
Sarcopenic Obesity in Cervical Carcinoma: A Strong and Independent Prognostic Factor beyond the Conventional Predictors (ESTHER Study—AFRAID Project)

 , , , ,
, , , ,  , , ,
, , ,  ,
,  , ,
, , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Objective and Design
2.2. Staging, Treatment, and Follow-Up
2.3. Examined Parameters
2.3.1. Patient, Tumor, and Treatment Information
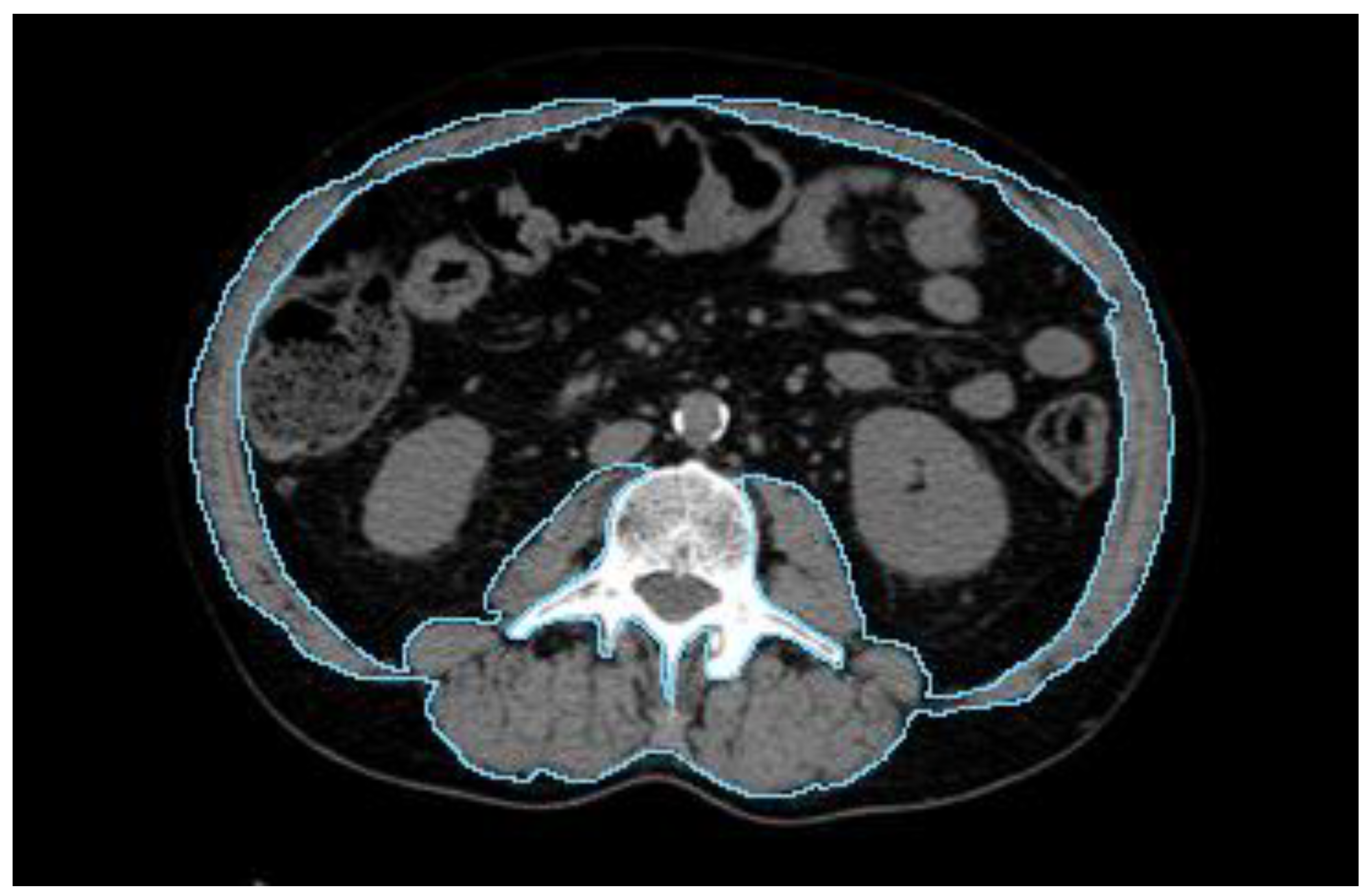
2.3.2. Body Composition Parameters
2.4. Statistical Analysis
3. Results
3.1. Patient Demographics
3.2. Treatment Details
3.3. Univariate Analysis
3.4. Multivariate Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef]
- Morris, M.; Eifel, P.J.; Lu, J.; Grigsby, P.W.; Levenback, C.; Stevens, R.E.; Rotman, M.; Gershenson, D.M.; Mutch, D.G. Pelvic Radiation with Concurrent Chemotherapy Compared with Pelvic and Para-Aortic Radiation for High-Risk Cervical Cancer. N. Engl. J. Med. 1999, 340, 1137–1143. [Google Scholar] [CrossRef]
- Chemoradiotherapy for Cervical Cancer Meta-Analysis Collaboration. Reducing uncertainties about the effects of chemoradiotherapy for cervical cancer: A systematic review and meta-analysis of individual patient data from 18 randomized trials. J. Clin. Oncol. 2008, 26, 5802–5812. [Google Scholar] [CrossRef] [PubMed]
- Templeton, A.J.; Ace, O.; McNamara, M.G.; Al-Mubarak, M.; Vera-Badillo, F.E.; Hermanns, T.; Seruga, B.; Ocaña, A.; Tannock, I.F.; Amir, E. Prognostic Role of Platelet to Lymphocyte Ratio in Solid Tumors: A Systematic Review and Meta-Analysis. Cancer Epidemiol. Biomark. Prev. 2014, 23, 1204–1212. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.H. Management of recurrent cervical cancer. Chang Gung Med. J. 2004, 27, 711–717. [Google Scholar] [PubMed]
- Atahan, I.L.; Onal, C.; Ozyar, E.; Yiliz, F.; Selek, U.; Kose, F. Long-term outcome and prognostic factors in patients with cervical carcinoma: A retrospective study. Int. J. Gynecol. Cancer 2007, 17, 833–842. [Google Scholar] [CrossRef]
- Winter, W.E.; Maxwel, G.L.; Tian, C.; Sobel, E.; Rose, G.S.; Thomas, G.; Carlson, J.W. Association of hemoglobin level with survival in cervical carcinoma patients treated with concurrent cisplatin and radiotherapy: A Gynecologic Oncology Group Study. Gynecol. Oncol. 2004, 94, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Grogan, M.; Thomas, G.M.; Melamed, I.; Wong, F.L.; Pearcey, R.G.; Joseph, P.K.; Portelance, L.; Crook, J.; Jones, K.D. The importance of hemoglobin levels during radiotherapy for carcinoma of the cervix. Cancer 1999, 86, 1528–1536. [Google Scholar] [CrossRef]
- Thomas, G. The effect of hemoglobin level on radiotherapy outcomes: The Canadian experience. Semin. Oncol. 2001, 28 (Suppl. S8), 60–65. [Google Scholar] [CrossRef] [PubMed]
- Koulis, T.A.; Kornaga, E.N.; Banerjee, R.; Phan, T.; Ghatage, P.; Magliocco, A.M.; Lees-Miller, S.P.; Doll, C.M. Anemia, leukocytosis and thrombocytosis as prognostic factors in patients with cervical cancer treated with radical chemoradiotherapy: A retrospective cohort study. Clin. Transl. Radiat. Oncol. 2017, 4, 51–56. [Google Scholar] [CrossRef]
- Medici, F.; Rizzo, S.; Buwenge, M.; Arcelli, A.; Ferioli, M.; Macchia, G.; Deodato, F.; Cilla, S.; De Iaco, P.; Perrone, A.M.; et al. Everything You Always Wanted to Know about Sarcopenia but Were Afraid to Ask: A Quick Guide for Radiation Oncologists (Impact of Sarcopenia in Radiotherapy: The AFRAID Project). Curr. Oncol. 2022, 29, 8513–8528. [Google Scholar] [CrossRef] [PubMed]
- Medici, F.; Bazzocchi, A.; Buwenge, M.; Zamagni, A.; Macchia, G.; Deodato, F.; Cilla, S.; De Iaco, P.; Perrone, A.M.; Strigari, L.; et al. Impact and Treatment of Sarcopenia in Patients Undergoing Radiotherapy: A Multidisciplinary, AMSTAR-2 Compliant Review of Systematic Reviews and Metanalyses. Front. Oncol. 2022, 12, 887156. [Google Scholar] [CrossRef]
- Kiyotoki, T.; Nakamura, K.; Haraga, J.; Omichi, C.; Ida, N.; Saijo, M.; Nishida, T.; Kusumoto, T.; Masuyama, H. Sarcopenia Is an Important Prognostic Factor in Patients With Cervical Cancer Undergoing Concurrent Chemoradiotherapy. Int. J. Gynecol. Cancer 2018, 28, 168–175. [Google Scholar] [CrossRef]
- Abe, A.; Yuasa, M.; Imai, Y.; Kagawa, T.; Mineda, A.; Nishimura, M.; Tonoiso, C.; Kubo, A.; Kawanaka, T.; Ikushima, H.; et al. Extreme leanness, lower skeletal muscle quality, and loss of muscle mass during treatment are predictors of poor prognosis in cervical cancer treated with concurrent chemoradiation therapy. Int. J. Clin. Oncol. 2022, 27, 983–991. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Chang, C.L.; Lin, J.B.; Wu, M.H.; Sun, F.J.; Jan, Y.T.; Hsu, S.M.; Chen, Y.J. Skeletal Muscle Loss Is an Imaging Biomarker of Outcome after Definitive Chemoradiotherapy for Locally Advanced Cervical Cancer. Clin. Cancer Res. 2018, 24, 5028–5036. [Google Scholar] [CrossRef] [PubMed]
- Gnade, C.M.; Hill, E.K.; Botkin, H.E.; Hefel, A.R.; Hansen, H.E.; Sheets, K.A.; Mott, S.L.; Hardy-Fairbanks, A.J.; Stockdale, C.K. Effect of Obesity on Cervical Cancer Screening and Outcomes. J. Low Genit. Tract Dis. 2020, 24, 358–362. [Google Scholar] [CrossRef]
- Clark, L.H.; Jackson, A.L.; Soo, A.E.; Orrey, D.C.; Gehrig, P.A.; Kim, K.H. Extremes in body mass index affect overall survival in women with cervical cancer. Gynecol. Oncol. 2016, 141, 497–500. [Google Scholar] [CrossRef]
- Münstedt, K.; Wagner, M.; Kullmer, U.; Hackethal, A.; Franke, F.E. Influence of body mass index on prognosis in gynecological malignancies. Cancer Causes Control. 2008, 19, 909–916. [Google Scholar] [CrossRef]
- Haraga, J.; Nakamura, K.; Omichi, C.; Nishida, T.; Haruma, T.; Kusumoto, T.; Seki, N.; Masuyama, H.; Katayama, N.; Kanazawa, S.; et al. Pretreatment prognostic nutritional index is a significant predictor of prognosis in patients with cervical cancer treated with concurrent chemoradiotherapy. Mol. Clin. Oncol. 2016, 5, 567–574. [Google Scholar] [CrossRef]
- Wang, H.B.; Xu, X.T.; Tian, M.X.; Ding, C.C.; Tang, J.; Qian, Y.; Jin, X. Prognostic values of the prognostic nutritional index, geriatric nutritional risk index, and systemic inflammatory indexes in patients with stage IIB-III cervical cancer receiving radiotherapy. Front. Nutr. 2023, 10, 1000326. [Google Scholar] [CrossRef]
- Guo, J.; Lv, W.; Wang, Z.; Shang, Y.; Yang, F.; Zhang, X.; Xiao, K.; Zhang, S.; Pan, X.; Han, Y.; et al. Prognostic Value of Inflammatory and Nutritional Markers for Patients With Early-Stage Poorly-to Moderately-Differentiated Cervical Squamous Cell Carcinoma. Cancer Control 2023, 30, 10732748221148913. [Google Scholar] [CrossRef]
- Ferioli, M.; Benini, A.; Malizia, C.; Forlani, L.; Medici, F.; Laghi, V.; Ma, J.; Galuppi, A.; Cilla, S.; Buwenge, M.; et al. Classical Prognostic Factors Predict Prognosis Better than Inflammatory Indices in Locally Advanced Cervical Cancer: Results of a Comprehensive Observational Study including Tumor-, Patient-, and Treatment-Related Data (ESTHER Study). J. Personal. Med. 2023, 13, 1229. [Google Scholar] [CrossRef]
- Medici, F.; Ferioli, M.; Forlani, L.; Laghi, V.; Ma, J.; Cilla, S.; Buwenge, M.; Macchia, G.; Deodato, F.; Vadalà, M.; et al. Decoding the Complexity of Systemic Inflammation Predictors in Locally Advanced Cervical Cancer, with Hemoglobin as the Hidden Key (the ESTHER Study). Cancers 2023, 15, 5056. [Google Scholar] [CrossRef]
- Deodato, F.; Cilla, S.; Massaccesi, M.; Macchia, G.; Ippolito, E.; Caravatta, L.; Picardi, V.; Romanella, M.; Di Falco, C.; Bartollino, A.; et al. Daily on-line set-up correction in 3D-conformal radiotherapy: Is it feasible? Tumori 2012, 98, 441–444. [Google Scholar] [CrossRef]
- Weir, C.B.; Jan, A. BMI Classification Percentile and Cut off Points. StatPearls. 2023. Available online: http://www.ncbi.nlm.nih.gov/books/NBK541070/ (accessed on 9 October 2023).
- Amini, B.; Boyle, S.P.; Boutin, R.D.; Lenchik, L. Approaches to Assessment of Muscle Mass and Myosteatosis on Computed Tomography: A Systematic Review. J. Gerontol. A Biol. Sci. Med. Sci. 2019, 74, 1671–1678. [Google Scholar] [CrossRef]
- Shen, W.; Punyanitya, M.; Wang, Z.; Gallagher, D.; St-Onge, M.-P.; Albu, J.; Heymsfield, S.B.; Heshka, S. Total body skeletal muscle and adipose tissue volumes: Estimation from a single abdominal cross-sectional image. J. Appl. Physiol. 2004, 97, 2333–2338. [Google Scholar] [CrossRef] [PubMed]
- Prado, C.M.M.; Lieffers, J.R.; McCargar, L.J.; Reiman, T.; Sawyer, M.B.; Martin, L.; Baracos, V.E. Prevalence and clinical implications of sarcopenic obesity in patients with solid tumours of the respiratory and gastrointestinal tracts: A population-based study. Lancet Oncol. 2008, 9, 629–635. [Google Scholar] [CrossRef]
- Martin, L.; Birdsell, L.; Macdonald, N.; Reiman, T.; Clandinin, M.T.; McCargar, L.J.; Murphy, R.; Ghosh, S.; Sawyer, M.B.; Baracos, V.E. Cancer cachexia in the age of obesity: Skeletal muscle depletion is a powerful prognostic factor, independent of body mass index. J. Clin. Oncol. 2013, 31, 1539–1547. [Google Scholar] [CrossRef]
- Quinn, B.A.; Deng, X.; Colton, A.; Bandyopadhyay, D.; Carter, J.S.; Fields, E.C. Increasing age predicts poor cervical cancer prognosis with subsequent effect on treatment and overall survival. Brachytherapy 2019, 18, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Perez, C.A. Dose fractionation and biological optimization in carcinoma of the uterine cervix. Rays 2004, 29, 253–270. [Google Scholar] [PubMed]
- Legge, F.; Margariti, P.A.; Lucidi, A.; Macchia, G.; Petrillo, M.; Iannone, V.; Carone, V.; Morganti, A.G.; Scambia, G. Completion surgery after concomitant chemoradiation in obese women with locally advanced cervical cancer: Evaluation of toxicity and outcome measures. Acta Oncol. 2013, 52, 166–173. [Google Scholar] [CrossRef] [PubMed]
- Anandavadivelan, P.; Brismar, T.B.; Nilsson, M.; Johar, A.M.; Martin, L. Sarcopenic obesity: A probable risk factor for dose limiting toxicity during neo-adjuvant chemotherapy in oesophageal cancer patients. Clin. Nutr. 2016, 35, 724–730. [Google Scholar] [CrossRef] [PubMed]
- Baracos, V.E.; Arribas, L. Sarcopenic obesity: Hidden muscle wasting and its impact for survival and complications of cancer therapy. Ann. Oncol. 2018, 29 (Suppl. S2), ii1–ii9. [Google Scholar] [CrossRef] [PubMed]
- Malietzis, G.; Johns, N.; Al-Hassi, H.O.; Knight, S.C.; Kennedy, R.H.; Fearon, K.C.; Aziz, O.; Jenkins, J.T. Low Muscularity and Myosteatosis Is Related to the Host Systemic Inflammatory Response in Patients Undergoing Surgery for Colorectal Cancer. Ann. Surg. 2016, 263, 320–325. [Google Scholar] [CrossRef] [PubMed]
- Kalinkovich, A.; Livshits, G. Sarcopenic obesity or obese sarcopenia: A cross talk between age-associated adipose tissue and skeletal muscle inflammation as a main mechanism of the pathogenesis. Ageing Res. Rev. 2017, 35, 200–221. [Google Scholar] [CrossRef]
- Nishigori, T.; Obama, K.; Sakai, Y. Assessment of body composition and impact of sarcopenia and sarcopenic obesity in patients with gastric cancer. Transl. Gastroenterol. Hepatol. 2020, 5, 22. [Google Scholar] [CrossRef]
- Khaddour, K.; Gomez-Perez, S.L.; Jain, N.; Patel, J.D.; Boumber, Y. Obesity, Sarcopenia, and Outcomes in Non-Small Cell Lung Cancer Patients Treated With Immune Checkpoint Inhibitors and Tyrosine Kinase Inhibitors. Front. Oncol. 2020, 10, 576314. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Lima, G.M.; Matti, A.; Vara, G.; Dondi, G.; Naselli, N.; De Crescenzo, E.M.; Morganti, A.G.; Perrone, A.M.; De Iaco, P.; Nanni, C.; et al. Prognostic value of posttreatment 18F-FDG PET/CT and predictors of metabolic response to therapy in patients with locally advanced cervical cancer treated with concomitant chemoradiation therapy: An analysis of intensity- and volume-based PET parameters. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 2139–2146. [Google Scholar] [CrossRef]
- Laliscia, C.; Gadducci, A.; Mattioni, R.; Orlandi, F.; Giusti, S.; Barcellini, A.; Gabelloni, M.; Morganti, R.; Neri, E.; Paiar, F. MRI-based radiomics: Promise for locally advanced cervical cancer treated with a tailored integrated therapeutic approach. Tumori 2022, 108, 376–385. [Google Scholar] [CrossRef]
- Wang, J.; Mao, Y.; Gao, X.; Zhang, Y. Recurrence risk stratification for locally advanced cervical cancer using multi-modality transformer network. Front. Oncol. 2023, 13, 1100087. [Google Scholar] [CrossRef]
- Sun, C.; Tian, X.; Liu, Z.; Li, W.; Li, P.; Chen, J.; Zhang, W.; Fang, Z.; Du, P.; Duan, H.; et al. Radiomic analysis for pretreatment prediction of response to neoadjuvant chemotherapy in locally advanced cervical cancer: A multicentre study. EBioMedicine 2019, 46, 160–169. [Google Scholar] [CrossRef] [PubMed]
- Herbst, J.; Pantel, K.; Effenberger, K.; Wikman, H. Clinical applications and utility of cell-free DNA-based liquid biopsy analyses in cervical cancer and its precursor lesions. Br. J. Cancer 2022, 127, 1403–1410. [Google Scholar] [CrossRef] [PubMed]
- Han, K.; Leung, E.; Barbera, L.; Barnes, E.; Croke, J.; Di Grappa, M.A.; Fyles, A.; Metser, U.; Milosevic, M.; Pintilie, M.; et al. Circulating Human Papillomavirus DNA as a Biomarker of Response in Patients With Locally Advanced Cervical Cancer Treated With Definitive Chemoradiation. JCO Precis. Oncol. 2018, 2, 1–8. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Value | Patients No | 2 y LC | 5 y LC | p | 2 y DMFS | 5 y DMFS | p | 2 y DFS | 5 y DFS | p | 2 y OS | 5 y OS | p |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age (years) | <55 | 77 | 84.2 | 82.3 | 0.909 | 84.7 | 83.1 | 0.049 | 70.3 | 66.7 | 0.418 | 90.2 | 79.3 | 0.003 |
| 55 ≤ age < 70 | 62 | 81.1 | 81.1 | 82.2 | 72.6 | 73.0 | 66.1 | 87.7 | 69.7 | |||||
| ≥70 | 34 | 83.7 | 83.7 | 64.8 | 60.5 | 59.5 | 55.2 | 79.2 | 49.4 | |||||
| cN stage | 0 | 102 | 86.9 | 85.3 | 0.271 | 86.1 | 81.6 | 0.045 | 75.0 | 68.9 | 0.101 | 87.2 | 75.1 | 0.194 |
| 1–2 | 71 | 77.3 | 77.3 | 70.8 | 64.7 | 61.0 | 57.1 | 87.5 | 64.6 | |||||
| Total dose (Gy) | ≤75 | 129 | 81.1 | 81.1 | 0.317 | 79.1 | 73.4 | 0.899 | 67.7 | 62.0 | 0.596 | 83.9 | 66.6 | 0.012 |
| >75 | 44 | 88.4 | 85.8 | 81.8 | 77.0 | 72.7 | 68.0 | 97.4 | 81.6 | |||||
| FIGO stage | I–II | 77 | 93.4 | 91.5 | 0.005 | 90.3 | 85.1 | 0.021 | 82.2 | 74.8 | 0.003 | 93.3 | 80.5 | 0.032 |
| III | 73 | 77.7 | 77.7 | 71.1 | 63.8 | 61.2 | 56.6 | 84.4 | 58.8 | |||||
| IV | 23 | 64.2 | 64.2 | 72.8 | 72.8 | 49.7 | 49.7 | 74.7 | 68.5 | |||||
| Maximum tumor diameter | ≤4 | 55 | 91.9 | 89.0 | 0.114 | 84,3 | 75.9 | 0.910 | 77.0 | 68.4 | 0.403 | 88.3 | 74,3 | 0.675 |
| >4 | 118 | 78.8 | 78.8 | 77.8 | 74.2 | 65.5 | 62.0 | 87.0 | 69.1 | |||||
| Histological type | SCC | 139 | 82.8 | 81.6 | 0.598 | 80.0 | 74.4 | 0.799 | 69.1 | 63.6 | 0.917 | 89.0 | 72.3 | 0.305 |
| N-SCC | 34 | 84.4 | 84.4 | 80.0 | 76.6 | 69.6 | 66.4 | 81.6 | 63.9 | |||||
| Overall treatment | ≤54 | 92 | 83.4 | 81.7 | 0.888 | 78.1 | 73.1 | 0.536 | 68.4 | 63.7 | 0.892 | 86.1 | 75.9 | 0.254 |
| >54 | 81 | 82.8 | 82.8 | 82.0 | 76.6 | 70.0 | 64.5 | 88.8 | 65.5 | |||||
| Hemoglobin | <10 | 16 | 49.2 | 49.2 | <0.001 | 72.3 | 72.3 | 0.270 | 48.1 | 48.1 | 0.007 | 55.0 | 55.0 | 0.040 |
| 10 ≤ Hb < 12 | 42 | 73.3 | 69.7 | 79.5 | 79.5 | 63.4 | 60.1 | 79.5 | 66.8 | |||||
| ≥12 | 115 | 91.4 | 91.4 | 81.4 | 73.9 | 74.3 | 67.7 | 94.2 | 73.9 | |||||
| Body Mass Index | <18.5 | 7 | 85.7 | 85.7 | 0.247 | 71.4 | 71.4 | 0.033 | 71.4 | 71.4 | 0.018 | 85.7 | 42.9 | 0.023 |
| 18.5 ≤ BMI < 25 | 90 | 89.9 | 88.3 | 87.0 | 85.6 | 79.0 | 75.8 | 91.9 | 79.9 | |||||
| 25 ≤ BMI < 30 | 49 | 74.4 | 74.4 | 72.8 | 62.7 | 60.5 | 52.1 | 82.1 | 61.3 | |||||
| ≥30 | 27 | 75.5 | 75.5 | 71.1 | 60.2 | 51.9 | 46.7 | 82.5 | 56.2 | |||||
| Sarcopenia | ≤7.53 | 19 | 94.7 | 94.7 | 0.175 | 77.5 | 77.5 | 0.902 | 77.5 | 77.5 | 0.284 | 94.7 | 78.9 | 0.266 |
| >7.53 | 153 | 81.5 | 80.5 | 80.1 | 74.2 | 67.9 | 62.3 | 86.4 | 69.4 | |||||
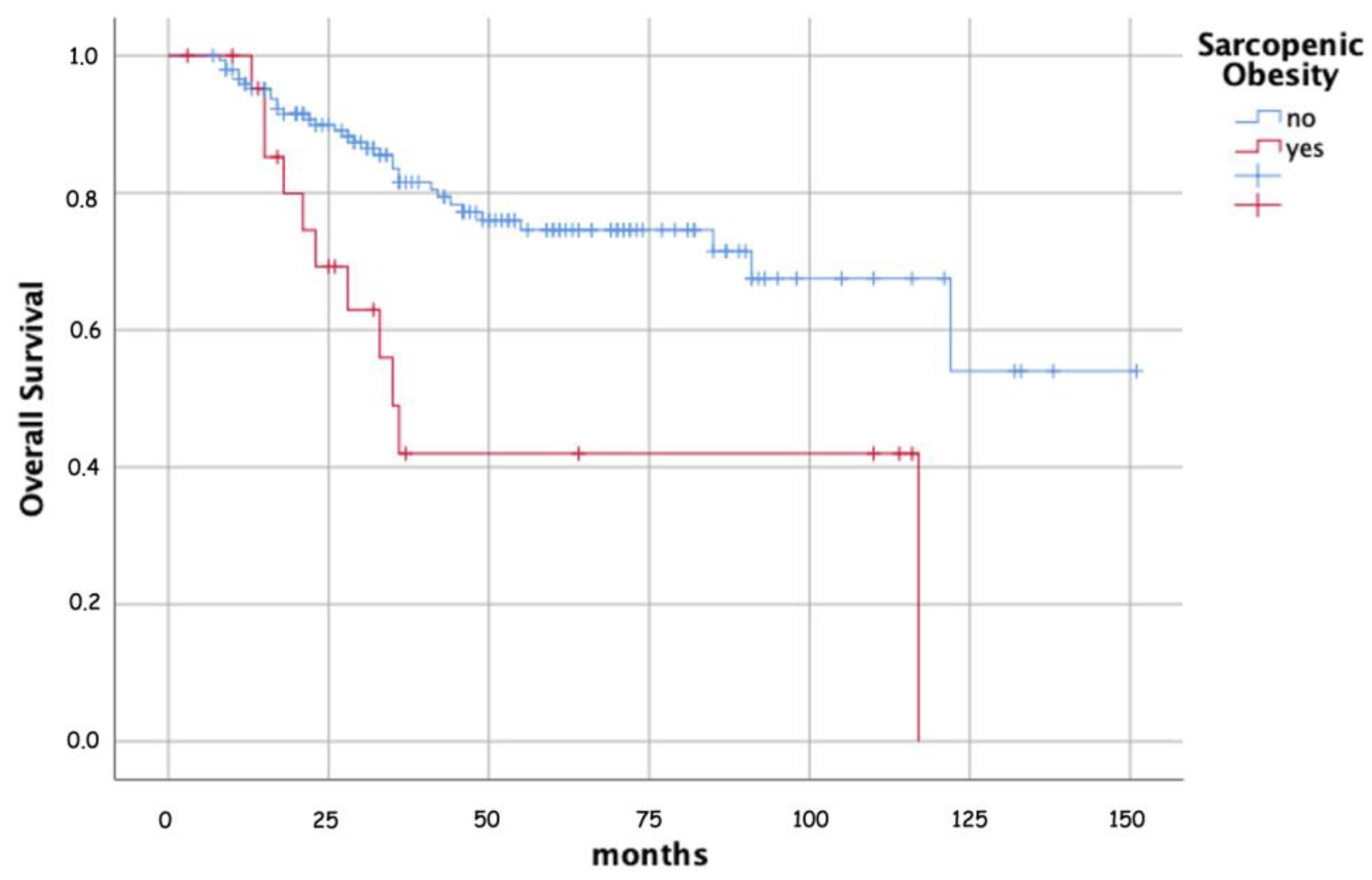
| Sarcopenic obesity | 0 | 148 | 85.4 | 84.3 | 0.066 | 81.8 | 77.7 | 0.110 | 73.3 | 68.3 | 0.005 | 89.9 | 74.6 | <0.001 |
| 1 | 23 | 66.7 | 66.7 | 69.9 | 55.9 | 43.0 | 36.8 | 69.2 | 42.0 |
| Parameter | Values | Patients N (%) | LC | DMFS | DFS | OS | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HR | 95%CI | p | HR | 95%CI | p | HR | 95%CI | p | HR | 95%CI | p | |||
| Age (years) | <55 | 77 | 1 | rif. | 0.024 | 1 | rif. | 0.003 | ||||||
| 55 ≤ age < 70 | 62 | 1.336 | 0.642–2.781 | 0.438 | 2.052 | 0.936–4.502 | 0.073 | |||||||
| ≥70 | 34 | 2.919 | 1.334–6.388 | 0.007 | 4.403 | 1.878–10.322 | <0.001 | |||||||
| Total dose (Gy) | ≤75 | 129 | 1 | rif. | 0.016 | |||||||||
| >75 | 44 | 0.368 | 0.163–0.831 | |||||||||||
| FIGO stage | I–II | 77 | 1 | rif. | 0.083 | 1 | rif. | 0.019 | 1 | rif. | 0.031 | 1 | rif. | 0.008 |
| III | 73 | 2.128 | 0.858–5.227 | 0.103 | 2.664 | 1.318–5.384 | 0.006 | 2.148 | 1.187–3.884 | 0.011 | 3.077 | 1.515–6.250 | 0.002 | |
| IV | 23 | 3.210 | 1.135–9.083 | 0.028 | 2.676 | 0.974–7.352 | 0.056 | 2.124 | 0.959–4.707 | 0.063 | 2.496 | 0.873–7.139 | 0.088 | |
| Hemoglobin | <10 | 16 | 1 | rif. | <0.001 | 1 | rif. | 0.024 | 1 | rif. | 0.010 | |||
| 10 ≤ Hb < 12 | 42 | 0.395 | 0.155–1.009 | 0.052 | 0.394 | 0.168–0.922 | 0.032 | 0.400 | 0.147–1.087 | 0.072 | ||||
| ≥12 | 115 | 0.129 | 0.049–0.340 | <0.001 | 0.347 | 0.161–0.747 | 0.007 | 0.227 | 0.086–0.601 | 0.003 | ||||
| Sarcopenic obesity | 0 | 148 | 1 | rif. | 0.071 | 1 | rif. | 0.020 | 1 | rif. | 0.009 | |||
| 1 | 23 | 2.257 | 0.933–5.457 | 5.289 | 1.298–21.546 | 2.645 | 1.275–5.488 | |||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Medici, F.; Ferioli, M.; Cammelli, S.; Forlani, L.; Laghi, V.; Ma, J.; Cilla, S.; Buwenge, M.; Macchia, G.; Deodato, F.; et al. Sarcopenic Obesity in Cervical Carcinoma: A Strong and Independent Prognostic Factor beyond the Conventional Predictors (ESTHER Study—AFRAID Project). Cancers 2024, 16, 929. https://doi.org/10.3390/cancers16050929
Medici F, Ferioli M, Cammelli S, Forlani L, Laghi V, Ma J, Cilla S, Buwenge M, Macchia G, Deodato F, et al. Sarcopenic Obesity in Cervical Carcinoma: A Strong and Independent Prognostic Factor beyond the Conventional Predictors (ESTHER Study—AFRAID Project). Cancers. 2024; 16(5):929. https://doi.org/10.3390/cancers16050929
Chicago/Turabian StyleMedici, Federica, Martina Ferioli, Silvia Cammelli, Ludovica Forlani, Viola Laghi, Johnny Ma, Savino Cilla, Milly Buwenge, Gabriella Macchia, Francesco Deodato, and et al. 2024. "Sarcopenic Obesity in Cervical Carcinoma: A Strong and Independent Prognostic Factor beyond the Conventional Predictors (ESTHER Study—AFRAID Project)" Cancers 16, no. 5: 929. https://doi.org/10.3390/cancers16050929
APA StyleMedici, F., Ferioli, M., Cammelli, S., Forlani, L., Laghi, V., Ma, J., Cilla, S., Buwenge, M., Macchia, G., Deodato, F., Vadalà, M., Malizia, C., Tagliaferri, L., Perrone, A. M., De Iaco, P., Strigari, L., Bazzocchi, A., Rizzo, S., Arcelli, A., & Morganti, A. G. (2024). Sarcopenic Obesity in Cervical Carcinoma: A Strong and Independent Prognostic Factor beyond the Conventional Predictors (ESTHER Study—AFRAID Project). Cancers, 16(5), 929. https://doi.org/10.3390/cancers16050929