Simple Summary
Biomarker-guided therapies offer the possibility for targeted cancer therapies. For gastric cancer, HER2 plays a pivotal role. To date, with trastuzumab and trastuzumab-deruxtecan, two HER2-targeting options exist for the treatment of metastatic HER2-positive gastric cancer. However, these therapies rarely lead to long-lasting results as resistance mechanisms and heterogeneity limit their success. This review gives an overview of the current standard-of-care treatment of HER2-positive gastric cancer and new developments in the field.
Abstract
Despite a decreasing incidence in Western countries, gastric cancer is among the most common cancer subtypes globally and is associated with one of the highest tumor-related mortality rates. Biomarkers play an increasing role in the treatment against gastric cancer. HER2 was one of the first biomarkers that found its way into clinical practice. Since the ToGA trial, trastuzumab has been part of first-line palliative chemotherapy in metastatic or unresectable gastric cancer. HER2-targeting agents, such as the tyrosine kinase inhibitor lapatinib, the antibody drug conjugate (ADC) trastuzumab-emtansine or dual HER2 inhibition (pertuzumab and trastuzumab), have been investigated in the second-line setting but led to negative study results. More recently, the ADC trastuzumab-deruxtecan was authorized after the failure of trastuzumab-based treatment. However, further improvements in HER2-directed therapy are required as resistance mechanisms and HER2 heterogeneity limit the existing treatment options. This review aims to give an overview of the current standard-of-care HER2-directed therapy in gastric cancer, as well as its challenges and future developments.
1. Introduction
Gastric cancer still imposes a major health threat, with over one million new cases in 2020 and 769,000 deaths, ranking it the fourth leading cause of cancer-related deaths globally [1]. Human epidermal growth factor receptor-2 (HER2), also referred to as HER2/neu or ERBB2, is present in about 20% of gastric cancer cases [2,3].
HER2 is encoded on chromosome 17q21 and is part of the EGFR family, which also includes EGFR/HER1, HER3 and HER4 [4]. The ligand of the tyrosine kinase receptor is still not identified. HER2 forms either homodimers or heterodimers with other members of the EGFR family receptors [5]. HER2 homodimers can lead to ligand-independent activation in case of HER2 overexpression [6]. Heterodimers, however, rely on receptor-specific ligand binding [7]. In particular, the HER2/HER3 heterodimer was found to produce a potent mitogenic signal induced by its ligand, heregulin [8].
HER2 activation leads to downstream signaling via the PI3K/AKT/mTOR pathway or the RAS/MEK/MAPK pathways, inducing cell cycle progression, cell growth, proliferation of the cell, metastasis and inhibiting cell death [4,7,9].
Amplification or overexpression of HER2 can be found in various cancer entities. In gastric cancer, ERBB2 alterations are mainly present in the chromosomal unstable (CIN) subtype [10]. These aberrations mainly consist of missense mutations (74%) and, only to a lesser extent, insertions (22%) or fusions (0.7%) [11]. HER2 expression is more common in intestinal subtype according to Lauren’s classification, as well as proximal gastric cancer or gastroesophageal junction cancer, metastatic disease (especially liver metastasis) and lymph node invasion. Its prognostic relevance is still up for debate [4,5,7,12].
This review aims to give an overview of the current standard-of-care treatment as well as new therapeutic approaches to targeting HER2-positive gastric cancer.
2. Treatment of Metastatic HER2-Positive Gastric Cancer
Compared to the broad therapeutic options that are available for breast cancer, HER2-targeting therapies for gastric cancer remain limited [13].
2.1. Introduction of Trastuzumab
The monoclonal antibody trastuzumab inhibits downstream signaling by directly binding the juxtamembrane region (extracellular domain IV) of the HER2 receptor. This leads to endocytosis of the receptor, a blockade of either the constitutive active forms or the dimerization of HER2, and antibody-dependent cell-mediated cytotoxicity (ADCC) [5,7]. The ToGA study, including patients with gastric or gastroesophageal junction adenocarcinoma, was the first study to implement HER2-directed therapy with trastuzumab into the treatment of metastatic HER2-positive gastric cancer [14]. Trastuzumab plus cisplatin and capecitabin or fluorouracil improved overall survival (OS 13.8 vs. 11.1 months, HR 0.74), progression-free survival (PFS 6.7 vs. 5.5 months, HR 0.71) and objective response rate (ORR 47% vs. 35%) compared to chemotherapy alone in 584 treated patients. An exploratory analysis of the ToGA trial revealed that prolongation of OS correlated with HER2 expression. In HER2 highly expressing tumors (IHC 2+/ISH-positive or IHC3+), an OS of 16 months compared to 11.8 months for chemotherapy alone was achieved (HR 0.65). Importantly, HER2 expression but not amplification levels correlated with a better response to trastuzumab, and HER2 testing is therefore firstly based on immunohistochemistry [2]. Patients received six cycles (about 3.5 months) of trastuzumab plus chemotherapy before trastuzumab maintenance was initiated. Various smaller studies and case reports have described long-term responses under trastuzumab maintenance [15,16]. Recently, a retrospective biomarker analysis revealed that patients with a prolonged PFS under trastuzumab maintenance have higher PD-L1 CPS scores, which correlate with increased CD4+ memory T cells. The tumor mutational burden, ERBB2 score or resistance-associated genetic alterations (see below) did not differ between short-term and long-term responders [17]. Attempts to further improve maintenance strategies have not led to success so far. A higher maintenance dose (8 mg/kg vs. 6 mg/kg) in the HELOISE trial did not increase efficacy (HR 1.24) [18]. The addition of fluoropyrimidines to trastuzumab maintenance showed no prolongation of OS (15.2 vs. 17.0 months for trastuzumab alone) or PFS (5.1 months in both cases) in the large retrospective AGEO trial [19]. Of note, the reintroduction of initial chemotherapy upon progression achieved a longer OS than standard second-line regimens in the AGEO trial and might be a valuable option to preserve later treatment lines.
The results of the ToGA trial led to the authorization of trastuzumab in the first-line treatment of metastatic or unresectable HER2-positive gastric cancer combined with capecitabine or 5-fluorouracil (5-FU) and cisplatin. In the ToGA trial, 88% of the patients received capecitabine and cisplatin [14]. The current ESMO guidelines recommend a combination of trastuzumab and platinum/fluoropyrimidine-based chemotherapy, whereas oxaliplatin and cisplatin, as well as 5-FU, capecitabin and S-1, are stated as possible combination partners [20]. Real-world data of the German observational study HerMES revealed that only half of 364 included patients were treated in-label [21]. Other common chemotherapy regimens were FLOT, monotherapy with 5-FU/capecitabine and FOLFOX. PFS and OS ranged from 6.4 to 9.5 months and 12.3 to 15.8 months, respectively. In a meta-analysis, Ter Veer et al. showed that the doublet chemotherapy backbone of oxaliplatin and 5-FU/capecitabine prolonged OS in comparison to the ToGA regimen (cisplatin and 5-FU, HR 0.75) and reduced toxicity [22]. Cisplatin plus S-1 caused less hand–foot syndrome, but showed no survival benefit compared to ToGA. Furthermore, a triplet cytotoxic backbone could not improve survival but increased toxicity, while monotherapy with cisplatin or capecitabine provided insufficient results compared to the ToGA regimen. The authors claimed that a doublet therapy containing oxaliplatin is favorable over the ToGA regimen with cisplatin [22].
2.2. Trastuzumab and Checkpoint Inhibition
Recently, the placebo-controlled phase III KEYNOTE-811 study evaluated the addition of immune checkpoint inhibition (ICI) to standard first-line therapy with trastuzumab and chemotherapy for HER2-positive esophagogastric cancer [23]. The study demonstrated a significant and clinically meaningful improvement regarding tumor response rate (ORR) for ICI plus trastuzumab/chemotherapy [23]. Based on these results, the FDA granted approval for pembrolizumab in first-line chemotherapy with trastuzumab.
Survival data were presented at the ESMO 2023 [24]. Although there was an advantage in PFS (10.0 vs. 8.1 months; HR 0.73) and OS (20.0 vs. 16.9 months; HR 0.84) for all tumors, the subgroup analysis revealed that only PD-L1-positive tumors benefit from additional ICI (PFS 10.9 vs. 7.3 months; HR 0.71). The proportion of PD-L1-positive tumors in this study was high (CPS ≥ 1 in 88%), which might be due to co-expression of HER2 and PD-L1 [3]. In comparison, among HER2-negative tumors in the CHECKMATE-649 study, about 82% had a positive PD-L1 score (PD-L1 CPS expression ≥ 1) [25]. The FDA therefore restricted approval to PD-L1-positive tumors (CPS ≥ 1). In August 2023, pembrolizumab was also authorized by the EMA for tumors with CPS ≥1. Pembrolizumab plus trastuzumab and fluoropyrimidine/platinum-based chemotherapy is therefore a new standard-of-care regimen for PD-L1- and HER2-positive unresectable or metastatic gastric and gastroesophageal junction adenocarcinoma.
2.3. Beyond Progression to Trastuzumab
Upon progression to trastuzumab, the combination of trastuzumab and paclitaxel was proven ineffective in the Japanese T-ACT trial, with similar PFS (3.7 vs. 3.2 months) and OS (10 months in both arms) compared to paclitaxel alone (see Table 1) [26]. However, the combination of trastuzumab and standard second-line therapy consisting of the VEGF inhibitor ramucirumab and paclitaxel showed promising anti-tumor activity even after progression to trastuzumab in first-line therapy. An ORR of 54% and a DCR of 96% were reported in the single-arm Her-RAM study [27].

Table 1.
Randomized phase II or III trials for second-line therapy of HER2-positive gastric cancer.
The antibody–drug conjugate (ADC) trastuzumab-deruxtecan (Enhertu, T-DXd) is the first new therapeutic agent targeting HER2 to enter standard therapy for metastatic HER2-positive gastric cancer since the approval of trastuzumab. Antibody–drug conjugates (ADCs) link a cytotoxic drug to a monoclonal antibody by a chemical bond and therefore provide cytotoxicity as well as target specificity, stability and favorable pharmacokinetics [28]. T-DXd combines trastuzumab with a novel topoisomerase I inhibitor (exatecan mesylate) that has more potent efficacy than conventional SN-38, the active metabolite of irinotecan. With an antibody-to-drug ratio of 8:1, T-DXd has a higher payload than most ADCs. The linker consists of a tetrapeptide which is decomposed by cytosolic lysosomal enzymes expressed in tumor cells, releasing its cytotoxic load into the tumor cell. The binding activity to HER2 of T-DXd is comparable to unconjugated HER2-targeting agents. Besides its ADCC activity, T-DXd inhibits Akt phosphorylation and induces DNA damage [29]. Due to the membrane permeability of exatecan mesylate, T-DXd exhibits a bystander killing effect on surrounding tumor cells, which helps to overcome HER2 heterogeneity (see below) [30,31]. For metastatic breast cancer, T-DXd is already an available option after failure of trastuzumab in HER2-positive cancer and, since 2022, also in HER2-low expressing cancers (see below) [32].
T-DXd in gastric cancer was first tested in the Asian phase II DESTINY-Gastric01 trial. Upon the failure of at least two lines of therapy (including previous therapy with trastuzumab), T-DXd achieved better objective response rates (ORR 51% vs. 14%; p < 0.001) and confirmed objective response rates (i.e., an ORR lasting ≥ 4 weeks, cORR 43% vs. 12%) as well as longer OS (12.5 vs. 8.4 months) and PFS (5.6 vs. 3.5 months) than conventional chemotherapy (irinotecan or paclitaxel). Based on these data, T-DXd was approved by the FDA for HER2-positive metastatic gastric cancer [33]. Subgroup analysis revealed that HER2 3+ tumors benefit more from T-DXd than HER2 2+/FISH+ tumors, which is in line with in vitro results indicating that the anti-tumor efficacy of T-DXd is dependent on HER2 expression levels [31,33].
The EMA authorized T-DXd based on the results of the DESTINY-Gastric02 trial, which confirmed the efficacy of T-DXd in Western patients after the failure of trastuzumab-containing first-line therapy [34]. T-DXd showed a confirmed objective response of 42%, a median OS of 12.1 months and a median PFS of 5.6 months, which is consistent with the data from the DESTINY-Gastric01 study. Even though the current approval is granted without requiring re-biopsies to confirm HER2 status, histological reassessment should be discussed due to possible downregulation of HER2 after trastuzumab-containing therapy (see below).
Overall, the side effects of T-DXd were manageable, but severe treatment-emergent adverse events (CTCAE ≥ 3) occurred in over half of patients. The most common TEAEs were nausea and myelosuppression, which was addressed by dose reduction. The current NCCN guidelines classify T-DXd as a highly emetogenic substance and recommend triple prophylaxis consisting of NK1 receptor antagonist, 5-HT3 receptor antagonist and dexamethasone, which should be combined with olanzapine if necessary [35]. Interstitial lung disease (ILD) and pneumonitis are notable risks during T-DXd therapy, of which 10% were reported in each of the DESTINY-Gastric01 and 02 trials, with two cases ending fatally in DESTINY-Gastric02 [33,34]. Of note, the onset of ILD was late, within a median of 84.5 (DESTINY-Gastric01) and 80.5 (DESTINY-Gastric02) days after the start of therapy. Appropriate education on possible side effects and a close monitoring thereof are crucial during T-DXd therapy.
New therapeutic approaches and combinations with T-DXd are currently being assessed. DESTINY-Gastric04 (NCT04704934) compares T-DXd to the current second-line standard of ramucirumab and paclitaxel in a phase III trial. T-DXd plus chemotherapy and/or ICI is also under investigation as first-line therapy for metastatic HER2-positive gastric cancer in the phase Ib/II DESTINY-Gastric03 study (NCT04379596). Furthermore, T-DXd expresses activity in metastatic HER2-low breast cancer, and current ESMO expert consensus statements recommend the use of T-DXd in metastatic HER2-low breast cancer (IHC1+ or IHC2+/ISH−) after failure of prior CDK4/6 inhibitor therapy and at least one previous line of chemotherapy [36,37]. For gastric cancer, a small study with 21 patients recently provided preliminary evidence of the efficacy of T-DXd in IHC1+ (confirmed ORR 9.5%) or IHC2+/ISH− (confirmed ORR 26.3%) gastric cancer [38]. The ongoing DESTINY-Gastric03 trial will also partly include HER2-low gastric cancer.
Altogether, trastuzumab and T-DXd are, to date, the only HER2-targeting treatment options available for gastric cancer. In the metastatic setting, these two drugs are part of standard-of-care regimens (see Figure 1).
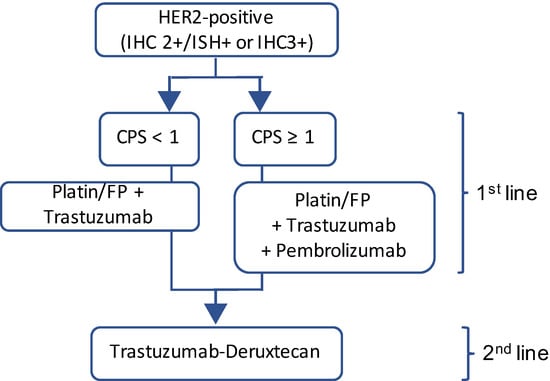
Figure 1.
HER2 directed therapy in metastatic HER2-positive gastric cancer. FP = Fluoropyrimidine.
3. Resistance to Trastuzumab
Even though the introduction of trastuzumab and, more recently, T-DXd can be seen as a great success in the treatment of HER2-positive gastric cancer, it has to be considered that long-term responses are only achieved in a minority of patients. Resistance to trastuzumab presents as primary resistance or occurs in a relatively short amount of time as secondary resistance (time to progression in ToGA trial 7.1 months) [7,14]. To further overcome such resistance, it is crucial to understand the underlying mechanisms. These can be divided into (a) masking, downregulation or cleavage of the receptor, (b) interaction or cross-signaling with other receptors and (c) aberrations in downstream pathways.
Masking of HER2 was shown by membrane-associated glycoprotein MUC4 and hyaluronan, which prevents the binding of trastuzumab. The use of 4-MU, a hyaluronan synthase inhibitor, improved the binding of trastuzumab. Furthermore, the hyaluronan receptor CD44 plays a role in HER2 downregulation. The siRNA-mediated suppression of CD44 results in decreased internalization of trastuzumab [39]. Downregulation of the HER2 receptor upon progression to trastuzumab is described in 30 to 60% of the patients and occurs preferably in IHC 2+ scored tumors [40,41,42]. Janjigian et al. recently showed in next-generation sequencing data that the level of ERBB2 amplification is linked to the response to trastuzumab. Upon failure of trastuzumab, ERBB2 amplification was lost in resistant tumors [43]. Moreover, cleavage of the HER2 receptor results in a 95 kDa membrane-associated fragment (p95HER2) with increased activity [5].
Various interactions of HER2 with other receptors are described, serving as escape mechanisms for HER2-targeting agents. Members of the EGFR family such as EGFR or HER3 are upregulated or form heterodimers with HER2 [5,44,45]. In breast cancer cells, interactions and cross-signaling with other receptors like MET and heterodimers with insulin-like growth factor (IGFR1) were found. Importantly, in gastric cancer cells, IGFR1 can induce PI3K signaling upon its upregulation in a HER2-independent manner [5,46]. The upregulation of other tyrosine kinases such as the proto-oncogene Src or the receptor tyrosine kinase FGFR3 also contribute to the resistance against HER2-directed drugs [45,47,48]. A small proportion of HER2-positive tumors also show EGFR and/or cMET overexpression. Concomitant overexpression of receptor tyrosine kinases (RTKs) is associated with a poor prognosis, with the worst results being observed in triple (HER2+/MET+/EGFR+)-positive gastric cancer [49].
A significant alteration and/or constitutive activation of multiple pathways can be detected in trastuzumab-resistant cell lines. In a proteomic analysis, Liu et al. found that the mTOR, Wnt, p53, metabolic and B-cell receptor signaling pathways were activated in trastuzumab-resistant cell lines. Trastuzumab-resistant cells also grew faster and showed morphological signs of EMT (epithelial–mesenchymal transition) [50,51]. In particular, the mTOR pathway showed an upregulation of key signaling components such as mTOR, AKT and RPS6KB1, whereas expression levels of AKT1S1, a mTOR inhibitor, were decreased. Importantly, trastuzumab-resistant cells lines were susceptible to the mTOR inhibitor AZD8055, which reduced the migration of the cells. Janjigian et al. confirmed that multiple mutations in significant pathways such as the RAS and PI3K pathways mark important resistance mechanisms to trastuzumab [43].
The PI3K pathway plays a crucial role in tumorigenesis in various entities. In gastric cancer, HER2 overexpression significantly correlates with pAKT expression [52,53]. In multiple analysis, the activation of the PI3K pathway was one key factor contributing to trastuzumab resistance. The detection of PIK3CA mutations in liquid biopsies was associated with primary resistance to trastuzumab, even though other studies found no association between trastuzumab resistance and PIK3CA mutations [41,54]. One mechanism resulting in overactivation of the PI3K pathway is the inactivation of PTEN. PTEN acts as a tumor suppressor gene by dephosphorylating PIP3, the product of PI3K and a messenger in various pathways inducing cell growth and migration. The loss of PTEN leads to the constitutive activation of the PI3K pathway and inhibits apoptosis and G1 cell cycle arrest [5,55]. PTEN loss is associated with primary resistance to trastuzumab and represents a negative prognostic factor [56]. Other mechanisms of PI3K activation and mediating trastuzumab resistance include the upregulation of NES1/KLK10, the proto-oncogene XB130 or the c-MET-associated MACC1 [57,58,59]. As a response to trastuzumab, the HER3 ligand heregulin (or neuregulin1β) is released by the metalloprotease ADAM 10 and mediates resistance to HER2-targeting agents. Benefitting from residual HER2 activity, heregulin induces resistance through HER3 and AKT activation and upregulates the PI3K pathway [44,60,61].
A better understanding of the mechanisms of resistance might offer new therapeutic options to overcome such resistance, like the additional use of mTOR inhibitors or the combination with trastuzumab to delay resistance [51]. However, in the clinical setting, mTOR inhibition with everolimus could not significantly improve overall survival compared to BSC in pretreated advanced gastric cancer [62]. This might be due to compensatory PI3K upregulation by the phosphorylation of Akt that diminishes the anti-tumor effect of monotherapy with mTOR inhibition [63]. The PI3K pathway might therefore be another promising target [53]. In vitro, the PI3K inhibitor copanlisib and the MEK inhibitor refametinib could reinstall sensitivity to trastuzumab and lapatinib in breast cancer cells with acquired resistance to either trastuzumab and/or lapatinib [64,65]. Accordingly, for HER2-positive gastric cancer cell lines, the combination of copanlisib and trastuzumab demonstrated more anti-proliferative effects than either of the inhibitors alone. Importantly, the combination of trastuzumab and refametinib or copanlisib showed synergistic effects in some cell lines, and trastuzumab plus copanlisib even overcame resistance to either drug as a single agent in one cell line [53].
For clinical practice, it is crucial to monitor the success of HER2-targeting drugs. Liquid biopsies can be one way to identify resistance to therapy. HER2 somatic copy number alterations (SCNAs) in plasma predicted tumor shrinkage and progression more reliably than carcinoembryonic antigen levels. Moreover, patients with primary resistance to trastuzumab showed high HER2 SCNAs upon progression, whereas HER2 SCNAs decreased in patients with acquired resistance compared to baseline. Trastuzumab resistance was often accompanied by NF1 and ERBB2/4 gene mutations detectable in liquid biopsies [54].
Metabolic reprogramming plays a critical role in tumor cells, enabling cell growth and proliferation. Gastric cancer cells resistant to trastuzumab exhibit increased glycolysis, and 6-phosphofructo-2-kinase (PFKFB3) was shown to activate glycolytic pathways, resulting in distinct changes in the tumor microenvironment [57,66].
HER2-Positive or Not?
Besides resistance mechanisms, HER2 heterogeneity represents an obstacle when targeting HER2. The definition of HER2 positivity relies on a pathological evaluation of tumor tissue samples. HER2-positive samples are commonly defined as IHC score 2+ and ISH-positive or IHC score 3+. For FISH assessment, a HER2:CEP17 (centromeric probe 17) ratio of ≥2 is defined as positive for HER2 amplification [67]. Due to the higher occurrence of glands in the gastric epithelium, incomplete (U-shaped or basolateral only) membranous staining is more common in gastric cancer than in breast cancer. Pathological HER2 scoring systems differ accordingly between the two entities, as for gastric cancer, samples with only basolateral staining in ≥10% of the cells are also considered positive. Because of the heterogeneity of HER2 expression in gastric cancer, the 10% cut-off was replaced by the absolute number of five cohesive cells with strong reactivity in biopsy specimens [67,68].
In a comparative analysis of 1414 cases of whole-tissue sections and 595 cases of tissue microarrays, samples scored 3+ stained ≥ 50% of the tumor area in over 90% of cases, whereas only 40% of 2+-scored samples achieved the same. Staining in less than 50% of the tumor area worsened the prognosis [12]. Even though the definition of heterogeneity in HER2 scoring is not clear, heterogeneity seems to be foremost relevant in lower IHC stained tumors [2]. In the HER2 screening data of the ToGA trial, IHC2+ and 3+ stained tumors showed a benefit from trastuzumab regardless of staining variability. However, a numerical trend towards better results was observed in tumors with >30% cells stained than tumors with ≤30% staining [2]. Another small study observed a significant difference in response to trastuzumab due to heterogeneity: tumors with a homogenous expression of HER2 had better PFS and OS than heterogeneously HER2-expressing tumors [69]. The recent VARIANZ study observed major discrepancies in the HER2 testing of tumors between local and central assessment (deviation rate of 22.7%, mainly due to false-positive testing locally). These tumors showed mostly intermediate HER2 expression. Only patients with a centrally confirmed HER2 positivity (central HER2+ and local HER2+) benefitted from a trastuzumab-based treatment compared to only locally positive tested tumors. HER2 expression and the HER2:CEP17 ratio were higher and more homogenous among centrally and locally positive tested tumors. The authors argue, that HER2 thresholds might have to be reconsidered to reliably identify patients who benefit from trastuzumab, and calculated a minimum of 40% HER2+ cells and an amplification ratio of 3.0 as optimized criteria [70]. Recently, Janijigan et al. demonstrated that the response to trastuzumab is increased in patients with high levels of ERBB2 amplifications in sequencing [43].
Moreover, the method of specimen taking might influence HER2 testing. The screening data of the ToGA trial revealed a numerically higher rate of HER2-positive tested tumors in biopsies than surgical specimens (23.2% vs. 19.7%) [2]. Van Cutsem et al. attributed this effect to few biopsy samples taken and the different criteria for HER2 positivity in biopsies (five cohesive cells) vs. tissue samples (≥10% of the cells). The GASTHER1 study confirmed the importance of multiple biopsies to assess the correct HER2 status. Patients who were initially considered as HER2-negative showed a conversion rate of 8.7% in immediate re-biopsies [71]. In particular, IHC 1+- or 2+-positive tumors compared to IHC 0 were more likely to be HER2-positive in re-biopsies. In a larger study, 17.6% had a rescued HER2 positivity after reassessment. Of note, rescued HER2-positive tumors showed a prognostic relevance with worse PFS and OS in the subgroup of IHC 3+ tumors than initially positive tested tumors [72]. Hence, current guidelines recommend taking multiple biopsies to correctly assess suspicious lesions: the German S3 guidelines suggest at least eight biopsies, and the NCCN guidelines and ESMO guidelines recommend 6–8 and 5–8, respectively [20,73,74].
Nevertheless, sampling errors due to HER2 heterogeneity still impose an obstacle even though multiple biopsies are taken. One study compared tissue microarrays (TMAs) serving as a “biopsy procedure” to whole-tissue sections from the same paraffin blocks. Whilst the VARIANZ study observed discrepancies in central and local HER2 testing, mostly due to false-positive testing locally with a significant impact on survival upon trastuzumab-based therapy, this study found a higher false-negative rate of 24% and only a minor false-positive rate of 3% [75]. The authors argue that unresectable gastric cancers might not receive HER2-directed therapy due to sampling errors in performed biopsies. Both studies considered the heterogeneity of HER2 expression as cause for discrepancies in HER2 testing.
Another aspect of spatial heterogeneity in HER2-positive gastric cancer is not only the discrepancies within the primary tumor but also varying HER2 expressions between different tumor lesions. In a small number of patients in the GASTHER1 trial, recurrent or metastatic (especially liver metastases) tumor lesions were HER2-positive in 5.7% even though the primary tumor was tested as HER2-negative [71]. Multiregion sequencing of the primary tumor and metastatic sites revealed differences in the genomic profiling, including oncogene amplifications such as EGFR, ERBB2, MET and PIK3CA [76]. Autopsies upon failure of HER2-targeting therapy confirmed a heterogeneous distribution of driver amplifications in different tumor lesions [77]. The authors argued that the limited efficacy of HER2-directed therapy was also due to heterogeneity and rapid selection of sensitizing or resistance-related genomic alterations [77].
Altogether, biopsies seem to be insufficient to capture the heterogeneity and complexity of HER2-positive gastric cancer. cfDNA obtained from peripheral blood plasma could be a suitable option to complete tumor assessment and to determine the indicated targeted therapies. In a pilot study, cfDNA enabled the detection of genomic alterations that were not exhibited in the sequencing of the primary tumor [76]. Simultaneously, high concordance rates for targetable alterations between metastases and cfDNA were shown, rendering cfDNA as a possible diagnostic tool to overcome spatial heterogeneity between different tumor lesions without the need for excessive and invasive biopsies [76]. However, the sensitivity of ctDNA might be dependent on disease site and burden, as detection was shown to be lower in peritoneal metastases than in liver or lung lesions and in tumors with fewer lesion sites [78]. In one trial, only 60% of clinically HER2-positive tumors were found to be positive in ctDNA evaluation. The combination of ctDNA plus tissue NGS might be the most accurate way to avoid false-negative results. HER2 amplification by ctDNA-NGA and/or tissue NGS was also prognostically relevant upon HER2 targeting (OS 26.3 vs. 7.4 months) [78].
An interesting non-invasive approach to circumvent the obstacle of heterogeneity could be the use of 89Zr-trastuzumab PETs. The HER2-directed functional imaging could potentially predict therapy response prior to disease progression in conventional CT/MRI imaging [77]. A pilot study showed that 89Zr-trastuzumab-PET was able to detect tumor lesions, especially in the bones [79]. In contrast, 18F-FDG-PET might be more sensitive for tumor manifestations in the lymph nodes. The HER2-PET is also limited in evaluating hepatic lesions due to high background signals. Furthermore, HER2-PET reflects HER2 heterogeneity throughout the entire body by varying tracer uptake between different tumor lesions, and might help to guide HER2-directed therapy and clinical decision making. The biomarker analysis of a phase II study including 89Zr-trastuzumab PETs and serial ctDNA demonstrated that the combination of these non-invasive assessments may predict PFS [80]. Concerning ctDNA, the clearance of all tumor-matched alterations was associated with a benefit in PFS.
4. New Perspectives in HER2 Targeting
HER2 heterogeneity and resistance mechanisms to HER2-targeting agents limit the efficacy of standard-of-care treatment with trastuzumab and T-DXd. Further attempts at HER2 targeting have been made to circumvent these obstacles.
4.1. Monoclonal and Bispecific Antibodies
Pertuzumab is a monoclonal antibody targeting extracellular domain II of HER2, preventing the formation of heterodimers such as the highly mitogenic HER2/HER3 dimer (see Table 2) [7]. In the JACOB trial, adding pertuzumab to first-line chemotherapy plus trastuzumab in metastatic HER2-positive esophagogastric cancer failed to significantly improve overall survival in spite of a positive trend in PFS and ORR. Moreover, the therapy showed more grade ≥ 3 diarrhea and nausea and led to a greater dose reduction of the chemotherapy [81].
Table 2.
Overview of selected HER2-targeting drugs.
Margetuximab is an Fc-modified chimeric antibody that increases the affinity to activated FcR (CD16A; FcγRIIIa) and reduces its affinity for inhibitory FcR (CD32B; FcγIIb). It enhances ADCC and boosts T-cell activity and PD-L1 expression [28]. In 2020, margetuximab was granted orphan drug status for esophagogastric cancer by the FDA. The MAHOGANY trial investigated margetuximab plus retifanlimab, a monoclonal antibody against PD-1, for first-line therapy of HER2/PD-L1-positive esophagogastric cancer. Compared to historical controls, margetuximab/retifanlimab showed a favorable toxicity in Cohort A. Given that this was a chemotherapy-free option, objective response rates were also improved. Nevertheless, the enrolment of the study was discontinued due to business reasons of the sponsor [82].
New developments for monoclonal antibodies also include, e.g., the combination of trastuzumab and BI-1607. BI-1607 is a monoclonal antibody against CD32b or FcγIIb and aims to enhance trastuzumab efficacy and escape resistance against it (NCT05555251). A phase I/IIa trial (CONTRAST) is currently ongoing for advanced solid HER2-positive tumors after failure of trastuzumab and HER2-targeting ADCs.
Furthermore, HLX22 is tested in combination with trastuzumab and chemotherapy (XELOX) for first-line therapy of advanced HER2-positive gastric cancer (NCT04908813). HLX22 is a novel monoclonal antibody against domain IV of HER2. The targeted epitope is different compared to trastuzumab, enabling the simultaneous binding of both antibodies [83]. In a phase I study, HLX22 was tolerable and showed moderate anti-tumor activity after the failure of standard therapy lines in HER2-positive advanced solid cancer [83].
Bispecific antibodies such as, e.g., KN026 and zanidatamab (ZW25) are subjects of ongoing clinical studies and bind extracellular domains II (pertuzumab-binding site) and IV (trastuzumab-binding site) [28]. KN026 exhibited promising anti-tumor activity in a phase II trial in HER2-expressing (ORR 56%) and HER2-low tumors (ORR 14%) after failure of one line of standard treatment [84].
Zanidatamab induces ADCC, HER2 internalization and downregulation, the inhibition of cell signaling, and tumor growth and shows superior anti-tumor activity in preclinical models compared to trastuzumab plus pertuzumab [85]. In untreated advanced or metastatic gastroesophageal adenocarcinoma, zanidatamab plus chemotherapy achieved an ORR of 68.2% and a DCR of 90.9% in a phase II study [86]. While guaranteeing a manageable safety profile, the most common treatment-related adverse events were diarrhea (grade 3 in 43%), vomiting and hypokalemia. The ongoing phase III HERIZON-GEA-01 trial evaluates the combination of zanidatamab and chemotherapy ± the checkpoint inhibitor tislelizumab for the first-line treatment of HER2-positive esophagogastric cancer [87].
Cinrebafusp alfa, a bispecific antibody against HER2 and the co-stimulatory immune receptor 4-1BB on T cells, has shown tolerability and anti-tumor activity in a phase I trial and is currently under investigation for second-line therapy of HER2-positive (high and low) gastric cancer [88].
4.2. Antibody–Drug Conjugates (ADCs)
To date, T-DXd remains the only authorized ADC for HER2-positive gastric cancer. Contrary to the results in breast cancer, trastuzumab-emtansin (T-DM1) was unsuccessful in esophagogastric cancer. In the phase II/III GATSBY trial, T-DM1 was not superior to conventional chemotherapy with taxane in previously treated HER2-positive advanced gastric cancer (OS: 7.9 vs. 8.6 months) (s. Table 1) [89]. The addition of capecitabine to T-DM1 in a phase I/II study also did not improve the ORR significantly [90]. T-DM1 is an ADC linking trastuzumab to the potent microtubule inhibitor emtansine (DM1), a derivative of maytansine [7,89]. Reasons for the failure of T-DM1 could be its lower drug-to-antibody ratio (3.4:1), the less potent payload and its poorer membrane permeability [29,30,33]. In contrast to T-DXd, the payload of T-DM1 remains attached to its linker even after degradation in the tumor cell. T-DM1 is therefore less capable of killing bystander tumor cells than T-DXd, which contributes significantly to the success of T-DXd in even heterogeneously HER2-expressing tumors. Moreover, reassessment of HER2 status was not required before enrolment in the GATSBY trial, so it has to be assumed that some of the tumors lost their HER2 expression after receiving prior HER2-directed therapy.
Other ADCs are currently under investigation. For disitamab-vedotin (RC48), an anti-HER2 monoclonal antibody–MMAE conjugate, a phase II trial with 179 patients showed an ORR of 24.8%, as well as a PFS and OS of 4.1 months and 7.9 months, respectively [91]. A previous phase I study including various solid tumors, but mostly (82.5%) gastric cancer, indicated similar responses in HER2-high and HER2-low expressing tumors [92]. Another phase I trial is currently recruiting patients to evaluate disitamab-vedotin plus the PD-1 inhibitor toripalimab for first-line treatment of HER2-low expressing advanced gastric cancer (NCT06078982). Furthermore, a phase II/III trial evaluates disitamab-vedotin plus chemotherapy, toripalimab and trastuzumab in HER2-expressing (high vs. low) tumors (NCT05980481). An overview of other ADCs currently under investigation in clinical trials is given in Table 3.
Table 3.
Selection of ongoing HER2-targeting studies in advanced gastric cancer.
4.3. Small-Molecule Inhibitors
As an oral dual HER2/EGFR tyrosine kinase inhibitor, lapatinib could provide anti-cancer efficacy in pretreated and trastuzumab-resistant breast cancer patients, and the combination of trastuzumab and lapatinib improved the outcome in the neoadjuvant and metastatic setting [93,94,95]. In vitro, anti-tumor activity was shown in gastric cancer [96]. Lapatinib was able to inhibit cross-signaling with IGF1 in solid cancer and breast cancer, providing a rationale for its use upon progression to trastuzumab [97,98].
However, despite these promising preclinical data, lapatinib has only achieved disappointing results in the clinical setting for gastric cancer. In the TRIO-013/LOGiC trial, the combination of lapatinib and CAPOX for first-line therapy of advanced gastric cancer could not significantly improve OS and PFS, even though the response rates were higher than in the control arm. Differences in the effect of lapatinib in region and age were observed, with a prolongation of OS in Asian and younger patients [99]. Insufficient activity and increased toxic sides effects (mainly diarrhea) were confirmed in other studies evaluating lapatinib for second-line treatment [100,101]. In the TyTAN study, the addition of lapatinib to paclitaxel vs. paclitaxel alone in second-line treatment of advanced gastric cancer led to better results regarding ORR, but did not translate into a significant improvement in OS or PFS (see Table 1) [100]. Again, better results were observed in Asian patients and, contrary to the results of the LOGiC trial, were dependent on HER2 IHC status, with a greater effect on HER2 3+ tumors.
Liquid biopsies with cfDNA detecting the ERBB2 copy number were able to predict the response and sensitivity to lapatinib in a small phase II study combining lapatinib with CAPOX in the neoadjuvant setting [102]. Resistance to lapatinib is linked to the rephosphorylation and reactivation of EGFR and HER3 kinases, which can be delayed by combining anti-HER2 therapies in vitro [103]. Combining HER2-targeting therapies like lapatinib and trastuzumab might therefore be an option that is already proven to be effective in breast cancer. Accordingly, in gastric cancer cell lines and xenografts, a synergistic effect of trastuzumab and lapatinib was demonstrated [104].
Altogether, monotherapy with lapatinib has not provided convincing clinical results so far. Other small molecules inhibiting transphosphorylation or their combination might lead to more success and are currently under investigation [28].
The irreversible pan-HER (HER1, 2 and 4) inhibitor afatinib induced a sustained inhibition of EGFR and HER3 as sufficiently as the dual blockade of lapatinib and trastuzumab and provided a durable tumor regression in vitro [77,103,104]. In a small study with pretreated metastatic GC (including at least one line with trastuzumab), afatinib monotherapy showed modest clinical benefit with a PFS of 2 months and an OS of 7 months [77]. Whilst the co-amplification of ERBB2 and EGFR demonstrated a clinical benefit, tumors with KRAS, PIK3CA or NF1 mutations progressed rapidly. MET amplification also led to afatinib resistance. A modest anti-tumor effect was further described upon dual inhibition with trastuzumab and afatinib, even for ERBB2-amplified tumors lacking an EGFR amplification [77]. In the AGAPP trial, on the other hand, afatinib plus chemotherapy for the first-line treatment of metastatic GC showed no further advantage compared to present regimens, with a median PFS of 5.0 and an OS of 8.7 months. However, it must be taken into account that only 12.7% of the tumors were HER2-positive [105].
With tucatinib, a new orally available, highly selective and reversible HER2-targeting small-molecule tyrosine kinase inhibitor is on the horizon with promising anti-tumor activity in gastric cancer xenograft models and CRC cancer if combined with trastuzumab [106,107]. The ongoing MOUNTAINEER02 (NCT04499924) trial is investigating tucatinib plus trastuzumab, ramucirumab and paclitaxel in second-line treatment of advanced HER2-positive gastric cancer after progression to anti-HER2 targeted first-line therapy [108]. A phase I/II trial evaluating tucatinib and trastuzumab as first-line therapy is also in progress (NCT04430738). Combinations with checkpoint inhibition (pembrolizumab) and chemotherapy (FOLFOX/CAPOX) are available in this trial.
Dual HER2 inhibition is also under investigation using the pan-HER inhibitor neratinib and trastuzumab plus chemotherapy in the first-line treatment of HER2-positive gastroesophageal cancer (NCT06109467).
5. Other Developments in HER2 Targeting
Genetically engineered T cells with chimeric antigen receptors (CARs) have led to major success in hematologic neoplasms by coupling an extracellular antigen-identifying domain to an intracellular stimulating domain that activates the CAR T cells [109]. However, targeting solid tumors with CAR T cells is a challenge due to antigen heterogeneity, infiltration difficulties and the immunosuppressive tumor microenvironment in solid cancer [109]. So far, HER2-targeting CAR T cells exhibited persistent anti-tumor activity in vitro and in vivo [110], and various phase I studies evaluate HER2-directed CAR T cells for solid tumors, including gastric cancer (see Table 3).
Other approaches include the modification of T cells. T-cell antigen couplers (TACs) are a novel technology to modify T cells in order to recognize HER2+ tumors. The TAC receptor recognizes tumor cells and co-opts with the endogenous TCR, mediating a more efficient anti-tumor response with less toxicity than CAR T cells [111]. In the phase I/II TAC01-HER2 trial, TACs showed manageable safety and promising clinical activity in various HER2+ tumors, including gastric and gastroesophageal junction cancer [112]. In the ongoing trial, TACs are combined with pembrolizumab (see Table 3).
Cancer vaccines provide tumor neoantigens (whole cells or characteristic components) to prime T and B lymphocytes against tumor epitopes [113]. In case of HER2-overexpressing gastric cancer, the IMU-131/HER-Vaxx was tolerable and safe in a phase I study and provided humoral, cellular and clinical responses in a dose-dependent manner. The vaccine consists of three fused B-cell epitopes from the HER2 extracellular domain coupled to the diphtheria toxoid and combined with the adjuvant montanide [114]. In the phase II HERIZON study, CAPOX plus HER-Vaxx improved the outcome compared to CAPOX alone in HER2-positive gastric adenocarcinoma naïve to HER2-targeting therapy [115]. The addition of HER-Vaxx resulted in a 42% survival benefit (HR 0.58, p = 0.066) and a median OS of 13.9 months (vs. 8.3 months for chemotherapy alone). HER-Vaxx is currently being evaluated in a phase II trial upon progression to trastuzumab (NCT05311176).
Another B-cell epitope HER2 vaccine is being tested in China (NCT05315830), and recently, a B-cell- and monocyte-based immunotherapeutic vaccine (BVAC-B) transfected with recombinant HER2 showed activation of immune cells and manageable toxicity. However, the clinical tumor response was limited in heavily pretreated patients [116].
Immune modulation is also achieved by CYNK-101, a human placental hematopoietic stem/progenitor cell-derived NK cell product. By expressing a variant of CD16, FcyRIII, it enhances ADCC. Dose-limiting toxicities are evaluated in a phase I trial, treating patients with CYNK-101, pembrolizumab and trastuzumab after lymphodepletion (NCT05207722).
Furthermore, the ASPEN-01 trial investigated the fusion protein evorpacept or ALX148 in various solid tumors. ALX148 blocks CD47, which is a surface protein acting as an immune checkpoint by suppressing tumor cell phagocytosis and innate immune functions. In preclinical studies, ALX148 enhanced phagocytosis as well as trastuzumab-associated tumor inhibition and elicited innate and adaptive anti-tumor responses [117]. In the ASPEN-01 study, 19 patients with HER2-positive gastric and gastroesophageal junction cancer received ALX148 and trastuzumab upon progression to HER2-direceted therapy. An ORR of 21%, a PFS of 2.2 months and an OS of 11.1 months were reported. ALX148 received fast-track designation by the FDA for development in HER2-postive gastric or gastroesophageal junction cancer [118]. The ongoing ASPEN-06 study evaluates the use of ALX148 plus trastuzumab and standard second-line therapy (ramucirumab/paclitaxel) in further treatment lines (NCT05002127).
A completely different approach to HER2-targeting is pursued with the use of CAM-H2 (131I-SGMIB anti-HER2-VHH1), a radioligand directed at HER2. A phase I study showed its tolerability and uptake into HER2-overexpressing lesions [119]. A dose escalation phase I/II study upon progression to anti-HER2 treatment is underway (NCT04467515).
Altogether, these new agents bare the potential to overcome resistance to trastuzumab in HER2-positve gastric cancer. T-DXd is, to date, the only available HER2-targeting therapeutic option upon progression to trastuzumab. Even though HER2 downregulation took place during trastuzumab therapy, T-DXd might be effective due to its bystander killing effect. Other ADCs such as disitamab-vedotin might lead to comparable results. Combining different therapeutical strategies such as different monoclonal antibodies, TKIs or immune modulators could also be an option to re-enable trastuzumab efficacy. Even though lapatinib has not led to success so far, other TKIs (afatinib and tucatinib in combination with trastuzumab) have shown promising results even upon progression to trastuzumab in vitro and in vivo [77,108,120]. A multitude of ongoing clinical studies (see Table 3) include patients in second and further lines. These studies will demonstrate whether new therapeutic agents are still effective after standard first-line therapy with trastuzumab and can potentially overcome resistance to trastuzumab.
6. Perioperative Treatment of HER2 Gastric Cancer
After the introduction of trastuzumab and T-DXd into the therapeutical landscape of metastatic and unresectable HER2-positive gastric cancer, efforts are made to implement HER2 targeting into the perioperative treatment of locally advanced gastric cancer to further improve surgical und survival outcomes. Standard therapy for ≥T2 and/N+ tumors consists of perioperative chemotherapy with FLOT (docetaxel, 5-fluorouracil, leucovorin, oxaliplatin). In the FLOT-4 study, FLOT generated pCR rates of 16%, a median DFS of 30 months and a median OS of 50 months [121,122].
The phase II single-arm HERFLOT study demonstrated that the addition of trastuzumab to perioperative chemotherapy with FLOT results in a pCR rate of 21.4% [123]. This is of great interest, as high pCR rates are associated with favorable outcome [124,125,126]. In the HERFLOT study, only intestinal subtypes according to Laurén benefitted from trastuzumab compared to diffuse subtypes (pCR rate 33.3% vs. 0%). The median DFS was 42.5 months.
Similar to the JACOB trial in a metastatic setting, the following phase II PETRARCA study combined a dual HER2 blockade of trastuzumab and pertuzumab with perioperative FLOT [127]. In 81 patients, FLOT/pertuzumab/trastuzumab significantly improved the pCR rate (35% vs. 12%, p = 0.02) and survival rates at 24 months (DFS 70% vs. 54%; OS 84% vs. 77%) compared to FLOT alone. However, the addition of pertuzumab and trastuzumab led to an unfavorable toxicity profile. Higher rates of diarrhea as well as leukopenia and more dose modifications were described. The study was terminated prematurely.
The three-arm phase II EORTC INNOVATION study confirmed the great toxicity of dual HER2 blockade in the perioperative setting [128]. Perioperative chemotherapy (cisplatin/capecitabin in 42.2% and FLOT in 46.6%) was compared to trastuzumab or trastuzumab plus pertuzumab. A significant advantage in pathological response was only observed for the addition of trastuzumab (major pathologic response corresponding to <10% residual tumor in 37.0% vs. 23.3%, p = 0.099) and not for dual inhibition with trastuzumab and pertuzumab (26.4% vs. 23.3%, p = 0.378). This could be due to the toxicity of the dual inhibition, which led to less completion of the neoadjuvant treatment. Although the primary endpoint analysis did not meet the pre-specified criteria of efficacy for the combination of chemotherapy, trastuzumab and pertuzumab (increase in major pathologic remissions from 25% to 45%), the combination of chemotherapy and trastuzumab showed promising major pathologic response rates (mpRRs), especially with FLOT as the chemotherapy backbone (20% improvement in mpRR versus chemotherapy alone; 53% vs. 33%). EFS and OS data are still pending.
In Asian countries, gastrectomy and adjuvant chemotherapy alone represents the standard-of-care treatment. Preoperative chemotherapy is only applied in case of bulky lymph node disease [129,130]. For the latter, the combination of trastuzumab, S-1 and cisplatin preoperatively and S-1 adjuvant was feasible and safe in the TRIGGER study [131]. Radiological and pathological responses favored the trastuzumab group.
In summary, the combination of trastuzumab and perioperative chemotherapy showed promising results for increased pCR and survival rates, whereas dual inhibition might be too toxic. Nevertheless, more data are needed in this indication, and the use of anti-HER2 treatment in the perioperative setting is only recommended within clinical trials.
Recently, the synergism between ICI and HER2-targeted therapy further improved response and survival rates in the KEYNOTE-811 [24]. Multiple phase II trials are currently investigating the combination of ICI and trastuzumab plus chemotherapy for the perioperative setting (see Table 4). Other approaches in the perioperative setting include vaccination after standard adjuvant treatment with the pDNA-based AST-301 encoding HER2 (NCT05771584) or the use of ADCs (NCT05034887, NCT06155383).
Table 4.
Overview of trials for locally advanced HER2-positive gastric cancer.
7. Conclusions
In summary, HER2 remains an important biomarker for the treatment of gastric cancer. With T-DXd, significant progress has been made for the first time since the introduction of trastuzumab into the palliative treatment of metastatic gastric cancer. Other drugs are underway to further improve clinical outcomes and to face the challenges of-anti HER2 treatment, such as resistance mechanisms and HER2 heterogeneity.
Besides HER2, other important biomarkers make their way into clinical practice: The Claudin18.2-directed monoclonal antibody Zolbetuximab showed promising results in the SPOTLIGHT and GLOW studies [132,133]. The monoclonal antibody against FGFR2b, Bemarituzumab, is the subject of ongoing phase III studies (NCT05052801, NCT05111626). The treatment of gastric cancer will therefore involve further steps towards personalized therapy.
Author Contributions
Conceptualization: M.K.S. and S.L.; writing—original draft: M.K.S.; writing—review and editing: M.K.S., R.D.H. and S.L. All authors have read and agreed to the published version of the manuscript.
Funding
This review received no external funding.
Conflicts of Interest
MKS has nothing to declare. RDH reports personal fees from Abbvie, Amgen, Astra Zeneca, Bayer, BMS, Boehringer, Daiichi, GSK, Leo, Lilly, medupdate, Merck, MSD, Nordic, Onkowissen, Piere Fabre, Roche, Saladax, Sanofi, Servier, Synlab, Takeda and WALA. RDH reports an advisory function for Abbvie, Amgen, Astra Zeneca, Bayer, BMS, Boehringer, Daiichi, GSK, Leo, Lilly, Merck, MSD, Nordic, Onkowissen, Pierre Fabre, Roche, Saladax, Sanofi, Servier, Takeda and WALA. RDH reports study grants from Amgen, medac, Merck, Roche, Saladax and Sanofi. RDH reports expert activities for Deutsche Krebshilfe. SL reports personal fees from Amgen, AstraZeneca, BMS, Eli Lilly, Elsevier, Merck Serono, Merck Sharp & Dohme, Roche, Servier. SL reports an advisory function for Eli Lilly, Roche, Servier, Merck-Serono, Sanofi-Aventis, MSD. SL reports study grants from Eli Lilly.
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Van Cutsem, E.; Bang, Y.-J.; Feng-Yi, F.; Xu, J.M.; Lee, K.-W.; Jiao, S.-C.; Chong, J.L.; López-Sanchez, R.I.; Price, T.; Gladkov, O.; et al. HER2 Screening Data from ToGA: Targeting HER2 in Gastric and Gastroesophageal Junction Cancer. Gastric Cancer Off. J. Int. Gastric Cancer Assoc. Jpn. Gastric Cancer Assoc. 2015, 18, 476–484. [Google Scholar] [CrossRef] [PubMed]
- Janjigian, Y.; Rha, S.; Oh, D.; Díez García, M.; van Laarhoven, H.; Chao, Y.; Di Bartolomeo, M.; Haj Mohammad, N.; Zhong, W.; Croydon, E.; et al. SO-7 Co-Occurring HER2 and PD-L1 Expression in Patients with HER2-Positive Trastuzumab-Refractory Gastric Cancer (GC)/Gastroesophageal Junction Adenocarcinoma (GEJA): Biomarker Analysis from the Trastuzumab Deruxtecan (T-DXd) DESTINY-Gastric03 Trial. Ann. Oncol. 2022, 33, S358–S359. [Google Scholar] [CrossRef]
- Janjigian, Y.Y.; Werner, D.; Pauligk, C.; Steinmetz, K.; Kelsen, D.P.; Jäger, E.; Altmannsberger, H.M.; Robinson, E.; Tafe, L.J.; Tang, L.H.; et al. Prognosis of Metastatic Gastric and Gastroesophageal Junction Cancer by HER2 Status: A European and USA International Collaborative Analysis. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2012, 23, 2656–2662. [Google Scholar] [CrossRef] [PubMed]
- Sukawa, Y.; Yamamoto, H.; Nosho, K.; Ito, M.; Igarashi, H.; Naito, T.; Mitsuhashi, K.; Matsunaga, Y.; Takahashi, T.; Mikami, M.; et al. HER2 Expression and PI3K-Akt Pathway Alterations in Gastric Cancer. Digestion 2014, 89, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Worthylake, R.; Opresko, L.K.; Wiley, H.S. ErbB-2 Amplification Inhibits down-Regulation and Induces Constitutive Activation of Both ErbB-2 and Epidermal Growth Factor Receptors. J. Biol. Chem. 1999, 274, 8865–8874. [Google Scholar] [CrossRef] [PubMed]
- Okines, A.F.C.; Cunningham, D. Trastuzumab: A Novel Standard Option for Patients with HER-2-Positive Advanced Gastric or Gastro-Oesophageal Junction Cancer. Ther. Adv. Gastroenterol. 2012, 5, 301–318. [Google Scholar] [CrossRef] [PubMed]
- Pinkas-Kramarski, R.; Soussan, L.; Waterman, H.; Levkowitz, G.; Alroy, I.; Klapper, L.; Lavi, S.; Seger, R.; Ratzkin, B.J.; Sela, M.; et al. Diversification of Neu Differentiation Factor and Epidermal Growth Factor Signaling by Combinatorial Receptor Interactions. EMBO J. 1996, 15, 2452–2467. [Google Scholar] [CrossRef]
- Ersahin, T.; Tuncbag, N.; Cetin-Atalay, R. The PI3K/AKT/mTOR Interactive Pathway. Mol. Biosyst. 2015, 11, 1946–1954. [Google Scholar] [CrossRef]
- Cancer Genome Atlas Research Network. Comprehensive Molecular Characterization of Gastric Adenocarcinoma. Nature 2014, 513, 202–209. [Google Scholar] [CrossRef]
- Hyman, D.M.; Piha-Paul, S.A.; Won, H.; Rodon, J.; Saura, C.; Shapiro, G.I.; Juric, D.; Quinn, D.I.; Moreno, V.; Doger, B.; et al. HER Kinase Inhibition in Patients with HER2- and HER3-Mutant Cancers. Nature 2018, 554, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.C.; Koh, Y.W.; Chang, H.-M.; Kim, T.H.; Yook, J.H.; Kim, B.S.; Jang, S.J.; Park, Y.S. Evaluation of HER2 Protein Expression in Gastric Carcinomas: Comparative Analysis of 1414 Cases of Whole-Tissue Sections and 595 Cases of Tissue Microarrays. Ann. Surg. Oncol. 2011, 18, 2833–2840. [Google Scholar] [CrossRef] [PubMed]
- Shimoyama, S. Unraveling Trastuzumab and Lapatinib Inefficiency in Gastric Cancer: Future Steps (Review). Mol. Clin. Oncol. 2014, 2, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Bang, Y.-J.; Van Cutsem, E.; Feyereislova, A.; Chung, H.C.; Shen, L.; Sawaki, A.; Lordick, F.; Ohtsu, A.; Omuro, Y.; Satoh, T.; et al. Trastuzumab in Combination with Chemotherapy versus Chemotherapy Alone for Treatment of HER2-Positive Advanced Gastric or Gastro-Oesophageal Junction Cancer (ToGA): A Phase 3, Open-Label, Randomised Controlled Trial. Lancet Lond. Engl. 2010, 376, 687–697. [Google Scholar] [CrossRef] [PubMed]
- Fu, X.; Zhang, Y.; Yang, J.; Qi, Y.; Ming, Y.; Sun, M.; Shang, Y.; Yang, Y.; Zhu, X.; Gao, Q. Efficacy and Safety of Trastuzumab as Maintenance or Palliative Therapy in Advanced HER2-Positive Gastric Cancer. OncoTargets Ther. 2018, 11, 6091–6100. [Google Scholar] [CrossRef] [PubMed]
- Haider, S.; Ahmad, H.; Shah, S.; Neelma, F.; Ullah, W. Robust Anti-Tumor Response in a Patient with Metastatic Gastroesophageal Junction Adenocarcinoma on Long-Term Maintenance Chemotherapy With Trastuzumab Alone: An Unusual Occurrence. Cureus 2020, 12, e11472. [Google Scholar] [CrossRef] [PubMed]
- Porth, I.; Hirsch, D.; Ceribas, Y.; Weidner, P.; Weichert, W.; Götze, T.O.; Perner, S.; Luley, K.; Heyer, C.M.; de la Torre, C.; et al. Comprehensive Biomarker Analysis of Long-Term Response to Trastuzumab in Patients with HER2-Positive Advanced Gastric or Gastroesophageal Adenocarcinoma. Eur. J. Cancer 2023, 183, 119–130. [Google Scholar] [CrossRef]
- Shah, M.A.; Xu, R.-H.; Bang, Y.-J.; Hoff, P.M.; Liu, T.; Herráez-Baranda, L.A.; Xia, F.; Garg, A.; Shing, M.; Tabernero, J. HELOISE: Phase IIIb Randomized Multicenter Study Comparing Standard-of-Care and Higher-Dose Trastuzumab Regimens Combined With Chemotherapy as First-Line Therapy in Patients With Human Epidermal Growth Factor Receptor 2-Positive Metastatic Gastric or Gastroesophageal Junction Adenocarcinoma. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2017, 35, 2558–2567. [Google Scholar] [CrossRef]
- Bergen, E.S.; Pilla, L.; Auclin, E.; Ilhan-Mutlu, A.; Prager, G.W.; Pietrantonio, F.; Antista, M.; Ghelardi, F.; Basile, D.; Aprile, G.; et al. Optimal Treatment Strategy after First-Line Induction Therapy in Advanced HER2-Positive Oeso-Gastric Adenocarcinoma—A Retrospective, International, Multicentric AGEO Study. Gastric Cancer 2023, 26, 425–437. [Google Scholar] [CrossRef]
- Lordick, F.; Carneiro, F.; Cascinu, S.; Fleitas, T.; Haustermans, K.; Piessen, G.; Vogel, A.; Smyth, E.C. Gastric Cancer: ESMO Clinical Practice Guideline for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2022, 33, 1005–1020. [Google Scholar] [CrossRef]
- Al-Batran, S.-E.; Moorahrend, E.; Maintz, C.; Goetze, T.O.; Hempel, D.; Thuss-Patience, P.; Gaillard, V.E.; Hegewisch-Becker, S. Clinical Practice Observation of Trastuzumab in Patients with Human Epidermal Growth Receptor 2-Positive Metastatic Adenocarcinoma of the Stomach or Gastroesophageal Junction. Oncologist 2020, 25, e1181–e1187. [Google Scholar] [CrossRef] [PubMed]
- Ter Veer, E.; Creemers, A.; De Waal, L.; Van Oijen, M.G.H.; Van Laarhoven, H.W.M. Comparing Cytotoxic Backbones for First-line Trastuzumab-containing Regimens in Human Epidermal Growth Factor Receptor 2-positive Advanced Oesophagogastric Cancer: A Meta-analysis. Int. J. Cancer 2018, 143, 438–448. [Google Scholar] [CrossRef]
- Janjigian, Y.Y.; Kawazoe, A.; Yañez, P.; Li, N.; Lonardi, S.; Kolesnik, O.; Barajas, O.; Bai, Y.; Shen, L.; Tang, Y.; et al. The KEYNOTE-811 Trial of Dual PD-1 and HER2 Blockade in HER2-Positive Gastric Cancer. Nature 2021, 600, 727–730. [Google Scholar] [CrossRef] [PubMed]
- Janjigian, Y.Y.; Kawazoe, A.; Bai, Y.; Xu, J.; Lonardi, S.; Metges, J.P.; Yanez, P.; Wyrwicz, L.S.; Shen, L.; Ostapenko, Y.; et al. Pembrolizumab plus Trastuzumab and Chemotherapy for HER2-Positive Gastric or Gastro-Oesophageal Junction Adenocarcinoma: Interim Analyses from the Phase 3 KEYNOTE-811 Randomised Placebo-Controlled Trial. Lancet 2023, 402, 2197–2208. [Google Scholar] [CrossRef] [PubMed]
- Janjigian, Y.Y.; Shitara, K.; Moehler, M.; Garrido, M.; Salman, P.; Shen, L.; Wyrwicz, L.; Yamaguchi, K.; Skoczylas, T.; Campos Bragagnoli, A.; et al. First-Line Nivolumab plus Chemotherapy versus Chemotherapy Alone for Advanced Gastric, Gastro-Oesophageal Junction, and Oesophageal Adenocarcinoma (CheckMate 649): A Randomised, Open-Label, Phase 3 Trial. Lancet 2021, 398, 27–40. [Google Scholar] [CrossRef]
- Makiyama, A.; Sukawa, Y.; Kashiwada, T.; Kawada, J.; Hosokawa, A.; Horie, Y.; Tsuji, A.; Moriwaki, T.; Tanioka, H.; Shinozaki, K.; et al. Randomized, Phase II Study of Trastuzumab Beyond Progression in Patients With HER2-Positive Advanced Gastric or Gastroesophageal Junction Cancer: WJOG7112G (T-ACT Study). J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2020, 38, 1919–1927. [Google Scholar] [CrossRef]
- Kim, C.G.; Jung, M.; Kim, H.S.; Lee, C.; Jeung, H.-C.; Koo, D.-H.; Bae, W.K.; Zang, D.Y.; Kim, B.J.; Kim, H.; et al. Trastuzumab Combined With Ramucirumab and Paclitaxel in Patients With Previously Treated Human Epidermal Growth Factor Receptor 2–Positive Advanced Gastric or Gastroesophageal Junction Cancer. J. Clin. Oncol. 2023, 41, 4394–4405. [Google Scholar] [CrossRef]
- Rha, S.Y.; Chung, H.C. Breakthroughs in the Systemic Treatment of HER2-Positive Advanced/Metastatic Gastric Cancer: From Singlet Chemotherapy to Triple Combination. J. Gastric Cancer 2023, 23, 224–249. [Google Scholar] [CrossRef]
- Ogitani, Y.; Aida, T.; Hagihara, K.; Yamaguchi, J.; Ishii, C.; Harada, N.; Soma, M.; Okamoto, H.; Oitate, M.; Arakawa, S.; et al. DS-8201a, A Novel HER2-Targeting ADC with a Novel DNA Topoisomerase I Inhibitor, Demonstrates a Promising Antitumor Efficacy with Differentiation from T-DM1. Clin. Cancer Res. 2016, 22, 5097–5108. [Google Scholar] [CrossRef]
- Ogitani, Y.; Hagihara, K.; Oitate, M.; Naito, H.; Agatsuma, T. Bystander Killing Effect of DS -8201a, a Novel Anti-human Epidermal Growth Factor Receptor 2 Antibody–Drug Conjugate, in Tumors with Human Epidermal Growth Factor Receptor 2 Heterogeneity. Cancer Sci. 2016, 107, 1039–1046. [Google Scholar] [CrossRef]
- Takegawa, N.; Tsurutani, J.; Kawakami, H.; Yonesaka, K.; Kato, R.; Haratani, K.; Hayashi, H.; Takeda, M.; Nonagase, Y.; Maenishi, O.; et al. [Fam-] Trastuzumab Deruxtecan, Antitumor Activity Is Dependent on HER2 Expression Level Rather than on HER2 Amplification. Int. J. Cancer 2019, 145, 3414–3424. [Google Scholar] [CrossRef] [PubMed]
- Gennari, A.; André, F.; Barrios, C.H.; Cortés, J.; de Azambuja, E.; DeMichele, A.; Dent, R.; Fenlon, D.; Gligorov, J.; Hurvitz, S.A.; et al. ESMO Clinical Practice Guideline for the Diagnosis, Staging and Treatment of Patients with Metastatic Breast Cancer. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2021, 32, 1475–1495. [Google Scholar] [CrossRef] [PubMed]
- Shitara, K.; Bang, Y.-J.; Iwasa, S.; Sugimoto, N.; Ryu, M.-H.; Sakai, D.; Chung, H.-C.; Kawakami, H.; Yabusaki, H.; Lee, J.; et al. Trastuzumab Deruxtecan in Previously Treated HER2-Positive Gastric Cancer. N. Engl. J. Med. 2020, 382, 2419–2430. [Google Scholar] [CrossRef]
- Van Cutsem, E.; Di Bartolomeo, M.; Smyth, E.; Chau, I.; Park, H.; Siena, S.; Lonardi, S.; Wainberg, Z.A.; Ajani, J.; Chao, J.; et al. Trastuzumab Deruxtecan in Patients in the USA and Europe with HER2-Positive Advanced Gastric or Gastroesophageal Junction Cancer with Disease Progression on or after a Trastuzumab-Containing Regimen (DESTINY-Gastric02): Primary and Updated Analyses from a Single-Arm, Phase 2 Study. Lancet Oncol. 2023, 24, 744–756. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) Antiemesis Version 1; NCCN: Plymouth Meeting, PA, USA, 2023. [Google Scholar]
- Modi, S.; Jacot, W.; Yamashita, T.; Sohn, J.; Vidal, M.; Tokunaga, E.; Tsurutani, J.; Ueno, N.T.; Prat, A.; Chae, Y.S.; et al. Trastuzumab Deruxtecan in Previously Treated HER2-Low Advanced Breast Cancer. N. Engl. J. Med. 2022, 387, 9–20. [Google Scholar] [CrossRef]
- Tarantino, P.; Viale, G.; Press, M.F.; Hu, X.; Penault-Llorca, F.; Bardia, A.; Batistatou, A.; Burstein, H.J.; Carey, L.A.; Cortes, J.; et al. ESMO Expert Consensus Statements (ECS) on the Definition, Diagnosis, and Management of HER2-Low Breast Cancer. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2023, 34, 645–659. [Google Scholar] [CrossRef]
- Yamaguchi, K.; Bang, Y.-J.; Iwasa, S.; Sugimoto, N.; Ryu, M.-H.; Sakai, D.; Chung, H.C.; Kawakami, H.; Yabusaki, H.; Lee, J.; et al. Trastuzumab Deruxtecan in Anti-Human Epidermal Growth Factor Receptor 2 Treatment-Naive Patients With Human Epidermal Growth Factor Receptor 2-Low Gastric or Gastroesophageal Junction Adenocarcinoma: Exploratory Cohort Results in a Phase II Trial. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2023, 41, 816–825. [Google Scholar] [CrossRef] [PubMed]
- Pályi-Krekk, Z.; Barok, M.; Isola, J.; Tammi, M.; Szöllosi, J.; Nagy, P. Hyaluronan-Induced Masking of ErbB2 and CD44-Enhanced Trastuzumab Internalisation in Trastuzumab Resistant Breast Cancer. Eur. J. Cancer 2007, 43, 2423–2433. [Google Scholar] [CrossRef]
- Pietrantonio, F.; Caporale, M.; Morano, F.; Scartozzi, M.; Gloghini, A.; De Vita, F.; Giommoni, E.; Fornaro, L.; Aprile, G.; Melisi, D.; et al. HER2 Loss in HER2-Positive Gastric or Gastroesophageal Cancer after Trastuzumab Therapy: Implication for Further Clinical Research. Int. J. Cancer 2016, 139, 2859–2864. [Google Scholar] [CrossRef]
- Saeki, H.; Oki, E.; Kashiwada, T.; Arigami, T.; Makiyama, A.; Iwatsuki, M.; Narita, Y.; Satake, H.; Matsuda, Y.; Sonoda, H.; et al. Re-Evaluation of HER2 Status in Patients with HER2-Positive Advanced or Recurrent Gastric Cancer Refractory to Trastuzumab (KSCC1604). Eur. J. Cancer 2018, 105, 41–49. [Google Scholar] [CrossRef]
- Seo, S.; Ryu, M.-H.; Park, Y.S.; Ahn, J.Y.; Park, Y.; Park, S.R.; Ryoo, B.-Y.; Lee, G.H.; Jung, H.-Y.; Kang, Y.-K. Loss of HER2 Positivity after Anti-HER2 Chemotherapy in HER2-Positive Gastric Cancer Patients: Results of the GASTric Cancer HER2 Reassessment Study 3 (GASTHER3). Gastric Cancer Off. J. Int. Gastric Cancer Assoc. Jpn. Gastric Cancer Assoc. 2019, 22, 527–535. [Google Scholar] [CrossRef] [PubMed]
- Janjigian, Y.Y.; Sanchez-Vega, F.; Jonsson, P.; Chatila, W.K.; Hechtman, J.F.; Ku, G.Y.; Riches, J.C.; Tuvy, Y.; Kundra, R.; Bouvier, N.; et al. Genetic Predictors of Response to Systemic Therapy in Esophagogastric Cancer. Cancer Discov. 2018, 8, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Ebbing, E.A.; Medema, J.P.; Damhofer, H.; Meijer, S.L.; Krishnadath, K.K.; van Berge Henegouwen, M.I.; Bijlsma, M.F.; van Laarhoven, H.W.M. ADAM10-Mediated Release of Heregulin Confers Resistance to Trastuzumab by Activating HER3. Oncotarget 2016, 7, 10243–10254. [Google Scholar] [CrossRef] [PubMed]
- Sampera, A.; Sánchez-Martín, F.J.; Arpí, O.; Visa, L.; Iglesias, M.; Menéndez, S.; Gaye, É.; Dalmases, A.; Clavé, S.; Gelabert-Baldrich, M.; et al. HER-Family Ligands Promote Acquired Resistance to Trastuzumab in Gastric Cancer. Mol. Cancer Ther. 2019, 18, 2135–2145. [Google Scholar] [CrossRef] [PubMed]
- Zuo, Q.; Liu, J.; Zhang, J.; Wu, M.; Guo, L.; Liao, W. Development of Trastuzumab-Resistant Human Gastric Carcinoma Cell Lines and Mechanisms of Drug Resistance. Sci. Rep. 2015, 5, 11634. [Google Scholar] [CrossRef]
- Piro, G.; Carbone, C.; Cataldo, I.; Di Nicolantonio, F.; Giacopuzzi, S.; Aprile, G.; Simionato, F.; Boschi, F.; Zanotto, M.; Mina, M.M.; et al. An FGFR3 Autocrine Loop Sustains Acquired Resistance to Trastuzumab in Gastric Cancer Patients. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2016, 22, 6164–6175. [Google Scholar] [CrossRef]
- Jin, M.H.; Nam, A.-R.; Park, J.E.; Bang, J.-H.; Bang, Y.-J.; Oh, D.-Y. Resistance Mechanism against Trastuzumab in HER2-Positive Cancer Cells and Its Negation by Src Inhibition. Mol. Cancer Ther. 2017, 16, 1145–1154. [Google Scholar] [CrossRef] [PubMed]
- Ha, S.Y.; Lee, J.; Jang, J.; Hong, J.Y.; Do, I.-G.; Park, S.H.; Park, J.O.; Choi, M.-G.; Sohn, T.S.; Bae, J.M.; et al. HER2-Positive Gastric Cancer with Concomitant MET and/or EGFR Overexpression: A Distinct Subset of Patients for Dual Inhibition Therapy. Int. J. Cancer 2015, 136, 1629–1635. [Google Scholar] [CrossRef] [PubMed]
- Ebbing, E.A.; Steins, A.; Fessler, E.; Stathi, P.; Lesterhuis, W.J.; Krishnadath, K.K.; Vermeulen, L.; Medema, J.P.; Bijlsma, M.F.; Van Laarhoven, H.W.M. Esophageal Adenocarcinoma Cells and Xenograft Tumors Exposed to Erb-B2 Receptor Tyrosine Kinase 2 and 3 Inhibitors Activate Transforming Growth Factor Beta Signaling, Which Induces Epithelial to Mesenchymal Transition. Gastroenterology 2017, 153, 63–76.e14. [Google Scholar] [CrossRef]
- Liu, W.; Chang, J.; Liu, M.; Yuan, J.; Zhang, J.; Qin, J.; Xia, X.; Wang, Y. Quantitative Proteomics Profiling Reveals Activation of mTOR Pathway in Trastuzumab Resistance. Oncotarget 2017, 8, 45793–45806. [Google Scholar] [CrossRef]
- Sukawa, Y.; Yamamoto, H.; Nosho, K.; Kunimoto, H.; Suzuki, H.; Adachi, Y.; Nakazawa, M.; Nobuoka, T.; Kawayama, M.; Mikami, M.; et al. Alterations in the Human Epidermal Growth Factor Receptor 2-Phosphatidylinositol 3-Kinase-v-Akt Pathway in Gastric Cancer. World J. Gastroenterol. 2012, 18, 6577–6586. [Google Scholar] [CrossRef] [PubMed]
- Mezynski, M.J.; Farrelly, A.M.; Cremona, M.; Carr, A.; Morgan, C.; Workman, J.; Armstrong, P.; McAuley, J.; Madden, S.; Fay, J.; et al. Targeting the PI3K and MAPK Pathways to Improve Response to HER2-Targeted Therapies in HER2-Positive Gastric Cancer. J. Transl. Med. 2021, 19, 184. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.-S.; Liu, Z.-X.; Lu, Y.-X.; Bao, H.; Wu, X.; Zeng, Z.-L.; Liu, Z.; Zhao, Q.; He, C.-Y.; Lu, J.-H.; et al. Liquid Biopsies to Track Trastuzumab Resistance in Metastatic HER2-Positive Gastric Cancer. Gut 2019, 68, 1152–1161. [Google Scholar] [CrossRef] [PubMed]
- Deguchi, Y.; Okabe, H.; Oshima, N.; Hisamori, S.; Minamiguchi, S.; Muto, M.; Sakai, Y. PTEN Loss Is Associated with a Poor Response to Trastuzumab in HER2-Overexpressing Gastroesophageal Adenocarcinoma. Gastric Cancer Off. J. Int. Gastric Cancer Assoc. Jpn. Gastric Cancer Assoc. 2017, 20, 416–427. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.; Lee, C.-K.; Chon, H.J.; Kim, J.H.; Park, H.S.; Heo, S.J.; Kim, H.J.; Kim, T.S.; Kwon, W.S.; Chung, H.C.; et al. PTEN Loss and Level of HER2 Amplification Is Associated with Trastuzumab Resistance and Prognosis in HER2-Positive Gastric Cancer. Oncotarget 2017, 8, 113494–113501. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Pan, C.; Guo, L.; Wu, M.; Guo, J.; Peng, S.; Wu, Q.; Zuo, Q. A New Mechanism of Trastuzumab Resistance in Gastric Cancer: MACC1 Promotes the Warburg Effect via Activation of the PI3K/AKT Signaling Pathway. J. Hematol. Oncol. J. Hematol. Oncol. 2016, 9, 76. [Google Scholar] [CrossRef]
- Tang, L.; Long, Z.; Zhao, N.; Feng, G.; Guo, X.; Yu, M. NES1/KLK10 Promotes Trastuzumab Resistance via Activation of PI3K/AKT Signaling Pathway in Gastric Cancer. J. Cell. Biochem. 2018, 119, 6398–6407. [Google Scholar] [CrossRef]
- Yang, S.; Wang, B.; Liao, J.; Hong, Z.; Zhong, X.; Chen, S.; Wu, Z.; Zhang, X.; Zuo, Q. Molecular Mechanism of XB130 Adaptor Protein Mediates Trastuzumab Resistance in Gastric Cancer. Clin. Transl. Oncol. Off. Publ. Fed. Span. Oncol. Soc. Natl. Cancer Inst. Mex. 2023, 25, 685–695. [Google Scholar] [CrossRef]
- Sato, Y.; Yashiro, M.; Takakura, N. Heregulin Induces Resistance to Lapatinib-Mediated Growth Inhibition of HER2-Amplified Cancer Cells. Cancer Sci. 2013, 104, 1618–1625. [Google Scholar] [CrossRef]
- Nonagase, Y.; Yonesaka, K.; Kawakami, H.; Watanabe, S.; Haratani, K.; Takahama, T.; Takegawa, N.; Ueda, H.; Tanizaki, J.; Hayashi, H.; et al. Heregulin-Expressing HER2-Positive Breast and Gastric Cancer Exhibited Heterogeneous Susceptibility to the Anti-HER2 Agents Lapatinib, Trastuzumab and T-DM1. Oncotarget 2016, 7, 84860–84871. [Google Scholar] [CrossRef]
- Ohtsu, A.; Ajani, J.A.; Bai, Y.-X.; Bang, Y.-J.; Chung, H.-C.; Pan, H.-M.; Sahmoud, T.; Shen, L.; Yeh, K.-H.; Chin, K.; et al. Everolimus for Previously Treated Advanced Gastric Cancer: Results of the Randomized, Double-Blind, Phase III GRANITE-1 Study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2013, 31, 3935–3943. [Google Scholar] [CrossRef] [PubMed]
- Sun, S.-Y.; Rosenberg, L.M.; Wang, X.; Zhou, Z.; Yue, P.; Fu, H.; Khuri, F.R. Activation of Akt and eIF4E Survival Pathways by Rapamycin-Mediated Mammalian Target of Rapamycin Inhibition. Cancer Res. 2005, 65, 7052–7058. [Google Scholar] [CrossRef] [PubMed]
- Elster, N.; Cremona, M.; Morgan, C.; Toomey, S.; Carr, A.; O’Grady, A.; Hennessy, B.T.; Eustace, A.J. A Preclinical Evaluation of the PI3K Alpha/Delta Dominant Inhibitor BAY 80-6946 in HER2-Positive Breast Cancer Models with Acquired Resistance to the HER2-Targeted Therapies Trastuzumab and Lapatinib. Breast Cancer Res. Treat. 2015, 149, 373–383. [Google Scholar] [CrossRef]
- O’Shea, J.; Cremona, M.; Morgan, C.; Milewska, M.; Holmes, F.; Espina, V.; Liotta, L.; O’Shaughnessy, J.; Toomey, S.; Madden, S.F.; et al. A Preclinical Evaluation of the MEK Inhibitor Refametinib in HER2-Positive Breast Cancer Cell Lines Including Those with Acquired Resistance to Trastuzumab or Lapatinib. Oncotarget 2017, 8, 85120–85135. [Google Scholar] [CrossRef] [PubMed]
- Yao, X.; He, Z.; Qin, C.; Zhang, P.; Sui, C.; Deng, X.; Fang, Y.; Li, G.; Shi, J. Inhibition of PFKFB3 in HER2-Positive Gastric Cancer Improves Sensitivity to Trastuzumab by Inducing Tumour Vessel Normalisation. Br. J. Cancer 2022, 127, 811–823. [Google Scholar] [CrossRef]
- Hofmann, M.; Stoss, O.; Shi, D.; Büttner, R.; van de Vijver, M.; Kim, W.; Ochiai, A.; Rüschoff, J.; Henkel, T. Assessment of a HER2 Scoring System for Gastric Cancer: Results from a Validation Study. Histopathology 2008, 52, 797–805. [Google Scholar] [CrossRef]
- Rüschoff, J.; Dietel, M.; Baretton, G.; Arbogast, S.; Walch, A.; Monges, G.; Chenard, M.-P.; Penault-Llorca, F.; Nagelmeier, I.; Schlake, W.; et al. HER2 Diagnostics in Gastric Cancer-Guideline Validation and Development of Standardized Immunohistochemical Testing. Virchows Arch. Int. J. Pathol. 2010, 457, 299–307. [Google Scholar] [CrossRef]
- Wakatsuki, T.; Yamamoto, N.; Sano, T.; Chin, K.; Kawachi, H.; Takahari, D.; Ogura, M.; Ichimura, T.; Nakayama, I.; Osumi, H.; et al. Clinical Impact of Intratumoral HER2 Heterogeneity on Trastuzumab Efficacy in Patients with HER2-Positive Gastric Cancer. J. Gastroenterol. 2018, 53, 1186–1195. [Google Scholar] [CrossRef] [PubMed]
- Haffner, I.; Schierle, K.; Raimúndez, E.; Geier, B.; Maier, D.; Hasenauer, J.; Luber, B.; Walch, A.; Kolbe, K.; Riera Knorrenschild, J.; et al. HER2 Expression, Test Deviations, and Their Impact on Survival in Metastatic Gastric Cancer: Results From the Prospective Multicenter VARIANZ Study. J. Clin. Oncol. 2021, 39, 1468–1478. [Google Scholar] [CrossRef]
- Park, S.R.; Park, Y.S.; Ryu, M.-H.; Ryoo, B.-Y.; Woo, C.G.; Jung, H.-Y.; Lee, J.H.; Lee, G.H.; Kang, Y.-K. Extra-Gain of HER2-Positive Cases through HER2 Reassessment in Primary and Metastatic Sites in Advanced Gastric Cancer with Initially HER2-Negative Primary Tumours: Results of GASTric Cancer HER2 Reassessment Study 1 (GASTHER1). Eur. J. Cancer 2016, 53, 42–50. [Google Scholar] [CrossRef]
- Bang, K.; Cheon, J.; Park, Y.S.; Kim, H.-D.; Ryu, M.-H.; Park, Y.; Moon, M.; Lee, H.; Kang, Y.-K. Association between HER2 Heterogeneity and Clinical Outcomes of HER2-Positive Gastric Cancer Patients Treated with Trastuzumab. Gastric Cancer 2022, 25, 794–803. [Google Scholar] [CrossRef]
- Moehler, M.; Al-Batran, S.-E.; Andus, T.; Arends, J.; Arnold, D.; Baretton, G.; Bornschein, J.; Budach, W.; Daum, S.; Dietrich, C.; et al. S3-Leitlinie Magenkarzinom—Diagnostik und Therapie der Adenokarzinome des Magens und des ösophagogastralen Übergangs—Langversion 2.0. Z. Gastroenterol. 2019, 57, 1517–1632. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) Gastric Cancer Version 2; NCCN: Plymouth Meeting, PA, USA, 2023. [Google Scholar]
- Warneke, V.S.; Behrens, H.-M.; Böger, C.; Becker, T.; Lordick, F.; Ebert, M.P.A.; Röcken, C. Her2/Neu Testing in Gastric Cancer: Evaluating the Risk of Sampling Errors. Ann. Oncol. 2013, 24, 725–733. [Google Scholar] [CrossRef]
- Pectasides, E.; Stachler, M.D.; Derks, S.; Liu, Y.; Maron, S.; Islam, M.; Alpert, L.; Kwak, H.; Kindler, H.; Polite, B.; et al. Genomic Heterogeneity as a Barrier to Precision Medicine in Gastroesophageal Adenocarcinoma. Cancer Discov. 2018, 8, 37–48. [Google Scholar] [CrossRef]
- Sanchez-Vega, F.; Hechtman, J.F.; Castel, P.; Ku, G.Y.; Tuvy, Y.; Won, H.; Fong, C.J.; Bouvier, N.; Nanjangud, G.J.; Soong, J.; et al. EGFR and MET Amplifications Determine Response to HER2 Inhibition in ERBB2-Amplified Esophagogastric Cancer. Cancer Discov. 2019, 9, 199–209. [Google Scholar] [CrossRef] [PubMed]
- Maron, S.B.; Chase, L.M.; Lomnicki, S.; Kochanny, S.; Moore, K.L.; Joshi, S.S.; Landron, S.; Johnson, J.; Kiedrowski, L.A.; Nagy, R.J.; et al. Circulating Tumor DNA Sequencing Analysis of Gastroesophageal Adenocarcinoma. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2019, 25, 7098–7112. [Google Scholar] [CrossRef] [PubMed]
- Lumish, M.A.; Maron, S.B.; Paroder, V.; Chou, J.F.; Capanu, M.; Philemond, S.; O’Donoghue, J.A.; Schöder, H.; Lewis, J.S.; Lyashchenko, S.K.; et al. Noninvasive Assessment of Human Epidermal Growth Factor Receptor 2 (HER2) in Esophagogastric Cancer Using 89 Zr-Trastuzumab PET: A Pilot Study. J. Nucl. Med. 2023, 64, 724–730. [Google Scholar] [CrossRef] [PubMed]
- Maron, S.B.; Chatila, W.; Walch, H.; Chou, J.F.; Ceglia, N.; Ptashkin, R.; Do, R.K.G.; Paroder, V.; Pandit-Taskar, N.; Lewis, J.S.; et al. Determinants of Survival with Combined HER2 and PD-1 Blockade in Metastatic Esophagogastric Cancer. Clin. Cancer Res. 2023, 29, 3633–3640. [Google Scholar] [CrossRef] [PubMed]
- Tabernero, J.; Hoff, P.M.; Shen, L.; Ohtsu, A.; Shah, M.A.; Cheng, K.; Song, C.; Wu, H.; Eng-Wong, J.; Kim, K.; et al. Pertuzumab plus Trastuzumab and Chemotherapy for HER2-Positive Metastatic Gastric or Gastro-Oesophageal Junction Cancer (JACOB): Final Analysis of a Double-Blind, Randomised, Placebo-Controlled Phase 3 Study. Lancet Oncol. 2018, 19, 1372–1384. [Google Scholar] [CrossRef]
- Catenacci, D.V.T.; Kang, Y.-K.; Yoon, H.H.; Shim, B.Y.; Kim, S.T.; Oh, D.-Y.; Spira, A.I.; Ulahannan, S.V.; Avery, E.J.; Boland, P.M.; et al. Margetuximab with Retifanlimab as First-Line Therapy in HER2+/PD-L1+ Unresectable or Metastatic Gastroesophageal Adenocarcinoma: MAHOGANY Cohort A. ESMO Open 2022, 7, 100563. [Google Scholar] [CrossRef]
- Zhu, X.; Ding, Y.; Wang, Q.; Yang, G.; Zhou, L.; Wang, Q. HLX22, an Anti-HER-2 Monoclonal Antibody, in Patients with Advanced Solid Tumors Overexpressing Human Epidermal Growth Factor Receptor 2: An Open-Label, Dose-Escalation, Phase 1 Trial. Investig. New Drugs 2023, 41, 473–482. [Google Scholar] [CrossRef]
- Xu, J.; Ying, J.; Liu, R.; Wu, J.; Ye, F.; Xu, N.; Zhang, Y.; Zhao, R.; Xiang, X.; Wang, J.; et al. KN026 (Anti-HER2 Bispecific Antibody) in Patients with Previously Treated, Advanced HER2-Expressing Gastric or Gastroesophageal Junction Cancer. Eur. J. Cancer 2023, 178, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Weisser, N.E.; Sanches, M.; Escobar-Cabrera, E.; O’Toole, J.; Whalen, E.; Chan, P.W.Y.; Wickman, G.; Abraham, L.; Choi, K.; Harbourne, B.; et al. An Anti-HER2 Biparatopic Antibody That Induces Unique HER2 Clustering and Complement-Dependent Cytotoxicity. Nat. Commun. 2023, 14, 1394. [Google Scholar] [CrossRef]
- Ku, G.; Elimova, E.; Denlinger, C.S.; Mehta, R.; Lee, K.-W.; Iqbal, S.; Kang, Y.-K.; Oh, D.-Y.; Rha, S.Y.; Kim, Y.H.; et al. 1380P Phase (Ph) II Study of Zanidatamab + Chemotherapy (Chemo) in First-Line (1L) HER2 Expressing Gastroesophageal Adenocarcinoma (GEA). Ann. Oncol. 2021, 32, S1044–S1045. [Google Scholar] [CrossRef]
- Tabernero, J.; Shen, L.; Elimova, E.; Ku, G.; Liu, T.; Shitara, K.; Lin, X.; Boyken, L.; Li, H.; Grim, J.; et al. HERIZON-GEA-01: Zanidatamab + Chemo ± Tislelizumab for 1L Treatment of HER2-Positive Gastroesophageal Adenocarcinoma. Future Oncol. Lond. Engl. 2022, 18, 3255–3266. [Google Scholar] [CrossRef]
- Ku, G.; Piha-Paul, S.; Gupta, M.; Oh, D.; Kim, Y.; Lee, J.; Rha, S.; Kang, Y.; Díez García, M.; Fleitas Kanonnikoff, T.; et al. P-53 A Phase 2, Multi-Center, Open-Label Study of Cinrebafusp Alfa (PRS-343) in Patients with HER2-High and HER2-Low Gastric or Gastroesophageal Junction (GEJ) Adenocarcinoma. Ann. Oncol. 2022, 33, S265. [Google Scholar] [CrossRef]
- Thuss-Patience, P.C.; Shah, M.A.; Ohtsu, A.; Van Cutsem, E.; Ajani, J.A.; Castro, H.; Mansoor, W.; Chung, H.C.; Bodoky, G.; Shitara, K.; et al. Trastuzumab Emtansine versus Taxane Use for Previously Treated HER2-Positive Locally Advanced or Metastatic Gastric or Gastro-Oesophageal Junction Adenocarcinoma (GATSBY): An International Randomised, Open-Label, Adaptive, Phase 2/3 Study. Lancet Oncol. 2017, 18, 640–653. [Google Scholar] [CrossRef] [PubMed]
- Cortés, J.; Diéras, V.; Lorenzen, S.; Montemurro, F.; Riera-Knorrenschild, J.; Thuss-Patience, P.; Allegrini, G.; De Laurentiis, M.; Lohrisch, C.; Oravcová, E.; et al. Efficacy and Safety of Trastuzumab Emtansine Plus Capecitabine vs Trastuzumab Emtansine Alone in Patients with Previously Treated ERBB2 (HER2)-Positive Metastatic Breast Cancer: A Phase 1 and Randomized Phase 2 Trial. JAMA Oncol. 2020, 6, 1203–1209. [Google Scholar] [CrossRef]
- Peng, Z.; Liu, T.; Wei, J.; Wang, A.; He, Y.; Yang, L.; Zhang, X.; Fan, N.; Luo, S.; Li, Z.; et al. Efficacy and Safety of a Novel Anti-HER2 Therapeutic Antibody RC48 in Patients with HER2-Overexpressing, Locally Advanced or Metastatic Gastric or Gastroesophageal Junction Cancer: A Single-Arm Phase II Study. Cancer Commun. Lond. Engl. 2021, 41, 1173–1182. [Google Scholar] [CrossRef]
- Xu, Y.; Wang, Y.; Gong, J.; Zhang, X.; Peng, Z.; Sheng, X.; Mao, C.; Fan, Q.; Bai, Y.; Ba, Y.; et al. Phase I Study of the Recombinant Humanized Anti-HER2 Monoclonal Antibody-MMAE Conjugate RC48-ADC in Patients with HER2-Positive Advanced Solid Tumors. Gastric Cancer Off. J. Int. Gastric Cancer Assoc. Jpn. Gastric Cancer Assoc. 2021, 24, 913–925. [Google Scholar] [CrossRef]
- Geyer, C.E.; Forster, J.; Lindquist, D.; Chan, S.; Romieu, C.G.; Pienkowski, T.; Jagiello-Gruszfeld, A.; Crown, J.; Chan, A.; Kaufman, B.; et al. Lapatinib plus Capecitabine for HER2-Positive Advanced Breast Cancer. N. Engl. J. Med. 2006, 355, 2733–2743. [Google Scholar] [CrossRef]
- Baselga, J.; Bradbury, I.; Eidtmann, H.; Di Cosimo, S.; de Azambuja, E.; Aura, C.; Gómez, H.; Dinh, P.; Fauria, K.; Van Dooren, V.; et al. Lapatinib with Trastuzumab for HER2-Positive Early Breast Cancer (NeoALTTO): A Randomised, Open-Label, Multicentre, Phase 3 Trial. Lancet Lond. Engl. 2012, 379, 633–640. [Google Scholar] [CrossRef] [PubMed]
- Blackwell, K.L.; Burstein, H.J.; Storniolo, A.M.; Rugo, H.S.; Sledge, G.; Aktan, G.; Ellis, C.; Florance, A.; Vukelja, S.; Bischoff, J.; et al. Overall Survival Benefit with Lapatinib in Combination with Trastuzumab for Patients with Human Epidermal Growth Factor Receptor 2-Positive Metastatic Breast Cancer: Final Results from the EGF104900 Study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2012, 30, 2585–2592. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.W.; Kim, H.-P.; Im, S.-A.; Kang, S.; Hur, H.S.; Yoon, Y.-K.; Oh, D.-Y.; Kim, J.H.; Lee, D.S.; Kim, T.-Y.; et al. The Growth Inhibitory Effect of Lapatinib, a Dual Inhibitor of EGFR and HER2 Tyrosine Kinase, in Gastric Cancer Cell Lines. Cancer Lett. 2008, 272, 296–306. [Google Scholar] [CrossRef] [PubMed]
- Spector, N.L.; Xia, W.; Burris, H.; Hurwitz, H.; Dees, E.C.; Dowlati, A.; O’Neil, B.; Overmoyer, B.; Marcom, P.K.; Blackwell, K.L.; et al. Study of the Biologic Effects of Lapatinib, a Reversible Inhibitor of ErbB1 and ErbB2 Tyrosine Kinases, on Tumor Growth and Survival Pathways in Patients with Advanced Malignancies. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2005, 23, 2502–2512. [Google Scholar] [CrossRef] [PubMed]
- Nahta, R.; Yuan, L.X.H.; Du, Y.; Esteva, F.J. Lapatinib Induces Apoptosis in Trastuzumab-Resistant Breast Cancer Cells: Effects on Insulin-like Growth Factor I Signaling. Mol. Cancer Ther. 2007, 6, 667–674. [Google Scholar] [CrossRef]
- Hecht, J.R.; Bang, Y.-J.; Qin, S.K.; Chung, H.C.; Xu, J.M.; Park, J.O.; Jeziorski, K.; Shparyk, Y.; Hoff, P.M.; Sobrero, A.; et al. Lapatinib in Combination with Capecitabine Plus Oxaliplatin in Human Epidermal Growth Factor Receptor 2–Positive Advanced or Metastatic Gastric, Esophageal, or Gastroesophageal Adenocarcinoma: TRIO-013/LOGiC—A Randomized Phase III Trial. J. Clin. Oncol. 2016, 34, 443–451. [Google Scholar] [CrossRef]
- Satoh, T.; Xu, R.-H.; Chung, H.C.; Sun, G.-P.; Doi, T.; Xu, J.-M.; Tsuji, A.; Omuro, Y.; Li, J.; Wang, J.-W.; et al. Lapatinib Plus Paclitaxel Versus Paclitaxel Alone in the Second-Line Treatment of HER2 -Amplified Advanced Gastric Cancer in Asian Populations: TyTAN—A Randomized, Phase III Study. J. Clin. Oncol. 2014, 32, 2039–2049. [Google Scholar] [CrossRef]
- Lorenzen, S.; Riera Knorrenschild, J.; Haag, G.-M.; Pohl, M.; Thuss-Patience, P.; Bassermann, F.; Helbig, U.; Weißinger, F.; Schnoy, E.; Becker, K.; et al. Lapatinib versus Lapatinib plus Capecitabine as Second-Line Treatment in Human Epidermal Growth Factor Receptor 2-Amplified Metastatic Gastro-Oesophageal Cancer: A Randomised Phase II Trial of the Arbeitsgemeinschaft Internistische Onkologie. Eur. J. Cancer 2015, 51, 569–576. [Google Scholar] [CrossRef]
- Kim, S.T.; Banks, K.C.; Pectasides, E.; Kim, S.Y.; Kim, K.; Lanman, R.B.; Talasaz, A.; An, J.; Choi, M.G.; Lee, J.H.; et al. Impact of Genomic Alterations on Lapatinib Treatment Outcome and Cell-Free Genomic Landscape during HER2 Therapy in HER2+ Gastric Cancer Patients. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2018, 29, 1037–1048. [Google Scholar] [CrossRef]
- Leto, S.M.; Sassi, F.; Catalano, I.; Torri, V.; Migliardi, G.; Zanella, E.R.; Throsby, M.; Bertotti, A.; Trusolino, L. Sustained Inhibition of HER3 and EGFR Is Necessary to Induce Regression of HER2-Amplified Gastrointestinal Carcinomas. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2015, 21, 5519–5531. [Google Scholar] [CrossRef] [PubMed]
- Wainberg, Z.A.; Anghel, A.; Desai, A.J.; Ayala, R.; Luo, T.; Safran, B.; Fejzo, M.S.; Hecht, J.R.; Slamon, D.J.; Finn, R.S. Lapatinib, a Dual EGFR and HER2 Kinase Inhibitor, Selectively Inhibits HER2-Amplified Human Gastric Cancer Cells and Is Synergistic with Trastuzumab in Vitro and in Vivo. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2010, 16, 1509–1519. [Google Scholar] [CrossRef] [PubMed]
- Zarkavelis, G.; Samantas, E.; Koliou, G.-A.; Papadopoulou, K.; Mauri, D.; Aravantinos, G.; Batistatou, A.; Pazarli, E.; Tryfonopoulos, D.; Tsipoura, A.; et al. AGAPP: Efficacy of First-Line Cisplatin, 5-Fluorouracil with Afatinib in Inoperable Gastric and Gastroesophageal Junction Carcinomas. A Hellenic Cooperative Oncology Group Study. Acta Oncol. Stockh. Swed. 2021, 60, 785–793. [Google Scholar] [CrossRef] [PubMed]
- Kulukian, A.; Lee, P.; Taylor, J.; Rosler, R.; de Vries, P.; Watson, D.; Forero-Torres, A.; Peterson, S. Preclinical Activity of HER2-Selective Tyrosine Kinase Inhibitor Tucatinib as a Single Agent or in Combination with Trastuzumab or Docetaxel in Solid Tumor Models. Mol. Cancer Ther. 2020, 19, 976–987. [Google Scholar] [CrossRef] [PubMed]
- Strickler, J.H.; Cercek, A.; Siena, S.; André, T.; Ng, K.; Van Cutsem, E.; Wu, C.; Paulson, A.S.; Hubbard, J.M.; Coveler, A.L.; et al. Tucatinib plus Trastuzumab for Chemotherapy-Refractory, HER2-Positive, RAS Wild-Type Unresectable or Metastatic Colorectal Cancer (MOUNTAINEER): A Multicentre, Open-Label, Phase 2 Study. Lancet Oncol. 2023, 24, 496–508. [Google Scholar] [CrossRef] [PubMed]
- Catenacci, D.V.T.; Strickler, J.H.; Nakamura, Y.; Shitara, K.; Janjigian, Y.Y.; Barzi, A.; Bekaii-Saab, T.S.; Lenz, H.-J.; Chung, H.C.C.; Tabernero, J.; et al. MOUNTAINEER-02: Phase 2/3 Study of Tucatinib, Trastuzumab, Ramucirumab, and Paclitaxel in Previously Treated HER2+ Gastric or Gastroesophageal Junction Adenocarcinoma—Trial in Progress. J. Clin. Oncol. 2022, 40, TPS371. [Google Scholar] [CrossRef]
- Marofi, F.; Motavalli, R.; Safonov, V.A.; Thangavelu, L.; Yumashev, A.V.; Alexander, M.; Shomali, N.; Chartrand, M.S.; Pathak, Y.; Jarahian, M.; et al. CAR T Cells in Solid Tumors: Challenges and Opportunities. Stem Cell Res. Ther. 2021, 12, 81. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Tong, C.; Wang, Y.; Gao, Y.; Dai, H.; Guo, Y.; Zhao, X.; Wang, Y.; Wang, Z.; Han, W.; et al. Effective and Persistent Antitumor Activity of HER2-Directed CAR-T Cells against Gastric Cancer Cells in Vitro and Xenotransplanted Tumors in Vivo. Protein Cell 2018, 9, 867–878. [Google Scholar] [CrossRef] [PubMed]
- Helsen, C.W.; Hammill, J.A.; Lau, V.W.C.; Mwawasi, K.A.; Afsahi, A.; Bezverbnaya, K.; Newhook, L.; Hayes, D.L.; Aarts, C.; Bojovic, B.; et al. The Chimeric TAC Receptor Co-Opts the T Cell Receptor Yielding Robust Anti-Tumor Activity without Toxicity. Nat. Commun. 2018, 9, 3049. [Google Scholar] [CrossRef]
- Schlechter, B.L.; Olson, D.; George, M.A.; Saibil, S.; Giordano, A.; Bouvier, R.; Gavriliuc, M.; Pieke, B.; Gruber, K.; Lichtenstein, E.; et al. A Phase I/II Trial Investigating Safety and Efficacy of Autologous TAC01-HER2 in Relapsed or Refractory Solid Tumors. J. Clin. Oncol. 2023, 41, 2519. [Google Scholar] [CrossRef]
- Eralp, Y.; Ates, U. Clinical Applications of Combined Immunotherapy Approaches in Gastrointestinal Cancer: A Case-Based Review. Vaccines 2023, 11, 1545. [Google Scholar] [CrossRef]
- Wiedermann, U.; Garner-Spitzer, E.; Chao, Y.; Maglakelidze, M.; Bulat, I.; Dechaphunkul, A.; Arpornwirat, W.; Charoentum, C.; Yen, C.-J.; Yau, T.C.; et al. Clinical and Immunologic Responses to a B-Cell Epitope Vaccine in Patients with HER2/Neu-Overexpressing Advanced Gastric Cancer—Results from Phase Ib Trial IMU.ACS.001. Clin. Cancer Res. 2021, 27, 3649–3660. [Google Scholar] [CrossRef]
- Maglakelidze, M.; Ryspayeva, D.E.; Andric, Z.; Petrovic, Z.; Bulat, I.; Nikolic, I.; Nagarkar, R.; Wiedermann, U.; Blumenstein, B.A.; Chong, L.M.O.; et al. HERIZON: A Phase 2 Study of HER-Vaxx (IMU-131), a HER2-Targeting Peptide Vaccine, plus Standard of Care Chemotherapy in Patients with HER2-Overexpressing Metastatic or Advanced Gastric/GEJ Adenocarcinoma—Overall Survival Analysis. J. Clin. Oncol. 2023, 41, 289. [Google Scholar] [CrossRef]
- Jung, M.; Lee, J.B.; Kim, H.S.; Kwon, W.S.; Kim, H.O.; Kim, S.; Park, M.; Kim, W.; Choi, K.-Y.; Oh, T.; et al. First-in-Human Phase 1 Study of a B Cell– and Monocyte-Based Immunotherapeutic Vaccine against HER2-Positive Advanced Gastric Cancer. Cancer Res. Treat. 2024, 56, 208–218. [Google Scholar] [CrossRef] [PubMed]
- Kauder, S.E.; Kuo, T.C.; Harrabi, O.; Chen, A.; Sangalang, E.; Doyle, L.; Rocha, S.S.; Bollini, S.; Han, B.; Sim, J.; et al. ALX148 Blocks CD47 and Enhances Innate and Adaptive Antitumor Immunity with a Favorable Safety Profile. PLoS ONE 2018, 13, e0201832. [Google Scholar] [CrossRef]
- Lakhani, N.J.; Chow, L.Q.M.; Gainor, J.F.; LoRusso, P.; Lee, K.-W.; Chung, H.C.; Lee, J.; Bang, Y.-J.; Hodi, F.S.; Kim, W.S.; et al. Evorpacept Alone and in Combination with Pembrolizumab or Trastuzumab in Patients with Advanced Solid Tumours (ASPEN-01): A First-in-Human, Open-Label, Multicentre, Phase 1 Dose-Escalation and Dose-Expansion Study. Lancet Oncol. 2021, 22, 1740–1751. [Google Scholar] [CrossRef]
- D’Huyvetter, M.; Vos, J.D.; Caveliers, V.; Vaneycken, I.; Heemskerk, J.; Duhoux, F.P.; Fontaine, C.; Vanhoeij, M.; Windhorst, A.D.; van der Aa, F.; et al. Phase I Trial of 131I-GMIB-Anti-HER2-VHH1, a New Promising Candidate for HER2-Targeted Radionuclide Therapy in Breast Cancer Patients. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2021, 62, 1097–1105. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Kang, S.K.; Kwon, W.S.; Jeong, I.; Kim, T.S.; Yu, S.Y.; Cho, S.W.; Chung, H.C.; Rha, S.Y. Novel HER2-Targeted Therapy to Overcome Trastuzumab Resistance in HER2-Amplified Gastric Cancer. Sci. Rep. 2023, 13, 22648. [Google Scholar] [CrossRef] [PubMed]
- Al-Batran, S.-E.; Hofheinz, R.D.; Pauligk, C.; Kopp, H.-G.; Haag, G.M.; Luley, K.B.; Meiler, J.; Homann, N.; Lorenzen, S.; Schmalenberg, H.; et al. Histopathological Regression after Neoadjuvant Docetaxel, Oxaliplatin, Fluorouracil, and Leucovorin versus Epirubicin, Cisplatin, and Fluorouracil or Capecitabine in Patients with Resectable Gastric or Gastro-Oesophageal Junction Adenocarcinoma (FLOT4-AIO): Results from the Phase 2 Part of a Multicentre, Open-Label, Randomised Phase 2/3 Trial. Lancet Oncol. 2016, 17, 1697–1708. [Google Scholar] [CrossRef]
- Al-Batran, S.-E.; Homann, N.; Pauligk, C.; Goetze, T.O.; Meiler, J.; Kasper, S.; Kopp, H.-G.; Mayer, F.; Haag, G.M.; Luley, K.; et al. Perioperative Chemotherapy with Fluorouracil plus Leucovorin, Oxaliplatin, and Docetaxel versus Fluorouracil or Capecitabine plus Cisplatin and Epirubicin for Locally Advanced, Resectable Gastric or Gastro-Oesophageal Junction Adenocarcinoma (FLOT4): A Randomised, Phase 2/3 Trial. Lancet 2019, 393, 1948–1957. [Google Scholar] [CrossRef]
- Hofheinz, R.; Hegewisch-Becker, S.; Kunzmann, V.; Thuss-Patience, P.; Fuchs, M.; Homann, N.; Graeven, U.; Schulte, N.; Merx, K.; Pohl, M.; et al. Trastuzumab in Combination with 5-fluorouracil, Leucovorin, Oxaliplatin and Docetaxel as Perioperative Treatment for Patients with Human Epidermal Growth Factor Receptor 2-positive Locally Advanced Esophagogastric Adenocarcinoma: A Phase II Trial of the Arbeitsgemeinschaft Internistische Onkologie Gastric Cancer Study Group. Int. J. Cancer 2021, 149, 1322–1331. [Google Scholar] [CrossRef] [PubMed]
- Lorenzen, S.; Thuss-Patience, P.; Al-Batran, S.E.; Lordick, F.; Haller, B.; Schuster, T.; Pauligk, C.; Luley, K.; Bichev, D.; Schumacher, G.; et al. Impact of Pathologic Complete Response on Disease-Free Survival in Patients with Esophagogastric Adenocarcinoma Receiving Preoperative Docetaxel-Based Chemotherapy. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2013, 24, 2068–2073. [Google Scholar] [CrossRef] [PubMed]
- Blum Murphy, M.; Xiao, L.; Patel, V.R.; Maru, D.M.; Correa, A.M.; G Amlashi, F.; Liao, Z.; Komaki, R.; Lin, S.H.; Skinner, H.D.; et al. Pathological Complete Response in Patients with Esophageal Cancer after the Trimodality Approach: The Association with Baseline Variables and Survival-The University of Texas MD Anderson Cancer Center Experience. Cancer 2017, 123, 4106–4113. [Google Scholar] [CrossRef] [PubMed]
- Soror, T.; Kho, G.; Zhao, K.-L.; Ismail, M.; Badakhshi, H. Impact of Pathological Complete Response Following Neoadjuvant Chemoradiotherapy in Esophageal Cancer. J. Thorac. Dis. 2018, 10, 4069–4076. [Google Scholar] [CrossRef] [PubMed]
- Al-Batran, S.-E.; Haag, G.M.; Ettrich, T.J.; Borchert, K.; Kretzschmar, A.; Teschendorf, C.; Siegler, G.M.; Ebert, M.; Goekkurt, E.; Welslau, M.K.; et al. 1421MO Final Results and Subgroup Analysis of the PETRARCA Randomized Phase II AIO Trial: Perioperative Trastuzumab and Pertuzumab in Combination with FLOT versus FLOT Alone for HER2 Positive Resectable Esophagogastric Adenocarcinoma. Ann. Oncol. 2020, 31, S899. [Google Scholar] [CrossRef]
- Wagner, A.D.; Grabsch, H.I.; Mauer, M.; Fumagalli Romario, U.; Kang, Y.-K.; Bouche, O.; Lorenzen, S.; Moehler, M.H.; Thuss-Patience, P.C.; Elme, A.; et al. Integration of Trastuzumab (T), with or without Pertuzumab (P), into Perioperative Chemotherapy (CT) of HER-2 Positive Gastric (GC) and Esophagogastric Junction Cancer (EGJC): First Results of the EORTC 1203 INNOVATION Study, in Collaboration with the Korean Cancer Study Group, and the Dutch Upper GI Cancer Group. J. Clin. Oncol. 2023, 41, 4057. [Google Scholar] [CrossRef]
- Wang, F.-H.; Zhang, X.-T.; Li, Y.-F.; Tang, L.; Qu, X.-J.; Ying, J.-E.; Zhang, J.; Sun, L.-Y.; Lin, R.-B.; Qiu, H.; et al. The Chinese Society of Clinical Oncology (CSCO): Clinical Guidelines for the Diagnosis and Treatment of Gastric Cancer, 2021. Cancer Commun. Lond. Engl. 2021, 41, 747–795. [Google Scholar] [CrossRef] [PubMed]
- Japanese Gastric Cancer Association Japanese Gastric Cancer Treatment Guidelines 2021 (6th Edition). Gastric Cancer Off. J. Int. Gastric Cancer Assoc. Jpn. Gastric Cancer Assoc. 2023, 26, 1–25. [CrossRef]
- Tokunaga, M.; Machida, N.; Mizusawa, J.; Yabusaki, H.; Yasui, H.; Hirao, M.; Watanabe, M.; Yasuda, T.; Kinoshita, T.; Imamura, H.; et al. A Randomized Phase II Trial of Preoperative Chemotherapy of S-1/CDDP with or without Trastuzumab Followed by Surgery in HER2 Positive Advanced Gastric or Esophagogastric Junction Adenocarcinoma with Extensive Lymph Node Metastasis: Japan Clinical Oncology Group Study JCOG1301C (Trigger Study). J. Clin. Oncol. 2022, 40, 285. [Google Scholar] [CrossRef]
- Shitara, K.; Lordick, F.; Bang, Y.-J.; Enzinger, P.C.; Ilson, D.H.; Shah, M.A.; Van Cutsem, E.; Xu, R.; Aprile, G.; Xu, J.; et al. Zolbetuximab + mFOLFOX6 as First-Line (1L) Treatment for Patients (Pts) Withclaudin-18.2+ (CLDN18.2+)/HER2− Locally Advanced (LA) Unresectable or Metastatic Gastric or Gastroesophageal Junction (mG/GEJ) Adenocarcinoma: Primary Results from Phase 3 SPOTLIGHT Study. J. Clin. Oncol. 2023, 41, LBA292. [Google Scholar] [CrossRef]
- Lordick, F.; Shah, M.A.; Shitara, K.; Ajani, J.A.; Bang, Y.-J.; Enzinger, P.C.; Ilson, D.H.; Van Cutsem, E.; Gallego Plazas, J.; Huang, J.; et al. 134MO Updated Efficacy and Safety Results from Phase III GLOW Study Evaluating Zolbetuximab + CAPOX as First-Line (1L) Treatment for Patients with Claudin-18 Isoform 2-Positive (CLDN18.2+), HER2−, Locally Advanced (LA) Unresectable or Metastatic Gastric or Gastroesophageal Junction (mG/GEJ) Adenocarcinoma. Ann. Oncol. 2023, 34, S1524. [Google Scholar] [CrossRef]
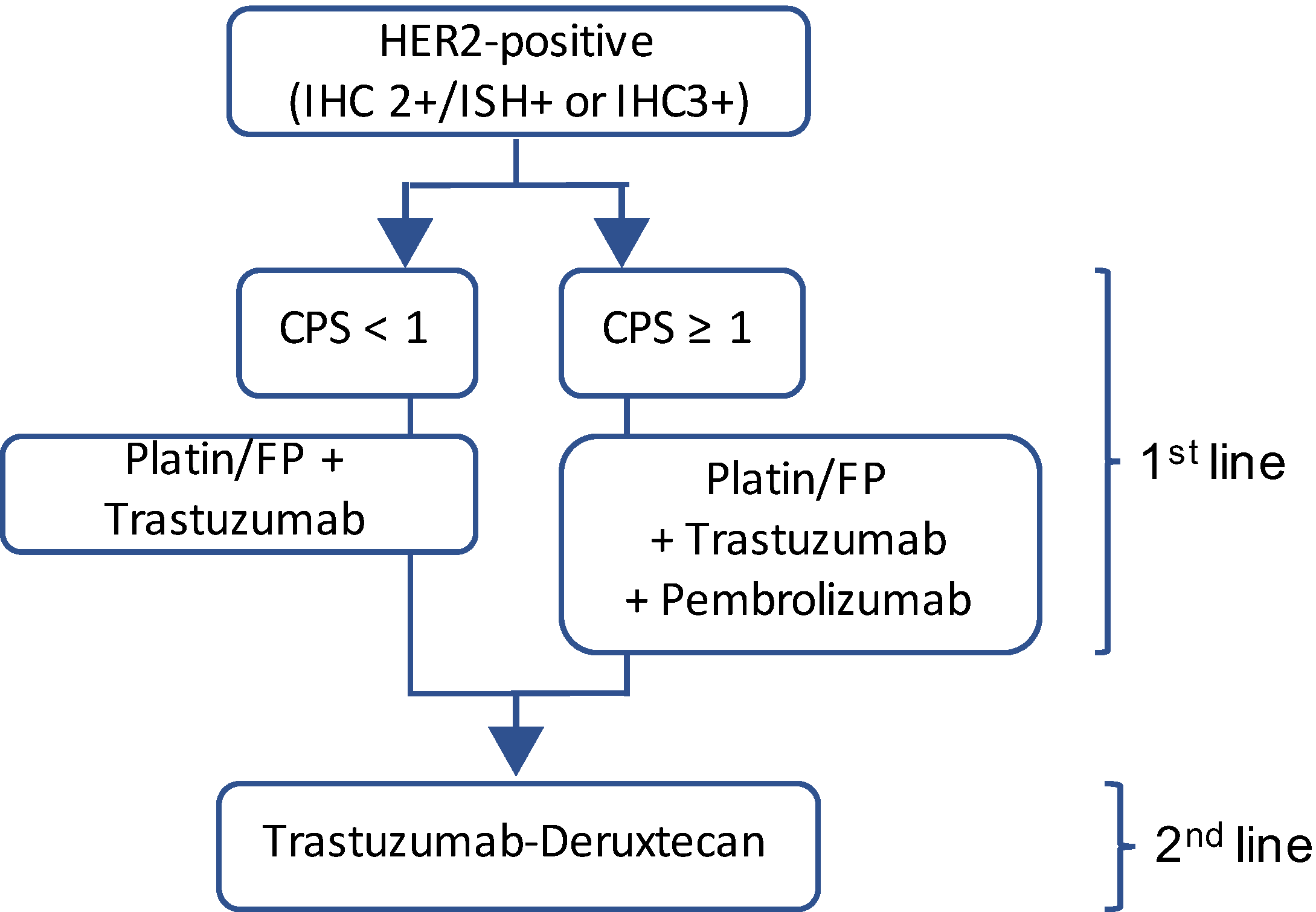
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).