Simple Summary
The present systematic review and meta-analysis aimed to assess how anxiety and depression conditions among cancer patients vary according to sex. This systematic review and meta-analysis was registered in PROSPERO with id no. CRD42024512553. The search strategy involved combining keywords using Boolean operators, including “Anxiety”, “Cancer”, and “Depression”, across several databases: British Nursing Database, CINAHL, Embase, Nursing & Allied Health Database, PubMed, Scopus, and Web of Science. The outcomes were evaluated using the Hospital Anxiety and Depression Scale (HADS). Data were collected from five studies, enrolling a total of 6317 cancer patients, of whom 2961 were females and 3356 males. Generally, females reported significant higher levels of depression scores than males and, conversely, males reported significantly greater levels of anxiety than females.
Abstract
(1) Background: Evidence suggested inconsistent results in anxiety and depression scores among female and male cancer patients. The present systematic review and meta-analysis aimed to assess how anxiety and depression conditions among cancer patients vary according to sex. (2) Methods: This systematic review and meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA). The protocol was registered in PROSPERO with id no. CRD42024512553. The search strategy involved combining keywords using Boolean operators, including “Anxiety”, “Cancer”, and “Depression”, across several databases: Embase, PubMed, Scopus, and Web of Science. The outcomes were evaluated using the Hospital Anxiety and Depression Scale (HADS). (3) Results: Data were collected from five studies, enrolling a total of 6317 cancer patients, of whom 2961 were females and 3356 males. For each study, HADS-A and HADS-D scores were considered, also differentiating HADS scores according to cancer typology, and then three different meta-analyses were performed. Generally, females reported significantly higher levels of depression scores than males and, conversely, males reported significantly greater levels of anxiety than females. (4) Conclusions: Previous studies suggested higher rates of depression and anxiety conditions in females than in males, but the present data highlighted controversial findings, since males reported significantly higher levels of anxiety than females. In this scenario, the theoretical approach justified females being more open than males to expressing anxiety or depression conditions. It would be necessary for healthcare professionals to improve effective measures purposed at assessing and mitigating depressive symptoms in cases of advanced cancer, thereby improving their mental health, given the high rates of depression in advanced cancer patients, due to the difficulty level of performing their daily living activities, which deteriorate further over time.
1. Introduction
Cancer is a leading cause of death worldwide, accounting for nearly 10 million deaths in 2020, or nearly one in six deaths. The most prevalent types of cancer are those of the breast, lung, colon and rectum, and prostate [1]. The reported increase in incidence may be partially explained by an increase in risk behavior in terms of excessive tobacco use, high body mass index, alcohol consumption, low fruit and vegetable intake, and lack of physical activity [1].
Despite oncology improvements, cancer is still commonly overlapped with the death concept, pain, and affliction [2]. Cancer is not only a unique incident with a persistent condition distinguished by constant ambiguity and the delayed consequences of the disease, but it also has care and concomitant psychological concerns [3]. Various physical and psychological troubles have been considered as direct consequences of neoplasms, and the treatment dimensions have been often considered as interference with the patients’ daily activities and skills to preserve family and social relationships [4]. Past researchers have just explained a positive association between cancer diseases and psychiatric ones [5,6], since cancer diagnosis and treatment have generally impacted on distress and negatively interfered in daily activities [7], with increasing rates in new diagnoses of clinical reports of anxiety (10 to 58%) and depression (14 to 30%) [8,9]. However, data from the current literature seem to be inconsistent, since there are some studies which report decreases in anxiety and depression symptoms [10] and others which report worsened depression conditions associated with a cancer diagnosis [11]. However, further researchers present reasonable evidence that cancer patients with a psychiatric morbidity, such as depression or anxiety symptoms, appear to record poor survival and a lower quality of life [12,13]. Additionally, in a healthy general population, particularly among sexual minorities, it has been registered that there is nearly a 1.5 times higher risk of anxiety and depression than in the heterosexual population [14,15], with worse anxiety and depression levels being reported. In a systematic review involving cancer patients, females report higher levels of depression than males; however, other studies suggest the contrary [12]. In cases of advanced cancer, women and younger patients record higher depressive symptoms than men and older individuals [16,17]. Additionally, social characteristics could also play a determinant role in patients’ emotional condition [18,19]. In fact, females, younger patients, and unmarried individuals with recurring cancer show more depressive symptoms than males, older patients, married patients, and those discovering cancer for the first time [16,17].
By considering all the abovementioned literature, the present systematic review and meta-analysis aims to assess how anxiety and depression conditions vary among cancer patients according to sex.
2. Materials and Methods
2.1. Search Strategy
The present systematic review and meta-analysis was conducted according to the Equator checklist for reviews, like the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) [20]. The protocol was registered in PROSPERO with id no. CRD42024512553.
Keywords and MeSH expressions were combined with the Boolean operators, such as “Anxiety”, “Cancer”, and “Depression” (Supplementary Materials File S1), and the “Population-Intervention-Outcome” (PIO) arrangement was built (Table 1). The Embase, PubMed, Scopus, and Web of Science databases were consulted for this review.

Table 1.
The PIO tool for the present systematic review and meta-analysis.
The review included all the interventional (randomized clinical trials, quasi-experimental) studies recording anxiety and depression conditions with the Hospital Anxiety and Depression Scale (HADS) [21,22,23] among cancer patients. Specifically, the HADS covers a total of 14 items. Of these, 7 items explore anxiety (HADS-A) and 7 ones quantify depression (HADS-D). Each subdimension ranges from 0 to 21 and higher scores indicate a greater distress level. Evidence suggests a high reliability and validity of the scale for both of the two subdimensions. Additionally, the present review only included manuscripts published in the English language available in their full-text versions.
2.2. Peer Review and Data Extraction
Initially, records were identified through a systematic database search, uploaded to reference management software, and duplicate studies were removed. Then, two independent reviewers (E.V. and H.K.) assessed the title and abstract of the identified studies, inclusion was assessed, and unsuitable reports were removed. After that, articles were uploaded, and the full-text version of each article was assessed more closely according to the fixed eligibility criteria. Disagreements about whether a study should be included or not were resolved by discussion and consensus. If the disagreement remained, arbitration from another reviewer was provided. Data collection was performed by considering the following: study characteristics (author, year of publication, aim, design, sample size, and setting), participants (age, cancer stage, and type of treatments performed), and the outcomes both in anxiety and depression were also appropriately assessed by the HADS [21].
2.3. Records Assessed
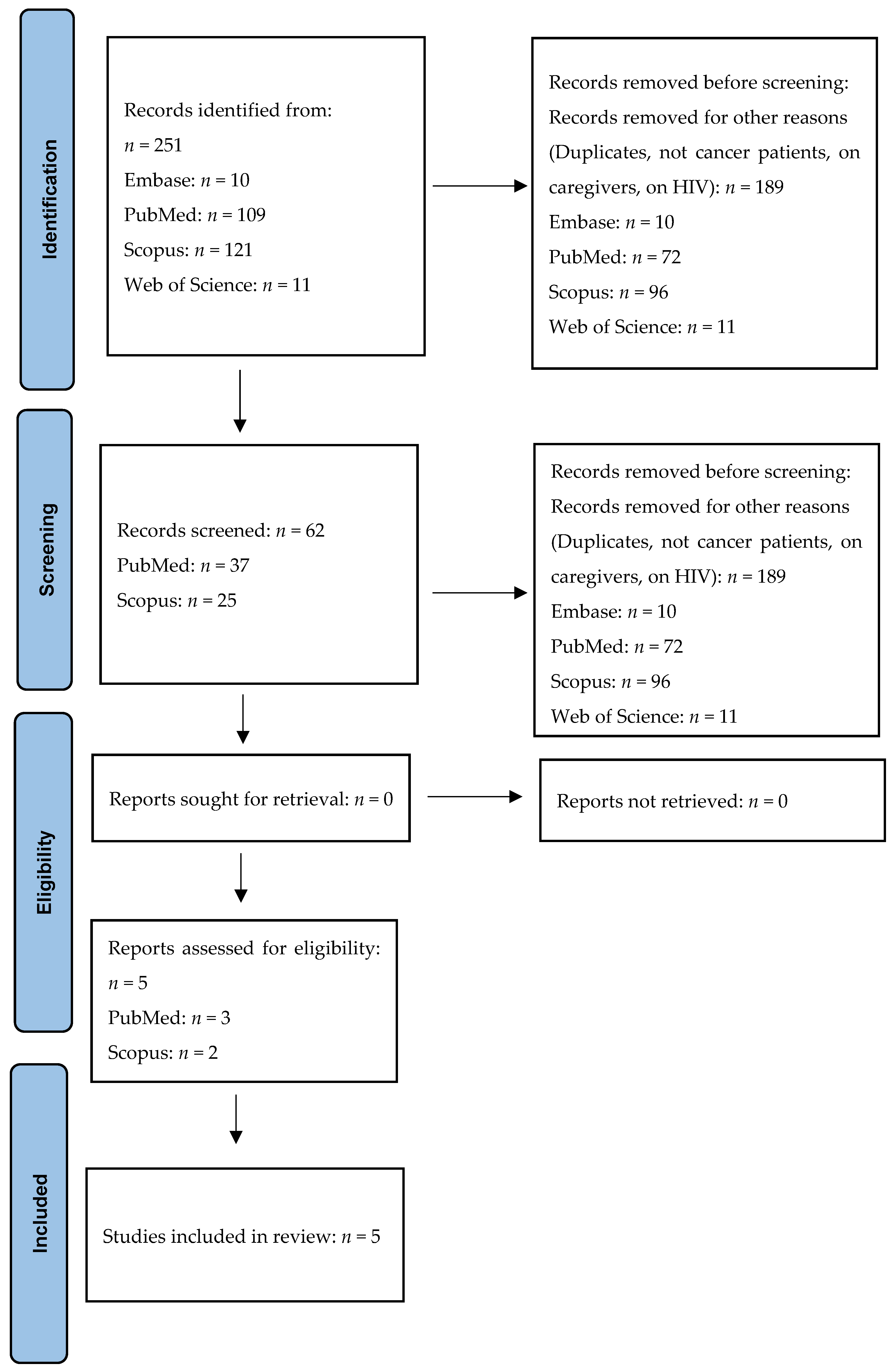
A total of 251 records were searched at the first phase of the present literature review (Figure 1). Then, 189 articles were removed as their titles were not in accordance with the purpose of this review. After selecting the remaining articles, a total of 57 eligible records were further screened, since their abstracts did not meet all the inclusion criteria fixed in our protocol, as both anxiety and depression were not assessed through the HADS, the participants were cancer patients’ caregivers, patients did not suffer from a cancer disease, manuscripts were written in other languages different from the English one, or the full-text version was not available. Additionally, the same manuscripts present in all the databases considered were screened and taken into consideration only once. Thus, only 5 articles were considered as eligible for the present systematic review and meta-analysis (Figure 1).
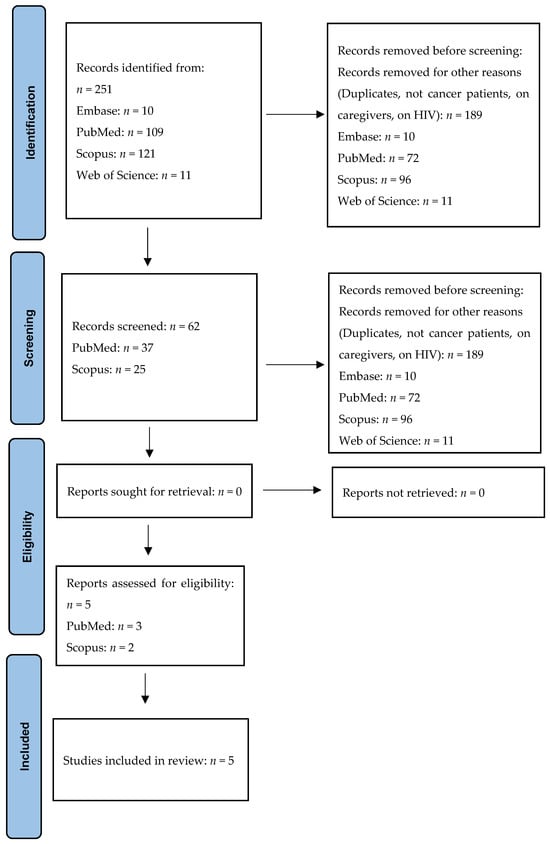
Figure 1.
The PRISMA flow-chart.
2.4. Interventions and Outcomes
The present systematic review and meta-analysis embraced all interventional, randomized clinical trials, and quasi-experimental studies recording anxiety and depression conditions with the Hospital Anxiety and Depression Scale (HADS) [21], before and after a coaching intervention in any cancer treatment, such as surgery, chemotherapy, radiotherapy, or endocrine therapy. The HADS includes a total of 14 items, of which 7 items assess anxiety (HADS-A) and 7 items quantify depression (HADS-D) [22]. Each subdimension ranges from 0 to 21 and higher scores indicate a greater pathological condition level. Evidence suggests a high reliability and validity of the scale for both the two subdimensions investigated [23]. Although the literature suggested several anxiety and depression self-reported questionnaires, we chose the HADS self-reported questionnaire as our outcome tool as it reports both anxiety and depression in a unique questionnaire [23].
No pre-existing psychiatric conditions were highlighted: all studies included considered only health psychiatric patients, who, after a cancer diagnosis, might consequentially develop an anxious or depressive disorder.
Additionally, data were collected from patients who self-reported their sex identities as female/male.
2.5. Quality and Bias Assessments
The quality assessment of all the selected studies was assessed by considering the study design of each manuscript included in the present review, in accordance with the Evidence-Based Nursing (EBN) approach [24]. The EBN methodology included a total of seven levels of evidence, ranging from I to VII, suggesting the weakest quality of study design, specifically as follows:
- Level I: Evidence from systematic reviews or meta-analysis of randomized control trials;
- Level II: Evidence from well-designed randomized control trials;
- Level III: Evidence from well-designed control trials that are not randomized;
- Level IV: Evidence from case–control or cohort studies;
- Level V: Evidence from systematic reviews of descriptive or qualitative studies;
- Level VI: Evidence from a single descriptive or qualitative study;
- Level VII: Evidence from expert opinions.
Furthermore, due to the nature of primary studies selected, we employed the Downs and Black checklist [25] to evaluate the quality of the included studies. This instrument evaluates the quality of both randomized and non-randomized studies. The tool consists of 27 items with 3 related subheadings: external validity, internal validity, and power. Based on these assessments, the tool has the categories of “low” (score less than 14), “fair” (score between 15 and 19), “good” (score between 20 and 25), and “excellent” (score between 26 and 27) [25].
2.6. Main Outcome(s)
The Hospital Anxiety and Depression Scale (HADS) was used to assess differences in cancer patients between females and males, and then we considered the cancer typologies included in the literature.
2.7. Measures of Effect
Previous studies showed that the HADS contains a total of 14 items on a self-rating scale with two subdimensions, one assessing anxiety (HADS-A) and the other one assessing depression (HADS-D). Anxiety and depression cutoff values for pathological conditions ranged from 8 to 11 in oncologic settings and the data were presented as means and standard deviations [26].
2.8. Data Synthesis
Studies were assessed for quality as per protocol recommendations. The information retrieved from the final selected studies was expressed using both a narrative approach and tables. Descriptive statistics were presented as means, standard deviations, and number of cases (n) in a Forest plot. Statistical analysis was performed using the R environment (version 4.2). A random effects meta-analysis based on estimates and their standard errors was implemented. To assess the consistency across studies, the I2 statistic was adopted with 25%, 50%, and 75% suggesting low, moderate, and high heterogeneity degrees, respectively. However, I2 should be presented and interpreted cautiously in small meta-analyses [27]. For this reason, 95% confidence intervals (95% CI) were presented in addition to the point estimate. The χ2-based Q test was also applied to look for the heterogeneity of effects among studies. The Q statistic at a cut-off significance level of 0.10 suggested the presence of significant heterogeneity. The τ2 statistic was also presented to check the variance of the true effects.
3. Results
Data were collected from five studies [28,29,30,31,32], enrolling a total of 6317 cancer patients, of whom 2961 were females and 3356 males. For each study, HADS-A and HADS-D scores were considered, HADS scores were differentiated according to cancer typology, and then three different meta-analyses were performed.
Table 2 explained all study characteristics, specifically the following: author(s) and year of publication, study design, level of evidence, sample size according to sex, range of age, eligible criteria, instruments to assess both anxiety and depression, and findings revealed.
Table 2.
Anxiety and depression assessed with the HADS in oncology, comparing females and males (n = 5).
3.1. Study Characteristics
In the Skarstein et al. study [28], a total of 568 cancer patients were enrolled and simultaneously evaluated with the Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ C33) and the Hospital Anxiety and Depression Scale (HADS). Statistically significant negative associations were assessed between HADS-A, HADS-D, and HADS-T (total score). Males of all ages recorded worse HADS scores than females. In this regard, Nipp et al. [31] showed that males and younger patients receiving early palliative care assistance better perceived their quality of life and anxiety than those receiving usual oncology care. Conversely, females and older patients did not report any difference in their treatment impacts.
Evidence reported that nearly 47.2% and 57% of gastrointestinal cancer patients reported high levels of both anxiety and depression. However, there were no significant differences between sex, while patients who knew their cancer diagnosis reported very high anxiety and depression scores [29]. Moser et al. [30] considered that being female could inevitably be a risk factor for high perceived depression and anxiety levels. In this regard, they assessed a significant proportion of patients reporting high levels of anxiety, depression, and psychological distress, among females and both among patients and partners, too, by assigning to the female sex a negative trend in psychological conditions among cancer patients. Also, Oertelt-Prigione et al. [32] reported negative associations in emotional functions and female survivors, since female survivors had more moderate physical and cognitive functioning than males who reported a significant loss in their social roles. Therefore, a significant and unexpected long-term impact on male patients was reported by highlighting the need to further investigate these sex-related dimensions.
3.2. Bias Risk Assessment
In addition to this, we employed the Downs and Black checklist [25] to assess the quality of randomized trials and non-controlled studies. Two reviewers (E.V. and K.H.) independently assessed the quality of studies under the following headings: reporting, external validity, and internal validity (bias and confounding) against the rater checklist (Downs and Black checklist to 0.1.2). After the quality assessment, both reviewers mutually checked individual studies’ scores, and the third author (A.S.) sorted out any disagreements between the first two reviewers (E.V. and K.H.). This Downs and Black checklist included a total of 28 items under three headings, reporting, internal validity, and extremal validity, referring to the power of the study rating and whether or not the study was performed to the power calculation. The maximum score for each item was 1, as a power analysis assessed the five studies, and thus the highest possible score for the checklist was 28. The Downs and Black score varied according to the quality levels as follows: excellent (26–28); good (20–25); fair (15–19); and poor (≤14). To assess bias risk, the reviewers’ results were compared by an external reviewer, and discrepancies were resolved in a consensus meeting (Table 3).
Table 3.
Quality assessment of all the studies included in the present systematic review.
3.3. Meta-Analysis Results for HADS-Anxiety (HADS-A)
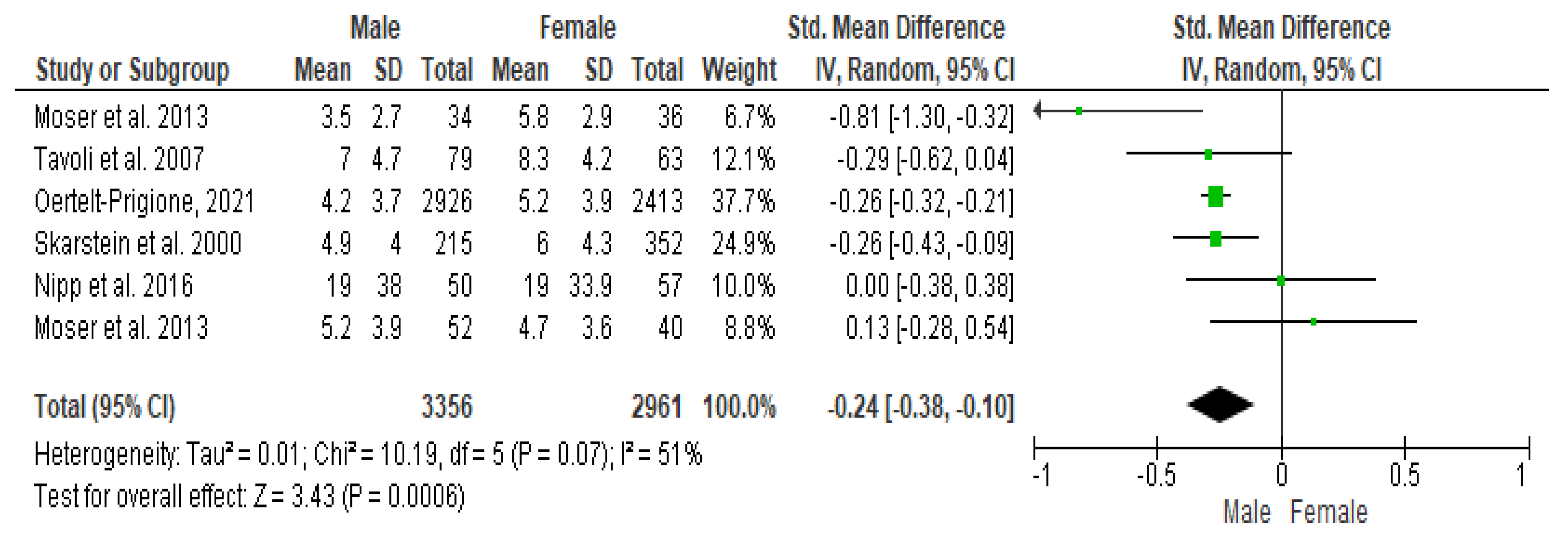
The Cochrane Q-test revealed the presence of a significant heterogeneity between the studies (PQ = 0.001; tau2 = 0.01; I2 = 51%) (Figure 2). Figure 3 suggests the absence of publication bias, and Egger’s regression intercept confirmed this result (β = −0.24; 95% CI = [−0.38–0.10]). Finally, the overall effect showed a significant difference between the two sexes (Z = 3.43; p = 0.0006), as males recorded significantly higher values of anxiety than females.
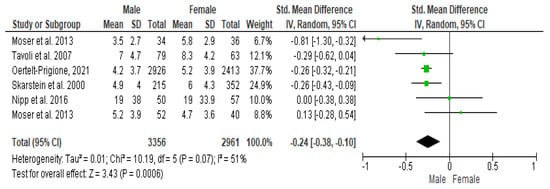
Figure 2.
Forest plot of HADS-A between female and male cancer patients. The Cochrane Q-test explained the presence of a significant heterogeneity between the studies selected.
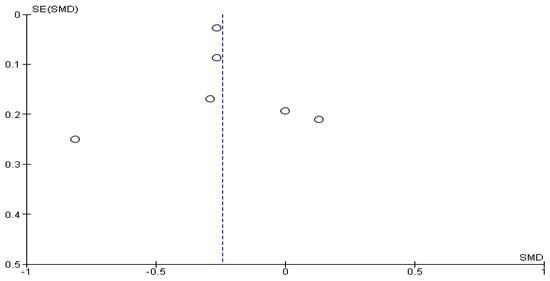
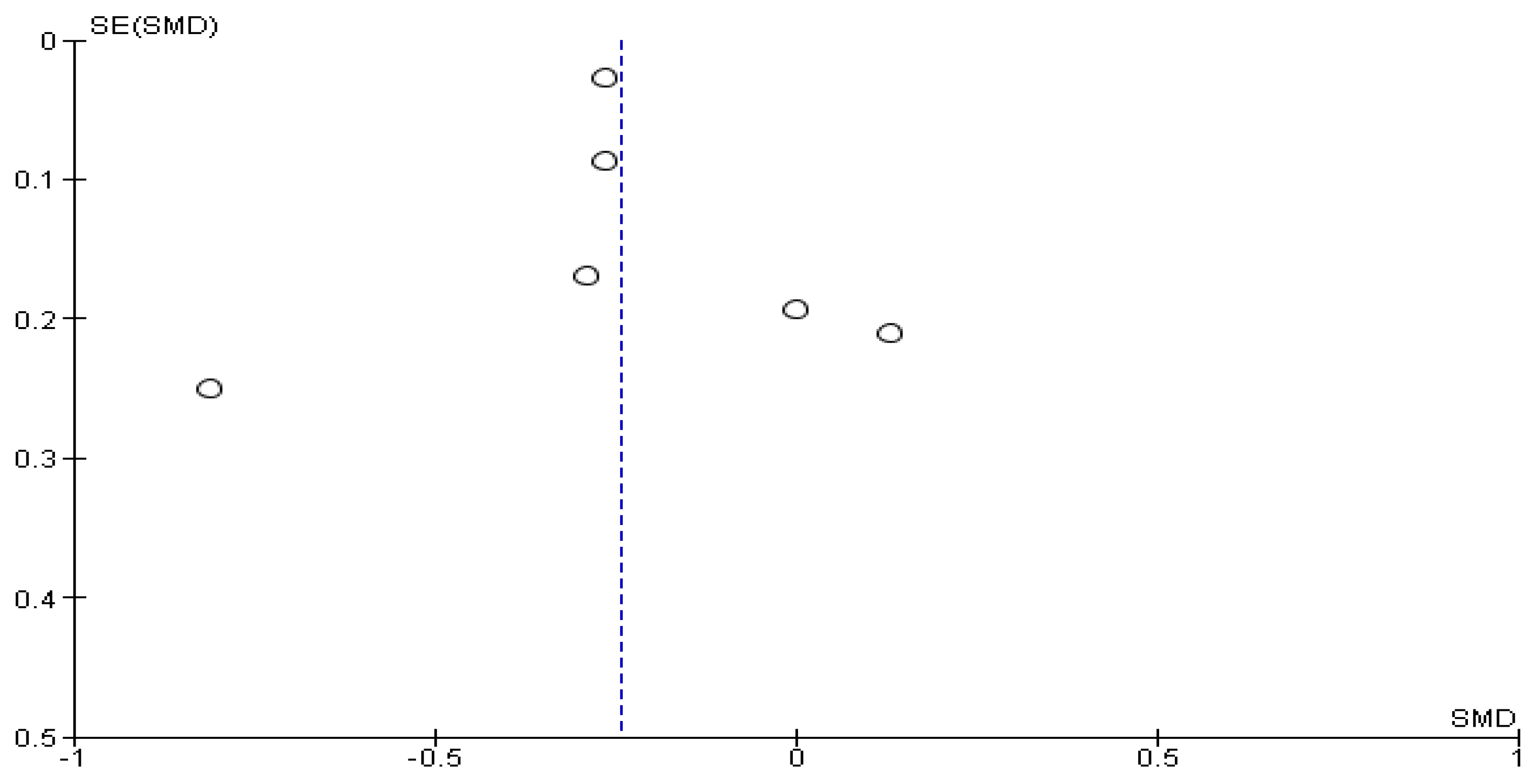
Figure 3.
Publication bias of HADS-A between female and male cancer patients. The absence of publication bias and Egger’s regression intercept confirmed this result. A significant difference between the two sexes (Z = 3.43; p = 0.0006) confirmed that males recorded significantly higher values of anxiety than females.
3.4. Meta-Analysis Results for HADS-Depression (HADS-D)
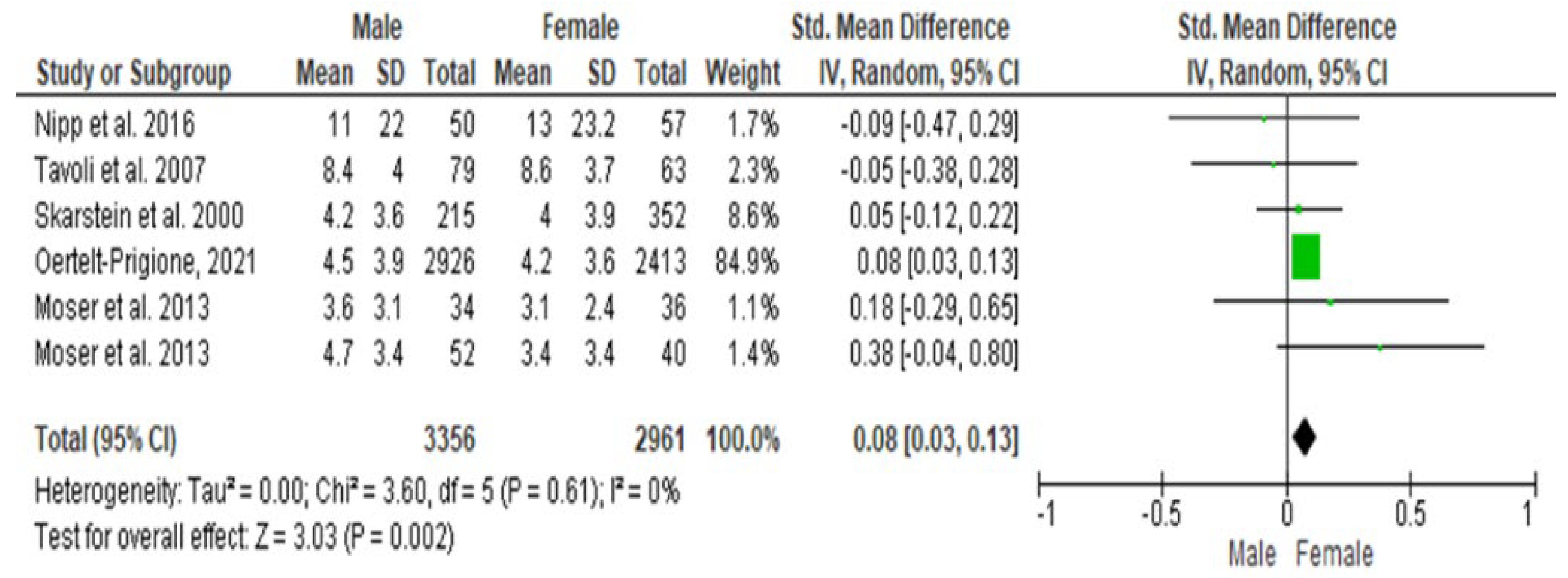
The Cochrane Q-test revealed the presence of a significant heterogeneity between the studies (PQ = 0.61; tau2 < 0.001; I2 = 0%) (Figure 4). Figure 5 suggests the absence of publication bias, and the regression intercept confirmed this result (β = 0.08; 95% CI = [0.03–0.13]). Finally, the overall effect showed a significant difference between the two sexes (Z = 3.03; p = 0.002), as females recorded significantly higher values of depression scores than males.
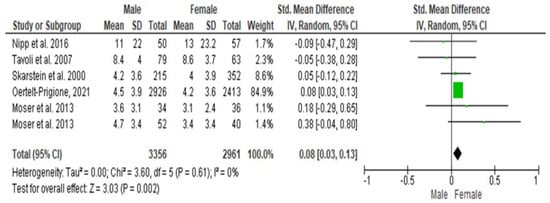
Figure 4.
Forest plot of HADS-D between female and male cancer patients. The Cochrane Q-test revealed the presence of a significant heterogeneity between the selected studies.
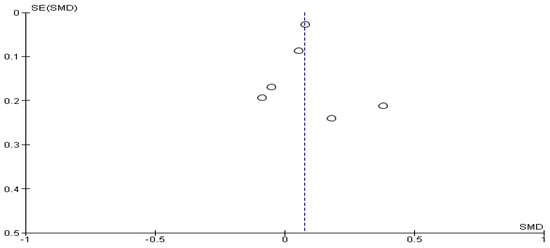
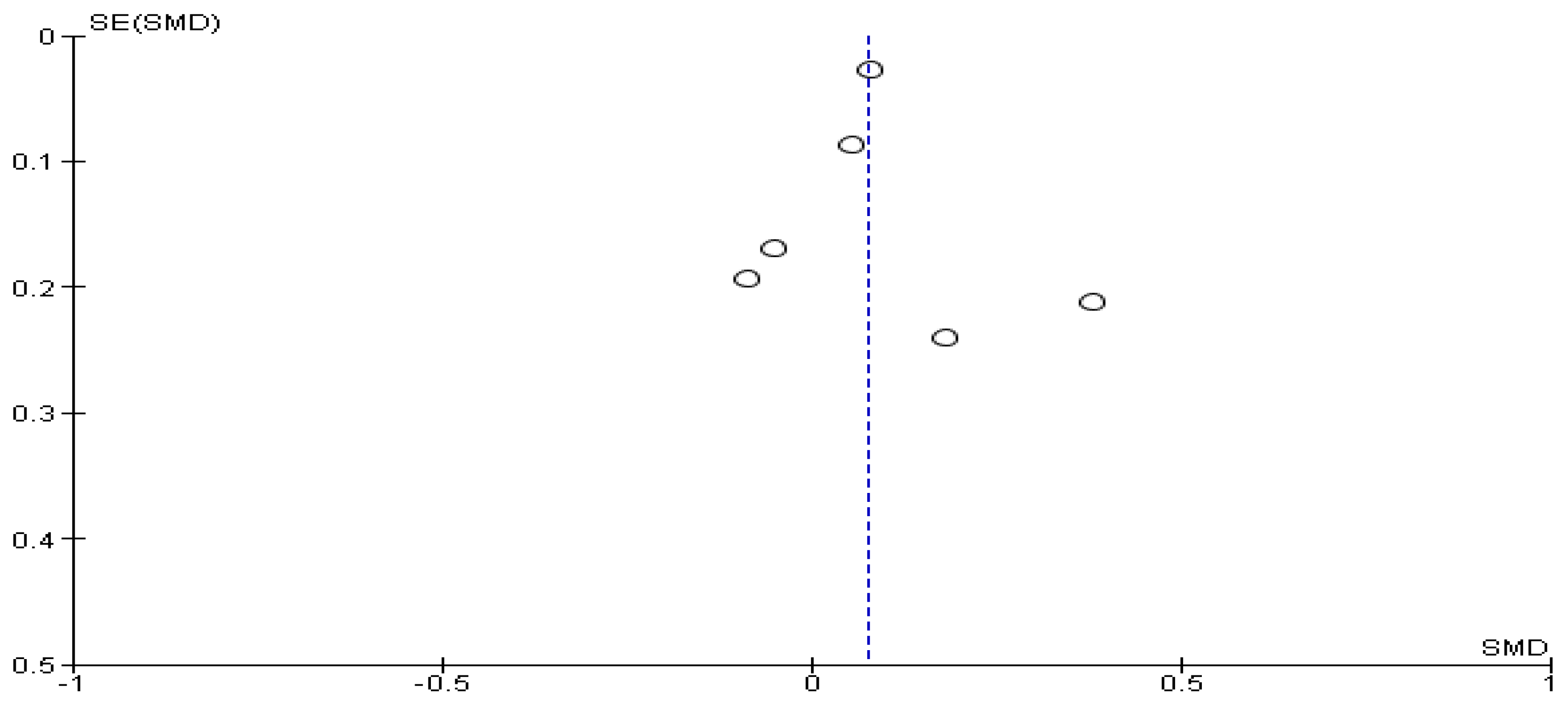
Figure 5.
Publication bias of HADS-D between female and male cancer patients. Figure 5 suggested the absence of publication bias, and the regression intercept confirmed this result: females recorded significantly higher values of depression scores than males.
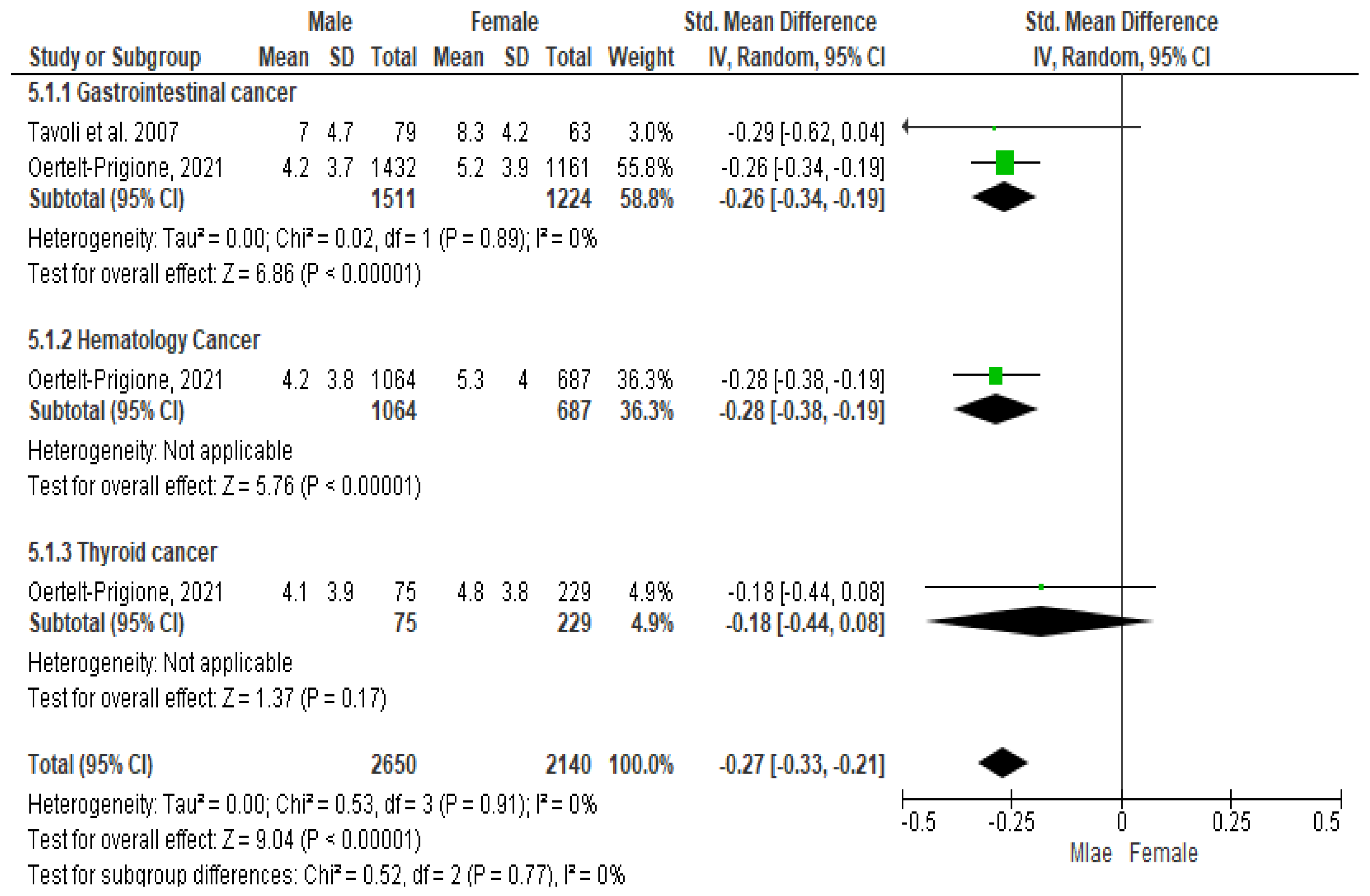
3.5. Meta-Analysis Results for HADS-Anxiety (HADS-A) among Patients Diagnosed with Gastrointestinal, Blood, and Thyroid Cancers
As regards gastrointestinal cancer, the Cochrane Q-test revealed the presence of a significant heterogeneity between the selected studies (PQ = 0.02; tau2 < 0001; I2 = 0%) (Figure 6). The Funnel plot suggested the absence of publication bias (Figure 6), and Egger’s regression intercept confirmed this result (β = −0.26; 95% CI = [−0.34–0.191]). Finally, the overall effect showed a significant difference between the two sexes (Z = 6.86; p < 0.00001), as males recorded significantly higher values of depression than females.
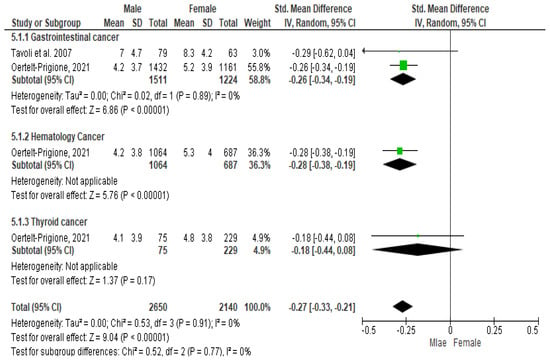
Figure 6.
Anxiety symptoms among patients diagnosed with gastrointestinal, blood, and thyroid cancers.
As regards hematologic cancers, the presence of a significant heterogeneity between the studies was not assessed, since there was only one article for this typology (Figure 4). The Funnel plot suggested the absence of publication bias (Figure 6) and the Egger’s regression intercept confirmed this result (β = −0.28; 95% CI = [−0.38–0.19]), too. Finally, the overall effect showed a significant difference between the two sexes (Z = 6.86; p < 0.00001), as males recorded significantly higher values of anxiety than females.
As regards thyroid cancer, the presence of a significant heterogeneity between the studies was not assessed, since there was only one article for this typology (Figure 4). The Funnel plot suggested the absence of publication bias (Figure 6) and the Egger’s regression intercept confirmed this result (β = −0.18; 95% CI = [−0.44–0.08]). Finally, the overall effect showed a significant difference between the two sexes (Z = 1.37; p = 0.17), as males recorded significantly higher values of anxiety than females.
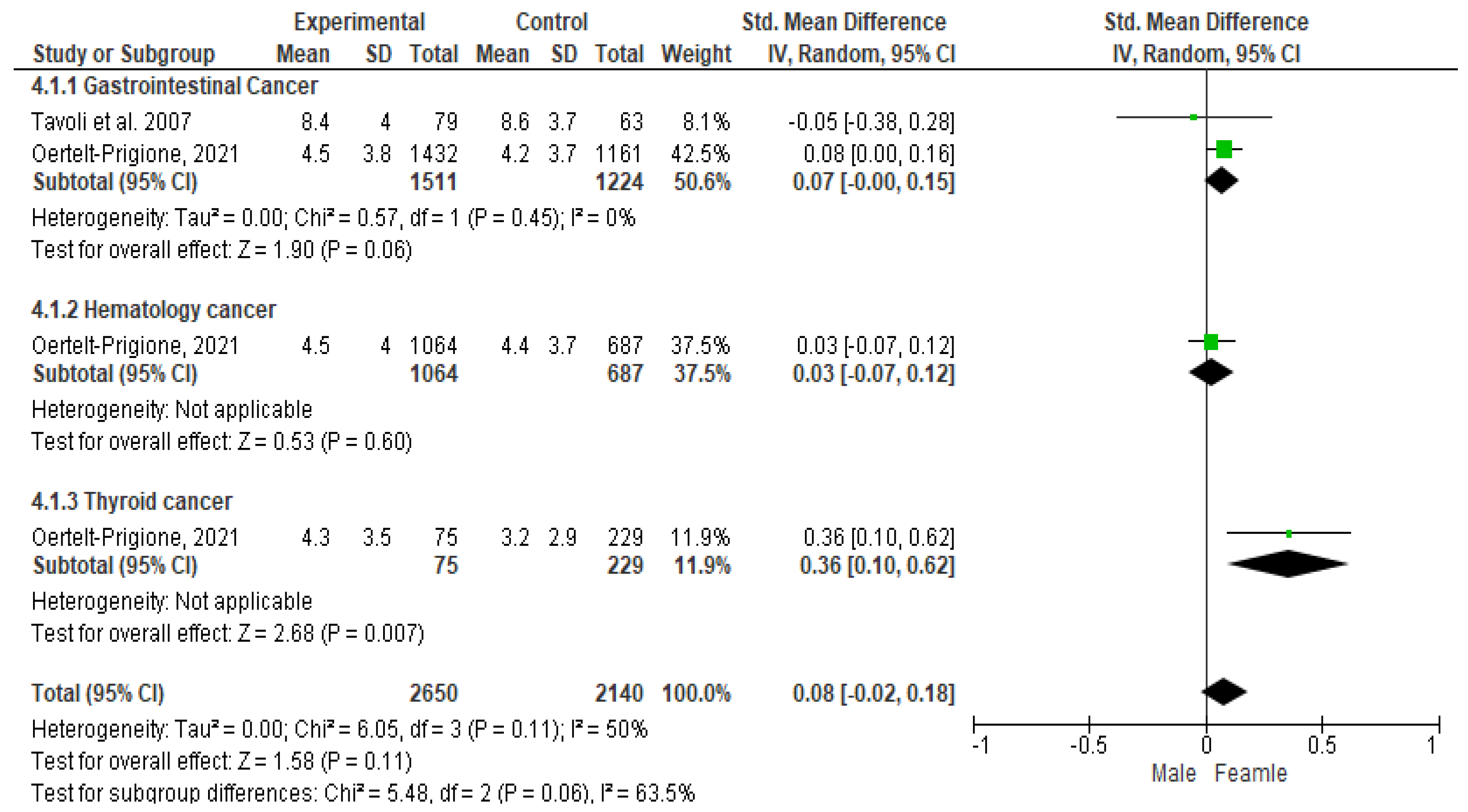
3.6. Meta-Analysis Results for HADS-Depression (HADS-D) among Patients Diagnosed with Gastrointestinal, Blood, and Thyroid Cancers
As regards gastrointestinal cancer, the Cochrane Q-test revealed the presence of a significant heterogeneity between the studies (PQ = 0.57; tau2 < 0001; I2 = 0%) (Figure 7). The Funnel plot suggested the absence of publication bias (Figure 5) and the Egger’s regression intercept supported this result (β = 0.07; 95% CI = [−0.00–0.15]). Finally, the overall effect showed a significant difference between the two sexes (Z = 1.90; p = 0.06), as females recorded significantly higher values of anxiety than males.
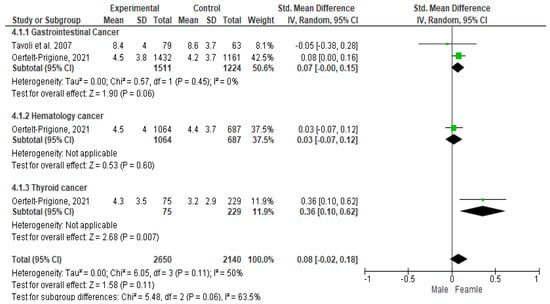
Figure 7.
Depression symptoms among patients diagnosed with gastrointestinal, blood, and thyroid cancers.
In hematologic cancers, the presence of a significant heterogeneity between the studies was not assessed, since there was only one article for this typology (Figure 7). The Funnel plot suggested the absence of publication bias (Figure 5) and the Egger’s regression intercept endorsed this finding (β = 0.03; 95% CI = [−0.07–0.12]). Finally, the overall effect did not show any significant difference between the two sexes (Z = 0.53; p = 0.60), as males and females recorded overlapping values of depression outcomes.
As regards thyroid cancer, the presence of a significant heterogeneity between the studies was not assessed, since there was only one article for this typology (Figure 5). The Funnel plot suggested the absence of publication bias (Figure 5) and the Egger’s regression intercept supported this result (β = 0.36; 95% CI = [0.10–0.62]). Finally, the overall effect showed a significant difference between the two sexes (Z = 2.68; p = 0.007), as females recorded significantly higher values of depression than males.
4. Discussion
The present systematic review and meta-analysis aimed to assess how anxiety and depression conditions vary between female and male cancer patients. The literature has explained how anxiety and depression have been commonly mentioned in psychological distress, due to the diagnosis of cancer [33], and most cancer patients have different levels of psychological difficulty, which depends on the progression of cancer [34]. In this regard, the American Psychiatric Association declared that individuals respond differently to the diagnosis of neoplasms; while some show specific anxious or depressive symptoms, others simultaneously experience both of the psychiatric conditions. However, each individual might respond differently thanks to different innate predispositions to handle the disease condition encountered [35].
In our systematic review and meta-analysis, data were collected from five studies [28,29,30,31,32] enrolling a total of 6317 cancer patients, of whom 2961 were females and 3356 males. For each study, HADS-A and HADS-D scores were considered, HADS scores were differentiated according to cancer typology, and then three different meta-analyses were performed. Generally, females reported significantly higher levels of depression scores than males and, conversely, males reported significantly greater levels of anxiety than females. Our data partially agreed with the Götze et al. study [36], in which moderate-to-severe depression and anxiety levels were reported in 17% and 9% of cancer survivors, with significant differences between females and males, since there were higher depression and anxiety levels (p < 0.001). Even Mitchell et al. highlighted a frequency of 17.9% for anxiety and 11.6% for depression among long-term cancer survivors (2 years after “any” cancer diagnosis) [8]. Linden et al. [37] showed that younger females registered more clinical and sub-clinical conditions of anxiety and depression than other patients, who better managed their emotions after their cancer diagnosis. Additionally, van’t Spijker et al.’s findings [38] suggested that females recorded lower rates of emotional distress, especially among female cancer patients recording higher prevalence rates of anxiety and depression than males. These data were in agreement with the high rates of anxiety and depression among healthy females compared to males [39]. This sex difference appeared to be in accordance with the concept regarding females who adopt emotional-related coping strategies [40,41].
However, as regards the anxiety dimension, our meta-analyzed data suggested that males recorded higher levels in the anxiety dimension than females. These data were in disagreement with the Hasan et al. study [34] in which females suffering from gynecological, hematological, head and neck, and lung cancers recorded significant higher levels of anxiety.
Moreover, anxiety could be positively associated with mental disengagement, negation, and requiring emotional social helping. In this regard, anxiety also showed a comparable association with a positive explanation, attitudinal detachment, and requiring emotional social support [42]. By considering the depression condition, our data could be explained by Hasan et al.’s study (2020), since depressed males could be positively correlated with mental disengagement and requiring social and emotional supports. In females, depression was positively correlated with behavioral detachment as well as negation [42]. However, by considering cancer typology, our meta-analysis showed that males recorded significantly higher values in the anxiety condition than females, in gastrointestinal, hematologic, and thyroid cancers. On the other hand, this trend seemed to be dissimilar when considering the depression condition, as in both gastrointestinal and thyroid cancer typologies, females recorded significantly higher values in the depression condition than males. This difference seemed to be overlaid by considering the hematologic cancer typology, since the overall effect did not show any significant difference between the two sexes. In this regard, previous studies highlighted several elements impacting on the anxiety and depression prevalence among cancer patients. However, very limited evidence was available among gastric cancer patients [43]. In this regard, Nordin et al. [44] reported 17% of gastrointestinal patients suffering from anxiety and 21% from depression overall [45,46]. Among hematologic cancer patients, Kuba et al. [47] reported significant differences in anxious and depressive symptomatologies. However, they did not consider sex-related differences. On the other hand, patients suffering from thyroid cancer experienced high levels of distress and worry, despite having a good prognosis, and reported more anxiety and depression rates than the other cancer typologies [48]. Further epidemiological studies [49,50] highlighted a positive association between anxiety and sex and age. However, our data were inconsistent with the current literature, since males reported significantly higher levels in the anxiety condition, and, for example, Noto et al. [51] considered female sex as a predictor for anxiety in thyroid cancer survivors.
Strengths and Limitations
The present study showed interesting findings in sex-related differences in anxiety and depression conditions. The literature data collected were dated from 2007 to 2021, highlighting the necessity of an additional study to bring this up to date in the next few years. We also tried to consider age, and all the participants included in our screened manuscripts were aged between 19 and 92 years.
However, another variable which will be considered in future studies is whether or not cancer patients were followed by a psychological/psychiatric service to better investigate how cancer patients are accomplished in their care pathways in cancer disease. Another limit could be that screening for anxiety or depression at the diagnosis communication stage could be very different from a chronic condition, too.
5. Conclusions
Since previous studies suggested higher rates in the depression and anxiety conditions among females than in males, the present data highlighted controversial findings, since males reported significantly higher levels of anxiety than females.
In this scenario, the theoretical approach [52] justified females being more open than males to expressing anxiety or depression conditions. In addition, males seemed to have more difficulties in expressing their emotions or in requiring assistance. In fact, they tended to experience more different symptoms associated with stress conditions, such as anger, obsession, and hostility. Hegemonic masculinity could be explained as a potential cause that could hinder males to require psychological support, in opposition to females who have always required psychological support [53]. In this scenario, the progression of depression and anxiety generally seemed to be more inclined to females and commonly underestimated in males [54]. In this scenario, it would be necessary for healthcare professionals to improve effective measures purposed at assessing and mitigating depressive symptoms in cases of advanced cancer, thereby improving their mental health, given the high rates of depression in advanced cancer patients [55,56,57], due to the difficulty level in performing their daily living activities [58], which deteriorate further over time [59].
Supplementary Materials
The following supporting information can be downloaded at https://www.mdpi.com/article/10.3390/cancers16111969/s1, File S1: Search strings carried out to perform this systematic and meta-analysis study.
Author Contributions
Conceptualization, E.V. and A.M.; methodology, E.V., K.H. and A.S.; formal analysis, K.H. and A.S.; investigation, E.V., K.H. and Y.-C.C.; resources, E.V., K.H. and R.M.; data curation, E.V. and W.-Y.H.; writing—original draft preparation, E.V.; writing—review and editing, E.V.; visualization and supervision, E.V. and A.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are available upon reasonable request to the corresponding author. Figures and tables within the manuscript are original.
Conflicts of Interest
The authors declare no conflicts of interest.
Additional Disclosure
The authors affiliated to the IRCCS Istituto Tumori “Giovanni Paolo II”, Bari are responsible for the views expressed in this article, which do not necessarily represent the Institute.
References
- World Health Organization (WHO). Cancers. 2020. Available online: https://www.who.int/news (accessed on 12 February 2024).
- Powe, B.D.; Finnie, R. Cancer fatalism: The state of the science. Cancer Nurs. 2003, 26, 454–467. [Google Scholar] [CrossRef] [PubMed]
- Naus, M.J.; Ishler, M.D.; Parrott, C.E.; Kovacs, S.A. Cancer survivor adaptation model: Conceptualizing cancer as a chronic illness. J. Clin. Psychol. 2009, 65, 1350–1359. [Google Scholar] [CrossRef] [PubMed]
- VanHoose, L.; Black, L.L.; Doty, K.; Sabata, D.; Twumasi-Ankrah, P.; Taylor, S.; Johnson, R. An analysis of the distress thermometer problem list and distress in patients with cancer. Support. Care Cancer 2015, 23, 1225–1232. [Google Scholar] [CrossRef] [PubMed]
- Aass, N.; Fosså, S.D.; Dahl, A.A.; Moe, T.J. Prevalence of anxiety and depression in cancer patients seen at the Norwegian Radium Hospital. Eur. J. Cancer 1997, 33, 1597–1604. [Google Scholar] [CrossRef]
- Ford, S.; Lewis, S.; Fallowfield, L. Psychological morbidity in newly referred patients with cancer. J. Psychosom. Res. 1995, 39, 193–202. [Google Scholar] [CrossRef] [PubMed]
- Bultz, B.D.; Carlson, L.E. Emotional distress: The sixth vital sign in cancer care. J. Clin. Oncol. 2005, 23, 6440–6441. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, A.J.; Chan, M.; Bhatti, H.; Halton, M.; Grassi, L.; Johansen, C.; Meader, N. Prevalence of depression, anxiety, and adjustment disorder in oncological, haematological, and palliative-care settings: A meta-analysis of 94 interview-based studies. Lancet Oncol. 2011, 12, 160–174. [Google Scholar] [CrossRef] [PubMed]
- Andersen, B.L.; DeRubeis, R.J.; Berman, B.S.; Gruman, J.; Champion, V.L.; Massie, M.J.; Holland, J.C.; Partridge, A.H.; Bak, K.; Somerfield, M.R.; et al. American Society of Clinical Oncology. Screening, assessment, and care of anxiety and depressive symptoms in adults with cancer: An American Society of Clinical Oncology guideline adaptation. J. Clin. Oncol. 2014, 32, 1605–1619. [Google Scholar] [CrossRef] [PubMed]
- Carlson, L.E.; Waller, A.; Groff, S.L.; Giese-Davis, J.; Bultz, B.D. What goes up does not always come down: Patterns of distress, physical and psychosocial morbidity in people with cancer over a one year period. Psychooncology 2013, 22, 168–176. [Google Scholar] [CrossRef]
- Sanford, S.D.; Beaumont, J.L.; Butt, Z.; Sweet, J.J.; Cella, D.; Wagner, L.I. Prospective longitudinal evaluation of a symptom cluster in breast cancer. J. Pain. Symptom Manag. 2014, 47, 721–730. [Google Scholar] [CrossRef]
- Aarstad, H.J.; Aarstad, A.K.; Heimdal, J.H.; Olofsson, J. Mood, anxiety and sense of humor in head and neck cancer patients in relation to disease stage, prognosis and quality of life. Acta Otolaryngol. 2005, 125, 557–565. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.M.; Wan Ahmad, W.A.; Yusof, M.M.; Ho, G.F.; Krupat, E. Effects of depression and anxiety on mortality in a mixed cancer group: A longitudinal approach using standardised diagnostic interviews. Psychooncology 2015, 24, 718–725. [Google Scholar] [CrossRef] [PubMed]
- King, M.; Semlyen, J.; Tai, S.S.; Killaspy, H.; Osborn, D.; Popelyuk, D.; Nazareth, I. A systematic review of mental disorder, suicide, and deliberate self-harm in lesbian, gay and bisexual people. BMC Psychiatry 2008, 8, 70. [Google Scholar] [CrossRef]
- Mols, F.; Schoormans, D.; de Hingh, I.; Oerlemans, S.; Husson, O. Symptoms of anxiety and depression among colorectal cancer survivors from the population-based, longitudinal PROFILES Registry: Prevalence, predictors, and impact on quality of life. Cancer 2018, 124, 2621–2628. [Google Scholar] [CrossRef] [PubMed]
- Obispo-Portero, B.; Cruz-Castellanos, P.; Jiménez-Fonseca, P.; Rogado, J.; Hernandez, R.; Castillo-Trujillo, O.A.; Asensio-Martínez, E.; González-Moya, M.; Carmona-Bayonas, A.; Calderon, C. Anxiety and depression in patients with advanced cancer during the COVID-19 pandemic. Support. Care Cancer 2022, 30, 3363–3370. [Google Scholar] [CrossRef]
- Abu-Odah, H.; Molassiotis, A.; Yat Wa Liu, J. Analysis of the unmet needs of Palestinian advanced cancer patients and their relationship to emotional distress: Results from a cross-sectional study. BMC Palliat. Care 2022, 21, 72. [Google Scholar] [CrossRef]
- Nguyen, T.; Tracy, K.; Ullah, A.; Karim, N.A. Effect of Exercise Training on Quality of Life, Symptoms, and Functional Status in Advanced-Stage Lung Cancer Patients: A Systematic Review. Clin. Pract. 2023, 13, 715–730. [Google Scholar] [CrossRef]
- Applebaum, A.J.; Stein, E.M.; Lord-Bessen, J.; Pessin, H.; Rosenfeld, B.; Breitbart, W. Optimism, social support, and mental health outcomes in patients with advanced cancer. Psychooncology 2014, 23, 299–306. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef] [PubMed]
- Bjelland, I.; Dahl, A.A.; Haug, T.T.; Neckelmann, D. The validity of the Hospital Anxiety and Depression Scale. An. updated literature review. J. Psychosom. Res. 2002, 52, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Vodermaier, A.; Millman, R.D. Accuracy of the Hospital Anxiety and Depression Scale as a screening tool in cancer patients: A systematic review and meta-analysis. Support Care Cancer 2011, 19, 1899–1908. [Google Scholar] [CrossRef]
- Michopoulos, I.; Douzenis, A.; Kalkavoura, C.; Christodoulou, C.; Michalopoulou, P.; Kalemi, G.; Fineti, K.; Patapis, P.; Protopapas, K.; Lykouras, L. Hospital Anxiety and Depression Scale (HADS): Validation in a Greek general hospital sample. Ann. Gen. Psychiatry 2008, 7, 4. [Google Scholar] [CrossRef] [PubMed]
- Melnyk, B.M.; Gallagher-Ford, L.; Long, L.E.; Fineout-Overholt, E. The establishment of evidence-based practice competencies for practicing registered nurses and advanced practice nurses in real-world clinical settings: Proficiencies to improve healthcare quality, reliability, patient outcomes, and costs. Worldviews Evid. Based Nurs. 2014, 11, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; The Cochrane Collaboration: London, UK, 2008. [Google Scholar]
- Skarstein, J.; Aass, N.; Fosså, S.D.; Skovlund, E.; Dahl, A.A. Anxiety and depression in cancer patients: Relation between the Hospital Anxiety and Depression Scale and the European Organization for Research and Treatment of Cancer Core Quality of Life Questionnaire. J. Psychosom. Res. 2000, 49, 27–34. [Google Scholar] [CrossRef]
- Tavoli, A.; Mohagheghi, M.A.; Montazeri, A.; Roshan, R.; Tavoli, Z.; Omidvari, S. Anxiety and depression in patients with gastrointestinal cancer: Does knowledge of cancer diagnosis matter? BMC Gastroenterol. 2007, 7, 28. [Google Scholar] [CrossRef] [PubMed]
- Moser, M.T.; Künzler, A.; Nussbeck, F.; Bargetzi, M.; Znoj, H.J. Higher emotional distress in female partners of cancer patients: Prevalence and patient-partner interdependencies in a 3-year cohort. Psychooncology 2013, 22, 2693–2701. [Google Scholar] [CrossRef] [PubMed]
- Nipp, R.D.; Greer, J.A.; El-Jawahri, A.; Traeger, L.; Gallagher, E.R.; Park, E.R.; Jackson, V.A.; Pirl, W.F.; Temel, J.S. Age and Sex Moderate the Impact of Early Palliative Care in Metastatic Non-Small Cell Lung Cancer. Oncologist 2016, 21, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Oertelt-Prigione, S.; de Rooij, B.H.; Mols, F.; Oerlemans, S.; Husson, O.; Schoormans, D.; Haanen, J.B.; van de Poll-Franse, L.V. Sex-differences in symptoms and functioning in >5000 cancer survivors: Results from the PROFILES registry. Eur. J. Cancer 2021, 156, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Thapa, S.; Sun, H.; Pokhrel, G.; Wang, B.; Dahal, S.; Yu, S. Performance of distress thermometer and associated factors of psychological distress among Chinese cancer patients. J. Oncol. 2020, 2020, 3293589. [Google Scholar] [CrossRef]
- Hasan, E.M.; Calma, C.L.; Tudor, A.; Oancea, C.; Tudorache, V.; Petrache, I.A.; Tudorache, E.; Papava, I. Coping, Anxiety, and Pain Intensity in Patients Requiring Thoracic Surgery. J. Pers. Med. 2021, 11, 1221. [Google Scholar] [CrossRef]
- Rand, K.L.; Cripe, L.D.; Monahan, P.O.; Tong, Y.; Schmidt, K.; Rawl, S.M. Illness appraisal, religious coping, and psychological responses in men with advanced cancer. Support. Care Cancer 2012, 20, 1719–1728. [Google Scholar] [CrossRef]
- Götze, H.; Friedrich, M.; Taubenheim, S.; Dietz, A.; Lordick, F.; Mehnert, A. Depression and anxiety in long-term survivors 5 and 10 years after cancer diagnosis. Support. Care Cancer 2020, 28, 211–220. [Google Scholar] [CrossRef]
- Linden, W.; Vodermaier, A.; Mackenzie, R.; Greig, D. Anxiety and depression after cancer diagnosis: Prevalence rates by cancer type, Sex, and age. J. Affect. Disord. 2012, 141, 343–351. [Google Scholar] [CrossRef] [PubMed]
- Van’t Spijker, A.; Trijsburg, R.W.; Duivenvoorden, H.J. Psychological sequelae of cancer diagnosis. Psychosom. Med. 1997, 59, 280–293. [Google Scholar] [CrossRef]
- Piccinelli, M.; Wilkinson, G. Sex differences in depression. Critical review. Br. J. Psychiatry 2000, 177, 486–492. [Google Scholar] [CrossRef] [PubMed]
- Goldzweig, G.; Andritsch, E.; Hubert, A.; Walach, N.; Perry, S.; Brenner, B.; Baider, L. How relevant is marital status and Sex variables in coping with colorectal cancer? A sample of middle-aged and older cancer survivors. Psychooncology 2009, 18, 866–874. [Google Scholar] [CrossRef] [PubMed]
- Jacobs-Lawson, J.M.; Schumacher, M.M.; Hughes, T.; Arnold, S. Sex differences in psychosocial responses to lung cancer. Gend. Med. 2010, 7, 137–148. [Google Scholar] [CrossRef] [PubMed]
- Hasan, E.M.; Calma, C.L.; Tudor, A.; Vernic, C.; Palade, E.; Tudorache, E.; Oancea, C.; Papava, I. Sex Differences in Coping, Depression, and Anxiety in Patients with Non-Metastatic Lung Cancer. Cancer Manag. Res. 2022, 14, 2041–2052. [Google Scholar] [CrossRef]
- Zhang, L. Anxiety and depression in recurrent gastric cancer: Their prevalence and independent risk factors analyses. Medicine 2021, 100, e28358. [Google Scholar] [CrossRef] [PubMed]
- Nordin, K.; Glimelius, B. Reactions to gastrointestinal cancer--variation in mental adjustment and emotional well-being over time in patients with different prognoses. Psychooncology 1998, 7, 413–423. [Google Scholar] [CrossRef]
- Nordin, K.; Glimelius, B.; Påhlman, L.; Sjödén, P.O. Anxiety, depression and worry in gastrointestinal cancer patients attending medical follow-up control visits. Acta Oncol. 1996, 35, 411–416. [Google Scholar] [CrossRef]
- Nordin, K.; Glimelius, B. Psychological reactions in newly diagnosed gastrointestinal cancer patients. Acta Oncol. 1997, 36, 803–810. [Google Scholar] [CrossRef] [PubMed]
- Kuba, K.; Esser, P.; Mehnert, A.; Hinz, A.; Johansen, C.; Lordick, F.; Götze, H. Risk for depression and anxiety in long-term survivors of hematologic cancer. Health Psychol. 2019, 38, 187–195. [Google Scholar] [CrossRef] [PubMed]
- Buchmann, L.; Ashby, S.; Cannon, R.B.; Hunt, J.P. Psychosocial distress in patients with thyroid cancer. Otolaryngol. Head. Neck Surg. 2015, 152, 644–649. [Google Scholar] [CrossRef] [PubMed]
- Stordal, E.; Mykletun, A.; Dahl, A.A. The association between age and depression in the general population: A multivariate examination. Acta Psychiatr. Scand. 2003, 107, 132–141. [Google Scholar] [CrossRef] [PubMed]
- Seedat, S.; Scott, K.M.; Angermeyer, M.C.; Berglund, P.; Bromet, E.J.; Brugha, T.S.; Demyttenaere, K.; de Girolamo, G.; Haro, J.M.; Jin, R.; et al. Cross-national associations between Sex and mental disorders in the World Health Organization World Mental Health Surveys. Arch. Gen. Psychiatry 2009, 66, 785–795. [Google Scholar] [CrossRef]
- Noto, B.; Asmus, I.; Schäfers, M.; Görlich, D.; Riemann, B. Predictors of Anxiety and Depression in Differentiated Thyroid Cancer Survivors: Results of a Cross-Sectional Study. Thyroid 2022, 32, 1077–1085. [Google Scholar] [CrossRef] [PubMed]
- Sammarco, A.; Konecny, L.M. Quality of life, social support, and uncertainty among Latina breast cancer survivors. Oncol. Nurs. Forum. 2008, 35, 844–849. [Google Scholar] [CrossRef] [PubMed]
- Rassoulian, A.; Gaiger, A.; Loeffler-Stastka, H. Sex differences in psychosocial, religious, and spiritual aspects in coping: A cross-sectional study with cancer patients. Women’s Health Rep. 2021, 2, 464–472. [Google Scholar] [CrossRef] [PubMed]
- Henrich, M.K.G. Illness-related distress: Does it mean the same for men and women?: Sex aspects in cancer patients’ distress and adjustment. Acta Oncol. 1999, 38, 747–755. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.; Ryu, E. Effects of symptom clusters and depression on the quality of life in patients with advanced lung cancer. Eur. J. Cancer Care 2018, 27, e12508. [Google Scholar] [CrossRef] [PubMed]
- Obispo, B.; Cruz-Castellanos, P.; Hernandez, R.; Gil-Raga, M.; González-Moya, M.; Rogado, J.; López-Ceballos, H.; García-Carrasco, M.; Jiménez-Fonseca, P.; Calderon, C. Perceived Dignity of Advanced Cancer Patients and Its Relationship to Sociodemographic, Clinical, and Psychological Factors. Front. Psychol. 2022, 13, 855704. [Google Scholar] [CrossRef] [PubMed]
- Lam, W.W.; Soong, I.; Yau, T.K.; Wong, K.Y.; Tsang, J.; Yeo, W.; Suen, J.; Ho, W.M.; Sze, W.K.; Ng, A.W.; et al. The evolution of psychological distress trajectories in women diagnosed with advanced breast cancer: A longitudinal study. Psychooncology 2013, 22, 2831–2839. [Google Scholar] [CrossRef] [PubMed]
- Neo, J.; Fettes, L.; Gao, W.; Higginson, I.J.; Maddocks, M. Disability in activities of daily living among adults with cancer: A systematic review and meta-analysis. Cancer Treat. Rev. 2017, 61, 94–106. [Google Scholar] [CrossRef] [PubMed]
- Granger, C.L.; McDonald, C.F.; Irving, L.; Clark, R.A.; Gough, K.; Murnane, A.; Mileshkin, L.; Krishnasamy, M.; Denehy, L. Low physical activity levels and functional decline in individuals with lung cancer. Lung Cancer 2014, 83, 292–299. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).