
Changing Prevalence of AIDS and Non-AIDS-Defining Cancers in an Incident Cohort of People Living with HIV over 28 Years

 , , , ,
, , , ,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Antiretroviral Therapy Cohort Collaboration. Survival of HIV-positive patients starting antiretroviral therapy between 1996 and 2013: A collaborative analysis of cohort studies. Lancet HIV 2017, 4, e349–e356. [Google Scholar] [CrossRef] [PubMed]
- Mazzitelli, M.; Sasset, L.; Gardin, S.; Leoni, D.; Trunfio, M.; Scaglione, V.; Mengato, D.; Agostini, E.; Vania, E.; Putaggio, C.; et al. Real-Life Experience on Dolutegravir and Lamivudine as Initial or Switch Therapy in a Silver Population Living with HIV. Viruses 2023, 15, 1740. [Google Scholar] [CrossRef] [PubMed]
- Fabbiani, M.; Rossetti, B.; Ciccullo, A.; Oreni, L.; Lagi, F.; Celani, L.; Colafigli, M.; De Vito, A.; Mazzitelli, M.; Dusina, A.; et al. Efficacy and durability of two- vs. three-drug integrase inhibitor-based regimens in virologically suppressed HIV-infected patients: Data from real-life ODOACRE cohort. HIV Med. 2021, 22, 843–853. [Google Scholar] [CrossRef] [PubMed]
- Mazzitelli, M.; Milinkovic, A.; Pereira, B.; Palmer, J.; Tong, T.; Asboe, D.; Boffito, M. Polypharmacy and evaluation of anticholinergic risk in a cohort of elderly people living with HIV. AIDS 2019, 33, 2439–2441. [Google Scholar] [CrossRef]
- Pereira, B.; Mazzitelli, M.; Milinkovic, A.; Casley, C.; Rubio, J.; Channa, R.; Girometti, N.; Asboe, D.; Pozniak, A.; Boffito, M. Evaluation of a Clinic Dedicated to People Aging with HIV at Chelsea and Westminster Hospital: Results of a 10-Year Experience. AIDS Res. Hum. Retroviruses 2022, 38, 188–197. [Google Scholar] [CrossRef]
- Ciccullo, A.; Baldin, G.; Borghi, V.; Sterrantino, G.; Madeddu, G.; Latini, A.; d’Ettorre, G.; Lanari, A.; Mazzitelli, M.; Colafigli, M.; et al. Overall Tolerability of Integrase Inhibitors in Clinical Practice: Results from a Multicenter Italian Cohort. AIDS Res. Hum. Retroviruses 2021, 37, 4–10. [Google Scholar] [CrossRef]
- Fontela, C.; Aguinaga, A.; Moreno-Iribas, C.; Reparaz, J.; Rivero, M.; Gracia, M.; Floristan, Y.; Fresan, U.; Miguel, R.S.; Ezpeleta, C.; et al. Trends and causes of mortality in a population-based cohort of HIV-infected adults in Spain: Comparison with the general population. Sci. Rep. 2020, 10, 8922. [Google Scholar] [CrossRef]
- Hadavandsiri, F.; Shafaati, M.; Mohammad Nejad, S.; Ebrahimzadeh Mousavi, M.; Najafi, A.; Mirzaei, M.; Narouee, S.; Akbarpour, S. Non-communicable disease comorbidities in HIV patients: Diabetes, hypertension, heart disease, and obstructive sleep apnea as a neglected issue. Sci. Rep. 2023, 13, 12730. [Google Scholar] [CrossRef]
- Shiels, M.S.; Althoff, K.N.; Pfeiffer, R.M.; Achenbach, C.J.; Abraham, A.G.; Castilho, J.; Cescon, A.; D’Souza, G.; Dubrow, R.; Eron, J.J.; et al. HIV Infection, Immunosuppression, and Age at Diagnosis of Non-AIDS-Defining Cancers. Clin. Infect. Dis. 2017, 64, 468–475. [Google Scholar] [CrossRef]
- Zicari, S.; Sessa, L.; Cotugno, N.; Ruggiero, A.; Morrocchi, E.; Concato, C.; Rocca, S.; Zangari, P.; Manno, E.C.; Palma, P. Immune Activation, Inflammation, and Non-AIDS Co-Morbidities in HIV-Infected Patients under Long-Term ART. Viruses 2019, 11, 200. [Google Scholar] [CrossRef]
- Hewavisenti, R.V.; Arena, J.; Ahlenstiel, C.L.; Sasson, S.C. Human papillomavirus in the setting of immunodeficiency: Pathogenesis and the emergence of next-generation therapies to reduce the high associated cancer risk. Front. Immunol. 2023, 14, 1112513. [Google Scholar] [CrossRef] [PubMed]
- Yuan, T.; Hu, Y.; Zhou, X.; Yang, L.; Wang, H.; Li, L.; Wang, J.; Qian, H.Z.; Clifford, G.M.; Zou, H. Incidence and mortality of non-AIDS-defining cancers among people living with HIV: A systematic review and meta-analysis. EClinicalMedicine 2022, 52, 101613. [Google Scholar] [CrossRef] [PubMed]
- 1993 revised classification system for HIV infection and expanded surveillance case definition for AIDS among adolescents and adults. MMWR Recomm. Rep. 1992, 41, 1–19.
- Cobucci, R.N.; Lima, P.H.; de Souza, P.C.; Costa, V.V.; Cornetta Mda, C.; Fernandes, J.V.; Goncalves, A.K. Assessing the impact of HAART on the incidence of defining and non-defining AIDS cancers among patients with HIV/AIDS: A systematic review. J. Infect. Public Health 2015, 8, 1–10. [Google Scholar] [CrossRef]
- Deeks, S.G.; Lewin, S.R.; Havlir, D.V. The end of AIDS: HIV infection as a chronic disease. Lancet 2013, 382, 1525–1533. [Google Scholar] [CrossRef]
- Shiels, M.S.; Islam, J.Y.; Rosenberg, P.S.; Hall, H.I.; Jacobson, E.; Engels, E.A. Projected Cancer Incidence Rates and Burden of Incident Cancer Cases in HIV-Infected Adults in the United States Through 2030. Ann. Intern. Med. 2018, 168, 866–873. [Google Scholar] [CrossRef]
- Trickey, A.; Sabin, C.A.; Burkholder, G.; Crane, H.; d’Arminio Monforte, A.; Egger, M.; Gill, M.J.; Grabar, S.; Guest, J.L.; Jarrin, I.; et al. Life expectancy after 2015 of adults with HIV on long-term antiretroviral therapy in Europe and North America: A collaborative analysis of cohort studies. Lancet HIV 2023, 10, e295–e307. [Google Scholar] [CrossRef]
- Shiels, M.S.; Pfeiffer, R.M.; Engels, E.A. Age at cancer diagnosis among persons with AIDS in the United States. Ann. Intern. Med. 2010, 153, 452–460. [Google Scholar] [CrossRef]
- Franzetti, M.; Adorni, F.; Parravicini, C.; Vergani, B.; Antinori, S.; Milazzo, L.; Galli, M.; Ridolfo, A.L. Trends and predictors of non-AIDS-defining cancers in men and women with HIV infection: A single-institution retrospective study before and after the introduction of HAART. J. Acquir. Immune Defic. Syndr. 2013, 62, 414–420. [Google Scholar] [CrossRef]
- De Socio, G.V.; Pasqualini, M.; Ricci, E.; Maggi, P.; Orofino, G.; Squillace, N.; Menzaghi, B.; Madeddu, G.; Taramasso, L.; Francisci, D.; et al. Smoking habits in HIV-infected people compared with the general population in Italy: A cross-sectional study. BMC Public Health 2020, 20, 734. [Google Scholar] [CrossRef]
- Scaggiante, R.; Andreis, S.; Basso, M.; Franchin, E.; Franzetti, M.; Del Vecchio, C.; Torti, C.; Mengoli, C.; Cruciani, M.; Sarmati, L.; et al. Epstein-Barr and cytomegalovirus DNA salivary shedding correlate with long-term plasma HIV RNA detection in HIV-infected men who have sex with men. J. Med. Virol. 2016, 88, 1211–1221. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; De Luca, A.; Smith, C.; Zangerle, R.; Sambatakou, H.; Bonnet, F.; Smit, C.; Schommers, P.; Thornton, A.; Berenguer, J.; et al. Chronic Hepatitis B and C Virus Infection and Risk for Non-Hodgkin Lymphoma in HIV-Infected Patients: A Cohort Study. Ann. Intern. Med. 2017, 166, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Strategies for Management of Antiretroviral Therapy Study Group (SMART); El-Sadr, W.M.; Lundgren, J.; Neaton, J.D.; Gordin, F.; Abrams, D.; Arduino, R.C.; Babiker, A.; Burman, W.; Clumeck, N.; et al. CD4+ count-guided interruption of antiretroviral treatment. N. Engl. J. Med. 2006, 355, 2283–2296. [Google Scholar] [CrossRef] [PubMed]
- TEMPRANO ANRS 12136 Study Group; Danel, C.; Moh, R.; Gabillard, D.; Badje, A.; Le Carrou, J.; Ouassa, T.; Ouattara, E.; Anzian, A.; Ntakpe, J.B.; et al. A Trial of Early Antiretrovirals and Isoniazid Preventive Therapy in Africa. N. Engl. J. Med. 2015, 373, 808–822. [Google Scholar] [CrossRef]
- Park, L.S.; Tate, J.P.; Sigel, K.; Brown, S.T.; Crothers, K.; Gibert, C.; Goetz, M.B.; Rimland, D.; Rodriguez-Barradas, M.C.; Bedimo, R.J.; et al. Association of Viral Suppression With Lower AIDS-Defining and Non-AIDS-Defining Cancer Incidence in HIV-Infected Veterans: A Prospective Cohort Study. Ann. Intern. Med. 2018, 169, 87–96. [Google Scholar] [CrossRef]
- Chiao, E.Y.; Coghill, A.; Kizub, D.; Fink, V.; Ndlovu, N.; Mazul, A.; Sigel, K. The effect of non-AIDS-defining cancers on people living with HIV. Lancet Oncol. 2021, 22, e240–e253. [Google Scholar] [CrossRef]
- Guiguet, M.; Boue, F.; Cadranel, J.; Lang, J.M.; Rosenthal, E.; Costagliola, D.; Clinical Epidemiology Group of the FHDH-ANRS CO4 Cohort. Effect of immunodeficiency, HIV viral load, and antiretroviral therapy on the risk of individual malignancies (FHDH-ANRS CO4): A prospective cohort study. Lancet Oncol. 2009, 10, 1152–1159. [Google Scholar] [CrossRef]
- Bannister, W.P.; Mast, T.C.; de Wit, S.; Gerstoft, J.; Wiese, L.; Milinkovic, A.; Hadziosmanovic, V.; Clarke, A.; Rasmussen, L.D.; Lacombe, K.; et al. Changes in body mass index and clinical outcomes after initiation of contemporary antiretroviral regimens. AIDS 2022, 36, 2107–2119. [Google Scholar] [CrossRef]
- Polesel, J.; Franceschi, S.; Suligoi, B.; Crocetti, E.; Falcini, F.; Guzzinati, S.; Vercelli, M.; Zanetti, R.; Tagliabue, G.; Russo, A.; et al. Cancer incidence in people with AIDS in Italy. Int. J. Cancer 2010, 127, 1437–1445. [Google Scholar] [CrossRef]
- Franceschi, S.; Lise, M.; Clifford, G.M.; Rickenbach, M.; Levi, F.; Maspoli, M.; Bouchardy, C.; Dehler, S.; Jundt, G.; Ess, S.; et al. Changing patterns of cancer incidence in the early- and late-HAART periods: The Swiss HIV Cohort Study. Br. J. Cancer 2010, 103, 416–422. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Overall N = 289 | ADC N = 120 | NADC N = 166 | p-Value | |
|---|---|---|---|---|---|
| Age (at cancer diagnosis), years, median (IQR) | 49 (41–58) | 43.5 (36.8–50) | 53 (46–61) | <0.0001 k | |
| Sex, male, N (%) | 225 (77.9) | 107 (89.2) | 116 (69.9) | 0.0001 c | |
| Italian nationality, n (%) | 263 (91) | 107 (89.2) | 154 (92.8) | 0.2869 c | |
| Risk factor, n (%) | Blood product | 2 (0.7) | 0 (0) | 2 (1.2) | <0.0001 f |
| Unprotected heterosexual sex | 75 (26) | 22 (18.3) | 52 (31.3) | ||
| Unprotected sex between men | 147 (50.9) | 82 (68.3) | 63 (38) | ||
| Intravenous drug use | 64 (22.1) | 16 (13.3) | 48 (28.9) | ||
| Vertical transmission | 1 (0.3) | 0 (0) | 1 (0.6) | ||
| HIV diagnosis coincides with tumor diagnosis, n (%) | 72 (24.9) | 71 (59.2) | 1 (0.6) | <0.0001 f | |
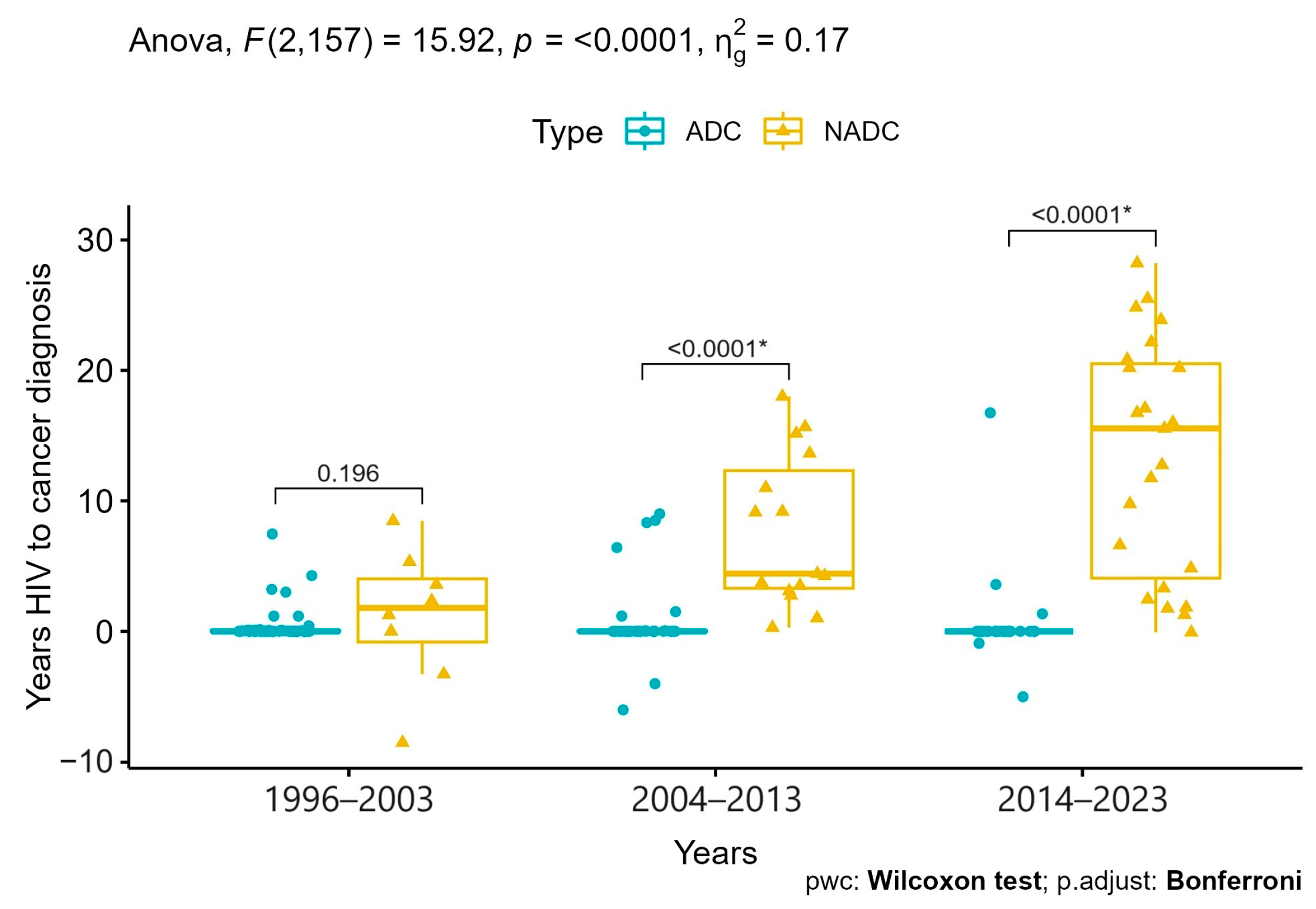
| Years from HIV to cancer diagnosis, median (IQR) | 0 (0–3.2) | 0 (0–0) | 7.5 (2.5–15.9) | <0.0001 k | |
| CD4 + T cell count at HIV diagnosis, cell/mm3, median (IQR) | 147 (70–290) | 100 (40–206) | 190 (90–318) | <0.0001 k | |
| CD4 + T cell count at cancer diagnosis, cell/mm3, median (IQR) | 266 (120–540) | 130 (45–246) | 469 (242–720) | <0.0001 k | |
| CD4 + T cell count at cancer diagnosis <200 CD4/mcL, n (%) | 111 (40.7) | 77 (67) | 33 (21.3) | <0.0001 c | |
| CD4 + T cell count at cancer diagnosis >500 CD4/mcL, n (%) | 80 (29.3) | 10 (8.7) | 67 (43.2) | <0.0001 c | |
| Undetectable viremia (<50 cp/mL), at cancer diagnosis n (%) | 141 (48.8) | 19 (15.8) | 120 (72.3) | <0.0001 c | |
| IHAART exposure at cancer diagnosis, n (%) | 188 (65.1) | 42 (35) | 143 (86.1) | <0.0001 c | |
| Decade of cancer diagnosis, n (%) | 1996–2003 | 75 (26) | 58 (48.3) | 17 (10.2) | <0.0001 c |
| 2004–2013 | 90 (31.1) | 35 (29.2) | 55 (33.1) | ||
| 2014–2023 | 124 (42.9) | 27 (22.5) | 94 (56.6) | ||
| Tumor, n (%) | Kaposi | 63 (21.8) | 63 (52.5) | 0 (0) | <0.0001 f |
| NHL | 58 (20.1) | 57 (47.5) | 1 (0.6) | ||
| HCC | 21 (7.3) | 0 (0) | 21 (12.7) | ||
| Anal cancer | 19 (6.6) | 0 (0) | 18 (10.8) | ||
| Non-melanoma skin cancer | 16 (5.5) | 0 (0) | 16 (9.6) | ||
| Neoplasms of the oral cavity, pharynx, and salivary glands | 14 (4.8) | 0 (0) | 14 (8.4) | ||
| Breast cancer | 14 (4.8) | 0 (0) | 14 (8.4) | ||
| Prostate cancer | 12 (4.2) | 0 (0) | 12 (7.2) | ||
| Cervical cancer | 12 (4.2) | 0 (0) | 11 (6.6) | ||
| Colorectal cancer | 11 (3.8) | 0 (0) | 11 (6.6) | ||
| Lung cancer | 9 (3.1) | 0 (0) | 8 (4.8) | ||
| Malignant lymphoproliferative diseases | 8 (2.8) | 0 (0) | 8 (4.8) | ||
| Bladder cancer | 7 (2.4) | 0 (0) | 7 (4.2) | ||
| Melanoma | 6 (2.1) | 0 (0) | 6 (3.6) | ||
| Other | 19 (6.6) | 0 (0) | 19 (11.4) | ||
| Characteristics | Overall N = 289 | ADC N = 120 | NADC N = 166 | p-Value | |
|---|---|---|---|---|---|
| Anticancer treatment, N (%) | 273 (94.8) | 114 (95.8) | 156 (94) | 0.4968 c | |
| Chemotherapy, n (%) | 135 (47.9) | 69 (58) | 65 (40.6) | 0.0041 c | |
| Radiotherapy, n (%) | 50 (17.7) | 18 (15.1) | 32 (20) | 0.2938 c | |
| Surgical treatment, n (%) | 115 (40.5) | 5 (4.2) | 108 (66.7) | <0.0001 c | |
| Tumor outcome, n (%) | 0.1430 c | ||||
| Progression | 71 (24.9) | 23 (19.3) | 48 (29.4) | ||
| Complete remission | 171 (60) | 78 (65.5) | 91 (55.8) | ||
| Partial remission | 43 (15.1) | 18 (15.1) | 24 (14.7) | ||
| Deaths | 85 (29.4) | 39 (32.5) | 46 (27.7) | ||
| 2-year mortality, n (%) | 55 (19.1) | 30 (25) | 25 (15.2) | 0.0375 c | |
| 10-year mortality, n (%) | 78 (27.1) | 35 (29.2) | 43 (26.1) | 0.5615 c | |
| Follow-up, person-years | 1731.7 | 899.9 | 825.4 | - | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cattelan, A.M.; Mazzitelli, M.; Presa, N.; Cozzolino, C.; Sasset, L.; Leoni, D.; Bragato, B.; Scaglione, V.; Baldo, V.; Parisi, S.G. Changing Prevalence of AIDS and Non-AIDS-Defining Cancers in an Incident Cohort of People Living with HIV over 28 Years. Cancers 2024, 16, 70. https://doi.org/10.3390/cancers16010070
Cattelan AM, Mazzitelli M, Presa N, Cozzolino C, Sasset L, Leoni D, Bragato B, Scaglione V, Baldo V, Parisi SG. Changing Prevalence of AIDS and Non-AIDS-Defining Cancers in an Incident Cohort of People Living with HIV over 28 Years. Cancers. 2024; 16(1):70. https://doi.org/10.3390/cancers16010070
Chicago/Turabian StyleCattelan, Anna Maria, Maria Mazzitelli, Nicolò Presa, Claudia Cozzolino, Lolita Sasset, Davide Leoni, Beatrice Bragato, Vincenzo Scaglione, Vincenzo Baldo, and Saverio Giuseppe Parisi. 2024. "Changing Prevalence of AIDS and Non-AIDS-Defining Cancers in an Incident Cohort of People Living with HIV over 28 Years" Cancers 16, no. 1: 70. https://doi.org/10.3390/cancers16010070
APA StyleCattelan, A. M., Mazzitelli, M., Presa, N., Cozzolino, C., Sasset, L., Leoni, D., Bragato, B., Scaglione, V., Baldo, V., & Parisi, S. G. (2024). Changing Prevalence of AIDS and Non-AIDS-Defining Cancers in an Incident Cohort of People Living with HIV over 28 Years. Cancers, 16(1), 70. https://doi.org/10.3390/cancers16010070