
Effect of Prior Transurethral Prostate Resection (TURP) or Laser Enucleation (ThuLEP) on Radiotherapy-Induced Toxicity and Quality of Life in Prostate Cancer Patients Undergoing Definitive Radiotherapy
 , ,
, , 
Abstract
Simple Summary
Abstract

1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Characteristics
2.2. Analysis of Quality of Life: IPSS, QoL, CTC-GU, and CTC-GI
2.3. Transurethral Resection of the Prostate (TURP) and Thulium Laser Enucleation of the Prostate (ThuLEP)
2.4. Radiotherapy
2.5. Statistical Analyses and Outcome Measures
3. Results
3.1. Patient and Treatment Characteristics

{kind=link}
{kind=link}
{kind=link}
| Parameter | TURP (n = 23) | ThuLEP (n = 19) | p Value | TURP or ThuLEP (n = 42) | No TURP/ThuLEP (n = 90) | p Value |
|---|---|---|---|---|---|---|
| Median age at diagnosis (years) | 74 (range, 54–87) | 74 (range, 66–90) | 0.498 | 74 (range, 54–90) | 73 (range, 51–89) | 0.702 |
| Median pre-treatment PSA (ng/mL) | 8.6 (0.3–92.5) | 7.9 (0.7–32) | 0.01 | 8.3 (0.3–92.5) | 10.5 (range, 0.1–84) | 0.08 |
| T stage: T1–2a/T2b–T2c/T3–T4/TX (%) | 78/9/13/0 | 74/5/21/0 | 0.546 | 76/7/17/0 | 71/23/6/0 | 0.115 |
| Median pre-RT prostate volume (cm3) | 18 (range, 12–35) | 17 (range, 10–30) | 0.651 | 18 (range, 10–35) | 39 (range, 22–123) | <0.001 |
| Median pre-TURP/ThuLEP prostate volume (cm3) | 78 (range, 34–120) | 89 (range, 55–180) | 0.651 | 80 (range, 34–180) | 39 (range, 22–123) | <0.001 |
| N stage: N0/N1/NX (%) | 88/22/0 | 84/5/11 | 0.539 | 81/14/5 | 90/10/0 | 0.597 |
| Gleason score: 6/7/≥8 (%) | 26/39/35 | 16/31/53 | 0.159 | 19/36/45 | 13/51/36 | 0.859 |
| Risk stratification: low/intermediate/high risk (%) | 26/30/44 | 16/26/58 | 0.448 | 21/29/50 | 6/51/43 | 0.392 |
| PIRADS-Score by mpMRI: 3/4/5 (%) | 20/40/40 | 24/29/47 | 0.189 | 21/36/43 | 8/30/61 | 0.825 |
| EBRT dose (Gy) | 78.9 (range, 72.0–80.0) | 78.8 (range, 72.0–80.0) | 0.734 | 78.9 (range, 72–80) | 73.8 (range, 72–80) | 0.013 |
| Radiation technique: 3D-CRT /static/dynamic IMRT (dynamic: VMAT/Tomotherapy) (%) | 0/13/87 | 0/11/89 | 0.656 | 0/12/88 | 0/27/73 | 0.926 |
| Median bladder volume receiving 70 Gy (V70Gy) (cm3) | 31 (range, 4–73) | 33 (range, 6–77) | 0.859 | 32 (range, 4–77) | 35 (range, 5–81) | 0.065 |
| Use of ADT/mean duration (%/months) | 56/9 | 47/12 | 0.845 | 52/11 | 56/9 | 0.634 |
| Median follow-up (months) | 30 (range, 12–84) | 36 (range, 18–48) | 0.17 | 36 (range, 12–98) | 36 (range, 8–60) | 0.473 |
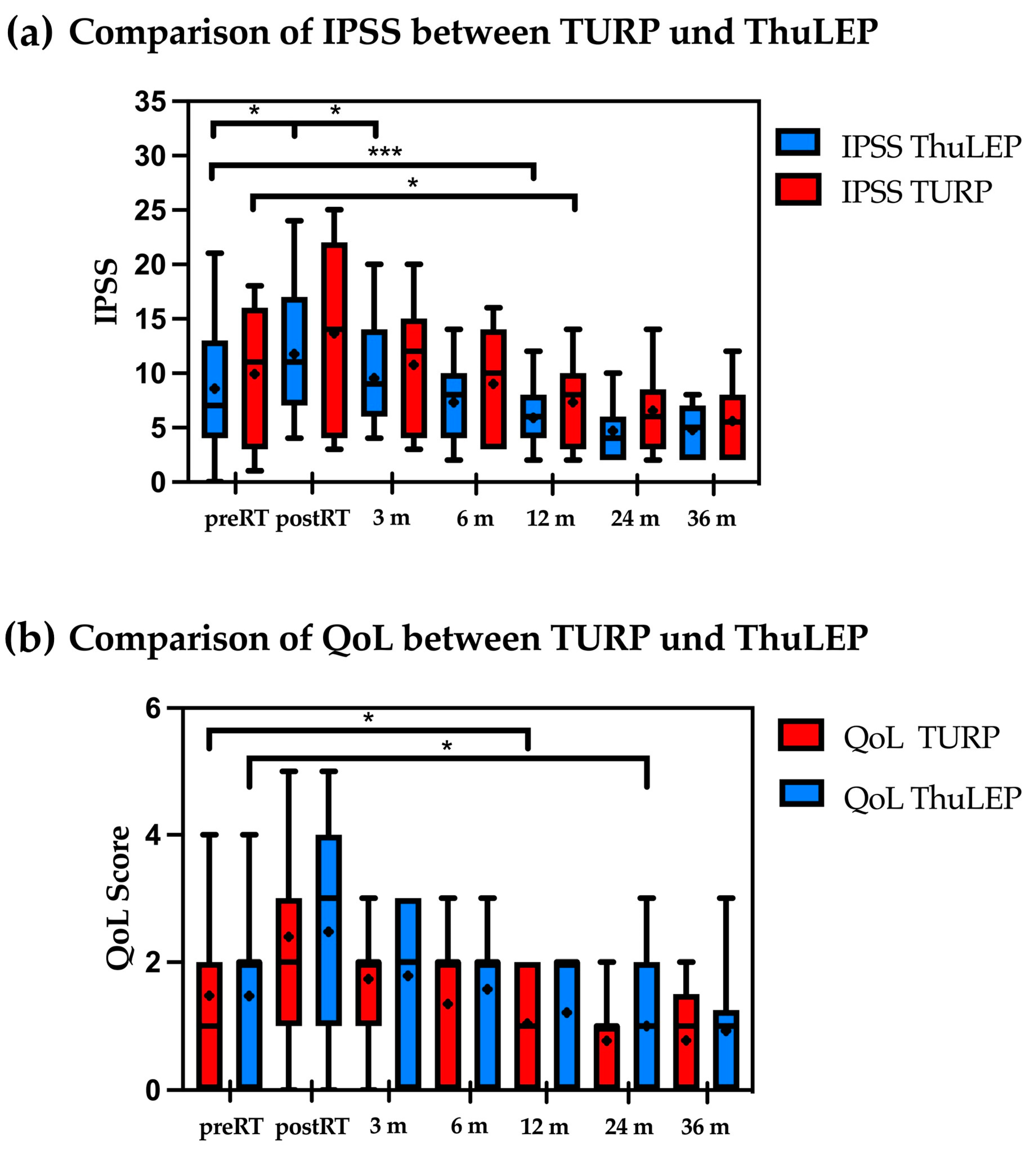
3.2. Comparison between TURP and ThuLEP: Patients with Prior TURP Showed a Significant Increase in IPSS and QoL Immediately Post-RT
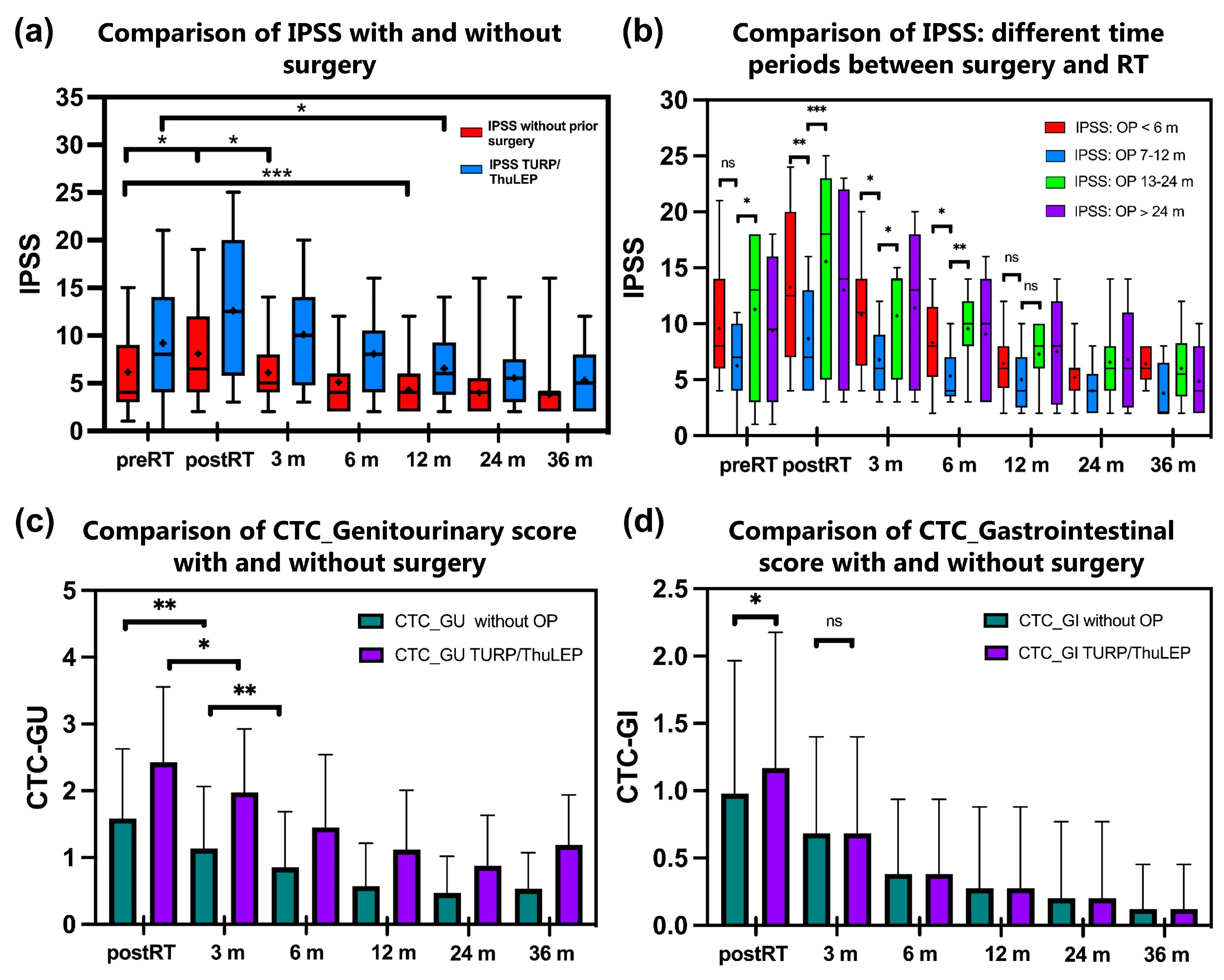
3.3. Patients Who Underwent TURP/ThuLEP Showed Higher IPSS Post-RT and a Longer Period until the Baseline Value Was Reached
3.4. Comparison of Different Time Periods between Surgery and Radiotherapy Shows That a Period between 6 and 12 Months Is Associated with Less Toxicity
3.5. No Significant Differences in a Further Small Subgroup Analysis of Patients with Different Prostate Volumes before TURP/ThuLEP and before Radiotherapy
4. Discussion
4.1. GU Toxicities in Patients with Prior TURP Versus ThuLEP and Versus Non-Operated Patients
4.2. Rectal Toxicities
4.3. Quality of Life in Relation to GU Toxicities
4.4. Parameters Affecting Toxicity Profile
4.4.1. Use of ADT
4.4.2. Radiation Treatment Technique
4.4.3. The Time Interval between Surgery and EBRT
4.5. Limitations
4.6. Clinical Prospects
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dai, X.; Fang, X.; Ma, Y.; Xianyu, J. Benign Prostatic Hyperplasia and the Risk of Prostate Cancer and Bladder Cancer: A Meta-Analysis of Observational Studies. Medicine 2016, 95, e3493. [Google Scholar] [CrossRef] [PubMed]
- Zelefsky, M.J.; Whitmore, W.F.; Leibel, S.A.; Wallner, K.E.; Fuks, Z. Impact of Transurethral Resection on the Long-Term Outcome of Patients with Prostatic Carcinoma. J. Urol. 1993, 150, 1860–1864. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, C.; Vetterlein, M.; Fisch, M.; Reiss, P.; Worst, T.; Kranz, J.; Steffens, J.; Kluth, L.; Pfalzgraf, D.; on behalf of the Trauma and Reconstructive Urology Working Party of the European Association of Urology (EAU) Young Academic Urologists (YAU). Contemporary Outcomes after Transurethral Procedures for Bladder Neck Contracture Following Endoscopic Treatment of Benign Prostatic Hyperplasia. JCM 2021, 10, 2884. [Google Scholar] [CrossRef] [PubMed]
- Hart, A.J.; Fowler, J.W. Incidence of Urethral Stricture after Transurethral Resection of Prostate. Effects of Urinary Infection, Urethral Flora, and Catheter Material and Size. Urology 1981, 18, 588–591. [Google Scholar] [CrossRef]
- Wani, M.M.; Sriprasad, S.; Bhat, T.; Madaan, S. Is Thulium Laser Enucleation of Prostate an Alternative to Holmium and TURP Surgeries-A Systematic Review? Turk. J. Urol. 2020, 46, 419–426. [Google Scholar] [CrossRef]
- Huang, S.-W.; Tsai, C.-Y.; Tseng, C.-S.; Shih, M.-C.; Yeh, Y.-C.; Chien, K.-L.; Pu, Y.-S.; Tu, Y.-K. Comparative Efficacy and Safety of New Surgical Treatments for Benign Prostatic Hyperplasia: Systematic Review and Network Meta-Analysis. BMJ 2019, 367, l5919. [Google Scholar] [CrossRef]
- Liu, M.; Pickles, T.; Berthelet, E.; Agranovich, A.; Kwan, W.; Tyldesley, S.; McKenzie, M.; Keyes, M.; Morris, J.; Pai, H.; et al. Urinary Incontinence in Prostate Cancer Patients Treated with External Beam Radiotherapy. Radiother. Oncol. 2005, 74, 197–201. [Google Scholar] [CrossRef]
- Seymore, H.; Schellhammer, P.F. Impact of Prior Transurethral Resection of the Prostate on Post-Radiation Urethral Strictures and Bladder Neck Contractures. Int. J. Radiat. Oncol. Biol. Phys. 1986, 12, 1597–1600. [Google Scholar] [CrossRef]
- Ishiyama, H.; Hirayama, T.; Jhaveri, P.; Satoh, T.; Paulino, A.C.; Xu, B.; Butler, E.B.; Teh, B.S. Is There an Increase in Genitourinary Toxicity in Patients Treated with Transurethral Resection of the Prostate and Radiotherapy?: A Systematic Review. Am. J. Clin. Oncol. 2014, 37, 297–304. [Google Scholar] [CrossRef]
- Perez, C.A.; Lee, H.K.; Georgiou, A.; Lockett, M.A. Technical Factors Affecting Morbidity in Definitive Irradiation for Localized Carcinoma of the Prostate. Int. J. Radiat. Oncol. Biol. Phys. 1994, 28, 811–819. [Google Scholar] [CrossRef]
- Pilepich, M.V.; Perez, C.A.; Walz, B.J.; Zivnuska, F.R. Complications of Definitive Radiotherapy for Carcinoma of the Prostate. Int. J. Radiat. Oncol. Biol. Phys 1981, 7, 1341–1348. [Google Scholar] [CrossRef] [PubMed]
- Lawton, C.A.; Won, M.; Pilepich, M.V.; Asbell, S.O.; Shipley, W.U.; Hanks, G.E.; Cox, J.D.; Perez, C.A.; Sause, W.T.; Doggett, S.R. Long-Term Treatment Sequelae Following External Beam Irradiation for Adenocarcinoma of the Prostate: Analysis of RTOG Studies 7506 and 7706. Int. J. Radiat. Oncol. Biol. Phys. 1991, 21, 935–939. [Google Scholar] [CrossRef] [PubMed]
- Tomita, N.; Oze, I.; Shimizu, H.; Yoshida, M.; Kimura, K.; Takehana, K.; Shimizu, A.; Makita, C.; Tachibana, H.; Kodaira, T.; et al. International Prostate Symptom Score (IPSS) Change and Changing Factor in Intensity-Modulated Radiotherapy Combined with Androgen Deprivation Therapy for Prostate Cancer. Nagoya J. Med. Sci. 2015, 77, 637–646. [Google Scholar] [PubMed]
- Malik, R.; Jani, A.B.; Liauw, S.L. External Beam Radiotherapy for Prostate Cancer: Urinary Outcomes for Men with High International Prostate Symptom Scores (IPSS). Int. J. Radiat. Oncol. Biol. Phys. 2011, 80, 1080–1086. [Google Scholar] [CrossRef] [PubMed]
- Cockett, A.T.; Aso, Y.; Denis, L.; Khoury, S.; Barry, M.; Carlton, C.E.; Coffey, D.; Fitzpatrick, J.; Griffiths, K.; Hald, T. World Health Organization Consensus Committee Recommendations Concerning the Diagnosis of BPH. Prog. Urol. 1991, 1, 957–972. [Google Scholar]
- Common Terminology Criteria for Adverse Events (CTCAE). Version 5.0 Published: 27 November 2017, U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES. Available online: https://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm (accessed on 23 September 2024).
- Cornu, J.N.; Gacci, M.; Hashim, H.; Herrmann, T.R.W.; Malde, S.; Netsch, C.; De Nunzio, C.; Rieken, M.; Sakalis, V.; Tutolo, M.; et al. Summary Paper on Underactive Bladder from the European Association of Urology Guidelines on Non-neurogenic Male Lower Urinary Tract Symptoms. EAU Guidel. Non-Neurogenic Male Low. Urin. Tract Symptoms (LUTS) 2024, 86, 213–220. [Google Scholar] [CrossRef]
- Zhang, T.R.; Thorogood, S.L.; Sze, C.; Fisch, R.; Chughtai, B.; Te, A.; Lee, R.K.; Hu, J.C. Current Practice Patterns in the Surgical Management of Benign Prostatic Hyperplasia. Urology 2023, 175, 157–162. [Google Scholar] [CrossRef]
- Miernik, A.; Fritzsche, J.; Libutzki, B.; Malka, V.; Kilemnik, I.; Mohebbi, D.; May, M.; Gratzke, C.; Suarez-Ibarrola, R. Real-World Data and Treatment Patterns of Patients with Lower Urinary Tract Symptoms Due to Benign Prostatic Hyperplasia in Germany: An Observational Study Using Health Insurance Claims Data. World J. Urol. 2021, 39, 4381–4388. [Google Scholar] [CrossRef]
- Gulliford, S.L.; Partridge, M.; Sydes, M.R.; Webb, S.; Evans, P.M.; Dearnaley, D.P. Parameters for the Lyman Kutcher Burman (LKB) Model of Normal Tissue Complication Probability (NTCP) for Specific Rectal Complications Observed in Clinical Practise. Radiother. Oncol. 2012, 102, 347–351. [Google Scholar] [CrossRef]
- Yuan, R.; Boyu, Y.; Fujun, Z.; Chengyi, J.; Yifeng, J.; Xiaohai, W.; Di, C.; Shujie, X.; Bangmin, H. Transurethral Thulium Laser Enucleation versus Resection of the Prostate for Treating Benign Prostatic Hyperplasia: A Retrospective Study. Lasers Med. Sci. 2019, 34, 329–334. [Google Scholar] [CrossRef]
- Devisetty, K.; Zorn, K.C.; Katz, M.H.; Jani, A.B.; Liauw, S.L. External Beam Radiation Therapy After Transurethral Resection of the Prostate: A Report on Acute and Late Genitourinary Toxicity. Int. J. Radiat. Oncol. Biol. Phys. 2010, 77, 1060–1065. [Google Scholar] [CrossRef] [PubMed]
- Taylor, B.L.; Jaffe, W.I. Electrosurgical Transurethral Resection of the Prostate and Transurethral Incision of the Prostate (Monopolar Techniques). Can. J. Urol. 2015, 22 (Suppl. S1), 24–29. [Google Scholar] [PubMed]
- Silva, L.A.; Andriolo, R.B.; Atallah, Á.N.; da Silva, E.M.K. Surgery for Stress Urinary Incontinence Due to Presumed Sphincter Deficiency after Prostate Surgery. Cochrane Database Syst. Rev. 2014, 2014, CD008306. [Google Scholar] [CrossRef] [PubMed]
- Hirshberg, E.D.; Klotz, L.H. Post Transurethral Resection of Prostate Incontinence in Previously Radiated Prostate Cancer Patients. Can. J. Urol. 1998, 5, 560–563. [Google Scholar] [PubMed]
- Merrick, G.S.; Butler, W.M.; Wallner, K.E.; Galbreath, R.W. Effect of Transurethral Resection on Urinary Quality of Life after Permanent Prostate Brachytherapy. Int. J. Radiat. Oncol. Biol. Phys. 2004, 58, 81–88. [Google Scholar] [CrossRef]
- Peeters, S.T.H.; Heemsbergen, W.D.; van Putten, W.L.J.; Slot, A.; Tabak, H.; Mens, J.W.; Lebesque, J.V.; Koper, P.C.M. Acute and Late Complications after Radiotherapy for Prostate Cancer: Results of a Multicenter Randomized Trial Comparing 68 Gy to 78 Gy. Int. J. Radiat. Oncol. Biol. Phys. 2005, 61, 1019–1034. [Google Scholar] [CrossRef]
- Nakamura, R.A.; Monti, C.R.; Castilho, L.N.; Trevisan, F.A.; Valim, A.C.; Reinato, J.A. Prognostic Factors for Late Urinary Toxicity Grade 2-3 after Conformal Radiation Therapy on Patients with Prostate Cancer. Int. Braz. J. Urol. 2007, 33, 652–661. [Google Scholar] [CrossRef]
- Sandhu, A.S.; Lombardi, D. Long-Term Urinary Toxicity after 3-Dimensional Conformal Radiotherapy for Prostate Cancer in Patients with Prior History of Transurethral Resection. Int. J. Radiat. Oncol. Biol. Phys. 2000, 48, 643–647. [Google Scholar] [CrossRef]
- Lee, W.R.; Schultheiss, T.E.; Hanlon, A.L.; Hanks, G.E. Urinary Incontinence Following External-Beam Radiotherapy for Clinically Localized Prostate Cancer. Urology 1996, 48, 95–99. [Google Scholar] [CrossRef]
- Green, N.; Treible, D.; Wallack, H. Prostate Cancer: Post-Irradiation Incontinence. J. Urol. 1990, 144, 307–309. [Google Scholar] [CrossRef]
- Laughlin, B.S.; Narang, G.L.; Cheney, S.M.; Humphreys, M.R.; Vargas, C.E.; Keole, S.R.; Rwigema, J.M.; Schild, S.E.; Wong, W.W. Toxicity and Outcomes after External Beam Irradiation for Prostate Cancer in Patients with Prior Holmium Laser Enucleation of the Prostate: Early Experience. Cancer Rep. 2023, 6, 1672. [Google Scholar] [CrossRef] [PubMed]
- Pinkawa, M.; Klotz, J.; Djukic, V.; Petz, D.; Holy, R.; Eble, M.J. Transurethral Resection of the Prostate after Radiotherapy for Prostate Cancer: Impact on Quality of Life. Int. J. Urol. 2014, 21, 899–903. [Google Scholar] [CrossRef] [PubMed]
- Simone, N.L.; Ménard, C.; Soule, B.P.; Albert, P.S.; Guion, P.; Smith, S.; Godette, D.; Crouse, N.S.; Sciuto, L.C.; Cooley-Zgela, T.; et al. Intrarectal Amifostine During External Beam Radiation Therapy for Prostate Cancer Produces Significant Improvements in Quality of Life Measured by EPIC Score. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.T.; Dunn, R.L.; Litwin, M.S.; Sandler, H.M.; Sanda, M.G. Development and Validation of the Expanded Prostate Cancer Index Composite (EPIC) for Comprehensive Assessment of Health-Related Quality of Life in Men with Prostate Cancer. Urology 2000, 56, 899–905. [Google Scholar] [CrossRef] [PubMed]
- Kupelian, P.A.; Reddy, C.A.; Klein, E.A.; Willoughby, T.R. Short-Course Intensity-Modulated Radiotherapy (70 GY at 2.5 GY per Fraction) for Localized Prostate Cancer: Preliminary Results on Late Toxicity and Quality of Life. Int. J. Radiat. Oncol. Biol. Phys. 2001, 51, 988–993. [Google Scholar] [CrossRef]
- Zapatero, A.; Álvarez, A.; Guerrero, A.; Maldonado, X.; González San Segundo, C.; Cabeza, M.A.; Martín de Vidales, C.; Solé, J.M.; Pedro Olivé, A.; Casas, F.; et al. Prognostic Value of Testosterone Castration Levels Following Androgen Deprivation and High-Dose Radiotherapy in Localized Prostate Cancer: Results from a Phase III Trial. Radiother. Oncol. 2021, 160, 115–119. [Google Scholar] [CrossRef]
- Zapatero, A.; Guerrero, A.; Maldonado, X.; Álvarez, A.; González-San Segundo, C.; Cabeza Rodriguez, M.A.; Macías, V.; Pedro Olive, A.; Casas, F.; Boladeras, A.; et al. Late Radiation and Cardiovascular Adverse Effects after Androgen Deprivation and High-Dose Radiation Therapy in Prostate Cancer: Results from the DART 01/05 Randomized Phase 3 Trial. Int. J. Radiat. Oncol. Biol. Phys. 2016, 96, 341–348. [Google Scholar] [CrossRef]
- Odrazka, K.; Dolezel, M.; Vanasek, J.; Vaculikova, M.; Zouhar, M.; Sefrova, J.; Paluska, P.; Vosmik, M.; Kohlova, T.; Kolarova, I.; et al. Late Toxicity after Conformal and Intensity-Modulated Radiation Therapy for Prostate Cancer: Impact of Previous Surgery for Benign Prostatic Hyperplasia. Int. J. Urol. 2010, 17, 784–790. [Google Scholar] [CrossRef]
- Hoffman, R.M.; MacDonald, R.; Wilt, T. Laser Prostatectomy for Benign Prostatic Obstruction. Cochrane Database Syst. Rev. 2000, 2009, CD001987. [Google Scholar] [CrossRef]
- Kollmeier, M.A.; Stock, R.G.; Cesaretti, J.; Stone, N.N. Urinary Morbidity and Incontinence Following Transurethral Resection of the Prostate after Brachytherapy. J. Urol. 2005, 173, 808–812. [Google Scholar] [CrossRef]
| Factor | p Value Patients with Prior ThuLEP and TURP (IPSS preRT/Immediately Post-RT) | p Value Patients without Surgery (IPSS preRT/Immediately Post-RT) |
|---|---|---|
| Age at diagnosis (years): ≥80 | 0.477/0.972 | 0.499/0.672 |
| T stage: ≥T2c | 0.097/0.298 | 0.308/0.807 |
| External beam radiotherapy (EBRT) dose (Gy): ≥79.2 | 0.047 | 0.259 |
| Radiation technique: volumetric intensity arc therapy (VMAT instead of static IMRT) | 0.434 | 0.61 |
| Use of androgen deprivation therapy (ADT) | 0.006/<0.001 | 0.032/0.003 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Steike, D.R.; Troschel, F.M.; Roers, J.; Siats, J.J.; Kittel, C.; Pepper, N.B.; Gravemeyer, S.; Papavassilis, P.; Schrader, A.J.; Eich, H.T.; et al. Effect of Prior Transurethral Prostate Resection (TURP) or Laser Enucleation (ThuLEP) on Radiotherapy-Induced Toxicity and Quality of Life in Prostate Cancer Patients Undergoing Definitive Radiotherapy. Cancers 2024, 16, 3403. https://doi.org/10.3390/cancers16193403
Steike DR, Troschel FM, Roers J, Siats JJ, Kittel C, Pepper NB, Gravemeyer S, Papavassilis P, Schrader AJ, Eich HT, et al. Effect of Prior Transurethral Prostate Resection (TURP) or Laser Enucleation (ThuLEP) on Radiotherapy-Induced Toxicity and Quality of Life in Prostate Cancer Patients Undergoing Definitive Radiotherapy. Cancers. 2024; 16(19):3403. https://doi.org/10.3390/cancers16193403
Chicago/Turabian StyleSteike, David Rene, Fabian Martin Troschel, Julian Roers, Jan Jakob Siats, Christopher Kittel, Niklas Benedikt Pepper, Stefan Gravemeyer, Philipp Papavassilis, Andres Jan Schrader, Hans Theodor Eich, and et al. 2024. "Effect of Prior Transurethral Prostate Resection (TURP) or Laser Enucleation (ThuLEP) on Radiotherapy-Induced Toxicity and Quality of Life in Prostate Cancer Patients Undergoing Definitive Radiotherapy" Cancers 16, no. 19: 3403. https://doi.org/10.3390/cancers16193403
APA StyleSteike, D. R., Troschel, F. M., Roers, J., Siats, J. J., Kittel, C., Pepper, N. B., Gravemeyer, S., Papavassilis, P., Schrader, A. J., Eich, H. T., & Scobioala, S. (2024). Effect of Prior Transurethral Prostate Resection (TURP) or Laser Enucleation (ThuLEP) on Radiotherapy-Induced Toxicity and Quality of Life in Prostate Cancer Patients Undergoing Definitive Radiotherapy. Cancers, 16(19), 3403. https://doi.org/10.3390/cancers16193403