
ERBB2 Amplification as a Predictive and Prognostic Biomarker in Upper Tract Urothelial Carcinoma

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population and Clinicopathological Data Assessment
2.2. Construction of Tissue Microarrays (TMAs)
2.3. IHC
2.4. FISH
2.5. Statistical Analysis
3. Results
3.1. Tumor and Patients Characteristics
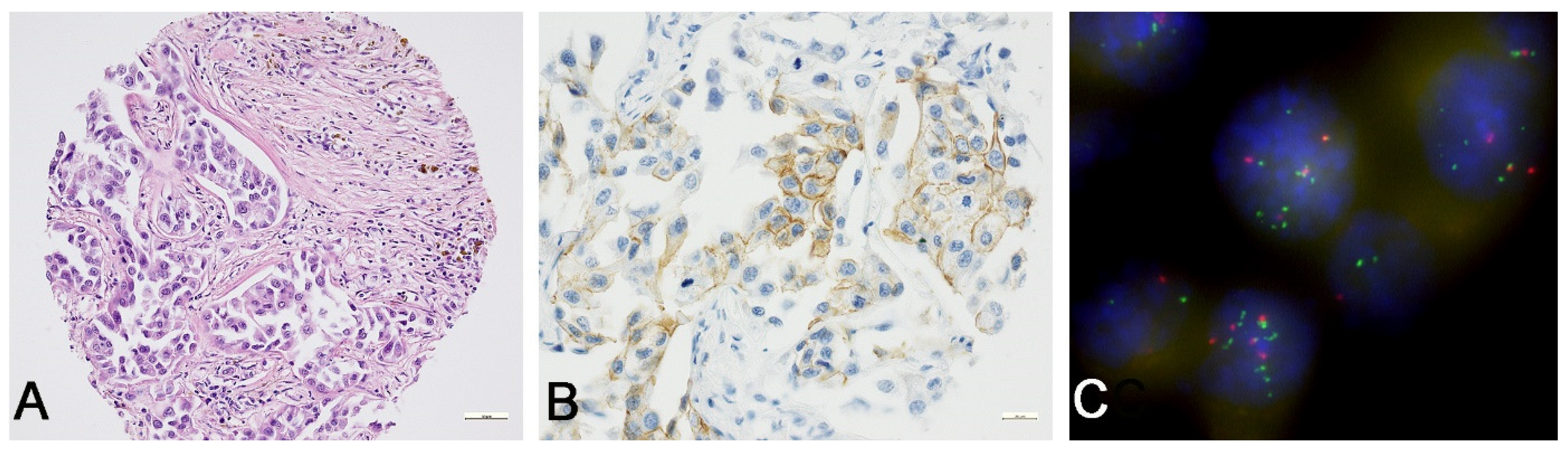
3.2. Morphological Evaluation (H&E Stains)
3.3. Determination of ERBB2 Status
3.3.1. ERBB2 Immunoscoring
3.3.2. ERBB2 FISH Analysis
3.3.3. Quality Parameters and Correlation Analyses
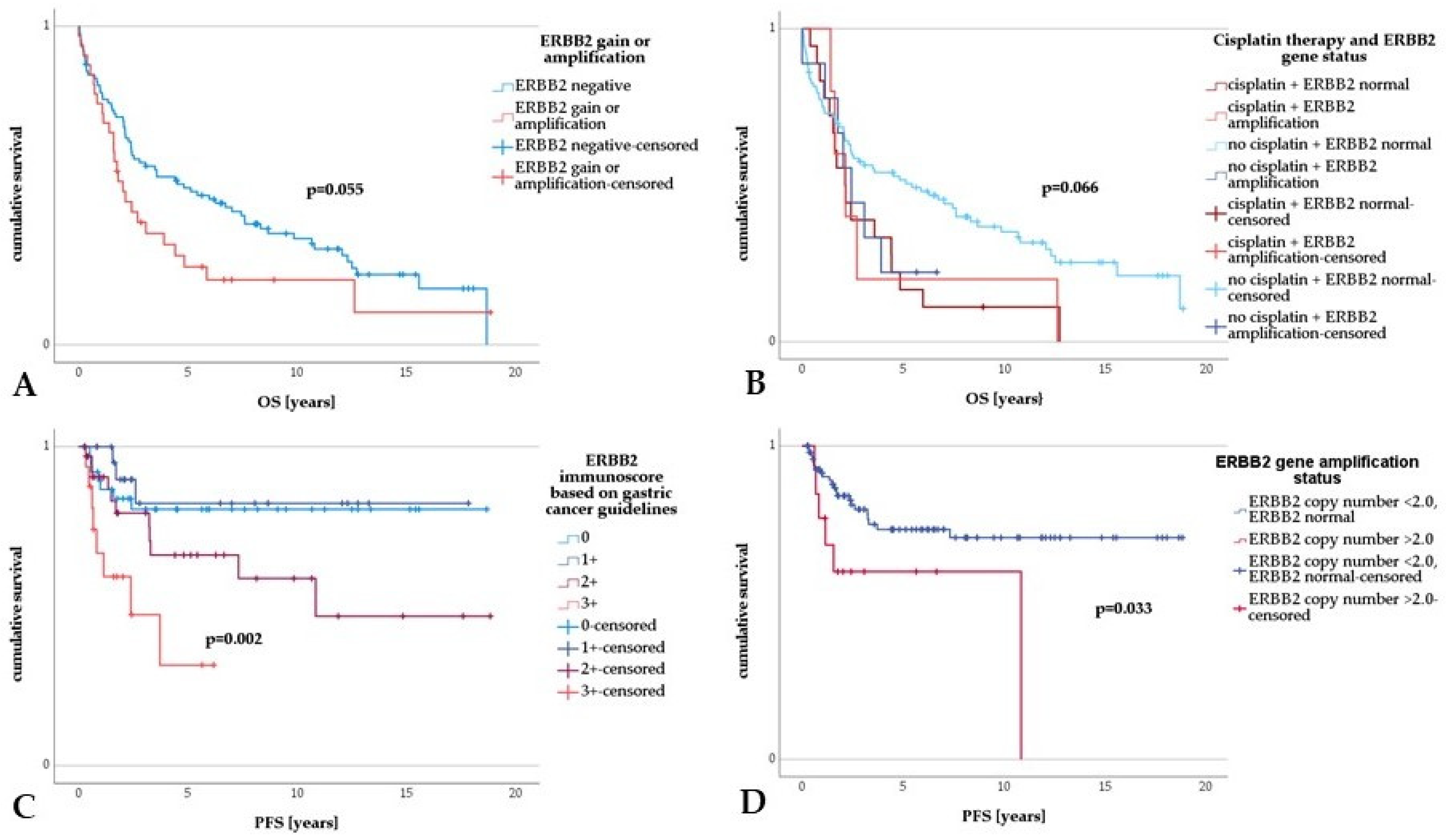
3.4. Survival Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rouprêt, M.; Babjuk, M.; Burger, M.; Capoun, O.; Cohen, D.; Compérat, E.M.; Cowan, N.C.; Dominguez-Escrig, J.L.; Gontero, P.; Hugh Mostafid, A.; et al. European Association of Urology Guidelines on Upper Urinary Tract Urothelial Carcinoma: 2020 Update. Eur. Urol. 2020, 79, 62–79. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef]
- Rouprêt, M.; Babjuk, M.; Compérat, E.; Zigeuner, R.; Sylvester, R.J.; Burger, M.; Cowan, N.C.; Böhle, A.; van Rhijn, B.W.G.; Kaasinen, E.; et al. European Association of Urology Guidelines on Upper Urinary Tract Urothelial Cell Carcinoma: 2015 Update. Eur. Urol. 2015, 68, 868–879. [Google Scholar] [CrossRef] [PubMed]
- Olgac, S.; Mazumdar, M.; Dalbagni, G.; Reuter, V.E. Urothelial carcinoma of the renal pelvis: A clinicopathologic study of 130 cases. Am. J. Surg. Pathol. 2004, 28, 1545–1552. [Google Scholar] [CrossRef]
- Maruschke, M.; Kram, W.; Zimpfer, A.; Kundt, G.; Hakenberg, O.W. Upper Urinary Tract Tumors: Which Diagnostic Methods Are Needed? Urol. Int. 2017, 98, 304–311. [Google Scholar] [CrossRef]
- Margulis, V.; Shariat, S.F.; Matin, S.F.; Kamat, A.M.; Zigeuner, R.; Kikuchi, E.; Lotan, Y.; Weizer, A.; Raman, J.D.; Wood, C.G. Outcomes of Radical Nephroureterectomy: A Series from the Upper Tract Urothelial Carcinoma Collaboration. Cancer 2009, 115, 1224–1233. [Google Scholar] [CrossRef]
- Abouassaly, R.; Alibhai, S.M.H.; Shah, N.; Timilshina, N.; Fleshner, N.; Finelli, A. Troubling outcomes from population-level analysis of surgery for upper tract urothelial carcinoma. Urology 2010, 76, 895–901. [Google Scholar] [CrossRef] [PubMed]
- Jeldres, C.; Sun, M.; Isbarn, H.; Lughezzani, G.; Budäus, L.; Alasker, A.; Shariat, S.F.; Lattouf, J.-B.; Widmer, H.; Pharand, D.; et al. A population-based assessment of perioperative mortality after nephroureterectomy for upper-tract urothelial carcinoma. Urology 2010, 75, 315–320. [Google Scholar] [CrossRef]
- Birtle, A.; Johnson, M.; Chester, J.; Jones, R.; Dolling, D.; Bryan, R.T.; Harris, C.; Winterbottom, A.; Blacker, A.; Catto, J.W.F.; et al. Adjuvant chemotherapy in upper tract urothelial carcinoma (the POUT trial): A phase 3, open-label, randomised controlled trial. Lancet 2020, 395, 1268–1277. [Google Scholar] [CrossRef]
- Moasser, M.M. The oncogene HER2: Its signaling and transforming functions and its role in human cancer pathogenesis. Oncogene 2007, 26, 6469–6487. [Google Scholar] [CrossRef] [PubMed]
- Ménard, S.; Pupa, S.M.; Campiglio, M.; Tagliabue, E. Biologic and therapeutic role of HER2 in cancer. Oncogene 2003, 22, 6570–6578. [Google Scholar] [CrossRef]
- Torres-Jiménez, J.; Esteban-Villarrubia, J.; Ferreiro-Monteagudo, R. Precision Medicine in Metastatic Colorectal Cancer: Targeting ERBB2 (HER-2) Oncogene. Cancers 2022, 14, 3718. [Google Scholar] [CrossRef] [PubMed]
- Yan, M.; Schwaederle, M.; Arguello, D.; Millis, S.Z.; Gatalica, Z.; Kurzrock, R. HER2 expression status in diverse cancers: Review of results from 37,992 patients. Cancer Metastasis Rev. 2015, 34, 157–164. [Google Scholar] [CrossRef]
- Ursini-Siegel, J.; Schade, B.; Cardiff, R.D.; Muller, W.J. Insights from transgenic mouse models of ERBB2-induced breast cancer. Nat. Rev. Cancer 2007, 7, 389–397. [Google Scholar] [CrossRef] [PubMed]
- Bang, Y.-J.; van Cutsem, E.; Feyereislova, A.; Chung, H.C.; Shen, L.; Sawaki, A.; Lordick, F.; Ohtsu, A.; Omuro, Y.; Satoh, T.; et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): A phase 3, open-label, randomised controlled trial. Lancet 2010, 376, 687–697. [Google Scholar] [CrossRef]
- Audenet, F.; Isharwal, S.; Cha, E.K.; Donoghue, M.T.A.; Drill, E.N.; Ostrovnaya, I.; Pietzak, E.J.; Sfakianos, J.P.; Bagrodia, A.; Murugan, P.; et al. Clonal Relatedness and Mutational Differences between Upper Tract and Bladder Urothelial Carcinoma. Clin. Cancer Res. 2019, 25, 967–976. [Google Scholar] [CrossRef]
- Aumayr, K.; Klatte, T.; Neudert, B.; Birner, P.; Shariat, S.; Schmidinger, M.; Susani, M.; Haitel, A. HER2 and TOP2A Gene Amplification and Protein Expression in Upper Tract Urothelial Carcinomas. Pathol. Oncol. Res. 2018, 24, 575–581. [Google Scholar] [CrossRef]
- Ehsani, L.; Osunkoya, A.O. Human epidermal growth factor receptor 2 expression in urothelial carcinoma of the renal pelvis: Correlation with clinicopathologic parameters. Int. J. Clin. Exp. Pathol. 2014, 7, 2544–2550. [Google Scholar] [PubMed]
- Galanakis, I.; Spyropoulos, E.; Gkialas, I.; Nomikos, A.; Souka, E.; Mitropoulos, D. ErbB2, ErbB3 and ErbB4 expression in urothelial tumors of the upper urinary tract and their prognostic significance. J. BUON 2013, 18, 653–659. [Google Scholar] [PubMed]
- Imai, T.; Kimura, M.; Takeda, M.; Tomita, Y. Significance of epidermal growth factor receptor and c-erbB-2 protein expression in transitional cell cancer of the upper urinary tract for tumour recurrence at the urinary bladder. Br. J. Cancer 1995, 71, 69–72. [Google Scholar] [CrossRef]
- Kim, G.; Chung, Y.R.; Kim, B.; Song, B.; Moon, K.C. Comparison of the FDA and ASCO/CAP Criteria for HER2 Immunohistochemistry in Upper Urinary Tract Urothelial Carcinoma. J. Pathol. Transl. Med. 2016, 50, 436–441. [Google Scholar] [CrossRef]
- Langner, C.; Gross, C.; Rehak, P.; Ratschek, M.; Rüschoff, J.; Zigeuner, R. HER2 protein overexpression and gene amplification in upper urinary tract transitional cell carcinoma: Systematic analysis applying tissue microarray technique. Urology 2005, 65, 176–180. [Google Scholar] [CrossRef]
- Sasaki, Y.; Sasaki, T.; Kawai, T.; Morikawa, T.; Matsusaka, K.; Kunita, A.; Kume, H.; Aoki, I.; Homma, Y.; Fukayama, M. HER2 protein overexpression and gene amplification in upper urinary tract urothelial carcinoma-an analysis of 171 patients. Int. J. Clin. Exp. Pathol. 2014, 7, 699–708. [Google Scholar]
- Soria, F.; Moschini, M.; Haitel, A.; Wirth, G.J.; Karam, J.A.; Wood, C.G.; Rouprêt, M.; Margulis, V.; Karakiewicz, P.I.; Briganti, A.; et al. HER2 overexpression is associated with worse outcomes in patients with upper tract urothelial carcinoma (UTUC). World J. Urol. 2017, 35, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Tsai, Y.-S.; Tzai, T.-S.; Chow, N.-H.; Wu, C.-L. Frequency and clinicopathologic correlates of ErbB1, ErbB2, and ErbB3 immunoreactivity in urothelial tumors of upper urinary tract. Urology 2005, 66, 1197–1202. [Google Scholar] [CrossRef] [PubMed]
- Vershasselt-Crinquette, M.; Colin, P.; Ouzzane, A.; Gnemmi, V.; Robin, Y.-M.; Aubert, S.; Villers, A.; Leroy, X. Assessment of human epidermal growth factor receptor 2 status in urothelial carcinoma of the upper urinary tract: A study using dual-color in situ hybridization and immunohistochemistry. Appl. Immunohistochem. Mol. Morphol. 2012, 20, 363–366. [Google Scholar] [CrossRef] [PubMed]
- Yorozu, T.; Sato, S.; Kimura, T.; Iwatani, K.; Onuma, H.; Yanagisawa, T.; Miki, J.; Egawa, S.; Ikegami, M.; Takahashi, H. HER2 Status in Molecular Subtypes of Urothelial Carcinoma of the Renal Pelvis and Ureter. Clin. Genitourin. Cancer 2020, 18, e443–e449. [Google Scholar] [CrossRef]
- Marín, A.P.; Arranz, E.E.; Sánchez, A.R.; Auñón, P.Z.; Barón, M.G. Role of anti-Her-2 therapy in bladder carcinoma. J. Cancer Res. Clin. Oncol. 2010, 136, 1915–1920. [Google Scholar] [CrossRef]
- Wolff, A.C.; Hammond, M.E.H.; Allison, K.H.; Harvey, B.E.; Mangu, P.B.; Bartlett, J.M.S.; Bilous, M.; Ellis, I.O.; Fitzgibbons, P.; Hanna, W.; et al. Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Focused Update. Arch. Pathol. Lab. Med. 2018, 142, 1364–1382. [Google Scholar] [CrossRef]
- Bartley, A.N.; Washington, M.K.; Colasacco, C.; Ventura, C.B.; Ismaila, N.; Benson, A.B.; Carrato, A.; Gulley, M.L.; Jain, D.; Kakar, S.; et al. HER2 Testing and Clinical Decision Making in Gastroesophageal Adenocarcinoma: Guideline From the College of American Pathologists, American Society for Clinical Pathology, and the American Society of Clinical Oncology. J. Clin. Oncol. 2017, 35, 446–464. [Google Scholar] [CrossRef]
- WHO Classification of Tumours, 5th ed.; Amin, M.B. (Ed.) International Agency for Research on Cancer: Lyon, France, 2022; ISBN 9789283245124. [Google Scholar]
- Brierley, J.D.; Gospodarowicz, M.K.; Wittekind, C. TNM Classification of Malignant Tumours, 8th ed.; John Wiley & Sons, Inc.: Chichester, UK; West Sussex, UK; Hoboken, NJ, USA, 2017; ISBN 9781119263579. [Google Scholar]
- Kononen, J.; Bubendorf, L.; Kallioniemi, A.; Bärlund, M.; Schraml, P.; Leighton, S.; Torhorst, J.; Mihatsch, M.J.; Sauter, G.; Kallioniemi, O.P. Tissue microarrays for high-throughput molecular profiling of tumor specimens. Nat. Med. 1998, 4, 844–847. [Google Scholar] [CrossRef]
- Schneider, B.; Glass, Ä.; Jagdmann, S.; Hühns, M.; Claus, J.; Zettl, H.; Dräger, D.-L.; Maruschke, M.; Hakenberg, O.W.; Erbersdobler, A.; et al. Loss of Mismatch-repair Protein Expression and Microsatellite Instability in Upper Tract Urothelial Carcinoma and Clinicopathologic Implications. Clin. Genitourin. Cancer 2020, 18, E563–E572. [Google Scholar] [CrossRef]
- Sassen, A.; Rochon, J.; Wild, P.; Hartmann, A.; Hofstaedter, F.; Schwarz, S.; Brockhoff, G. Cytogenetic analysis of HER1/EGFR, HER2, HER3 and HER4 in 278 breast cancer patients. Breast Cancer Res. 2008, 10, R2. [Google Scholar] [CrossRef] [PubMed]
- Lenhard, W.; Lenhard, A. Berechnung von Testgütekriterien für Screeningverfahren. Available online: http://www.psychometrica.de/testkennwerte.html (accessed on 23 August 2022).
- Choi, Y.H.; Ahn, J.H.; Kim, S.-B.; Jung, K.-H.; Gong, G.-Y.; Kim, M.-J.; Son, B.-H.; Ahn, S.-H.; Kim, W.K. Tissue microarray-based study of patients with lymph node-negative breast cancer shows that HER2/neu overexpression is an important predictive marker of poor prognosis. Ann. Oncol. 2009, 20, 1337–1343. [Google Scholar] [CrossRef]
- O’Sullivan, C.C.; Swain, S.M. Pertuzumab: Evolving therapeutic strategies in the management of HER2-overexpressing breast cancer. Expert Opin. Biol. Ther. 2013, 13, 779–790. [Google Scholar] [CrossRef]
- Wolff, A.C.; Hammond, M.E.H.; Schwartz, J.N.; Hagerty, K.L.; Allred, D.C.; Cote, R.J.; Dowsett, M.; Fitzgibbons, P.L.; Hanna, W.M.; Langer, A.; et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for human epidermal growth factor receptor 2 testing in breast cancer. J. Clin. Oncol. 2007, 25, 118–145. [Google Scholar] [CrossRef]
- Wolff, A.C.; Hammond, M.E.H.; Hicks, D.G.; Dowsett, M.; McShane, L.M.; Allison, K.H.; Allred, D.C.; Bartlett, J.M.S.; Bilous, M.; Fitzgibbons, P.; et al. Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline update. J. Clin. Oncol. 2013, 31, 3997–4013. [Google Scholar] [CrossRef]
- Zhao, J.; Xu, W.; Zhang, Z.; Song, R.; Zeng, S.; Sun, Y.; Xu, C. Prognostic role of HER2 expression in bladder cancer: A systematic review and meta-analysis. Int. Urol. Nephrol. 2015, 47, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Marchioni, M.; Cindolo, L.; Autorino, R.; Primiceri, G.; Arcaniolo, D.; Sio, M.D.; Schips, L. High Neutrophil-to-lymphocyte Ratio as Prognostic Factor in Patients Affected by Upper Tract Urothelial Cancer: A Systematic Review and Meta-analysis. Clin. Genitourin. Cancer 2017, 15, 343–349. [Google Scholar] [CrossRef]
- Kamoun, A.; Reyniès, A.D.; Allory, Y.; Sjödahl, G.; Robertson, A.G.; Seiler, R.; Hoadley, K.A.; Groeneveld, C.S.; Al-Ahmadie, H.; Choi, W.; et al. A Consensus Molecular Classification of Muscle-invasive Bladder Cancer. Eur. Urol. 2020, 77, 420–433. [Google Scholar] [CrossRef] [PubMed]
- Xylinas, E.; Rink, M.; Margulis, V.; Clozel, T.; Lee, R.K.; Comploj, E.; Novara, G.; Raman, J.D.; Lotan, Y.; Weizer, A.; et al. Impact of renal function on eligibility for chemotherapy and survival in patients who have undergone radical nephro-ureterectomy. BJU Int. 2013, 112, 453–461. [Google Scholar] [CrossRef] [PubMed]
- Oudard, S.; Culine, S.; Vano, Y.; Goldwasser, F.; Théodore, C.; Nguyen, T.; Voog, E.; Banu, E.; Vieillefond, A.; Priou, F.; et al. Multicentre randomised phase II trial of gemcitabine+platinum, with or without trastuzumab, in advanced or metastatic urothelial carcinoma overexpressing Her2. Eur. J. Cancer 2015, 51, 45–54. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Number of Patients | 157 | |
| Age and gender n (%) | Mean 70.14 yrs, range 34.99–94.19 yrs 99 (63.1) males, 58 females (36.9) | |
| Localization n (%) Total n = 160 | Renal pelvis Ureter Renal pelvis and ureter | 99 (62.7) 34 (21.5) 25 (15.8) |
| WHO grading n (%) Total n = 160 | G1 G2 G3 | 17 (10.6) 60 (37.5) 83 (51.9) |
| Tumor size (mm) | Mean ± SD Range | 44.23 ± 32.93 1–230 |
| pT n (%) Total n = 160 | a 1 2 3 4 is | 31 (19.4) 36 (22.5) 17 (10.6) 50 (31.3) 25 (15.6) 1 (0.6) |
| pN n (%) Total n = 114 | 0 1 2 | 82 (71.9) 6 (5.3) 26 (22.8) |
| cM n (%) Total n = 106 | 0 1 | 91 (85.8) 15 (14.2) |
| L n (%) Total n = 141 | 0 1 | 87 (61.7) 54 (38.3) |
| V n (%) Total n = 142 | 0 1 2 | 92 (64.8) 48 (33.8) 2 (1.4) |
| Pn n (%) Total n = 69 | 0 1 | 50 (72.5) 19 (27.5) |
| Residual status n (%) Total n = 152 | 0 1 2 | 119 (78.3) 23 (15.1) 10 (6.6) * |
| Growth pattern n (%) Total n = 160 | Papillary Papillary-solid/inverted Solid Mixed pattern Micropapillary Sarcomatoid Cis | 49 (30.6) 25 (15.6) 28 (17.5) 52 (32.5) 2 (1.3) 3 (1.9) 1 (0.6) |
| Necrosis n (%) Total n = 128 | Absent Present (>10%) | 65 (50.8) 63 (49.2) |
| Chronic lymphofollicular inflammation n (%) Total n = 128 | Absent Present | 115 (85.8) 19 (14.2) |
| ERBB2 Immunoscore | Immunoscoring (According to ASCO/CAP 2018 Guidelines for ERBB2/HER2 Testing in BC) | Immunoscoring (According to ASCO/CAP 2017 Guidelines for ERBB2/HER2 Testing in GC) | Number of Amplified ERBB2 Cases |
|---|---|---|---|
| n (%) | n (%) | n (%) | |
| 0 | 59 (36.9) | 59 (36.9) | 0 |
| 1+ | 72 (45.0) | 26 (16.3) | 1 (6.7) |
| 2+ | 5 (3.1) | 43 (26.9) | 6 (40.0) |
| 3+ | 10 (6.3) | 18 (11.3) | 7 (46.7) |
| n.a. | 14 (8.8) | 14 (8.8) | 1 (6.7) |
| Total n | 160 (100) | 160 (100) | 15 (100) |
| Patients and Tumor Properties | ERBB2-Immunoscoring According to Guidelines for Breast Cancer | ERBB2-Immunoscoring According to Guidelines for Gastric Adenocarcinoma | ERBB2 Amplification or Gain |
|---|---|---|---|
| p-Value | p-Value | p-Value | |
| Gender (male, female) | 0.994 | 0.537 | 0.557 |
| Age ≤ 60 yrs, >60 yrs | 0.041 | 0.820 | 1.000 |
| Survival | 0.939 | 0.906 | 0.939 |
| Progression | 0.195 | 0.028 | 0.549 |
| Morphology (papillary, papillary-solid/inverted, solid, mixed pattern, micropapillary, sarcomatoid, cis) | 0.945 | 0.805 | 0.057 |
| Necrosis | 0.204 | 0.146 | 0.048 |
| Lymphofollicular inflammation | 0.578 | 0.680 | 0.356 |
| WHO grading (G1, G2, G3) | 0.012 | 0.077 | <0.001 |
| Invasion, pTa or T1–4 | 0.257 | 0.359 | 0.003 |
| Stage | 0.701 | 0.226 | 0.014 |
| pN | 0.180 | 0.145 | 0.005 |
| cM | 0.547 | 0.878 | 0.064 |
| L | 0.496 | 0.676 | 0.005 |
| V | 0.893 | 0.389 | 0.065 |
| Pn | 0.773 | 0.862 | 0.005 |
| Residual status | 0.682 | 0.883 | 0.006 |
| ERBB2 amplification or gain | <0.001 | <0.001 | - |
| Overall Survival | Univariable Analyses | Multivariable Analysis | ||||
|---|---|---|---|---|---|---|
| Parameter | p-Value | 95% CI | HR | p-Value | 95% CI | Adj HR |
| Age > 60 yrs vs. * ≤ 60 yrs | 0.081 | 0.940–2.925 | 1.658 | - | - | - |
| Sex m vs. * f | 0.615 | 0.736–1.678 | 1.112 | - | - | - |
| Progression vs. * no progression | 0.008 | 1.178–3.001 | 1.880 | 0.451 | 0.324–12.674 | 2.025 |
| Pelvic localization vs. ureter vs. * both | 0.711 | 0.818–1.344 | 1.048 | - | - | - |
| Growth patterns: * Papillary vs. papillary-inverted/solid * Papillary vs. solid * Papillary vs. mixed type * Papillary vs. micropapillary * Papillary vs. sarcomatoid | 0.007 0.961 0.010 0.160 0.077 <0.001 | 0.504–1.919 1.214–4.066 0.864–2.432 0.868–15.725 2.899–35.123 | 0.983 2.222 1.449 3.694 10.09 | 0.002 0.049 0.763 0.209 0.579 <0.001 | 0.032–0.990 0.175–10.757 0.556–14.580 0.078–109.66 7.614–1364.9 | 0.178 1.373 2.846 2.826 101.942 |
| Necrosis vs. * no necrosis | 0.004 | 1.230–3.046 | 1.936 | 0.149 | 0.752–6.505 | 2.212 |
| Chronic lymphofollicular inflammation vs. * no inflammation | 0.983 | 0.558–1.771 | 0.994 | - | - | - |
| ERBB2 score ** 0 vs. 1+ vs. 2+ vs. * 3+ | 0.193 | 0.937–1.380 | 1.137 | - | - | - |
| ERBB2 amplification vs. * ERBB2 <2.0 | 0.176 | 0.827–2.822 | 1.528 | - | - | |
| ERBB2 gain or amplification vs. * no ERBB2 gain or amplification | 0.057 | 0.986–2.485 | 1.565 | 0.114 | 0.623–83.766 | 7.222 |
| Platin vs. * no platin-based therapy | 0.005 | 1.243–3.316 | 2.031 | 0.043 | 0.003–0.914 | 0.049 |
| ERBB2 status and CT | 0.006 | 0.020 | ||||
| ERBB2 negative and CT vs. * ERBB2 negative and no CT | 0.009 | 1.227–4.223 | 2.276 | 0.003 | 0.009–0.377 | 0.059 |
| ERBB2 positive and CT vs. * ERBB2 negative and no CT | 0.620 | 0.504–3.160 | 1.262 | 0.021 | 0.003–0.624 | 0.046 |
| ERBB2 positive and no CT vs. * ERBB2 negative and no CT | 0.003 | 1.341–4.028 | 2.324 | 0.086 | 0.003–1.458 | 0.071 |
| Grading | <0.001 | 0.071 | ||||
| G2 vs. * G1 | 0.125 | 0.828–4.709 | 1.974 | 0.738 | 0.169–3.522 | 0.772 |
| G3 vs. * G1 | 0.001 | 1.692–9.185 | 3.942 | 0.027 | 0.001–0.663 | 0.026 |
| pT | <0.001 | 0.004 | ||||
| pT1 vs. * pTa | 0.060 | 0.970–4.310 | 2.045 | 0.003 | 2.409–68.305 | 12.827 |
| pT2 vs. * pTa | 0.040 | 1.044–5.859 | 2.474 | 0.019 | 1.711–415-792 | 26.674 |
| T3 vs. * pTa | <0.001 | 1.673–6.410 | 3.274 | 0.012 | 2.346–1021.94 | 48.959 |
| pT4 vs. * pTa | <0.001 | 5.006–23.279 | 10.795 | <0.001 | 11.761–8238.9 | 311.28 |
| pN1 or pN2 vs. * pN0 | <0.001 | 1.921–5.125 | 3.138 | 0.678 | 1.189–4.677 | 2.358 |
| cM10 vs. * cM0 | <0.001 | 2.910–10.993 | 5.656 | 0.384 | 0.346–15.830 | 2.340 |
| Lymphatic invasion (L1 vs. * L0) | <0.001 | 1.525–3.602 | 2.344 | <0.001 | 4.130–71.603 | 17.196 |
| Venous invasion (V1 or V2 vs. * V0) | <0.001 | 1.483–3.465 | 2.267 | 0.090 | 0.095–1.187 | 0.335 |
| Perineural invasion (Pn1 vs. * Pn0) | <0.001 | 1.105–12.198 | 3.6718 | 0.442 | 0.229–1.903 | 0.660 |
| Residual status (R1 or R2 vs. * R0) | <0.001 | 2.917–7.280 | 4.608 | <0.001 | 4.116–76.914 | 17.793 |
| Progression-Free Survival | Univariable Analyses | Multivariable Analysis | ||||
|---|---|---|---|---|---|---|
| Parameter | p-Value | 95% CI | HR | p-Value | 95% CI | Adj HR |
| Age > 60 yrs vs. ≤ * 60 yrs | 0.909 | 0.430–2.579 | 1.054 | - | - | - |
| sex m vs. * f | 0.609 | 0.384–1.754 | 0.820 | - | - | - |
| Pelvic localization vs. ureter vs. * both | 0.181 | 0.872–2.067 | 1.342 | - | - | - |
| Growth patterns: * Papillary vs. papillary-inverted/solid * Papillary vs. solid * Papillary vs. mixed type * Papillary vs. micropapillary * Papillary vs. sarcomatoid | 0.019 0.333 0.944 0.070 0.983 0.004 | 0.099–2.193 0.277–3.963 0.938–5.135 0.000 2.799–246.9 | 0.465 1.048 2.195 0.000 26.29 | 0.869 | 0.583–1.577 | 0.959 |
| Necrosis vs. * no necrosis | 0.127 | 0.852–3.620 | 1.756 | - | - | - |
| Chronic lymphofollicular inflammation vs. * no inflammation | 0.663 | 0.275–2.274 | 0.791 | - | - | - |
| ERBB2 score ** 1+ vs. 2+ vs. * 3+ vs. * 0 | 0.003 | 1.2132.517 | 1.748 | 0.176 | 0.839–2.613 | 1.480 |
| ERBB2 amplification vs. * no amplification | 0.040 | 1.042–6.445 | 2.592 | 0.032 | 1.112–11.089 | 3.511 |
| Platin vs. * no platin-based therapy | <0.001 | 3.865–16.851 | 8.192 | <0.001 | 4.596–45.811 | 14.510 |
| ERBB2 status and CT | <0.001 | 0.296 | 0.419–1.303 | 0.739 | ||
| ERBB2 negative and CT vs. * ERBB2 negative and no CT | 0.859 | 0.271–2.968 | 0.898 | |||
| ERBB2 positive and CT vs. * ERBB2 negative and no CT | 0.014 | 0.052–0.717 | 0.194 | |||
| ERBB2 positive and no CT vs. * ERBB2 negative and no CT | <0.001 | 0.056–0.338 | 0.137 | |||
| Grading | 0.154 | - | - | - | ||
| G2 vs. * G1 | 0.450 | 0.396–8.083 | 1.789 | |||
| G3 vs. * G1 | 0.125 | 0.727–13.78 | 3.166 | |||
| pT | 0.037 | 0.791 | 0.546–1.587 | 0.930 | ||
| pT1 vs. * pTa | 0.665 | 0.359–4.988 | 1.337 | |||
| pT2 vs. * pTa | 0.491 | 0.378–7.611 | 1.696 | |||
| pT3 vs. * pTa | 0.059 | 0.958–9.096 | 2.951 | |||
| pT4 vs. * pTa | 0.006 | 1.690–24.657 | 6.456 | |||
| pN1 or pN2 vs. * pN0 | 0.015 | 1.234–7.247 | 2.991 | 0.070 | 0.082–1.101 | 0.300 |
| cM10 vs. * cM0 | 0.001 | 2.274–28.137 | 8.000 | 0.147 | 0.629–22.304 | 3.745 |
| Lymphatic invasion (L1 vs. * L0) | 0.121 | 0.852–3.975 | 1.840 | - | - | |
| Venous invasion (V1 or V2 vs. * V0) | 0.172 | 0.790–3.738 | 1.718 | - | - | - |
| Perineural invasion (Pn1 vs. * Pn0) | 0.288 | 0.538–8.083 | 2.085 | - | - | - |
| Residual status (R1 or R2 vs. * R0) | 0.018 | 1.201–6.833 | 2.865 | 0.581 | 0.139–3.023 | 0.648 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zimpfer, A.; Kdimati, S.; Mosig, M.; Rudolf, H.; Zettl, H.; Erbersdobler, A.; Hakenberg, O.W.; Maruschke, M.; Schneider, B. ERBB2 Amplification as a Predictive and Prognostic Biomarker in Upper Tract Urothelial Carcinoma. Cancers 2023, 15, 2414. https://doi.org/10.3390/cancers15092414
Zimpfer A, Kdimati S, Mosig M, Rudolf H, Zettl H, Erbersdobler A, Hakenberg OW, Maruschke M, Schneider B. ERBB2 Amplification as a Predictive and Prognostic Biomarker in Upper Tract Urothelial Carcinoma. Cancers. 2023; 15(9):2414. https://doi.org/10.3390/cancers15092414
Chicago/Turabian StyleZimpfer, Annette, Said Kdimati, Melanie Mosig, Henrik Rudolf, Heike Zettl, Andreas Erbersdobler, Oliver W. Hakenberg, Matthias Maruschke, and Björn Schneider. 2023. "ERBB2 Amplification as a Predictive and Prognostic Biomarker in Upper Tract Urothelial Carcinoma" Cancers 15, no. 9: 2414. https://doi.org/10.3390/cancers15092414
APA StyleZimpfer, A., Kdimati, S., Mosig, M., Rudolf, H., Zettl, H., Erbersdobler, A., Hakenberg, O. W., Maruschke, M., & Schneider, B. (2023). ERBB2 Amplification as a Predictive and Prognostic Biomarker in Upper Tract Urothelial Carcinoma. Cancers, 15(9), 2414. https://doi.org/10.3390/cancers15092414