
Validation of Inflammatory Prognostic Biomarkers in Pleural Mesothelioma

 , , ,
, , , 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Variables
2.3. Statistical Analyses
3. Results
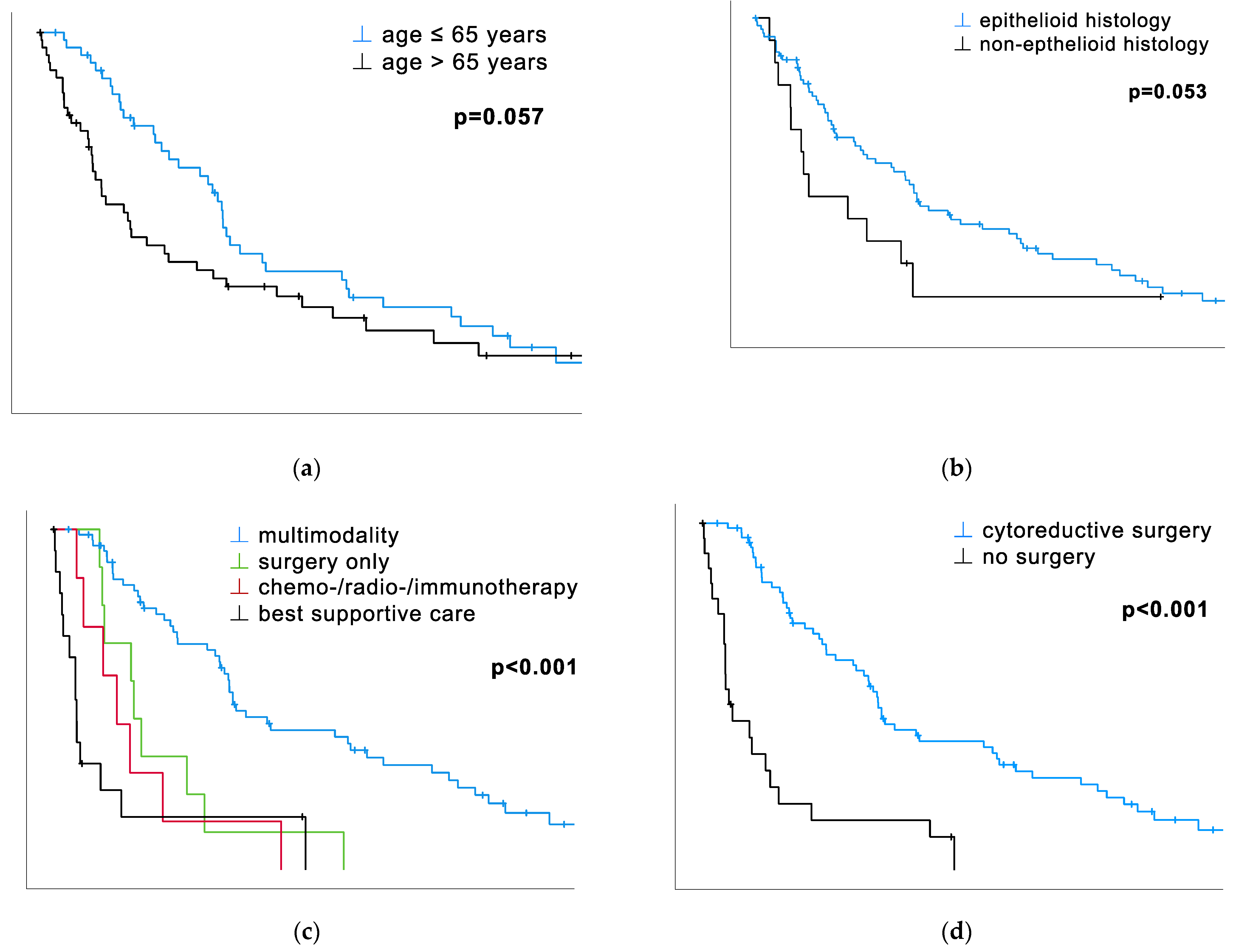
3.1. Therapy Modalities, Including Surgery, Have an Undeniable Impact on OS
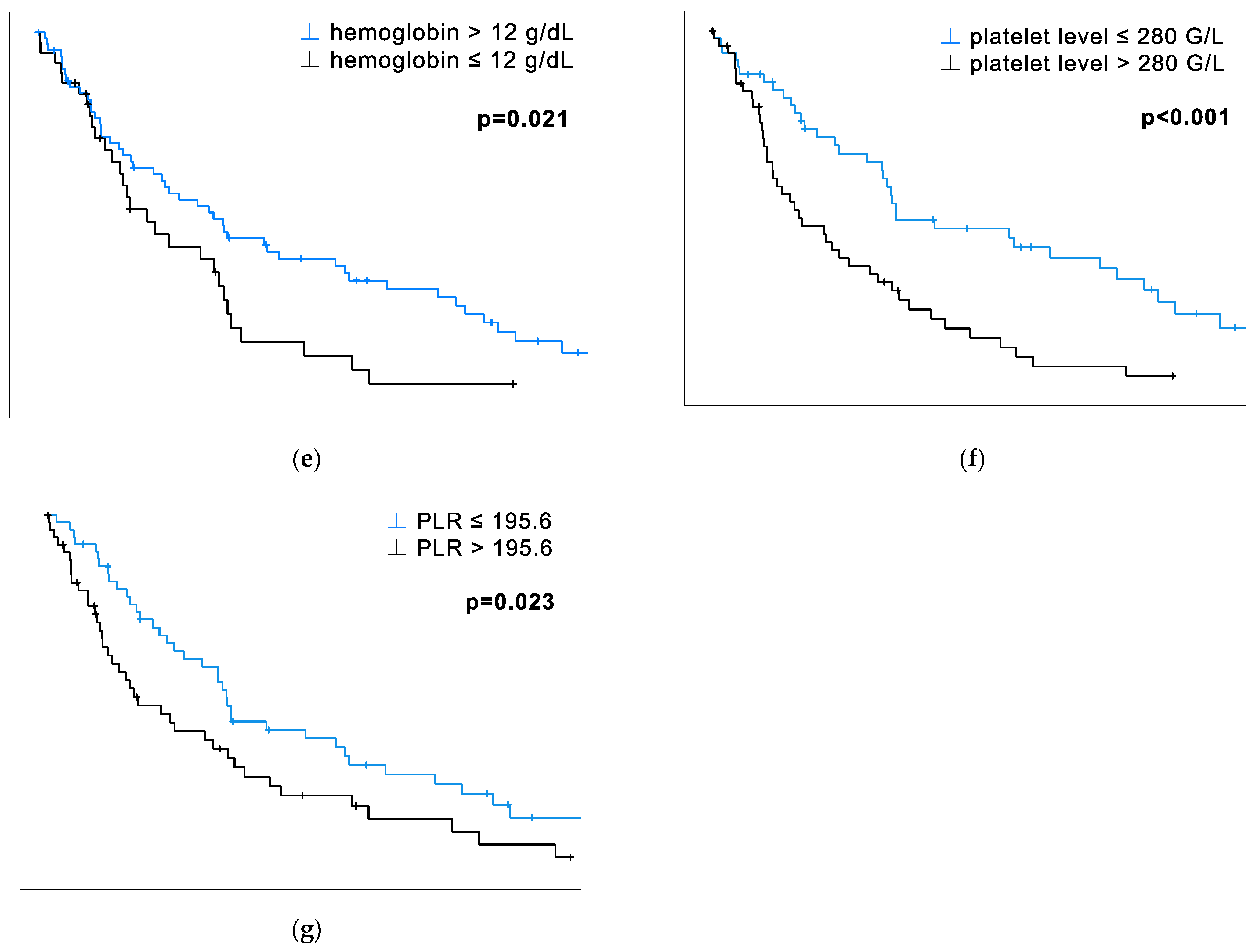
3.2. The Prognostic Impact of Platelet Count and PLR
3.3. Histology, Monocytes, and CRP Show a Trend of Statistical Significance
3.4. Multivariate Survival Analysis
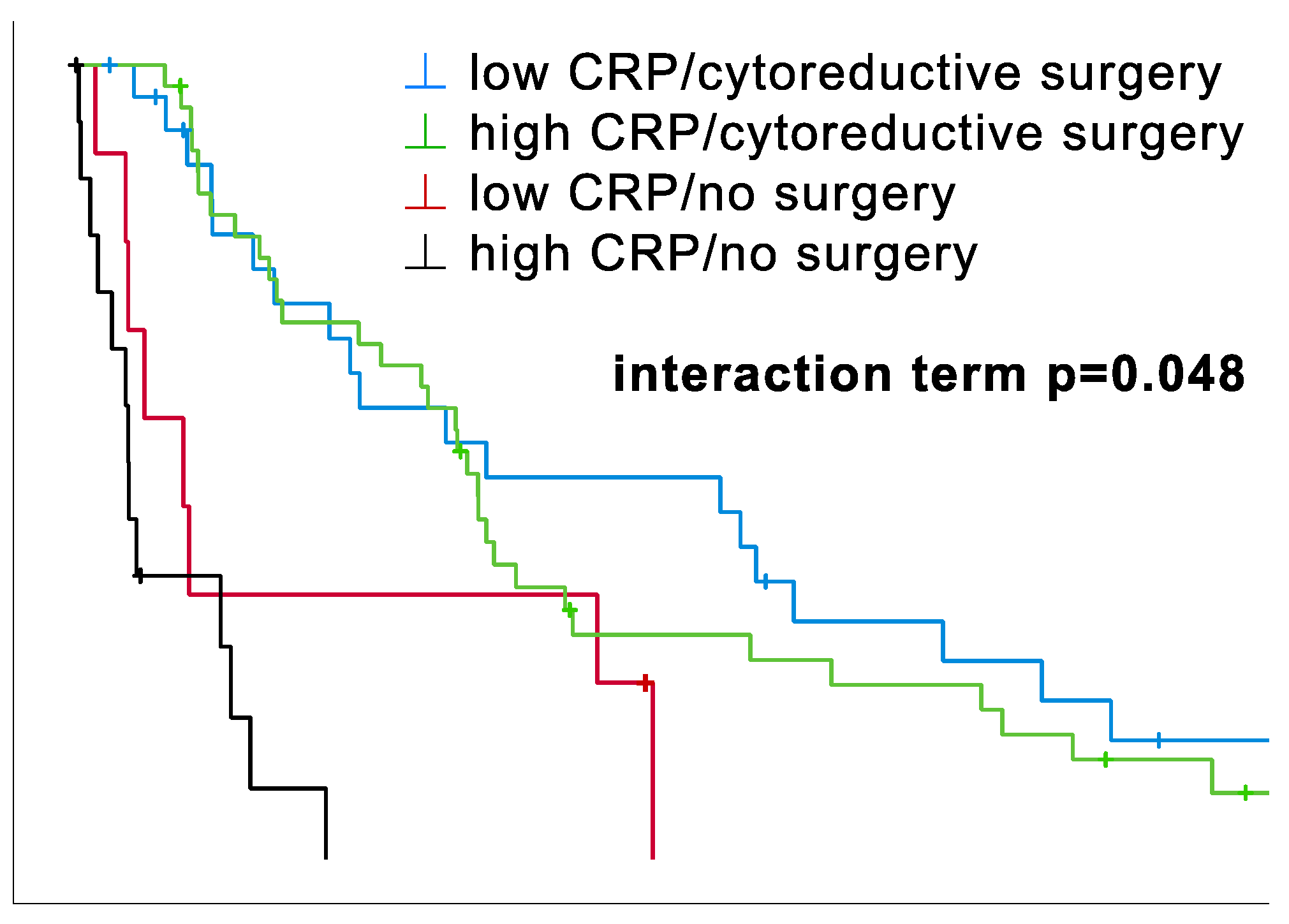
3.5. Surgery vs. No Surgery Stratified by CRP Level
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brims, F.J.H.; Maskell, N.A. Prognostic factors for malignant pleural mesothelioma. Curr. Respir. Care Rep. 2013, 2, 100–108. [Google Scholar] [CrossRef][Green Version]
- Tsao, A.S.; Wistuba, I.; Roth, J.A.; Kindler, H.L. Malignant pleural mesothelioma. J. Clin. Oncol. 2009, 27, 2081–2090. [Google Scholar] [CrossRef] [PubMed]
- Thieke, C.; Nicolay, N.H.; Sterzing, F.; Hoffmann, H.; Roeder, F.; Safi, S.; Debus, J.; Huber, P.E. Long-term results in malignant pleural mesothelioma treated with neoadjuvant chemotherapy, extrapleural pneumonectomy, and intensity-modulated radiotherapy. Radiat. Oncol. 2015, 10, 267. [Google Scholar] [CrossRef] [PubMed]
- Leal, J.L.; Hoang, W.; Xue, J.; Dunne, B.; John, T.; Harden, S. What’s Current and What’s New in Mesothelioma? Clin. Oncol. 2022, 34, 771–780. [Google Scholar] [CrossRef] [PubMed]
- Hajj, G.N.M.; Cavarson, C.H.; Pinto, C.A.L.; Venturi, G.; Navarro, J.R.; Lima, V.C.C.d. Malignant pleural mesothelioma: An update. J. Bras. Pneumol. 2021, 47, e20210129. [Google Scholar] [CrossRef]
- Kindler, H.L.; Ismaila, N.; Armato, S.G., 3rd; Bueno, R.; Hesdorffer, M.; Jahan, T.; Jones, C.M.; Miettinen, M.; Pass, H.; Rimner, A.; et al. Treatment of Malignant Pleural Mesothelioma: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2018, 36, 1343–1373. [Google Scholar] [CrossRef]
- Vogl, M.; Rosenmayr, A.; Bohanes, T.; Scheed, A.; Brndiar, M.; Stubenberger, E.; Ghanim, B. Biomarkers for Malignant Pleural Mesothelioma-A Novel View on Inflammation. Cancers 2021, 13, 658. [Google Scholar] [CrossRef]
- Baud, M.; Strano, S.; Dechartres, A.; Jouni, R.; Triponez, F.; Chouaid, C.; Forgez, P.; Damotte, D.; Roche, N.; Régnard, J.-F.; et al. Outcome and prognostic factors of pleural mesothelioma after surgical diagnosis and/or pleurodesis. J. Thorac. Cardiovasc. Surg. 2013, 145, 1305–1311. [Google Scholar] [CrossRef][Green Version]
- Takehiro, O.; Yuki, K.; Sawako, K.; Reika, I.K.I.; Masataka, H. Prognostic Impact of Inflammation-related Biomarkers on Overall Survival of Patients with Inoperable Malignant Pleural Mesothelioma. In Vivo 2018, 32, 445. [Google Scholar] [CrossRef]
- Janik, S.; Raunegger, T.; Hacker, P.; Ghanim, B.; Einwallner, E.; Müllauer, L.; Schiefer, A.I.; Moser, J.; Klepetko, W.; Ankersmit, H.J.; et al. Prognostic and diagnostic impact of fibrinogen, neutrophil-to-lymphocyte ratio, and platelet-to-lymphocyte ratio on thymic epithelial tumors outcome. Oncotarget 2018, 9, 21861–21875. [Google Scholar] [CrossRef]
- Diem, S.; Schmid, S.; Krapf, M.; Flatz, L.; Born, D.; Jochum, W.; Templeton, A.J.; Früh, M. Neutrophil-to-Lymphocyte ratio (NLR) and Platelet-to-Lymphocyte ratio (PLR) as prognostic markers in patients with non-small cell lung cancer (NSCLC) treated with nivolumab. Lung Cancer 2017, 11, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Ghanim, B.; Hoda, M.A.; Klikovits, T.; Winter, M.P.; Alimohammadi, A.; Grusch, M.; Dome, B.; Arns, M.; Schenk, P.; Jakopovic, M.; et al. Circulating fibrinogen is a prognostic and predictive biomarker in malignant pleural mesothelioma. Br. J. Cancer 2014, 110, 984–990. [Google Scholar] [CrossRef]
- Ghanim, B.; Hoda, M.A.; Winter, M.P.; Klikovits, T.; Alimohammadi, A.; Hegedus, B.; Dome, B.; Grusch, M.; Arns, M.; Schenk, P.; et al. Pretreatment serum C-reactive protein levels predict benefit from multimodality treatment including radical surgery in malignant pleural mesothelioma: A retrospective multicenter analysis. Ann. Surg. 2012, 256, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Ruffie, P.; Feld, R.; Minkin, S.; Cormier, Y.; Boutan-Laroze, A.; Ginsberg, R.; Ayoub, J.; Shepherd, F.A.; Evans, W.K.; Figueredo, A. Diffuse malignant mesothelioma of the pleura in Ontario and Quebec: A retrospective study of 332 patients. J. Clin. Oncol. 1989, 7, 1157–1168. [Google Scholar] [CrossRef] [PubMed]
- Ruffie, P.A. Pleural mesothelioma. Curr. Opin. Oncol. 1991, 3, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Billé, A.; Krug, L.M.; Woo, K.M.; Rusch, V.W.; Zauderer, M.G. Contemporary Analysis of Prognostic Factors in Patients with Unresectable Malignant Pleural Mesothelioma. J. Thorac. Oncol. 2016, 11, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Zhuo, Y.; Lin, L.; Zhang, M. Pretreatment thrombocytosis as a significant prognostic factor in malignant mesothelioma: A meta-analysis. Platelets 2017, 28, 560–566. [Google Scholar] [CrossRef]
- Ghanim, B.; Rosenmayr, A.; Stockhammer, P.; Vogl, M.; Celik, A.; Bas, A.; Kurul, I.C.; Akyurek, N.; Varga, A.; Plönes, T.; et al. Tumour cell PD-L1 expression is prognostic in patients with malignant pleural effusion: The impact of C-reactive protein and immune-checkpoint inhibition. Sci. Rep. 2020, 10, 5784. [Google Scholar] [CrossRef]
- Rokkam, V.R.; Killeen, R.B.; Kotagiri, R. Secondary Thrombocytosis; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Haemmerle, M.; Stone, R.L.; Menter, D.G.; Afshar-Kharghan, V.; Sood, A.K. The Platelet Lifeline to Cancer: Challenges and Opportunities. Cancer Cell 2018, 33, 965–983. [Google Scholar] [CrossRef]
- Zhang, F.; Chen, Z.; Wang, P.; Hu, X.; Gao, Y.; He, J. Combination of platelet count and mean platelet volume (COP-MPV) predicts postoperative prognosis in both resectable early and advanced stage esophageal squamous cell cancer patients. Tumor Biol. 2016, 37, 9323–9331. [Google Scholar] [CrossRef]
- Gao, L.; Zhang, H.; Zhang, B.; Zhang, L.; Wang, C. Prognostic value of combination of preoperative platelet count and mean platelet volume in patients with resectable non-small cell lung cancer. Oncotarget 2017, 8, 15632–15641. [Google Scholar] [CrossRef] [PubMed]
- Gong, Z.; Xin, R.; Li, L.; Lv, L.; Wu, X. Platelet-to-lymphocyte ratio associated with the clinicopathological features and prognostic value of breast cancer: A meta-analysis. Int. J. Biol. Markers 2022, 37, 339–348. [Google Scholar] [CrossRef] [PubMed]
- Tural Onur, S.; Sokucu, S.N.; Dalar, L.; Iliaz, S.; Kara, K.; Buyukkale, S.; Altin, S. Are neutrophil/lymphocyte ratio and platelet/lymphocyte ratio reliable parameters as prognostic indicators in malignant mesothelioma? Ther. Clin. Risk Manag. 2016, 12, 651–656. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Li, J.; Zhang, S. Prognostic significance of inflammation-related and electrolyte laboratory variables in patients with malignant pleural mesothelioma. Front. Med. 2023, 10, 1099685. [Google Scholar] [CrossRef] [PubMed]
- Cihan, Y.B.; Ozturk, A.; Mutlu, H. Relationship between prognosis and neutrophil: Lymphocyte and platelet:lymphocyte ratios in patients with malignant pleural mesotheliomas. Asian Pac. J. Cancer Prev. 2014, 15, 2061–2067. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Dacic, S. Pleural mesothelioma classification-update and challenges. Mod. Pathol. 2022, 35, 51–56. [Google Scholar] [CrossRef]
- Wang, C.S.; Sun, C.F. C-reactive protein and malignancy: Clinico-pathological association and therapeutic implication. Chang. Gung Med. J. 2009, 32, 471–482. [Google Scholar]
- Bueno, R.; Opitz, I. Surgery in Malignant Pleural Mesothelioma. J. Thorac. Oncol. 2018, 13, 1638–1654. [Google Scholar] [CrossRef]
- Bertoglio, P.; Waller, D.A. The role of thoracic surgery in the management of mesothelioma: An expert opinion on the limited evidence. Expert Rev. Respir. Med. 2016, 10, 663–672. [Google Scholar] [CrossRef]
- Gebhart, F. MARS2: Decortication Plus Chemotherapy Associated with Worse Outcomes for Resectable Mesothelioma. Available online: https://www.ilcn.org/mars2-decortication-plus-chemotherapy-associated-with-worse-outcomes-for-resectable-mesothelioma/ (accessed on 20 October 2023).




{kind=link}
{kind=link}
{kind=link}
| Variable | Cut-Off | n | % of the Whole Study Population | Median OS (Months) | 95% CI | p * |
|---|---|---|---|---|---|---|
| Age at diagnosis | ≤median 65.5 years >median | 49 49 | 50.0 50.0 | 25.6 12.3 | 23.2–28.0 7.8–16.8 | 0.057 |
| Sex | female male | 25 73 | 25.5 74.5 | 25.6 18.1 | 11.2–40.0 9.7–26.5 | 0.842 |
| Histology | epithelioid non-epithelioid | 84 14 | 85.7 14.3 | 24.2 7.8 | 16.7–31.7 5.6–10.0 | 0.053 |
| Treatment modality | multimodal surgery alone C/R/I BSC | 65 9 7 17 | 66.3 9.2 7.1 17.3 | 26.1 11.7 9.2 3.2 | 23.1–29.2 10.5–13.0 4.1–14.4 1.8–4.5 | <0.001 |
| Surgery vs. none | cytoreductive surgery no surgery | 74 24 | 75.5 24.5 | 25.5 3.8 | 23.0–28.0 2.3–5.4 | <0.001 |
| Hemoglobin | ≤cut-off 12 g/dL >cut-off 12 g/dL ≤median 12.7 g/dL >median | 36 62 49 49 | 36.7 63.3 50.0 50.0 | 15.0 24.2 16.1 23.6 | 9.2–20.7 15.8–32.6 4.5–27.8 13.7–33.5 | 0.021 0.250 |
| Platelets | ≤median 280 G/L >median | 49 49 | 50.0 50.0 | 26.1 11.7 | 17.7–34.6 7.0–16.4 | <0.001 |
| Leukocytes | ≤median 7.5 G/L >median | 46 45 | 46.9 45.9 | 23.6 17.0 | 7.6–39.6 11.4–22.6 | 0.716 |
| Neutrophils | ≤median 5.2 G/L >median | 49 49 | 50.0 50.0 | 24.9 16.1 | 16.9–32.9 9.0–23.3 | 0.794 |
| Monocytes | ≤median 0.7 G/L >median | 45 45 | 45.9 45.9 | 25.6 12.8 | 21.1–30.1 7.0–18.6 | 0.051 |
| Lymphocytes | ≤median 1.5 G/L >median | 49 49 | 50.0 50.0 | 15.0 24.3 | 7.0–22.9 16.6–32.0 | 0.602 |
| NLR | ≤median 3.3 >median | 49 49 | 50.0 50.0 | 23.6 16.1 | 15.7–31.5 9.0–23.3 | 0.727 |
| LMR | ≤median 2.4 >median | 45 45 | 45.9 45.9 | 15.0 24.3 | 8.7–21.2 15.2–33.4 | 0.601 |
| PLR | ≤median 195.6 >median | 49 49 | 50.0 50.0 | 25.5 12.3 | 23.4–27.6 4.8–19.8 | 0.023 |
| CRP | ≤cut-off 1 mg/dL >cut-off 1 mg/dL ≤median 2 mg/dL >median | 35 53 44 44 | 35.7 54.1 44.9 44.9 | 23.6 18.0 24.2 13.3 | 9.9–37.2 6.9–29.1 13.4–35.0 5.3–21.0 | 0.393 0.437 |
| Variables | Cut-Off/Subgroup | HR | 95% CI | p ** |
|---|---|---|---|---|
| Age | metric median 65.5 years | 1.03 1.54 | 1.01–1.06 0.98–2.40 | 0.041 0.059 |
| Gender | female, male | 0.95 | 0.56–1.60 | 0.842 |
| Histology | epithelioid, non-epithelioid | 1.84 | 0.98–3.44 | 0.056 |
| Treatment modality | multimodal, surgery alone, C/R/I, BSC | 1.83 | 1.51–2.23 | <0.001 |
| Surgery vs. none | cytoreductive surgery, no surgery | 0.23 | 0.14–0.40 | <0.001 |
| Hemoglobin | metric cut-off 12 g/dL median 12.7 g/dL | 0.87 0.57 0.77 | 0.77–0.99 0.35–0.92 0.49–1.21 | 0.037 0.022 0.251 |
| Platelets | metric median 280 G/L | 1.003 2.39 | 1.001–1.004 1.49–3.84 | 0.001 <0.001 |
| Leukocytes | metric median 7.5 G/L | 1.01 1.09 | 0.94–1.09 0.69–1.73 | 0.741 0.716 |
| Neutrophils | metric median 5.2 G/L | 1.01 1.06 | 0.93–1.09 0.68–1.66 | 0.836 0.794 |
| Monocytes | metric median 0.7 G/L | 1.20 1.59 | 0.94–1.29 0.99–2.54 | 0.260 0.053 |
| Lymphocytes | metric median 1.5 G/L | 0.92 0.89 | 0.66–1.29 0.57–1.39 | 0.628 0.603 |
| NLR | metric median 3.3 | 0.99 1.08 | 0.92–1.07 0.69–1.70 | 0.836 0.728 |
| LMR | metric median 2.4 | 0.82 0.89 | 0.64–1.05 0.56–1.41 | 0.122 0.611 |
| PLR | metric median 195.6 | 1.002 1.68 | 1.00–1.004 1.07–2.64 | 0.012 0.025 |
| CRP | metric cut-off 1 mg/dL median 2 mg/dL | 1.05 1.23 1.20 | 0.99–1.10 0.77–1.96 0.76–1.90 | 0.059 0.394 0.438 |
| Variables | Adjusted HR for Death | 95% CI | p *** | |
|---|---|---|---|---|
| Age at diagnosis | ≤65.5 years >65.5 years | 1 1.59 | 0.93–2.73 | 0.09 |
| Sex | female male | 1 1.02 | 0.55–1.90 | 0.96 |
| Histology | epithelioid non-epithelioid | 1 3.45 | 1.60–7.40 | 0.002 |
| Stage | early (I, II) late (III, IV) | 1 1.38 | 0.73–2.62 | 0.33 |
| Surgery vs. no surgery | cytoreductive surgery no surgery | 1 3.04 | 1.43–6.43 | 0.004 |
| Platelet level | ≤280 G/L >280 G/L | 1 2.01 | 1.09–3.70 | 0.025 |
| CRP level | ≤1 mg/dL >1 mg/dL | 1 1.76 | 1.03–3.00 | 0.039 |
| Variable | HR | 95% CI | p *** | |
|---|---|---|---|---|
| CRP | ≤1 mg/dL >1 mg/dL | 1 3.42 | 1.33–8.75 | 0.011 |
| Surgery vs. no surgery | no surgery cytoreductive surgery | 1 0.39 | 0.17–0.90 | 0.028 |
| CRP × surgery vs. no surgery | (=interaction term) | 0.33 | 0.11–0.99 | 0.048 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iser, S.; Hintermair, S.; Varga, A.; Çelik, A.; Sayan, M.; Kankoç, A.; Akyürek, N.; Öğüt, B.; Bertoglio, P.; Capozzi, E.; et al. Validation of Inflammatory Prognostic Biomarkers in Pleural Mesothelioma. Cancers 2024, 16, 93. https://doi.org/10.3390/cancers16010093
Iser S, Hintermair S, Varga A, Çelik A, Sayan M, Kankoç A, Akyürek N, Öğüt B, Bertoglio P, Capozzi E, et al. Validation of Inflammatory Prognostic Biomarkers in Pleural Mesothelioma. Cancers. 2024; 16(1):93. https://doi.org/10.3390/cancers16010093
Chicago/Turabian StyleIser, Stephanie, Sarah Hintermair, Alexander Varga, Ali Çelik, Muhammet Sayan, Aykut Kankoç, Nalan Akyürek, Betül Öğüt, Pietro Bertoglio, Enrico Capozzi, and et al. 2024. "Validation of Inflammatory Prognostic Biomarkers in Pleural Mesothelioma" Cancers 16, no. 1: 93. https://doi.org/10.3390/cancers16010093
APA StyleIser, S., Hintermair, S., Varga, A., Çelik, A., Sayan, M., Kankoç, A., Akyürek, N., Öğüt, B., Bertoglio, P., Capozzi, E., Solli, P., Ventura, L., Waller, D., Weber, M., Stubenberger, E., & Ghanim, B. (2024). Validation of Inflammatory Prognostic Biomarkers in Pleural Mesothelioma. Cancers, 16(1), 93. https://doi.org/10.3390/cancers16010093