, I. HE4 and CA125 as a diagnostic test in ovarian cancer: Prospective validation of the Risk of Ovarian Malignancy Algorithm. Br. J. Cancer 2011, 104, 863–870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karlsen, N.S.; Karlsen, M.A.; Høgdall, C.K.; Høgdall, E. HE4 tissue expression and serum HE4 levels in healthy individuals and patients with benign or malignant tumours-a systematic review. Cancer Epidemiol. Prev. Biomark. 2014, 23, 2285–2295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hellström, I.; Raycraft, J.; Hayden-Ledbetter, M.; Ledbetter, J.A.; Schummer, M.; McIntosh, M.; Drescher, C.; Urban, N.; Hellström, K.E. The HE4 (WFDC2) protein is a biomarker for ovarian carcinoma. Cancer Res. 2003, 63, 3695–3700. [Google Scholar]
- Huang, J.; Chen, J.; Huang, Q. Diagnostic value of HE4 in ovarian cancer: A meta-analysis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 231, 35–42. [Google Scholar] [CrossRef]
- Moore, R.G.; Brown, A.K.; Miller, M.C.; Skates, S.; Allard, W.J.; Verch, T.; Steinhoff, M.; Messerlian, G.; DiSilvestro, P.; Granai, C. The use of multiple novel tumor biomarkers for the detection of ovarian carcinoma in patients with a pelvic mass. Gynecol. Oncol. 2008, 108, 402–408. [Google Scholar] [CrossRef]
- Dochez, V.; Caillon, H.; Vaucel, E.; Dimet, J.; Winer, N.; Ducarme, G. Biomarkers and algorithms for diagnosis of ovarian cancer: CA125, HE4, RMI and ROMA, a review. J. Ovarian Res. 2019, 12, 28. [Google Scholar] [CrossRef] [Green Version]
- Gentry-Maharaj, A.; Blyuss, O.; Ryan, A.; Burnell, M.; Karpinskyj, C.; Gunu, R.; Kalsi, J.K.; Dawnay, A.; Marino, I.P.; Manchanda, R.; et al. Multi-marker longitudinal algorithms incorporating HE4 and CA125 in ovarian cancer screening of postmenopausal women. Cancers 2020, 12, 1931. [Google Scholar] [CrossRef]
- Moore, R.G.; McMeekin, D.S.; Brown, A.K.; DiSilvestro, P.; Miller, M.C.; Allard, W.J.; Gajewski, W.; Kurman, R.; Bast, R.C.; Skates, S.J. A novel multiple marker bioassay utilizing HE4 and CA125 for the prediction of ovarian cancer in patients with a pelvic mass. Gynecol. Oncol. 2009, 112, 40–46. [Google Scholar] [CrossRef] [Green Version]
- The Cancer Genome Atlas Research Network; Weinstein, J.N.; Collisson, E.A.; Mills, G.B.; Shaw, K.R.; Ozenberger, B.A.; Ellrott, K.; Shmulevich, I.; Sander, C.; Stuart, J.M. The Cancer Genome Atlas Pan-Cancer analysis project. Nat. Genet. 2013, 45, 1113–1120. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Kim, B.; Song, Y.S. Ascites modulates cancer cell behavior, contributing to tumor heterogeneity in ovarian cancer. Cancer Sci. 2016, 107, 1173–1178. [Google Scholar] [CrossRef] [PubMed]
- da Silva, R.F.; Yoshida, A.; Cardozo, D.M.; Jales, R.M.; Paust, S.; Derchain, S.; Guimaraes, F. Natural Killer Cells Response to IL-2 Stimulation Is Distinct between Ascites with the Presence or Absence of Malignant Cells in Ovarian Cancer Patients. Int. J. Mol. Sci. 2017, 18, 856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Curiel, T.J.; Coukos, G.; Zou, L.; Alvarez, X.; Cheng, P.; Mottram, P.; Evdemon-Hogan, M.; Conejo-Garcia, J.R.; Zhang, L.; Burow, M.; et al. Specific recruitment of regulatory T cells in ovarian carcinoma fosters immune privilege and predicts reduced survival. Nat. Med. 2004, 10, 942–949. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, N.; Stenvers, K.L. Getting to know ovarian cancer ascites: Opportunities for targeted therapy-based translational research. Front. Oncol. 2013, 3, 256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Browning, L.; Patel, M.R.; Horvath, E.B.; Tawara, K.; Jorcyk, C.L. IL-6 and ovarian cancer: Inflammatory cytokines in promotion of metastasis. Cancer Manag. Res. 2018, 10, 6685. [Google Scholar] [CrossRef] [Green Version]
- Kampan, N.C.; Madondo, M.T.; Reynolds, J.; Hallo, J.; McNally, O.M.; Jobling, T.W.; Stephens, A.N.; Quinn, M.A.; Plebanski, M. Pre-operative sera interleukin-6 in the diagnosis of high-grade serous ovarian cancer. Sci. Rep. 2020, 10, 2213. [Google Scholar] [CrossRef] [Green Version]
- Maccio, A.; Madeddu, C. Inflammation and ovarian cancer. Cytokine 2012, 58, 133–147. [Google Scholar] [CrossRef] [Green Version]
- Kampan, N.; Xiang, S.; McNally, O.; Stephens, A.; Quinn, M.; Plebanski, M. Immunotherapeutic Interleukin-6 or Interleukin-6 receptor blockade in cancer: Challenges and opportunities. Curr. Med. Chem. 2018, 25, 4785–4806. [Google Scholar] [CrossRef]
- Nagarsheth, N.; Wicha, M.S.; Zou, W. Chemokines in the cancer microenvironment and their relevance in cancer immunotherapy. Nat. Rev. Immunol. 2017, 17, 559–572. [Google Scholar] [CrossRef] [Green Version]
- Becker, C.; Fantini, M.C.; Wirtz, S.; Nikolaev, A.; Lehr, H.A.; Galle, P.R.; Rose-John, S.; Neurath, M.F. IL-6 signaling promotes tumor growth in colorectal cancer. Cell Cycle 2005, 4, 217–220. [Google Scholar] [CrossRef]
- von Strandmann, E.P.; Reinartz, S.; Wager, U.; Müller, R. Tumor–Host Cell Interactions in Ovarian Cancer: Pathways to Therapy Failure. Trends Cancer 2017, 3, 137–148. [Google Scholar] [CrossRef]
- Duan, Z.; Foster, R.; Bell, D.A.; Mahoney, J.; Wolak, K.; Vaidya, A.; Hampel, C.; Lee, H.; Seiden, M.V. Signal transducers and activators of transcription 3 pathway activation in drug-resistant ovarian cancer. Clin. Cancer Res. 2006, 12, 5055–5063. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kampan, N.C.; Madondo, M.T.; McNally, O.M.; Quinn, M.; Plebanski, M. Paclitaxel and Its Evolving Role in the Management of Ovarian Cancer. Biomed Res. Int. 2015, 2015, 413076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Niu, X.L.; Qu, Y.; Wu, J.; Zhu, Y.Q.; Sun, W.J.; Li, L.Z. Autocrine production of interleukin-6 confers cisplatin and paclitaxel resistance in ovarian cancer cells. Cancer Lett. 2010, 295, 110–123. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Bruchim, I.; Graiver, D.; Evron, Z.; Oron-Karni, V.; Pasmanik-Chor, M.; Eitan, R.; Bernheim, J.; Levavi, H.; Fishman, A. Platinum-resistance in ovarian cancer cells is mediated by IL-6 secretion via the increased expression of its target cIAP-2. J. Mol. Med. 2013, 91, 357–368. [Google Scholar] [CrossRef]
- Dijkgraaf, E.; Santegoets, S.; Reyners, A.; Goedemans, R.; Wouters, M.; Kenter, G.; van Erkel, A.; van Poelgeest, M.; Nijman, H.; van der Hoeven, J. A phase I trial combining carboplatin/doxorubicin with tocilizumab, an anti-IL-6R monoclonal antibody, and interferon-α2b in patients with recurrent epithelial ovarian cancer. Ann. Oncol. 2015, 26, 2141–2149. [Google Scholar] [CrossRef]
- Kishimoto, T. Interleukin-6: Discovery of a pleiotropic cytokine. Arthritis Res. 2006, 8, S2. [Google Scholar] [CrossRef] [Green Version]
- Dobrzycka, B.; Mackowiak-Matejczyk, B.; Terlikowska, K.M.; Kulesza-Bronczyk, B.; Kinalski, M.; Terlikowski, S.J. Serum levels of IL-6, IL-8 and CRP as prognostic factors in epithelial ovarian cancer. Eur. Cytokine Netw. 2013, 24, 106–113. [Google Scholar] [CrossRef] [Green Version]
- Dijkgraaf, E.M.; Welters, M.J.; Nortier, J.W.; van der Burg, S.H.; Kroep, J.R. Interleukin-6/interleukin-6 receptor pathway as a new therapy target in epithelial ovarian cancer. Curr. Pharm. Des. 2012, 18, 3816–3827. [Google Scholar] [CrossRef]
- Chen, X.; Hamano, R.; Subleski, J.J.; Hurwitz, A.A.; Howard, O.M.; Oppenheim, J.J. Expression of costimulatory TNFR2 induces resistance of CD4+FoxP3- conventional T cells to suppression by CD4+FoxP3+ regulatory T cells. J. Immunol. 2010, 185, 174–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santinon, F.; Batignes, M.; Pouchy, C.; Salomon, B.; Decker, P.; Boissier, M.-C.; Semerano, L.; Bessis, N. 03.12 Tnfr2+ regulatory t cells subpopulations are highly suppressive and are increased on anti-tnf treatment. BMJ 2017, 76, A34–A35. [Google Scholar]
- Govindaraj, C.; Scalzo-Inguanti, K.; Madondo, M.; Hallo, J.; Flanagan, K.; Quinn, M.; Plebanski, M. Impaired Th1 immunity in ovarian cancer patients is mediated by TNFR2+ Tregs within the tumor microenvironment. Clin. Immunol. 2013, 149, 97–110. [Google Scholar] [CrossRef] [PubMed]
- Petrucelli, N.; Daly, M.B.; Pal, T. BRCA1-and BRCA2-Associated Hereditary Breast and Ovarian Cancer; University of Washington: Seattle, WA, USA, 2016. [Google Scholar]
- Prat, J.; FIGO Committee on Gynecologic Oncology. Staging classification for cancer of the ovary, fallopian tube, and peritoneum. Int. J. Gynecol. Obstet. 2014, 124, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Giuntoli, R.L.; Webb, T.J.; Zoso, A.; Rogers, O.; Diaz-Montes, T.P.; Bristow, R.E.; Oelke, M. Ovarian cancer-associated ascites demonstrates altered immune environment: Implications for antitumor immunity. Anticancer. Res. 2009, 29, 2875–2884. [Google Scholar] [PubMed]
- Finn, O.J. Immuno-oncology: Understanding the function and dysfunction of the immune system in cancer. Ann. Oncol. 2012, 23, VIII6–VIII9. [Google Scholar] [CrossRef] [PubMed]
- Darb-Esfahani, S.; Kunze, C.A.; Kulbe, H.; Sehouli, J.; Wienert, S.; Lindner, J.; Budczies, J.; Bockmayr, M.; Dietel, M.; Denkert, C.; et al. Prognostic impact of programmed cell death-1 (PD-1) and PD-ligand 1 (PD-L1) expression in cancer cells and tumor-infiltrating lymphocytes in ovarian high grade serous carcinoma. Oncotarget 2016, 7, 1486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colombo, M.P.; Piconese, S. Regulatory-T-cell inhibition versus depletion: The right choice in cancer immunotherapy. Nat. Rev. Cancer 2007, 7, 880–887. [Google Scholar] [CrossRef]
- Chen, X.; Wu, X.; Zhou, Q.; Howard, O.M.; Netea, M.G.; Oppenheim, J.J. TNFR2 is critical for the stabilization of the CD4+Foxp3+ regulatory T. cell phenotype in the inflammatory environment. J. Immunol. 2013, 190, 1076–1084. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Amarnath, S.; Chen, W. Requirement of CD28 signaling in homeostasis/survival of TGF-beta converted CD4+CD25+ Tregs from thymic CD4+CD25- single positive T cells. Transplantation 2006, 82, 953–964. [Google Scholar] [CrossRef]
- Zou, W. Regulatory T cells, tumour immunity and immunotherapy. Nat. Rev. Immunol. 2006, 6, 295–307. [Google Scholar] [CrossRef]
- Mavel, S.; Nadal-Desbarats, L.; Blasco, H.; Bonnet-Brilhault, F.; Barthélémy, C.; Montigny, F.; Sarda, P.; Laumonnier, F.; Vourc, P.; Andres, C.R. 1H–13C NMR-based urine metabolic profiling in autism spectrum disorders. Talanta 2013, 114, 95–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ito, T.; Hanabuchi, S.; Wang, Y.-H.; Park, W.R.; Arima, K.; Bover, L.; Qin, F.X.-F.; Gilliet, M.; Liu, Y.-J. Two functional subsets of FOXP3+ regulatory T cells in human thymus and periphery. Immunity 2008, 28, 870–880. [Google Scholar] [CrossRef] [PubMed]
- Edgell, T.; Martin-Roussety, G.; Barker, G.; Autelitano, D.; Allen, D.; Grant, P.L.; Rice, G. Phase II biomarker trial of a multimarker diagnostic for ovarian cancer. J. Cancer Res. Clin. Oncol. 2010, 136, 1079–1088. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kampan, N.C.; Madondo, M.T.; McNally, O.M.; Stephens, A.N.; Quinn, M.A.; Plebanski, M. Interleukin 6 Present in inflammatory ascites from advanced epithelial Ovarian cancer Patients Promotes Tumor necrosis Factor receptor 2-expressing regulatory T cells. Front. Immunol. 2017, 8, 1482. [Google Scholar] [CrossRef] [PubMed]
- Pinciroli, P.; Alberti, C.; Sensi, M.; Canevari, S.; Tomassetti, A. An IL6-correlated signature in serous epithelial ovarian cancer associates with growth factor response. BMC Genom. 2013, 14, 508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Yang, J.; Gao, Y.; Du, Y.; Bao, L.; Niu, W.; Yao, Z. Regulatory effect of e2, IL-6 and IL-8 on the growth of epithelial ovarian cancer cells. Cell. Mol. Immunol. 2005, 2, 365–372. [Google Scholar]
- Gorelik, E.; Landsittel, D.P.; Marrangoni, A.M.; Modugno, F.; Velikokhatnaya, L.; Winans, M.T.; Bigbee, W.L.; Herberman, R.B.; Lokshin, A.E. Multiplexed immunobead-based cytokine profiling for early detection of ovarian cancer. Cancer Epidemiol. Prev. Biomark. 2005, 14, 981–987. [Google Scholar] [CrossRef] [Green Version]
- Block, M.S.; Maurer, M.J.; Goergen, K.; Kalli, K.R.; Erskine, C.L.; Behrens, M.D.; Oberg, A.L.; Knutson, K.L. Plasma immune analytes in patients with epithelial ovarian cancer. Cytokine 2015, 73, 108–113. [Google Scholar] [CrossRef] [Green Version]
- Nowak, M.; Glowacka, E.; Szpakowski, M.; Szyllo, K.; Malinowski, A.; Kulig, A.; Tchorzewski, H.; Wilczynski, J. Proinflammatory and immunosuppressive serum, ascites and cyst fluid cytokines in patients with early and advanced ovarian cancer and benign ovarian tumors. Neuro Endocrinol. Lett. 2010, 31, 375–383. [Google Scholar]
- Tempfer, C.; Zeisler, H.; Sliutz, G.; Haeusler, G.; Hanzal, E.; Kainz, C. Serum evaluation of interleukin 6 in ovarian cancer patients. Gynecol. Oncol. 1997, 66, 27–30. [Google Scholar] [CrossRef] [PubMed]
- Vanamee, É.S.; Faustman, D.L. TNFR2: A Novel Target for Cancer Immunotherapy. Trends Mol. Med. 2017, 23, 1037–1046. [Google Scholar] [CrossRef] [PubMed]
- Okubo, Y.; Mera, T.; Wang, L.; Faustman, D.L. Homogeneous expansion of human T-regulatory cells via tumor necrosis factor receptor 2. Sci. Rep. 2013, 3, 3153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Govindaraj, C.; Madondo, M.; Kong, Y.Y.; Tan, P.; Wei, A.; Plebanski, M. Lenalidomide-based maintenance therapy reduces TNF receptor 2 on CD4 T cells and enhances immune effector function in acute myeloid leukemia patients. Am. J. Hematol. 2014, 89, 795–802. [Google Scholar] [CrossRef] [PubMed]
- Yan, F.; Du, R.; Wei, F.; Zhao, H.; Yu, J.; Wang, C.; Zhan, Z.; Ding, T.; Ren, X.; Chen, X. Expression of TNFR2 by regulatory T cells in peripheral blood is correlated with clinical pathology of lung cancer patients. Cancer Immunol. Immunother. 2015, 64, 1475–1485. [Google Scholar] [CrossRef]
- Wood, B.L.; Arroz, M.; Barnett, D.; DiGiuseppe, J.; Greig, B.; Kussick, S.J.; Oldaker, T.; Shenkin, M.; Stone, E.; Wallace, P. 2006 Bethesda International Consensus recommendations on the immunophenotypic analysis of hematolymphoid neoplasia by flow cytometry: Optimal reagents and reporting for the flow cytometric diagnosis of hematopoietic neoplasia. Cytom. Part B Clin. Cytom. 2007, 72, S14–S22. [Google Scholar] [CrossRef]
- Betters, D.M. Use of flow cytometry in clinical practice. J. Adv. Pract. Oncol. 2015, 6, 435. [Google Scholar]
- Chen, X.; Oppenheim, J.J. Targeting TNFR2, an immune checkpoint stimulator and oncoprotein, is a promising treatment for cancer. Sci. Signal. 2017, 10, eaal2328. [Google Scholar] [CrossRef]
- Torrey, H.; Butterworth, J.; Mera, T.; Okubo, Y.; Wang, L.; Baum, D.; Defusco, A.; Plager, S.; Warden, S.; Huang, D. Targeting TNFR2 with antagonistic antibodies inhibits proliferation of ovarian cancer cells and tumor-associated Tregs. Sci. Signal. 2017, 10, eaaf8608. [Google Scholar] [CrossRef]
- Masjedi, A.; Hashemi, V.; Hojjat-Farsangi, M.; Ghalamfarsa, G.; Azizi, G.; Yousefi, M.; Jadidi-Niaragh, F. The significant role of interleukin-6 and its signaling pathway in the immunopathogenesis and treatment of breast cancer. Biomed. Pharmacother. 2018, 108, 1415–1424. [Google Scholar] [CrossRef]
- Tan, Z.; Xue, H.; Sun, Y.; Zhang, C.; Song, Y.; Qi, Y. The role of tumor inflammatory microenvironment in lung cancer. Front. Pharmacol. 2021, 12, 688625. [Google Scholar] [CrossRef]
- Turano, M.; Cammarota, F.; Duraturo, F.; Izzo, P.; De Rosa, M. A potential role of IL-6/IL-6R in the development and management of colon cancer. Membranes 2021, 11, 312. [Google Scholar] [CrossRef] [PubMed]
- Waldner, M.J.; Foersch, S.; Neurath, M.F. Interleukin-6-a key regulator of colorectal cancer development. Int. J. Biol. Sci. 2012, 8, 1248. [Google Scholar] [CrossRef]
- Okuzono, Y.; Muraki, Y.; Sato, S. TNFR2 pathways are fully active in cancer regulatory T cells. Biosci. Biotechnol. Biochem. 2022, 86, 351–361. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, H.; Yoshimatsu, G.; Faustman, D.L. The Roles of TNFR2 Signaling in Cancer Cells and the Tumor Microenvironment and the Potency of TNFR2 Targeted Therapy. Cells 2022, 11, 1952. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.Y.; Papp, J.C.; Pellegrini, M.; Yu, H.; Sobel, E.M. Molecular Biology Networks and Key Gene Regulators for Inflammatory Biomarkers Shared by Breast Cancer Development: Multi-Omics Systems Analysis. Biomolecules 2021, 11, 1379. [Google Scholar] [CrossRef] [PubMed]
- Kopparam, J.; Meylan, E. RIP off STAT3 to counteract tumor progression. Cell Cycle 2017, 16, 1727–1728. [Google Scholar] [CrossRef]
- Lane, D.; Matte, I.; Garde-Granger, P.; Laplante, C.; Carignan, A.; Rancourt, C.; Piché, A. Inflammation-regulating factors in ascites as predictive biomarkers of drug resistance and progression-free survival in serous epithelial ovarian cancers. BMC cancer 2015, 15, 492. [Google Scholar] [CrossRef] [Green Version]
- Kroeger, P.T., Jr.; Drapkin, R. Pathogenesis and heterogeneity of ovarian cancer. Curr. Opin. Obstet. Gynecol. 2017, 29, 26. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, K.E.; Simmons, J.G.; Ding, S.; Van Landeghem, L.; Lund, P.K. Cytokine induction of tumor necrosis factor receptor 2 is mediated by STAT3 in colon cancer cells. Mol. Cancer Res. 2011, 9, 1718–1731. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Jia, M.; Wang, S.; Xu, S.; He, N. Antagonistic Antibody Targeting TNFR2 Inhibits Regulatory T Cell Function to Promote Anti-Tumor Activity. Front. Immunol. 2022, 13, 835690. [Google Scholar] [CrossRef] [PubMed]
- Sum, C.S.; Danton, M.; hu, Q.; Pritsker, A.; Lin, R.; Yu, R.; Chen, K.; Tang, F.; Pohl, T.; Wallner, S.; et al. Abstract 1869: Novel TNFR2 antibodies to overcome T cell exhaustion and suppressive tumor microenvironment. Cancer Res. 2021, 81 (Suppl. S13), 1869. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Age 18–80 | Age < 18 or >80 years |
| Signed written informed consent | Unable to give informed consent |
| Newly diagnosed, Stage III–IV, high-grade serous ovarian cancer (HGSOC) or benign ovarian tumour or normal ovaries, which are pathologically confirmed | Pregnant Cancer other than Stage III–IV HGSOC Concurrent other active cancers Concurrent significant pre-existing major medical conditions (such as heart, liver or vascular diseases) |
| No prior chemotherapy or radiotherapy | Major surgery, open biopsy or significant trauma or injury within 28 days prior to sampling |
| Receiving NSAIDS, anti-inflammatory steroids or immunosuppressive agents within 14 days prior to sampling | |
| Active inflammation, significant trauma or open wound |
| Ovarian Cancer n = 33 | Benign Ovaries n = 15 | Normal Ovaries n = 21 | p-Value | |
|---|---|---|---|---|
| Demographic data | ||||
| Mean age ± SD (years) Median Age range | 60.1 ± 1.59 60 41–83 | 54.8 ± 3.07 55.5 38–73 | 51 ± 2.20 48 40–84 | ap = 0.30 b p = 0.001 c p = 0.66 |
| Mean BMI ± SD (kg/m2) Median BMI range | 29.69 ± 0.85 28.5 24–40 | 29.73 ± 1.35 28 24–40 | 30.05 ± 1.20 28 24–43 | ns |
| Cancer characteristics | ||||
| Histology | High-grade papillary serous adenocarcinoma | Serous cystadenoma- n = 12 Fibrothecoma-n = 3 | No pathology | |
| Stage | IIIA-1 IIIB-2 IIIC-28 IV-2 | NA | NA | |
| Blood component counts | ||||
| Mean Hb (g/L) Median | 121.4 ± 16.8 122 | 121.2 ± 20.8 121 | 123 ± 15.7 122 | ns |
| Mean platelet Median | 327.8 ± 24.3 296 | 261 ± 21.1 229 | 267 ± 12.8 263 | ns |
| Mean WCC (×109/L) Median | 8.51 ± 2.89 8.5 | 9.30 ± 3.23 10.2 | 10.16 ± 3.3 10.2 | ns |
| Mean absolute neutrophil count (×109/L) Median | 5.92 ± 3.09 5.04 | 5.93 ± 2.89 5.49 | 6.86 ± 3.35 6.28 | ns |
| Mean total lymphocytes (×109/L) Median | 1.88 ± 0.58 1.8 | 2.72 ± 0.88 2.58 | 2.43 ± 0.65 2.26 | ap = 0.005 b p = 0.002 c p = 0.99 |
| Factors | AUC a | SE | p-Value b | 95% CI |
|---|---|---|---|---|
| Demographic data | ||||
| Age | 0.760 | 0.057 | 0.001 | 0.649–0.872 |
| Menopause | 0.801 | 0.054 | 0.001 | 0.695–0.908 |
| Laboratory parameters | ||||
| Haemoglobin (Hb) | 0.422 | 0.069 | ns | 0.287–0.557 |
| Platelet | 0.635 | 0.070 | ns | 0.498–0.771 |
| White cell count (WCC) | 0.366 | 0.067 | ns | 0.236–0.497 |
| Absolute neutrophil Counts (ANC) | 0.399 | 0.069 | ns | 0.263–0.535 |
| Total lymphocytes | 0.183 | 0.049 | 0.001 | 0.088–0.279 |
| Clinical tests and biomarkers | ||||
| CA125 | 0.986 | 0.010 | <0.0001 | 0.966–1.000 |
| HE4 | 0.997 | 0.001 | <0.0001 | 0.988–1.000 |
| Tregs phenotypes | ||||
| CD95+ | 0.630 | 0.068 | ns | 0.497–0.763 |
| CTLA-4+ | 0.608 | 0.072 | ns | 0.467–0.749 |
| IL6R+ | 0.855 | 0.045 | 0.001 | 0.767–0.944 |
| PD-L1+ | 0.710 | 0.061 | 0.002 | 0.590–0.831 |
| PD-1+ | 0.613 | 0.073 | ns | 0.470–0.755 |
| STAT3+ | 0.822 | 0.048 | 0.001 | 0.729–0.915 |
| TNFR2+ | 1.000 | 0.001 | <0.0001 | 1.000–1.000 |
| CCR4+ | 0.714 | 0.062 | 0.002 | 0.593–0.836 |
| CCR6+ | 0.524 | 0.07 | ns | 0.386–0.662 |
| CXCR3+ | 0.505 | 0.073 | ns | 0.362–0.648 |
| CCR7+ | 0.701 | 0.064 | 0.004 | 0.576–0.826 |
| CCR2+ | 0.707 | 0.064 | 0.003 | 0.582–0.833 |
| Teff phenotypes | ||||
| CD95+ | 0.600 | 0.069 | ns | 0.464–0.736 |
| CTLA-4+ | 0.476 | 0.08 | ns | 0.320–0.633 |
| IL6R+ | 0.696 | 0.063 | 0.005 | 0.572–0.820 |
| PDL1+ | 0.46 | 0.071 | ns | 0.320–0.600 |
| PD-1+ | 0.846 | 0.046 | 0.001 | 0.756–0.935 |
| STAT3+ | 0.864 | 0.042 | 0.001 | 0.783–0.946 |
| TNFR2+ | 0.462 | 0.079 | ns | 0.307–0.617 |
| CCR4+ | 0.646 | 0.074 | ns | 0.502–0.791 |
| CCR6+ | 0.352 | 0.074 | ns | 0.207–0.496 |
| CXCR3+ | 0.590 | 0.076 | ns | 0.440–0.739 |
| CCR7+ | 0.495 | 0.080 | ns | 0.339–0.652 |
| CCR2+ | 0.475 | 0.078 | ns | 0.303–0.611 |
| Soluble Factors | AUC a | SE | p-Value b | 95% CI |
|---|---|---|---|---|
| IL-1b | 0.611 | 0.067 | ns | 0.479–0.743 |
| IL-10 | 0.536 | 0.070 | ns | 0.398–0.674 |
| IL-13 | 0.42 | 0.070 | ns | 0.282–0.558 |
| IL-6 | 0.976 | 0.014 | <0.0001 | 0.948–1.000 |
| IL-12 | 0.415 | 0.071 | ns | 0.275–0.555 |
| RANTES | 0.377 | 0.067 | ns | 0.246–0.507 |
| EOTAXIN | 0.438 | 0.070 | ns | 0.300–0.576 |
| MIP-1α | 0.536 | 0.071 | ns | 0.397–0.675 |
| GMCSF | 0.58 | 0.072 | ns | 0.44–0.721 |
| MIP-1β | 0.421 | 0.070 | ns | 0.284–0.559 |
| MCP-1 | 0.471 | 0.074 | ns | 0.326–0.617 |
| IL-15 | 0.517 | 0.069 | ns | 0.381–0.652 |
| IL-5 | 0.565 | 0.070 | ns | 0.428–0.702 |
| IFN-γ | 0.367 | 0.068 | ns | 0.234–0.501 |
| IFN-α | 0.526 | 0.069 | ns | 0.391–0.66 |
| IL-1RA | 0.42 | 0.070 | ns | 0.283–0.556 |
| TNF-α | 0.538 | 0.068 | ns | 0.405–0.672 |
| IL-2 | 0.431 | 0.067 | ns | 0.299–0.563 |
| IL-7 | 0.526 | 0.069 | ns | 0.39–0.661 |
| IP-10 | 0.427 | 0.077 | ns | 0.276–0.579 |
| IL-2RA | 0.585 | 0.069 | ns | 0.449–0.721 |
| MIG | 0.602 | 0.067 | ns | 0.472–0.733 |
| IL-4 | 0.533 | 0.069 | ns | 0.398–0.668 |
| IL-8 | 0.743 | 0.025 | 0.001 | 0.618–0.868 |
| sTNFR2 | 0.528 | 0.07 | ns | 0.391–0.665 |
| MDC | 0.36 | 0.069 | 0.042 | 0.224–0.495 |
| TGF-β1 | 0.355 | 0.067 | 0.036 | 0.224–0.486 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kampan, N.C.; Kartikasari, A.E.R.; Deceneux, C.; Madondo, M.T.; McNally, O.M.; Flanagan, K.L.; Aziz, N.A.; Stephens, A.N.; Reynolds, J.; Quinn, M.A.; et al. Combining TNFR2-Expressing Tregs and IL-6 as Superior Diagnostic Biomarkers for High-Grade Serous Ovarian Cancer Masses. Cancers 2023, 15, 667. https://doi.org/10.3390/cancers15030667
Kampan NC, Kartikasari AER, Deceneux C, Madondo MT, McNally OM, Flanagan KL, Aziz NA, Stephens AN, Reynolds J, Quinn MA, et al. Combining TNFR2-Expressing Tregs and IL-6 as Superior Diagnostic Biomarkers for High-Grade Serous Ovarian Cancer Masses. Cancers. 2023; 15(3):667. https://doi.org/10.3390/cancers15030667
Chicago/Turabian StyleKampan, Nirmala Chandralega, Apriliana Ellya Ratna Kartikasari, Cyril Deceneux, Mutsa Tatenda Madondo, Orla M. McNally, Katie Louise Flanagan, Norhaslinda A. Aziz, Andrew N. Stephens, John Reynolds, Michael A. Quinn, and et al. 2023. "Combining TNFR2-Expressing Tregs and IL-6 as Superior Diagnostic Biomarkers for High-Grade Serous Ovarian Cancer Masses" Cancers 15, no. 3: 667. https://doi.org/10.3390/cancers15030667
APA StyleKampan, N. C., Kartikasari, A. E. R., Deceneux, C., Madondo, M. T., McNally, O. M., Flanagan, K. L., Aziz, N. A., Stephens, A. N., Reynolds, J., Quinn, M. A., & Plebanski, M. (2023). Combining TNFR2-Expressing Tregs and IL-6 as Superior Diagnostic Biomarkers for High-Grade Serous Ovarian Cancer Masses. Cancers, 15(3), 667. https://doi.org/10.3390/cancers15030667