
Comparing R-Bendamustine vs. R-CHOP Plus Maintenance Therapy as First-Line Systemic Treatment in Follicular Lymphoma: A Multicenter Retrospective GELTAMO Study

 , , , , , , and add
Show full author list
, , , , , , and add
Show full author list
Abstract
Simple Summary
Abstract
1. Introduction
2. Material and Methods
2.1. Patients
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bastos-Oreiro, M.; Muntañola, A.; Panizo, C.; Gonzalez-Barca, E.; de Villambrosia, S.G.; Córdoba, R.; López, J.L.B.; González-Sierra, P.; Terol, M.J.; Gutierre, A.; et al. RELINF: Prospective epidemiological registry of lymphoid neoplasms in Spain. A project from the GELTAMO group. Ann. Hematol. 2020, 99, 799–808. [Google Scholar] [CrossRef]
- Swerdlow, S.H.; Campo, E.; Pileri, S.A.; Harris, N.L.; Stein, H.; Siebert, R.; Advani, R.; Ghielmini, M.; Salles, G.A.; Zelenetz, A.D.; et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood 2016, 127, 2375–2390. [Google Scholar] [CrossRef]
- Alaggio, R.; Amador, C.; Anagnostopoulos, I.; Attygalle, A.D.; de Oliveira Araujo, I.B.; Berti, E.; Bhagat, G.; Borges, A.M.; Boyer, D.; Calaminici, M.; et al. The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Lymphoid Neoplasms. Leukemia 2022, 36, 1720–1748. [Google Scholar] [CrossRef]
- Sarkozy, C.; Maurer, M.J.; Link, B.K.; Ghesquieres, H.; Nicolas, E.; Thompson, C.A.; Traverse-Glehen, A.; Feldman, A.L.; Allmer, C.; Slager, S.L.; et al. Cause of Death in Follicular Lymphoma in the First Decade of the Rituximab Era: A Pooled Analysis of French and US Cohorts. J. Clin. Oncol. 2019, 37, 144–152. [Google Scholar] [CrossRef]
- Casulo, C.; Byrtek, M.; Dawson, K.L.; Ghesquieres, H.; Nicolas, E.; Thompson, C.A.; Traverse-Glehen, A.; Feldman, A.L.; Allmer, C.; Slager, S.L.; et al. Early Relapse of Follicular Lymphoma After Rituximab Plus Cyclophosphamide, Doxorubicin, Vincristine, and Prednisone Defines Patients at High Risk for Death: An Analysis From the National LymphoCare Study. J. Clin. Oncol. 2015, 33, 2516–2522. [Google Scholar] [CrossRef]
- Montoto, S.; Davies, A.J.; Matthews, J.; Calaminici, M.; Norton, A.J.; Amess, J.; Vinnicombe, S.; Waters, R.; Rohatiner, A.Z.S.; Lister, T.A. Risk and clinical implications of transformation of follicular lymphoma to diffuse large B-cell lymphoma. J. Clin. Oncol. 2007, 25, 2426–2433. [Google Scholar] [CrossRef]
- Solal-Céligny, P.; Roy, P.; Colombat, P.; White, J.; Armitage, J.O.; Arranz-Saez, R.; Au, W.Y.; Bellei, M.; Brice, P.; Caballero, D.; et al. Follicular Lymphoma International Prognostic Index. Blood 2004, 104, 1258–1265. [Google Scholar] [CrossRef]
- Pastore, A.; Jurinovic, V.; Kridel, R.; White, J.; Armitage, J.O.; Arranz-Saez, R.; Au, W.Y.; Bellei, M.; Brice, P.; Caballero, D.; et al. Integration of gene mutations in risk prognostication for patients receiving first-line immunochemotherapy for follicular lymphoma: A retrospective analysis of a prospective clinical trial and validation in a population-based registry. Lancet Oncol. 2015, 16, 1111–1122. [Google Scholar] [CrossRef]
- Dreyling, M.; Ghielmini, M.; Rule, S.; Salles, G.; Vitolo, U.; Ladetto, M.; ESMO Guidelines Committee. Newly diagnosed and relapsed follicular lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2016, 27, v83–v90. [Google Scholar] [CrossRef]
- Brice, P.; Bastion, Y.; Lepage, E.; Brousse, N.; Haïoun, C.; Moreau, P.; Straetmans, N.; Tilly, H.; Tabah, I.; Solal-Céligny, P. Comparison in low-tumor-burden follicular lymphomas between an initial no-treatment policy, prednimustine, or interferon alfa: A randomized study from the Groupe d’Etude des Lymphomes Folliculaires. Groupe d’Etude des Lymphomes de l’Adulte. J. Clin. Oncol. 1997, 15, 1110–1117. [Google Scholar] [CrossRef]
- Hiddemann, W.; Kneba, M.; Dreyling, M.; Schmitz, N.; Lengfelder, E.; Schmits, R.; Reiser, M.; Metzner, B.; Harder, H.; Hegewisch-Becker, S.; et al. Frontline therapy with rituximab added to the combination of cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP) significantly improves the outcome for patients with advanced-stage follicular lymphoma compared with therapy with CHOP alone: Results of a prospective randomized study of the German Low-Grade Lymphoma Study Group. Blood 2005, 106, 3725–3732. [Google Scholar]
- Flinn, I.W.; van der Jagt, R.; Kahl, B.; Wood, P.; Hawkins, T.; MacDonald, D.; Simpson, D.; Kolibaba, K.; Issa, S.; Chang, J.; et al. First-Line Treatment of Patients With Indolent Non-Hodgkin Lymphoma or Mantle-Cell Lymphoma With Bendamustine Plus Rituximab Versus R-CHOP or R-CVP: Results of the BRIGHT 5-Year Follow-Up Study. J. Clin. Oncol. 2019, 37, 984–991. [Google Scholar] [CrossRef]
- Marcus, R.; Imrie, K.; Belch, A.; Cunningham, D.; Flores, E.; Catalano, J.; Solal-Celigny, P.; Offner, F.; Walewski, J.; Raposo, J.; et al. CVP chemotherapy plus rituximab compared with CVP as first-line treatment for advanced follicular lymphoma. Blood 2005, 105, 1417–1423. [Google Scholar] [CrossRef]
- Rummel, M.J.; Niederle, N.; Maschmeyer, G.; Banat, G.A.; von Grünhagen, U.; Losem, C.; Kofahl-Krause, D.; Heil, G.; Welslau, M.; Balser, C.; et al. Bendamustine plus rituximab versus CHOP plus rituximab as first-line treatment for patients with indolent and mantle-cell lymphomas: An open-label, multicentre, randomised, phase 3 non-inferiority trial. Lancet 2013, 381, 1203–1210. [Google Scholar] [CrossRef]
- Marcus, R.; Davies, A.; Ando, K.; Klapper, W.; Opat, S.; Owen, C.; Phillips, E.; Sangha, R.; Schlag, R.; Seymou, J.F.; et al. Obinutuzumab for the First-Line Treatment of Follicular Lymphoma. N. Engl. J. Med. 2017, 377, 1331–1344. [Google Scholar] [CrossRef]
- Salles, G.; Seymour, J.F.; Offner, F.; López-Guillermo, A.; Belada, D.; Xerri, L.; Feugier, P.; Bouabdallah, R.; Catalano, J.V.; Brice, P.; et al. Rituximab maintenance for 2 years in patients with high tumour burden follicular lymphoma responding to rituximab plus chemotherapy (PRIMA): A phase 3, randomised controlled trial. Lancet 2011, 377, 42–51. [Google Scholar] [CrossRef]
- Bachy, E.; Seymour, J.F.; Feugier, P.; Offner, F.; López-Guillermo, A.; Belada, D.; Xerri, L.; Catalano, J.V.; Brice, P.; Lemonnier, F.; et al. Sustained Progression-Free Survival Benefit of Rituximab Maintenance in Patients With Follicular Lymphoma: Long-Term Results of the PRIMA Study. J. Clin. Oncol. 2019, 37, 2815–2824. [Google Scholar] [CrossRef]
- Hiddemann, W.; Barbui, A.M.; Canales, M.A.; Cannell, P.K.; Collins, G.P.; Dürig, J.; Forstpointner, R.; Herold, M.; Hertzberg, M.; Klanova, M.; et al. Immunochemotherapy With Obinutuzumab or Rituximab for Previously Untreated Follicular Lymphoma in the GALLIUM Study: Influence of Chemotherapy on Efficacy and Safety. J. Clin. Oncol. 2018, 36, 2395–2404. [Google Scholar] [CrossRef]
- Rummel, M.J.; Maschmeyer, G.; Ganser, A.; Heider, A.; von Gruenhagen, U.; Losem, C.; Heil, G.; Welslau, M.; Balser, C.; Kaiser, U.; et al. Bendamustine plus rituximab (B-R) versus CHOP plus rituximab (CHOP-R) as first-line treatment in patients with indolent lymphomas: Nine-year updated results from the StiL NHL1 study. J. Clin. Oncol. 2017, 35 (Suppl. 15), 7501. [Google Scholar] [CrossRef]
- Wang, Y.; Zhou, S.; Qi, X.; Yang, F.; Maurer, M.J.; Habermann, T.M.; Witzig, T.E.; Wang, M.L.; Nowakowski, G.S. Efficacy of front-line immunochemotherapy for follicular lymphoma: A network meta-analysis of randomized controlled trials. Blood Cancer J. 2022, 12, 1. [Google Scholar] [CrossRef]
- Hill, B.T.; Nastoupil, L.; Winter, A.M.; Becnel, M.R.; Cerhan, J.R.; Habermann, T.M.; Link, B.K.; Maurer, M.J.; Fakhri, B.; Reddy, P.; et al. Maintenance rituximab or observation after frontline treatment with bendamustine-rituximab for follicular lymphoma. Br. J. Haematol. 2019, 184, 524–535. [Google Scholar] [CrossRef]
- Pettitt, A.R.; Barrington, S.; Kalakonda, N.; Khan, U.T.; Jackson, R.; Carruthers, S.; Oates, M.; Lin, K.; Ardeshna, K.; Eyre, T.; et al. Ncri Petrea Trial: A Phase 3 Evaluation of Pet-Guided, Response-Adapted Therapy in Patients with Previously Untreated, Advanced-Stage, High-Tumour-Burden Follicular Lymphoma. Hematol. Oncol. 2019, 37 (Suppl. 2), 67–68. [Google Scholar] [CrossRef]
- Mondello, P.; Steiner, N.; Willenbacher, W.; Cerchione, C.; Nappi, D.; Mauro, E.; Ferrero, S.; Cuzzocrea, S.; Mian, M. Bendamustine plus Rituximab Versus R-CHOP as First-Line Treatment for Patients with Follicular Lymphoma Grade 3A: Evidence from a Multicenter, Retrospective Study. Oncologist 2018, 23, 454–460. [Google Scholar] [CrossRef]
- Pouyiourou, M.; Meyer, A.; Stroux, A.; Viardot, A.; La Rosée, P.; Maschmeyer, G.; Kämpfe, D.; Kahl, C.; Vucinic, V.; Monecke, A.; et al. First-line treatment with R-CHOP or rituximab-bendamustine in patients with follicular lymphoma grade 3A-results of a retrospective analysis. Ann. Hematol. 2020, 99, 2821–2829. [Google Scholar] [CrossRef]
- Margiotta-Casaluci, G.; Bigliardi, S.; Cocito, F.; Meli, E.; Petrucci, L.; Nicolosi, M.; Annibali, O.; Boccomini, C.; Bozzoli, V.; Castellino, A.; et al. Comparison of first-line treatment with bendamustine plus rituximab versus R-CHOP for patients with follicular lymphoma grade 3A: Results of a retrospective study from the Fondazione Italiana Linfomi. Front. Oncol. 2023, 13, 1120967. [Google Scholar] [CrossRef]
- Ma, S. Risk Factors of Follicular Lymphoma. Expert Opin. Med. Diagn. 2012, 6, 323–333. [Google Scholar] [CrossRef]
- Alig, S.; Jurinovic, V.; Pastore, A.; Haebe, S.; Schmidt, C.; Zoellner, A.K.; Dreyling, M.; Unterhalt, M.; Hoster, E.; Hiddemann, W.; et al. Impact of age on clinical risk scores in follicular lymphoma. Blood Adv. 2019, 3, 1033–1038. [Google Scholar] [CrossRef]
- Iacoboni, G.; Martin Lopez, A.A.; Jalowiec, K.A.; Rejeski, K.; Kwon, M.; Jalowiec, K.A.; Amat, P.; Reguera-Ortega, J.L.; Gallur, L.; Blumenberg, V.; et al. Recent Bendamustine Treatment before Apheresis Has a Negative Impact on Outcomes in Patients with Large B-Cell Lymphoma Receiving Chimeric Antigen Receptor T-Cell Therapy. Blood 2022, 140 (Suppl. 1), 1592–1594. [Google Scholar] [CrossRef]
- Wang, M.; Munoz, J.; Goy, A.; Wang, M.; Munoz, J.; Goy, A.; Locke, F.L.; Jacobson, C.A.; Hill, B.T.; Timmerman, J.M.; et al. Three-Year Follow-Up of KTE-X19 in Patients With Relapsed/Refractory Mantle Cell Lymphoma, Including High-Risk Subgroups, in the ZUMA-2 Study. J. Clin. Oncol. 2022, 41, 555. [Google Scholar] [CrossRef]
- Leszek, P.; Klotzka, A.; Bartuś, S.; Leszek, P.; Klotzka, A.; Bartuś, S.; Burchardt, P.; Czarnecka, A.M.; Długosz-Danecka, M.; Gierlotka, M.; et al. A practical approach to the 2022 ESC cardio-oncology guidelines: Comments by a team of experts-cardiologists and oncologists. Pol. Heart J. 2023, 81, 1047–1063. [Google Scholar] [CrossRef]
- Lyon, A.R.; López-Fernández, T.; Couch, L.S.; Asteggiano, R.; Aznar, M.C.; Bergler-Klein, J.; Boriani, G.; Cardinale, D.; Cordoba, R.; Cosyns, B. 2022 ESC Guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur. Heart J. 2022, 43, 4229–4361. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Global Group (N = 405) | R-CHOP (N = 245) | R-BENDA (N = 160) | p | |
|---|---|---|---|---|
| Median months from biopsy to initial treatment median (range) | 0.90 (0–144) | 0.73 (0–144) | 1.30 (0–66) | <0.001 |
| Median age at first line (range) | 59 (21–100) | 57 (21–83) | 62 (30–100) | 0.003 |
| Sex Male Female Missing | 201 (50%) 202 (50%) 2 | 125 (51%) 119 (49%) | 76 (48%) 83 (52%) | 0.54 |
| Age (years) ≤60 >60 Missing | 208 (52%) 188 (47%) 9 | 138 (56%) 107 (44%) | 70 (46%) 81 (54%) | 0.062 |
| Ann Arbor stage I-II bulky III-IV Missing | 31 (8%) 361 (92%) 13 | 20 (8%) 219 (92%) | 11 (7%) 142 (93%) | 0.71 |
| B symptoms present No Yes Missing | 242 (64%) 136 (35%) 27 | 154 (65%) 81 (34%) | 88 (61%) 55 (38%) | 0.44 |
| ECOG performance status 0–1 2–4 Missing | 307 (93%) 23 (7%) 75 | 186 (92%) 16 (8%) | 121 (94%) 7 (5%) | 0.51 |
| Bone marrow involvement No Yes Missing | 198 (50%) 195 (50%) 12 | 128 (53%) 115 (47%) | 70 (47%) 80 (53%) | 0.25 |
| FLIPI score 0–1 2 3–5 Missing | 66 (17) 145 (38) 171 (45) 23 | 39 (17%) 78 (33%) 118 (50%) | 27 (18%) 67 (46%) 53 (36%) | 0.020 |
| Histological grade 1 2 3a Missing | 145 (39) 151 (41) 75 (20) 34 | 82 (36%) 85 (37%) 60 (26%) | 63 (44%) 66 (46%) 15 (10%) | <0.001 |
| Induction regimen R-CHOP R-Bendamustine | 245 (60) 160 (40) | --- | --- | --- |
| Rituximab maintenance: Yes No | 392 (97%) 13 (3%) | 237 (97%) 8 (3%) | 155 (97%) 5 (3%) | 1 |
|
Global Group (N = 405) |
R-CHOP (N = 245) |
R-BENDA (N = 160) | p | |
|---|---|---|---|---|
| Median follow-up (95%CI) | 81 (77–86) | 96 (88–103) | 68 (60–75) | |
Response:
| 316 (78%) 77 (19%) 6 (1.5%) 6 (1.5%) | 180 (73%) 56 (23%) 3 (1%) 6 (2%) | 136 (85%) 21 (13%) 3 (2%) 0 (0%) | 0.014 |
Relapse/progression:
| 77 (19%) 30 (7%) 298 (74%) | 62 (25%) 20 (8%) 164 (67%) | 16 (10%) 10 (6%) 134 (84%) | <0.001 |
Transformation:
| 19 (5%) 364 (95%) | 14 (6%) 216 (94%) | 5 (3%) 148 (97%) | 0.24 |
| POD24: | 39 (10%) | 25 (10%) | 14 (9%) | 0.73 |
| Death: | 50 (12%) | 34 (14%) | 16 (10%) | 0.28 |
Causes of death:
| 19 (5%) 13 (3%) 7 (2%) 11 (3%) | 15 (6%) 6 (2%) 5 (2%) 8 (3%) | 4 (2%) 7 (4%) 2 (1%) 3 (2%) | 0.28 |
|
Global Group (N = 405) |
R-CHOP (N = 245) |
R-BENDA (N = 160) | p | |
|---|---|---|---|---|
| Pneumocystis carinii prophylaxis (induction): | 184 (48%) | 125 (55%) | 59 (39%) | 0.003 |
| Herpes prophylaxis (induction): | 124 (32%) | 64 (28%) | 60 (39%) | 0.02 |
G-CSF during induction:
| 158 (42%) 114 (30%) 107 (28%) | 69 (30%) 97 (42%) 65 (28%) | 89 (60%) 17 (11%) 42 (28%) | <0.001 |
| Median number of cycles (range) | 6 (2–8) | 6 (3–8) | 6 (2–8) | <0.001 |
| 1st line discontinuation: | 13 (3%) | 4 (2%) | 9 (6%) | 0.04 |
Neutropenia:
| 167 (43%) 66 (17%) 157 (40%) | 82 (35%) 51 (22%) 102 (43%) | 85 (55%) 15 (10%) 55 (35%) | <0.001 |
Anemia:
| 255 (65%) 126 (32%) 14 (3%) | 125 (52%) 104 (43%) 12 (5%) | 130 (84%) 22 (14%) 2 (1%) | <0.001 |
Thrombocytopenia:
| 327 (82%) 68 (16%) 2 (1%) | 196 (81%) 45 (19%) 1 (0.4%) | 131 (84%) 23 (15%) 1 (1%) | 0.46 |
Liver toxicity:
| 377 (95%) 13 (3%) 1 (1%) | 226 (94%) 11 (5%) 4 (2%) | 151 (98%) 2 (1%) 1 (1%) | 0.14 |
Renal toxicity:
| 388 (98%) 5 (1%) 3 (1%) | 238 (99%) 2 (1%) 1 (0.5%) | 150 (97%) 3 (2%) 2 (1%) | 0.39 |
| Infections: | 93 (24%) | 61 (25%) | 32 (21%) | 0.33 |
Infections during induction:
| 94 (24%) 299 (76%) 55 (14%) 39 (10%) | 61 (25%) 179 (75%) 35 (15%) 26 (11%) | 33 (22%) 120 (78%) 20 (13%) 13 (8%) | 0.4 0.65 |
Infections during maintenance:
| 64 (19%) 277 (81%) 49 (14%) 15 (4%) | 27 (13%) 177 (87%) 20 (10%) 7 (3%)) | 37 (27%) 100 (73%) 29 (21%) 8 (6%) | <0.001 0.006 |
| Dermatologic toxicity: | 35 (9%) | 20 (9%) | 15 (10%) | 0.72 |
| Hospitalization: | 70 (18%) | 48 (20%) | 22 (14%) | 0.18 |
|
Global Group (N = 405) |
R-CHOP (N = 245) |
R-BENDA (N = 160) | p | |
|---|---|---|---|---|
| Pneumocystis carinii prophylaxis (maintenance): | 165 (45%) | 109 (49%) | 57 (40%) | 0.13 |
| Herpes prophylaxis (maintenance): | 113 (31%) | 55 (25%) | 58 (39%) | 0.004 |
G-CSF during maintenance:
| 312 (87%) 9 (2%) 39 (11%) | 200 (91%) 6 (3%) 13 (6%) | 112 (79%) 3 (2%) 26 (18%) | <0.001 |
| Rituximab maintenance: | 392 (97%) | 237 (97%) | 155 (97%) | 1 |
| Maintenance discontinuation: | 75 (19%) | 29 (12%) | 46 (30%) | <0.001 |
Causes of discontinuation:
| 17 (22%) 31 (41%) 28 (27%) | 7 (24%) 4 (14%) 18 (62%) | 10 (21%) 27 (57%) 10 (21%) | <0.001 |
Neutropenia:
| 286 (77%) 42 (11%) 44 (12%) | 190 (84%) 20 (9%) 15 (7%) | 96 (65%) 22 (15%) 29 (20%) | <0.001 |
Anemia:
| 324 (88%) 42 (11%) 3 (1%) | 196 (88%) 26 (12%) 1 (0.4%) | 128 (88%) 16 (11%) 2 (1%) | 0.62 |
Thrombocytopenia:
| 331 (89%) 31 (8%) 9 (2%) | 199 (88%) 21 (9%) 6 (3%) | 132 (91%) 10 (7%) 3 (2%) | 0.66 |
| Infections: | 68 (18%) | 27 (12%) | 41 (28%) | <0.001 |
| Severe infections | ||||
| Hospitalization: | 25 (7%) | 13 (6%) | 12 (8%) | 0.4 |
Second malignancies:
| 29 (7%) 257 (63%) 119 (29%) | 16 (6%) 156 (64%) 73 (30%) | 13 (8%) 101 (63%) 46 (29%) | 0.82 |
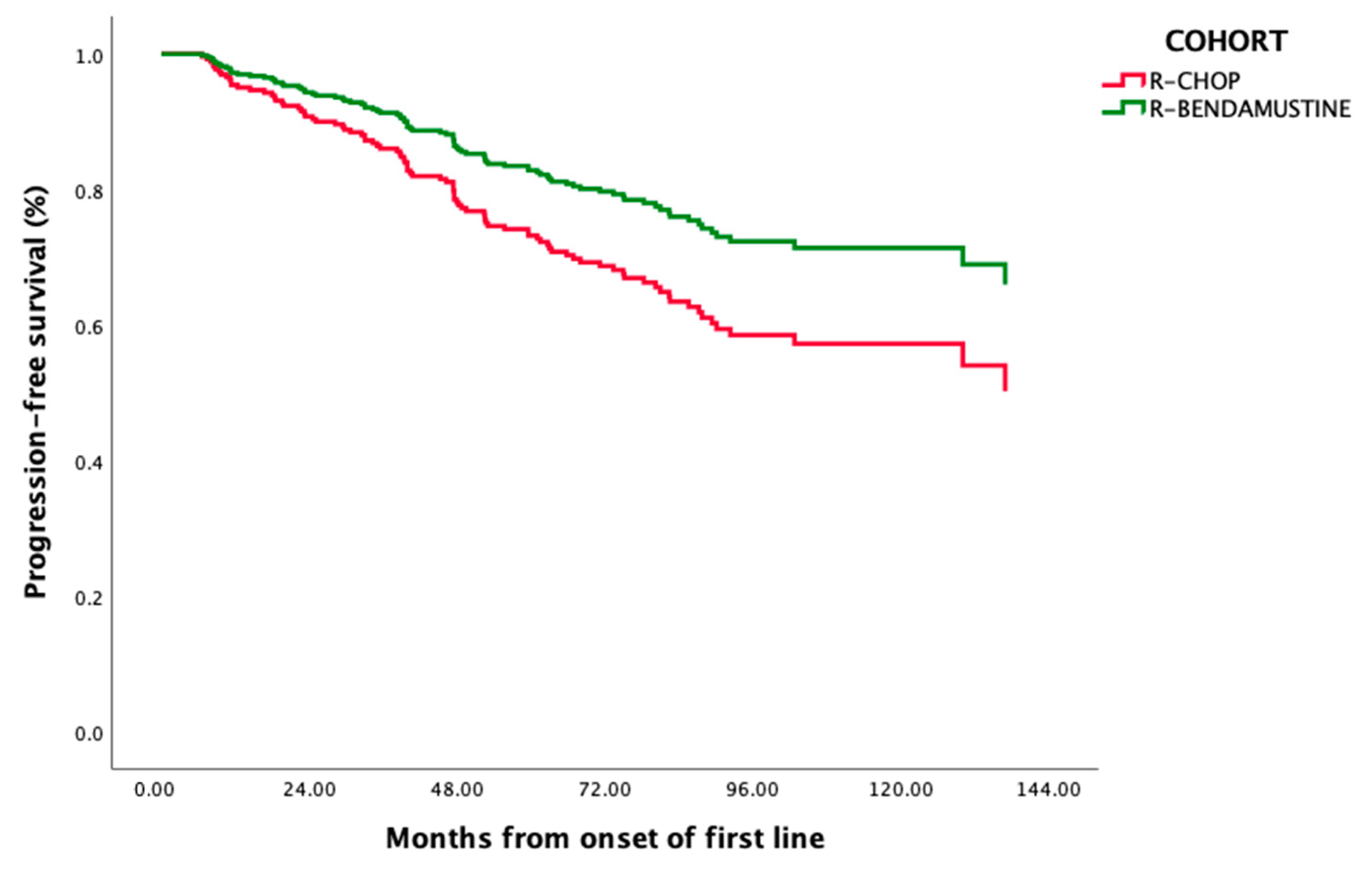
| PFS | HR (95%CI) | p |
|---|---|---|
| R-CHOP | 1.65 (1.01–2.71) | 0.045 |
| FLIPI 3–5 | 6.58 (1.13–2.62) | 0.01 |
| OS | ||
| Age > 60 | 6.52 (2.7–15.74) | <0.001 |
| ECOG > 1 | 4.39 (1.97–9.79) | <0.001 |
| Male gender | 1.51 (1.07–2.13) | 0.018 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bastos-Oreiro, M.; Gutierrez, A.; Cabero, A.; López, J.; Villafuerte, P.; Jiménez-Ubieto, A.; de Oña, R.; De la Fuente, A.; Navarro, B.; Peñalver, J.; et al. Comparing R-Bendamustine vs. R-CHOP Plus Maintenance Therapy as First-Line Systemic Treatment in Follicular Lymphoma: A Multicenter Retrospective GELTAMO Study. Cancers 2024, 16, 1285. https://doi.org/10.3390/cancers16071285
Bastos-Oreiro M, Gutierrez A, Cabero A, López J, Villafuerte P, Jiménez-Ubieto A, de Oña R, De la Fuente A, Navarro B, Peñalver J, et al. Comparing R-Bendamustine vs. R-CHOP Plus Maintenance Therapy as First-Line Systemic Treatment in Follicular Lymphoma: A Multicenter Retrospective GELTAMO Study. Cancers. 2024; 16(7):1285. https://doi.org/10.3390/cancers16071285
Chicago/Turabian StyleBastos-Oreiro, Mariana, Antonio Gutierrez, Almudena Cabero, Javier López, Paola Villafuerte, Ana Jiménez-Ubieto, Raquel de Oña, Adolfo De la Fuente, Belén Navarro, Javier Peñalver, and et al. 2024. "Comparing R-Bendamustine vs. R-CHOP Plus Maintenance Therapy as First-Line Systemic Treatment in Follicular Lymphoma: A Multicenter Retrospective GELTAMO Study" Cancers 16, no. 7: 1285. https://doi.org/10.3390/cancers16071285
APA StyleBastos-Oreiro, M., Gutierrez, A., Cabero, A., López, J., Villafuerte, P., Jiménez-Ubieto, A., de Oña, R., De la Fuente, A., Navarro, B., Peñalver, J., Martínez, P., Alonso, C., Infante, M., Córdoba, R., Perez-Montero, B., Pérez de Oteyza, J., González de Villambrosio, S., Fernández-Caldas, P., del Campo, R., ... Sancho, J.-M. (2024). Comparing R-Bendamustine vs. R-CHOP Plus Maintenance Therapy as First-Line Systemic Treatment in Follicular Lymphoma: A Multicenter Retrospective GELTAMO Study. Cancers, 16(7), 1285. https://doi.org/10.3390/cancers16071285