
Wellbeing and Complementary Therapies in Breast Cancer Peripheral Neuropathy Care: A Scoping Review Focused on Foot Health

 , , ,
, , ,
Abstract
Simple Summary
Abstract
1. Introduction
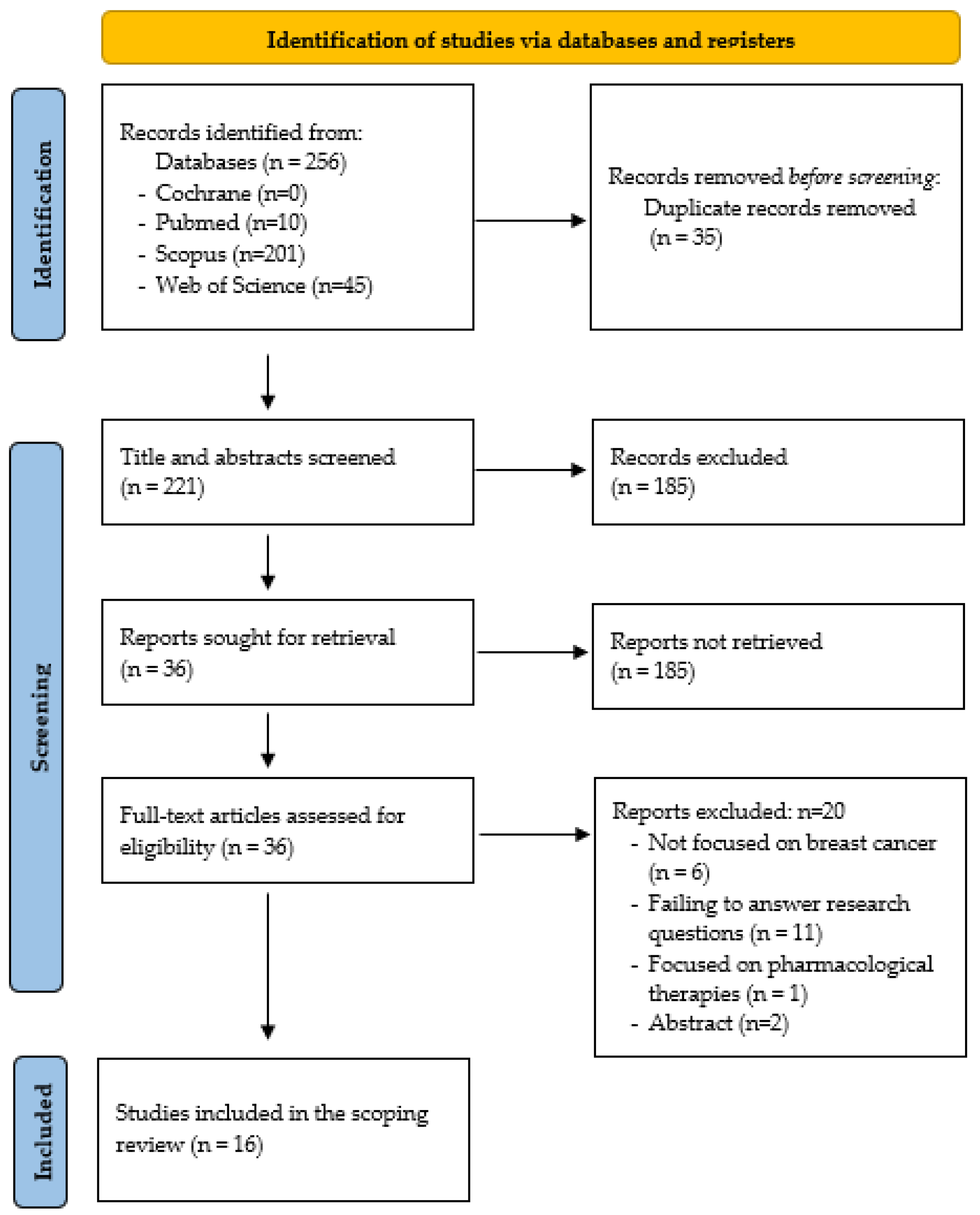
2. Materials and Methods
2.1. Identify the Research Questions
2.2. Identifying Relevant Studies
2.3. Study Selection, Charting the Data, and Analysis
3. Results
3.1. Bibliometric Characteristics
3.1.1. General Characteristics of the Documents Included
3.1.2. Study Population, Chemotherapeutic Agents, and Assessment of Neuropathy
3.2. Thematic Categories
3.2.1. Impact of Peripheral Neuropathy on Quality of Life and the Development of Comorbidities
3.2.2. Foot Health Repercussions: Gait and Active Lifestyle Issues
3.2.3. Complementary Therapies: The Focus of New Strategies for Peripheral Neuropathy
3.2.4. Need for Clinicians and Researchers to Become Involved in This Secondary Effect
4. Discussion
4.1. Quality of Life, Foot Health, and Gait Implications
4.2. Assessment Protocol
4.3. Complementary Therapies
4.4. Implications for Clinical Practice and Future Research
- (a)
- The study of the implications of CIPN on foot health and an active lifestyle, as there is a gap in knowledge about this field.
- (b)
- Agreeing on the CIPN assessment methods so the results can be comparable in terms of effectiveness between studies. Standardizing clinical assessment and creating procedural checklists will be necessary to ensure greater accuracy, as helpful diagnostic and assessment tools are lacking.
- (c)
- Developing, deepening, and confirming safe and effective preventive strategies that can take place in oncology centers. Taken together, these findings do not support strong recommendations to validate a complementary therapy that healthcare professionals should recommend. Further research could also be conducted to determine the effectiveness of exercise [30]. Likewise, few studies aimed to compare therapies with each other [21]. Lastly, one study found that a range of activities can be effective for the self-care of CIPN symptoms in the feet, but more research is needed [46].
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Web Site. Available online: https://www.who.int/es/health-topics/cancer#tab=tab_3 (accessed on 1 September 2022).
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Web Site. Available online: https://www.who.int/es/news-room/fact-sheets/detail/breast-cancer (accessed on 1 September 2022).
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Cancer statistics for the year 2020: An overview. Int. J. Cancer 2021, 149, 778–789. [Google Scholar] [CrossRef] [PubMed]
- DeSantis, C.E.; Bray, F.; Ferlay, J.; Lortet-Tieulent, J.; Anderson, B.O.; Jemal, A. International variation in female breast cancer incidence and mortality rates. Cancer Epidemiol. Biomark. Prev. 2015, 24, 1495–1506. [Google Scholar] [CrossRef] [PubMed]
- Pilleron, S.; Alqurini, N.; Ferlay, J.; Haase, K.R.; Hannan, M.; Janssen-Heijnen, M.; Kantilal, K.; Katanoda, K.; Kenis, C.; Lu-Yao, G.; et al. International trends in cancer incidence in middle-aged and older adults in 44 countries. J. Geriatr. Oncol. 2022, 13, 346–355. [Google Scholar] [CrossRef]
- Lipscombe, L.L.; Fischer, H.D.; Austin, P.C.; Fu, L.; Jaakkimainen, R.L.; Ginsburg, O.; Rochon, P.A.; Narod, S.; Paszat, L. The association between diabetes and breast cancer stage at diagnosis: A population-based study. Breast Cancer Res. Treat. 2015, 150, 613–620. [Google Scholar] [CrossRef]
- American Cancer Society. Cancer Web Site. Available online: https://www.cancer.org/cancer/breast-cancer/treatment/chemotherapy-for-breast-cancer.html (accessed on 1 September 2022).
- Rivera, D.R.; Ganz, P.A.; Weyrich, M.S.; Bandos, H.; Melnikow, J. Chemotherapy-associated peripheral neuropathy in patients with early-stage breast cancer: A systematic review. J. Natl. Cancer Inst. 2018, 110, djx140. [Google Scholar] [CrossRef]
- American Cancer Society. Cancer Web Site. Available online: https://www.cancer.org/treatment/treatments-and-side-effects/physical-side-effects/peripheral-neuropathy/what-is-peripherial-neuropathy.html (accessed on 1 September 2022).
- Seretny, M.; Currie, G.L.; Sena, E.S.; Ramnarine, S.; Grant, R.; MacLeod, M.R.; Colvin, L.A.; Fallon, M. Incidence, prevalence, and pre-dictors of chemotherapy-induced peripheral neuropathy: A systematic review and meta-analysis. Pain 2014, 155, 2461–2470. [Google Scholar] [CrossRef]
- Jordan, B.; Margulies, A.; Cardoso, F.; Cavaletti, G.; Haugness, H.S.; Jahn, P.; Rhun, E.L.; Preusser, M.; Scotté, F.; Taphoom, M.J.B.; et al. Systemic anticancer therapy-induced peripheral and central neurotoxicity: ESMO–EONS–EANO Clinical Practice Guidelines for diagnosis, prevention, treatment and follow-up. Ann. Oncol. 2020, 31, 1306–1319. [Google Scholar] [CrossRef]
- Ducic, I.; Short, K.W.; Dellon, A.L. Relationship between loss of pedal sensibility, balance, and falls in patients with peripheral neuropathy. Ann. Plast. Surg. 2004, 52, 535–540. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Wang, M.; Molassiotis, A. Mapping chemotherapy-induced peripheral neuropathy phenotype and health-related quality of life in patients with cancer through exploratory analysis of multimodal assessment data. Support. Care Cancer 2022, 30, 4007–4017. [Google Scholar] [CrossRef]
- Emine, K.E.; Gulbeyaz, C. The effect of salt-water bath in the management of treatment-related peripheral neuropathy in cancer patients receiving taxane and platinum-based treatment. Explore 2022, 18, 347–356. [Google Scholar] [CrossRef]
- Jue, M.; Shah, D.; Stiles, A.; Nisar, T. Impact of Cold Therapy on Paclitaxel-Induced Peripheral Neuropathy and Quality of Life in Patients With Breast Cancer. Clin. J. Oncol. Nurs. 2022, 26, 93–99. [Google Scholar] [CrossRef]
- Engvall, K.; Gréen, H.; Fredrikson, M.; Lagerlund, M.; Lewin, F.; Avall-Lundqvist, E. Impact of persistent peripheral neuropathy on health-related quality of life among early-stage breast cancer survivors: A population-based cross-sectional study. Breast Cancer Res. Treat. 2022, 195, 379–391. [Google Scholar] [CrossRef]
- Coolbrandt, A.; Vancoille, K.; Dejaeger, E.; Peeters, H.; Laenen, A.; Neven, P.; Punie, K.; Wildiers, H. Preventing taxane-related peripheral neuropathy, pain and nail toxicity: A prospective self-controlled trial comparing hilotherapy with frozen gloves in early breast cancer. Breast Cancer Res. Treat. 2022, 192, 293–301. [Google Scholar] [CrossRef]
- Simsek, N.Y.; Demir, A. Cold application and exercise on development of peripheral neuropathy during taxane chemotherapy in breast cancer patients: A randomized controlled trial. Asia-Pac. J. Oncol. Nurs. 2021, 8, 255–268. [Google Scholar] [CrossRef]
- Müller, J.; Weiler, M.; Schneeweiss, A.; Martin Haag, G.; Steindorf, K.; Wick, W.; Wiskemann, J. Preventive effect of sensorimotor exercise and resistance training on chemotherapy-induced peripheral neuropathy: A randomised-controlled trial. Br. J. Cancer 2021, 125, 955–965. [Google Scholar] [CrossRef]
- Oneda, E.; Meriggi, F.; Zanotti, L.; Zaina, E.; Bighè, S.; Andreis, F.; Rueda, S.; Zaniboni, A. Innovative approach for the prevention of chemotherapy-induced peripheral neuropathy in cancer patients: A pilot study with the hilotherm device, the poliambulanza hospital experience. Integr. Cancer Ther. 2020, 19, 1534735420943287. [Google Scholar] [CrossRef]
- Hirose, C.; Fujii, H.; Iihara, H.; Ishihara, M.; Nawa-Nishigaki, M.; Kato-Hayashi, H.; Ohata, K.; Sekiya, K.; Kitahora, M.; Matsuhashi, N. Real-world data of the association between quality of life using the EuroQol 5 Dimension 5 Level utility value and adverse events for outpatient cancer chemotherapy. Support. Care Cancer 2020, 28, 5943–5952. [Google Scholar] [CrossRef]
- Ruddy, K.J.; Le-Rademacher, J.; Lacouture, M.E.; Wilkinson, M.; Onitilo, A.A.; Vander Woude, A.C.; Grosse-Perdekamp, M.T.; Dockter, T.; Tan, D.A.; Beutler, A.; et al. Randomized controlled trial of cryotherapy to prevent paclitaxel-induced peripheral neuropathy (RU221511I); an ACCRU trial. Breast 2019, 48, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, C.; Kwon, N.; Beaumont, J.L.; Paice, J.A. Cold therapy to prevent paclitaxel-induced peripheral neuropathy. Support. Care Cancer 2018, 26, 3461–3469. [Google Scholar] [CrossRef] [PubMed]
- Kleckner, I.R.; Kamen, C.; Gewandter, J.S.; Mohile, N.A.; Heckler, C.E.; Culakova, E.; Fung, C.; Janelsins, M.; Asare, M.; Lin, P.; et al. Effects of exercise during chemotherapy on chemotherapy-induced peripheral neuropathy: A multicenter, randomized controlled trial. Support. Care Cancer 2018, 26, 1019–1028. [Google Scholar] [CrossRef] [PubMed]
- Bao, T.; Basal, C.; Seluzicki, C.; Li, S.; Seidman, A.; Mao, J. Long-term chemotherapy-induced peripheral neuropathy among breast cancer survivors: Prevalence, risk factors, and fall risk. Breast Cancer Res. Treat. 2016, 159, 327–333. [Google Scholar] [CrossRef]
- Pachman, D.R.; Weisbrod, B.L.; Seisler, D.K.; Barton, D.L.; Fee-Schroeder, K.C.; Smith, T.J.; Lachance, D.H.; Liu, H.; Sjeñerid, R.A.; Cheville, A.L.; et al. Pilot evaluation of Scrambler therapy for the treatment of chemotherapy-induced peripheral neuropathy. Support. Care Cancer 2015, 23, 943–951. [Google Scholar] [CrossRef]
- Bland, K.A.; Kirkham, A.A.; Bovard, J.; Shenkier, T.; Zucker, D.; McKenzie, D.C.; Davis, M.K.; Gelmon, K.A.; Campbell, K.L. Effect of exercise on taxane chemotherapy–induced peripheral neuropathy in women with breast cancer: A randomized controlled trial. Clin. Breast Cancer 2019, 19, 411–422. [Google Scholar] [CrossRef]
- Hanai, A.; Ishiguro, H.; Sozu, T.; Tsuda, M.; Yano, I.; Nakagawa, T.; Imai, S.; Hamabe, Y.; Masakazu, T.; Arai, H.; et al. Effects of cryotherapy on objective and subjective symptoms of paclitaxel-induced neuropathy: Prospective self-controlled trial. J. Natl. Cancer Inst. 2018, 110, 141–148. [Google Scholar] [CrossRef]
- Dieci, M.V.; Guarneri, V.; Conte, P. The Future of Chemotherapy in the Era of Personalized Medicine. Curr. Breast Cancer Rep. 2013, 5, 57–68. [Google Scholar] [CrossRef]
- Kerckhove, N.; Collin, A.; Condé, S.; Chaleteix, C.; Pezet, D.; Balayssac, D. Long-term effects, pathophysiological mechanisms, and risk factors of chemotherapy-induced peripheral neuropathies: A comprehensive literature review. Front. Pharmacol. 2017, 8, 86. [Google Scholar] [CrossRef]
- Shah, A.; Hoffman, E.M.; Mauermann, M.L.; Loprinzi, C.L.; Windebank, A.J.; Klein, C.J.; Staff, N.P. Incidence and disease burden of chemotherapy-induced peripheral neuropathy in a population-based cohort. J. Neurol. Neurosurg. Psychiatry 2018, 89, 636–641. [Google Scholar] [CrossRef]
- Ganz, P.A.; Dougherty, P.M. Painful Hands and Feet After Cancer Treatment: Inflammation Affecting the Mind-Body Connection. J. Clin. Oncol. 2016, 34, 649–652. [Google Scholar] [CrossRef]
- Nemenov, M.I.; Alaverdyan, H.; Burk, C.; Roles, K.; Frey, K.; Yan, Y.; Kazinets, G.; Haroutounian, S. Characterization of Patients With and Without Painful Peripheral Neuropathy After Receiving Neurotoxic Chemotherapy: Traditional Quantitative Sensory Testing vs. C-Fiber and Aδ-Fiber Selective Diode Laser Stimulation. J. Pain 2022, 23, 796–809. [Google Scholar] [CrossRef]
- Timmins, H.C.; Li, T.; Kiernan, M.C.; Baron-Hay, S.; Marx, G.; Boyle, F.; Goldstein, D.; Park, S.B. Taxane-induced peripheral neuropathy: Differences in patient report and objective assessment. Support. Care Cancer 2020, 28, 4459–4466. [Google Scholar] [CrossRef]
- Smith, E.M.; Pang, H.; Cirrincione, C.; Fleishman, S.; Paskett, E.D.; Ahles, T.; Bressler, L.R.; Faul, C.E.; Know, C.; Le-Lindqwister, N.; et al. Effect of duloxetine on pain, function, and quality of life among patients with chemotherapy-induced painful peripheral neuropathy: A randomized clinical trial. JAMA 2013, 309, 1359–1367. [Google Scholar] [CrossRef]
- Jones, K.F.; Wechsler, S.; Zulewski, D.; Wood, L. Pharmacological and non-pharmacological management of chemotherapy-induced peripheral neuropathy: A scoping review of randomized controlled trials. J. Palliat. Med. 2022, 25, 964–995. [Google Scholar] [CrossRef]
- Pachman, D.R.; Dockter, T.; Zekan, P.J.; Fruth, B.; Ruddy, K.J.; Ta, L.E.; Lakfy, J.M.; Dentchev, T.; Le-Lindqwister, N.; Sikov, W.M.; et al. A pilot study of minocycline for the prevention of paclitaxel-associated neuropathy: ACCRU study RU221408I. Support. Care Cancer 2017, 25, 3407–3416. [Google Scholar] [CrossRef]
- Greenlee, H.; DuPont-Reyes, M.J.; Balneaves, L.G.; Carlson, L.E.; Cohen, M.R.; Deng, G.; Johnson, J.A.; Mumber, M.; Seely, D.; Zick, S.M.; et al. Clinical practice guidelines on the evidence-based use of integrative therapies during and after breast cancer treatment. CA Cancer J. Clin. 2017, 67, 194–232. [Google Scholar] [CrossRef] [PubMed]
- Tamburin, S.; Park, S.B.; Schenone, A.; Mantovani, E.; Hamedani, M.; Alberti, P.; Yildiz-Kabak, V.; Kleckner, I.R.; Kolb, N.; Mazzucchelli, M.; et al. Rehabilitation, exercise, and related non-pharmacological interventions for chemotherapy-induced peripheral neurotoxicity: Systematic review and evidence-based recommendations. Crit. Rev. Oncol. Hematol. 2022, 171, 103575. [Google Scholar] [CrossRef] [PubMed]
- Yoo, Y.; Cho, O. Relationship between quality of life and nurse-led bedside symptom evaluations in patients with chemotherapy-induced peripheral neuropathy. Asian Nurs. Res. 2014, 8, 36–41. [Google Scholar] [CrossRef]
- Kaley, T.J.; DeAngelis, L.M. Therapy of chemotherapy-induced peripheral neuropathy. Br. J. Haematol. 2009, 145, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Tolotti, A.; Pedrazzani, C.; Bonetti, L.; Bianchi, M.; Valcarenghi, D. Patients’ and Nurses’ Perceptions of the Effectiveness of an Oral Cancer Agent Education Process: A Mixed-Methods Study. Cancer Nurs. 2021, 44, E151–E162. [Google Scholar] [CrossRef]
- Ogle, T.; Alexander, K.; Yates, P.; Paul, S.M.; Kober, K.M.; Conley, Y.P.; Schumacher, M.; David, J.; Miaskowski, C. Occurrence and perceived effectiveness of activities used to decrease chemotherapy-induced peripheral neuropathy symptoms in the feet. Eur. J. Oncol. Nurs. 2021, 54, 102025. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Inclusion Criteria |
|---|---|
| Year | Last 10 years |
| Study type | Original articles (randomized controlled trials, controlled clinical trials, case series, case reports, pilot clinical studies, longitudinal studies, and observational studies), reviews, and conference papers |
| Language | English, Portuguese, and Spanish |
| Population | >18 years |
| Cancer type | Breast cancer |
| Drug therapy | Chemotherapy |
| Scoping objective(s) |
|
| Author, Year, Country | Journal | Type of Study | Sample | Chemotherapy | Research Aim | Main Results | Assessment/ Complementary Therapy |
|---|---|---|---|---|---|---|---|
| Wang et al. [16] (2022), Hong Kong | Supportive Care in Cancer | Cross-sectional study | n = 87 Breast (42.5%) and colorectal (34.5%) cancer | Taxane, platinum | To identify the phenotype of CIPN and to examine the association with general symptoms and QoL. | Sensory symptoms are the most relevant. Worsening neuropathy contributes to a deteriorating QoL. It is associated with increased symptom burden, decreased physical wellbeing, and impaired tendon reflex. | Assessment NCI-CTCAE, TNSc, BPI, FACT/GOG-NtxS |
| Emine et al. [17] (2022), Turkey | Explore | Prospective experimental pilot study | n = 103 Breast (46.6%), colon (11.6%), gynecological (28.1%), and other (13.6%) cancers | Taxane, platinum, Taxane- platinum | To determine the effect of bathing with salt water in the management of CIPN. | Baths with cold salt water statistically significantly decrease the scores associated with the symptoms of peripheral neuropathy developed by taxanes and platinum. It is an effective approach to improve QoL. | Assessment NCI-CTCAE Therapy: Intervention Salt-water bath
|
| Jue et al. [18] (2022), United States | Clinical Journal of Oncology Nursing | Randomized controlled trial | n = 48 Breast cancer | Taxane | To examine the difference in the severity and frequency of CIPN and QoL between the group receiving cold therapy and those receiving standard care. | Cold therapy effectively reduces peripheral neuropathy caused by taxanes. Regarding QoL, both groups had no significant differences. | Assessment FACT-Taxane questionnaire, CTCAE Therapy: Preventive Cold Therapy
|
| Engvall et al. [19] (2022), Sweden | Breast Cancer Research and Treatment | Cohort study | n = 646 Breast cancer | Taxane | To explore the impact of CIPN on QoL. | CIPN triggers clinically relevant deterioration in global QoL, functioning, and economics. The domains “Difficulty walking due to foot drop” and “problems standing/walking due to difficulty feeling the ground underfoot” are especially highlighted. | Assessment EORTC QLQ-C30, CIPN20 |
| Coolbrandt et al. [20] (2022), Belgium | Breast Cancer Research and Treatment | Prospective self-controlled study | n = 63 Breast cancer | Taxane | To explore the efficacy of thread therapy on the right hand and foot and frozen gloves on the left hand and foot in people with breast cancer treated with paclitaxel or docetaxel. | Hilotherapy is a better alternative to prevent clinically significant taxane-related side effects compared to frozen gloves. Perceived comfort was statistically significantly better for hilotherapy (<0.0001). | Assessment NCI-CTCAE Therapy: Preventive Hilotherapy vs. frozen gloves
|
| Simsek et al. [21] (2021), Turkey | Asia-Pacific Journal of Oncology Nursing | Multicenter three-arm parallel randomized clinical trial | n = 90 Breast cancer | Taxane | To compare the effect of cold application and exercise on the development of peripheral neuropathy in people with breast cancer and chemotherapy. | Exercise significantly reduces neuropathy symptoms of numbness in both hands and feet compared to cold application. The exercise program is more effective than cold application for preventing neuropathy in people receiving taxanes. | Assessment CIPNAT Therapy: Intervention Cold application vs. Exercise
|
| Müller et al. [22] (2021), Germany | British Journal of Cancer | Intervention trial | n = 170 Breast (74%), pancreatic (6%), prostate (3%) and other cancers (17%) | Taxane, taxane-platinum, platinum | To investigate the preventive potential of sensorimotor and resistance training for peripheral neuropathy. | Sensorimotor and/or resistance training alleviate subjectively perceived sensory symptoms in the feet. Other clinically relevant results related to cancer therapy are achieved if an adequate training stimulus is achieved. | Assessment TNS, EORTC QLQ-CIPN15, EORTC QLQ-C30 Therapy: Preventive Sensorimotor and resistance exercise Program: sensorimotor 3/week for 35 min. Resistance 2/week for 45 min. |
| Oneda et al. [23] (2020), Italy | Integrative Cancer Therapies | Single-arm, single-center clinical pilot trial | n = 64 Breast (65.6%), gynecologic (31.3%), and pancreatic (3.1%) cancer | Taxane, platinum | To evaluate the prevention and reduction of peripheral neuropathy through the constant application of cold sleeves on the hands and feet. | Hilotherapy presents adequate efficacy and tolerability. This research shows that it seems to be able to prevent or reduce the symptoms of neuropathy. It is necessary to expand the study sample and add other treatment arms to the trial. | Assessment EORTC QLQ-C30, CTCAE Therapy: Preventive Hilotherm Device
|
| Hirose, et al. [24] (2020), Japan | Supportive Care in Cancer | Descriptive single-center study | n = 4695 Colorectal (16.8%), breast (11.5%) cancer, and others | Taxane platinum | To investigate the relationship between chemotherapy-induced adverse events and QoL. | Peripheral neuropathy, malaise, extremity edema, and dry skin are significantly correlated with decreased QoL, regardless of the type of cancer or anticancer drugs used. | Assessment EuroQoL 5 Dimensión 5 Level (EQ-5D-5L) |
| Ruddy et al. [25] (2019), United States | Breast | Randomized prospective clinical pilot trial | n = 42 Breast cancer | Taxane | To assess the cooling of hands and feet during paclitaxel treatment to prevent peripheral neuropathy. | There were no significant differences in peripheral neuropathy between the group that received cryotherapy and the group that received control care. More research is needed, as the group that received cryotherapy had less neuropathy. | Assessment EORTC QLQ CIPN-20 Therapy: Preventive Cryotherapy
|
| Griffiths et al. [26] (2018), United States | Supportive Care in Cancer | Cases and controls | n = 29 Breast cancer | Antracycline plus taxane | To assess the efficacy of cryotherapy in preventing taxane-induced neuropathic pain. | There were no significant differences in peripheral neuropathy between treated and untreated hands or feet. Safe and effective preventive strategies for peripheral neuropathy pain in oncology centers should be implemented. | Assessment BPI, QST, NPSI Therapy: Preventive Cold therapy
|
| Kleckner et al. [27] (2018), United States | Supportive Care in Cancer | Multicenter randomized controlled clinical trial | n = 355 Breast (79%), lymphoma (5%), colon (5%), lung (3%), and other (7%) cancers | Taxane, platinum, taxane-platinum | To examine the effects of exercise on the symptoms of CIPN. | Exercise appears to reduce the symptoms of CIPN in patients receiving taxane, platinum, or alkaloid-based chemotherapy. Health professionals are encouraged to prescribe exercise for these patients. | Assessment CIPN Symptoms Therapy: Preventive Walking and resistance exercise
|
| Bao et al. [28] (2016), United States | Breast Cancer Research and Treatment | Longitudinal prospective study | n = 296 Breast cancer | Taxane | To determine the prevalence of CIPN, risk factors, and their association with long-term psychological distress and falls. | Of all studied patients, 58.4% reported neuropathic symptoms. People with neuropathy have greater psychological distress and numbers of falls. Obesity is a significant risk factor. Interventions should focus on incorporating fall prevention strategies and psycho-emotional interventions. | Assessment Neuropathic symptoms |
| Pachman et al. [29] (2015), United States | Supportive Care in Cancer | Open pilot trial | n = 37 Cancer types: 13 breast, 7 ovarian, 6 colon, and others | Taxane, platinum, taxane-platinum | To investigate the effect of Scrambler therapy for the treatment of CIPN. | Scrambler therapy using non-invasive cutaneous electrostimulation can be effective for the treatment of neuropathy. More research and placebo-controlled clinical trials with larger sample sizes are needed to assess its efficacy better. | Assessment Peripheral neuropathy symptom questionnaire Therapy: Intervention Scrambler therapy
|
| Bland et al. [30] (2019), Canada | Clinical Breast Cancer | Randomized controlled trial | n = 27 Breast cancer | Taxane | To assess the effect of exercise on taxane-induced peripheral neuropathy in women with breast cancer. | Exercise may attenuate CIPN during the course of taxane chemotherapy and possibly improve adherence to taxanes in women with breast cancer. These findings need to be confirmed in more extensive trials. | Assessment EORTC QLQ CIPN20, Vibration Timing Test Therapy: Intervention Aerobic and resistance exercise.
|
| Hanai et al. [31] (2018), Japan | Journal of the National Cancer Institute | Self-controlled clinical trial | n = 40 Breast cancer | Taxane | To assess the efficacy of cryotherapy in preventing neuropathy caused by chemotherapy. | Cryotherapy is useful in preventing both objective and subjective symptoms and dysfunction resulting from CIPN. The incidence of objective and subjective signs was clinically and statistically significantly lower in the intervention group than in the control group, being a simple and effective preventive strategy in the case of paclitaxel. | Assessment Tactile, Thermosensory, Vibration Disturbance and Patient-Reported Assessment Therapy: Prevent Cryotherapy
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Veiga-Seijo, R.; Perez-Lopez, M.E.; Fernandez-Lopez, U.; Mosquera-Fernandez, A.; Seijo-Bestilleiro, R.; Gonzalez-Martin, C. Wellbeing and Complementary Therapies in Breast Cancer Peripheral Neuropathy Care: A Scoping Review Focused on Foot Health. Cancers 2023, 15, 2110. https://doi.org/10.3390/cancers15072110
Veiga-Seijo R, Perez-Lopez ME, Fernandez-Lopez U, Mosquera-Fernandez A, Seijo-Bestilleiro R, Gonzalez-Martin C. Wellbeing and Complementary Therapies in Breast Cancer Peripheral Neuropathy Care: A Scoping Review Focused on Foot Health. Cancers. 2023; 15(7):2110. https://doi.org/10.3390/cancers15072110
Chicago/Turabian StyleVeiga-Seijo, Raquel, Maria Eva Perez-Lopez, Uxia Fernandez-Lopez, Abian Mosquera-Fernandez, Rocio Seijo-Bestilleiro, and Cristina Gonzalez-Martin. 2023. "Wellbeing and Complementary Therapies in Breast Cancer Peripheral Neuropathy Care: A Scoping Review Focused on Foot Health" Cancers 15, no. 7: 2110. https://doi.org/10.3390/cancers15072110
APA StyleVeiga-Seijo, R., Perez-Lopez, M. E., Fernandez-Lopez, U., Mosquera-Fernandez, A., Seijo-Bestilleiro, R., & Gonzalez-Martin, C. (2023). Wellbeing and Complementary Therapies in Breast Cancer Peripheral Neuropathy Care: A Scoping Review Focused on Foot Health. Cancers, 15(7), 2110. https://doi.org/10.3390/cancers15072110