
A Descriptive Study of 103 Primary Cutaneous B-Cell Lymphomas: Clinical and Pathological Characteristics and Treatment from the Spanish Lymphoma Oncology Group (GOTEL)

 , ,
, ,  ,
,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
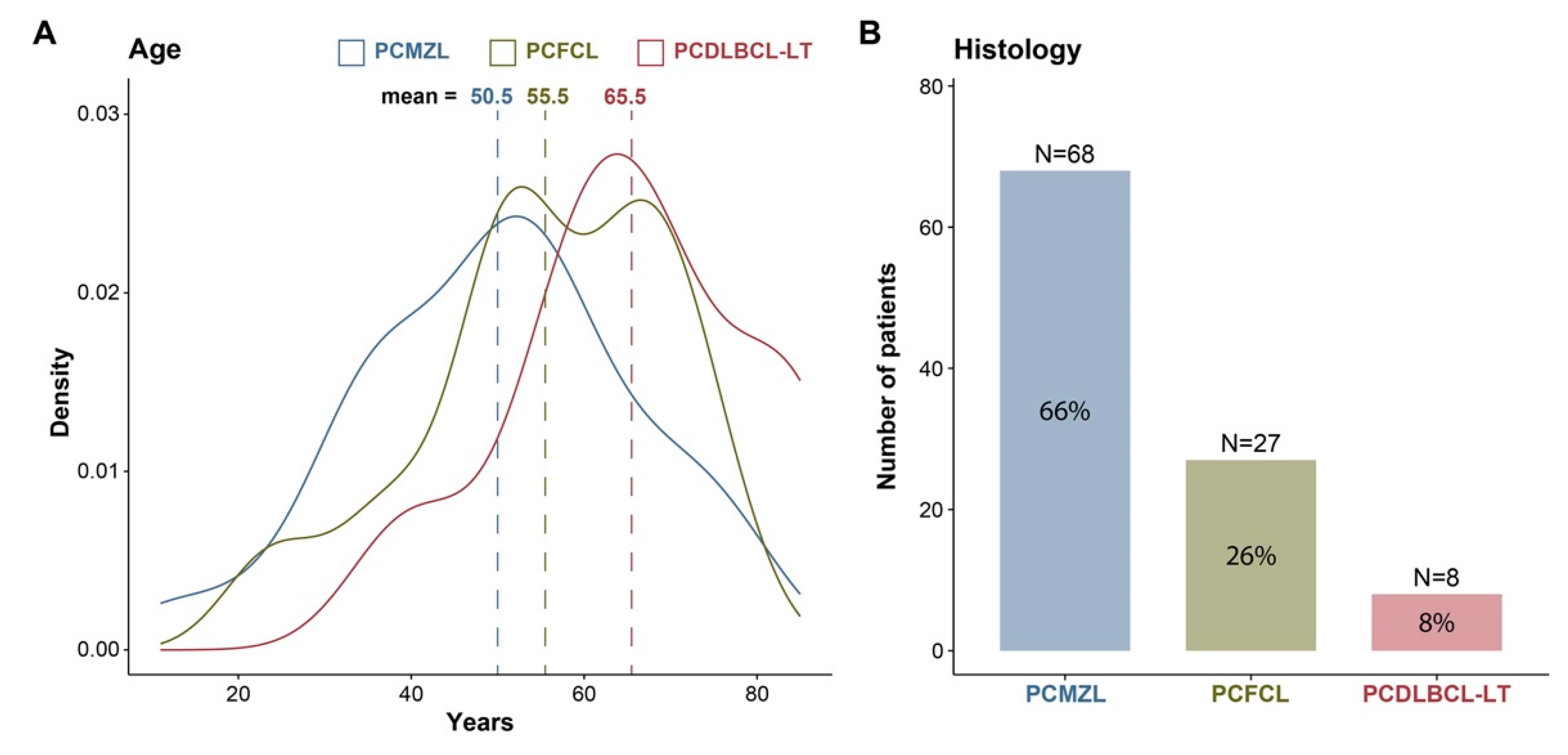
3.1. Epidemiology
3.2. Histology
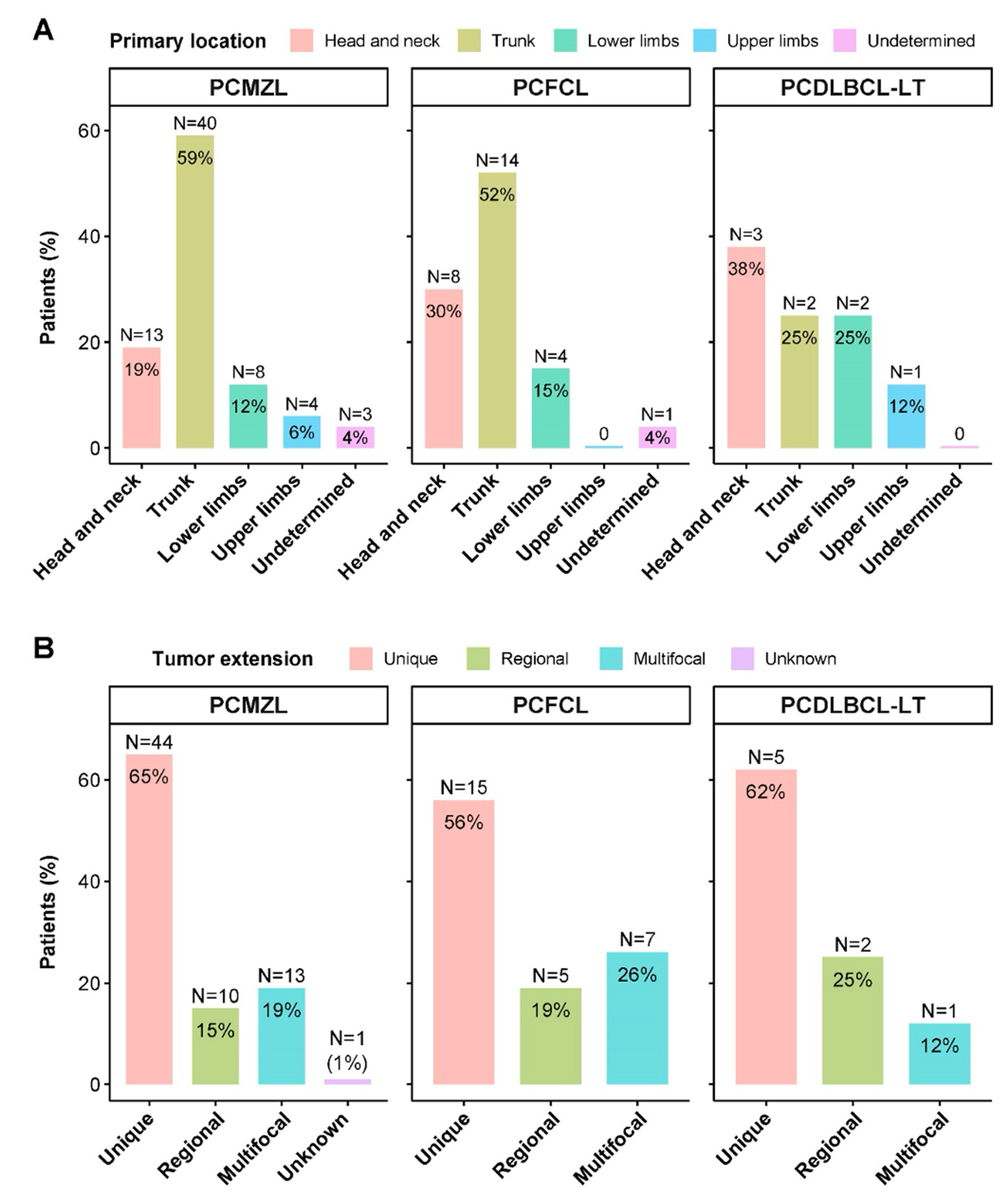
3.3. Location and Extension
3.4. Types of Treatments
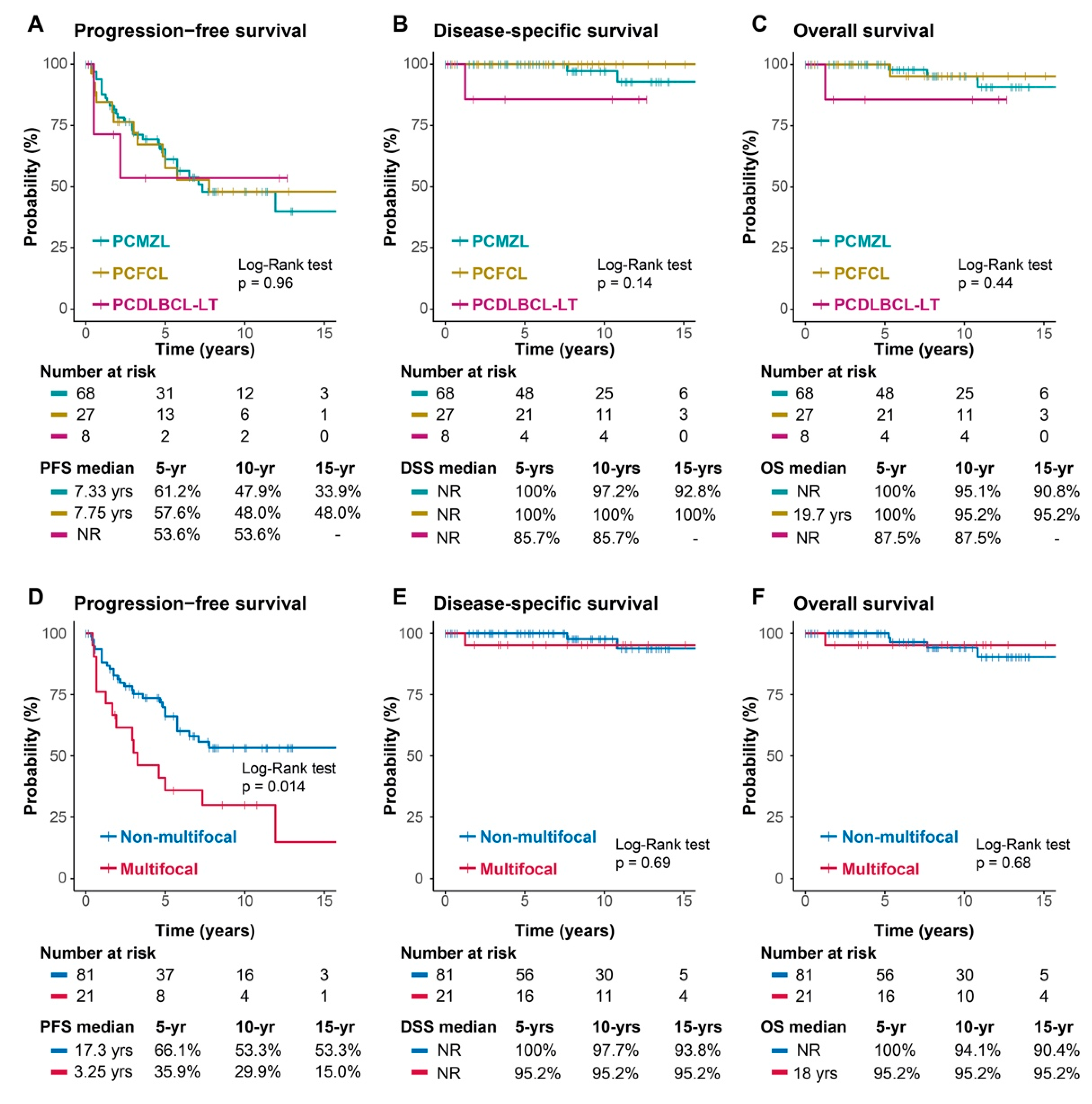
3.5. Response, Recurrence, and Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bradford, P.T.; Devesa, S.S.; Anderson, W.F.; Toro, J.R. Cutaneous lymphoma incidence patterns in the United States: A population-based study of 3884 cases. Blood 2009, 113, 5064–5073. [Google Scholar] [CrossRef]
- Senff, N.J.; Hoefnagel, J.J.; Jansen, P.M.; Vermeer, M.H.; van Baarlen, J.; Blokx, W.A.; Canniga-van Dijk, M.R.; Geerts, M.L.; Hebeda, K.M.; Kluin, P.M.; et al. Reclassification of 300 primary cutaneous B-Cell lymphomas according to the new WHO-EORTC classification for cutaneous lymphomas: Comparison with previous classifications and identification of prognostic markers. J. Clin. Oncol. 2007, 25, 1581–1587. [Google Scholar] [CrossRef] [PubMed]
- Willemze, R.; Cerroni, L.; Kempf, W.; Berti, E.; Facchetti, F.; Swerdlow, S.H.; Jaffe, E.S. The 2018 update of the WHO-EORTC classification for primary cutaneous lymphomas. Blood 2019, 134, 1112. [Google Scholar] [CrossRef] [PubMed]
- Willemze, R.; Kerl, H.; Sterry, W.; Berti, E.; Cerroni, L.; Chimenti, S.; Díaz-Pérez, J.L.; Geerts, M.L.; Goos, M.; Knobler, R.; et al. EORTC classification for primary cutaneous lymphomas: A proposal from the Cutaneous Lymphoma Study Group of the European Organization for Research and Treatment of Cancer. Blood 1997, 90, 354–371. [Google Scholar] [PubMed]
- Willemze, R.; Jaffe, E.S.; Burg, G.; Cerroni, L.; Berti, E.; Swerdlow, S.H.; Ralfkiaer, E.; Chimenti, S.; Díaz-Perez, J.L.; Duncan, L.M.; et al. WHO-EORTC classification for cutaneous lymphomas. Blood 2005, 105, 3768–3785. [Google Scholar] [CrossRef]
- Willemze, R.; Hodak, E.; Zinzani, P.L.; Specht, L.; Ladetto, M.; Committee, E.G. Primary cutaneous lymphomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29 (Suppl. 4), iv30–iv40. [Google Scholar] [CrossRef]
- Goyal, N.; O’Leary, D.; Carter, J.B.; Comfere, N.; Sokumbi, O.; Goyal, A. A Practical Review of the Presentation, Diagnosis, and Management of Cutaneous B-Cell Lymphomas. Dermatol. Clin. 2023, 41, 187–208. [Google Scholar] [CrossRef]
- Kim, Y.H.; Willemze, R.; Pimpinelli, N.; Whittaker, S.; Olsen, E.A.; Ranki, A.; Dummer, R.; Hoppe, R.T. TNM classification system for primary cutaneous lymphomas other than mycosis fungoides and Sezary syndrome: A proposal of the International Society for Cutaneous Lymphomas (ISCL) and the Cutaneous Lymphoma Task Force of the European Organization of Research and Treatment of Cancer (EORTC). Blood 2007, 110, 479–484. [Google Scholar]
- Pham-Ledard, A.; Cowppli-Bony, A.; Doussau, A.; Prochazkova-Carlotti, M.; Laharanne, E.; Jouary, T.; Belaud-Rotureau, M.A.; Vergier, B.; Merlio, J.P.; Beylot-Barry, M. Diagnostic and prognostic value of BCL2 rearrangement in 53 patients with follicular lymphoma presenting as primary skin lesions. Am. J. Clin. Pathol. 2015, 143, 362–373. [Google Scholar] [CrossRef]
- Guinard, E.; Alenezi, F.; Lamant, L.; Szablewski, V.; Tournier, E.; Laurent, C.; Paul, C.; Meyer, N.; Dereure, O.; Boulinguez, S. Staging of primary cutaneous follicle centre B-cell lymphoma: Bone marrow biopsy, CD10, BCL2 and t(14;18) are not relevant prognostic factors. Eur. J. Dermatol. 2019. [Google Scholar]
- Amitay-Laish, I.; Tavallaee, M.; Kim, J.; Hoppe, R.T.; Million, L.; Feinmesser, M.; Fenig, E.; Wolfe, M.E.L.; Hodak, E.; Kim, Y.H. Paediatric primary cutaneous marginal zone B-cell lymphoma: Does it differ from its adult counterpart? Br. J. Dermatol. 2017, 176, 1010–1020. [Google Scholar] [CrossRef]
- Campo, E.; Jaffe, E.S.; Cook, J.R.; Quintanilla-Martínez, L.; Swerdlow, S.H.; Anderson, K.C.; Brousset, P.; Cerroni, L.; de Leval, L.; Dirnhofer, S.; et al. The International Consensus Classification of Mature Lymphoid Neoplasms: A report from the Clinical Advisory Committee. Blood 2022, 140, 1229–1253. [Google Scholar] [CrossRef]
- Dumont, M.; Battistella, M.; Ram-Wolff, C.; Bagot, M.; de Masson, A. Diagnosis and Treatment of Primary Cutaneous B-Cell Lymphomas: State of the Art and Perspectives. Cancers 2020, 12, 1497. [Google Scholar] [CrossRef]
- Swerdlow, S.H. Cutaneous marginal zone lymphomas. Semin. Diagn. Pathol. 2017, 34, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Cerroni, L.; Zöchling, N.; Pütz, B.; Kerl, H. Infection by Borrelia burgdorferi and cutaneous B-cell lymphoma. J. Cutan. Pathol. 1997, 24, 457–461. [Google Scholar] [CrossRef] [PubMed]
- Mandekou-Lefaki, I.; Delli, F.S.; Kountouras, J.; Athanasiou, E.; Mattheou-Vakali, G. Primary cutaneous MALT-type lymphoma and Helicobacter pylori: A possible relationship. J. Eur. Acad. Dermatol. Venereol. 2006, 20, 606–608. [Google Scholar] [CrossRef] [PubMed]
- May, S.A.; Netto, G.; Domiati-Saad, R.; Kasper, C. Cutaneous lymphoid hyperplasia and marginal zone B-cell lymphoma following vaccination. J. Am. Acad. Dermatol. 2005, 53, 512–516. [Google Scholar] [CrossRef] [PubMed]
- Guitart, J.; Deonizio, J.; Bloom, T.; Martinez-Escala, M.E.; Kuzel, T.M.; Gerami, P.; Gerami, P.; Kwasny, M.; Rosen, S.T. High incidence of gastrointestinal tract disorders and autoimmunity in primary cutaneous marginal zone B-cell lymphomas. JAMA Dermatol. 2014, 150, 412–418. [Google Scholar] [CrossRef] [PubMed]
- Edinger, J.T.; Kant, J.A.; Swerdlow, S.H. Cutaneous marginal zone lymphomas have distinctive features and include 2 subsets. Am. J. Surg. Pathol. 2010, 34, 1830–1841. [Google Scholar] [CrossRef] [PubMed]
- Vermeer, M.H.; Geelen, F.A.; van Haselen, C.W.; van Voorst Vader, P.C.; Geerts, M.L.; van Vloten, W.A.; Willzeme, R. Primary cutaneous large B-cell lymphomas of the legs. A distinct type of cutaneous B-cell lymphoma with an intermediate prognosis. Dutch Cutaneous Lymphoma Working Group. Arch. Dermatol. 1996, 132, 1304–1308. [Google Scholar] [CrossRef] [PubMed]
- Pham-Ledard, A.; Prochazkova-Carlotti, M.; Andrique, L.; Cappellen, D.; Vergier, B.; Martinez, F.; Grange, F.; Petrella, T.; Beylot-Barry, M.; Merlio, J.P. Multiple genetic alterations in primary cutaneous large B-cell lymphoma, leg type support a common lymphomagenesis with activated B-cell-like diffuse large B-cell lymphoma. Mod. Pathol. 2014, 27, 402–411. [Google Scholar] [CrossRef]
- Mitteldorf, C.; Berisha, A.; Pfaltz, M.C.; Broekaert, S.M.C.; Schön, M.P.; Kerl, K.; Kempf, W. Tumor Microenvironment and Checkpoint Molecules in Primary Cutaneous Diffuse Large B-Cell Lymphoma-New Therapeutic Targets. Am. J. Surg. Pathol. 2017, 41, 998–1004. [Google Scholar] [CrossRef]
- Pashtan, I.; Mauch, P.M.; Chen, Y.H.; Dorfman, D.M.; Silver, B.; Ng, A.K. Radiotherapy in the management of localized primary cutaneous B-cell lymphoma. Leuk. Lymphoma. 2013, 54, 726–730. [Google Scholar] [CrossRef]
- Specht, L.; Dabaja, B.; Illidge, T.; Wilson, L.D.; Hoppe, R.T.; Group, I.L.R.O. Modern radiation therapy for primary cutaneous lymphomas: Field and dose guidelines from the International Lymphoma Radiation Oncology Group. Int. J. Radiat. Oncol. Biol. Phys. 2015, 92, 32–39. [Google Scholar] [CrossRef]
- Neelis, K.J.; Schimmel, E.C.; Vermeer, M.H.; Senff, N.J.; Willemze, R.; Noordijk, E.M. Low-dose palliative radiotherapy for cutaneous B- and T-cell lymphomas. Int. J. Radiat. Oncol. Biol. Phys. 2009, 74, 154–158. [Google Scholar] [CrossRef]
- Izu-Belloso, R.M.; García-Ruiz, J.C. Treatment of cutaneous lymphomas: An update. Actas Dermosifiliogr. 2012, 103, 694–707. [Google Scholar] [CrossRef]
- Quéreux, G.; Brocard, A.; Peuvrel, L.; Nguyen, J.M.; Knol, A.C.; Dréno, B. Systemic rituximab in multifocal primary cutaneous follicle centre lymphoma. Acta Derm. Venereol. 2011, 91, 562–567. [Google Scholar] [CrossRef]
- Peñate, Y.; Hernández-Machín, B.; Pérez-Méndez, L.I.; Santiago, F.; Rosales, B.; Servitje, O.; Estrach, T.; Fernández-Guarino, M.; Calzado, L.; Acebo, E.; et al. Intralesional rituximab in the treatment of indolent primary cutaneous B-cell lymphomas: An epidemiological observational multicentre study. The Spanish Working Group on Cutaneous Lymphoma. Br. J. Dermatol. 2012, 167, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Leary, D.O.; Goyal, N.; Rubin, N.; Goyal, A. Characterization of Primary and Secondary Cutaneous B-Cell Lymphomas: A Population-Based Study of 4758 Patients. Clin. Lymphoma Myeloma Leuk. 2022, 22, e269–e278. [Google Scholar] [CrossRef] [PubMed]
- Travaglino, A.; Varricchio, S.; Pace, M.; Russo, D.; Picardi, M.; Baldo, A.; Staibano, S.; Mascolo, M. Borrelia burgdorferi in primary cutaneous lymphomas: A systematic review and meta-analysis. J. Dtsch. Dermatol. Ges. 2020, 18, 1379–1384. [Google Scholar] [CrossRef] [PubMed]
- Falkenhain-López, D.; Muniesa, C.; Estrach, M.T.; Morillo-Andújar, M.; Peñate, Y.; Acebo, E.; Pujol, R.M.; García-Muret, M.P.; Machan, S.; Medina, S.; et al. Primary Cutaneous Lymphoma Registry of the Spanish Academy of Dermatology and Venereology (AEDV): Data for the First 5 Years. Actas Dermosifiliogr. 2023, 114, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Dobos, G.; de Masson, A.; Ram-Wolff, C.; Beylot-Barry, M.; Pham-Ledard, A.; Ortonne, N.; Ingen-Housz-Oro, S.; Battistella, M.; d’Incan, M.; Rouanet, J.; et al. Epidemiological changes in cutaneous lymphomas: An analysis of 8593 patients from the French Cutaneous Lymphoma Registry. Br. J. Dermatol. 2021, 184, 1059–1067. [Google Scholar] [CrossRef] [PubMed]
- Hoefnagel, J.J.; Dijkman, R.; Basso, K.; Jansen, P.M.; Hallermann, C.; Willemze, R.; Tensen, C.P.; Vermeer, M.H. Distinct types of primary cutaneous large B-cell lymphoma identified by gene expression profiling. Blood 2005, 105, 3671–3678. [Google Scholar] [CrossRef]
- Menguy, S.; Beylot-Barry, M.; Parrens, M.; Ledard, A.P.; Frison, E.; Comoz, F.; Battistella, M.; Szablewski, V.; Balme, B.; Croue, A.; et al. Primary cutaneous large B-cell lymphomas: Relevance of the 2017 World Health Organization classification: Clinicopathological and molecular analyses of 64 cases. Histopathology 2019, 74, 1067–1080. [Google Scholar] [CrossRef]
- Olszewska-Szopa, M.; Sobas, M.; Laribi, K.; Bao Perez, L.; Drozd-Sokołowska, J.; Subocz, E.; Jocks, M.; Zduniak, K.; Gajewska, M.; de Nalecz, A.K.; et al. Primary cutaneous indolent B-cell lymphomas—A retrospective multicenter analysis and a review of literature. Acta Oncol. 2021, 60, 1361–1368. [Google Scholar] [CrossRef]
- Oertel, M.; Elsayad, K.; Weishaupt, C.; Steinbrink, K.; Eich, H.T. De-escalated radiotherapy for indolent primary cutaneous B-cell lymphoma. Strahlenther. Onkol. 2020, 196, 126–131. [Google Scholar] [CrossRef]
- Vitiello, P.; Sica, A.; Ronchi, A.; Caccavale, S.; Franco, R.; Argenziano, G. Primary Cutaneous B-Cell Lymphomas: An Update. Front. Oncol. 2020, 10, 651. [Google Scholar] [CrossRef]
- Kraft, R.M.; Ansell, S.M.; Villasboas, J.C.; Bennani, N.N.; Wang, Y.; Habermann, T.M.; Thanarajasingam, G.; Lester, S.C.; Macon, W.; Inwards, D.J.; et al. Outcomes in primary cutaneous diffuse large B-cell lymphoma, leg type. Hematol. Oncol. 2021, 39, 658–663. [Google Scholar] [CrossRef] [PubMed]
- Krenitsky, A.; Klager, S.; Hatch, L.; Sarriera-Lazaro, C.; Chen, P.L.; Seminario-Vidal, L. Update in Diagnosis and Management of Primary Cutaneous B-Cell Lymphomas. Am. J. Clin. Dermatol. 2022, 23, 689–706. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total Cases N = 103 | PCMZL N = 68 | PCFCL N = 27 | PCDLBCL-LT N = 8 | |
|---|---|---|---|---|---|
| Gender | Female | 53 (51%) | 32 (47%) | 18 (67%) | 3 (38%) |
| Male | 50 (49%) | 36 (53%) | 9 (33%) | 5 (62%) | |
| Age | Median (range) | 53 (11, 85) | 51 (11, 82) | 56 (24, 77) | 66 (40, 85) |
| ECOG | 0 | 90 (87%) | 62 (91%) | 23 (85%) | 5 (56%) |
| 1 | 9 (9%) | 5 (7%) | 2 (7%) | 2 (25%) | |
| 2 | 1 (1%) | 0 | 0 | 1 (12%) | |
| ≥3 | 0 | 0 | 0 | 0 | |
| Unknown | 3 (3%) | 1 (1.4%) | 2 (7%) | 0 | |
| Stage | I | 79 (77%) | 54 (79%) | 20 (74%) | 5 (62%) |
| II | 22 (21%) | 13 (19%) | 7 (26%) | 2 (25%) | |
| III | 0 | 0 | 0 | 0 | |
| IV | 2 (2%) | 1 (1%) | 0 | 1 (12%) | |
| Prior skin disease | Yes | 15 (14.6%) | 12 (18%) | 3 (11%) | 0 |
| No | 81 (78.6%) | 50 (74%) | 24 (89%) | 7 (88%) | |
| Unknown | 7 (6.8%) | 6 (9%) | 0 | 1 (12%) | |
| Tumour main location | Head and neck | 24 (23%) | 13 (19%) | 8 (30%) | 3 (38%) |
| Trunk | 56 (54%) | 40 (59%) | 14 (52%) | 2 (25%) | |
| Upper limbs | 14 (14%) | 8 (12%) | 4 (15%) | 2 (25%) | |
| Lower limbs | 5 (5%) | 4 (6%) | 0 | 1 (12%) | |
| Undetermined | 4 (4%) | 3 (4%) | 1 (4%) | 0 | |
| Tumour extension | Unique | 64 (62%) | 44 (65%) | 15 (56%) | 5 (62%) |
| Regional | 17 (17%) | 10 (15%) | 5 (19%) | 2 (25%) | |
| Multifocal | 21 (20%) | 13 (19%) | 7 (26%) | 1 (12%) | |
| Unknown | 1 (1%) | 1 (1%) | 0 | 0 | |
| Primary outcome | Complete response | 99 (96%) | 67 (99%) | 25 (93%) | 7 (88%) |
| No response | 4 (4%) | 1 (1%) | 2 (7%) | 1 (12%) | |
| Relapse | Yes | 45 (44%) | 30 (44%) | 12 (44%) | 3 (38%) |
| Number of relapses | 1–3 relapses | 35 (34%) | 24 (35%) | 9 (33%) | 2 (25%) |
| >3 relapses | 8 (7.8%) | 5 (7.4%) | 3 (11%) | 0 | |
| Unknown number | 2 (1.9%) | 1 (1.5%) | 0 | 1 (13%) | |
| Site of relapse | Local | 22 (21%) | 14 (21%) | 6 (22%) | 2 (25%) |
| Regional | 9 (8.7%) | 8 (12%) | 1 (3.7%) | 0 | |
| Distant | 10 (9.7%) | 6 (8.8%) | 4 (15%) | 0 | |
| Unknown | 4 (3.9%) | 2 (2.9%) | 1 (3.7%) | 1 (13%) | |
| Deaths | By lymphoma | 3 (3%) | 2 (3%) | 0 | 1 (12%) |
| By other causes | 4 (4%) | 2 (3%) | 2 (7%) | 0 |
| Treatments | Total Cases N = 103 | PCMZL N = 68 | PCFCL N = 27 | PCDLBCL-LT N = 8 | |
|---|---|---|---|---|---|
| Only local | 73 (70.9%) | 51 (75%) | 19 (70.4%) | 3 (37.5%) | |
| Only S | 24 (23.3%) | 19 (28%) | 5 (18.5%) | 0 | |
| Only RT | 27 (26.2%) | 20 (29%) | 7 (25.9%) | 0 | |
| S + RT | 22 (21.4%) | 12 (18%) | 7 (25.9%) | 3 (37.5%) | |
| Only systemic | 14 (13.6%) | 9 (13.2%) | 3 (11.1%) | 2 (25%) | |
| Only CT or R-CT | 10 (9.7%) | 6 (8.8%) | 2 (7.4%) | 2 (25%) | |
| Only systemic rituximab | 4 (3.9%) | 3 (4.4%) | 1 (3.7%) | 0 | |
| Local + Systemic | 12 (11.6%) | 7 (8.8%) | 3 (11.1%) | 3 (37.5%) | |
| S + ST | 5 (4.8%) | 2 (2.9%) | 1 (3.7%) | 2 (25%) | |
| RT + ST | 6 (5.8%) | 3 (4.4%) | 2 (7.4%) | 1 (12.5%) | |
| S + RT + ST | 1 (1%) | 1 (1.5%) | 0 | 0 | |
| Other therapies | 4 (3.9%) | 2 (3%) | 1 (7.4%) | 0 | |
| RT + ILR | 1 (1%) | 1 (1.5%) | 0 | 0 | |
| Only ILR | 1 (1%) | 0 | 1 (3.7%) | 0 | |
| Only Intralesional corticoids | 1 (1%) | 0 | 1 (3.7%) | 0 | |
| Doxycycline | 1 (1%) | 1 (1.5%) | 0 | 0 |
| Treatments | Total Cases N = 103 | PCMZL N = 68 | PCFCL N = 27 | PCDLBCL-LT N = 8 | |
|---|---|---|---|---|---|
| Any surgery | 52 (50%) | 34 (49%) | 13 (48%) | 5 (62%) | |
| Any CT | 26 (25%) | 15 (22%) | 6 (22%) | 5 (62%) | |
| CHOP | 4 (15%) | 2 (13%) | 1 (17%) | 1 (20%) | |
| R-CHOP | 8 (31%) | 4 (27%) | 1 (17%) | 3 (60%) | |
| R-CTX/R-CVP | 3 (12%) | 1 (7%) | 1 (17%) | 1 (20%) | |
| Rituximab | 7 (27%) | 4 (27%) | 3 (50%) | 0 | |
| Cyclophosphamide | 1 (4%) | 1 (7%) | 0 | 0 | |
| Chlorambucil | 2 (8%) | 2 (13%) | 0 | 0 | |
| CT not specified | 1 (4%) | 1 (7%) | 0 | 0 | |
| Any RT | 57 (55%) | 37 (54%) | 16 (59%) | 4 (50%) | |
| 30–35 Gy | 6 (11%) | 5 (14%) | 1 (6%) | 0 | |
| 36–40 Gy | 24 (42%) | 19 (51%) | 5 (31%) | 0 | |
| 41–45 Gy | 4 (7%) | 2 (5%) | 1 (6%) | 1 (25%) | |
| 46–50 Gy | 2 (4%) | 2 (5%) | 0 | 0 | |
| Dose not specified | 21 (37%) | 9 (24%) | 9 (56%) | 3 (75%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Banaclocha, N.; Martínez-Madueño, F.; Caballé, B.; Badia, J.; Blanes, M.; Bujanda, D.A.; Calvo, V.; Gómez Codina, J.; Blanco, C.Q.; Espinosa, P.; et al. A Descriptive Study of 103 Primary Cutaneous B-Cell Lymphomas: Clinical and Pathological Characteristics and Treatment from the Spanish Lymphoma Oncology Group (GOTEL). Cancers 2024, 16, 1034. https://doi.org/10.3390/cancers16051034
Martínez-Banaclocha N, Martínez-Madueño F, Caballé B, Badia J, Blanes M, Bujanda DA, Calvo V, Gómez Codina J, Blanco CQ, Espinosa P, et al. A Descriptive Study of 103 Primary Cutaneous B-Cell Lymphomas: Clinical and Pathological Characteristics and Treatment from the Spanish Lymphoma Oncology Group (GOTEL). Cancers. 2024; 16(5):1034. https://doi.org/10.3390/cancers16051034
Chicago/Turabian StyleMartínez-Banaclocha, Natividad, Francisca Martínez-Madueño, Berta Caballé, Joan Badia, Mar Blanes, David Aguiar Bujanda, Virginia Calvo, Jose Gómez Codina, Cristina Quero Blanco, Pablo Espinosa, and et al. 2024. "A Descriptive Study of 103 Primary Cutaneous B-Cell Lymphomas: Clinical and Pathological Characteristics and Treatment from the Spanish Lymphoma Oncology Group (GOTEL)" Cancers 16, no. 5: 1034. https://doi.org/10.3390/cancers16051034