
Microsatellite Instability Testing and Prognostic Implications in Colorectal Cancer

 ,
,  , , , , ,
, , , , ,  ,
, 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Overview and Sample Selection
2.2. FFPE Tissue Processing and DNA Extraction
2.3. Bio-Rad ddPCR MSI Assay
2.4. IHC for MMR Proteins
2.5. Statistical Analysis and Data Acquisition
3. Results
3.1. Study Population
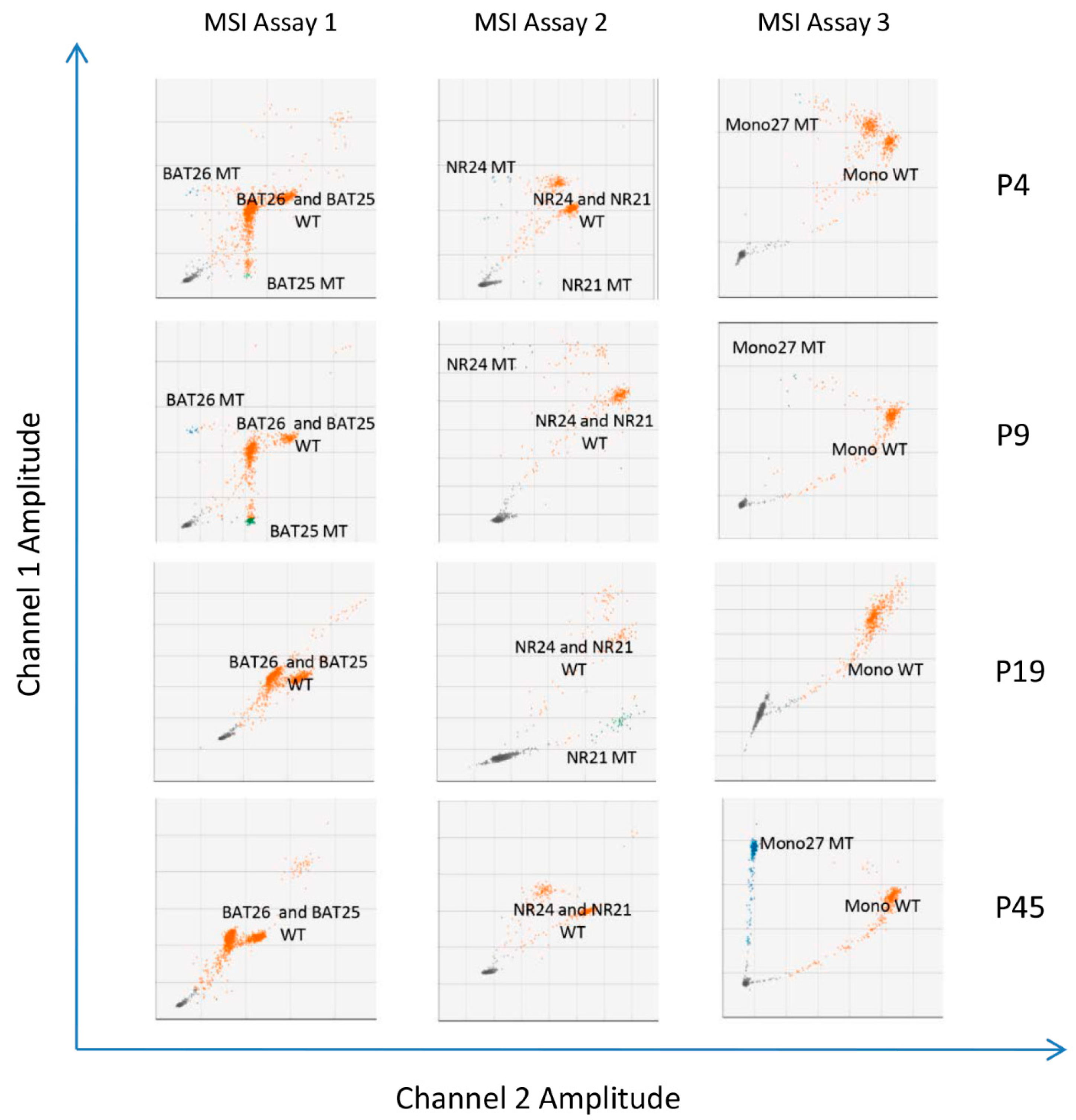
3.2. Concordance between Routine IHC and MSI Testing by ddPCR
3.3. Association between MSI Status and Clinicopathological Features
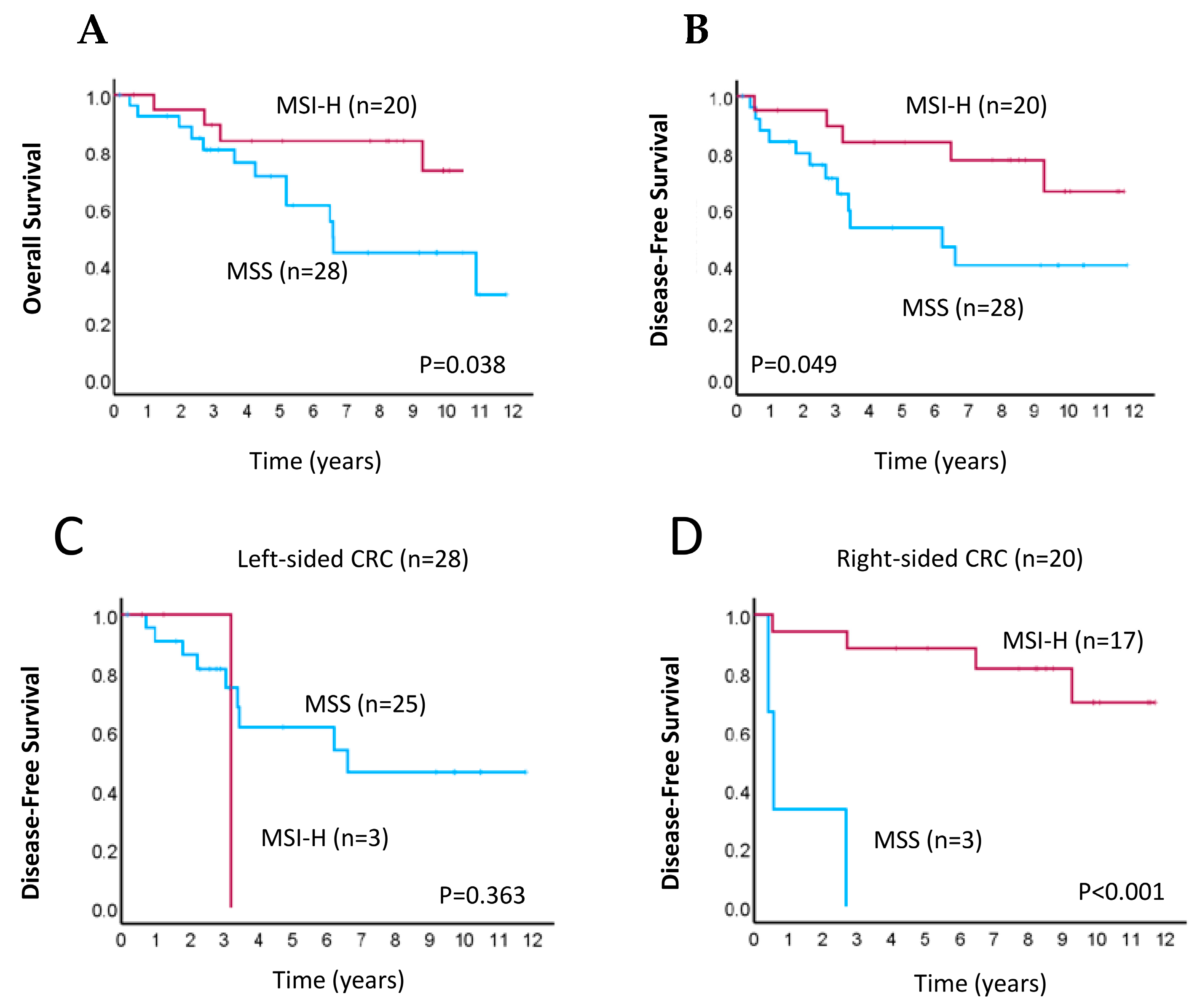
3.4. Prognostic Implications of MSI Status Determined by ddPCR in CRC
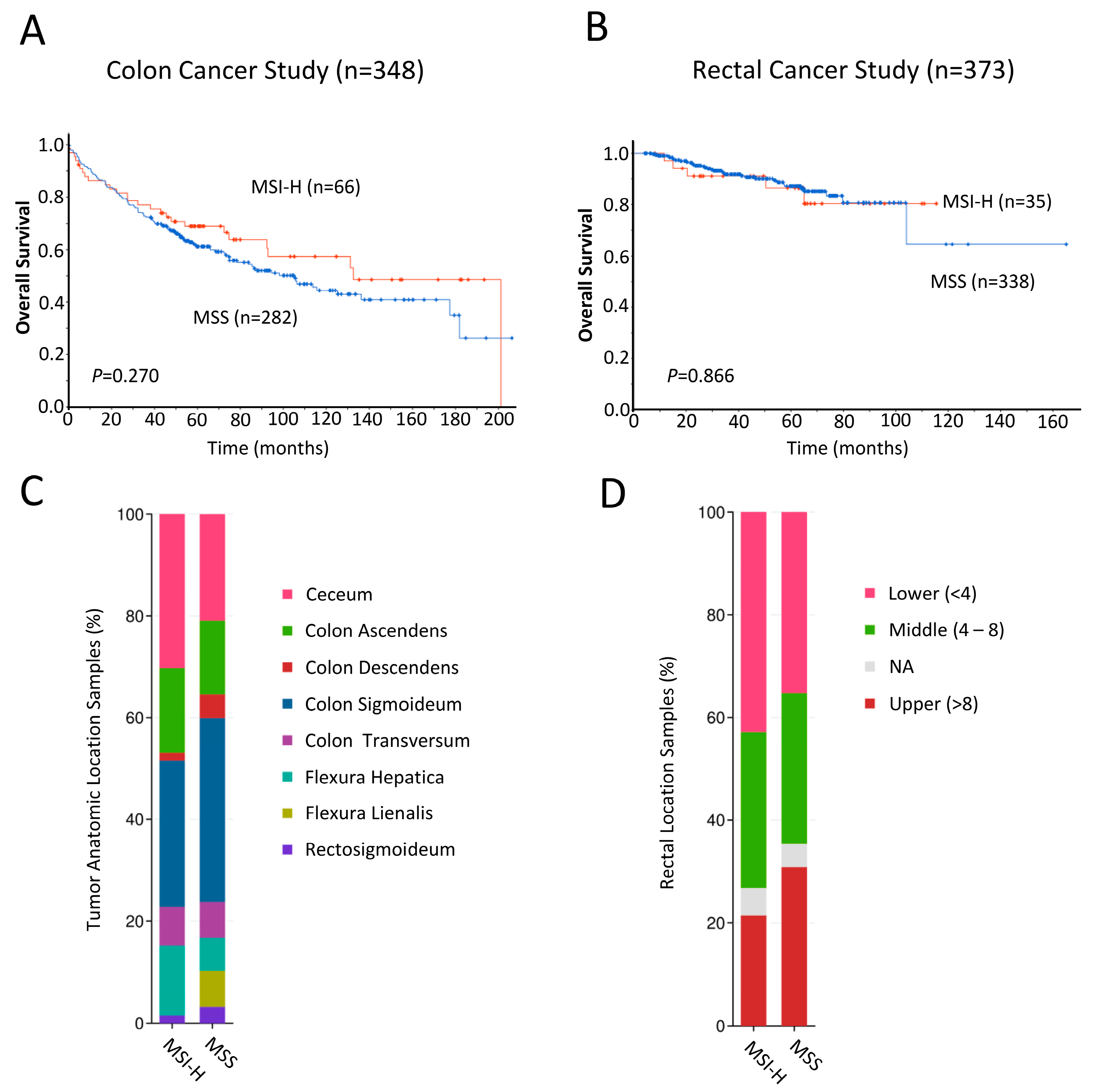
3.5. Clinical Significance of MSI in CRC Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vilar, E.; Gruber, S.B. Microsatellite Instability in Colorectal Cancer—The Stable Evidence. Nat. Rev. Clin. Oncol. 2010, 7, 153–162. [Google Scholar] [CrossRef]
- Kinzler, K.W. The Genetic Basis of Human Cancer; McGraw-Hill Professional Publishing: New York, NY, USA, 2002. [Google Scholar]
- Hendriks, Y.M.C.; de Jong, A.E.; Morreau, H.; Tops, C.M.J.; Vasen, H.F.; Wijnen, J.T.; Breuning, M.H.; Bröcker-Vriends, A.H.J.T. Diagnostic Approach and Management of Lynch Syndrome (Hereditary Nonpolyposis Colorectal Carcinoma): A Guide for Clinicians. CA Cancer J. Clin. 2006, 56, 213–225. [Google Scholar] [CrossRef]
- Lynch, H.T.; Lynch, P.M.; Lanspa, S.J.; Snyder, C.L.; Lynch, J.F.; Boland, C.R. Review of the Lynch Syndrome: History, Molecular Genetics, Screening, Differential Diagnosis, and Medicolegal Ramifications. Clin. Genet. 2009, 76, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Boland, C.R.; Goel, A. Microsatellite Instability in Colorectal Cancer. Gastroenterology 2010, 138, 2073–2087.e3. [Google Scholar] [CrossRef]
- Abu-Ghazaleh, N.; Kaushik, V.; Gorelik, A.; Jenkins, M.; Macrae, F. Worldwide Prevalence of Lynch Syndrome in Patients with Colorectal Cancer: Systematic Review and Meta-Analysis. Genet. Med. 2022, 24, 971–985. [Google Scholar] [CrossRef]
- Vasen, H.F.; Watson, P.; Mecklin, J.P.; Lynch, H.T. New Clinical Criteria for Hereditary Nonpolyposis Colorectal Cancer (HNPCC, Lynch Syndrome) Proposed by the International Collaborative Group on HNPCC. Gastroenterology 1999, 116, 1453–1456. [Google Scholar] [CrossRef]
- Umar, A.; Boland, C.R.; Terdiman, J.P.; Syngal, S.; de la Chapelle, A.; Rüschoff, J.; Fishel, R.; Lindor, N.M.; Burgart, L.J.; Hamelin, R.; et al. Revised Bethesda Guidelines for Hereditary Nonpolyposis Colorectal Cancer (Lynch Syndrome) and Microsatellite Instability. J. Natl. Cancer Inst. 2004, 96, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Vasen, H.F.A.; Blanco, I.; Aktan-Collan, K.; Gopie, J.P.; Alonso, A.; Aretz, S.; Bernstein, I.; Bertario, L.; Burn, J.; Capella, G.; et al. Revised Guidelines for the Clinical Management of Lynch Syndrome (HNPCC): Recommendations by a Group of European Experts. Gut 2013, 62, 812–823. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, J.L.; Lan, L.; Zou, L. DNA Repair Defects in Cancer and Therapeutic Opportunities. Genes Dev. 2022, 36, 278–293. [Google Scholar] [CrossRef]
- Jenkins, M.A.; Hayashi, S.; O’shea, A.-M.; Burgart, L.J.; Smyrk, T.C.; Shimizu, D.; Waring, P.M.; Ruszkiewicz, A.R.; Pollett, A.F.; Redston, M.; et al. Pathology Features in Bethesda Guidelines Predict Colorectal Cancer Microsatellite Instability: A Population-Based Study. Gastroenterology 2007, 133, 48–56. [Google Scholar] [CrossRef]
- Han, S.A.; Kim, J.H.; Choi, J.H.; Lee, D.H.; Jung, K.; Kim, S.E.; Moon, W.; Park, M.I.; Park, S.J. The Clinical Significance of Microsatellite Instability in Patients with Right-Sided Colorectal Cancer. Korean J. Gastroenterol. 2019, 73, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Flecchia, C.; Zaanan, A.; Lahlou, W.; Basile, D.; Broudin, C.; Gallois, C.; Pilla, L.; Karoui, M.; Manceau, G.; Taieb, J. MSI Colorectal Cancer, All You Need to Know. Clin. Res. Hepatol. Gastroenterol. 2022, 46, 101983. [Google Scholar] [CrossRef] [PubMed]
- Samowitz, W.S.; Curtin, K.; Ma, K.N.; Schaffer, D.; Coleman, L.W.; Leppert, M.; Slattery, M.L. Microsatellite Instability in Sporadic Colon Cancer Is Associated with an Improved Prognosis at the Population Level. Cancer Epidemiol. Biomarkers Prev. 2001, 10, 917–923. [Google Scholar] [PubMed]
- Sinicrope, F.A.; Rego, R.L.; Halling, K.C.; Foster, N.; Sargent, D.J.; La Plant, B.; French, A.J.; Laurie, J.A.; Goldberg, R.M.; Thibodeau, S.N.; et al. Prognostic Impact of Microsatellite Instability and DNA Ploidy in Human Colon Carcinoma Patients. Gastroenterology 2006, 131, 729–737. [Google Scholar] [CrossRef] [PubMed]
- Popat, S.; Hubner, R.; Houlston, R.S. Systematic Review of Microsatellite Instability and Colorectal Cancer Prognosis. J. Clin. Oncol. 2005, 23, 609–618. [Google Scholar] [CrossRef] [PubMed]
- Guastadisegni, C.; Colafranceschi, M.; Ottini, L.; Dogliotti, E. Microsatellite Instability as a Marker of Prognosis and Response to Therapy: A Meta-Analysis of Colorectal Cancer Survival Data. Eur. J. Cancer 2010, 46, 2788–2798. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.; Na, Y.; Joung, S.Y.; Lee, S.I.; Oh, S.C.; Min, B.W. The Significance of Microsatellite Instability in Colorectal Cancer after Controlling for Clinicopathological Factors. Medicine 2018, 97, e0019. [Google Scholar] [CrossRef] [PubMed]
- Drescher, K.M.; Sharma, P.; Watson, P.; Gatalica, Z.; Thibodeau, S.N.; Lynch, H.T. Lymphocyte Recruitment into the Tumor Site Is Altered in Patients with MSI-H Colon Cancer. Fam. Cancer 2009, 8, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Fallik, D.; Borrini, F.; Boige, V.; Viguier, J.; Jacob, S.; Miquel, C.; Sabourin, J.-C.; Ducreux, M.; Praz, F. Microsatellite Instability Is a Predictive Factor of the Tumor Response to Irinotecan in Patients with Advanced Colorectal Cancer. Cancer Res. 2003, 63, 5738–5744. [Google Scholar]
- Bertagnolli, M.M.; Niedzwiecki, D.; Compton, C.C.; Hahn, H.P.; Hall, M.; Damas, B.; Jewell, S.D.; Mayer, R.J.; Goldberg, R.M.; Saltz, L.B.; et al. Microsatellite Instability Predicts Improved Response to Adjuvant Therapy with Irinotecan, Fluorouracil, and Leucovorin in Stage III Colon Cancer: Cancer and Leukemia Group B Protocol 89803. J. Clin. Oncol. 2009, 27, 1814–1821. [Google Scholar] [CrossRef]
- Le, D.T.; Uram, J.N.; Wang, H.; Bartlett, B.R.; Kemberling, H.; Eyring, A.D.; Skora, A.D.; Luber, B.S.; Azad, N.S.; Laheru, D.; et al. PD-1 Blockade in Tumors with Mismatch-Repair Deficiency. N. Engl. J. Med. 2015, 372, 2509–2520. [Google Scholar] [CrossRef] [PubMed]
- Ribic, C.M.; Sargent, D.J.; Moore, M.J.; Thibodeau, S.N.; French, A.J.; Goldberg, R.M.; Hamilton, S.R.; Laurent-Puig, P.; Gryfe, R.; Shepherd, L.E.; et al. Tumor Microsatellite-Instability Status as a Predictor of Benefit from Fluorouracil-Based Adjuvant Chemotherapy for Colon Cancer. N. Engl. J. Med. 2003, 349, 247–257. [Google Scholar] [CrossRef]
- Jover, R.; Zapater, P.; Castells, A.; Llor, X.; Andreu, M.; Cubiella, J.; Balaguer, F.; Sempere, L.; Xicola, R.M.; Bujanda, L.; et al. The Efficacy of Adjuvant Chemotherapy with 5-Fluorouracil in Colorectal Cancer Depends on the Mismatch Repair Status. Eur. J. Cancer 2009, 45, 365–373. [Google Scholar] [CrossRef] [PubMed]
- Sargent, D.J.; Marsoni, S.; Monges, G.; Thibodeau, S.N.; Labianca, R.; Hamilton, S.R.; French, A.J.; Kabat, B.; Foster, N.R.; Torri, V.; et al. Defective Mismatch Repair As a Predictive Marker for Lack of Efficacy of Fluorouracil-Based Adjuvant Therapy in Colon Cancer. J. Clin. Oncol. 2010, 28, 3219–3226. [Google Scholar] [CrossRef] [PubMed]
- Luchini, C.; Bibeau, F.; Ligtenberg, M.J.L.; Singh, N.; Nottegar, A.; Bosse, T.; Miller, R.; Riaz, N.; Douillard, J.-Y.; Andre, F.; et al. ESMO Recommendations on Microsatellite Instability Testing for Immunotherapy in Cancer, and Its Relationship with PD-1/PD-L1 Expression and Tumour Mutational Burden: A Systematic Review-Based Approach. Ann. Oncol. 2019, 30, 1232–1243. [Google Scholar] [CrossRef] [PubMed]
- Lindor, N.M.; Burgart, L.J.; Leontovich, O.; Goldberg, R.M.; Cunningham, J.M.; Sargent, D.J.; Walsh-Vockley, C.; Petersen, G.M.; Walsh, M.D.; Leggett, B.A.; et al. Immunohistochemistry versus Microsatellite Instability Testing in Phenotyping Colorectal Tumors. J. Clin. Oncol. 2002, 20, 1043–1048. [Google Scholar] [CrossRef] [PubMed]
- Boland, C.R.; Thibodeau, S.N.; Hamilton, S.R.; Sidransky, D.; Eshleman, J.R.; Burt, R.W.; Meltzer, S.J.; Rodriguez-Bigas, M.A.; Fodde, R.; Ranzani, G.N.; et al. A National Cancer Institute Workshop on Microsatellite Instability for Cancer Detection and Familial Predisposition: Development of International Criteria for the Determination of Microsatellite Instability in Colorectal Cancer. Cancer Res. 1998, 58, 5248–5257. [Google Scholar] [PubMed]
- Goel, A.; Nagasaka, T.; Hamelin, R.; Boland, C.R. An Optimized Pentaplex PCR for Detecting DNA Mismatch Repair-Deficient Colorectal Cancers. PLoS ONE 2010, 5, e9393. [Google Scholar] [CrossRef] [PubMed]
- Suraweera, N.; Duval, A.; Reperant, M.; Vaury, C.; Furlan, D.; Leroy, K.; Seruca, R.; Iacopetta, B.; Hamelin, R. Evaluation of Tumor Microsatellite Instability Using Five Quasimonomorphic Mononucleotide Repeats and Pentaplex PCR. Gastroenterology 2002, 123, 1804–1811. [Google Scholar] [CrossRef]
- Gilson, P.; Levy, J.; Rouyer, M.; Demange, J.; Husson, M.; Bonnet, C.; Salleron, J.; Leroux, A.; Merlin, J.-L.; Harlé, A. Evaluation of 3 Molecular-Based Assays for Microsatellite Instability Detection in Formalin-Fixed Tissues of Patients with Endometrial and Colorectal Cancers. Sci. Rep. 2020, 10, 16386. [Google Scholar] [CrossRef]
- Roelands, J.; Kuppen, P.J.K.; Ahmed, E.I.; Mall, R.; Masoodi, T.; Singh, P.; Monaco, G.; Raynaud, C.; de Miranda, N.F.C.C.; Ferraro, L.; et al. An Integrated Tumor, Immune and Microbiome Atlas of Colon Cancer. Nat. Med. 2023, 29, 1273–1286. [Google Scholar] [CrossRef]
- Chatila, W.K.; Kim, J.K.; Walch, H.; Marco, M.R.; Chen, C.-T.; Wu, F.; Omer, D.M.; Khalil, D.N.; Ganesh, K.; Qu, X.; et al. Genomic and Transcriptomic Determinants of Response to Neoadjuvant Therapy in Rectal Cancer. Nat. Med. 2022, 28, 1646–1655. [Google Scholar] [CrossRef] [PubMed]
- de’Angelis Gian, L.; Lorena, B.; Cinzia, A.; de’Angelis, N.; Gioacchino, L.; Francesco, D.M.; Federica, G.; Francesca, N. Microsatellite Instability in Colorectal Cancer. Acta Biomed. 2018, 89, 97–101. [Google Scholar] [CrossRef]
- Hindson, B.J.; Ness, K.D.; Masquelier, D.A.; Belgrader, P.; Heredia, N.J.; Makarewicz, A.J.; Bright, I.J.; Lucero, M.Y.; Hiddessen, A.L.; Legler, T.C.; et al. High-Throughput Droplet Digital PCR System for Absolute Quantitation of DNA Copy Number. Anal. Chem. 2011, 83, 8604–8610. [Google Scholar] [CrossRef] [PubMed]
- Droplet Digital PCR (ddPCR) Technology|Bio-Rad. Available online: https://www.bio-rad.com/en-us/life-science/learning-center/introduction-to-digital-pcr/what-is-droplet-digital-pcr (accessed on 21 February 2024).
- Zhang, P.; Wang, A.; Bian, C.; Zhang, J.; Jiang, C.; Zhou, H. Evaluation of mismatch-repair and microsatellite-instability status in a Chinese colorectal cancer Cohort. Asian J. Surg. 2024, 47, 959–967. [Google Scholar] [CrossRef]
- Shen, H.; Yang, J.; Huang, Q.; Jiang, M.-J.; Tan, Y.-N.; Fu, J.-F.; Zhu, L.-Z.; Fang, X.-F.; Yuan, Y. Different Treatment Strategies and Molecular Features between Right-Sided and Left-Sided Colon Cancers. World J. Gastroenterol. 2015, 21, 6470–6478. [Google Scholar] [CrossRef] [PubMed]
- Glebov, O.K.; Rodriguez, L.M.; Nakahara, K.; Jenkins, J.; Cliatt, J.; Humbyrd, C.-J.; DeNobile, J.; Soballe, P.; Simon, R.; Wright, G.; et al. Distinguishing Right from Left Colon by the Pattern of Gene Expression. Cancer Epidemiol. Biomark. Prev. 2003, 12, 755–762. [Google Scholar]
- Muzny, D.M.; Bainbridge, M.N.; Chang, K.; Dinh, H.H.; Drummond, J.A.; Fowler, G.; Kovar, C.L.; Lewis, L.R.; Morgan, M.B.; Newsham, I.F.; et al. Comprehensive Molecular Characterization of Human Colon and Rectal Cancer. Nature 2012, 487, 330–337. [Google Scholar] [CrossRef]
- Koestler, D.C.; Li, J.; Baron, J.A.; Tsongalis, G.J.; Butterly, L.F.; Goodrich, M.; Lesseur, C.; Karagas, M.R.; Marsit, C.J.; Moore, J.H.; et al. Distinct Patterns of DNA Methylation in Conventional Adenomas Involving the Right and Left Colon. Mod. Pathol 2014, 27, 145–155. [Google Scholar] [CrossRef]
- Missiaglia, E.; Jacobs, B.; D’Ario, G.; Di Narzo, A.F.; Soneson, C.; Budinska, E.; Popovici, V.; Vecchione, L.; Gerster, S.; Yan, P.; et al. Distal and Proximal Colon Cancers Differ in Terms of Molecular, Pathological, and Clinical Features. Ann. Oncol. 2014, 25, 1995–2001. [Google Scholar] [CrossRef]
- Brulé, S.Y.; Jonker, D.J.; Karapetis, C.S.; O’Callaghan, C.J.; Moore, M.J.; Wong, R.; Tebbutt, N.C.; Underhill, C.; Yip, D.; Zalcberg, J.R.; et al. Location of Colon Cancer (Right-Sided versus Left-Sided) as a Prognostic Factor and a Predictor of Benefit from Cetuximab in NCIC CO.17. Eur. J. Cancer 2015, 51, 1405–1414. [Google Scholar] [CrossRef] [PubMed]
- Baran, B.; Mert Ozupek, N.; Yerli Tetik, N.; Acar, E.; Bekcioglu, O.; Baskin, Y. Difference Between Left-Sided and Right-Sided Colorectal Cancer: A Focused Review of Literature. Gastroenterol. Res. 2018, 11, 264–273. [Google Scholar] [CrossRef] [PubMed]
- Carethers, J.M. One Colon Lumen but Two Organs. Gastroenterology 2011, 141, 411–412. [Google Scholar] [CrossRef] [PubMed]
- Weiss, J.M.; Pfau, P.R.; O’Connor, E.S.; King, J.; LoConte, N.; Kennedy, G.; Smith, M.A. Mortality by Stage for Right- versus Left-Sided Colon Cancer: Analysis of Surveillance, Epidemiology, and End Results—Medicare Data. J. Clin. Oncol. 2011, 29, 4401–4409. [Google Scholar] [CrossRef] [PubMed]
- Herman, J.G.; Umar, A.; Polyak, K.; Graff, J.R.; Ahuja, N.; Issa, J.-P.J.; Markowitz, S.; Willson, J.K.V.; Hamilton, S.R.; Kinzler, K.W.; et al. Incidence and Functional Consequences of hMLH1 Promoter Hypermethylation in Colorectal Carcinoma. Proc. Natl. Acad. Sci. USA 1998, 95, 6870–6875. [Google Scholar] [CrossRef] [PubMed]
- Weisenberger, D.J.; Siegmund, K.D.; Campan, M.; Young, J.; Long, T.I.; Faasse, M.A.; Kang, G.H.; Widschwendter, M.; Weener, D.; Buchanan, D.; et al. CpG Island Methylator Phenotype Underlies Sporadic Microsatellite Instability and Is Tightly Associated with BRAF Mutation in Colorectal Cancer. Nat. Genet. 2006, 38, 787–793. [Google Scholar] [CrossRef] [PubMed]
- Carethers, J.M. Hereditary, sporadic and metastatic colorectal cancer are commonly driven by specific spectrums of defective dna mismatch repair components. Trans. Am. Clin. Climatol. Assoc. 2016, 127, 81–97. [Google Scholar]
- Liu, G.-C.; Liu, R.-Y.; Yan, J.-P.; An, X.; Jiang, W.; Ling, Y.-H.; Chen, J.-W.; Bei, J.-X.; Zuo, X.-Y.; Cai, M.-Y.; et al. The Heterogeneity Between Lynch-Associated and Sporadic MMR Deficiency in Colorectal Cancers. JNCI J. Natl. Cancer Inst. 2018, 110, 975–984. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinicopathological Characteristics | Number of Patients |
|---|---|
| Age median/patients | 67/48 |
| <67 | 26 (54.2%) |
| ≥67 | 22 (45.8%) |
| Sex | |
| Male | 26 (54.2%) |
| Female | 22 (45.8%) |
| Tumor stage | |
| T1, T2 | 11 (22.9%) |
| T3, T4 | 37 (77.1%) |
| Node stage | |
| N0 | 27 (56.3%) |
| N1, N2 | 21 (43.7%) |
| Metastasis stage | |
| M0 | 47 (97.9%) |
| M1 | 1 (2.1%) |
| Differentiation | |
| Well/moderate | 31 (64.6%) |
| Poor | 17 (35.4%) |
| LVI/PNI | |
| Absent | 38 (79.2%) |
| Present | 10 (20.8%) |
| Primary tumor site | |
| Right-sided | 20 (41.7%) |
| Left-sided | 28 (58.3%) |
| Treatment | |
| Neoadjuvant therapy | |
| No | 22 (45.8%) |
| Yes | 26 (54.2%) |
| Adjuvant therapy | |
| No | 30 (62.5%) |
| Yes | 18 (37.5%) |
| Sample ID | MMR by IHC (Undetectable MMR Proteins) | MSI Testing by Bio-Rad ddPCR MSI Assay |
|---|---|---|
| P1 | pMMR | MSS |
| P2 | dMMR (MLH1, PMS2) | MSI-H |
| P3 | dMMR (MLH1, PMS2) | MSI-H |
| P4 | dMMR (MSH2, MSH6) | MSI-H |
| P5 | pMMR | MSI-L |
| P6 | pMMR | MSS |
| P7 | pMMR | MSS |
| P8 | pMMR | MSS |
| P9 | dMMR (MLH1, PMS2) | MSI-H |
| P10 | dMMR (MLH1, PMS2) | MSI-H |
| P11 | dMMR (MLH1, PMS2) | MSI-H |
| P12 | dMMR (PMS2) | MSI-H |
| P13 | dMMR (MLH1, PMS2) | MSI-H |
| P14 | pMMR | MSS |
| P15 | dMMR (MLH1, PMS2) | MSI-H |
| P16 | dMMR (MLH1, PMS2) | MSI-H |
| P17 | pMMR | MSS |
| P18 | dMMR (MLH1) | MSI-H |
| P19 | dMMR (PMS2) | MSI-L |
| P20 | dMMR (MLH1, PMS2) | MSI-H |
| P21 | dMMR (MLH1, PMS2) | MSI-H |
| P22 | pMMR | MSS |
| P23 | dMMR (MSH2, MSH6) | MSI-H |
| P24 | pMMR | MSS |
| P25 | dMMR (MSH2, MSH6) | MSI-H |
| P26 | pMMR | MSS |
| P27 | pMMR | MSS |
| P28 | pMMR | MSS |
| P29 | dMMR (MLH1) | MSI-H |
| P30 | dMMR (MLH1) | MSI-H |
| P31 | dMMR (MLH1) | MSI-H |
| P32 | dMMR (PMS2) | MSI-H |
| P33 | dMMR (MLH1) | MSI-H |
| P34 | pMMR | MSS |
| P35 | pMMR | MSS |
| P36 | pMMR | MSS |
| P37 | pMMR | MSS |
| P38 | pMMR | MSS |
| P39 | pMMR | MSS |
| P40 | pMMR | MSS |
| P41 | pMMR | MSS |
| P42 | pMMR | MSS |
| P43 | pMMR | MSS |
| P44 | pMMR | MSS |
| P45 | dMMR (MSH6) | MSI-L |
| P46 | pMMR | MSS |
| P47 | pMMR | MSS |
| P48 | pMMR | MSS |
| Bio-Rad ddPCR MSI Assay | |
|---|---|
| Kappa agreement measure (k) | 0.915 |
| p-value | <0.001 |
| Sensitivity % (N) | 90.9% (20/22) |
| Specificity % (N) | 92.9% (26/28) |
| Clinical-Histopathological Features | MSI Testing * | |||
|---|---|---|---|---|
| MSS/MSI-L (%) | MSI-H (%) | p-Value | ||
| Sex | Male | 69.2 | 30.8 | 0.096 |
| Female | 45.5 | 54.5 | ||
| Age | <67 | 65.4 | 34.6 | 0.281 |
| ≥67 | 50.0 | 50.0 | ||
| Tumor stage | T1/2 | 81.8 | 18.2 | 0.072 |
| T3/4 | 51.4 | 48.6 | ||
| Node stage | Negative | 44.4 | 55.6 | 0.027 |
| Positive | 76.2 | 23.8 | ||
| Metastasis stage | M0 | 57.4 | 42.6 | 0.393 |
| M1 | 100 | 0 | ||
| Differentiation | Well/moderate | 67.7 | 32.3 | 0.074 |
| Poor | 41.2 | 58.8 | ||
| LVI/PNI | Absent | 68.4 | 31.6 | 0.006 |
| Present | 20 | 80 | ||
| Adjuvant therapy | No | 45.5 | 54.5 | 0.525 |
| Yes | 55.6 | 44.4 | ||
| Neoadjuvant therapy | No | 18.2 | 81.8 | 0.232 |
| Yes | 92.3 | 7.7 | ||
| MLH1 | Normal IHC | 78.8 | 21.2 | <0.001 |
| Loss of staining | 13.3 | 86.7 | ||
| MSH2 | Normal IHC | 60.5 | 39.5 | 0.380 |
| Loss of staining | 40 | 60 | ||
| MSH6 | Normal IHC | 62.8 | 37.2 | 0.066 |
| Loss of staining | 20 | 80 | ||
| PMS2 | Normal IHC | 70.3 | 29.7 | 0.002 |
| Loss of staining | 18.2 | 81.8 | ||
| Univariate | Multivariate | ||||||
|---|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | ||
| MSI test | MSS | 0.324 | 0.105–0.998 | 0.046 | 0.221 | 0.026–0.870 | 0.042 |
| MSI-H | |||||||
| Sex | Male | 1.190 | 0.445–3.115 | 0.723 | 3.126 | 0.296–32.99 | 0.343 |
| Female | |||||||
| Age | <67 | 1.623 | 0.604–4.636 | 0.337 | 2.314 | 1.576–3.396 | 0.750 |
| ≥67 | |||||||
| Tumor stage | T1/2 | 0.782 | 0.528–1.158 | 0.219 | 0.587 | 0.045–3.720 | 0.428 |
| T3/4 | |||||||
| Node stage | Negative | 1.194 | 0.726–5.043 | 0.189 | 0.537 | 0.045–6.441 | 0.623 |
| Positive | |||||||
| Differentiation | Well /moderate | 1.073 | 0.396–2.906 | 0.890 | 0.954 | 0.904–27.981 | 0.964 |
| Poor | |||||||
| LVI/PNI | Absent | 0.797 | 0.228–2.787 | 0.722 | 1.956 | 0.050–75.891 | 0.719 |
| Present | |||||||
| Adjuvant therapy | No | 0.783 | 0.248–2.496 | 0.676 | 2.415 | 0.184–0.451 | 0.564 |
| Yes | |||||||
| Neoadjuvant therapy | No | 2.408 | 0.885–6.701 | 0.081 | 2.473 | 0.056–7.088 | 0.099 |
| Yes | |||||||
| MLH1 | Normal IHC | 0.222 | 0.050–0.979 | 0.047 | 0.133 | 0.001–1.152 | 0.049 |
| Loss of staining | |||||||
| MSH2 | Normal IHC | 0.466 | 0.061–3.588 | 0.464 | 0.478 | 0.082–4.719 | 0.878 |
| Loss of staining | |||||||
| MSH6 | Normal IHC | 0.717 | 0.320–6.268 | 0.646 | 0.959 | 0.341–8.632 | 0.872 |
| Loss of staining | |||||||
| PMS2 | Normal IHC | 0.666 | 0.190–2.344 | 0.527 | 0.744 | 0.530–9.702 | 0.490 |
| Loss of staining | |||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ho, V.; Chung, L.; Wilkinson, K.; Ma, Y.; Rutland, T.; Lea, V.; Lim, S.H.; Abubakar, A.; Ng, W.; Lee, M.; et al. Microsatellite Instability Testing and Prognostic Implications in Colorectal Cancer. Cancers 2024, 16, 2005. https://doi.org/10.3390/cancers16112005
Ho V, Chung L, Wilkinson K, Ma Y, Rutland T, Lea V, Lim SH, Abubakar A, Ng W, Lee M, et al. Microsatellite Instability Testing and Prognostic Implications in Colorectal Cancer. Cancers. 2024; 16(11):2005. https://doi.org/10.3390/cancers16112005
Chicago/Turabian StyleHo, Vincent, Liping Chung, Kate Wilkinson, Yafeng Ma, Tristan Rutland, Vivienne Lea, Stephanie H. Lim, Askar Abubakar, Weng Ng, Mark Lee, and et al. 2024. "Microsatellite Instability Testing and Prognostic Implications in Colorectal Cancer" Cancers 16, no. 11: 2005. https://doi.org/10.3390/cancers16112005
APA StyleHo, V., Chung, L., Wilkinson, K., Ma, Y., Rutland, T., Lea, V., Lim, S. H., Abubakar, A., Ng, W., Lee, M., Roberts, T. L., Becker, T. M., Mackenzie, S., Chua, W., & Lee, C. S. (2024). Microsatellite Instability Testing and Prognostic Implications in Colorectal Cancer. Cancers, 16(11), 2005. https://doi.org/10.3390/cancers16112005