Simple Summary
This study investigated the impact of tumor size on T3b differentiated thyroid cancer prognosis. No significant difference was found in the prognosis of small T3b tumors compared to the T1 tumors. Disease-specific survival, disease-free survival, and overall survival were significantly lower only in large T3b tumors compared to T2 and T3a. If T3b tumors are 2 cm or smaller, downstaging may be considered. The modified T category, reclassifying T3b (≤2 cm) as T1, showed better staging performance than the existing category. Adopting this modified T category could improve the prognostic accuracy of the AJCC/TNM staging.
Abstract
The prognostic significance of tumor size in T3b differentiated thyroid cancer (DTC) remains debated and underexplored. This study aimed to examine the varying impact of T3b based on tumor size, analyzing disease-specific survival, disease-free survival, and overall survival. A retrospective review of 6282 DTC patients who underwent thyroid surgery at Seoul St. Mary’s Hospital from September 2000 to December 2017 was conducted. T3b was classified into three subcategories, T3b-1 (≤2 cm), T3b-2 (2–4 cm), and T3b-3 (>4 cm), using the same size criteria for T1, T2, and T3a. T3b-1 showed no significant difference in disease specific survival compared to T1, and both disease-free and disease-specific survival curves were sequentially ranked as T1, T3b-1, T2, T3a, T3b-2, and T3b-3. The modified T category, reclassifying T3b-1 as T1, demonstrated superior staging performance compared to the classic T category (c-index: 0.8961 vs. 0.8959 and AUC: 0.8573 vs. 0.8518). Tumors measuring 2 cm or less within the T3b category may require downstaging, and a modified T category could improve the precision of prognostic staging compared to the current T category.
1. Introduction
Differentiated thyroid cancer (DTC) is widely recognized for its favorable prognosis due to its low disease-specific mortality (DSM) rate [1,2,3,4,5]. Despite the generally low DSM of DTC, the American Joint Committee on Cancer/Union for International Cancer Control (AJCC/UICC) TNM staging system determines each tumor (T), regional lymph node (N), and distant metastasis (M) category based on their impact on disease-specific survival (DSS) [6,7,8]. Therefore, the AJCC/UICC TNM staging system should clearly indicate the stratification of DSS corresponding to each disease stage. The current eighth edition of the AJCC/TNM staging system primarily differentiates between T1, T2, and T3a based on tumor size [9,10,11]. However, the classifications of T3b, T4a, and T4b are determined by the presence of cancer invasion into the surrounding structures. Specifically, T3b is defined by gross extrathyroidal extension (gETE) into the strap muscles, determined by the surgeon’s visual assessment, irrespective of the tumor size [9,12,13,14,15].
In 2017, the redefinition of T3b was based on gETE rather than minimal ETE (mETE). In response to this, numerous studies have been conducted to validate the change in the T3b classification [16,17,18,19,20,21,22]. Several studies suggest that gETE limited only to the strap muscles does not affect the prognosis [16,18,19,20,21], while other research indicates that it significantly worsens the prognosis [23,24,25,26]. Such inconsistent results may be due to overlooking the impact of the tumor size in T3b. Several studies have evaluated the influence of T3b based on the size of the primary tumor [19,20,21]. In our prior institutional research, we established that there was no difference in recurrence rates between T3b with a small tumor size and T2 disease [17]. However, the study was constrained by limitations, such as solely investigating disease-free survival (DFS) instead of DSS, and omitting T1 and T3a. Building on these findings, our objective is to elucidate the impact of T3b across all tumor size categories. We conducted a thorough prognosis assessment covering DFS, DSS, and overall survival (OS) across not only T2, but also T1 and T3a categories.
This study aimed to clarify the significance of tumor size in T3b on the DFS and DSS of DTC through comparing T3b subcategories with other T categories and by analyzing the risk factors for DSM. Ultimately, our goal is to propose a modified T category.
2. Materials and Methods
2.1. Patients
We conducted a retrospective review on 6811 patients with DTC who underwent thyroid surgery at Seoul St. Mary’s Hospital (Seoul, South Korea) from September 2000 to December 2017. The exclusion criteria for this study included 31 patients detected with distant metastasis at the time of their initial diagnosis, 231 patients who underwent initial surgery at other hospitals, 182 patients with incomplete data, and 85 patients lost to follow-up. Ultimately, a total of 6282 patients were incorporated into the study (Figure 1). Clinicopathological information was validated through pathologic reports, with the exception of T3b, which was confirmed intraoperatively by the surgeons [17]. This study was conducted in accordance with the principles stated in the Declaration of Helsinki (revised in 2013). The Institutional Review Board of Seoul St. Mary’s Hospital at the Catholic University of Korea has approved the research protocol (IRB No: KC22RISI0611 and date of approval: 30 August 2022), and due to the retrospective nature of the study, the requirement for informed consent was waived.
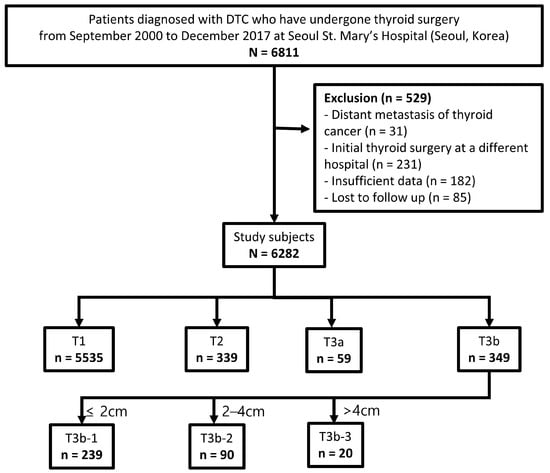
Figure 1.
Participant flow diagram of patient selection and T3b subcategories.
2.2. Subcategories of T3b Category
To analyze the impact of tumor size on T3b, it was divided based on the size criteria that differentiate the traditional classifications of T1, T2, and T3a. Therefore, T3b was subdivided into T3b-1 (≤2 cm), T3b-2 (2–4 cm), and T3b-3 (>4 cm), and these were included in the T subcategories. (Figure 1).
2.3. Perioperative Management and Follow-Up Evaluation
All patients received preoperative evaluation and follow-up in accordance with the 2015 ATA management guidelines [27]. Physical examinations, serum thyroid function tests, thyroglobulin, and anti-thyroglobulin antibody measurements were performed at 2 weeks, 3 months, and 6 months after surgery, and were subsequently conducted annually. Neck ultrasound was conducted annually. Patients who needed additional radioactive iodine (RAI) ablation underwent treatment at least 12 weeks post-thyroidectomy, and whole-body scans were conducted approximately 1 week following the RAI ablation. Patients suspected of recurrence underwent additional imaging procedures, such as computed tomography, positron emission tomography/computed tomography, and RAI whole-body scans, to determine the location and severity of the recurrence. The confirmation of disease recurrence was accomplished through a pathological diagnosis from ultrasound-guided fine-needle aspiration/core needle biopsy or surgical biopsy. The mortality rate data were supplied by the Cancer Center Operations Team at Seoul St. Mary’s Hospital and Central Cancer Registry data, which is based on death records from the Korean Statistical Office.
2.4. Primary and Secondary Endpoints
The primary endpoint was a comparison of DSS and DFS among the subclassified T categories, and the secondary endpoint was the predictive accuracy of DSS between the traditional and newly modified T categories.
2.5. Statistical Analysis
Continuous variables are represented by means and standard deviations, and numbers described in percentages represent categorical variables. Student’s t-test was used to compare continuous variables. To investigate the differences in categorical features among T subcategories, either Pearson’s chi-square test or Fisher’s exact test was used. Univariate and multivariate Cox regression models were utilized to validate significant DSS predictors. The hazard ratios (HR) and their 95% confidence intervals (CI) were calculated. Kaplan–Meier survival curves were plotted for DSS, DFS, and OS, and statistically significant differences were identified using a log-rank test. To assess the predictive capability of the newly modified T categories, Harrell’s concordance index (c-index) [28] and the time-dependent Receiver Operating Characteristic (ROC) curve analysis, as explained by Heagerty et al. [29], were utilized to compute the integrated area under the curve (AUC). Differences with p-values less than 0.05 were deemed to be statistically significant. Statistical analyses were conducted using the Statistical Package for the Social Sciences (version 24.0) and R software (version 4.3.1).
3. Results
3.1. Baseline Characteristics and Comparisons between T Categories and T3b Subcategories According to Size Range
Table 1 shows the baseline characteristics of the study population. The average age was 46.6 years (range, 11–88), and the male-to-female ratio was 1:3.8. According to the traditional T category, 5535 patients (88.1%) were classified as T1, 339 (5.4%) as T2, 59 (0.9%) as T3a, and 349 (5.6%) as T3b. Based on the T3b subcategories, the 349 patients classified as T3b were further subdivided into 239 (3.8%) as T3b-1, 90 (1.4%) as T3b-2, and 20 (0.3%) as T3b-3. The average duration of the follow-up investigation was 119.2 ± 31.7 months (range, 1–226 months).

Table 1.
Baseline clinicopathological characteristics of the study population.
Supplementary Table S1 illustrates the comparison of baseline characteristics between T categories and T3b subcategories within the same size range (T1 vs. T3b-1, T2 vs. T3b-2, and T3a vs. T3b-3). The gETE to the strap muscles had a significant impact on DSM only in cases with tumors > 2 cm (Supplementary Table S1). In tumors ≤ 2 cm, T3b-1 tumors showed no significant difference compared to T1 in overall mortality (OM) and DSM. Within the size range of 2–4 cm, T3b-2 tumors showed an increase in disease severity markers such as multifocality, lymphatic invasion, and BRAFV600E positivity compared to T2 tumors. Furthermore, in T3b-2, more advanced N categories and TNM stages were recorded. Notably, in T3b-2, there was a significant increase in both OM (11.1% vs. 3.5%; p = 0.012) and DSM (6.7% vs. 0.6%; p = 0.001) compared to T2. For tumors larger than 4 cm, the severity of the disease in T3b-3 tumors increased compared to T3a. The rates of both OM (30.0% vs. 6.8%; p = 0.014) and DSM (25.0% vs. 1.7%; p = 0.003) were significantly higher in T3b-3 compared to T3a.
3.2. Univariate and Multivariate Analyses for Disease-Specific Mortality Risk Factors
As indicated in Table 2, for tumors ≤ 2 cm (T1 or T3b-1), the gETE to the strap muscles did not have a significant impact on DSM (HR, 2.754; CI, 0.344–22.036; p = 0.340). The univariate analysis identified age and tumor size as significant risk factors. However, in the multivariate analysis, only age was identified as an independent risk factor (HR, 1.165; CI, 1.086–1.250; p < 0.001).
Table 2.
Univariate and multivariate analyses of disease-specific mortality risk factors in patients with T1 and T3b-1 (≤2 cm).
As indicated in Table 3, regarding tumors in a size range of 2–4 cm (T2 or T3b-2), age, vascular invasion, and T category emerged as significant risk factors for DSM in the univariate analysis. The multivariate analysis reaffirmed the significance of age (HR, 1.088; CI, 1.026–1.154; p = 0.005), vascular invasion (HR, 15.159; CI, 3.511–65.450; p < 0.001), and T category (HR, 11.173; CI, 2.120–58.867; p = 0.004), emphasizing that the DSM risk for T3b-2 is higher than that for T2.
Table 3.
Univariate and multivariate analyses of disease-specific mortality risk factors in patients with T2 and T3b-2 (2–4 cm).
As detailed in Table 4, for tumors larger than 4 cm (T3a or T3b-3), age, tumor size, and T category were identified as significant risk factors for DSM in the univariate analysis. In line with this, the multivariate analysis indicated that age (HR, 1.069; CI, 1.008–1.134; p = 0.027), tumor size (HR, 2.131; CI, 1.253–3.626; p = 0.005), and T category (HR, 28.902; CI, 1.984–421.006; p = 0.014) maintained their significance. Results in Table 3 and Table 4 underscored that gETE into the strap muscle significantly increased the DSM risk in tumors larger than 2 cm.
Table 4.
Univariate and multivariate analyses of disease-specific mortality risk factors in patients with T3a and T3b-3 (>4 cm).
3.3. Revision of T Category Based on Survival Analysis of T3b Subcategories
In Figure 2, we conduct an analysis of DSS, DFS, and OS based on the categories T1, T2, T3a, T3b-1, T3b-2, and T3b-3. In the DSS curve analysis, T3b-1, which is characterized by a smaller primary tumor size, demonstrated a higher DSS compared to T2 (log-rank p < 0.001) (Figure 2a). In the survival curve analysis for DFS and OS, T3b-1 consistently exhibited a higher DSS than T2 (log-rank p < 0.001) (Figure 2b,c). As a result, in all aspects of DSS, DFS, and OS, the survival curves were arranged in the sequence of T1, T3b-1, T2, T3a, T3b-2, and T3b-3.
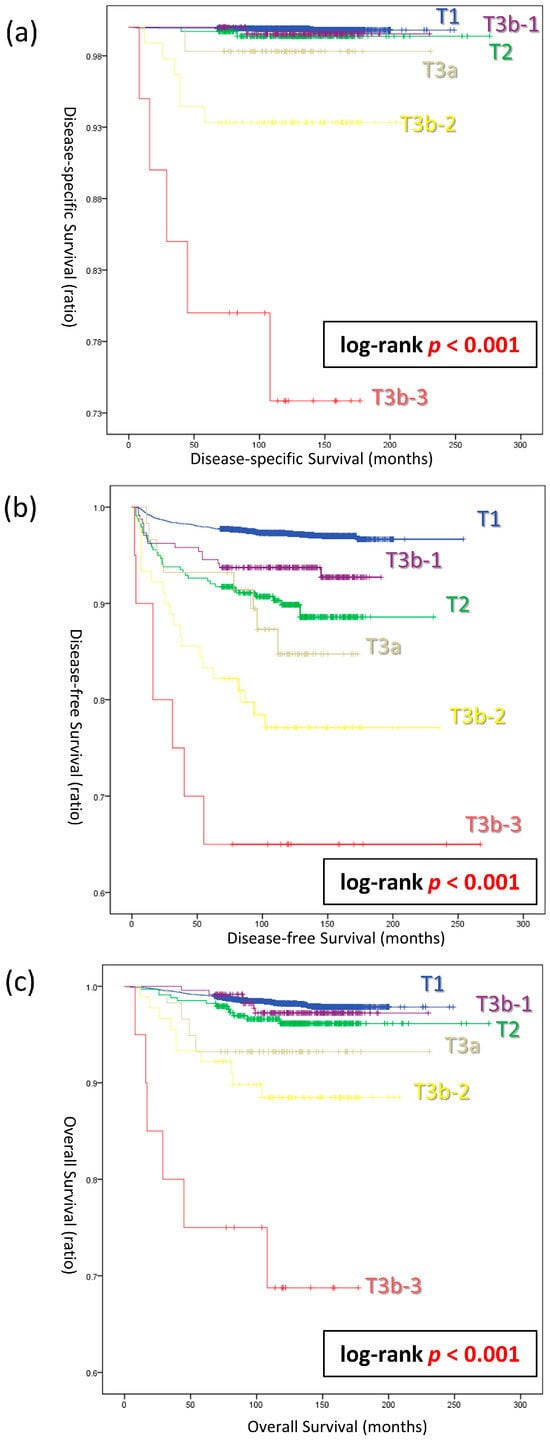
Figure 2.
Survival analysis based on T3b subcategories. (a) Disease-specific survival curves (log-rank p < 0.001). (b) Disease-free survival curves (log-rank p < 0.001). (c) Overall survival curves (log-rank p < 0.001).
Based on the results shown in Table 2, Table 3 and Table 4 and Figure 2, tumors measuring 2 cm or less were classified as ‘T1’, regardless of the presence or absence of strap muscle invasion (Figure 3). Only for tumors larger than 2 cm, those infiltrating the strap muscles have been newly defined as T3b′ in the proposed modified category. DSS curves were plotted for both the classic T categories (T1, T2, T3a, and T3b) and the modified T categories (T1′, T2′, T3a′, and T3b′). Both staging systems stratifying DSS in the sequence of T1, T2, T3a, and T3b (T1′, T2′, T3a′, and T3b′). However, a significant difference in DSS between T3a′ and T3b-3′ was observed only in the modified T categories (log-rank p = 0.048).
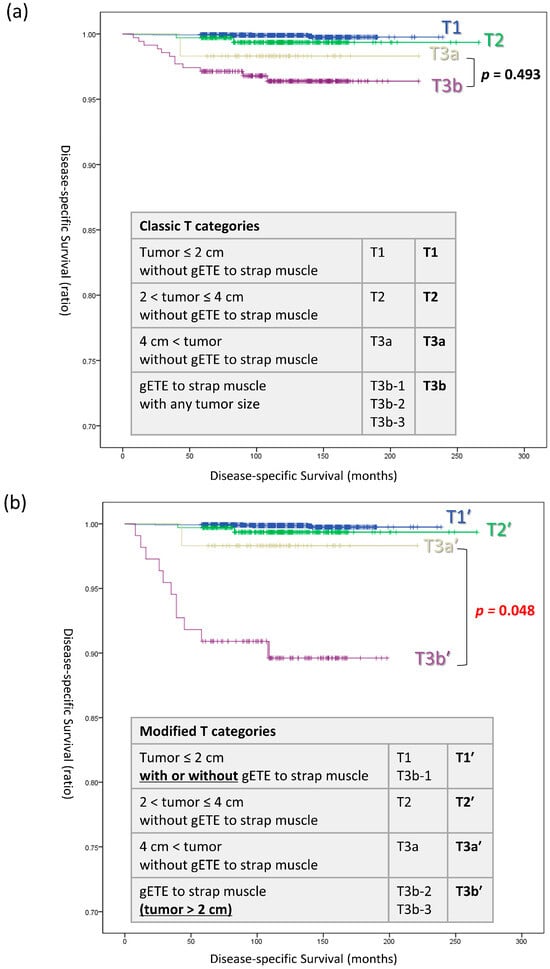
Figure 3.
Disease-specific survival curves in (a) classic T categories and (b) modified T categories. Abbreviations: T, tumor; gETE, gross extrathyroidal extension.
3.4. Predictive Performance of Classic vs. Modified T Categories for DSS
Table 5 presents the Harrell’s c-index and the AUC of the time-dependent ROC, used to compare the predictive capabilities of the classic T category and the modified T category for DSS. Harrell’s c-index was higher in the modified T category than in the classic T category (0.8961 vs. 0.8959). The AUC of the time-dependent ROC for 5-year DSS was also higher in the modified T category compared to the classic T category (AUC, 0.8573 vs. 0.8518).
Table 5.
Comparison of Staging systems in Classic T categories and Modified T categories.
4. Discussion
This study demonstrates the clinical significance of tumor size in the T3b category of DTC. In cases where the tumor is ≤2 cm, there was no significant difference between DSM and OM, regardless of the presence or absence of gETE. In multivariate analyses, it was emphasized that the T3b category significantly impacts the DSM risk only in tumors larger than 2 cm, underscoring the importance of size in determining the prognosis in the T3b category. In the survival curves, including DSS, DFS, and OS, they were consistently ranked in the following order: T1, T3b-1, T2, T3a, T3b-2, and T3b-3. In summary, the modified T category, which incorporated T3b-1 into the new T1′ category, demonstrated superior predictive capability for DSS compared to the existing T category. These results highlight a significant interaction between the tumor size and gETE to the strap muscles.
DTC, primarily characterized by its favorable prognosis, has been subjected to various classifications over the years, especially concerning the definitions of the T categories [6,12,13,14,30,31]. This debate primarily focuses on the significance of ETE into the strap muscles for staging, especially after its 2017 redefinition. Numerous studies have shown that mETE does not affect the recurrence or mortality in DTC [32,33,34,35,36,37,38]. Therefore, mETE was eliminated from T3, and gETE, which only invades the strap muscle, was classified as T3b. This led to the complete exclusion of the mETE concept in staging [6,8,12,13,14,39]. Despite this, the debate regarding the prognostic impact of gETE continues unabated. Some studies indicate that gETE is a significant risk factor for recurrence and mortality [24,25,26], while other studies suggest that gETE does not impact the prognosis [16,18,19,20,21].
Song et al. reported that there was no significant difference in DSS when comparing cases with gETE to those without gETE [19,21]. The reason is presumed to be that the majority of T3b tumors are under 2 cm in size. In our study, out of 349 patients diagnosed with T3b, 239 patients were classified under T3b-1 with tumors less than 2 cm, accounting for 68.5%. In the classic T category, there was no difference in the DSS between T3a and T3b, which supports the findings of previous studies. However, in the modified T category, when T3b-1 was downstaged to T1, a significant difference was observed in the DSS between T3a′ and T3b′. This reemphasizes that in order to accurately reflect the impact of strap muscle invasion, it is necessary to concurrently evaluate tumor size.
Numerous studies have compared mETE and gETE in patients diagnosed with DTC [35,40,41,42,43]. The fact that mETE and gETE present different prognoses can be extrapolated to explain that the influence of ETE changes according to tumor size. The majority of these studies indicate that the presence of gETE usually suggests a worse prognosis than mETE, including higher rates of recurrence or mortality [35,41,42]. According to the research conducted by Park et al., mETE has a more favorable prognosis than gETE, and the extent of ETE impacts the recurrence of the tumor [43]. This distinction is based on whether it can be seen under a microscope or with the naked eye, but there is a need for a more objective and accurate size standard. According to our study, the criterion is determined to be 2 cm based on the objective results of comprehensive analyses.
Another possible explanation for the varying impact of T3b depending on the tumor size could be that the possibility of complete surgical removal of the tumor may differ based on tumor size. In the MACIS (Metastases, Age, Completeness of resection, Invasion, Size) scoring system, a key indicator for assessing the prognosis of thyroid cancer, the principle of complete resection has been deemed to be significant for a long time [44,45]. However, due to the lack of standardized guidelines regarding the extent of strap muscle resection, many surgeons rely more on visual assessment than on confirming the safe margin through frozen-section analysis, even when they encounter a T3b stage intraoperatively [46]. Khan et al. reported in a study of the National Cancer Database, which involved a large cohort of 14,471 individuals, that the size of a large tumor significantly influenced margin positivity (p = 0.021), and margin positivity significantly decreased survival rates (p = 0.038) [47,48]. If tumor size is less than 2 cm, there is a possibility that the depth of invasion into the strap muscle may also be less, potentially making R0 resection more achievable. Shaha also emphasized the importance of complete resection in gETE [49]. Based on the aforementioned studies, the critical prognostic determinant within gETE may be the completeness of the tumor excision, which is affected by the tumor size.
To the best of our knowledge, there has been no study so far that has subdivided T3b based on tumor size using the same criteria as applied to T1, T2, and T3a. Furthermore, we compared the performance of the new stage with that of the traditional stage. In numerous prior stage comparison studies, Harrell’s c-index has been employed, functioning as an objective measure to evaluate the predictive ability of a model [9,28,50,51]. Furthermore, by calculating the AUC of the time-dependent ROC [29,52], it was demonstrated that the modified T category in this study is superior in evaluating DSS using both evaluation methods.
This study has clear strengths. First, it is emphasized by a comprehensive cohort that includes 6282 patients with DTC, who have been tracked for nearly a decade, providing substantial long-term follow-up. Second, the comprehensive analysis evaluated not only DFS, but also DSS and OS, providing a holistic perspective on prognosis, which includes not only recurrence, but also DSM. It is particularly noteworthy that this study explored the DSM, a crucial indicator ideally suited for evaluating the AJCC-TNM staging system. Finally, a notable characteristic of our research is that it provides objective indicators through the prediction of stage performance using various methodologies, including Harrell’s c-index and time-dependent ROC. This has enabled a comparative analysis between the existing staging and the modified staging, further strengthening the robustness of our research results.
Nonetheless, this study has several limitations. First, this is a retrospective study from a single center, which may carry the potential for selection bias. Second, the evaluation of gETE relied on the surgeon’s visual judgment, introducing a subjective element that could be susceptible to observation bias. Developing a method to evaluate ETE with standardized procedures could provide substantial benefits in the future.
5. Conclusions
In conclusion, T3b with a smaller tumor size (≤2 cm) demonstrated no significant difference in DSS and DFS compared to T1 in the current 8th edition of the AJCC-TNM Staging system. The modified T category, which reclassifies T3b (≤2 cm) as T1, demonstrated a more efficient performance than the existing category. If the smaller T3b is reclassified to T1, the new stage could potentially indicate a better stratification for prognosis, possibly eliminating the need for aggressive treatment.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/cancers16142577/s1, Table S1: Comparisons of baseline characteristics between T categories and T3b subcategories within the same size range (T1 vs. T3b-1, T2 vs. T3b-2, and T3a vs. T3b-3).
Author Contributions
Conceptualization, J.P. and J.S.B.; methodology, K.K., J.S.B. and J.S.K.; software, J.P., S.A. and J.S.B.; validation, J.P. and J.S.B.; formal analysis, J.P. and J.S.B.; investigation, J.P. and J.S.B.; resources, K.K., J.S.B. and J.S.K.; data curation, S.A. and J.P.; writing—original draft preparation, J.P. and J.S.B.; writing—review and editing, all authors; visualization, J.P. and J.S.B.; supervision, K.K. and J.S.K.; project administration, J.S.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki, and was approved by the Institutional Review Board of Seoul St. Mary’s Hospital, The Catholic University of Korea (IRB No: KC22RISI0611; date of approval: 30 August 2022).
Informed Consent Statement
Patient consent was waived due to the retrospective nature of this study.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Acknowledgments
We would like to thank all of the nurses who participated in the surgery and who contributed to this study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Jeon, M.J.; Kim, H.K.; Kim, E.H.; Kim, E.S.; Yi, H.-S.; Kim, T.Y.; Kang, H.-C.; Shong, Y.K.; Kim, W.B.; Kim, B.H. Decreasing disease-specific mortality of differentiated thyroid cancer in Korea: A multicenter cohort study. Thyroid 2018, 28, 1121–1127. [Google Scholar] [CrossRef] [PubMed]
- Jeon, M.J.; Kim, W.G.; Kim, T.H.; Kim, H.K.; Kim, B.H.; Yi, H.-S.; Kim, E.S.; Kim, H.; Kim, Y.N.; Kim, E.H. Disease-specific mortality of differentiated thyroid cancer patients in Korea: A multicenter cohort study. Endocrinol. Metab. 2017, 32, 434–441. [Google Scholar] [CrossRef]
- Correct, P.; Chen, V.W. Endocrine gland cancer. Cancer 1995, 75, 338–352. [Google Scholar] [CrossRef]
- Hay, I. Papillary thyroid cancer. Endocrinol. Metab. Clin. N. Am. 1990, 19, 545–576. [Google Scholar] [CrossRef]
- Degroot, L.J.; Kaplan, E.L.; McCormick, M.; Straus, F.H. Natural history, treatment, and course of papillary thyroid carcinoma. J. Clin. Endocrinol. Metab. 1990, 71, 414–424. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.B.; Edge, S.B.; Greene, F.L.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C. AJCC Cancer Staging Manual; Springer: Berlin/Heidelberg, Germany, 2017; Volume 1024. [Google Scholar]
- Brierley, J.D.; Gospodarowicz, M.K.; Wittekind, C. TNM Classification of Malignant Tumours; John Wiley & Sons: Hoboken, NJ, USA, 2017. [Google Scholar]
- Kim, T.H.; Kim, Y.N.; Kim, H.I.; Park, S.Y.; Choe, J.-H.; Kim, J.-H.; Kim, J.S.; Oh, Y.L.; Hahn, S.Y.; Shin, J.H. Prognostic value of the eighth edition AJCC TNM classification for differentiated thyroid carcinoma. Oral. Oncol. 2017, 71, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Kim, W.G.; Oh, H.-S.; Park, S.; Kwon, H.; Song, D.E.; Kim, T.Y.; Shong, Y.K.; Kim, W.B.; Sung, T.-Y. Comparison of the seventh and eighth editions of the American Joint Committee on Cancer/Union for International Cancer Control tumor-node-metastasis staging system for differentiated thyroid cancer. Thyroid 2017, 27, 1149–1155. [Google Scholar] [CrossRef] [PubMed]
- Nixon, I.J.; Wang, L.Y.; Migliacci, J.C.; Eskander, A.; Campbell, M.J.; Aniss, A.; Morris, L.; Vaisman, F.; Corbo, R.; Momesso, D. An international multi-institutional validation of age 55 years as a cutoff for risk stratification in the AJCC/UICC staging system for well-differentiated thyroid cancer. Thyroid 2016, 26, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Pontius, L.N.; Oyekunle, T.O.; Thomas, S.M.; Stang, M.T.; Scheri, R.P.; Roman, S.A.; Sosa, J.A. Projecting survival in papillary thyroid cancer: A comparison of the seventh and eighth editions of the American Joint Commission on Cancer/Union for International Cancer Control staging systems in two contemporary national patient cohorts. Thyroid 2017, 27, 1408–1416. [Google Scholar] [CrossRef]
- Shteinshnaider, M.; Muallem Kalmovich, L.; Koren, S.; Or, K.; Cantrell, D.; Benbassat, C. Reassessment of differentiated thyroid cancer patients using the eighth TNM/AJCC classification system: A comparative study. Thyroid 2018, 28, 201–209. [Google Scholar] [CrossRef]
- Kim, K.; Kim, J.K.; Lee, C.R.; Kang, S.-W.; Lee, J.; Jeong, J.J.; Nam, K.-H.; Chung, W.Y. Comparison of long-term prognosis for differentiated thyroid cancer according to the 7th and 8th editions of the AJCC/UICC TNM staging system. Ther. Adv. Endocrinol. Metab. 2020, 11, 2042018820921019. [Google Scholar] [CrossRef]
- Cavalheiro, B.G.; de Matos, L.L.; Leite, A.K.N.; Kulcsar, M.A.V.; Cernea, C.R.; Kowalski, L.P. Survival in differentiated thyroid carcinoma: Comparison between the 7th and 8th editions of the AJCC/UICC TNM staging system and the ATA initial risk stratification system. Head. Neck 2021, 43, 2913–2922. [Google Scholar] [CrossRef] [PubMed]
- Xiang, J.; Wang, Z.; Sun, W.; Zhang, H. The new T3b category has clinical significance? SEER-based study. Clin. Endocrinol. 2021, 94, 449–459. [Google Scholar] [CrossRef] [PubMed]
- Amit, M.; Boonsripitayanon, M.; Goepfert, R.P.; Tam, S.; Busaidy, N.L.; Cabanillas, M.E.; Dadu, R.; Varghese, J.; Waguespack, S.G.; Gross, N.D. Extrathyroidal extension: Does strap muscle invasion alone influence recurrence and survival in patients with differentiated thyroid cancer? Ann. Surg. Oncol. 2018, 25, 3380–3388. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Kang, I.K.; Bae, J.S.; Kim, J.S.; Kim, K. Clinical Significance of Tumor Size in Gross Extrathyroidal Extension to Strap Muscles (T3b) in Papillary Thyroid Carcinoma: Comparison with T2. Cancers 2022, 14, 4615. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Kim, H.; Kim, J.; Kim, J.; Oh, Y.; Kim, S.; Chung, J.; Jang, H.; Kim, T. Prognostic significance of gross extrathyroidal extension invading only strap muscles in differentiated thyroid carcinoma. J. Br. Surg. 2018, 105, 1155–1162. [Google Scholar] [CrossRef] [PubMed]
- Song, E.; Lee, Y.-M.; Oh, H.-S.; Jeon, M.J.; Song, D.E.; Kim, T.Y.; Kim, W.B.; Shong, Y.K.; Sung, T.-Y.; Kim, W.G. A relook at the T stage of differentiated thyroid carcinoma with a focus on gross extrathyroidal extension. Thyroid 2019, 29, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.K.; Lee, J.; Kim, E.-K.; Yoon, J.H.; Park, V.Y.; Han, K.; Kwak, J.Y. Strap muscle invasion in differentiated thyroid cancer does not impact disease-specific survival: A population-based study. Sci. Rep. 2020, 10, 18248. [Google Scholar] [CrossRef]
- Song, E.; Kim, W.W.; Jeon, M.J.; Sung, T.-Y.; Song, D.E.; Kim, T.Y.; Chung, K.W.; Kim, W.B.; Shong, Y.K.; Hong, S.J. Clinical significance of gross invasion of strap muscles in patients with 1-to 4-cm-sized papillary thyroid carcinoma undergoing lobectomy. Ann. Surg. Oncol. 2019, 26, 4466–4471. [Google Scholar] [CrossRef]
- Li, G.; Li, R.; Song, L.; Chen, W.; Jiang, K.; Tang, H.; Wei, T.; Li, Z.; Gong, R.; Lei, J. Implications of extrathyroidal extension invading only the strap muscles in papillary thyroid carcinomas. Thyroid 2020, 30, 57–64. [Google Scholar] [CrossRef]
- Zhang, L.; Liu, J.; Wang, P.; Xue, S.; Li, J.; Chen, G. Impact of gross strap muscle invasion on outcome of differentiated thyroid cancer: Systematic review and meta-analysis. Front. Oncol. 2020, 10, 1687. [Google Scholar] [CrossRef] [PubMed]
- Harries, V.; McGill, M.; Yuan, A.; Wang, L.Y.; Tuttle, R.M.; Shaha, A.R.; Shah, J.P.; Wong, R.J.; Patel, S.G.; Ganly, I. Does macroscopic extrathyroidal extension to the strap muscles alone affect survival in papillary thyroid carcinoma? Surgery 2022, 171, 1341–1347. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.W.; Roh, J.-L.; Gong, G.; Cho, K.-J.; Choi, S.-H.; Nam, S.Y.; Kim, S.Y. Extent of extrathyroidal extension as a significant predictor of nodal metastasis and extranodal extension in patients with papillary thyroid carcinoma. Ann. Surg. Oncol. 2017, 24, 460–468. [Google Scholar] [CrossRef] [PubMed]
- Youngwirth, L.M.; Adam, M.A.; Scheri, R.P.; Roman, S.A.; Sosa, J.A. Extrathyroidal extension is associated with compromised survival in patients with thyroid cancer. Thyroid 2017, 27, 626–631. [Google Scholar] [CrossRef] [PubMed]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: The American Thyroid Association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef]
- Harrell, F.E., Jr.; Lee, K.L.; Mark, D.B. Multivariable prognostic models: Issues in developing models, evaluating assumptions and adequacy, and measuring and reducing errors. Stat. Med. 1996, 15, 361–387. [Google Scholar] [CrossRef]
- Heagerty, P.J.; Zheng, Y. Survival model predictive accuracy and ROC curves. Biometrics 2005, 61, 92–105. [Google Scholar] [CrossRef] [PubMed]
- Lang, B.; Lo, C.-Y.; Chan, W.-F.; Lam, K.-Y.; Wan, K.-Y. Restaging of differentiated thyroid carcinoma by the sixth edition AJCC/UICC TNM staging system: Stage migration and predictability. Ann. Surg. Oncol. 2007, 14, 1551–1559. [Google Scholar] [CrossRef]
- Wada, N.; Nakayama, H.; Suganuma, N.; Masudo, Y.; Rino, Y.; Masuda, M.; Imada, T. Prognostic value of the sixth edition AJCC/UICC TNM classification for differentiated thyroid carcinoma with extrathyroid extension. J. Clin. Endocrinol. Metab. 2007, 92, 215–218. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.H.; Ha, T.K.; Park, H.K.; Ahn, M.S.; Kim, K.H.; Bae, K.B.; Kim, T.H.; Choi, C.S.; Kim, T.K.; Bae, S.K. Implication of minimal extrathyroidal extension as a prognostic factor in papillary thyroid carcinoma. Int. J. Surg. 2013, 11, 944–947. [Google Scholar] [CrossRef]
- Nixon, I.J.; Ganly, I.; Patel, S.; Palmer, F.L.; Whitcher, M.M.; Tuttle, R.M.; Shaha, A.R.; Shah, J.P. The impact of microscopic extrathyroid extension on outcome in patients with clinical T1 and T2 well-differentiated thyroid cancer. Surgery 2011, 150, 1242–1249. [Google Scholar] [CrossRef] [PubMed]
- Hay, I.D.; Johnson, T.R.; Thompson, G.B.; Sebo, T.J.; Reinalda, M.S. Minimal extrathyroid extension in papillary thyroid carcinoma does not result in increased rates of either cause-specific mortality or postoperative tumor recurrence. Surgery 2016, 159, 11–21. [Google Scholar] [CrossRef]
- Arora, N.; Turbendian, H.K.; Scognamiglio, T.; Wagner, P.L.; Goldsmith, S.J.; Zarnegar, R.; Fahey, T.J., 3rd. Extrathyroidal extension is not all equal: Implications of macroscopic versus microscopic extent in papillary thyroid carcinoma. Surgery 2008, 144, 942–948. [Google Scholar] [CrossRef] [PubMed]
- Tam, S.; Amit, M.; Boonsripitayanon, M.; Busaidy, N.L.; Cabanillas, M.E.; Waguespack, S.G.; Gross, N.D.; Grubbs, E.G.; Williams, M.D.; Lai, S.Y. Effect of tumor size and minimal extrathyroidal extension in patients with differentiated thyroid cancer. Thyroid 2018, 28, 982–990. [Google Scholar] [CrossRef]
- Rivera, M.; Ricarte-Filho, J.; Tuttle, R.M.; Ganly, I.; Shaha, A.; Knauf, J.; Fagin, J.; Ghossein, R. Molecular, morphologic, and outcome analysis of thyroid carcinomas according to degree of extrathyroid extension. Thyroid 2010, 20, 1085–1093. [Google Scholar] [CrossRef] [PubMed]
- Andersen, P.E.; Kinsella, J.; Loree, T.R.; Shaha, A.R.; Shah, J.P. Differentiated carcinoma of the thyroid with extrathyroidal extension. Am. J. Surg. 1995, 170, 467–470. [Google Scholar] [CrossRef]
- Tuttle, R.M.; Haugen, B.; Perrier, N.D. Updated American Joint Committee on Cancer/Tumor-Node-Metastasis Staging System for Differentiated and Anaplastic Thyroid Cancer: What Changed and Why? Mary Ann Liebert, Inc.: New Rochelle, NY, USA, 2017; Volume 27, pp. 751–756. [Google Scholar]
- Danilovic, D.L.; Castroneves, L.A.; Suemoto, C.K.; Elias, L.O.; Soares, I.C.; Camargo, R.Y.; Correa, F.A.; Hoff, A.O.; Marui, S. Is there a difference between minimal and gross extension into the strap muscles for the risk of recurrence in papillary thyroid carcinomas? Thyroid 2020, 30, 1008–1016. [Google Scholar] [CrossRef]
- Ito, Y.; Tomoda, C.; Uruno, T.; Takamura, Y.; Miya, A.; Kobayashi, K.; Matsuzuka, F.; Kuma, K.; Miyauchi, A. Prognostic significance of extrathyroid extension of papillary thyroid carcinoma: Massive but not minimal extension affects the relapse-free survival. World J. Surg. 2006, 30, 780–786. [Google Scholar] [CrossRef]
- Radowsky, J.S.; Howard, R.S.; Burch, H.B.; Stojadinovic, A. Impact of degree of extrathyroidal extension of disease on papillary thyroid cancer outcome. Thyroid 2014, 24, 241–244. [Google Scholar] [CrossRef]
- Park, J.S.; Chang, J.W.; Liu, L.; Jung, S.-N.; Koo, B.S. Clinical implications of microscopic extrathyroidal extension in patients with papillary thyroid carcinoma. Oral. Oncol. 2017, 72, 183–187. [Google Scholar] [CrossRef]
- Dwamena, S.; Patel, N.; Egan, R.; Stechman, M.; Scott-Coombes, D. Impact of the change from the seventh to eighth edition of the AJCC TNM classification of malignant tumours and comparison with the MACIS prognostic scoring system in non-medullary thyroid cancer. BJS Open 2019, 3, 623–628. [Google Scholar] [CrossRef] [PubMed]
- Hay, I.D.; Bergstralh, E.J.; Goellner, J.R.; Ebersold, J.R.; Grant, C.S. Predicting outcome in papillary thyroid carcinoma: Development of a reliable prognostic scoring system in a cohort of 1779 patients surgically treated at one institution during 1940 through 1989. Surgery 1993, 114, 1050–1058. [Google Scholar] [PubMed]
- Park, J.-O.; Kim, J.H.; Joo, Y.H.; Kim, S.-Y.; Kim, G.-J.; Kim, H.B.; Lee, D.-H.; Hong, H.J.; Park, Y.M.; Chung, E.-J. Guideline for the Surgical Management of Locally Invasive Differentiated Thyroid Cancer From the Korean Society of Head and Neck Surgery. Clin. Exp. Otorhinolaryngol. 2023, 16, 1–19. [Google Scholar] [CrossRef]
- Khan, Z.F.; Kutlu, O.; Picado, O.; Lew, J.I. Margin positivity and survival outcomes: A review of 14,471 patients with 1-cm to 4-cm papillary thyroid carcinoma. J. Am. Coll. Surg. 2021, 232, 545–550. [Google Scholar] [CrossRef] [PubMed]
- Bearelly, S.; Morris-Wiseman, L.F. Interpreting Microscopic Positive Margins in Differentiated Thyroid Cancer. Clin. Thyroidol. 2021, 33, 184–186. [Google Scholar] [CrossRef]
- Shaha, A.R. Extrathyroidal extension—What does it mean. Oral. Oncol. 2017, 68, 50–52. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Kim, Y.N.; Kim, W.G.; Park, S.; Kwon, H.; Jeon, M.J.; Ahn, H.S.; Jung, S.H.; Kim, S.W.; Kim, W.B. Optimal cut-off age in the TNM Staging system of differentiated thyroid cancer: Is 55 years better than 45 years? Clin. Endocrinol. 2017, 86, 438–443. [Google Scholar] [CrossRef] [PubMed]
- Sapuppo, G.; Grasso, S.; Di Benedetto, G.; Belfiore, A.; Pellegriti, G. Prospective study and proposal of an outcome predictive nomogram in a consecutive prospective series of differentiated thyroid cancer based on the new ATA risk categories and TNM. Front. Endocrinol. 2023, 14, 1128963. [Google Scholar] [CrossRef]
- Ma, Q.; Chen, Z.; Fang, Y.; Wei, X.; Wang, N.; Zhou, X.; Li, S.; Ying, C. Development and validation of survival nomograms for patients with differentiated thyroid cancer with distant metastases: A SEER Program-based study. J. Endocrinol. Investig. 2023, 47, 115–129. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).