
The 3-Biomarker Classifier—A Novel and Simple Molecular Risk Score Predicting Overall Survival in Patients with Colorectal Cancer

 , , , , ,
, , , , , 
Abstract
Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Patients and Data Retrieval
2.2. Statistics
- 3-biomarker classifier: high/very high risk vs. low/intermediate risk
- pT-status: T3/4 vs. T1/2
- Grade: G3/4 vs. G1/2
- Nodal status: pN+ vs. pN0
- Localization: right vs. left/transversum
3. Results
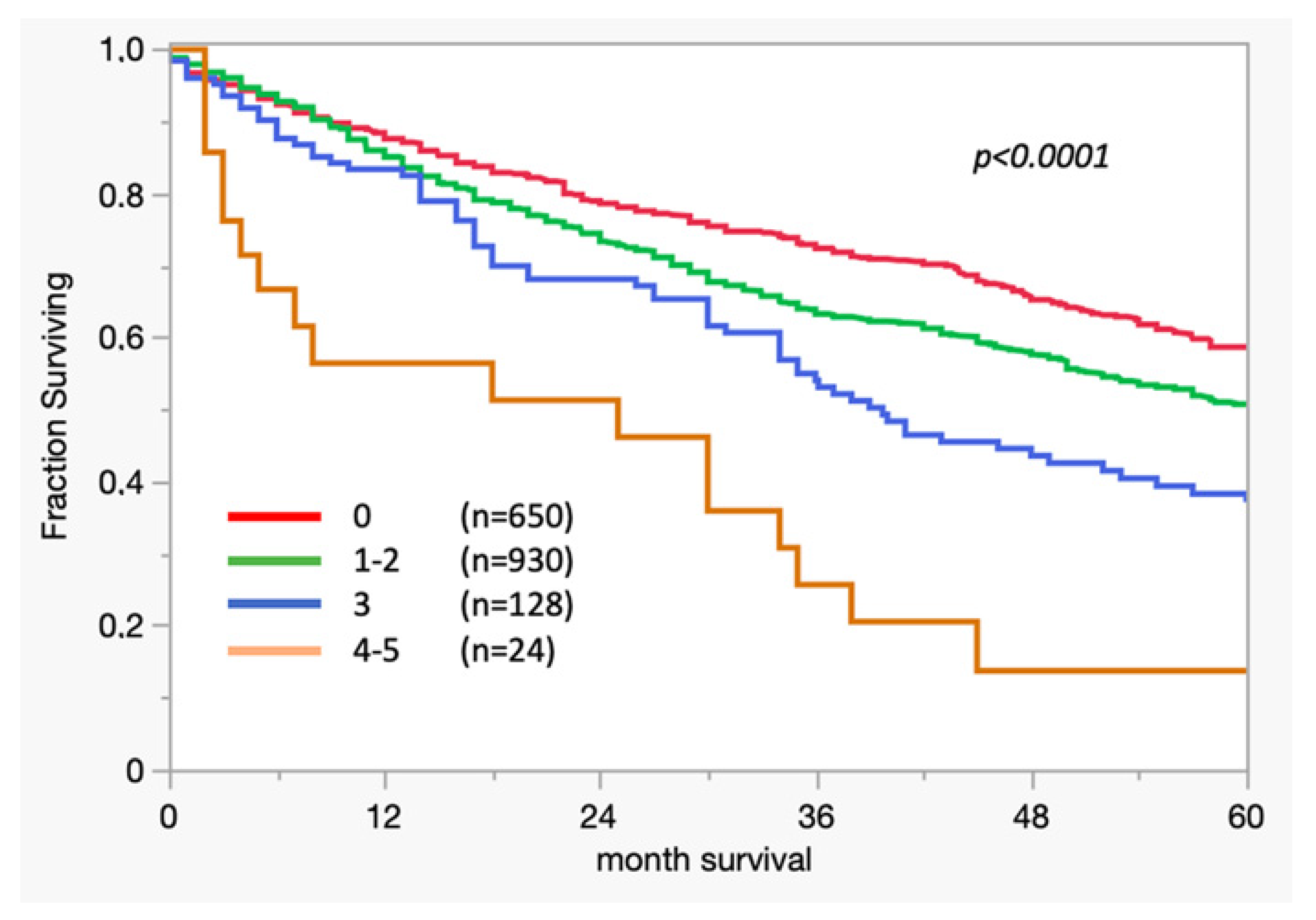
3.1. Survival Analysis
3.2. Cox Regression
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F.; Bsc, M.F.B.; Me, J.F.; Soerjomataram, M.I.; et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Gill, S.; Loprinzi, C.L.; Sargent, D.J.; Thomé, S.D.; Alberts, S.R.; Haller, D.G.; Benedetti, J.; Francini, G.; Shepherd, L.E.; Francois Seitz, J.; et al. Pooled analysis of fluorouracil-based adjuvant therapy for stage II and III colon cancer: Who benefits and by how much? J. Clin. Oncol. 2004, 22, 1797–1806. [Google Scholar] [CrossRef]
- Tosi, F.; Magni, E.; Amatu, A.; Mauri, G.; Bencardino, K.; Truini, M.; Veronese, S.; De Carlis, L.; Ferrari, G.; Nichelatti, M.; et al. Effect of KRAS and BRAF Mutations on Survival of Metastatic Colorectal Cancer After Liver Resection: A Systematic Review and Meta-Analysis. Clin. Color. Cancer 2017, 16, e153–e163. [Google Scholar] [CrossRef]
- Cunningham, D.; Atkin, W.; Lenz, H.-J.; Lynch, H.T.; Minsky, B.; Nordlinger, B.; Starling, N. Colorectal cancer. Lancet 2010, 375, 1030–1047. [Google Scholar] [CrossRef]
- Hyslop, T.; Waldman, S.A. Molecular staging of node negative patients with colorectal cancer. J. Cancer 2013, 4, 193–199. [Google Scholar] [CrossRef]
- Melling, N.; Simon, R.; Mirlacher, M.; Izbicki, J.R.; Stahl, P.; Terracciano, L.M.; Bokemeyer, C.; Sauter, G.; Marx, A.H. Loss of RNA-binding motif protein 3 expression is associated with right-sided localization and poor prognosis in colorectal cancer. Histopathology 2016, 68, 191–198. [Google Scholar] [CrossRef]
- Melling, N.; Kowitz, C.M.; Simon, R.; Bokemeyer, C.; Terracciano, L.; Sauter, G.; Izbicki, J.R.; Marx, A.H. High Ki67 expression is an independent good prognostic marker in colorectal cancer. J. Clin. Pathol. 2016, 69, 209–214. [Google Scholar] [CrossRef]
- Melling, N.; Grimm, N.; Simon, R.; Stahl, P.; Bokemeyer, C.; Terracciano, L.; Sauter, G.; Izbicki, J.R.; Marx, A.H. Loss of H2Bub1 Expression is Linked to Poor Prognosis in Nodal Negative Colorectal Cancers. Pathol. Oncol. Res. 2016, 22, 95–102. [Google Scholar] [CrossRef]
- Marsh, D.J.; Ma, Y.; Dickson, K.A. Histone Monoubiquitination in Chromatin Remodelling: Focus on the Histone H2B Interactome and Cancer. Cancers 2020, 12, 3462. [Google Scholar] [CrossRef]
- Sadeghi, L.; Siggens, L.; Svensson, J.P.; Ekwall, K. Centromeric histone H2B monoubiquitination promotes noncoding transcription and chromatin integrity. Nat. Struct. Mol. Biol. 2014, 21, 236–243. [Google Scholar] [CrossRef]
- Jonsson, L.; Hedner, C.; Gaber, A.; Korkocic, D.; Nodin, B.; Uhlén, M.; Eberhard, J.; Jirström, K. High expression of RNA-binding motif protein 3 in esophageal and gastric adenocarcinoma correlates with intestinal metaplasia-associated tumours and independently predicts a reduced risk of recurrence and death. Biomark. Res. 2014, 2, 11. [Google Scholar] [CrossRef]
- Jonsson, L.; Bergman, J.; Nodin, B.; Manjer, J.; Pontén, F.; Uhlén, M.; Jirström, K. Low RBM3 protein expression correlates with tumour progression and poor prognosis in malignant melanoma: An analysis of 215 cases from the Malmo Diet and Cancer Study. J. Transl. Med. 2011, 9, 114. [Google Scholar] [CrossRef]
- Jögi, A.; Brennan, D.J.; Rydén, L.; Magnusson, K.; Fernö, M.; Stål, O.; Borgquist, S.; Uhlen, M.; Landberg, G.; Påhlman, S.; et al. Nuclear expression of the RNA-binding protein RBM3 is associated with an improved clinical outcome in breast cancer. Mod. Pathol. 2009, 22, 1564–1574. [Google Scholar] [CrossRef]
- Siesing, C.; Sorbye, H.; Dragomir, A.; Pfeiffer, P.; Qvortrup, C.; Pontén, F.; Jirström, K.; Glimelius, B.; Eberhard, J. High RBM3 expression is associated with an improved survival and oxaliplatin response in patients with metastatic colorectal cancer. PLoS ONE 2017, 12, e0182512. [Google Scholar] [CrossRef]
- Gerdes, J.; Lemke, H.; Baisch, H.; Wacker, H.H.; Schwab, U.; Stein, H. Cell cycle analysis of a cell proliferation-associated human nuclear antigen defined by the monoclonal antibody Ki-67. J. Immunol. 1984, 133, 1710–1715. [Google Scholar] [CrossRef]
- Pavel, M.; Öberg, K.; Falconi, M.; Krenning, E.P.; Sundin, A.; Perren, A.; Berruti, A. Gastroenteropancreatic neuroendocrine neoplasms: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 844–860. [Google Scholar] [CrossRef]
- Bubendorf, L.; Tapia, C.; Gasser, T.C.; Casella, R.; Grunder, B.; Moch, H.; Mihatsch, M.J.; Sauter, G. Ki67 labeling index in core needle biopsies independently predicts tumor-specific survival in prostate cancer. Hum. Pathol. 1998, 29, 949–954. [Google Scholar] [CrossRef]
- Sun, J.; Zhao, J.; Jiang, F.; Wang, L.; Xiao, Q.; Han, F.; Chen, J.; Yuan, S.; Wei, J.; Larsson, S.C.; et al. Identification of novel protein biomarkers and drug targets for colorectal cancer by integrating human plasma proteome with genome. Genome Med. 2023, 15, 75. [Google Scholar] [CrossRef]
- Guan, B.; Xu, M.; Zheng, R.; Guan, G.; Xu, B. Novel biomarkers to predict treatment response and prognosis in locally advanced rectal cancer undergoing neoadjuvant chemoradiotherapy. BMC Cancer 2023, 23, 1099. [Google Scholar] [CrossRef]
- Bresalier, R.S.; Grady, W.M.; Markowitz, S.D.; Nielsen, H.J.; Batra, S.K.; Lampe, P.D. Biomarkers for Early Detection of Colorectal Cancer: The Early Detection Research Network, a Framework for Clinical Translation. Cancer Epidemiol. Biomark. Prev. 2020, 29, 2431–2440. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Luo, J.; Yang, W.; Ye, W.C. CircRNAs in colorectal cancer: Potential biomarkers and therapeutic targets. Cell Death Dis. 2023, 14, 353. [Google Scholar] [CrossRef] [PubMed]
- Waldman, S.A.; Hyslop, T.; Schulz, S.; Barkun, A.; Nielsen, K.; Haaf, J.; Bonaccorso, C.; Li, Y.; Weinberg, D.S. Association of GUCY2C expression in lymph nodes with time to recurrence and disease-free survival in pN0 colorectal cancer. JAMA 2009, 301, 745–752. [Google Scholar] [CrossRef]
- Mejia, A.; Schulz, S.; Hyslop, T.; Weinberg, D.S.; Waldman, S.A. Molecular staging estimates occult tumor burden in colorectal cancer. Adv. Clin. Chem. 2010, 52, 19–39. [Google Scholar]
- Wang, S.; Guan, X.; Ma, M.; Zhuang, M.; Ma, T.; Liu, Z.; Chen, H.; Jiang, Z.; Chen, Y.; Wang, G.; et al. Reconsidering the prognostic significance of tumour deposit count in the TNM staging system for colorectal cancer. Sci. Rep. 2020, 10, 89. [Google Scholar] [CrossRef]
- Ahluwalia, P.; Mondal, A.K.; Bloomer, C.; Fulzele, S.; Jones, K.; Ananth, S.; Gahlay, G.K.; Heneidi, S.; Rojiani, A.M.; Kota, V.; et al. Identification and Clinical Validation of a Novel 4 Gene-Signature with Prognostic Utility in Colorectal Cancer. Int. J. Mol. Sci. 2019, 20, 3818. [Google Scholar] [CrossRef]
- Gao, G.; Shi, X.; Long, Y.; Yao, Z.; Shen, J.; Shen, L. The prognostic and clinicopathological significance of RBM3 in the survival of patients with tumor: A Prisma-compliant meta-analysis. Medicine 2020, 99, e20002. [Google Scholar] [CrossRef]
- Sugai, T.; Yamada, N.; Osakabe, M.; Hashimoto, M.; Uesugi, N.; Eizuka, M.; Tanaka, Y.; Sugimoto, R.; Yanagawa, N.; Matsumoto, T. Microenvironmental markers are correlated with lymph node metastasis in invasive submucosal colorectal cancer. Histopathology 2021, 79, 584–598. [Google Scholar] [CrossRef]
- Tarcic, O.; Pateras, I.S.; Cooks, T.; Shema, E.; Kanterman, J.; Ashkenazi, H.; Boocholez, H.; Hubert, A.; Rotkopf, R.; Baniyash, M.; et al. RNF20 Links Histone H2B Ubiquitylation with Inflammation and Inflammation-Associated Cancer. Cell Rep. 2016, 14, 1462–1476. [Google Scholar] [CrossRef]
- Mahar, A.L.; Compton, C.; Halabi, S.; Hess, K.R.; Weiser, M.R.; Groome, P.A. Personalizing prognosis in colorectal cancer: A systematic review of the quality and nature of clinical prognostic tools for survival outcomes. J. Surg. Oncol. 2017, 116, 969–982. [Google Scholar] [CrossRef] [PubMed]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): The TRIPOD Statement. BMC Med. 2015, 13, 1. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Clinical/Pathological Features | n Available | |
|---|---|---|
| Gender | Female | 898 |
| Male | 893 | |
| Age | Mean: 69 (29–96) | |
| Tumor grade | G1 | 33 |
| G2 | 1497 | |
| G3 | 242 | |
| Tumor stage | pT1 | 80 |
| pT2 | 283 | |
| pT3 | 1143 | |
| pT4 | 269 | |
| Nodal status | pN0 | 909 |
| pN1 | 448 | |
| pN2 | 392 | |
| Tumor type | Tubular carcinoma | 1264 |
| Mucinous carcinoma | 119 | |
| Others | 22 | |
| Localization | Right colon | 355 |
| Transverse colon | 134 | |
| Left colon | 418 | |
| Rectum | 482 | |
| Total number of patients (n evaluable) | 1791 | |
| 3-Biomarker Classifier Risk | ||||||
|---|---|---|---|---|---|---|
| Parameter | n Evaluable | Low (%) | Intermediate (%) | High (%) | Very High (%) | p Value |
| All cancers | 2212 | 993 (44.9) | 1061 (48.0) | 130 (5.9) | 28 (1.2) | |
| Tumor stage | <0.0001 | |||||
| pT1 | 80 | 47 (58.8) | 31 (38.8) | 2 (2.5) | 0 (0.0) | |
| pT2 | 283 | 126 (44.5) | 141 (49.8) | 16 (5.7) | 0 (0.0) | |
| pT3 | 1143 | 428 (37.4) | 623 (54.5) | 81 (7.1) | 11 (1.0) | |
| pT4 | 269 | 74 (27.5) | 154 (57.2) | 28 (10.4) | 13 (4.8) | |
| Lymph node metastasis | 0.2559 | |||||
| pN0 | 909 | 353 (38.8) | 492 (54.1) | 58 (6.4) | 6 (0.7) | |
| pN1 | 448 | 168 (37.5) | 237 (52.9) | 35 (7.8) | 8 (1.8) | |
| pN2 | 392 | 142 (36.2) | 208 (53.1) | 32 (8.2) | 10 (2.6) | |
| Grading | 0.0065 | |||||
| G1 | 33 | 20 (60.6) | 13 (39.4) | 0 (0.0) | 0 (0.0) | |
| G2 | 1497 | 550 (36.7) | 821 (54.8) | 109 (7.3) | 16 (1.1) | |
| G3 | 242 | 105 (43.4) | 114 (47.1) | 17 (7.0) | 6 (2.5) | |
| Tumor localization | 0.2130 | |||||
| Right | 355 | 132 (37.2) | 184 (51.8) | 29 (8.2) | 10 (2.8) | |
| Transverse | 134 | 42 (31.3) | 72 (53.7) | 16 (11.9) | 4 (3.0) | |
| Left | 418 | 148 (35.4) | 240 (57.4) | 25 (6.0) | 5 (1.2) | |
| Rectum | 482 | 173 (35.9) | 267 (55.4) | 37 (7.7) | 5 (1.0) | |
| Histological type | 0.1805 | |||||
| Adenocarcinoma | 1264 | 442 (35.0) | 704 (55.7) | 96 (7.6) | 21 (1.7) | |
| Mucinous | 119 | 53 (44.5) | 58 (48.7) | 8 (6.7) | 0 (0.0) | |
| Others | 22 | 9 (40.9) | 10 (45.5) | 2 (9.1) | 1 (4.5) | |
| Peritumoral lymphocytes | 0.1453 | |||||
| Absent | 787 | 297 (37.7) | 427 (54.3) | 52 (6.6) | 11 (1.4) | |
| Present | 602 | 198 (32.9) | 339 (56.3) | 54 (9.0) | 11 (1.8) | |
| Vascular invasion | 0.0022 | |||||
| No | 783 | 299 (38.2) | 428 (54.7) | 50 (6.4) | 6 (0.8) | |
| Yes | 605 | 196 (32.4) | 337 (55.7) | 56 (9.3) | 16 (2.6) | |
| 3-Biomarker-Classifier | Tumor Status | Grading | Nodal Status | Tumor Localization | |
|---|---|---|---|---|---|
| High/Very High Risk vs. Low/Intermediate Risk | T3/4 vs. T1/2 | G3/4 vs. G1/2 | pN+ vs. pN0 | Right vs. Left/Transversum | |
| Hazard Ratio | 1.45 | 2.23 | 1.32 | 2.49 | 1.00 |
| p-value | 0.0016 | <0.001 | 0.0126 | <0.001 | 0.9618 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Melling, N.; Fard-Aghaie, M.H.; Hube-Magg, C.; Kluth, M.; Simon, R.; Tachezy, M.; Ghadban, T.; Reeh, M.; Izbicki, J.R.; Sauter, G.; et al. The 3-Biomarker Classifier—A Novel and Simple Molecular Risk Score Predicting Overall Survival in Patients with Colorectal Cancer. Cancers 2024, 16, 3223. https://doi.org/10.3390/cancers16183223
Melling N, Fard-Aghaie MH, Hube-Magg C, Kluth M, Simon R, Tachezy M, Ghadban T, Reeh M, Izbicki JR, Sauter G, et al. The 3-Biomarker Classifier—A Novel and Simple Molecular Risk Score Predicting Overall Survival in Patients with Colorectal Cancer. Cancers. 2024; 16(18):3223. https://doi.org/10.3390/cancers16183223
Chicago/Turabian StyleMelling, Nathaniel, Mohammad H. Fard-Aghaie, Claudia Hube-Magg, Martina Kluth, Ronald Simon, Michael Tachezy, Tarik Ghadban, Matthias Reeh, Jakob R. Izbicki, Guido Sauter, and et al. 2024. "The 3-Biomarker Classifier—A Novel and Simple Molecular Risk Score Predicting Overall Survival in Patients with Colorectal Cancer" Cancers 16, no. 18: 3223. https://doi.org/10.3390/cancers16183223
APA StyleMelling, N., Fard-Aghaie, M. H., Hube-Magg, C., Kluth, M., Simon, R., Tachezy, M., Ghadban, T., Reeh, M., Izbicki, J. R., Sauter, G., & Grupp, K. (2024). The 3-Biomarker Classifier—A Novel and Simple Molecular Risk Score Predicting Overall Survival in Patients with Colorectal Cancer. Cancers, 16(18), 3223. https://doi.org/10.3390/cancers16183223