Simple Summary
Hepatocellular carcinoma (HCC) is a common cancer and a leading cause of cancer-related deaths worldwide. However, HCC can be effectively treated in selected cases, with liver transplantation representing one of the limited options for potential cure. Unfortunately, many patients are ineligible for liver transplantation either due to an advanced tumor at initial diagnosis or due to disease progression while awaiting liver transplantation. Our review discusses the role of systemic therapies as a bridging treatment to liver transplantation, thereby enabling more HCC patients to undergo potentially curative liver transplantation.
Abstract
Hepatocellular carcinoma (HCC) is the third most common cause of cancer-related deaths. Classically, liver transplantation (LT) can be curative for HCC tumors within the Milan criteria. Bridging strategies to reduce the dropouts from LT waiting lists and/or to downstage patients who are beyond the Milan criteria are widely utilized. We conducted a literature-based review to evaluate the role of systemic therapies as a bridging treatment to liver transplantation (LT) in HCC patients. Tyrosine kinase inhibitors (TKIs) can be used as a systemic bridging therapy to LT in patients with contraindications for locoregional liver-directed therapies. Immune checkpoint inhibitor (ICI) treatment can be utilized either as a monotherapy or as a combination therapy with bevacizumab or TKIs prior to LT. Acute rejection after liver transplantation is a concern in the context of ICI treatment. Thus, a safe ICI washout period before LT and cautious post-LT immunosuppression strategies are required to reduce post-LT rejections and to optimize clinical outcomes. Nevertheless, prospective clinical trials are needed to establish definitive conclusions about the utility of systemic therapy as a bridging modality prior to LT in HCC patients.
1. Introduction
Liver cancer is the sixth most commonly diagnosed cancer and the third most common cause of cancer-related deaths worldwide [1]. Hepatocellular carcinoma (HCC) accounts for approximately 80% of liver cancers, most often against the background of liver cirrhosis secondary to multiple risk factors, including hepatitis C virus (HCV) infection, hepatitis B virus (HBV) infection, alcohol-related liver disease (ALD) or metabolic dysfunction-associated steatotic liver disease (MASLD) [2,3].
Liver transplantation (LT) is the treatment of choice for HCC patients in the early stages if the tumor is unresectable [4,5]. There are various criteria used to assess eligibility for LT in HCC. Classically, the Milan criteria are utilized to define eligibility for LT, with the goal of achieving 4-year overall survival (OS) of more than 75%. The Milan criteria are included in the Barcelona Clinic Liver Cancer (BCLC) staging system, the American Association for the Study of Liver Diseases (AASLD) and the European Association for the Study of the Liver-European Organization for Research and Treatment of Cancer (EASL-EORTC) guidelines [5,6]. The University of California-San Francisco (UCSF) criteria represent another important expanded set of criteria for LT in HCC patients with comparable outcomes to the Milan criteria. The UCSF criteria are adopted in countries such as Australia and New Zealand [7,8,9]. Moreover, the United Network of Organ Sharing (UNOS) Down-Staging Criteria for LT are widely adopted in the USA, with a successful 5-year post-LT OS rate of 74% [10].
The biggest challenge for LT is organ shortage and long LT waiting lists, leading to patients’ dropout due to disease progression or liver decompensation [11]. In the USA, the national dropout rate from the transplant list for HCC patients reaches up to 29% as per the UNOS figures [12]. Thus, there is a need to implement therapies that control HCC until the availability of liver transplantation. This “bridging therapy” approach to transplantation aims either to reduce the number of dropouts from LT waiting lists for patients within the Milan criteria and/or to downstage patients who are beyond the Milan criteria [13]. Bridging strategies are either locoregional liver-directed or systemic therapies. Liver-directed therapies include radiofrequency ablation (RFA), microwave ablation (MWA), transarterial chemoembolization (TACE), transarterial radioembolization (TARE) and stereotactic body radiotherapy (SBRT) [14,15].
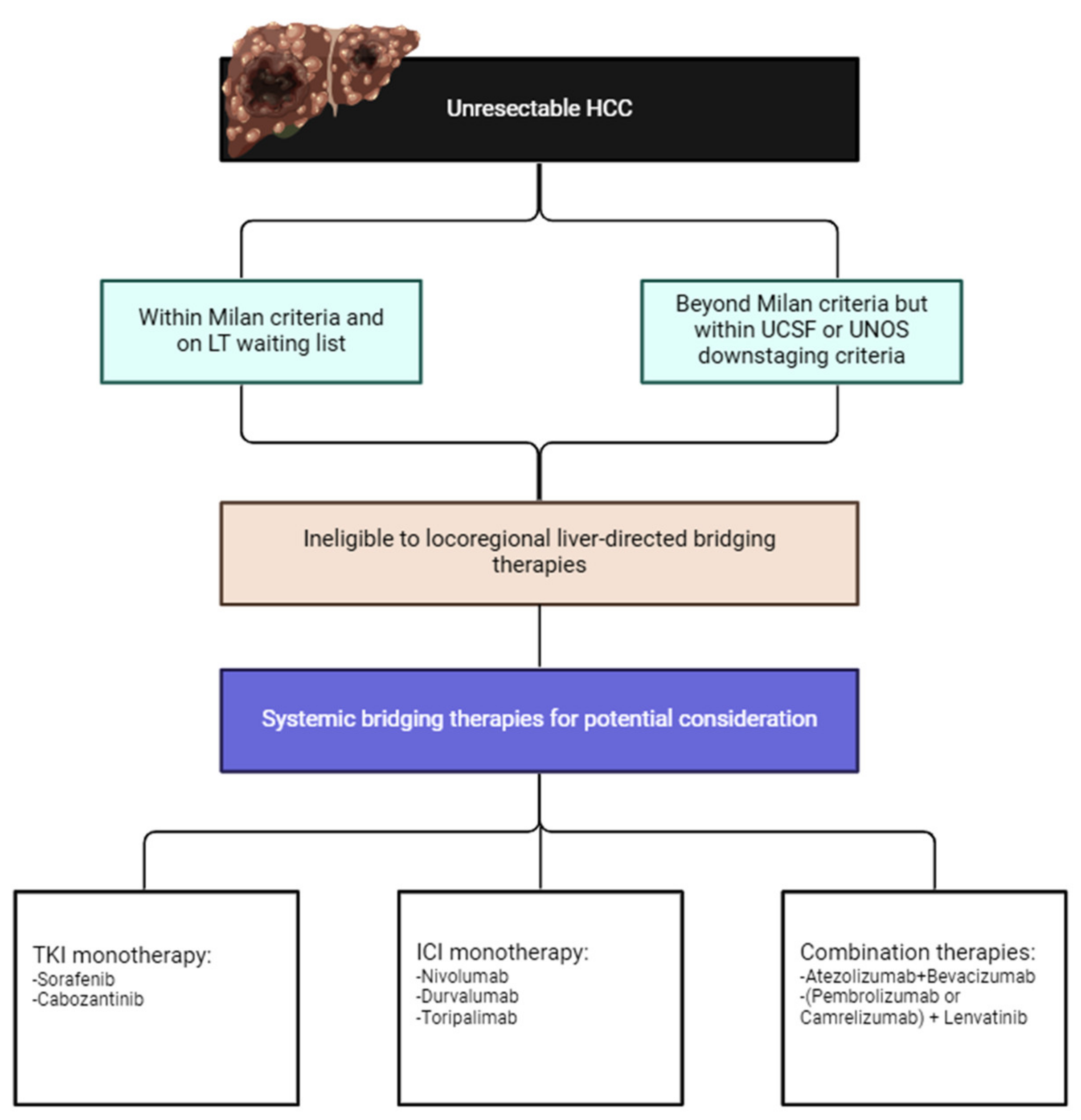
This review will focus on systemic therapies, including tyrosine kinase inhibitors (TKIs) and immune checkpoint inhibitors (ICIs), as bridging strategies to LT in HCC patients (Figure 1).
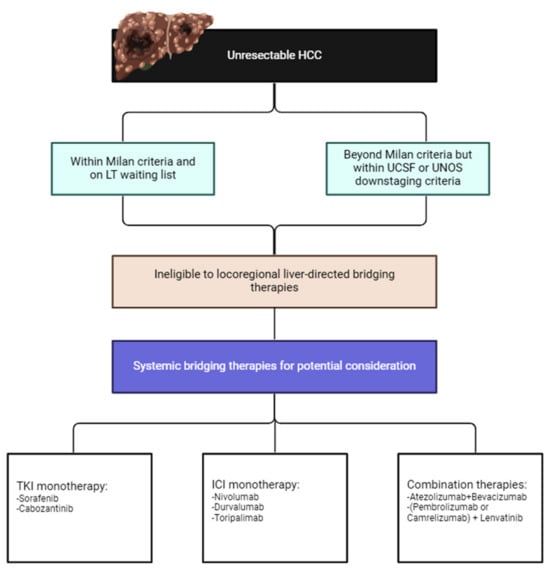
Figure 1.
Potential role of systemic therapies as bridging treatments to LT in HCC.
2. Systemic Therapies
2.1. Tyrosine Kinase Inhibitors (TKIs)
The therapeutic effect of TKIs is attained by binding to various tyrosine kinase receptors, thereby inhibiting downstream intracellular signaling, eventually resulting in apoptosis and anti-angiogenic effects, which play a major role in the tumor microenvironment of HCC [16]. Sorafenib, a small molecule TKI, was approved by the FDA for the treatment of advanced HCC based on the breakthrough results of the SHARP Trial in 2008 [17].
After approval for advanced HCC, TKIs were investigated as bridging treatments to LT. In 2010, Saidi et al. reported a case series of seven HCC patients whose tumors met the Milan criteria. All the patients were treated with sorafenib and six of them successfully underwent LT without local recurrence or distant metastasis [18]. In 2013, Vitale et al. reported another case series of six HCC patients who had Child–Pugh class A and intermediate stage disease. These patients received sorafenib before LT and the 4 patients who received sorafenib for a period of ≥2 months before LT were disease-free 27 to 41 months after LT [19]. In 2018, Golse et al. reported a cases series of five HCC patients, three of whom underwent hepatectomy or TACE and then received sorafenib as a bridging therapy before LT, while the other two patients received sorafenib as a downstaging therapy before LT. There were no tumor recurrences after LT within a 27-month follow-up [20]. In 2022, an observational study from France found that 62 out of 327 HCC patients listed for LT were treated with sorafenib; 50% of these patients received sorafenib because of HCC progression after locoregional therapy (LRT), the other 50% received sorafenib because of ineligibility to receive LRT. A total of 26 patients could progress to LT, where the 5-year OS and RFS were 77% and 48%, respectively [21].
Combination therapy with LRT and sorafenib as a bridging strategy to improve outcomes was also investigated. In 2014, 20 HCC patients who met the UCSF criteria for LT were randomized in a prospective trial to Y90 radioembolization with or without sorafenib (1:1 randomization ratio). Of the 20 patients, 17 underwent LT. The survival rates at 3 years were similar between the two groups. Combination therapy was associated with higher peri-transplant biliary complications and a trend toward more acute rejections [22]. In 2015, another prospective trial was published on 50 HCC patients who met the Milan criteria for LT and were randomized to TACE plus either sorafenib or placebo. A total of 17 patients could proceed to LT, and both groups had similar results in terms of the time to progression (TTP), tumor response and time to LT [23]. In 2022, a retrospective study on 128 HCC patients, whose tumors were either within or beyond the Milan criteria, found that those patients who received TACE plus sorafenib before LT achieved significantly better 5-year DFS compared to those who received TACE only; however, there was no significant difference in the 5-year OS rates between the two groups (77.8% vs. 61.5%, p value: 0.51) [24].
Cabozantinib is another TKI that is approved as a subsequent line of treatment for advanced HCC patients [25]. In 2022, Bhardwaj et al. reported two HCC patients who received cabozantinib after prior treatments with sorafenib and LRT. Both patients managed to progress to LT. The first patient developed disease recurrence 5 months after LT and the other patient was disease-free at the 21-month follow-up post LT [26].
In the Reflect trial, lenvatinib, a multi-kinase inhibitor, was compared to sorafenib in the first-line treatment of advanced HCC patients. Lenvatinib was non-inferior to sorafenib for survival. Lenvatinib achieved higher responses rates and better time to progression than sorafenib [27]. The effectiveness of lenvatinib compared to sorafenib was further confirmed in a meta-analysis [28]. Therefore, further exploration of lenvatinib in the bridging setting preceding LT can be promising.
Summary and Recommendations
The utilization of TKIs as a bridging treatment to LT in HCC patients with contraindications for locoregional liver-directed therapies is reported in the literature (Table 1). Most published reports examined sorafenib and found encouraging survival rates. However, prospective clinical trials are needed to establish definitive conclusions about the utility of TKI monotherapy as a bridging modality prior to LT in HCC patients.

Table 1.
Overview of the studies on TKIs used as a bridging therapy to liver transplant.
2.2. Immune Checkpoint Inhibitors (ICIs)
2.2.1. Efficacy and Safety
Over the past few years, immune checkpoint inhibitors (ICIs) have revolutionized the field of oncology, leading to prolonged survival with manageable side effects in various cancers [29]. In 2020, the combination therapy of atezolizumab (ICI) with bevacizumab was granted FDA approval for the first-line treatment of advanced HCC patients based on the superior survival outcome compared to the classical treatment with sorafenib [30].
The mechanism of action of ICIs involves activation of the suppressed innate immune system, which is contradictory to the functions of the immunosuppressant agents that are typically used post-LT. Consequently, the use of ICIs may increase the risk of rejection of the transplanted liver, a formidable potential consequence of using ICIs after liver transplantation. In a retrospective study by Wang et al., 16 HCC patients received ICI treatment before LT, and the study showed that the median time of acute rejection was 7 days post-LT and a shorter time interval (TI) between the last dose of ICI and LT increased the risk of postoperative rejection (median TI: 21 days vs. 60 days, p = 0.01); however, there were no immune-related graft losses [31]. Therefore, it is essential to establish a safe washout period, which is defined as the period between the last ICI dose and LT. In 2023, Kuo et al. concluded in a retrospective study that 42 days is a safe washout period for bridging ICI therapy with either atezolizumab, nivolumab or pembrolizumab before LT [32].
Data on the efficacy and safety of ICIs as bridging treatment to LT are accumulating. In 2021, Tabrizian et al. reported a single-center case series of nine HCC patients whose tumors met either the Milan or UCSF criteria. All the patients received nivolumab ICI therapy before being successfully bridged to liver transplant. Interestingly, 80% of the patients underwent LT within 4 weeks of the last dose of nivolumab and there were no instances of severe allograft rejections, tumor recurrences, or deaths at a median follow-up of 16 months after LT [33]. Moreover, in 2021, Chen et al. reported a case series of five HCC patients whose tumors were beyond the Milan Criteria. They all received bridging/downstaging treatment with nivolumab, the mean washout period was 63.8 days, and none of the patients developed biopsy-proven acute rejection (BPAR); however, two of them had HCC recurrences on follow-up [34]. In 2022, Schnickel et al. reported a case series of five HCC patients who received nivolumab ICI therapy before LT. The 2 patients who underwent LT within 3 months from the last dose of nivolumab developed BPAR and severe hepatic necrosis; however, BPAR was observed in none of the patients who underwent LT >3 months from the last dose of nivolumab [35]. Multiple case reports are published on ICI monotherapy as a bridging treatment to LT [36,37,38,39].
Combination therapies of ICIs with TKIs were also investigated as a bridging treatment strategy to LT. In 2021, Qiao et al. reported a cohort of seven HCC patients who received lenvatinib in combination with either pembrolizumab or camrelizumab ICI therapy prior to LT. The biopsy-proven acute rejection rate was 14.3% [40]. In 2022, Abdelrahim et al. published a case report on an HCC patient whose tumor was beyond the Milan criteria. The patient received atezolizumab plus bevacizumab combination therapy prior to successfully progressing to LT, with no HCC recurrence after 12 months of follow-up [41]. In 2023, Schmiderer et al. published another case report on an HCC patient who was successfully transplanted after receiving the atezolizumab plus bevacizumab combination therapy [42].
Summary and Recommendations
There is growing evidence in the literature regarding the role of ICIs as bridging treatment to LT in HCC. ICI treatment can be utilized either as a monotherapy or as a combination therapy with bevacizumab or TKIs prior to LT (Table 2). Acute rejection after LT is a concern in the context of ICI treatment. Thus, a safe ICI washout period before LT and cautious post-LT immunosuppression strategies are required to reduce post-LT rejections and to optimize clinical outcomes [31,32]. Furthermore, prospective clinical trials are needed to establish definitive conclusions about the utility of ICIs as a bridging modality prior to LT in HCC patients.
Table 2.
Overview of the studies on ICIs used as a bridging therapy to liver transplant.
2.2.2. Response Assessment
The classic radiologic disease assessment criteria, such as the response evaluation criteria in solid tumors (RECIST), may not adequately evaluate the response in HCC. These criteria rely on the tumor size, which can remain unchanged in locally or systemically treated HCC due to multiple factors, such as treatment-induced necrosis, the presence of ascites and reactive lymph nodes [44]. This results in an underestimation of the HCC tumor response. Therefore, in 2001, the European Association for the Study of the Liver (EASL) criteria were put forward to evaluate viable lesions on abdominal magnetic resonance imaging (MRI) [45]. Using this method, the arterially enhancing tumor burden is calculated in two dimensions. In 2008, the RECIST criteria were modified to the mRECIST, which include changes in tumor arterial enhancement [46]. The mRECIST can be applied to contrast-enhanced, multiphasic computed tomography (CT) or MRI. One of the advantages over the EASL criteria is that mRECIST provides recommendations for new lesions and non-target lesion selection, such as portal vein thrombosis, lymph node at the porta hepatis, ascites or pleural effusion [47]. The objective response rate was evaluated as a surrogate endpoint for overall survival (OS) in a systematic review of 14,056 patients with HCC treated with ICIs. The results of the meta-analysis showed that the objective response predicted by mRECIST (OR-mRECIST) was an independent predictor of OS and that the OR-mRECIST correlated better with the OS than the RECIST [48].
With the addition of immunotherapy to the armamentarium of treatment for HCC, pseudo-progression on imaging became a concern but was dismissed as it is rarely seen in HCC [49]. Therefore the immune response evaluation criteria in solid tumors (iRECIST), as designed to assess pseudo-progression, may not be required in HCC treated with immunotherapy [49]. On the contrary, tumor shrinkage is seen with immune checkpoint inhibitors and thus the RECIST criteria can be applied in this setting, as was the case in several clinical trials on immunotherapy in HCC.
Summary and Recommendations
Both the RECIST and mRECIST criteria (Table 3) are recommended by the guidelines for disease evaluation after systemic treatment [50].
Table 3.
The RECIST and mRECIST criteria for response assessment in HCC.
2.2.3. Biomarkers
Companion diagnostic tests, such as PD-L1 expression, can help identify patients who would benefit the most from ICIs and are widely used in various malignancies. However, this approach does not apply to HCC, where ICIs are administered to all patients regardless of the PD-L1 expression, knowing that some cases will be resistant to ICIs. For example, in the atezolizumab/bevacizumab arm of the landmark IMbrave 150 study, 19% of the patients were refractory to treatment [51]. This highlights the need for predictive markers that can help select patients who are most likely to benefit from ICIs. This is particularly relevant in the context of the graft rejection risk when utilizing ICIs as bridging treatment to liver transplant.
PD-L1 Expression
In the Checkmate-040 trial, which compared nivolumab monotherapy to combination therapy with ipilimumab in advanced HCC patients who previously received sorafenib, an objective response was observed regardless of the PD-L1 status [52]. Similarly, in the HIMALAYA trial, treatment with durvalumab and tremelimumab showed OS benefit compared to durvalumab or sorafenib as single agents in advanced HCC regardless of the PD-L1 expression [53]. In the Checkmate-459 trial, which compared nivolumab vs. sorafenib for advanced HCC, patients with PD-L1 ≥1% achieved a higher response rate with nivolumab compared to those with PD-L1 expression <1% (28% vs. 12%). However, this did not translate into a survival benefit, and both subgroups had a similar median OS (16.1 months for PD-L1 ≥ 1% and 16.7 months for PD-L1 < 1%) [54]. The KEYNOTE-224 trial aimed to assess the safety and efficacy of pembrolizumab in patients with advanced HCC previously treated with sorafenib. The study found that PD-L1 expression assessed by a combined positive score (CPS) ≥1 was associated with response to pembrolizumab in a subgroup of patients. The tumor proportion score (TPS) ≥1% was not significantly associated with the response, which could imply that the combination of immune and tumor cell scoring might improve the predictive value of PD-L1 testing [55]. A systematic review and meta-analysis by Yang et al. evaluated the predictive value of PD-L1 in patients with HCC treated with ICIs, and it found that patients with a positive PD-L1 expression had better ORR (pooled odds ratio, 1.86, 95% CI, 1.35–2.55). However, there was no difference in the disease control rate compared to those who were PD-L1 negative [56].
Summary and Recommendations
In the absence of substantial evidence from clinical trials, PD-L1 expression is not recommended for routine use as a predictor of the response to ICI in advanced HCC. Taking into consideration that there is a significant inter-assay heterogeneity in detecting PD-L1 in HCC, as was evident in the Blueprint-HCC study [57], further efforts are needed to standardize the measurement of PD-L1 expression in HCC to improve its consistency as a potential biomarker of the response to ICIs.
Microsatellite Instability
Microsatellite instability (MSI) is the result of a deficiency in DNA mismatch repair (MMR) mechanisms. MSI-high tumors accumulate somatic mutations that lead to neoantigen formation, which in turn activates an immune inflammatory cascade, thus making these tumors sensitive to ICIs. The efficacy of ICIs in different types of MSI-high malignancies has been demonstrated in the KEYNOTE-016, -164, -012, -028, and -158 trials [58,59,60,61,62]. However, the prevalence of high MSI in HCC is low, and it was found to be between 0% and 2.9% in a review of the literature [63]. Despite the limited evidence supporting the use of immunotherapy in MSI-high HCC [64,65], the low occurrence of microsatellite instability in this cancer diminishes the value of the MMR status as a predictive biomarker.
Tumor Mutational Burden
The tumor mutational burden (TMB) refers to the number of DNA mutations per megabase (Mb) within the coding genome of tumors [66]. An elevated TMB (>10 mutations/Mb) leads to increased neoantigen expression, which can trigger an immune response, making it a potential predictive marker for the effectiveness of immunotherapy. A high TMB was significantly associated with better objective response rates (ORRs) with pembrolizumab in the Keynote-158 trial, which led to the FDA approval of this drug in advanced solid tumors with high TMB. However, the improved ORR did not translate into a survival benefit and none of the included patients with biliary cancers had a high TMB [67,68]. Indeed, compared to other types of malignancies, HCC has a relatively low TMB (a median of 5 mutations/Mb) [69]. Additionally, the TMB in HCC can fluctuate depending on the type of pathology sample between paraffin-embedded or fresh-frozen section, and on the geographic origin of the patient [66]. In summary, the methodological variations and low TMB in HCC render the use of this predictive tool limited.
Tumor-Infiltrating Lymphocytes
ICIs exert their anti-tumor effect by activating the immune cells in the tumor microenvironment. This includes tumor-infiltrating lymphocytes (TILs) such as cytotoxic CD8+ cells and natural killer (NK) cells. A post hoc analysis of the CheckMate 040 trial showed that increased CD3+ and CD8+ cell infiltration led to an improvement in the OS in patients treated with nivolumab, but it did not reach statistical significance [70].
Inflammatory Markers
Systemic inflammation, often triggered by a local pro-inflammatory response in the tumor microenvironment, can lead to poor survival outcomes in patients with cancer. Two inflammatory markers were studied in HCC patients treated with ICIs: the neutrophil to lymphocyte ratio (NLR) and the platelet to lymphocyte ratio (PLR). A study found that patients with HCC treated with nivolumab who achieved a partial or complete response had a significantly lower post-treatment NLR and PLR (p < 0.001 for both) compared to those with stable disease or progression. Both ratios were significantly associated with survival in a multivariable analysis [71]. In a retrospective analysis of 362 patients treated with ICIs for HCC, patients with NLR ≥ 5 had significantly worse OS (7.7 vs. 17.6 months, p < 0.0001), PFS (2.1 vs. 3.8 months, p = 0.025), and ORR (12% vs. 22%, p = 0.034). Patients with PLR ≥ 300 had similar results, with significantly shorter OS (6.4 vs. 16.5 months, p < 0.0001) and PFS (1.8 vs. 3.7 months, p = 0.0006) [66].
Summary and Recommendations
Although these results are encouraging, the utility of inflammatory markers as predictive biomarkers is limited by the fluctuation during the course of the illness and treatment. Further validation in larger cohorts is necessary.
Gut Microbiota
The commensal microbes of the digestive system are being highlighted as key players in cancer pathogenesis and the response to treatment in several types of malignancies, particularly in colorectal cancer [72]. A systematic review and meta-analysis assessed the relation of the gut microbiota composition and the response to ICIs in 775 patients with different types of solid organ malignancies. This effort resulted in identifying Faecalibacterium prausnitzii, Streptococcus parasanguinis, Bacteroides caccae, and Prevotella copri to be more commonly present in responders to ICIs and to be associated with a better prognosis. In contrast, Blautia obeum and Bacteroides ovatus were associated with a poorer prognosis [73]. Zheng et al. examined fecal samples from eight patients with HCC receiving camrelizumab and compared the microbiota of responders vs. non-responders at different time points during treatment. Responders were characterized by having higher taxa richness and more gene counts than non-responders. Furthermore, the study found a dynamic variation in the composition of the microbiota over the course of treatment, such as an increase in Proteobacteria in non-responders between weeks 3 and 12 of PD-1 blockade. Therefore, examining the variation in the gut microbiota can be a promising predictor of the response to ICIs in HCC as early as within 3 to 6 weeks of treatment administration [74]. In a larger cohort of 65 patients with advanced hepatobiliary cancers receiving anti-PD-1 treatment, Lachnospiraceae bacterium-GAM79 and Alistipes sp. Marseille-P5997 were significantly more enriched in responders, and their abundance was associated with better progression-free and overall survival. In contrast, the Veillonellaceae were significantly more abundant in non-responders and were associated with worse PFS and OS. Another observation from this study was that a more diverse gut microbiota is associated with a lower risk of immune-related adverse events [75]. Another study found that Lachnoclostridium enrichment conferred a survival benefit (median OS of 22.8 months vs. 5.6 months, p = 0.032), while patients with enriched fecal Prevotella 9 had significantly worse OS compared to others (median OS of 8.6 months vs. 17.2 months, p = 0.039). The best median OS was in patients with both Lachnoclostridium enrichment and Prevotella 9 depletion in the feces (22.8 months) [76].
Summary and Recommendations
Overall, the gut microbiota’s composition and its dynamic variation throughout immunotherapy administration is a promising biomarker to predict the response to treatment, but it still needs validation in larger studies. Additionally, its clinical application may be challenging given the high susceptibility of the microbiome to external factors, such as antibiotic administration and dietary changes, which may complicate the interpretation and utility of this marker.
Genomic Characteristics
HCC has a heterogeneous genomic profile, and several studies have been conducted to identify potential genomic biomarkers that can inform treatment decisions. HCCs can be categorized into two molecular types: proliferative and non-proliferative. Proliferative HCCs have a subclass characterized by a high number of infiltrating CD4+ and CD8+ T cells, which respond well to ICIs [77]. On the other hand, non-proliferative HCCs are dominated by Wnt signaling and tend to be less aggressive, have lower levels of AFP and are more differentiated [78]. The role of this molecular classification is not yet clear in clinical practice, and further evidence is needed to support its utility as a predictive biomarker.
A promising predictive biomarker is the Wnt-β-catenin pathway, since its activation is one of the main cancer-driver gene mutations in HCC, causing the upregulation of oncogenes and favoring immune resistance. Activation of this pathway occurs in 30% to 50% of cases of HCC, triggered by mutations in the CTNNB1 that encodes β-catenin and the inactivation of AXIN1 or APC, which are inhibitors of the Wnt pathway [11]. To test this in a clinical context, Harding et al. used next-generation sequencing to determine predictive and prognostic biomarkers for HCC. Among the patients treated with ICIs, activating alterations in the Wnt-β-catenin pathway was associated with worse outcomes in terms of the disease control rate (0% vs. 53%), median PFS (2.0 vs. 7.4 months), and median OS (9.1 vs. 15.2 months) [79]. Morita et al. evaluated the molecular and immunological features of HCC as predictive markers of the response to ICIs. The study concluded that the absence of staining of the molecules in Wnt/β-catenin signaling, high infiltration of CD8+ cells, and high CPS of PD-L1 were significant contributors to the response to PD-1 blockade [80].
Summary and Recommendations
Additional research in larger groups of patients is necessary to delineate the predictive value of HCC’s genomic characteristics and their correlation to treatments, including ICIs.
3. Future Directions
Multiple prospective studies are ongoing to assess the safety and efficacy of bridging systemic therapies before LT.
The PLENTY202001 trial is investigating the safety and efficacy of pembrolizumab in combination with lenvatinib as neoadjuvant therapy in 192 anticipated participants with HCC exceeding the Milan criteria before LT. The study aims to determine whether this combination as a neoadjuvant treatment for advanced HCC could decrease postoperative recurrence and to analyze potential immune biomarkers of the therapeutic response [81]. ESR-20-21010 is a single-arm, phase II, multicenter clinical trial aiming to assess the safety and efficacy of durvalumab and tremelimumab for the treatment of 30 anticipated patients with HCC within the UCSF criteria who are listed for liver transplant and have cirrhosis or portal hypertension. The primary endpoint of this study is post-transplant rejection within 30 days of transplant [82]. The combinations of ICIs plus either lenvatinib or bevacizumab are currently under investigation in two other clinical trials too [83,84]. Finally, Sun Yat-Sen Memorial Hospital in China is studying single-agent ICIs as bridging/downstaging treatment to LT in HCC patients who are beyond the Milan criteria [85].
Summary and Recommendations
Ongoing clinical trials on systemic bridging therapies to LT are examining ICIs alone or in combination with either TKIs or bevacizumab (Table 4). An important endpoint is the rejection rates post LT. Publication of the results of these ongoing clinical trials will have a favorable impact on the management of this particular subset of HCC patients.
Table 4.
Overview of the ongoing studies on systemic bridging therapy to liver transplant.
4. Conclusions
Enhancing HCC patients’ bridging to LT via systemic treatments is an evolving field, especially when locoregional liver-directed therapy is contraindicated. Investigations into single-agent TKIs, ICIs, or their combinations as bridging modalities are being conducted. ICIs in combination with TKIs or VEGF inhibitors likely represent the most promising approach. However, concerns remain regarding post-LT rejection after bridging with ICIs, necessitating further prospective clinical trials to determine the optimal pre-LT ICI washout periods to ensure safety and efficacy. Concurrently, efforts to identify biomarkers, particularly of ICIs, are underway to better predict the HCC tumor response to treatment and to mitigate the risks associated with post-LT rejection.
Author Contributions
Conceptualization, Y.S., R.T., T.A.H.; methodology, Y.S., R.T., T.A.H., M.A.; writing—original draft preparation, Y.S., R.T., T.A.H., A.S., L.C., T.A.; writing—review and editing, Y.S., R.T., T.A.H., M.A., A.S., L.C., T.A., I.M., M.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Rumgay, H.; Arnold, M.; Ferlay, J.; Lesi, O.; Cabasag, C.J.; Vignat, J.; Laversanne, M.; McGlynn, K.A.; Soerjomataram, I. Global Burden of Primary Liver Cancer in 2020 and Predictions to 2040. J. Hepatol. 2022, 77, 1598–1606. [Google Scholar] [CrossRef] [PubMed]
- Rumgay, H.; Ferlay, J.; de Martel, C.; Georges, D.; Ibrahim, A.S.; Zheng, R.; Wei, W.; Lemmens, V.E.P.P.; Soerjomataram, I. Global, Regional and National Burden of Primary Liver Cancer by Subtype. Eur. J. Cancer 2022, 161, 108–118. [Google Scholar] [CrossRef] [PubMed]
- Singal, A.G.; Kanwal, F.; Llovet, J.M. Global Trends in Hepatocellular Carcinoma Epidemiology: Implications for Screening, Prevention and Therapy. Nat. Rev. Clin. Oncol. 2023, 20, 864–884. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Villanueva, A.; Marrero, J.A.; Schwartz, M.; Meyer, T.; Galle, P.R.; Lencioni, R.; Greten, T.F.; Kudo, M.; Mandrekar, S.J.; et al. Trial Design and Endpoints in Hepatocellular Carcinoma: AASLD Consensus Conference. Hepatology 2021, 73, 158–191. [Google Scholar] [CrossRef] [PubMed]
- Mazzaferro, V.; Regalia, E.; Doci, R.; Andreola, S.; Pulvirenti, A.; Bozzetti, F.; Montalto, F.; Ammatuna, M.; Morabito, A.; Gennari, L. Liver Transplantation for the Treatment of Small Hepatocellular Carcinomas in Patients with Cirrhosis. N. Engl. J. Med. 1996, 334, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Pavel, M.-C.; Fuster, J. Expansion of the Hepatocellular Carcinoma Milan Criteria in Liver Transplantation: Future Directions. World J. Gastroenterol. 2018, 24, 3626–3636. [Google Scholar] [CrossRef] [PubMed]
- Yao, F.Y.; Roberts, J.P. Applying Expanded Criteria to Liver Transplantation for Hepatocellular Carcinoma: Too Much Too Soon, or Is Now the Time? Liver Transplant. 2004, 10, 919–921. [Google Scholar] [CrossRef] [PubMed]
- Barreto, S.G.; Strasser, S.I.; McCaughan, G.W.; Fink, M.A.; Jones, R.; McCall, J.; Munn, S.; Macdonald, G.A.; Hodgkinson, P.; Jeffrey, G.P.; et al. Expansion of Liver Transplantation Criteria for Hepatocellular Carcinoma from Milan to UCSF in Australia and New Zealand and Justification for Metroticket 2.0. Cancers 2022, 14, 2777. [Google Scholar] [CrossRef] [PubMed]
- Bento de Sousa, J.H.; Calil, I.L.; Tustumi, F.; da Cunha Khalil, D.; Felga, G.E.G.; de Arruda Pecora, R.A.; de Almeida, M.D. Comparison between Milan and UCSF Criteria for Liver Transplantation in Patients with Hepatocellular Carcinoma: A Systematic Review and Meta-Analysis. Transl. Gastroenterol. Hepatol. 2021, 6, 11. [Google Scholar] [CrossRef]
- Tan, D.J.H.; Lim, W.H.; Yong, J.N.; Ng, C.H.; Muthiah, M.D.; Tan, E.X.; Xiao, J.; Lim, S.Y.; Pin Tang, A.S.; Pan, X.H.; et al. UNOS Down-Staging Criteria for Liver Transplantation of Hepatocellular Carcinoma: Systematic Review and Meta-Analysis of 25 Studies. Clin. Gastroenterol. Hepatol. 2023, 21, 1475–1484. [Google Scholar] [CrossRef]
- Llovet, J.M.; Kelley, R.K.; Villanueva, A.; Singal, A.G.; Pikarsky, E.; Roayaie, S.; Lencioni, R.; Koike, K.; Zucman-Rossi, J.; Finn, R.S. Hepatocellular Carcinoma. Nat. Rev. Dis. Primers 2021, 7, 1–28. [Google Scholar] [CrossRef] [PubMed]
- Sokolich, J.; Buggs, J.; LaVere, M.; Robichaux, K.; Rogers, E.; Nyce, S.; Kumar, A.; Bowers, V. HCC Liver Transplantation Wait List Dropout Rates Before and After the Mandated 6-Month Wait Time. Am. Surg. 2020, 86, 1592–1595. [Google Scholar] [CrossRef] [PubMed]
- Gao, Q.; Anwar, I.J.; Abraham, N.; Barbas, A.S. Liver Transplantation for Hepatocellular Carcinoma after Downstaging or Bridging Therapy with Immune Checkpoint Inhibitors. Cancers 2021, 13, 6307. [Google Scholar] [CrossRef] [PubMed]
- Crocetti, L.; Bozzi, E.; Scalise, P.; Bargellini, I.; Lorenzoni, G.; Ghinolfi, D.; Campani, D.; Balzano, E.; De Simone, P.; Cioni, R. Locoregional Treatments for Bridging and Downstaging HCC to Liver Transplantation. Cancers 2021, 13, 5558. [Google Scholar] [CrossRef] [PubMed]
- Lewis, S.; Dawson, L.; Barry, A.; Stanescu, T.; Mohamad, I.; Hosni, A. Stereotactic Body Radiation Therapy for Hepatocellular Carcinoma: From Infancy to Ongoing Maturity. JHEP Rep. 2022, 4, 100498. [Google Scholar] [CrossRef] [PubMed]
- Mou, L.; Tian, X.; Zhou, B.; Zhan, Y.; Chen, J.; Lu, Y.; Deng, J.; Deng, Y.; Wu, Z.; Li, Q.; et al. Improving Outcomes of Tyrosine Kinase Inhibitors in Hepatocellular Carcinoma: New Data and Ongoing Trials. Front. Oncol. 2021, 11, 752725. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.-F.; de Oliveira, A.C.; Santoro, A.; Raoul, J.-L.; Forner, A.; et al. Sorafenib in Advanced Hepatocellular Carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef]
- Saidi, R.F.; Shah, S.A.; Rawson, A.P.; Grossman, S.; Piperdi, B.; Bozorgzadeh, A. Treating Hepatocellular Carcinoma with Sorafenib in Liver Transplant Patients: An Initial Experience. Transpl. Proc. 2010, 42, 4582–4584. [Google Scholar] [CrossRef] [PubMed]
- Aless; Vitale, R.; Salinas, F.; Zanus, G.; Lombardi, G.; Senzolo, M.; Russo, F.; Cillo, U. Could Sorafenib Disclose New Prospects as Bridging Therapy to Liver Transplantation in Patients with Hepatocellular Carcinoma? J. Liver 2013, 2, 1000134. [Google Scholar] [CrossRef]
- Golse, N.; Radenne, S.; Rode, A.; Ducerf, C.; Mabrut, J.-Y.; Merle, P. Liver Transplantation After Neoadjuvant Sorafenib Therapy: Preliminary Experience and Literature Review. Exp. Clin. Transpl. 2018, 16, 227–236. [Google Scholar] [CrossRef]
- Minoux, K.; Lassailly, G.; Ningarhari, M.; Lubret, H.; El Amrani, M.; Canva, V.; Truant, S.; Mathurin, P.; Louvet, A.; Lebuffe, G.; et al. Neo-Adjuvant Use of Sorafenib for Hepatocellular Carcinoma Awaiting Liver Transplantation. Transpl. Int. 2022, 35, 10569. [Google Scholar] [CrossRef]
- Kulik, L.; Vouche, M.; Koppe, S.; Lewandowski, R.J.; Mulcahy, M.F.; Ganger, D.; Habib, A.; Karp, J.; Al-Saden, P.; Lacouture, M.; et al. Prospective Randomized Pilot Study of Y90+/−sorafenib as Bridge to Transplantation in Hepatocellular Carcinoma. J. Hepatol. 2014, 61, 309–317. [Google Scholar] [CrossRef]
- Hoffmann, K.; Ganten, T.; Gotthardtp, D.; Radeleff, B.; Settmacher, U.; Kollmar, O.; Nadalin, S.; Karapanagiotou-Schenkel, I.; Von Kalle, C.; Jäger, D.; et al. Impact of Neo-Adjuvant Sorafenib Treatment on Liver Transplantation in HCC Patients—A Prospective, Randomized, Double-Blind, Phase III Trial. BMC Cancer 2015, 15, 392. [Google Scholar] [CrossRef]
- Abdelrahim, M.; Victor, D.; Esmail, A.; Kodali, S.; Graviss, E.A.; Nguyen, D.T.; Moore, L.W.; Saharia, A.; McMillan, R.; Fong, J.N.; et al. Transarterial Chemoembolization (TACE) Plus Sorafenib Compared to TACE Alone in Transplant Recipients with Hepatocellular Carcinoma: An Institution Experience. Cancers 2022, 14, 650. [Google Scholar] [CrossRef]
- Abou-Alfa, G.K.; Meyer, T.; Cheng, A.-L.; El-Khoueiry, A.B.; Rimassa, L.; Ryoo, B.-Y.; Cicin, I.; Merle, P.; Chen, Y.; Park, J.-W.; et al. Cabozantinib in Patients with Advanced and Progressing Hepatocellular Carcinoma. N. Engl. J. Med. 2018, 379, 54–63. [Google Scholar] [CrossRef]
- Bhardwaj, H.; Fritze, D.; Mais, D.; Kadaba, V.; Arora, S.P. Neoadjuvant Therapy with Cabozantinib as a Bridge to Liver Transplantation in Patients with Hepatocellular Carcinoma (HCC): A Case Report. Front. Transpl. 2022, 1, 863086. [Google Scholar] [CrossRef]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.-H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.-W.; Han, G.; Jassem, J.; et al. Lenvatinib versus Sorafenib in First-Line Treatment of Patients with Unresectable Hepatocellular Carcinoma: A Randomised Phase 3 Non-Inferiority Trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef] [PubMed]
- Facciorusso, A.; Tartaglia, N.; Villani, R.; Serviddio, G.; Ramai, D.; Mohan, B.P.; Chandan, S.; Abd El Aziz, M.A.; Evangelista, J.; Cotsoglou, C.; et al. Lenvatinib versus Sorafenib as First-Line Therapy of Advanced Hepatocellular Carcinoma: A Systematic Review and Meta-Analysis. Am. J. Transl. Res. 2021, 13, 2379–2387. [Google Scholar] [PubMed]
- Mandlik, D.S.; Mandlik, S.K.; Choudhary, H.B. Immunotherapy for Hepatocellular Carcinoma: Current Status and Future Perspectives. World J. Gastroenterol. 2023, 29, 1054–1075. [Google Scholar] [CrossRef]
- Atezolizumab Plus Bevacizumab in Unresectable Hepatocellular Carcinoma|NEJM. Available online: https://www.nejm.org/doi/full/10.1056/nejmoa1915745 (accessed on 26 February 2024).
- Wang, T.; Chen, Z.; Liu, Y.; Jia, Y.; Ju, W.; Chen, M.; Zhao, Q.; Wang, D.; Guo, Z.; Tang, Y.; et al. Neoadjuvant Programmed Cell Death 1 Inhibitor before Liver Transplantation for HCC Is Not Associated with Increased Graft Loss. Liver Transpl. 2023, 29, 598–606. [Google Scholar] [CrossRef]
- Kuo, F.-C.; Chen, C.-Y.; Lin, N.-C.; Liu, C.; Hsia, C.-Y.; Loong, C.-C. Optimizing the Safe Washout Period for Liver Transplantation Following Immune Checkpoint Inhibitors with Atezolizumab, Nivolumab, or Pembrolizumab. Transpl. Proc. 2023, 55, 878–883. [Google Scholar] [CrossRef] [PubMed]
- Tabrizian, P.; Florman, S.S.; Schwartz, M.E. PD-1 Inhibitor as Bridge Therapy to Liver Transplantation? Am. J. Transplant. 2021, 21, 1979–1980. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Hong, X.; Wang, T.; Guo, Y.; Huang, C.; Li, M.; He, X.; Ju, W.; Chen, M. Prognosis after Liver Transplantation in Patients Treated with Anti-PD-1 Immunotherapy for Advanced Hepatocellular Carcinoma: Case Series. Ann. Palliat. Med. 2021, 10, 9354–9361. [Google Scholar] [CrossRef] [PubMed]
- Schnickel, G.T.; Fabbri, K.; Hosseini, M.; Misel, M.; Berumen, J.; Parekh, J.; Mekeel, K.; Dehghan, Y.; Kono, Y.; Ajmera, V. Liver Transplantation for Hepatocellular Carcinoma Following Checkpoint Inhibitor Therapy with Nivolumab. Am. J. Transpl. 2022, 22, 1699–1704. [Google Scholar] [CrossRef] [PubMed]
- Sogbe, M.; López-Guerra, D.; Blanco-Fernández, G.; Sangro, B.; Narváez-Rodriguez, I. Durvalumab as a Successful Downstaging Therapy for Liver Transplantation in Hepatocellular Carcinoma: The Importance of a Washout Period. Transplantation 2021, 105, e398–e400. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.-H.; Wang, G.-B.; Huang, F.; Qin, R.; Yu, X.-J.; Wu, R.-L.; Hou, L.-J.; Ye, Z.-H.; Zhang, X.-H.; Zhao, H.-C. Pretransplant Use of Toripalimab for Hepatocellular Carcinoma Resulting in Fatal Acute Hepatic Necrosis in the Immediate Postoperative Period. Transpl. Immunol. 2021, 66, 101386. [Google Scholar] [CrossRef] [PubMed]
- Schwacha-Eipper, B.; Minciuna, I.; Banz, V.; Dufour, J.F. Immunotherapy as a Downstaging Therapy for Liver Transplantation. Hepatology 2020, 72, 1488–1490. [Google Scholar] [CrossRef] [PubMed]
- Nordness, M.F.; Hamel, S.; Godfrey, C.M.; Shi, C.; Johnson, D.B.; Goff, L.W.; O’Dell, H.; Perri, R.E.; Alexopoulos, S.P. Fatal Hepatic Necrosis after Nivolumab as a Bridge to Liver Transplant for HCC: Are Checkpoint Inhibitors Safe for the Pretransplant Patient? Am. J. Transplant. 2020, 20, 879–883. [Google Scholar] [CrossRef] [PubMed]
- Qiao, Z.; Zhang, Z.; Lv, Z.; Tong, H.; Xi, Z.; Wu, H.; Chen, X.; Xia, L.; Feng, H.; Zhang, J.; et al. Neoadjuvant Programmed Cell Death 1 (PD-1) Inhibitor Treatment in Patients with Hepatocellular Carcinoma Before Liver Transplant: A Cohort Study and Literature Review. Front. Immunol. 2021, 12, 653437. [Google Scholar] [CrossRef]
- Abdelrahim, M.; Esmail, A.; Umoru, G.; Westhart, K.; Abudayyeh, A.; Saharia, A.; Ghobrial, R.M. Immunotherapy as a Neoadjuvant Therapy for a Patient with Hepatocellular Carcinoma in the Pretransplant Setting: A Case Report. Curr. Oncol. 2022, 29, 4267–4273. [Google Scholar] [CrossRef]
- Schmiderer, A.; Zoller, H.; Niederreiter, M.; Effenberger, M.; Oberhuber, G.; Krendl, F.J.; Oberhuber, R.; Schneeberger, S.; Tilg, H.; Djanani, A. Liver Transplantation after Successful Downstaging of a Locally Advanced Hepatocellular Carcinoma with Systemic Therapy. Dig Dis. 2023, 41, 641–644. [Google Scholar] [CrossRef] [PubMed]
- Dave, S.; Yang, K.; Schnickel, G.T.; Kono, Y.; Delebecque, F.; Arellano, D.; Liu, A.; Zhang, X.; Tu, X.M.; Ajmera, V. The Impact of Treatment of Hepatocellular Carcinoma with Immune Checkpoint Inhibitors on Pre- and Post-Liver Transplant Outcomes. Transplantation 2022, 106, e308–e309. [Google Scholar] [CrossRef]
- Tsujita, Y.; Sofue, K.; Ueshima, E.; Ueno, Y.; Hori, M.; Tsurusaki, M.; Murakami, T. Evaluation and Prediction of Treatment Response for Hepatocellular Carcinoma. Magn. Reson. Med. Sci. 2023, 22, 209–220. [Google Scholar] [CrossRef] [PubMed]
- Bruix, J.; Sherman, M.; Llovet, J.M.; Beaugrand, M.; Lencioni, R.; Burroughs, A.K.; Christensen, E.; Pagliaro, L.; Colombo, M.; Rodés, J.; et al. Clinical Management of Hepatocellular Carcinoma. Conclusions of the Barcelona-2000 EASL Conference. European Association for the Study of the Liver. J. Hepatol. 2001, 35, 421–430. [Google Scholar] [CrossRef] [PubMed]
- Lencioni, R.; Llovet, J.M. Modified RECIST (mRECIST) Assessment for Hepatocellular Carcinoma. Semin. Liver Dis. 2010, 30, 52–60. [Google Scholar] [CrossRef]
- Kim, M.N.; Kim, B.K.; Han, K.-H.; Kim, S.U. Evolution from WHO to EASL and mRECIST for Hepatocellular Carcinoma: Considerations for Tumor Response Assessment. Expert Rev. Gastroenterol. Hepatol. 2015, 9, 335–348. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M.; Montal, R.; Finn, R.S.; Castet, F.; Ueshima, K.; Nishida, N.; Haber, P.K.; Hu, Y.; Chiba, Y.; Schwartz, M.; et al. Objective Response Predicts Survival in Advanced Hepatocellular Carcinoma Treated with Systemic Therapies. Clin. Cancer Res. 2022, 28, 3443–3451. [Google Scholar] [CrossRef]
- Lee, D.H.; Hwang, S.; Koh, Y.H.; Lee, K.-H.; Kim, J.Y.; Kim, Y.J.; Yoon, J.-H.; Lee, J.-H.; Park, J.-W. Outcome of Initial Progression During Nivolumab Treatment for Hepatocellular Carcinoma: Should We Use iRECIST? Front. Med. 2021, 8, 771887. [Google Scholar] [CrossRef]
- Galle, P.R.; Forner, A.; Llovet, J.M.; Mazzaferro, V.; Piscaglia, F.; Raoul, J.-L.; Schirmacher, P.; Vilgrain, V. EASL Clinical Practice Guidelines: Management of Hepatocellular Carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef]
- Cheng, A.-L.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.-Y.; Lim, H.Y.; Kudo, M.; Breder, V.; Merle, P.; et al. Updated Efficacy and Safety Data from IMbrave150: Atezolizumab plus Bevacizumab vs. Sorafenib for Unresectable Hepatocellular Carcinoma. J. Hepatol. 2022, 76, 862–873. [Google Scholar] [CrossRef]
- Yau, T.; Kang, Y.-K.; Kim, T.-Y.; El-Khoueiry, A.B.; Santoro, A.; Sangro, B.; Melero, I.; Kudo, M.; Hou, M.-M.; Matilla, A.; et al. Efficacy and Safety of Nivolumab Plus Ipilimumab in Patients with Advanced Hepatocellular Carcinoma Previously Treated with Sorafenib: The CheckMate 040 Randomized Clinical Trial. JAMA Oncol. 2020, 6, e204564. [Google Scholar] [CrossRef]
- Tremelimumab Plus Durvalumab in Unresectable Hepatocellular Carcinoma|NEJM Evidence. Available online: https://evidence.nejm.org/doi/full/10.1056/EVIDoa2100070 (accessed on 11 March 2024).
- Yau, T.; Park, J.-W.; Finn, R.S.; Cheng, A.-L.; Mathurin, P.; Edeline, J.; Kudo, M.; Harding, J.J.; Merle, P.; Rosmorduc, O.; et al. Nivolumab versus Sorafenib in Advanced Hepatocellular Carcinoma (CheckMate 459): A Randomised, Multicentre, Open-Label, Phase 3 Trial. Lancet Oncol. 2022, 23, 77–90. [Google Scholar] [CrossRef]
- Zhu, A.X.; Finn, R.S.; Edeline, J.; Cattan, S.; Ogasawara, S.; Palmer, D.; Verslype, C.; Zagonel, V.; Fartoux, L.; Vogel, A.; et al. Pembrolizumab in Patients with Advanced Hepatocellular Carcinoma Previously Treated with Sorafenib (KEYNOTE-224): A Non-Randomised, Open-Label Phase 2 Trial. Lancet Oncol. 2018, 19, 940–952. [Google Scholar] [CrossRef]
- Yang, Y.; Chen, D.; Zhao, B.; Ren, L.; Huang, R.; Feng, B.; Chen, H. The Predictive Value of PD-L1 Expression in Patients with Advanced Hepatocellular Carcinoma Treated with PD-1/PD-L1 Inhibitors: A Systematic Review and Meta-Analysis. Cancer Med. 2023, 12, 9282–9292. [Google Scholar] [CrossRef]
- Pinato, D.J.; Mauri, F.A.; Spina, P.; Cain, O.; Siddique, A.; Goldin, R.; Victor, S.; Pizio, C.; Akarca, A.U.; Boldorini, R.L.; et al. Clinical Implications of Heterogeneity in PD-L1 Immunohistochemical Detection in Hepatocellular Carcinoma: The Blueprint-HCC Study. Br. J. Cancer 2019, 120, 1033–1036. [Google Scholar] [CrossRef]
- Le, D.T.; Uram, J.N.; Wang, H.; Bartlett, B.R.; Kemberling, H.; Eyring, A.D.; Skora, A.D.; Luber, B.S.; Azad, N.S.; Laheru, D.; et al. PD-1 Blockade in Tumors with Mismatch-Repair Deficiency. N. Engl. J. Med. 2015, 372, 2509–2520. [Google Scholar] [CrossRef]
- Muro, K.; Chung, H.C.; Shankaran, V.; Geva, R.; Catenacci, D.; Gupta, S.; Eder, J.P.; Golan, T.; Le, D.T.; Burtness, B.; et al. Pembrolizumab for Patients with PD-L1-Positive Advanced Gastric Cancer (KEYNOTE-012): A Multicentre, Open-Label, Phase 1b Trial. Lancet Oncol. 2016, 17, 717–726. [Google Scholar] [CrossRef]
- Frenel, J.-S.; Le Tourneau, C.; O’Neil, B.; Ott, P.A.; Piha-Paul, S.A.; Gomez-Roca, C.; van Brummelen, E.M.J.; Rugo, H.S.; Thomas, S.; Saraf, S.; et al. Safety and Efficacy of Pembrolizumab in Advanced, Programmed Death Ligand 1-Positive Cervical Cancer: Results From the Phase Ib KEYNOTE-028 Trial. J. Clin. Oncol. 2017, 35, 4035–4041. [Google Scholar] [CrossRef]
- Marabelle, A.; Le, D.T.; Ascierto, P.A.; Di Giacomo, A.M.; De Jesus-Acosta, A.; Delord, J.-P.; Geva, R.; Gottfried, M.; Penel, N.; Hansen, A.R.; et al. Efficacy of Pembrolizumab in Patients with Noncolorectal High Microsatellite Instability/Mismatch Repair–Deficient Cancer: Results From the Phase II KEYNOTE-158 Study. J. Clin. Oncol. 2020, 38, 1–10. [Google Scholar] [CrossRef]
- Le, D.T.; Kim, T.W.; Cutsem, E.V.; Geva, R.; Jäger, D.; Hara, H.; Burge, M.; O’Neil, B.; Kavan, P.; Yoshino, T.; et al. Phase II Open-Label Study of Pembrolizumab in Treatment-Refractory, Microsatellite Instability-High/Mismatch Repair-Deficient Metastatic Colorectal Cancer: KEYNOTE-164. J. Clin. Oncol. 2020, 38, 11–19. [Google Scholar] [CrossRef]
- Eso, Y.; Shimizu, T.; Takeda, H.; Takai, A.; Marusawa, H. Microsatellite Instability and Immune Checkpoint Inhibitors: Toward Precision Medicine against Gastrointestinal and Hepatobiliary Cancers. J. Gastroenterol. 2020, 55, 15–26. [Google Scholar] [CrossRef] [PubMed]
- Ando, Y.; Yamauchi, M.; Suehiro, Y.; Yamaoka, K.; Kosaka, Y.; Fuji, Y.; Uchikawa, S.; Kodama, K.; Morio, K.; Fujino, H.; et al. Complete Response to Pembrolizumab in Advanced Hepatocellular Carcinoma with Microsatellite Instability. Clin. J. Gastroenterol. 2020, 13, 867–872. [Google Scholar] [CrossRef] [PubMed]
- Kawaoka, T.; Ando, Y.; Yamauchi, M.; Suehiro, Y.; Yamaoka, K.; Kosaka, Y.; Fuji, Y.; Uchikawa, S.; Morio, K.; Fujino, H.; et al. Incidence of Microsatellite Instability-High Hepatocellular Carcinoma among Japanese Patients and Response to Pembrolizumab. Hepatol. Res. 2020, 50, 885–888. [Google Scholar] [CrossRef] [PubMed]
- Muhammed, A.; Fulgenzi, C.A.M.; Dharmapuri, S.; Pinter, M.; Balcar, L.; Scheiner, B.; Marron, T.U.; Jun, T.; Saeed, A.; Hildebrand, H.; et al. The Systemic Inflammatory Response Identifies Patients with Adverse Clinical Outcome from Immunotherapy in Hepatocellular Carcinoma. Cancers 2021, 14, 186. [Google Scholar] [CrossRef] [PubMed]
- Marabelle, A.; Fakih, M.; Lopez, J.; Shah, M.; Shapira-Frommer, R.; Nakagawa, K.; Chung, H.C.; Kindler, H.L.; Lopez-Martin, J.A.; Miller, W.H.; et al. Association of Tumour Mutational Burden with Outcomes in Patients with Advanced Solid Tumours Treated with Pembrolizumab: Prospective Biomarker Analysis of the Multicohort, Open-Label, Phase 2 KEYNOTE-158 Study. Lancet Oncol. 2020, 21, 1353–1365. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, C.; Ben-Shachar, R.; Gao, Y.; Hyun, S.W.; Rivers, Z.; Epstein, C.; Kaneva, K.; Sangli, C.; Nimeiri, H.; Patel, J. Assessment of Tumor Mutational Burden and Outcomes in Patients with Diverse Advanced Cancers Treated with Immunotherapy. JAMA Netw. Open 2023, 6, e2311181. [Google Scholar] [CrossRef] [PubMed]
- Yarchoan, M.; Albacker, L.A.; Hopkins, A.C.; Montesion, M.; Murugesan, K.; Vithayathil, T.T.; Zaidi, N.; Azad, N.S.; Laheru, D.A.; Frampton, G.M.; et al. PD-L1 Expression and Tumor Mutational Burden Are Independent Biomarkers in Most Cancers. JCI Insight 2019, 4, e126908. [Google Scholar] [CrossRef] [PubMed]
- Sangro, B.; Melero, I.; Wadhawan, S.; Finn, R.S.; Abou-Alfa, G.K.; Cheng, A.-L.; Yau, T.; Furuse, J.; Park, J.-W.; Boyd, Z.; et al. Association of Inflammatory Biomarkers with Clinical Outcomes in Nivolumab-Treated Patients with Advanced Hepatocellular Carcinoma. J. Hepatol. 2020, 73, 1460–1469. [Google Scholar] [CrossRef]
- Dharmapuri, S.; Özbek, U.; Lin, J.-Y.; Sung, M.; Schwartz, M.; Branch, A.D.; Ang, C. Predictive Value of Neutrophil to Lymphocyte Ratio and Platelet to Lymphocyte Ratio in Advanced Hepatocellular Carcinoma Patients Treated with Anti-PD-1 Therapy. Cancer Med. 2020, 9, 4962–4970. [Google Scholar] [CrossRef]
- Wong, C.C.; Yu, J. Gut Microbiota in Colorectal Cancer Development and Therapy. Nat. Rev. Clin. Oncol. 2023, 20, 429–452. [Google Scholar] [CrossRef]
- Zeriouh, M.; Raskov, H.; Kvich, L.; Gögenur, I.; Bennedsen, A.L.B. Checkpoint Inhibitor Responses Can Be Regulated by the Gut Microbiota—A Systematic Review. Neoplasia 2023, 43, 100923. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Wang, T.; Tu, X.; Huang, Y.; Zhang, H.; Tan, D.; Jiang, W.; Cai, S.; Zhao, P.; Song, R.; et al. Gut Microbiome Affects the Response to Anti-PD-1 Immunotherapy in Patients with Hepatocellular Carcinoma. J. Immunother. Cancer 2019, 7, 193. [Google Scholar] [CrossRef] [PubMed]
- Mao, J.; Wang, D.; Long, J.; Yang, X.; Lin, J.; Song, Y.; Xie, F.; Xun, Z.; Wang, Y.; Wang, Y.; et al. Gut Microbiome Is Associated with the Clinical Response to Anti-PD-1 Based Immunotherapy in Hepatobiliary Cancers. J. Immunother. Cancer 2021, 9, e003334. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.-C.; Wu, C.-J.; Hung, Y.-W.; Lee, C.J.; Chi, C.-T.; Lee, I.-C.; Yu-Lun, K.; Chou, S.-H.; Luo, J.-C.; Hou, M.-C.; et al. Gut Microbiota and Metabolites Associate with Outcomes of Immune Checkpoint Inhibitor-Treated Unresectable Hepatocellular Carcinoma. J. Immunother. Cancer 2022, 10, e004779. [Google Scholar] [CrossRef] [PubMed]
- Sia, D.; Jiao, Y.; Martinez-Quetglas, I.; Kuchuk, O.; Villacorta-Martin, C.; Castro de Moura, M.; Putra, J.; Camprecios, G.; Bassaganyas, L.; Akers, N.; et al. Identification of an Immune-Specific Class of Hepatocellular Carcinoma, Based on Molecular Features. Gastroenterology 2017, 153, 812–826. [Google Scholar] [CrossRef] [PubMed]
- Zucman-Rossi, J.; Villanueva, A.; Nault, J.-C.; Llovet, J.M. Genetic Landscape and Biomarkers of Hepatocellular Carcinoma. Gastroenterology 2015, 149, 1226–1239.e4. [Google Scholar] [CrossRef] [PubMed]
- Harding, J.J.; Nandakumar, S.; Armenia, J.; Khalil, D.N.; Albano, M.; Ly, M.; Shia, J.; Hechtman, J.F.; Kundra, R.; El Dika, I.; et al. Prospective Genotyping of Hepatocellular Carcinoma: Clinical Implications of Next-Generation Sequencing for Matching Patients to Targeted and Immune Therapies. Clin. Cancer Res. 2019, 25, 2116–2126. [Google Scholar] [CrossRef]
- Morita, M.; Nishida, N.; Sakai, K.; Aoki, T.; Chishina, H.; Takita, M.; Ida, H.; Hagiwara, S.; Minami, Y.; Ueshima, K.; et al. Immunological Microenvironment Predicts the Survival of the Patients with Hepatocellular Carcinoma Treated with Anti-PD-1 Antibody. Liver Cancer 2021, 10, 380–393. [Google Scholar] [CrossRef]
- RenJi Hospital. Safety and Efficacy Study of Pembrolizumab in Combination with LENvatinib in Participants with Hepatocellular Carcinoma (HCC) before Liver Transplant as Neoadjuvant TherapY—PLENTY Randomized Clinical Trial. 2020. Available online: https://clinicaltrials.gov/study/NCT04425226 (accessed on 27 May 2024).
- Sohal, D. Durvalumab (MEDI4736) and Tremelimumab for Hepatocellular Carcinoma in Patients Listed for a Liver Transplant. 2023. Available online: https://clinicaltrials.gov/study/NCT05027425 (accessed on 27 May 2024).
- Abdelrahim, M. Atezolizumab and Bevacizumab Pre-Liver Transplantation for Patients with Hepatocellular Carcinoma Beyond Milan Criteria: A Feasibility Study. 2023. Available online: https://www.clinicaltrials.gov/study/NCT05185505 (accessed on 27 May 2024).
- RenJi Hospital. Safety and Efficacy Study of Durvalumab in Combination with Lenvatinib in Participants with Locally Advanced and Metastatic Hepatocellular Carcinoma—DULECT2020-1 Trial. 2020. Available online: https://clinicaltrials.gov/study/NCT04443322 (accessed on 27 May 2024).
- Sun Yat-Sen Memorial Hospital of Sun Yat-Sen University. A Prospective, Single-Arm Study of Downstaging Protocol Containing Immunotherapy for HCC Beyond the Milan Criteria Before Liver Transplantation. 2023. Available online: https://classic.clinicaltrials.gov/ct2/show/NCT05475613 (accessed on 27 May 2024).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).