
Relationship between Preoperative Pyuria and Bacille Calmette-Guerin Treatment in Intravesical Recurrence after Transurethral Resection of High-Risk, Non-Muscle Invasive, Bladder Carcinoma: A Retrospective Study of Human Data
 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Babjuk, M.; Oosterlinck, W.; Sylvester, R.; Kaasinen, E.; Böhle, A.; Palou-Redorta, J. EAU guidelines on non-muscle-invasive urothelial carcinoma of the bladder. Eur. Urol. 2008, 54, 303–314. [Google Scholar] [CrossRef]
- Chang, S.S.; Boorjian, S.A.; Chou, R.; Clark, P.E.; Daneshmand, S.; Konety, B.R.; Pruthi, R.; Quale, D.Z.; Ritch, C.R.; Seigne, J.D.; et al. Diagnosis and Treatment of Non-Muscle Invasive Bladder Cancer: AUA/SUO Guideline. J. Urol. 2016, 196, 1021–1029. [Google Scholar] [CrossRef]
- Sylvester, R.J.; van der Meijden, A.P.; Oosterlinck, W.; Witjes, J.A.; Bouffioux, C.; Denis, L.; Newling, D.D.; Kurth, K. Predicting recurrence and progression in individual patients with stage Ta T1 bladder cancer using EORTC risk tables: A combined analysis of 2596 patients from seven EORTC trials. Eur. Urol. 2006, 49, 466–477. [Google Scholar] [CrossRef]
- Nishimura, N.; Miyake, M.; Miyamoto, T.; Tomizawa, M.; Shimizu, T.; Morizawa, Y.; Hori, S.; Gotoh, D.; Nakai, Y.; Torimoto, K.; et al. The Japanese health care system-based cost-effectiveness of photodynamic diagnosis-assisted transurethral resection of bladder tumor for non-muscle invasive bladder cancer. Jpn. J. Clin. Oncol. 2022, hyac203. [Google Scholar] [CrossRef]
- Ferro, M.; Barone, B.; Crocetto, F.; Lucarelli, G.; Busetto, G.M.; Del Giudice, F.; Maggi, M.; Crocerossa, F.; Cantiello, F.; Damiano, R.; et al. Predictive clinico-pathological factors to identify BCG, unresponsive patients, after re-resection for T1 high grade non-muscle invasive bladder cancer. Urol. Oncol. 2022, 40, 490.e13–490.e20. [Google Scholar] [CrossRef]
- Ferro, M.; Tătaru, O.S.; Musi, G.; Lucarelli, G.; Abu Farhan, A.R.; Cantiello, F.; Damiano, R.; de Cobelli, O. Modified Glasgow Prognostic Score as a Predictor of Recurrence in Patients with High Grade Non-Muscle Invasive Bladder Cancer Undergoing Intravesical Bacillus Calmette-Guerin Immunotherapy. Diagnostics 2022, 12, 586. [Google Scholar] [CrossRef] [PubMed]
- Sazuka, T.; Sakamoto, S.; Imamura, Y.; Nakamura, K.; Yamamoto, S.; Arai, T.; Takeuchi, N.; Komiya, A.; Teishima, J.; Ichikawa, Y. Relationship between post-void residual urine volume, preoperative pyuria and intravesical recurrence after transurethral resection of bladder carcinoma. Int. J. Urol. 2020, 27, 1024–1030. [Google Scholar] [CrossRef] [PubMed]
- Sazuka, T.; Sakamoto, S.; Nakamura, K.; Imamura, Y.; Yamamoto, S.; Komiya, A.; Ichikawa, T. Impact of post-void residual urine volume on intravesical recurrence after nephroureterectomy for upper urinary tract urothelial carcinoma. Int. J. Urol. 2019, 26, 1106–1112. [Google Scholar] [CrossRef]
- Chou, R.; Selph, S.; Buckley, D.I.; Fu, R.; Griffin, J.C.; Grusing, S.; Gore, J.L. Intravesical Therapy for the Treatment of Nonmuscle Invasive Bladder Cancer: A Systematic Review and Meta-Analysis. J. Urol. 2017, 197, 1189–1199. [Google Scholar] [CrossRef]
- Matsumoto, K.; Kikuchi, E.; Shirakawa, H.; Hayakawa, N.; Tanaka, N.; Ninomiya, A.; Miyajima, A.; Nakamura, S.; Oya, M. Risk of subsequent tumour recurrence and stage progression in bacille Calmette-Guérin relapsing non-muscle-invasive bladder cancer. BJU Int. 2012, 110, E508–E513. [Google Scholar] [CrossRef] [PubMed]
- Suh, J.; Yuk, H.D.; Jeong, C.W.; Kwak, C.; Kim, H.H.; Ku, J.H. Pyuria as a Predictive Marker of Bacillus Calmette-Guérin Unresponsiveness in Non-Muscle Invasive Bladder Cancer. J. Clin. Med. 2021, 10, 3764. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, H.; Shiraishi, K.; Azuma, H.; Inoue, K.; Uemura, H.; Eto, M.; Ohyama, C.; Matsuyama, H. Clinical Practice Guidelines for Bladder Cancer 2019 update by the Japanese Urological Association: Summary of the revision. Int. J. Urol. 2020, 27, 702–709. [Google Scholar] [CrossRef] [PubMed]
- Del Giudice, F.; van Uem, S.; Li, S.; Vilson, F.L.; Sciarra, A.; Salciccia, S.; Busetto, G.M.; Maggi, M.; Tiberia, L.; Viscuso, P.; et al. Contemporary Trends of Systemic Neoadjuvant and Adjuvant Intravesical Chemotherapy in Patients with Upper Tract Urothelial Carcinomas Undergoing Minimally Invasive or Open Radical Nephroureterectomy: Analysis of US Claims on Perioperative Outcomes and Health Care Costs. Clin. Genitourin. Cancer 2022, 20, 198.e1–198.e9. [Google Scholar]
- Joice, G.A.; Bivalacqua, T.J.; Kates, M. Optimizing pharmacokinetics of intravesical chemotherapy for bladder cancer. Nat. Rev. Urol. 2019, 16, 599–612. [Google Scholar] [CrossRef] [PubMed]
- Krajewski, W.; Aumatell, J.; Subiela, J.D.; Nowak, Ł.; Tukiendorf, A.; Moschini, M.; Basile, G.; Poletajew, S.; Malkiewicz, B.; Del Giudice, F.; et al. Accuracy of the CUETO, EORTC 2016 and EAU 2021 scoring models and risk stratification tables to predict outcomes in high-grade non-muscle-invasive urothelial bladder cancer. Urol. Oncol. 2022, 40, 491.e11–491.e19. [Google Scholar] [CrossRef]
- Neuzillet, Y.; Pradère, B.; Xylinas, E.; Allory, Y.; Audenet, F.; Loriot, Y.; Masson-Lecomte, A.; Roumiguie, M.; Seisen, T.; Traxer, O.; et al. French AFU Cancer Committee Guidelines—Update 2022–2024: Non-muscle-invasive bladder cancer (NMIBC). Prog. Urol. 2022, 32, 1102–1140. [Google Scholar] [CrossRef]
- Jobczyk, M.; Stawiski, K.; Fendler, W.; Różański, W. Validation of EORTC, CUETO, and EAU risk stratification in prediction of recurrence, progression, and death of patients with initially non-muscle-invasive bladder cancer (NMIBC): A cohort analysis. Cancer Med. 2020, 9, 4014–4025. [Google Scholar] [CrossRef] [Green Version]
- Leo, M.C.; McMullen, C.K.; O’Keeffe-Rosetti, M.; Weinmann, S.; Garg, T.; Nielsen, M.E. External validation of the EORTC and NCCN bladder cancer recurrence and progression risk calculators in a U.S. community-based health system. Urol. Oncol. 2020, 38, 39.e21–39.e27. [Google Scholar] [CrossRef]
- Flaig, T.W.; Spiess, P.E.; Abern, M.; Agarwal, N.; Bangs, R.; Boorjian, S.A.; Buyyounouski, M.K.; Chan, K.; Chang, S.; Friedlander, T.; et al. NCCN Guidelines® Insights: Bladder Cancer, Version 2.2022. J. Natl. Compr. Canc. Netw. 2022, 20, 866–878. [Google Scholar] [CrossRef]
- Babjuk, M.; Burger, M.; Capoun, O.; Cohen, D.; Compérat, E.M.; Dominguez Escrig, J.L.; Mostafid, A.H.; Palou, J.; van Rhjin, B.W.; Roupret, M.; et al. European Association of Urology Guidelines on Non-muscle-invasive Bladder Cancer (Ta, T1, and Carcinoma in Situ). Eur. Urol. 2022, 81, 75–94. [Google Scholar] [CrossRef]
- Fankhauser, C.D.; Mostafid, H. Prevention of bladder cancer incidence and recurrence: Nutrition and lifestyle. Curr. Opin. Urol. 2018, 28, 88–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, S.; Redelman-Sidi, G. BCG in Bladder Cancer Immunotherapy. Cancers 2022, 14, 3073. [Google Scholar] [CrossRef]
- Gandhi, N.M.; Morales, A.; Lamm, D.L. Bacillus Calmette-Guérin immunotherapy for genitourinary cancer. BJU Int. 2013, 112, 288–297. [Google Scholar] [CrossRef] [PubMed]
- Miyake, M.; Nishimura, N.; Iida, K.; Fujii, T.; Nishikawa, R.; Teraoka, S.; Takenaka, A.; Kikuchi, H.; Abe, T.; Shinohara, N.; et al. Intravesical Bacillus Calmette-Guérin Treatment for T1 High-Grade Non-Muscle Invasive Bladder Cancer with Divergent Differentiation or Variant Morphologies. Cancers 2021, 13, 2615. [Google Scholar] [CrossRef]
- Blinova, E.; Enikeev, D.; Roshchin, D.; Samyshina, E.; Deryabina, O.; Tertychnyy, A.; Blinov, D.; Kogan, E.; Dudina, M.; Barakat, H.; et al. Relapse-Free Survival and PD-L1 Expression in First High- and Low-Grade Relapsed Luminal, Basal and Double-Negative P53-Mutant Non-Muscular Invasive Bladder Cancer Depending on Previous Chemo- and Immunotherapy. Cancers 2020, 12, 1316. [Google Scholar] [CrossRef] [PubMed]
- Savic, S.; Zlobec, I.; Thalmann, G.N.; Engeler, D.; Schmauss, M.; Lehmann, K.; Mattarelli, G.; Eichenberger, T.; Dalquen, P.; Spieler, P.; et al. The prognostic value of cytology and fluorescence in situ hybridization in the follow-up of nonmuscle-invasive bladder cancer after intravesical Bacillus Calmette-Guérin therapy. Int. J. Cancer 2009, 124, 2899–2904. [Google Scholar] [CrossRef] [PubMed]
- Roumiguié, M.; Kamat, A.M.; Bivalacqua, T.J.; Lerner, S.P.; Kassouf, W.; Böhle, A.; Brausi, M.; Buckley, R.; Persad, R.; Colombel, M.; et al. International Bladder Cancer Group Consensus Statement on Clinical Trial Design for Patients with Bacillus Calmette-Guérin-exposed High-risk Non-muscle-invasive Bladder Cancer. Eur. Urol. 2022, 82, 34–46. [Google Scholar] [CrossRef]
- Satake, N.; Ohno, Y.; Nakashima, J.; Ohori, M.; Tachibana, M. Prognostic value of preoperative pyuria in patients with non-muscle-invasive bladder cancer. Int. J. Urol. 2015, 22, 645–649. [Google Scholar] [CrossRef]
- Poletajew, S.; Gajewska, D.; Kaczmarek, K.; Krajewski, W.; Łykowski, M.; Sondka-Migdalska, J.; Borowik, M.; Buraczynski, P.; Dziegala, M.; Przudzik, M.; et al. Preoperative pyuria predicts the presence of high-grade bladder carcinoma in patients with bladder tumors. Cent. Eur. J. Urol. 2020, 73, 423–436. [Google Scholar]
- Azuma, T.; Nagase, Y.; Oshi, M. Pyuria predicts poor prognosis in patients with non-muscle-invasive bladder cancer. Clin. Genitourin. Cancer 2013, 11, 331–336. [Google Scholar] [CrossRef]
- Azuma, T.; Nagase, Y.; Oshi, M. Pyuria predicts poor prognosis in patients with non-muscle-invasive bladder cancer treated with bacillus Calmette-Guérin. Mol. Clin. Oncol. 2015, 3, 1113–1116. [Google Scholar] [CrossRef] [Green Version]
- Jimenez, D.G.; Sobti, A.; Askmyr, D.; Sakellariou, C.; Santos, S.C.; Swoboda, S.; Forslund, O.; Greiff, L.; Lindstedt, M. Tonsillar Cancer with High CD8(+) T-Cell Infiltration Features Increased Levels of Dendritic Cells and Transcriptional Regulation Associated with an Inflamed Tumor Microenvironment. Cancers 2021, 13, 5341. [Google Scholar] [CrossRef]
- Zhang, X.W.; Wald, A.; Salzmann, M.; Halama, N.; Hassel, J.C. Cytokine alterations during paraneoplastic neutrophilia and leukemoid reaction in patients with advanced melanoma. Cancer Immunol. Immunother. 2023, 72, 509–513. [Google Scholar] [CrossRef] [PubMed]
- Markowski, A.R.; Markowska, A.J.; Ustymowicz, W.; Pryczynicz, A.; Guzińska-Ustymowicz, K. Simultaneous analysis of tumor-infiltrating immune cells density, tumor budding status, and presence of lymphoid follicles in CRC tissue. Sci. Rep. 2022, 12, 21732. [Google Scholar] [CrossRef] [PubMed]
- Tazzyman, S.; Lewis, C.E.; Murdoch, C. Neutrophils: Key mediators of tumour angiogenesis. Int. J. Exp. Pathol. 2009, 90, 222–231. [Google Scholar] [CrossRef]
- Jablonska, J.; Leschner, S.; Westphal, K.; Lienenklaus, S.; Weiss, S. Neutrophils responsive to endogenous IFN-beta regulate tumor angiogenesis and growth in a mouse tumor model. J. Clin. Invest. 2010, 120, 1151–1164. [Google Scholar] [CrossRef] [PubMed]
- Müller, I.; Munder, M.; Kropf, P.; Hänsch, G.M. Polymorphonuclear neutrophils and T lymphocytes: Strange bedfellows or brothers in arms? Trends Immunol. 2009, 30, 522–530. [Google Scholar] [CrossRef] [PubMed]
- Devi-Marulkar, P.; Fastenackels, S.; Karapentiantz, P.; Goc, J.; Germain, C.; Kaplon, H.; Knockaert, S.; Olive, D.; Panouillot, M.; Validire, P.; et al. Regulatory T cells infiltrate the tumor-induced tertiary lymphoïd structures and are associated with poor clinical outcome in NSCLC. Commun. Biol. 2022, 5, 1416. [Google Scholar] [CrossRef]
- Del Giudice, F.; Flammia, R.S.; Chung, B.I.; Moschini, M.; Pradere, B.; Mari, A.; Soria, F.; Albisinni, S.; Krajewski, W.; Szydelko, T.; et al. Compared Efficacy of Adjuvant Intravesical BCG-TICE vs. BCG-RIVM for High-Risk Non-Muscle Invasive Bladder Cancer (NMIBC): A Propensity Score Matched Analysis. Cancers 2022, 14, 887. [Google Scholar] [CrossRef]
- Tzimenatos, L.; Mahajan, P.; Dayan, P.S.; Vitale, M.; Linakis, J.G.; Blumberg, S.; Borgialli, D.; Ruddy, R.M.; Van Buren, J.; Ramilo, O.; et al. Accuracy of the Urinalysis for Urinary Tract Infections in Febrile Infants 60 Days and Younger. Pediatrics 2018, 141, 743–744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stamm, W.E. Criteria for the diagnosis of urinary tract infection and for the assessment of therapeutic effectiveness. Infection 1992, 20 (Suppl. S3), 151–154. [Google Scholar] [CrossRef] [PubMed]
- Wilks, J.M. Urine microscopy and infection in general practice. J. R. Coll. Gen. Pract. 1979, 29, 103–107. [Google Scholar] [PubMed]
- Busetto, G.M.; Giovannone, R.; Antonini, G.; Rossi, A.; Del Giudice, F.; Tricarico, S.; Ragonesi, G.; Gentile, V.; De Berardinis, E. Short-term pretreatment with a dual 5α-reductase inhibitor before bipolar transurethral resection of the prostate (B-TURP): Evaluation of prostate vascularity and decreased surgical blood loss in large prostates. BJU Int. 2015, 116, 117–123. [Google Scholar] [CrossRef] [Green Version]
- Liu, G.; Li, B.; Xu, Z.; Wang, J.; Ma, S.; Kan, Y.; Mao, L. Bacillus Calmette-Guerin for the Treatment of Non-muscle Invasive Bladder Cancer: History and Current Status. Discov. Med. 2022, 33, 85–92. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total n = 424 | Pyuria Present (n = 83) | Pyuria Absent (n = 341) | p-Value | ||
|---|---|---|---|---|---|
| Age | Median (range) | 72.5 (38–94) | 75 (50–90) | 72 (38–94) | 0.041 |
| Sex | Male | 336 (79.2) | 25 (30.1) | 278 (81.5) | 0.019 |
| Female | 88 (20.8) | 58 (69.9) | 63 (18.5) | ||
| Preoperative cytology | Positive | 83 (19.6) | 19 (22.9) | 64 (18.8) | 0.396 |
| Negative | 341 (80.4) | 64 (77.1) | 277 (81.2) | ||
| BCG therapy | Yes | 179 (42.2) | 45 (54.2) | 134 (39.2) | 0.0136 |
| No | 245 (57.8) | 38 (46.8) | 207 (60.8) | ||
| Grade | High | 325 (76.7) | 69 (83.1) | 256 (75.1) | 0.1196 |
| Low | 99 (23.3) | 14 (16.9) | 85 (24.9) | ||
| Pathological T stage, n (%) | T1 | 109 (25.7) | 32 (38.6) | 77 (22.6) | 0.0028 |
| Others | 315 (74.3) | 51 (61.4) | 264 (77.4) | ||
| Concomitant CIS | Present | 49 (11.6) | 9 (10.8) | 40 (11.7) | 0.827 |
| Absent | 375 (88.4) | 74 (89.2) | 301 (88.3) |
| Factor | n | Univariate Model | Multivariate Model | ||
|---|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | ||
| Sex | |||||
| Male | 336 | 1.18 (0.75–1.88) | 0.4857 | ||
| Female | 88 | ||||
| Preoperative cytology | |||||
| Pogitive | 83 | 1.03 (0.65–1.62) | 0.9144 | ||
| Negative | 341 | ||||
| BCG therapy | |||||
| Yes | 179 | 0.54 (0.36–0.81) | 0.0027 | 0.52 (0.34–0.80) | 0.0026 |
| No | 245 | ||||
| Grade | |||||
| High | 325 | 1.32 (0.87–2.01) | 0.1945 | 0.88 (0.57–1.37) | 0.5814 |
| Low | 99 | ||||
| Pathological T stage | |||||
| pT1 | 109 | 0.89 (0.59–1.35) | 0.5752 | ||
| Others | 315 | ||||
| Concomitant CIS | |||||
| Present | 49 | 0.85 (0.47–1.56) | 0.5914 | ||
| Absent | 375 | ||||
| Pyuria | |||||
| Present | 83 | 1.42 (0.92–2.21) | 0.1125 | 1.93 (1.26–2.95) | 0.0329 |
| Absent | 341 | ||||
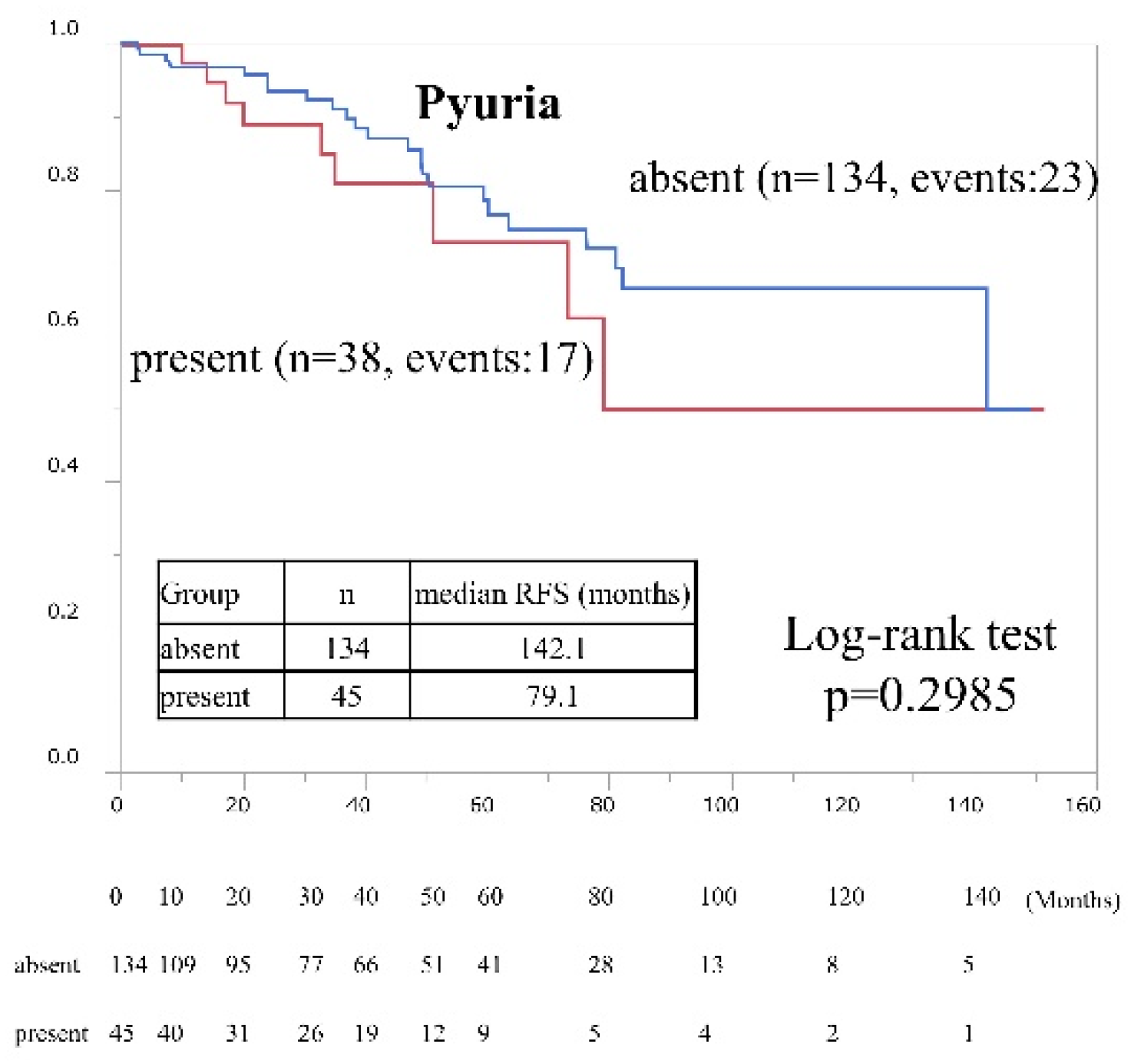
| Factor | n | Univariate Model | Multivariate Model | ||
|---|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | ||
| Sex | |||||
| Male | 141 | 1.14 (0.47–2.77) | 0.7774 | ||
| Female | 38 | ||||
| Preoperative cytology | |||||
| Pogitive | 55 | 0.81 (0.38–1.74) | 0.5967 | ||
| Negative | 124 | ||||
| Grade | |||||
| High | 160 | 0.47 (0.14–1.58) | 0.2533 | ||
| Low | 19 | ||||
| Pathological T stage | |||||
| pT1 | 64 | 0.89 (0.59–1.35) | 0.4008 | ||
| Others | 115 | ||||
| Concomitant CIS | |||||
| Present | 32 | 1.59 (0.72–3.55) | 0.2593 | ||
| Absent | 147 | ||||
| Pyuria | |||||
| Present | 45 | 1.50 (0.69–3.27) | 0.2985 | ||
| Absent | 134 | ||||
| Factor | n | Univariate Model | Multivariate Model | ||
|---|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | ||
| Sex | |||||
| Male | 195 | 1.22 (0.71–2.11) | 0.4699 | ||
| Female | 50 | ||||
| Preoperative cytology | |||||
| Positive | 217 | 1.75 (0.97–3.17) | 0.0645 | 1.84 (1.01–3.33) | 0.0459 |
| Negative | 28 | ||||
| Grade | |||||
| High | 165 | 1.00 (0.63–1.59) | 0.9999 | ||
| Low | 80 | ||||
| Pathological T stage | |||||
| pT1 | 45 | 0.87 (0.49–1.55) | 0.6477 | ||
| Others | 200 | ||||
| Concomitant CIS | |||||
| Present | 15 | 0.62 (0.23–1.69) | 0.3567 | ||
| Absent | 230 | ||||
| Pyuria | |||||
| Present | 38 | 1.70 (1.00–2.91) | 0.0485 | 1.77 (1.03–3.04) | 0.0371 |
| Absent | 207 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsukamoto, R.; Sazuka, T.; Hattori, Y.; Sato, H.; Arai, T.; Goto, Y.; Imamura, Y.; Sakamoto, S.; Ichikawa, T. Relationship between Preoperative Pyuria and Bacille Calmette-Guerin Treatment in Intravesical Recurrence after Transurethral Resection of High-Risk, Non-Muscle Invasive, Bladder Carcinoma: A Retrospective Study of Human Data. Cancers 2023, 15, 1638. https://doi.org/10.3390/cancers15061638
Tsukamoto R, Sazuka T, Hattori Y, Sato H, Arai T, Goto Y, Imamura Y, Sakamoto S, Ichikawa T. Relationship between Preoperative Pyuria and Bacille Calmette-Guerin Treatment in Intravesical Recurrence after Transurethral Resection of High-Risk, Non-Muscle Invasive, Bladder Carcinoma: A Retrospective Study of Human Data. Cancers. 2023; 15(6):1638. https://doi.org/10.3390/cancers15061638
Chicago/Turabian StyleTsukamoto, Ryo, Tomokazu Sazuka, Yoshinori Hattori, Hiroaki Sato, Takayuki Arai, Yusuke Goto, Yusuke Imamura, Shinichi Sakamoto, and Tomohiko Ichikawa. 2023. "Relationship between Preoperative Pyuria and Bacille Calmette-Guerin Treatment in Intravesical Recurrence after Transurethral Resection of High-Risk, Non-Muscle Invasive, Bladder Carcinoma: A Retrospective Study of Human Data" Cancers 15, no. 6: 1638. https://doi.org/10.3390/cancers15061638
APA StyleTsukamoto, R., Sazuka, T., Hattori, Y., Sato, H., Arai, T., Goto, Y., Imamura, Y., Sakamoto, S., & Ichikawa, T. (2023). Relationship between Preoperative Pyuria and Bacille Calmette-Guerin Treatment in Intravesical Recurrence after Transurethral Resection of High-Risk, Non-Muscle Invasive, Bladder Carcinoma: A Retrospective Study of Human Data. Cancers, 15(6), 1638. https://doi.org/10.3390/cancers15061638