
Clinical Workflow of Cone Beam Computer Tomography-Based Daily Online Adaptive Radiotherapy with Offline Magnetic Resonance Guidance: The Modular Adaptive Radiotherapy System (MARS)

 , , ,
, , , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
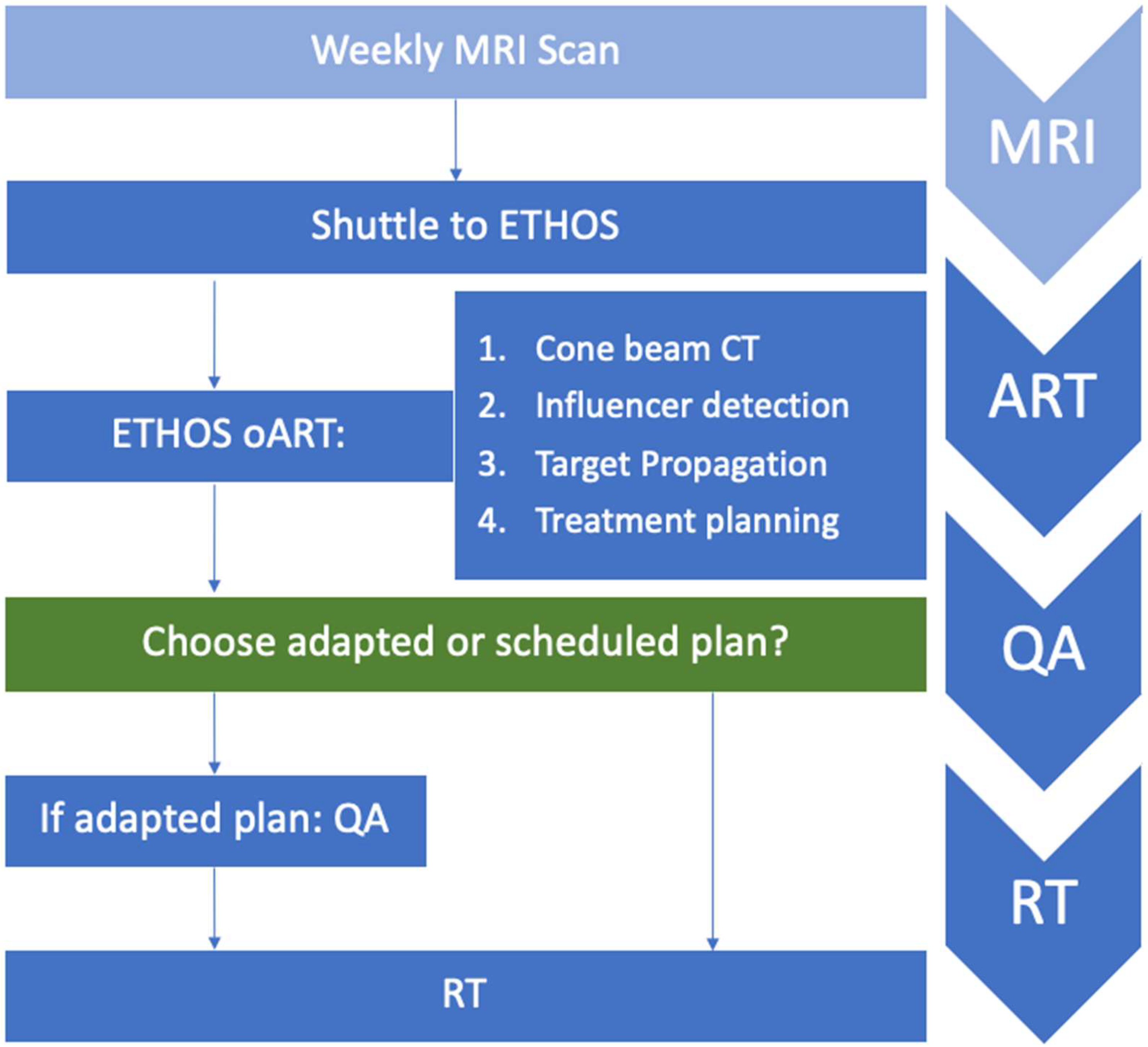
2.1. Ethos oART Workflow with Offline MR Guidance
2.1.1. Initial Treatment Planning
2.1.2. Weekly MRI for Offline MR Guidance and Integration into Ethos
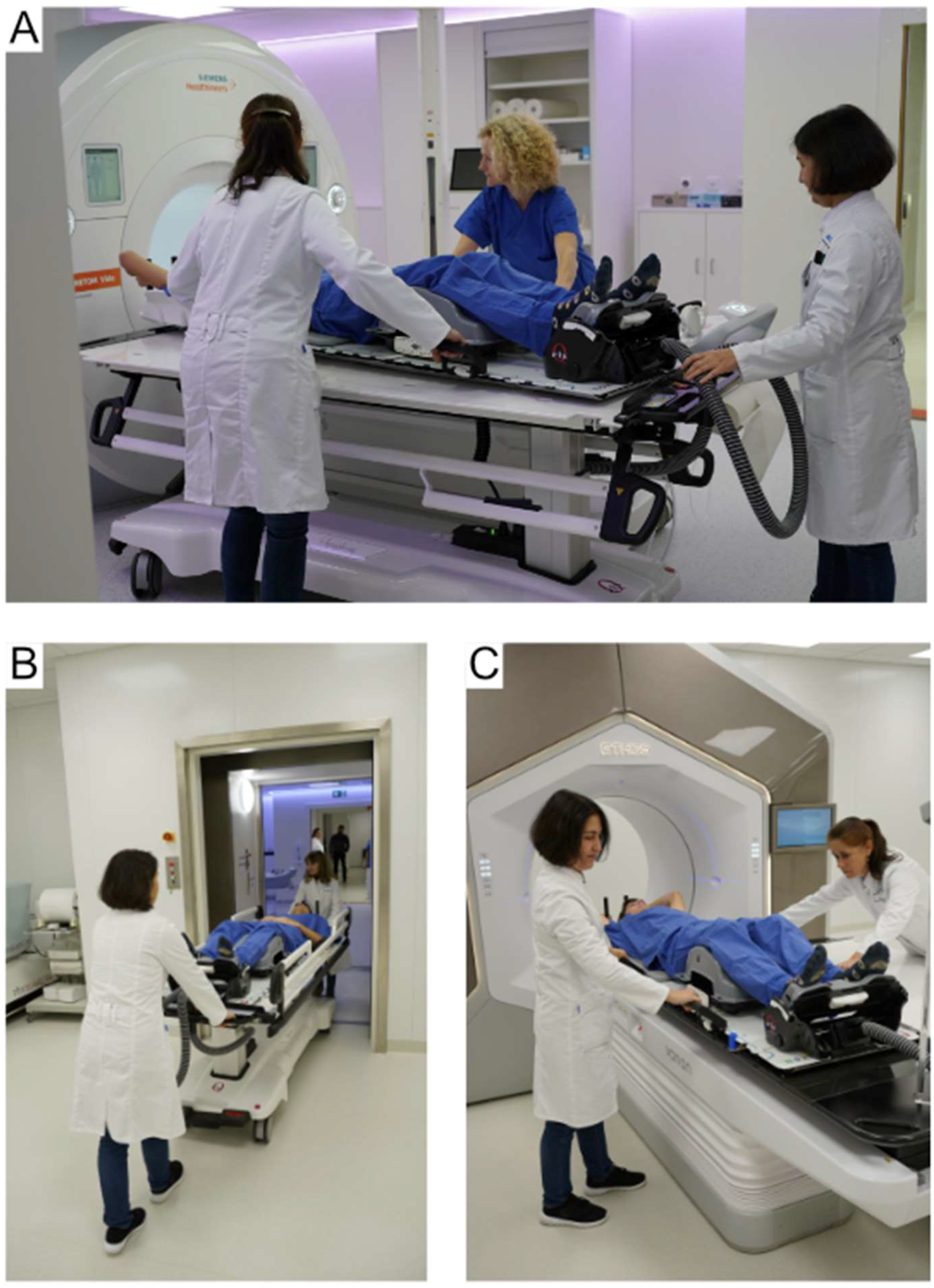
2.1.3. Shuttle-Based Transport System
2.1.4. Online ART with the Ethos System
2.1.5. Physicist QA
2.2. Data Acquisition and Analysis
2.3. Ethics Statement
3. Results
3.1. Patients
3.2. Adaptive Treatment Sessions
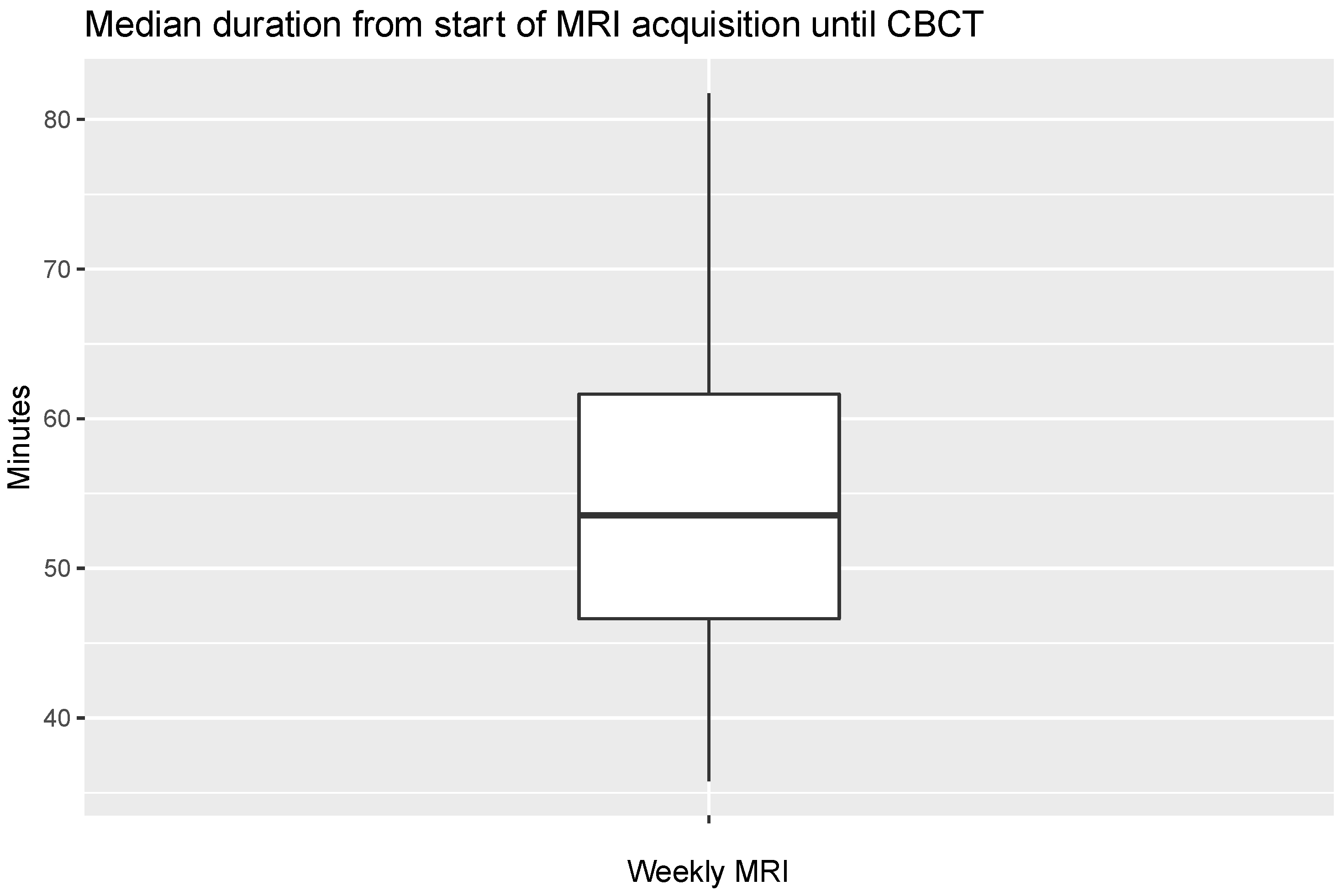
3.3. Weekly MR Imaging
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Correction Statement
References
- Yan, D.; Vicini, F.; Wong, J.; Martinez, A. Adaptive radiation therapy. Phys. Med. Biol. 1997, 42, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Sonke, J.J.; Aznar, M.; Rasch, C. Adaptive Radiotherapy for Anatomical Changes. Semin. Radiat. Oncol. 2019, 29, 245–257. [Google Scholar] [CrossRef]
- Stanley, D.N.; Harms, J.; Kole, A.J.; Dobelbower, M.C.; McCann, C.; Levine, L.; Russell, K.; McDonald, A.M. Daily Adaptive vs. Non-Adaptive External Beam Radiation Therapy with Concurrent Chemotherapy for Locally Advanced Non-Small Cell Lung Cancer (NSCLC): A Prospective Randomized Trial of an Individualized Approach for Toxicity Reduction (ARTIA-Lung). Int. J. Radiat. Oncol. Biol. Phys. 2023, 117 (Suppl. S2), e41–e42. [Google Scholar] [CrossRef]
- Ahunbay, E.E.; Peng, C.; Holmes, S.; Godley, A.; Lawton, C.; Li, X.A. Online adaptive replanning method for prostate radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2010, 77, 1561–1572. [Google Scholar] [CrossRef]
- Wang, G.; Wang, Z.; Guo, Y.; Zhang, Y.; Qiu, J.; Hu, K.; Li, J.; Yan, J.; Zhang, F. Evaluation of PTV margins with daily iterative online adaptive radiotherapy for postoperative treatment of endometrial and cervical cancer: A prospective single-arm phase 2 study. Radiat. Oncol. 2024, 19, 2. [Google Scholar] [CrossRef]
- Lu, H.; Lin, H.; Feng, G.; Chen, J.; Shu, L.; Pang, Q.; Cheng, J.; Peng, L.; Wu, D.; Liao, C.; et al. Interfractional and intrafractional errors assessed by daily cone-beam computed tomography in nasopharyngeal carcinoma treated with intensity-modulated radiation therapy: A prospective study. J. Radiat. Res. 2012, 53, 954–960. [Google Scholar] [CrossRef] [PubMed]
- Moller, D.S.; Holt, M.I.; Alber, M.; Tvilum, M.; Khalil, A.A.; Knap, M.M.; Hoffmann, L. Adaptive radiotherapy for advanced lung cancer ensures target coverage and decreases lung dose. Radiother. Oncol. 2016, 121, 32–38. [Google Scholar] [CrossRef]
- van Kranen, S.; Hamming-Vrieze, O.; Wolf, A.; Damen, E.; van Herk, M.; Sonke, J.J. Head and Neck Margin Reduction with Adaptive Radiation Therapy: Robustness of Treatment Plans against Anatomy Changes. Int. J. Radiat. Oncol. Biol. Phys. 2016, 96, 653–660. [Google Scholar] [CrossRef]
- Hehakaya, C.; Van der Voort van Zyp, J.R.; Lagendijk, J.J.W.; Grobbee, D.E.; Verkooijen, H.M.; Moors, E.H.M. Problems and Promises of Introducing the Magnetic Resonance Imaging Linear Accelerator Into Routine Care: The Case of Prostate Cancer. Front. Oncol. 2020, 10, 1741. [Google Scholar] [CrossRef]
- Hall, W.A.; Paulson, E.; Li, X.A.; Erickson, B.; Schultz, C.; Tree, A.; Awan, M.; Low, D.A.; McDonald, B.A.; Salzillo, T.; et al. Magnetic resonance linear accelerator technology and adaptive radiation therapy: An overview for clinicians. CA Cancer J. Clin. 2022, 72, 34–56. [Google Scholar] [CrossRef]
- Lim-Reinders, S.; Keller, B.M.; Al-Ward, S.; Sahgal, A.; Kim, A. Online Adaptive Radiation Therapy. Int. J. Radiat. Oncol. Biol. Phys. 2017, 99, 994–1003. [Google Scholar] [CrossRef]
- Paganetti, H.; Botas, P.; Sharp, G.C.; Winey, B. Adaptive proton therapy. Phys. Med. Biol. 2021, 66, 22TR01. [Google Scholar] [CrossRef]
- Pokharel, S.; Pacheco, A.; Tanner, S. Assessment of efficacy in automated plan generation for Varian Ethos intelligent optimization engine. J. Appl. Clin. Med. Phys. 2022, 23, e13539. [Google Scholar] [CrossRef]
- Varian. Ethos Algorithm Reference Guide; Varian: Palo Alto, CA, USA, 2019; Publication ID: P1035867-002-B. [Google Scholar]
- Stanley, D.N.; Harms, J.; Pogue, J.A.; Belliveau, J.G.; Marcrom, S.R.; McDonald, A.M.; Dobelbower, M.C.; Boggs, D.H.; Soike, M.H.; Fiveash, J.A.; et al. A roadmap for implementation of kV-CBCT online adaptive radiation therapy and initial first year experiences. J. Appl. Clin. Med. Phys. 2023, 24, e13961. [Google Scholar] [CrossRef]
- Sibolt, P.; Andersson, L.M.; Calmels, L.; Sjostrom, D.; Bjelkengren, U.; Geertsen, P.; Behrens, C.F. Clinical implementation of artificial intelligence-driven cone-beam computed tomography-guided online adaptive radiotherapy in the pelvic region. Phys. Imaging Radiat. Oncol. 2021, 17, 1–7. [Google Scholar] [CrossRef]
- Bak, M.E.; Jensen, N.K.G.; Nottrup, T.J.; Mathiesen, H.F.; Roed, H.; Sjolin, M.; Kjaer-Kristoffersen, F.; Hansen, V.N.; Vogelius, I.R. Clinical experiences with online adaptive radiotherapy of vulvar carcinoma. Acta Oncol. 2023, 62, 1230–1238. [Google Scholar] [CrossRef]
- Byrne, M.; Archibald-Heeren, B.; Hu, Y.; Teh, A.; Beserminji, R.; Cai, E.; Liu, G.; Yates, A.; Rijken, J.; Collett, N.; et al. Varian ethos online adaptive radiotherapy for prostate cancer: Early results of contouring accuracy, treatment plan quality, and treatment time. J. Appl. Clin. Med. Phys. 2022, 23, e13479. [Google Scholar] [CrossRef] [PubMed]
- Astrom, L.M.; Behrens, C.P.; Calmels, L.; Sjostrom, D.; Geertsen, P.; Mouritsen, L.S.; Serup-Hansen, E.; Lindberg, H.; Sibolt, P. Online adaptive radiotherapy of urinary bladder cancer with full re-optimization to the anatomy of the day: Initial experience and dosimetric benefits. Radiother. Oncol. 2022, 171, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Bostel, T.; Nicolay, N.H.; Grossmann, J.G.; Mohr, A.; Delorme, S.; Echner, G.; Haring, P.; Debus, J.; Sterzing, F. MR-guidance—A clinical study to evaluate a shuttle- based MR-linac connection to provide MR-guided radiotherapy. Radiat. Oncol. 2014, 9, 12. [Google Scholar] [CrossRef] [PubMed]
- Bostel, T.; Pfaffenberger, A.; Delorme, S.; Dreher, C.; Echner, G.; Haering, P.; Lang, C.; Splinter, M.; Laun, F.; Muller, M.; et al. Prospective feasibility analysis of a novel off-line approach for MR-guided radiotherapy. Strahlenther. Onkol. 2018, 194, 425–434. [Google Scholar] [CrossRef] [PubMed]
- Radford, J.; Illidge, T.; Counsell, N.; Hancock, B.; Pettengell, R.; Johnson, P.; Wimperis, J.; Culligan, D.; Popova, B.; Smith, P.; et al. Results of a trial of PET-directed therapy for early-stage Hodgkin’s lymphoma. N. Engl. J. Med. 2015, 372, 1598–1607. [Google Scholar] [CrossRef]
- Nestle, U.; Schimek-Jasch, T.; Kremp, S.; Schaefer-Schuler, A.; Mix, M.; Kusters, A.; Tosch, M.; Hehr, T.; Eschmann, S.M.; Bultel, Y.P.; et al. Imaging-based target volume reduction in chemoradiotherapy for locally advanced non-small-cell lung cancer (PET-Plan): A multicentre, open-label, randomised, controlled trial. Lancet Oncol. 2020, 21, 581–592. [Google Scholar] [CrossRef]
- Mahajan, A.; Engineer, R.; Chopra, S.; Mahanshetty, U.; Juvekar, S.L.; Shrivastava, S.K.; Desekar, N.; Thakur, M.H. Role of 3T multiparametric-MRI with BOLD hypoxia imaging for diagnosis and post therapy response evaluation of postoperative recurrent cervical cancers. Eur. J. Radiol. Open 2016, 3, 22–30. [Google Scholar] [CrossRef]
- Wang, Y.T.; Li, Y.C.; Yin, L.L.; Pu, H. Can Diffusion-weighted Magnetic Resonance Imaging Predict Survival in Patients with Cervical Cancer? A Meta-Analysis. Eur. J. Radiol. 2016, 85, 2174–2181. [Google Scholar] [CrossRef]
- van Houdt, P.J.; Yang, Y.; van der Heide, U.A. Quantitative Magnetic Resonance Imaging for Biological Image-Guided Adaptive Radiotherapy. Front. Oncol. 2020, 10, 615643. [Google Scholar] [CrossRef] [PubMed]
- Archambault, Y.; Boylan, C.; Bullock, D.; Morgas, T.; Peltola, J.; Ruokokoski, E.; Genghi, A.; Haas, B.; Suhonen, P.; Thompson, S. Making on-line adaptive radiotherapy possible using artificial intelligence and machine learning for efficient daily re-planning. Med. Phys. Int. J. 2020, 8, 77–86. [Google Scholar]
- Zhao, X.; Stanley, D.N.; Cardenas, C.E.; Harms, J.; Popple, R.A. Do we need patient-specific QA for adaptively generated plans? Retrospective evaluation of delivered online adaptive treatment plans on Varian Ethos. J. Appl. Clin. Med. Phys. 2023, 24, e13876. [Google Scholar] [CrossRef] [PubMed]
- Fink, C.A.; Wegener, D.; Sauer, L.D.; Lentz-Hommertgen, A.; Liermann, J.; Muller, A.C.; Zips, D.; Debus, J.; Herfarth, K.; Koerber, S.A. Pelvic Irradiation for Node-Positive Prostate Cancer After Prostatectomy: Long-Term Results of the Prospective PLATIN-4 and PLATIN-5 Trials. Int. J. Radiat. Oncol. Biol. Phys. 2024, 118, 1011–1017. [Google Scholar] [CrossRef]
- Zhang, S.; Nakamura, K.; Aizawa, R.; Akamatsu, S.; Mizowaki, T. Intensity-modulated radiation therapy for prostate cancer after rectal surgery: A single hospital long-term safety analysis. Int. J. Clin. Oncol. 2022, 27, 977–982. [Google Scholar] [CrossRef] [PubMed]
- Jaffray, D.A.; Carlone, M.C.; Milosevic, M.F.; Breen, S.L.; Stanescu, T.; Rink, A.; Alasti, H.; Simeonov, A.; Sweitzer, M.C.; Winter, J.D. A facility for magnetic resonance-guided radiation therapy. Semin. Radiat. Oncol. 2014, 24, 193–195. [Google Scholar] [CrossRef]
- Nyholm, T.; Nyberg, M.; Karlsson, M.G.; Karlsson, M. Systematisation of spatial uncertainties for comparison between a MR and a CT-based radiotherapy workflow for prostate treatments. Radiat. Oncol. 2009, 4, 54. [Google Scholar] [CrossRef] [PubMed]
- Regnery, S.; Katsigiannopulos, E.; Hoegen, P.; Weykamp, F.; Sandrini, E.; Held, T.; Deng, M.; Eichkorn, T.; Buchele, C.; Rippke, C.; et al. To fly or not to fly: Stereotactic MR-guided adaptive radiotherapy effectively treats ultracentral lung tumors with favorable long-term outcomes. Lung Cancer 2023, 179, 107175. [Google Scholar] [CrossRef] [PubMed]
- Weykamp, F.; Hoegen, P.; Regnery, S.; Katsigiannopulos, E.; Renkamp, C.K.; Lang, K.; Konig, L.; Sandrini, E.; Meixner, E.; Rippke, C.; et al. Long-Term Clinical Results of MR-Guided Stereotactic Body Radiotherapy of Liver Metastases. Cancers 2023, 15, 2786. [Google Scholar] [CrossRef] [PubMed]
- Riaz, N.; Sherman, E.; Pei, X.; Schoder, H.; Grkovski, M.; Paudyal, R.; Katabi, N.; Selenica, P.; Yamaguchi, T.N.; Ma, D.; et al. Precision Radiotherapy: Reduction in Radiation for Oropharyngeal Cancer in the 30 ROC Trial. J. Natl. Cancer Inst. 2021, 113, 742–751. [Google Scholar] [CrossRef]
- Ng, S.P.; Cardenas, C.E.; Bahig, H.; Elgohari, B.; Wang, J.; Johnson, J.M.; Moreno, A.C.; Shah, S.J.; Garden, A.S.; Phan, J.; et al. Changes in Apparent Diffusion Coefficient (ADC) in Serial Weekly MRI during Radiotherapy in Patients with Head and Neck Cancer: Results from the PREDICT-HN Study. Curr. Oncol. 2022, 29, 6303–6313. [Google Scholar] [CrossRef]
- Kooreman, E.S.; van Pelt, V.; Nowee, M.E.; Pos, F.; van der Heide, U.A.; van Houdt, P.J. Longitudinal Correlations Between Intravoxel Incoherent Motion (IVIM) and Dynamic Contrast-Enhanced (DCE) MRI During Radiotherapy in Prostate Cancer Patients. Front. Oncol. 2022, 12, 897130. [Google Scholar] [CrossRef]
- Sonke, J.J.; Belderbos, J. Adaptive radiotherapy for lung cancer. Semin. Radiat. Oncol. 2010, 20, 94–106. [Google Scholar] [CrossRef]
- Weykamp, F.; Meixner, E.; Arians, N.; Hoegen-Sassmannshausen, P.; Kim, J.Y.; Tawk, B.; Knoll, M.; Huber, P.; Konig, L.; Sander, A.; et al. Daily AI-Based Treatment Adaptation under Weekly Offline MR Guidance in Chemoradiotherapy for Cervical Cancer 1: The AIM-C1 Trial. J. Clin. Med. 2024, 13, 957. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Median (IQR) | |
|---|---|
| Age (years) | 70 (65–75) |
| Karnofsky performance score (%) | 90 (80–90) |
| Number of patients (n = 31) | |
| Sex | |
| Male | 18 |
| Female | 13 |
| Primary Tumor Site: | |
| Prostate | 16 |
| Lung | 7 |
| Cervix | 5 |
| Endometrium | 2 |
| Bladder | 1 |
| Treatment Site: | |
| Thorax | 7 |
| Abdomen | 3 |
| Pelvis | 21 |
| Previous RT (80% isodose) overlapping with target volume: | |
| No | 27 |
| Yes | 4 |
| Systemic Therapy: | |
| None | 12 |
| ADT | 9 |
| Preceding, sequential chemotherapy | 6 |
| Concurrent chemotherapy | 5 |
| Primary Tumor | Dose Concept | n = 31 | Total Fx | Target |
|---|---|---|---|---|
| Prostate | 20 × 3.0 Gy | 13 | 260 | Prostate, definitive |
| 34 × 2.25 Gy | 1 | 34 | Prostate, after rectal surgery | |
| 26 × 1.8 Gy ENI; 26 × 2.2Gy SIB | 2 | 52 | ENI + SIB | |
| Lung | 30–33 × 2.0 Gy | 5 | 181 | Lung, definitive |
| 25 × 1.8 Gy | 2 | 50 | Lung, local recurrence | |
| Cervix | 25–28 × 1.8 Gy + BT | 5 | 103 | Cervix, definitive |
| Endometrium | 25 × 1.8 Gy + BT | 1 | 25 | Pelvis, postoperative |
| 12 × 4 Gy | 1 | 12 | Adrenal metastasis | |
| Bladder | 20 × 2.75 Gy | 1 | 20 | Bladder |
| Study | Patients | Fractions | Entities | Ethos Total Treatment Time |
|---|---|---|---|---|
| Current study | 31 | 720 | Mult. | Median 30.7 min (IQR 24.7–39.2) † |
| Byrne et al. [18] | 6 | 184 | PC | Avg. 34.2 min (±SD 6.6) ‡ |
| Stanley et al. [15] | 97 | 1667 | Mult. | Avg. 34.5 min (±SD 11.4) ‡ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.-Y.; Tawk, B.; Knoll, M.; Hoegen-Saßmannshausen, P.; Liermann, J.; Huber, P.E.; Lifferth, M.; Lang, C.; Häring, P.; Gnirs, R.; et al. Clinical Workflow of Cone Beam Computer Tomography-Based Daily Online Adaptive Radiotherapy with Offline Magnetic Resonance Guidance: The Modular Adaptive Radiotherapy System (MARS). Cancers 2024, 16, 1210. https://doi.org/10.3390/cancers16061210
Kim J-Y, Tawk B, Knoll M, Hoegen-Saßmannshausen P, Liermann J, Huber PE, Lifferth M, Lang C, Häring P, Gnirs R, et al. Clinical Workflow of Cone Beam Computer Tomography-Based Daily Online Adaptive Radiotherapy with Offline Magnetic Resonance Guidance: The Modular Adaptive Radiotherapy System (MARS). Cancers. 2024; 16(6):1210. https://doi.org/10.3390/cancers16061210
Chicago/Turabian StyleKim, Ji-Young, Bouchra Tawk, Maximilian Knoll, Philipp Hoegen-Saßmannshausen, Jakob Liermann, Peter E. Huber, Mona Lifferth, Clemens Lang, Peter Häring, Regula Gnirs, and et al. 2024. "Clinical Workflow of Cone Beam Computer Tomography-Based Daily Online Adaptive Radiotherapy with Offline Magnetic Resonance Guidance: The Modular Adaptive Radiotherapy System (MARS)" Cancers 16, no. 6: 1210. https://doi.org/10.3390/cancers16061210
APA StyleKim, J.-Y., Tawk, B., Knoll, M., Hoegen-Saßmannshausen, P., Liermann, J., Huber, P. E., Lifferth, M., Lang, C., Häring, P., Gnirs, R., Jäkel, O., Schlemmer, H.-P., Debus, J., Hörner-Rieber, J., & Weykamp, F. (2024). Clinical Workflow of Cone Beam Computer Tomography-Based Daily Online Adaptive Radiotherapy with Offline Magnetic Resonance Guidance: The Modular Adaptive Radiotherapy System (MARS). Cancers, 16(6), 1210. https://doi.org/10.3390/cancers16061210