
Distribution of 14 High-Risk HPV Types and p16/Ki67 Dual-Stain Status in Post-Colposcopy Histology Results: Negative, Low- and High-Grade Cervical Squamous Intraepithelial Lesions

 , , , ,
, , , ,  and
and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
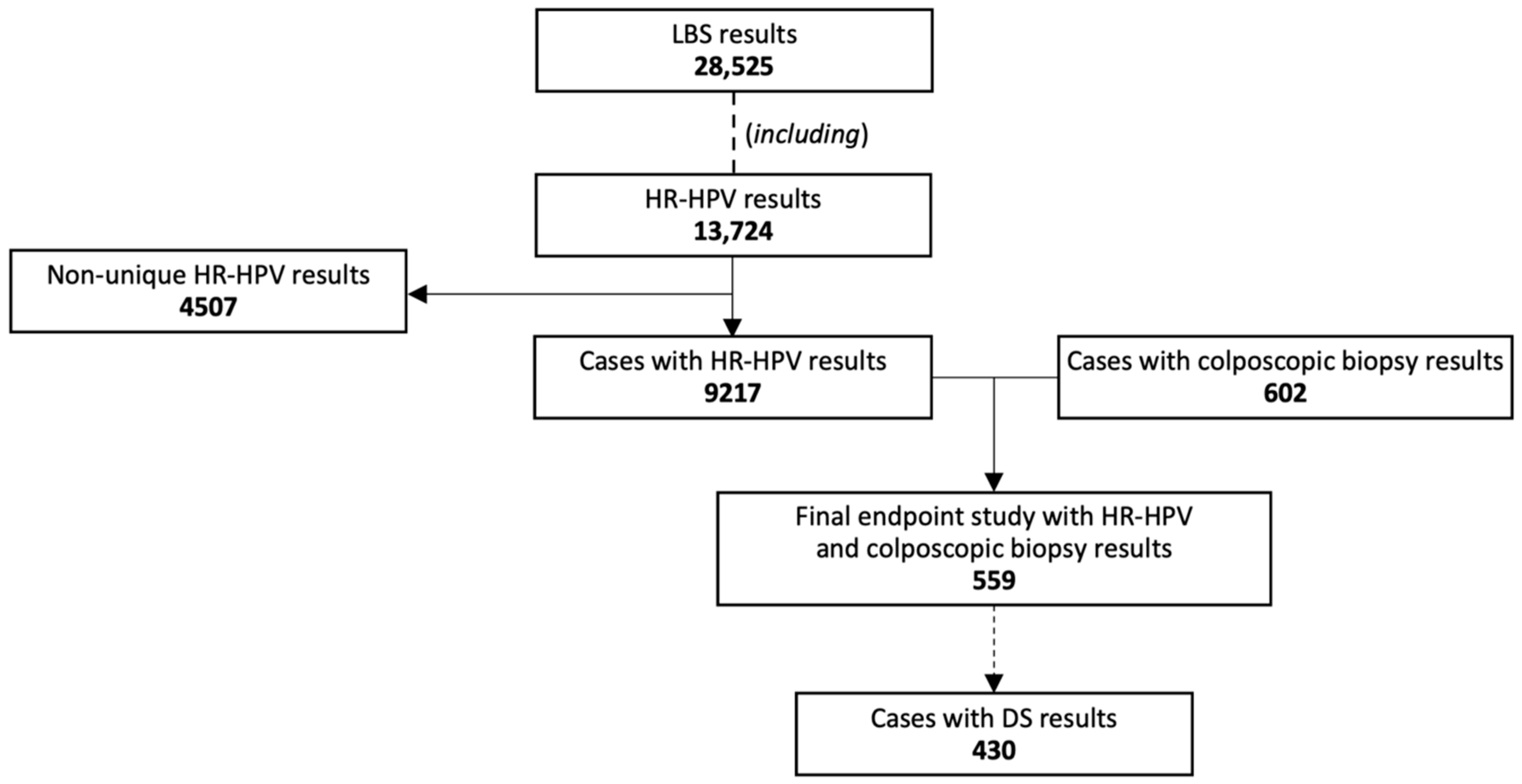
2.1. Study Population
2.2. Liquid-Based Screening (LBS), Sample Collection and Storage
2.3. HR-HPV Testing with Two Assays for Extended Genotyping
2.4. Liquid-Based Cytology and p16/Ki67 Dual-Stain Immunostaining
2.5. Colposcopic Biopsy and Histology
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferlay, J.; Ervik, M.; Lam, F.; Laversanne, M.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Today; International Agency for Research on Cancer: Lyon, France, 2024; Available online: https://gco.iarc.who.int/today (accessed on 13 May 2024).
- Schiffman, M.; Castle, P.E.; Jeronimo, J.; Rodriguez, A.C.; Wacholder, S. Human papillomavirus and cervical cancer. Lancet 2007, 370, 890–907. [Google Scholar] [CrossRef] [PubMed]
- de Sanjosé, S.; Brotons, M.; Pavón, M.A. The natural history of human papillomavirus infection. Best. Pract. Res. Clin. Obstet. Gynaecol. 2018, 47, 2–13. [Google Scholar] [CrossRef]
- IARC. Cervical Cancer Screening. In IARC Handbooks of Cancer Prevention; IARC: Lyon, France, 2022; Volume 18, pp. 1–456. Available online: https://publications.iarc.fr/604 (accessed on 4 June 2024).
- Perkins, R.B.; Wentzensen, N.; Guido, R.S.; Schiffman, M. Cervical Cancer Screening: A Review. JAMA 2023, 330, 547–558. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, N.; Bosch, F.X.; De Sanjosé, S.; Herrero, R.; Castellsagué, X.; Shah, K.V.; Snijders, P.J.F.; Meijer, C.J.L.M. Epidemiologic classification of human papillomavirus types associated with cervical cancer. N. Engl. J. Med. 2003, 348, 518–527. [Google Scholar] [CrossRef] [PubMed]
- Clifford, G.M.; Smith, J.S.; Plummer, M.; Muñoz, N.; Franceschi, S. Human papillomavirus types in invasive cervical cancer worldwide: A meta-analysis. Br. J. Cancer 2003, 88, 63–73. [Google Scholar] [CrossRef]
- Schiffman, M.; Wentzensen, N. Human papillomavirus infection and the multistage carcinogenesis of cervical cancer. Cancer Epidemiol. Biomark. Prev. 2013, 22, 553–560. [Google Scholar] [CrossRef]
- Wentzensen, N.; Fetterman, B.; Castle, P.E.; Schiffman, M.; Wood, S.N.; Stiemerling, E.; Tokugawa, D.; Bodelon, C.; Poitras, N.; Lorey, T.; et al. p16/Ki-67 Dual Stain Cytology for Detection of Cervical Precancer in HPV-Positive Women. J. Natl. Cancer Inst. 2015, 107, djv257. [Google Scholar] [CrossRef]
- Clarke, M.A.; Wentzensen, N.; Perkins, R.B.; Garcia, F.; Arrindell, D.; Chelmow, D.; Cheung, L.C.; Darragh, T.M.; Egemen, D.; Guido, R.; et al. Recommendations for Use of p16/Ki67 Dual Stain for Management of Individuals Testing Positive for Human Papillomavirus. J. Low. Genit. Tract. Dis. 2024, 28, 124–130. [Google Scholar] [CrossRef]
- Mazurec, K.; Trzeszcz, M.; Mazurec, M.; Streb, J.; Halon, A.; Jach, R. Should we use risk selection tests for HPV 16 and/or 18 positive cases: Comparison of p16/Ki67 and cytology. J. Med. Virol. 2024, 96, e29500. [Google Scholar] [CrossRef]
- Trzeszcz, M.; Mazurec, M.; Jach, R.; Mazurec, K.; Kotkowska-Szeps, I.; Kania, M.; Wantuchowicz, M.; Wasowska, J.; Duczek-Polakiewicz, M.; Rozmus, P.; et al. p16/Ki67 dual stain triage versus cytology in primary human papillomavirus-based cervical cancer screening with limited genotyping. J. Med. Virol. 2023, 95, e29271. [Google Scholar] [CrossRef]
- Mazurec, K.; Trzeszcz, M.; Mazurec, M.; Streb, J.; Halon, A.; Jach, R. Triage Strategies for Non-16/Non-18 HPV-Positive Women in Primary HPV-Based Cervical Cancer Screening: p16/Ki67 Dual Stain vs. Cytology. Cancers 2023, 15, 5095. [Google Scholar] [CrossRef]
- Wentzensen, N.; von Knebel Doeberitz, M. Biomarkers in cervical cancer screening. Dis. Mark. 2007, 23, 315–330. [Google Scholar] [CrossRef] [PubMed]
- Wright, T.C.; Behrens, C.M.; Ranger-Moore, J.; Rehm, S.; Sharma, A.; Stoler, M.H.; Ridder, R. Triaging HPV-positive women with p16/Ki-67 dual-stained cytology: Results from a sub-study nested into the ATHENA trial. Gynecol. Oncol. 2017, 144, 51–56. [Google Scholar] [CrossRef]
- Premarket Approval (PMA). 2020. Available online: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpma/pma.cfm?id=P190024 (accessed on 23 June 2024).
- Jach, R.; Mazurec, M.; Trzeszcz, M.; Zimmer, M.; Kedzia, W.; Wolski, H. Cervical cancer screening in Poland in current SARS-CoV-2 pandemic: Interim guidelines of the Polish Society of Gynecologists and Obstetricians and the Polish Society of Colposcopy and Cervical Pathophysiology—A summary January 2021. Ginekol. Pol. 2021, 92, 165–173. [Google Scholar] [CrossRef]
- Krajowa Izba Diagnostów Laboratoryjnych; Polskie Towarzystwo Ginekologiczne. Wytyczne dotyczace aplikacji testów molekularnych identyfikujacych DNA HPV HR w profilaktyce szyjki macicy. Stanowisko ekspertów PTG i KIDL [Guidelines for application of molecular tests identyfying HR HPV DNA in the prevention of cervical cancer. Statement of experts from PGS (PTG) and NCLD (KIDL)]. Ginekol. Pol. 2013, 84, 395–399. [Google Scholar]
- Jach, R.; Mazurec, M.; Trzeszcz, M.; Bartosinska-Dyc, A.; Galarowicz, B.; Kedzia, W.; Nowakowski, A.; Pitynski, K. COLPOSCOPY 2020-COLPOSCOPY PROTOCOLS: A Summary of the Clinical Experts Consensus Guidelines of the Polish Society of Colposcopy and Cervical Pathophysiology and the Polish Society of Gynaecologists and Obstetricians. Ginekol. Pol. 2020, 91, 362371. [Google Scholar] [CrossRef]
- Trzeszcz, M.; Mazurec, M.; Jach, R.; Mazurec, K.; Jach, Z.; Kotkowska-Szeps, I.; Kania, M.; Wantuchowicz, M.; Prokopyk, A.; Barcikowski, P.; et al. Liquid-Based Screening Tests Results: HPV, Liquid-Based Cytology, and P16/Ki67 Dual-Staining in Private-Based Opportunistic Cervical Cancer Screening. Diagnostics 2021, 11, 1420. [Google Scholar] [CrossRef] [PubMed]
- Loghavi, S.; Walts, A.E.; Bose, S. CINtec® PLUS dual immunostain: A triage tool for cervical pap smears with atypical squamous cells of undetermined significance and low grade squamous intraepithelial lesion. Diagn. Cytopathol. 2013, 41, 582–587. [Google Scholar] [CrossRef] [PubMed]
- National Cervical Cancer Screening Programme in Poland Coordinating Centre; Polish Gynaecological Society; Polish Society of Pathologists; Polish Society of Colposcopy and Uterine Cervix Pathology. Management of abnormal pap smear—Consensus guidelines of the National Cervical Cancer Screening Programme in Poland Coordinating Centre, the Polish Gynaecological Society, the Polish Society of Pathologists, and Polish Society of Colposcopy and Uterine Cervix Pathology. Ginekol. Pol. 2009, 80, 129–138. [Google Scholar]
- Massad, L.S.; Einstein, M.H.; Huh, W.K.; Katki, H.A.; Kinney, W.K.; Schiffman, M.; Solomon, D.; Wentzensen, N.; Lawson, H.W. 2012 updated consensus guidelines for the management of abnormal cervical cancer screening tests and cancer precursors. J. Low Genit. Tract. Dis. 2013, 17 (Suppl. S1), S1–S27, Correction in: J. Low Genit. Tract. Dis. 2013, 17, 367. [Google Scholar] [CrossRef]
- Huh, W.K.; Ault, K.A.; Chelmow, D.; Davey, D.D.; Goulart, R.A.; Garcia, F.A.R.; Kinney, W.K.; Massad, L.S.; Mayeaux, E.J.; Saslow, D.; et al. Use of primary high-risk human papillomavirus testing for cervical cancer screening: Interim clinical guidance. Obstet. Gynecol. 2015, 125, 330–337. [Google Scholar] [CrossRef] [PubMed]
- Darragh, T.M.; Colgan, T.J.; Cox, J.T.; Heller, D.S.; Henry, M.R.; Luff, R.D.; McCalmont, T.; Nayar, R.; Palefsky, J.M.; Stoler, M.H.; et al. The Lower Anogenital Squamous Terminology Standardization project for HPV-associated lesions: Background and consensus recommendations from the College of American Pathologists and the American Society for Colposcopy and Cervical Pathology. Int. J. Gynecol. Pathol. 2013, 32, 76–115, Correction in: Int. J. Gynecol. Pathol. 2013, 32, 241. [Google Scholar] [CrossRef] [PubMed]
- Kurman, R.J.; Carcangiu, M.L.; Herrington, C.S. WHO Classification of Tumours of Female Reproductive Organs, 4th ed.; International Agency for Research on Cancer (IARC): Lyon, France, 2014. [Google Scholar]
- WHO Classification of Tumours Editorial Board. Female Genital Tumours. In WHO Classification of Tumours, 5th ed.; International Agency for Research on Cancer: Lyon, France, 2020; Volume 4, p. 631. [Google Scholar]
- Inturrisi, F.; de Sanjosé, S.; Desai, K.T.; Dagnall, C.; Egemen, D.; Befano, B.; Rodriguez, A.C.; Jeronimo, J.A.; Zuna, R.E.; Hoffman, A.; et al. A rapid HPV typing assay to support global cervical cancer screening and risk-based management: A cross-sectional study. Int. J. Cancer 2024, 154, 241–250. [Google Scholar] [CrossRef] [PubMed]
- Siegler, E.; Reichman, Y.; Kugelman, N.; Mackuli, L.; Lavie, O.; Ostrovsky, L.; Shaked-Mishan, P.; Segev, Y. Low-Risk Human Papillomavirus Types in Cervical Intraepithelial Neoplasia 2-3 and in Invasive Cervical Cancer Patients. J. Low. Genit. Tract. Dis. 2019, 23, 248–252. [Google Scholar] [CrossRef]
- Zeng, M.; Zhang, X.; He, L.; Liu, X.; Liu, H.; Deng, R.; Qiu, B.; Liu, F.; Xiao, H.; Li, Q.; et al. Human papillomavirus infections among women with cervical lesions and cervical cancer in Yueyang, China: A cross-sectional study of 3674 women from 2019 to 2022. Virol. J. 2023, 20, 254. [Google Scholar] [CrossRef]
- Zhang, J.; Cheng, K.; Wang, Z. Prevalence and distribution of human papillomavirus genotypes in cervical intraepithelial neoplasia in China: A meta-analysis. Arch. Gynecol. Obstet. 2020, 302, 1329–1337. [Google Scholar] [CrossRef]
- de Sanjose, S.; Quint, W.G.V.; Alemany, L.; Geraets, D.T.; Klaustermeier, J.E.; Lloveras, B.; Tous, S.; Felix, A.; Bravo, L.E.; Shin, H.-R.; et al. Human papillomavirus genotype attribution in invasive cervical cancer: A retrospective cross-sectional worldwide study. Lancet Oncol. 2010, 11, 1048–1056. [Google Scholar] [CrossRef]
- Guan, P.; Howell-Jones, R.; Li, N.; Bruni, L.; de Sanjosé, S.; Franceschi, S.; Clifford, G.M. Human papillomavirus types in 115,789 HPV-positive women: A meta-analysis from cervical infection to cancer. Int. J. Cancer 2012, 131, 2349–2359. [Google Scholar] [CrossRef]
- Clifford, G.M.; Rana, R.K.; Franceschi, S.; Smith, J.S.; Gough, G.; Pimenta, J.M. Human papillomavirus genotype distribution in low-grade cervical lesions: Comparison by geographic region and with cervical cancer. Cancer Epidemiol. Biomark. Prev. 2005, 14, 1157–1164. [Google Scholar] [CrossRef]
- Bruni, L.; Diaz, M.; Castellsagué, X.; Ferrer, E.; Bosch, F.X.; de Sanjosé, S. Cervical human papillomavirus prevalence in 5 continents: Meta-analysis of 1 million women with normal cytological findings. J. Infect. Dis. 2010, 202, 1789–1799. [Google Scholar] [CrossRef]
- Wentzensen, N.; Schwartz, L.; Zuna, R.E.; Smith, K.; Mathews, C.; Gold, M.A.; Allen, R.A.; Zhang, R.; Dunn, S.T.; Walker, J.L.; et al. Performance of p16/Ki-67 immunostaining to detect cervical cancer precursors in a colposcopy referral population. Clin. Cancer Res. 2012, 18, 4154–4162. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
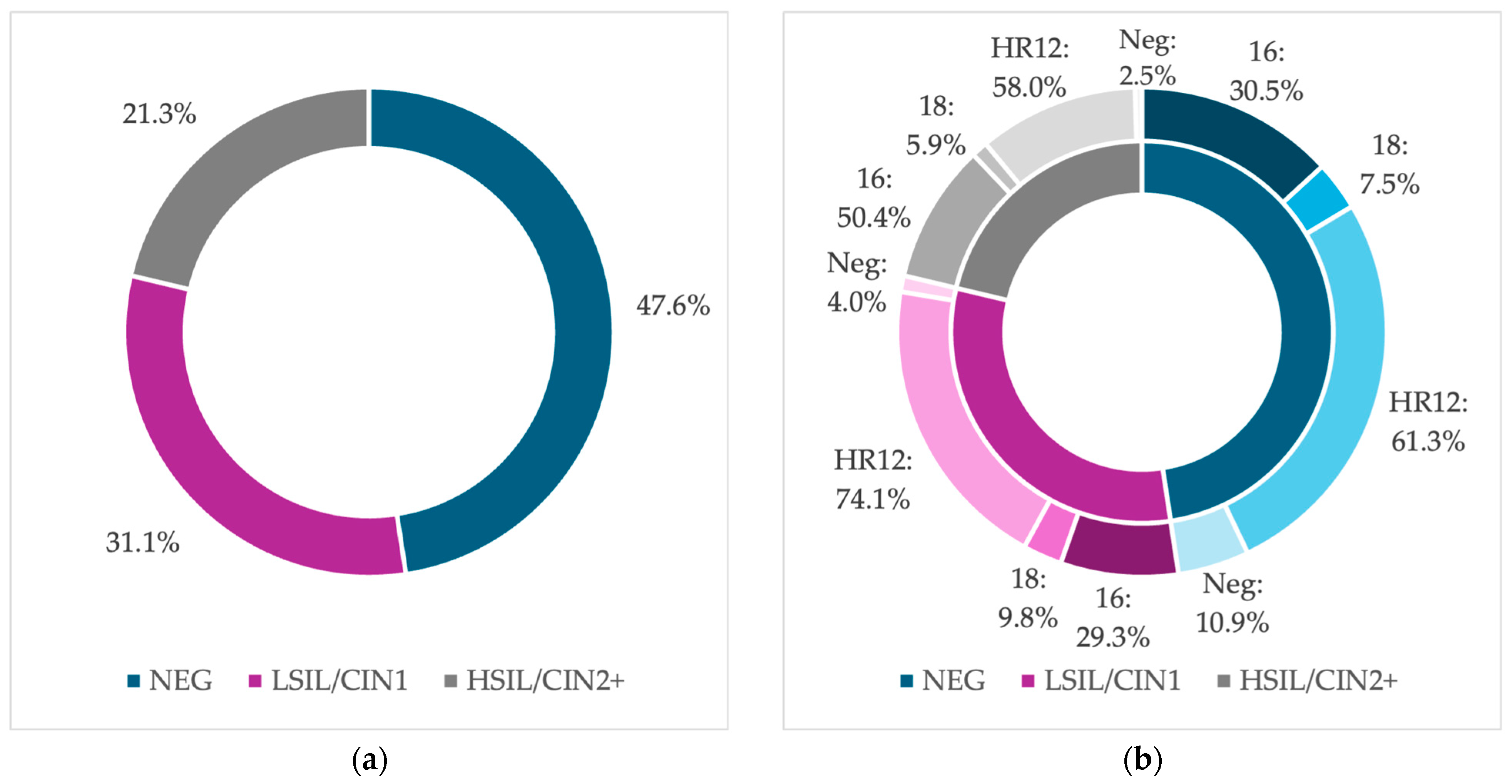
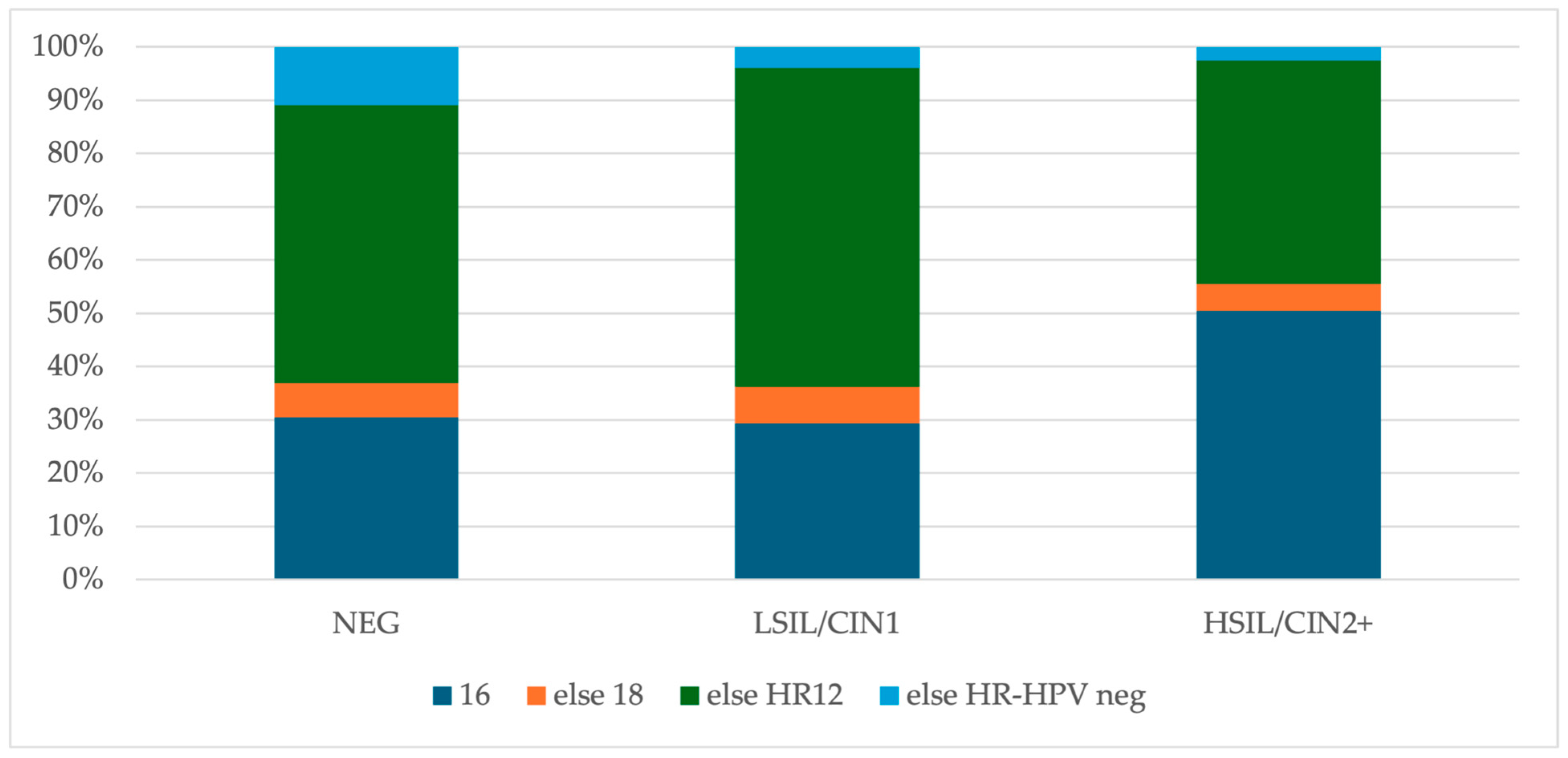
| Positive | NEG (n = 266), No (%) | LSIL/CIN1 (n = 174), No (%) | HSIL/CIN2+ (n = 119), No (%) |
|---|---|---|---|
| HR-HPV | 237 (89.1) | 167 (96.0) | 116 (97.5) |
| HPV 16 | 60 (22.6) | 28 (16.1) | 45 (37.8) |
| HPV 18 | 12 (4.5) | 7 (4.0) | 1 (0.8) |
| HPV 16 and 18 | 2 (0.8) | 3 (1.7) | 1 (0.8) |
| HPV 16 and HR12 | 18 (6.8) | 18 (10.3) | 14 (11.8) |
| HPV 16, 18 and HR12 | 1 (0.4) | 2 (1.1) | 0 (0.0) |
| HPV 18 and HR12 | 5 (1.9) | 5 (2.9) | 5 (4.2) |
| HR12 | 139 (52.3) | 104 (59.8) | 50 (42.0) |
| Negative | 29 (10.9) | 7 (4.0) | 3 (2.5) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazurec, K.; Trzeszcz, M.; Mazurec, M.; Kobierzycki, C.; Jach, R.; Halon, A. Distribution of 14 High-Risk HPV Types and p16/Ki67 Dual-Stain Status in Post-Colposcopy Histology Results: Negative, Low- and High-Grade Cervical Squamous Intraepithelial Lesions. Cancers 2024, 16, 3401. https://doi.org/10.3390/cancers16193401
Mazurec K, Trzeszcz M, Mazurec M, Kobierzycki C, Jach R, Halon A. Distribution of 14 High-Risk HPV Types and p16/Ki67 Dual-Stain Status in Post-Colposcopy Histology Results: Negative, Low- and High-Grade Cervical Squamous Intraepithelial Lesions. Cancers. 2024; 16(19):3401. https://doi.org/10.3390/cancers16193401
Chicago/Turabian StyleMazurec, Karolina, Martyna Trzeszcz, Maciej Mazurec, Christopher Kobierzycki, Robert Jach, and Agnieszka Halon. 2024. "Distribution of 14 High-Risk HPV Types and p16/Ki67 Dual-Stain Status in Post-Colposcopy Histology Results: Negative, Low- and High-Grade Cervical Squamous Intraepithelial Lesions" Cancers 16, no. 19: 3401. https://doi.org/10.3390/cancers16193401
APA StyleMazurec, K., Trzeszcz, M., Mazurec, M., Kobierzycki, C., Jach, R., & Halon, A. (2024). Distribution of 14 High-Risk HPV Types and p16/Ki67 Dual-Stain Status in Post-Colposcopy Histology Results: Negative, Low- and High-Grade Cervical Squamous Intraepithelial Lesions. Cancers, 16(19), 3401. https://doi.org/10.3390/cancers16193401