
Early Serum Markers for Immune Checkpoint Inhibitor Induced Hypophysitis in Melanoma Patients


Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Patient Selection and Clinical Data Collection
2.2. Statistical Analysis
3. Results
3.1. Patient Characteristics
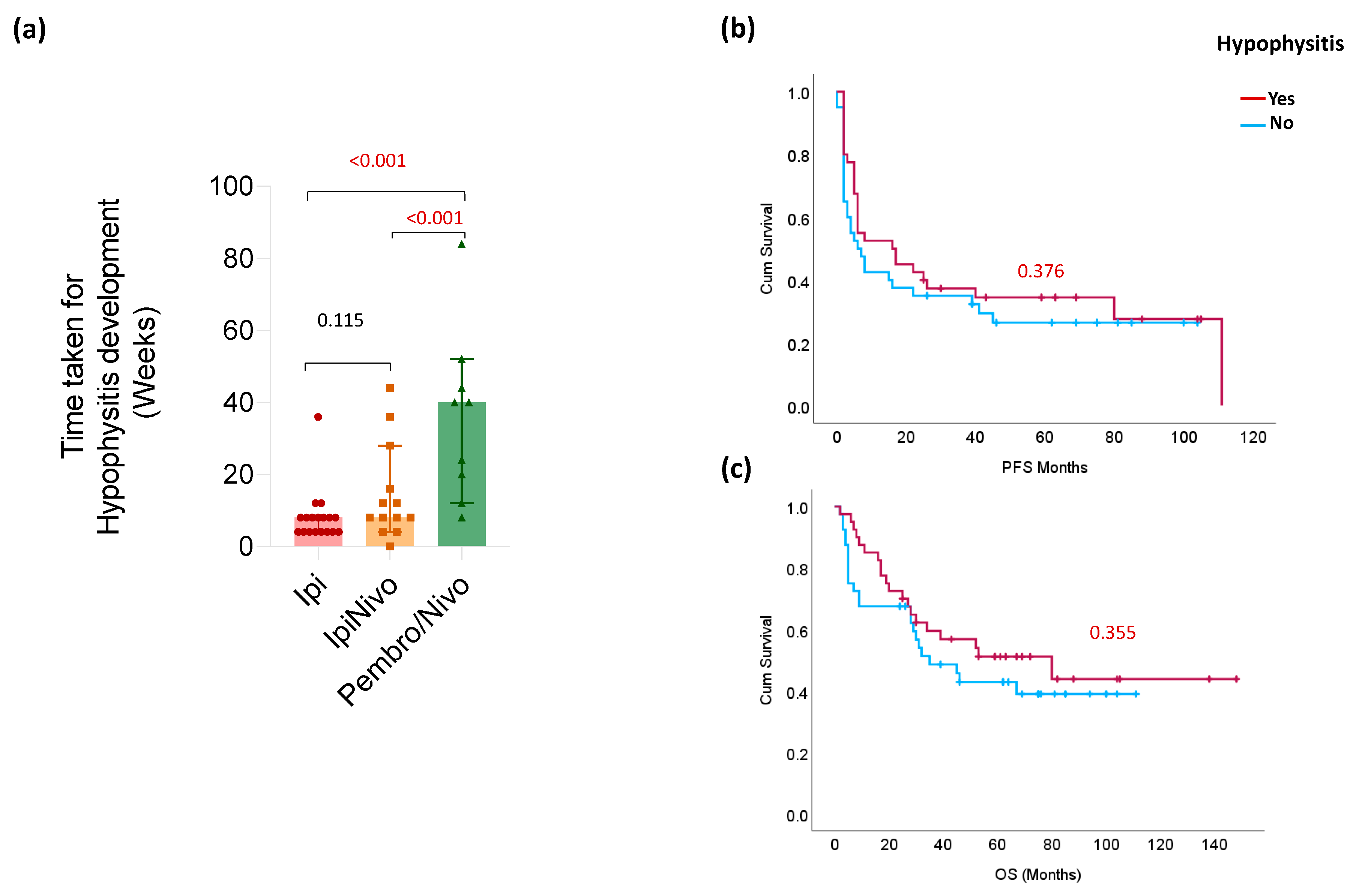
3.2. Clinical Characteristics of Ir-hypophysitis
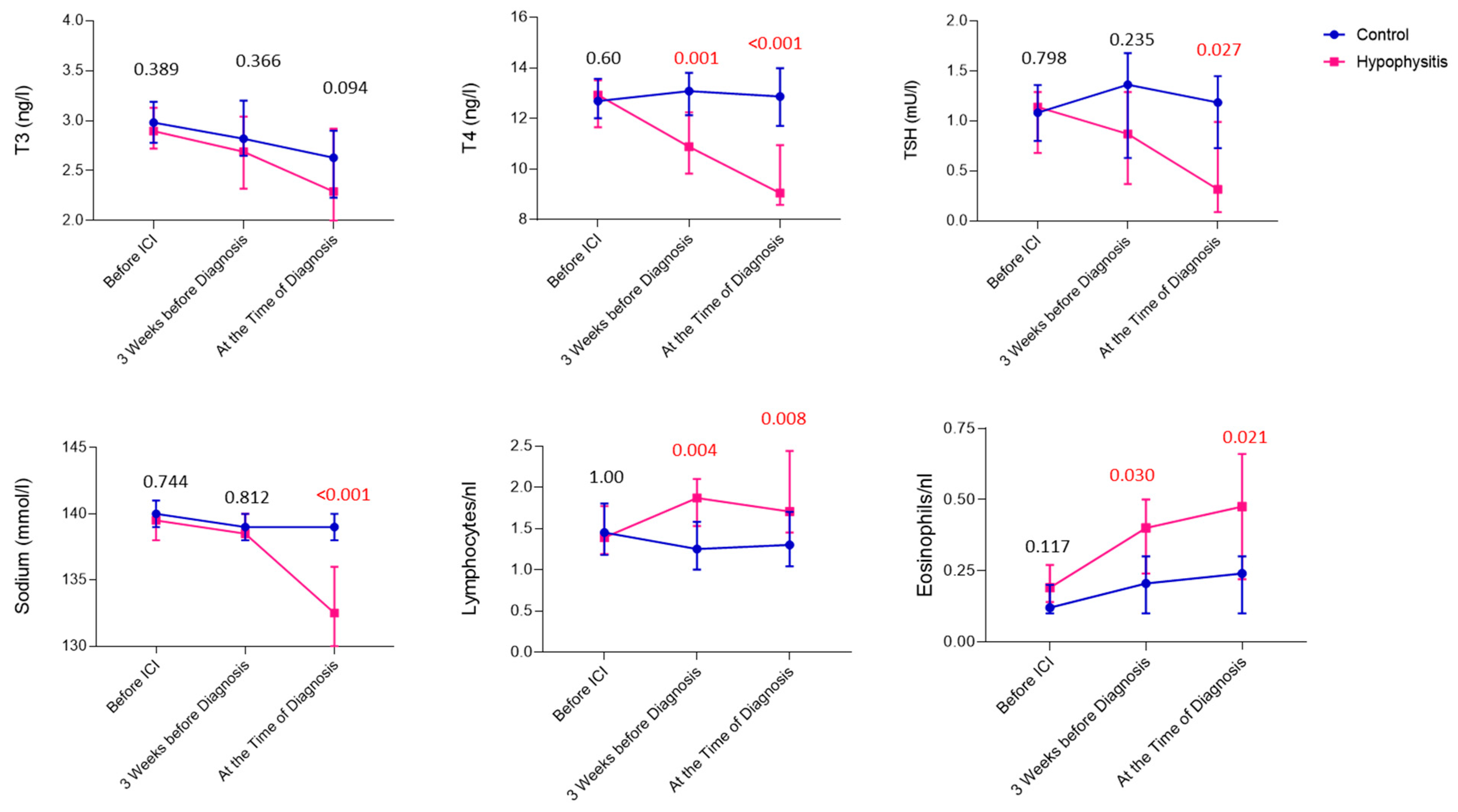
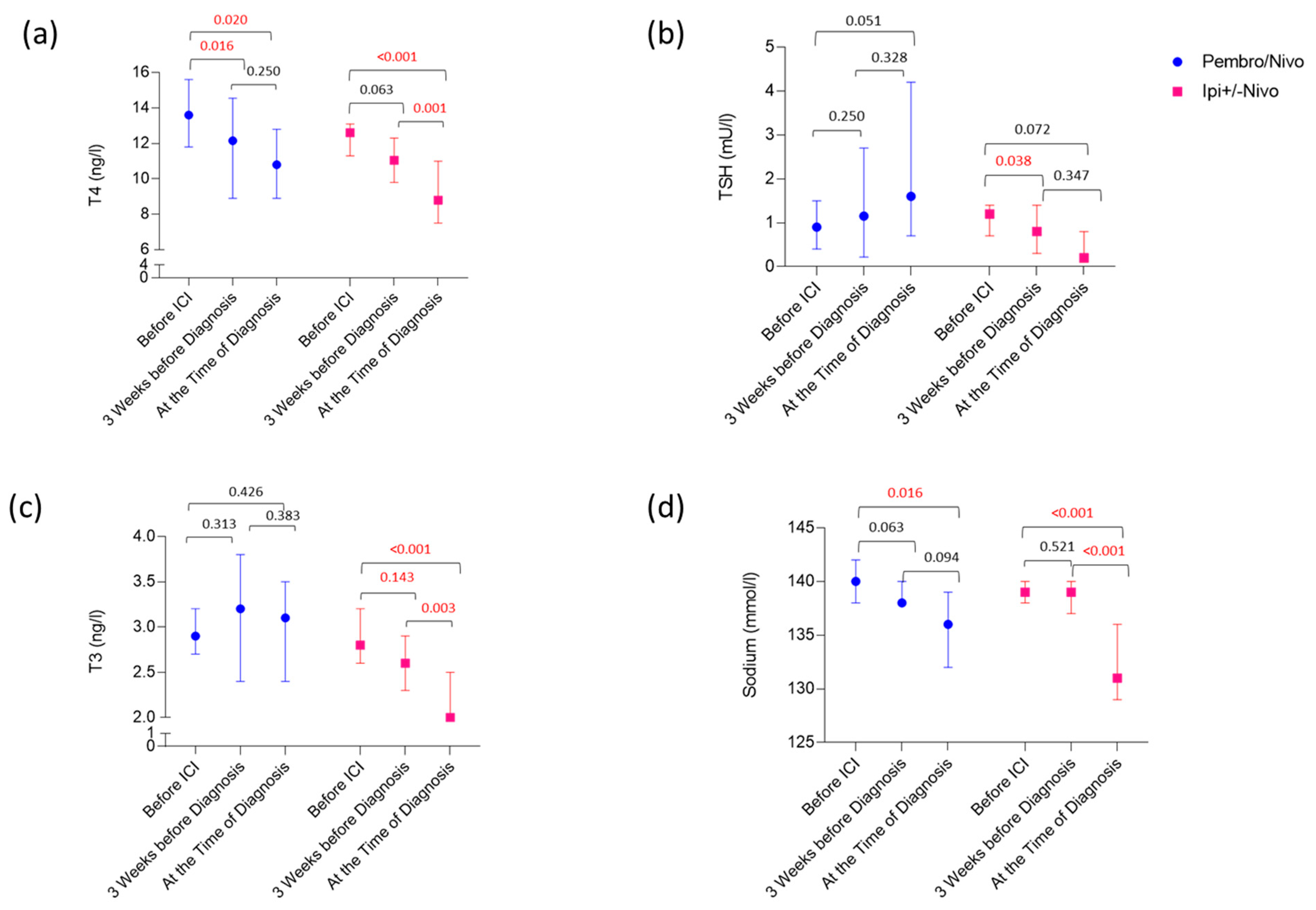
3.3. Laboratory Values Preceding and at the Time of Diagnosis of Ir-hypophysitis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Postow, M.A.; Callahan, M.K.; Wolchok, J.D. Immune checkpoint blockade in cancer therapy. J. Clin. Oncol. 2015, 33, 1974–1982. [Google Scholar] [CrossRef] [PubMed]
- Nogueira, E.; Newsom-Davis, T.; Morganstein, D.L. Immunotherapy-induced endocrinopathies: Assessment, management and monitoring. Ther. Adv. Endocrinol. Metab. 2019, 10, 2042018819896182. [Google Scholar] [CrossRef] [PubMed]
- Faje, A.; Reynolds, K.; Zubiri, L.; Lawrence, D.; Cohen, J.V.; Sullivan, R.J.; Nachtigall, L.; Tritos, N. Hypophysitis secondary to nivolumab and pembrolizumab is a clinical entity distinct from ipilimumab-associated hypophysitis. Eur. J. Endocrinol. 2019, 181, 211–219. [Google Scholar] [CrossRef] [PubMed]
- Caturegli, P.; Di Dalmazi, G.; Lombardi, M.; Grosso, F.; Larman, H.B.; Larman, T.; Taverna, G.; Cosottini, M.; Lupi, I. Hypophysitis Secondary to Cytotoxic T-Lymphocyte-Associated Protein 4 Blockade: Insights into Pathogenesis from an Autopsy Series. Am. J. Pathol. 2016, 186, 3225–3235. [Google Scholar] [CrossRef] [PubMed]
- Barroso-Sousa, R.; Barry, W.T.; Garrido-Castro, A.C.; Hodi, F.S.; Min, L.; Krop, I.E.; Tolaney, S.M. Incidence of Endocrine Dysfunction Following the Use of Different Immune Checkpoint Inhibitor Regimens: A Systematic Review and Meta-analysis. JAMA Oncol. 2018, 4, 173–182. [Google Scholar] [CrossRef] [PubMed]
- De Filette, J.; Andreescu, C.E.; Cools, F.; Bravenboer, B.; Velkeniers, B. A Systematic Review and Meta-Analysis of Endocrine-Related Adverse Events Associated with Immune Checkpoint Inhibitors. Horm. Metab. Res. 2019, 51, 145–156. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.; Li, J.; Tan, H. Progress and Challenges of Immune Checkpoint Inhibitor-Induced Hypophysitis. J. Clin. Med. 2023, 12, 3468. [Google Scholar] [CrossRef] [PubMed]
- Iwama, S.; De Remigis, A.; Callahan, M.K.; Slovin, S.F.; Wolchok, J.D.; Caturegli, P. Pituitary expression of CTLA-4 mediates hypophysitis secondary to administration of CTLA-4 blocking antibody. Sci. Transl. Med. 2014, 6, 230ra45. [Google Scholar] [CrossRef]
- Hassel, J.C.; Heinzerling, L.; Aberle, J.; Bähr, O.; Eigentler, T.K.; Grimm, M.O.; Grünwald, V.; Leipe, J.; Reinmuth, N.; Tietze, J.K.; et al. Combined immune checkpoint blockade (anti-PD-1/anti-CTLA-4): Evaluation and management of adverse drug reactions. Cancer Treat. Rev. 2017, 57, 36–49. [Google Scholar] [CrossRef]
- Abdallah, D.; Johnson, J.; Goldner, W.; Addasi, N.; Desouza, C.; Kotwal, A. Adrenal Insufficiency from Immune Checkpoint Inhibitors Masquerading as Sepsis. JCO Oncol. Pract. 2021, 17, 212–214. [Google Scholar] [CrossRef] [PubMed]
- Albarel, F.; Gaudy, C.; Castinetti, F.; Carré, T.; Morange, I.; Conte-Devolx, B.; Grob, J.J.; Brue, T. Long-term follow-up of ipilimumab-induced hypophysitis, a common adverse event of the anti-CTLA-4 antibody in melanoma. Eur. J. Endocrinol. 2015, 172, 195–204. [Google Scholar] [CrossRef] [PubMed]
- Ryder, M.; Callahan, M.; A Postow, M.; Wolchok, J.; A Fagin, J. Endocrine-related adverse events following ipilimumab in patients with advanced melanoma: A comprehensive retrospective review from a single institution. Endocr. Relat. Cancer 2014, 21, 371–381. [Google Scholar] [CrossRef] [PubMed]
- Chang, L.S.; Barroso-Sousa, R.; Tolaney, S.M.; Hodi, F.S.; Kaiser, U.B.; Min, L. Endocrine toxicity of cancer immunotherapy targeting immune checkpoints. Endocr. Rev. 2019, 40, 17–65. [Google Scholar] [CrossRef] [PubMed]
- Rao, S.; Mahadevan, A.; Maiti, T.; Ranjan, M.; Shwetha, S.D.; Arivazhagan, A.; Saini, J. Granulomatous and lymphocytic hypophysitis–Are they immunologically distinct? APMIS Acta Pathol. Microbiol. Immunol. Scand. 2016, 124, 1072–1077. [Google Scholar] [CrossRef]
- Kassi, E.; Angelousi, A.; Asonitis, N.; Diamantopoulos, P.; Anastasopoulou, A.; Papaxoinis, G.; Kokkinos, M.; Giovanopoulos, I.; Kyriakakis, G.; Petychaki, F.; et al. Endocrine-related adverse events associated with immune-checkpoint inhibitors in patients with melanoma. Cancer Med. 2019, 8, 6585–6594. [Google Scholar] [CrossRef] [PubMed]
- Percik, R.; Shlomai, G.; Tirosh, A.; Tirosh, A.; Leibowitz-Amit, R.; Eshet, Y.; Greenberg, G.; Merlinsky, A.; Barhod, E.; Steinberg-Silman, Y.; et al. Isolated autoimmune adrenocorticotropic hormone deficiency: From a rare disease to the dominant cause of adrenal insufficiency related to checkpoint inhibitors. Autoimmun. Rev. 2020, 19, 102454. [Google Scholar] [CrossRef] [PubMed]
- Fujisawa, Y.; Yoshino, K.; Otsuka, A.; Funakoshi, T.; Fujimura, T.; Yamamoto, Y.; Hata, H.; Gosho, M.; Tanaka, R.; Yamaguchi, K.; et al. Fluctuations in routine blood count might signal severe immune-related adverse events in melanoma patients treated with nivolumab. J. Dermatol. Sci. 2017, 88, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, Y.; Tanaka, R.; Maruyama, H.; Ishitsuka, Y.; Okiyama, N.; Watanabe, R.; Fujimoto, M.; Fujisawa, Y. Correlation between blood cell count and outcome of melanoma patients treated with anti-PD-1 antibodies. Jpn. J. Clin. Oncol. 2019, 49, 431–437. [Google Scholar] [CrossRef]
- Ariyasu, R.; Horiike, A.; Yoshizawa, T.; Dotsu, Y.; Koyama, J.; Saiki, M.; Sonoda, T.; Nishikawa, S.; Kitazono, S.; Yanagitani, N.; et al. adrenal insufficiency related to anti-programmed Death-1 therapy. Anticancer Res. 2017, 37, 4229–4232. [Google Scholar]
- Torino, F.; Barnabei, A.; Paragliola, R.M.; Marchetti, P.; Salvatori, R.; Corsello, S.M. Endocrine side-effects of anti-cancer drugs: mAbs and pituitary dysfunction: Clinical evidence and pathogenic hypotheses. Eur. J. Endocrinol. 2013, 169, R153–R164. [Google Scholar] [CrossRef] [PubMed]
- Di Dalmazi, G.; Ippolito, S.; Lupi, I.; Caturegli, P. Hypophysitis induced by immune checkpoint inhibitors: A 10-year assessment. Expert. Rev. Endocrinol. Metab. 2019, 14, 381–398. [Google Scholar] [CrossRef]
- Vidarsson, G.; Dekkers, G.; Rispens, T. IgG subclasses and allotypes: From structure to effector functions. Front. Immunol. 2014, 5, 520. [Google Scholar] [CrossRef] [PubMed]
- Jessel, S.; Weiss, S.A.; Austin, M.; Mahajan, A.; Etts, K.; Zhang, L.; Aizenbud, L.; Perdigoto, A.L.; Hurwitz, M.; Sznol, M.; et al. Immune Checkpoint Inhibitor-Induced Hypophysitis and Patterns of Loss of Pituitary Function. Front. Oncol. 2022, 12, 836859. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, M.S.; Lai, Z.M.; Spain, L.; Greener, V.; Turajlic, S.; Larkin, J.; Morganstein, D.L. Predicting development of ipilimumab-induced hypophysitis: Utility of T4 and TSH index but not TSH. J. Endocrinol. Investig. 2021, 44, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, T.; Iwama, S.; Yasuda, Y.; Okada, N.; Okuji, T.; Ito, M.; Onoue, T.; Goto, M.; Sugiyama, M.; Tsunekawa, T.; et al. Pituitary dysfunction induced by immune checkpoint inhibitors is associated with better overall survival in both malignant melanoma and non-small cell lung carcinoma: A prospective study. J. Immuno Ther. Cancer 2020, 8, e000779. [Google Scholar] [CrossRef] [PubMed]
- Snyders, T.; Chakos, D.; Swami, U.; Latour, E.; Chen, Y.; Fleseriu, M.; Milhem, M.; Zakharia, Y.; Zahr, R. Ipilimumab-induced hypophysitis, a single academic center experience. Pituitary 2019, 22, 488–496. [Google Scholar] [CrossRef] [PubMed]
- Sekizaki, T.; Kameda, H.; Oba, C.; Yong Cho, K.; Nakamura, A.; Miyoshi, H.; Osawa, T.; Shinohara, N.; Atsumi, T. Nivolumab-induced hypophysitis causing secondary adrenal insufficiency after transient ACTH elevation. Endocr. J. 2019, 66, 937–941. [Google Scholar] [CrossRef]
- Bando, H.; Yamamoto, M.; Urai, S.; Motomura, Y.; Sasaki, Y.; Ohmachi, Y.; Kobatake, M.; Tsujimoto, Y.; Oi-Yo, Y.; Suzuki, M.; et al. Fluctuations in serum adrenocorticotropic hormone concentration may predict the onset of immune checkpoint inhibitor-related hypophysitis. J. Immuno Ther. Cancer 2024, 12, e008634. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Control (40) | Ir-Hypophysitis (40) | p-Value | |
|---|---|---|---|
| Age (Years) | |||
| Median (Range) | 59 (17–77) | 59 (20–77) | 0.8 |
| n(%) | n(%) | ||
| Gender | 1.0 | ||
| Male | 27 (68) | 27 (68) | |
| Female | 13 (32) | 13 (32) | |
| Type of ICI | 1.0 | ||
| Pembro/Nivo | 9 (23) | 9 (23) | |
| Ipi+/−Nivo | 31 (77) | 31 (77) | |
| Other irAEs | 1.0 | ||
| Yes | 20 (50) | 20 (50) | |
| No | 20 (50) | 20 (50) | |
| CRP at Baseline | 0.06 | ||
| Normal | 19 (48) | 27 (68) | |
| Elevated | 20 (50) | 11 (28) | |
| Missing | 1 (2) | 2 (4) | |
| LDH at Baseline | 1.0 | ||
| Normal | 33 (83) | 33 (83) | |
| Elevated | 7 (17) | 6 (15) | |
| Missing | 1 (2) | ||
| PFS (Months) | 0.2 | ||
| Median (95%CI) | 7 (15–36) | 17 (19–41) | |
| OS (Months) | 0.3 | ||
| Median (95%CI) | 32 (30–51) | 48 (38–60) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mitri, F.; Machiraju, D.; Naoum, C.; Hassel, J.C. Early Serum Markers for Immune Checkpoint Inhibitor Induced Hypophysitis in Melanoma Patients. Cancers 2024, 16, 1340. https://doi.org/10.3390/cancers16071340
Mitri F, Machiraju D, Naoum C, Hassel JC. Early Serum Markers for Immune Checkpoint Inhibitor Induced Hypophysitis in Melanoma Patients. Cancers. 2024; 16(7):1340. https://doi.org/10.3390/cancers16071340
Chicago/Turabian StyleMitri, Fouad, Devayani Machiraju, Christina Naoum, and Jessica C. Hassel. 2024. "Early Serum Markers for Immune Checkpoint Inhibitor Induced Hypophysitis in Melanoma Patients" Cancers 16, no. 7: 1340. https://doi.org/10.3390/cancers16071340