
Precision Immuno-Oncology in NSCLC through Gender Equity Lenses
by
 , , , ,
, , , ,
Jennifer Marks
1,
Arthi Sridhar
2,
Angela Ai
3,
Lauren Kiel
4,
Rebekah Kaufman
4,
Oyepeju Abioye
4,
Courtney Mantz
4 and
Narjust Florez
4,5,* 1
Lombardi Comprehensive Cancer Center, Georgetown University, Washington, DC 20057, USA
2
Mayo Clinic, Rochester, MN 55905, USA
3
Olive View-UCLA Medical Center, University of California Los Angeles, Los Angeles, CA 90095, USA
4
Dana-Farber Cancer Institute, Boston, MA 02215, USA
5
Harvard Medical School, Boston, MA 02115, USA
*
Author to whom correspondence should be addressed.
Cancers 2024, 16(7), 1413; https://doi.org/10.3390/cancers16071413
Submission received: 7 March 2024
/
Revised: 2 April 2024
/
Accepted: 3 April 2024
/
Published: 4 April 2024
(This article belongs to the Special Issue Precision Immuno-Oncology in NSCLC)
Abstract
:Simple Summary
Precision immuno-oncology, the development of personalized treatments using the unique nature of an individual’s DNA, immune cells, and their tumor’s molecular profile, offers great promise. However, it has been well documented that biological sex considerably influences innate and adaptive immune responses, thereby conferring differences in the efficacy of lung cancer therapy between men and women. Despite this, women remain underrepresented in oncology clinical trials; this exclusion has resulted in our harboring of a limited understanding of the impact of immunotherapy on females and their survivorship, in addition to imprecise clinical recommendations. This review provides an overview of the sex-specific differences in immunity and immunotherapy efficacy, discusses contributing factors for the lack of women in clinical trials, and suggests future directions for precision oncology research, to ultimately aid in the development of treatment guidelines and recommendations that wholly consider the unique impact of immunotherapy on females and the intersectionality among them.
Abstract
Precision immuno-oncology involves the development of personalized cancer treatments that are influenced by the unique nature of an individual’s DNA, immune cells, and their tumor’s molecular characterization. Biological sex influences immunity; females typically mount stronger innate and adaptive immune responses than males. Though more research is warranted, we continue to observe an enhanced benefit for females with lung cancer when treated with combination chemoimmunotherapy in contrast to the preferred approach of utilizing immunotherapy alone in men. Despite the observed sex differences in response to treatments, women remain underrepresented in oncology clinical trials, largely as a result of gender-biased misconceptions. Such exclusion has resulted in the development of less efficacious treatment guidelines and clinical recommendations and has created a knowledge gap in regard to immunotherapy-related survivorship issues such as fertility. To develop a more precise approach to care and overcome the exclusion of women from clinical trials, flexible trial schedules, multilingual communication strategies, financial, and transportation assistance for participants should be adopted. The impact of intersectionality and other determinants of health that affect the diagnosis, treatment, and outcomes in women must also be considered in order to develop a comprehensive understanding of the unique impact of immunotherapy in all women with lung cancer.
Keywords:
immunotherapy; precision oncology; clinical trials; female; women; underrepresentation; NSCLC1. Introduction
Precision medicine involves tailoring interventions to patients by using their unique biomarkers within their genetic characteristics or molecular profiles [1]. Thus, in precision oncology, interventions extend beyond simply obtaining patient demographics and traditional clinical characteristics, and instead involve developing personalized treatment strategies using therapies targeted at a patient’s tumor’s molecular profile, as well as aiding in prognostication [2,3].
In tailoring interventions, it is important to consider sex disparities in the prognosis and outcomes of lung cancer, particularly non-small cell lung cancer (NSCLC). Compared to men, women are more frequently diagnosed with an adenocarcinoma subtype, at an earlier age, after less tobacco exposure, and are more susceptible to targeted approaches [4]. Women with NSCLC also show significantly better survival across all treatment modalities, regardless of stage or histology, though the magnitude of sex differences in mortality continues to decline due to increases in female mortality [4,5,6,7,8,9]. Nevertheless, it is crucial to recognize that cancer cells have the inherent capability to develop resistance to therapy, leading to a decreased duration of response and success of treatment. For instance, a wide variety of mechanisms, such as resistant EGFR-mutations, mutations in genes including PIK3CA, ALK, BRAF, KRAS, and TP53, and amplifications of MET and HER2 genes, are associated with acquired resistance to treatments such as osimertinib [10]. Understanding resistance mechanisms is an important aspect to improving treatment strategies.
Since the Human Genome Project, multiple large-scale studies have identified genomic, transcriptomic, and proteomic variations that may act as potential drug targets. We have also seen increased access to genomic sequencing on a patient-facing level, such that full genomic next-generation sequencing (NGS) can be completed in days and provide clinically relevant data [11]. With such advents of integrative genomics and advances in bioinformatics, we have been able to process an ample amount of genomic and transcription variations to identify potential targets with diagnostic and therapeutic implications [2,12]. This, combined with novel approaches to drug design, have contributed to the development of newfound therapies addressing targets previously thought to be “undruggable” due to factors such as their lacking defined ligand-binding pockets [13,14]. For instance, we may now target KRAS mutations due to the advent of selective KRASG12C inhibitors [13]. Additionally, there are multiple ongoing studies examining how to combine these selective inhibitors with other forms of therapy in addition to looking at non-G12C KRAS alleles [15]. Still, druggable driver mutations currently appear in low frequency amongst the cancer population, limiting the effectiveness of targeted treatment [16].
With advances in molecular immunology, immune checkpoint inhibitors (ICIs) have also become more sophisticated, with targeted immunotherapies more readily available. Even as immunotherapy becomes the first-line treatment for multiple types of cancer, though, there still remains a significant portion of patients who do not receive benefit [17,18], making it important to recognize immunotherapy-specific predictive biomarkers. One potential predictor of ICI response is the density of tumor-infiltrating lymphocytes (TILs) within a tumor [19,20,21] as well as natural-killer (NK) cells; in patients with advanced NSCLC receiving ICIs, lower NK cell values were independent prognostic factors for shorter OS and PFS. Sarcopenic patients with advanced NSCLC receiving ICIs also showed significantly worse PFS and had an 8.1 times higher risk of disease progression than non-sarcopenic patients [22,23]. As CXCR4 expression increases with stage progression in NSCLC, targeting the CXCL12/CXCR4 axis in immunotherapy has also emerged as a treatment approach, though this axis is not prognostic in early-stage NSCLC patients of either sex [24,25].
Another area garnering recent interest is a patient’s tumor microenvironment (TME) [26,27,28,29]. Notably, stromal cells are a cellular component within the TME and play a significant role in tumor metabolism, growth, metastasis, immune evasion, and treatment resistance [30]. There is emerging evidence that this stromal compartment can additionally shape antitumor immunity and responsiveness to immunotherapy [29,31]. For example, cancer-associated fibroblasts (CAFs) are the most common component of tumor stroma and are involved in tumorigenesis, tumor metastasis, and tumor angiogenesis [32,33,34]. One way that CAFs promote tumor progression is through the regulation of immune cells within the TME; strategies include inhibiting natural killer cells via the secretion of cytokines, chemokines, and MMPs [35]. Thus, several tailored strategies have been employed to combat these tactics, including anti-angiogenic therapy, immune modulation/reprogramming, CAF depletion, ECM targeting, and exosome or circulating tumor cell targeting, all of which are areas of active research [36].
Overall, immunotherapy has great promise, particularly considering how it is overall more effective and less toxic for patients [37,38,39,40]. However, the generalizability of current preliminary trial results are unclear due to their lack of representation of women [41,42]. Indeed, it is well documented that biological sex influences innate and adaptive immunity, as adult females typically mount stronger innate and adaptive immune responses compared to males [43,44,45,46]. Furthermore, for the majority of cancers, age-adjusted mortality rates and cancer-specific survival tend to be higher in males than females [47]. The implications of sex differences with regard to immunotherapy have not yet been well studied, offering opportunities for future research to provide more tailored data within populations that reflect our diverse clinical environment.
2. Sex Differences in Response to Immunotherapy
As previously noted, females typically express a more robust immune response, as they tend to have a higher B-cell response to various antigens and produce more interferons in macrophages and dendritic cells [48]. Sex hormones such as estrogen and testosterone also play a role in regulating the immune system; estrogen is thought to recruit immune cells that suppress the immune response, while androgens contrastingly may enhance it by promoting T-cell proliferation [48,49]. Estrogen-mediated immunomodulation also affects antigen-presenting cells and regulator T cells, with estrogen-enhancing PD-L1 expression [50]. Studies have further shown that sex chromosomes are determinants of sex dimorphism of anticancer immunity, owing to greater than fifty X-linked genes that play key roles in the innate immunity encoding for pro-inflammatory cytokines (e.g., TLR7 and TLR8) and in the regulation of adaptive immunity (e.g., IL2RG and IL13RA2) [51]. These X-linked genes are responsible for several transcription factors such as FOX-3 that are crucial for the development of regulatory T-cells and their functioning is responsible for suppressing immune responses [52]. Hormonal variations in women, such as those occurring during different phases of the menstrual cycle or menopause, may also influence immune responses and treatment efficacy [9,53]. Evidence suggests that females with early-stage NSCLC, specifically, also mount a stronger immune response due to their “hot” TME enriched with dendritic cells, CD4+ T cells, B cells, and a higher clonality of TILs. On the contrary, females with advanced NSCLC or those who are not treatment naïve have cancerous cells associated with complex resistance mechanisms and T-cell exhaustion, leading to the expression of multiple immune checkpoints; importantly, such differences are observed regardless of age, stage of disease, tumor histotype, and smoking status [54]. Sex differences in gut microbial composition may also play a role in the efficacy of immunotherapy. One study found that anti-PD-L1 could decrease the relative abundance of Lachnospiraceae, a bacteria associated with favorable responses to ICIs in female mice, while exerting no effect on male mice [55]. A higher relative abundance of Lachnospira has also been found in pre-menopausal women compared to post-menopausal women, who had similar levels to men [56]; the decline in microbiota diversity associated with aging might negatively influence ICIs [57]. Similarly, older adults have increased levels of regulatory T cells and pro-inflammatory cytokines such as interleukin (IL)-6, key mediators of immune evasion and resistance to ICIs. Though this decline might in principle result in an altered efficacy of immunotherapy in older patients, more research is needed; limited, non-generalizable subgroup analyses indicate that older patients may in fact gain the same benefit from immunotherapy as younger patients [57]. The breadth of recognized differences in the immunity between females and males has led to significant research aiming to determine if there is a difference in survival between women and men who are treated with ICIs. Several meta-analyses have been conducted with varying results.
A meta-analysis carried out by Conforti et al. explored sex-based differences in response to immunotherapy for lung cancer [58]. A prior meta-analysis conducted by this group included 20 randomized controlled trials (RCTs) and was the first to demonstrate a difference in the efficacy of ICIs in men and women [overall survival hazard ratio (OS-HR) 0.86 (95% CI 0.79–0.93) vs. 0.72 (95% CI 0.65–0.79) for females and males, respectively] [53]. In this subsequent study aiming to further investigate these findings, researchers integrated data from two meta-analyses, the first demonstrating how females derived a significantly greater benefit compared to males when receiving anti–PD-1/PD-L1 plus chemotherapy vs. chemotherapy for treatment across various solid tumors [0.48 (95% CI, 0.35–0.67) vs. 0.76 (95% CI, 0.66–0.87) for females and males, respectively]. The second meta-analysis included lung cancer trials alone and confirmed the prior observation that immunotherapy alone yielded greater benefits for males compared to females [0.78 (95% CI, 0.60 to 1.00) vs. 0.97 (95% CI, 0.79 to 1.19) for males and females, respectively]. Importantly, it also showed that the combined chemoimmunotherapy strategy proves more efficacious for females [0.44 (95% CI, 0.25–0.76)] compared to males [0.76 (95% CI, 0.64–0.91)], regardless of age, smoking status, or histology [58]. Kindred findings supporting the benefits of combined chemoimmunotherapy for females have been published in a meta-analysis conducted by Liang et al., which included 16 RCTs involving 10,155 patients with advanced NSCLC. This study demonstrated a more favorable OS-HR for women who were treated with ICI+ chemotherapy vs. chemotherapy alone when compared to males [0.63 (95% CI 0.42–0.92) vs. 0.79 (95% CI 0.70–0.89) for females and males, respectively] [59]. A later study conducted by Wu et al. encompassed 11 clinical trials (4 of which trials were for NSCLC) and corroborated the findings of Conforti et. al., demonstrating that males treated with ICIs were associated with a higher PFS and OS when compared to females, but notably, this difference was not observed with the NSCLC cohort [60]. Yet another meta-analysis that included only five phase-3 NSCLC trials (KEYNOTE 010, KEYNOTE 024, CHECKMATE 017, CHECKMATE 026, and CHECKMATE 057) comparing anti-PD1 ICI (pembrolizumab or nivolumab) to chemotherapy showed that a significant OS benefit was observed in males but not in females; this analysis, however, was limited by significant heterogeneity between studies and various cut-offs for biomarker expressions [61,62,63]. For instance, the inclusion criteria for the KEYNOTE 010, KEYNOTE 024, and CHECKMATE 026 trials involved PD-L1 tumor-expression positivity, while by contrast, the CHECKMATE 017 and CHECKMATE 057 trials enrolled patients with NSCLC without considering their PD-L1 status [64].
Despite the largely homogenous nature of the aforementioned data, several other meta-analyses examining the differences in the efficacy of ICIs among females and males have produced conflicting results [65,66]. For instance, a large-scale meta-analysis conducted by Wallis et al. encompassed 23 RCTs of patients, most of whom were in their 70s, and showed no statistically significant differences between the sexes when comparing ICIs to chemotherapy [65]. Boticelli et al. selected 36 clinical trials in which ICIs (anti-CTLA-4/PD-1/PD-L1) were studied and also did not appreciate any statistical differences in OS or PFS between the sexes; notably, however, this research did not include studies evaluating anti-PD-L1 ICIs in their final analysis [66]. Several other published studies (Table 1) have compared sex disparities in the outcomes for patients treated with ICIs. Despite varying results, a consistent theme noted continues to be the benefit for females when treated with combination chemoimmunotherapy; this contrasts with studies demonstrating that men experience a statistically significant benefit from ICIs alone compared to chemotherapy. It is important to recognize that limitations within all studies include the possibility for residual confounding factors such as the diverse range of tumor types considered, the absence of records pertaining to hormonal and PD-L1 status based on sex, and variations in biomarker expression cut-offs, which may influence the heterogenous results. Additionally, as meta-analyses rely on aggregate data instead of individual data, they may suffer from ecological fallacy. The inclusion of studies that are underpowered to explore the effect of sex disparities on outcomes, as well as the potential confounding impact of age on results, poses challenges, and more conclusive data are needed to delineate sex differences in response to ICIs. This includes addressing sex variations at the grassroot level and improving the gender-based diversity in the recruitment of patients to clinical trials.
3. Lack of Inclusion in Clinical Trials
Clinical trials are pivotal for shaping treatment protocols, yet persistent sex disparities exist affecting the inclusion of women. Indeed, research reveals a historical underrepresentation, with only 34.7% of participants in cancer preventive and therapy studies from 1990 to 2001 being female [69]. Though a more recent analysis involving data from 2008 to 2020 showed that females constituted 46.9% of participants in oncologic clinical trials, there were concerning proportional participation rates (PPR) of 0.912 across all trials, with women facing significant underrepresentation in surgical (PPR 0.74) and other invasive (PPR 0.69) oncology trials [70]. Further, recent immunotherapy trials such as the AEGEAN and KEYNOTE671, investigating perioperative chemoimmunotherapy in NSCLC, revealed a stark disparity of approximately 70% of participants in both treatment and placebo arms being male [71,72]. While the 2018 ADAURA trial did recruit over twice as many females as males (207 men, 471 women), it is important to note that this trial evaluated drug efficacy for an EGFR mutation, occurring over twice as often in females than in males (59% vs. 26%) [73]. Thus, appropriate representation is still needed for women when the mutation is not as prominent as EGFR. Underrepresentation also continues to be particularly pronounced among older women (>65 years) and those of minority race/ethnicity, though this trend extends to men as well [9].
The exclusion of women from clinical trials stems from a complex interplay of medical and societal considerations. A prominent factor is the potential impact of experimental treatments on fetal development, raising concerns related to pregnancy [74]. As women exhibit a higher incidence of autoimmunity and hypersensitivity reactions, caution is prompted regarding pregnant women’s inclusion in trials involving novel drugs or therapies [75]. Historical barriers also include a perception in the United States that women needed protection from clinical research, rooted in the adverse effects of thalidomide and diethylstilbestrol [69,74]. Past injustices such as the development of the HeLa cell line have also led to distrust of medical research [74]. Gender-specific barriers, including heightened time, financial costs, and increased familial responsibilities borne by women exacerbate such challenges [9]. The continuous lack of emphasis on women’s health research, limited awareness of trial opportunities, and fears related to randomization further compound the issue. More so, lingering gender-biased misconceptions that women are more difficult to recruit, are less willing to participate in trials, and are more difficult to work with [69] also persist as formidable obstacles to equitable representation [9,69]. For minoritized patient populations, additional barriers include stringent and narrow trial designs that may inadvertently exclude racial and ethnic minorities at a disproportionate rate [76,77], overly complex or lack of translated informational materials [78,79,80,81], and lack of local availability [76]. These patients may be hesitant to participate in clinical trials due to having a lack of trust in clinical research [82,83], as well as due to the financial toxicity [84,85] associated with trial participation, transportation needs, and other social determinants of health [86]. Owing to implicit biases, physicians also have less trust in and are less likely to offer a clinical trial to racial and ethnic minorities [87].
The repercussions of excluding women from clinical trials are extensive, impacting survivorship, treatment efficacy, sexual health, and fertility, and contribute to a lack of prospective validation for medication dosages and treatment protocols specifically tailored to women with lung cancer [9]. Consequently, women in targeted therapy trials are 25% more likely to experience severe adverse events than men, along with a heightened risk of underreporting [9,88,89,90]. Sex-specific variations in chemotherapy outcomes also reveal higher response rates but increased toxicities in women [91]. Immunotherapy, as previously noted, presents a different scenario, with men often experiencing greater efficacy, risk reduction, and benefits from the treatment alone, compared to women [53].
More so, limited prospective data assessing sexual dysfunction with cancer treatment, which remains underdiagnosed and undertreated [92], are available, resulting in a narrow understanding of how different cancer therapies affect libido, fertility, and overall sexual satisfaction in female patients [9]. Per the recently published SHAWL study, the largest study to date evaluating sexual health in patients with lung cancer, a resounding 77% of women experienced moderate to severe sexual dysfunction, with marked differences before and after cancer treatment [93]. However, these sexual health needs of women with cancer are often overlooked in clinical settings due to providers’ implicit discomfort, inexperience, or inaccurate perceptions of patient priorities [9,94]. In fact, a recent systematic study discovered that males with cancer had higher rates of patient–provider discussions of sexual issues than women [94]. Such disparities hinder the development of effective strategies to address issues such as vaginal dryness, pain during intercourse, or changes in body image [95].
Prospective information regarding the risks and long-term effects of cancer treatments on fertility is also lacking [96]. Compounded with the lack of general treatment guidance specifically tailored to women, this knowledge gap may result in even more poorly informed decision-making for women of reproductive age facing cancer diagnoses. Often, women may be unaware of fertility preservation options available to them or the impact of treatments on their ability to conceive in the future. Unsurprisingly, clinical recommendations about suitable treatments for pregnant patients with lung cancer are far from standardized, as most knowledge regarding treatment effects has been derived from research conducted in animal models or from data extrapolated from patients with breast cancer [97]. Though understudied, alkylating agents commonly used in lung cancer treatments have been associated with the highest risk of ovarian failure among cytotoxic chemotherapeutic medications [98], while the results from immunotherapy include the risk for hypogonadism, hypophysitis, hypothyroidism, low birth weight, increased miscarriage rates, stillbirth, and premature delivery [98,99]. Early-generation tyrosine kinase inhibitors, too, have been shown to negatively affect total follicle count, oocyte recovery, and ovarian reserve, reduce an embryo’s overall developmental potential, and even produce teratogenic effects [100]. Moreover, the evaluation of reproductive function and fertility is often insufficient when examining the consequences of cancer treatments [96]. As research reveals oncologists’ suboptimal knowledge, practices, and attitudes on fertility preservation and pregnancy during and after treatments [101,102,103], divergent survivorship experiences between men and women have been observed in discussions about fertility [9,96]. Unlike men, who were frequently advised to preserve sperm, women expressed negative sentiments regarding fertility preservation, citing inadequate information and presentation of their available options as contributing factors [9,104].
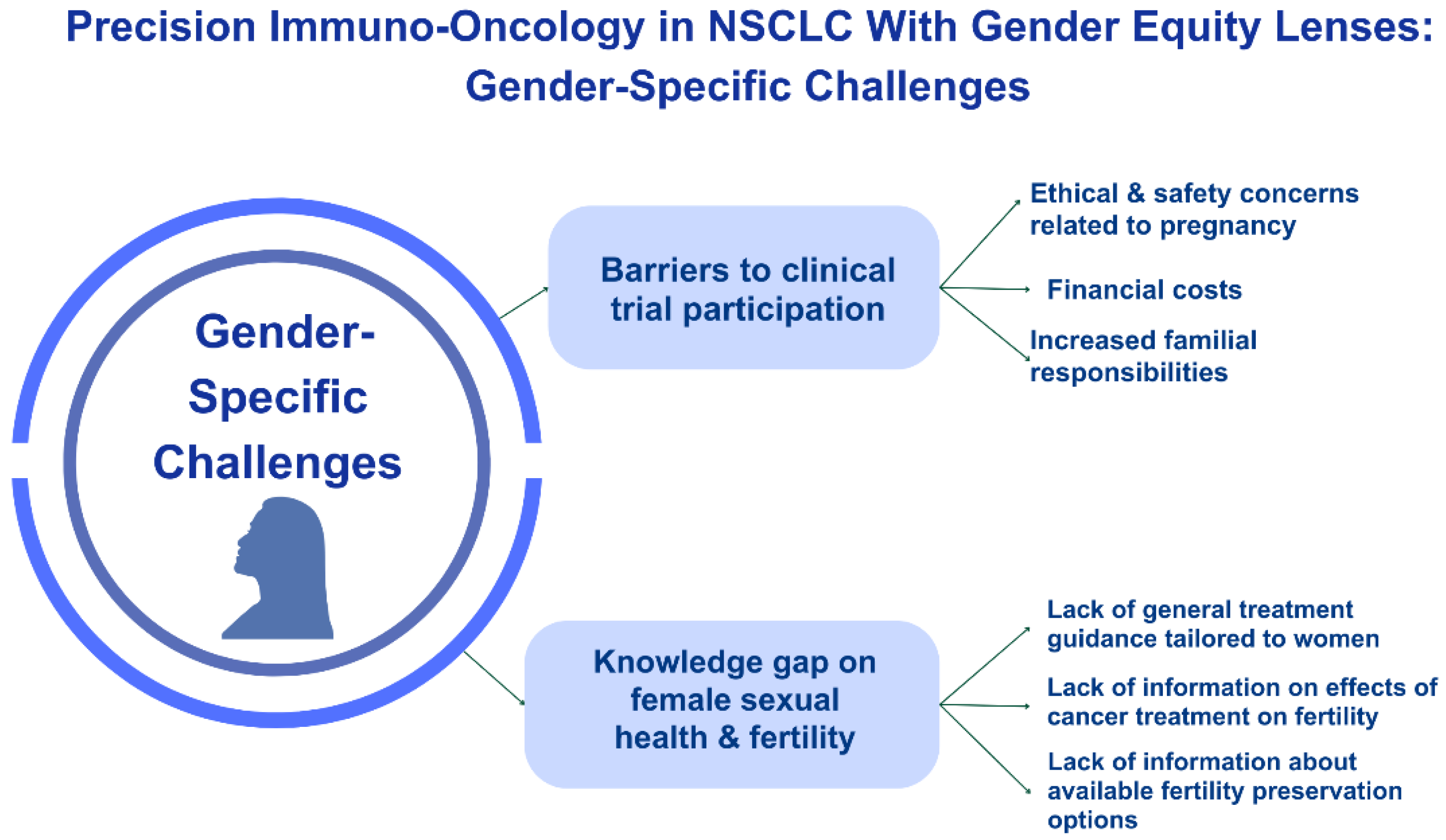
Despite the aforementioned implications, precision oncology discussions often overlook sex differences, which may unintentionally compromise the effectiveness of treatment strategies, limit informed decision-making, and impact the development of supportive care interventions (Figure 1). Without a diverse clinical trial participant pool, the efficacy, safety, pharmacokinetics, and pharmacodynamics of oncological treatments may not be adequately assessed for women, leading to disparities in outcomes [105,106]. The oversight of sex differences thereby undermines the fundamental principles of precision medicine, which aims to utilize treatments based on individual characteristics, including biological sex.
4. Future Directions
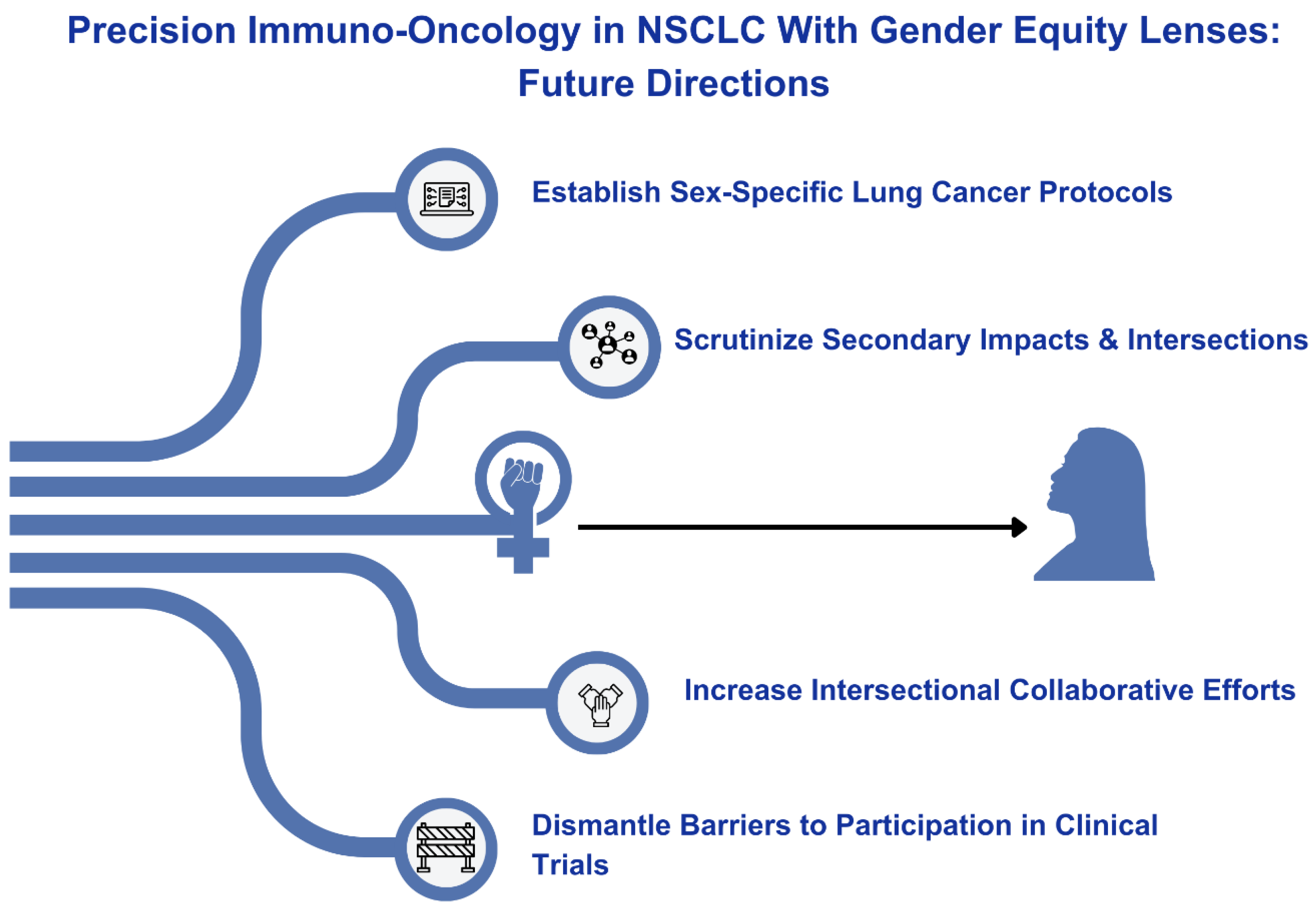
Sex-specific clinical research in women with lung cancer remains a pressing and unmet need (Figure 2). Future research initiatives should focus on sex-specific responses, hormonal influences, interactions with concurrent medications, and their effects on fertility, sexual health, survivorship, and overall outcomes [95,107]. These initiatives should also explore the interactions between immunotherapy and other medications commonly used by women, including hormone replacement therapies or contraceptives [108]. It is also imperative to scrutinize intersectionality; studying the diverse intersections of factors such as race, socio-economic status, and other determinants of health will shed light on disparities that affect the diagnosis, treatment, and outcomes in women with lung cancer [9,108].
A comprehensive approach involving healthcare providers, researchers, pharmaceutical companies, institutions, and governing bodies is also needed to promote a more unified understanding of clinical outcomes in women with lung cancer and enhance patient awareness and accessibility. Establishing standardized protocols and guidelines that consider sex-specific needs is necessary to ensure consistent and evidence-based care [96], but to increase the understandability of these guidelines, emphasis should be placed on community engagement and patient outreach. Implementing educational programs on cutting-edge therapies, treatment side effects, and sexual dysfunction to inform healthcare providers and women can empower patients to actively participate in treatment decisions [9]. Telemedicine initiatives can also enhance awareness and accessibility, particularly for those in remote or underserved areas, thereby enabling broader inclusion in clinical care and trials [9].
As socio-economic factors, access to care, and caregiver responsibilities can also affect women’s ability to enroll and remain engaged in clinical research, educating healthcare teams on the implications of clinical trial unenrollment is of paramount importance, as is adopting specific strategies for recruiting and retaining female participants. Measures such as flexible trial schedules, financial assistance, and transportation support can significantly enhance the participation rates among diverse groups of women [9,109]. Culturally sensitive and multilingual communication strategies should also be employed to reach a broader demographic, ensuring that research findings are representative of the diverse population affected by lung cancer. Involving patient advocates with clinical trial designs and utilizing patient navigators and community outreach may also help. Studies have also found that government-funded studies, as well as studies with first or senior female authors, had a higher percentage of female participants [9]. Furthermore, incentivizing clinical trialists and industry sponsors to address enrollment challenges could be implemented [109,110]. Although regulatory agencies have issued guidance to the pharmaceutical industry to study and reflect diversity within real-world populations, it is important to note that these directives are non-binding [110]. Innovative approaches, such as implementing hospital quality carrot-and-stick programs and drawing inspiration from industries outside of healthcare that have successfully tackled disparity gaps, can contribute to a more holistic and effective tactic in promoting equity [110].
5. Conclusions
The surging interest in precision immuno-oncology has highlighted a diverse range of promising therapeutic approaches for patients with cancer. Nevertheless, there remains a high priority to consider immunotherapy in the context of sex differences due to the more robust immune response of females, the immune-suppressing response of sex hormones such as estrogen, the vast array of X-linked genes that contribute to females’ immune-suppressing response, unique variations in the TME for females, and the observed sex differences in response to various lung cancer treatments. Though future large-scale, more standardized research is warranted to rectify conflicting results regarding the effectiveness of immunotherapy on females and males with lung cancer, we continue to observe an enhanced benefit for females when treated with combination chemoimmunotherapy in contrast to the more favorable approach of utilizing ICIs alone in men. Multi-disciplinary collaboration among healthcare providers, researchers, pharmaceutical companies, institutions, and governing bodies will be necessary to provide a more unified understanding of clinical outcomes in women with lung cancer.
Enhancing the effectiveness of treatment plans, guidelines, and recommendations that are specifically tailored to the unique needs of patients begins with improving the gender-based diversity of clinical trials. Sex-specific variations in immunotherapy, targeted therapy, and chemotherapy outcomes continue to be observed as a result of this inadequate representation; more so, treatment implications on issues related to sexual dysfunction, fertility, and other survivorship issues unique to women are largely unknown. To overcome persistent gender bias and societal obstacles facilitating the historic and current exclusion of women from clinical trials, efforts should be made to incorporate flexible trial schedules, multilingual communication strategies, and financial and transportation assistance for participants, as well as adopting strategies to incentivize trials to more equally represent the diverse body of patients with lung cancer. Of equal importance throughout all efforts is the need to consider the impact of intersectionality, including race, socio-economic status, and other determinants of health that affect the diagnosis, treatment, and outcomes in women with lung cancer. Such endeavors will aid in developing a more tailored understanding of the unique impact of immunotherapy on females, with an ultimate goal of constructing and implementing standardized protocols and guidelines that consider intersectionality, sex-specific needs, and opportunities across practices in various medical settings.
Author Contributions
Conceptualization, N.F.; methodology, N.F.; software, N.F.; validation, N.F., L.K. and R.K.; formal analysis, J.M., A.S., A.A., L.K. and N.F.; investigation, J.M., A.S., A.A., L.K. and N.F.; resources, J.M., A.S., A.A., L.K. and N.F.; data curation, J.M., A.S., A.A., L.K. and N.F.; writing—original draft preparation, J.M., A.S., A.A., L.K. and N.F.; writing—review and editing, N.F., L.K., R.K., C.M. and O.A.; visualization, J.M., A.S., A.A., L.K., R.K., O.A., C.M. and N.F.; supervision, N.F. and L.K.; project administration, N.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
The data presented in this study are openly available via access to their corresponding citations found in the References section of this manuscript.
Conflicts of Interest
NF: Merck, DSI, Pfizer, Novocure, Takeda, Genentech, Regeneron, Astrazeneca, BMS, Janssen, and Neogenomics. All other authors declare no conflicts of interest.
References
- National Research Council. Committee on A Framework for Developing a New Taxonomy of Disease. The National Academies Collection: Reports funded by National Institutes of Health. Toward Precision Medicine: Building a Knowledge Network for Biomedical Research and a New Taxonomy of Disease. 2011. Available online: https://pubmed.ncbi.nlm.nih.gov/22536618/ (accessed on 2 February 2024).
- Kumar-Sinha, C.; Chinnaiyan, A.M. Precision oncology in the age of integrative genomics. Nat. Biotechnol. 2018, 36, 46–60. [Google Scholar] [CrossRef] [PubMed]
- Boca, S.M.; Panagiotou, O.A.; Rao, S.; McGarvey, P.B.; Madhavan, S. Future of evidence synthesis in precision oncology: Between systematic reviews and biocuration. JCO Precis. Oncol. 2018, 2. [Google Scholar] [CrossRef] [PubMed]
- Paggi, M.G.; Vona, R.; Abbruzzese, C.; Malorni, W. Gender-related disparities in non-small cell lung cancer. Cancer Lett. 2010, 298, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, H.; Ando, K.; Shinmyo, T.; Morita, K.; Mochizuki, A.; Kurimoto, N.; Tatsunami, S. Female gender is an independent prognostic factor in non-small-cell lung cancer: A meta-analysis. Ann. Thorac. Cardiovasc. Surg. 2011, 17, 469–480. [Google Scholar] [CrossRef] [PubMed]
- Baiu, I.; Titan, A.L.; Martin, L.W.; Wolf, A.; Backhus, L. The role of gender in non-small cell lung cancer: A narrative review. J. Thorac. Dis. 2021, 13, 3816. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, Y.; Murayama, T.; Sato, Y.; Suzuki, Y.; Saito, H.; Nomura, Y. Gender Differences in Long-Term Survival after Surgery for Non-Small Cell Lung Cancer. Thorac. Cardiovasc. Surg. 2016, 64, 507–514. [Google Scholar] [CrossRef]
- Donington, J.S.; Colson, Y.L. Sex and gender differences in non-small cell lung cancer. Semin. Thorac. Cardiovasc. Surg. 2011, 23, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Florez, N.; Kiel, L.; Riano, I.; Patel, S.; DeCarli, K.; Dhawan, N.; Franco, I.; Odai-Afotey, A.; Meza, K.; Swami, N.; et al. Lung Cancer in Women: The Past, Present, and Future. Clin. Lung Cancer 2023, 25, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, F.; Yoneda, K.; Takenaka, M.; Kuroda, K. Treatment strategy of EGFR-mutated non-small cell lung cancer. J. Thorac. Dis. 2022, 14, 602. [Google Scholar] [CrossRef]
- Wetterstrand, K. The Cost of Sequencing a Human Genome. Genome. 2016. Available online: https://www.genome.gov/about-genomics/fact-sheets/Sequencing-Human-Genome-cost (accessed on 3 February 2024).
- Chen, H.Z.; Bonneville, R.; Roychowdhury, S. Implementing precision cancer medicine in the genomic era. Semin. Cancer Biol. 2019, 55, 16–27. [Google Scholar] [CrossRef]
- Huang, L.; Guo, Z.; Wang, F.; Fu, L. KRAS mutation: From undruggable to druggable in cancer. Signal Transduct. Target. Ther. 2021, 6, 386. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.; Zhang, J.; Gao, Y.; Li, Y.; Li, Y. Strategies for targeting undruggable targets. Expert Opin. Drug Discov. 2022, 17, 55–69. [Google Scholar] [CrossRef] [PubMed]
- Murciano-Goroff, Y.R.; Suehnholz, S.P.; Drilon, A.; Chakravarty, D. Precision Oncology: 2023 in Review. Cancer Discov. 2023, 13, 2525–2531. [Google Scholar] [CrossRef]
- Lawrence, M.S.; Stojanov, P.; Mermel, C.H.; Robinson, J.T.; Garraway, L.A.; Golub, T.R.; Meyerson, M.; Gabriel, S.B.; Lander, E.S.; Getz, G. Discovery and saturation analysis of cancer genes across 21 tumour types. Nature 2014, 505, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Gong, J.; Chehrazi-Raffle, A.; Reddi, S.; Salgia, R. Development of PD-1 and PD-L1 inhibitors as a form of cancer immunotherapy: A comprehensive review of registration trials and future considerations. J. Immunother. Cancer 2018, 6, 8. [Google Scholar] [CrossRef] [PubMed]
- Haslam, A.; Prasad, V. Estimation of the percentage of US patients with cancer who are eligible for and respond to checkpoint inhibitor immunotherapy drugs. JAMA Netw. Open 2019, 2, e192535. [Google Scholar] [CrossRef] [PubMed]
- Fridman, W.H.; Pagès, F.; Sautès-Fridman, C.; Galon, J. The immune contexture in human tumours: Impact on clinical outcome. Nat. Rev. Cancer 2012, 12, 298–306. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.S.; Mellman, I. Elements of cancer immunity and the cancer–immune set point. Nature 2017, 541, 321–330. [Google Scholar] [CrossRef]
- White, K.; Connor, K.; Meylan, M.; Bougoüin, A.; Salvucci, M.; Bielle, F.; O’farrell, A.C.; Sweeney, K.; Weng, L.; Bergers, G.; et al. Identification, validation and biological characterisation of novel glioblastoma tumour microenvironment subtypes: Implications for precision immunotherapy. Ann. Oncol. 2023, 34, 300–314. [Google Scholar] [CrossRef] [PubMed]
- Tenuta, M.; Pandozzi, C.; Sciarra, F.; Campolo, F.; Gelibter, A.J.; Sirgiovanni, G.; Cortesi, E.; Lenzi, A.; Isidori, A.M.; Sbardella, E.; et al. Circulating natural killer cells as prognostic value for non-small-cell lung cancer patients treated with immune checkpoint inhibitors: Correlation with sarcopenia. Cancers 2023, 15, 3592. [Google Scholar] [CrossRef] [PubMed]
- Tenuta, M.; Gelibter, A.; Pandozzi, C.; Sirgiovanni, G.; Campolo, F.; Venneri, M.A.; Caponnetto, S.; Cortesi, E.; Marchetti, P.; Isidori, A.M.; et al. Impact of sarcopenia and inflammation on patients with advanced non-small cell lung cancer (NCSCL) treated with immune checkpoint inhibitors (ICIs): A prospective study. Cancers 2021, 13, 6355. [Google Scholar] [CrossRef] [PubMed]
- Fung, A.S.; Kopciuk, K.; Dean, M.L.; D’Silva, A.; Otsuka, S.; Klimowicz, A.; Hao, D.; Morris, D.; Bebb, D.G. CXCR4 expression in lung carcinogenesis: Evaluating gender-specific differences in survival outcomes based on CXCR4 expression in early stage non-small cell lung cancer patients. PLoS ONE 2021, 16, e0241240. [Google Scholar] [CrossRef] [PubMed]
- Zhou, W.; Guo, S.; Liu, M.; Burow, M.E.; Wang, G. Targeting CXCL12/CXCR4 axis in tumor immunotherapy. Curr. Med. Chem. 2019, 26, 3026–3041. [Google Scholar] [CrossRef] [PubMed]
- Anagnostou, V.; Landon, B.V.; Medina, J.E.; Forde, P.; Velculescu, V.E. Translating the evolving molecular landscape of tumors to biomarkers of response for cancer immunotherapy. Sci. Transl. Med. 2022, 14, eabo3958. [Google Scholar] [CrossRef] [PubMed]
- Wheler, J.; Lee, J.J.; Kurzrock, R. Unique molecular landscapes in cancer: Implications for individualized, curated drug combinations. Cancer Res. 2014, 74, 7181–7184. [Google Scholar] [CrossRef]
- Hanahan, D.; Coussens, L.M. Accessories to the crime: Functions of cells recruited to the tumor microenvironment. Cancer Cell 2012, 21, 309–322. [Google Scholar] [CrossRef]
- Zhao, Y.; Shen, M.; Wu, L.; Yang, H.; Yao, Y.; Yang, Q.; Du, J.; Liu, L.; Li, Y.; Bai, Y. Stromal cells in the tumor microenvironment: Accomplices of tumor progression? Cell Death Dis. 2023, 14, 587. [Google Scholar] [CrossRef]
- Bussard, K.M.; Mutkus, L.; Stumpf, K.; Gomez-Manzano, C.; Marini, F.C. Tumor-associated stromal cells as key contributors to the tumor microenvironment. Breast Cancer Res. 2016, 18, 84. [Google Scholar] [CrossRef] [PubMed]
- Turley, S.J.; Cremasco, V.; Astarita, J.L. Immunological hallmarks of stromal cells in the tumour microenvironment. Nat. Rev. Immunol. 2015, 15, 669–682. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Li, W.; Lin, S.; Liu, B.; Wu, P.; Li, L. Fibroblast diversity and plasticity in the tumor microenvironment: Roles in immunity and relevant therapies. Cell Commun. Signal. 2023, 21, 234. [Google Scholar] [CrossRef]
- Kalluri, R. The biology and function of fibroblasts in cancer. Nat. Rev. Cancer 2016, 16, 582–598. [Google Scholar] [CrossRef] [PubMed]
- Valkenburg, K.C.; De Groot, A.E.; Pienta, K.J. Targeting the tumour stroma to improve cancer therapy. Nat. Rev. Clin. Oncol. 2018, 15, 366–381. [Google Scholar] [CrossRef] [PubMed]
- Mao, X.; Xu, J.; Wang, W.; Liang, C.; Hua, J.; Liu, J.; Zhang, B.; Meng, Q.; Yu, X.; Shi, S. Crosstalk between cancer-associated fibroblasts and immune cells in the tumor microenvironment: New findings and future perspectives. Mol. Cancer 2021, 20, 131. [Google Scholar] [CrossRef] [PubMed]
- Baghban, R.; Roshangar, L.; Jahanban-Esfahlan, R.; Seidi, K.; Ebrahimi-Kalan, A.; Jaymand, M.; Kolahian, S.; Javaheri, T.; Zare, P. Tumor microenvironment complexity and therapeutic implications at a glance. Cell Commun. Signal. 2020, 18, 59. [Google Scholar] [CrossRef] [PubMed]
- Almutairi, A.R.; Alkhatib, N.; Martin, J.; Babiker, H.M.; Garland, L.L.; McBride, A.; Abraham, I. Comparative efficacy and safety of immunotherapies targeting the PD-1/PD-L1 pathway for previously treated advanced non-small cell lung cancer: A Bayesian network meta-analysis. Crit. Rev. Oncol. Hematol. 2019, 142, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Zhao, W.; Jin, L.; Chen, P.; Li, D.; Gao, W.; Dong, G. Colorectal cancer immunotherapy-Recent progress and future directions. Cancer Lett. 2022, 545, 215816. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Verma, V.; Gay, C.M.; Chen, Y.; Liang, F.; Lin, Q.; Wang, J.; Zhang, W.; Hui, Z.; Zhao, M.; et al. Neoadjuvant immunotherapy for advanced, resectable non-small cell lung cancer: A systematic review and meta-analysis. Cancer 2023, 129, 1969–1985. [Google Scholar] [CrossRef] [PubMed]
- Jácome, A.A.; Castro, A.C.G.; Vasconcelos, J.P.S.; Silva, M.H.C.; Lessa, M.A.O.; Moraes, E.D.; Andrade, A.C.; Lima, F.M.; Farias, J.P.F.; Gil, R.A.; et al. Efficacy and safety associated with immune checkpoint inhibitors in unresectable hepatocellular carcinoma: A meta-analysis. JAMA Netw. Open 2021, 4, e2136128. [Google Scholar] [CrossRef]
- Duma, N.; Vera Aguilera, J.; Paludo, J.; Haddox, C.L.; Gonzalez Velez, M.; Wang, Y.; Leventakos, K.; Hubbard, J.M.; Mansfield, A.S.; Go, R.S.; et al. Representation of minorities and women in oncology clinical trials: Review of the past 14 years. J. Oncol. Pract. 2018, 14, e1–e10. [Google Scholar] [CrossRef] [PubMed]
- Murthy, V.H.; Krumholz, H.M.; Gross, C.P. Participation in cancer clinical trials: Race-, sex-, and age-based disparities. JAMA 2004, 291, 2720–2726. [Google Scholar] [CrossRef]
- Klein, S.L.; Flanagan, K.L. Sex differences in immune responses. Nat. Rev. Immunol. 2016, 16, 626–638. [Google Scholar] [CrossRef] [PubMed]
- Vom Steeg, L.G.; Klein, S.L. SeXX matters in infectious disease pathogenesis. PLoS Pathog. 2016, 12, e1005374. [Google Scholar] [CrossRef]
- Quintero, O.L.; Amador-Patarroyo, M.J.; Montoya-Ortiz, G.; Rojas-Villarraga, A.; Anaya, J.M. Autoimmune disease and gender: Plausible mechanisms for the female predominance of autoimmunity. J. Autoimmun. 2012, 38, J109–J119. [Google Scholar] [CrossRef] [PubMed]
- Klein, S.L.; Jedlicka, A.; Pekosz, A. The Xs and Y of immune responses to viral vaccines. Lancet Infect. Dis. 2010, 10, 338–349. [Google Scholar] [CrossRef]
- Cook, M.B.; McGlynn, K.A.; Devesa, S.S.; Freedman, N.D.; Anderson, W.F. Sex disparities in cancer mortality and survival. Cancer Epidemiol. Biomark. Prev. 2011, 20, 1629–1637. [Google Scholar] [CrossRef] [PubMed]
- Pala, L.; De Pas, T.; Catania, C.; Giaccone, G.; Mantovani, A.; Minucci, S.; Viale, G.; Gelber, R.D.; Conforti, F. Sex and cancer immunotherapy: Current understanding and challenges. Cancer Cell 2022, 40, 695–700. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Jin, J.; Yang, Y.; Sun, H.; Wu, L.; Shen, M.; Hong, X.; Li, W.; Lu, L.; Cao, D.; et al. Androgen receptor-mediated CD8+ T cell stemness programs drive sex differences in antitumor immunity. Immunity 2022, 55, 1268–1283.e9. [Google Scholar] [CrossRef] [PubMed]
- Polanczyk, M.J.; Hopke, C.; Vandenbark, A.A.; Offner, H. Estrogen-mediated immunomodulation involves reduced activation of effector T cells, potentiation of Treg cells, and enhanced expression of the PD-1 costimulatory pathway. J. Neurosci. Res. 2006, 84, 370–378. [Google Scholar] [CrossRef] [PubMed]
- Haupt, S.; Caramia, F.; Klein, S.L.; Rubin, J.B.; Haupt, Y. Sex disparities matter in cancer development and therapy. Nat. Rev. Cancer 2021, 21, 393–407. [Google Scholar] [CrossRef] [PubMed]
- Mertowska, P.; Mertowski, S.; Podgajna, M.; Grywalska, E. The Importance of the Transcription Factor Foxp3 in the Development of Primary Immunodeficiencies. J. Clin. Med. 2022, 11, 947. [Google Scholar] [CrossRef] [PubMed]
- Conforti, F.; Pala, L.; Bagnardi, V.; De Pas, T.; Martinetti, M.; Viale, G.; Gelber, R.D.; Goldhirsch, A. Cancer immunotherapy efficacy and patients’ sex: A systematic review and meta-analysis. Lancet Oncol. 2018, 19, 737–746. [Google Scholar] [CrossRef] [PubMed]
- Conforti, F.; Pala, L.; Pagan, E.; Bagnardi, V.; De Pas, T.; Queirolo, P.; Pennacchioli, E.; Catania, C.; Cocorocchio, E.; Ferrucci, P.F.; et al. Sex-Based Dimorphism of Anticancer Immune Response and Molecular Mechanisms of Immune Evasion. Clin. Cancer Res. 2021, 27, 4311–4324. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Tang, L.; Zhai, D.; Song, M.; Li, W.; Xu, S.; Jiang, S.; Meng, H.; Liang, J.; Wang, Y.; et al. The role of the sex hormone-gut microbiome axis in tumor immunotherapy. Gut Microbes 2023, 15, 2185035. [Google Scholar] [CrossRef]
- Santos-Marcos, J.A.; Rangel-Zuñiga, O.A.; Jimenez-Lucena, R.; Quintana-Navarro, G.M.; Garcia-Carpintero, S.; Malagon, M.M.; Landa, B.B.; Tena-Sempere, M.; Perez-Martinez, P.; Lopez-Miranda, J.; et al. Influence of gender and menopausal status on gut microbiota. Maturitas 2018, 116, 43–53. [Google Scholar] [CrossRef] [PubMed]
- Gomes, F.; Wong, M.; Battisti, N.M.L.; Kordbacheh, T.; Kiderlen, M.; Greystoke, A.; Luciani, A. Immunotherapy in older patients with non-small cell lung cancer: Young International Society of Geriatric Oncology position paper. Br. J. Cancer 2020, 123, 874–884. [Google Scholar] [CrossRef] [PubMed]
- Conforti, F.; Pala, L.; Bagnardi, V.; Viale, G.; De Pas, T.; Pagan, E.; Pennacchioli, E.; Cocorocchio, E.; Ferrucci, P.F.; De Marinis, F.; et al. Sex-Based Heterogeneity in Response to Lung Cancer Immunotherapy: A Systematic Review and Meta-Analysis. J. Natl. Cancer Inst. 2019, 111, 772–781. [Google Scholar] [CrossRef]
- Liang, J.; Hong, J.; Tang, X.; Qiu, X.; Zhu, K.; Zhou, L.; Guo, D. Sex difference in response to non-small cell lung cancer immunotherapy: An updated meta-analysis. Ann. Med. 2022, 54, 2605–2615. [Google Scholar] [CrossRef]
- Wu, Y.; Ju, Q.; Jia, K.; Yu, J.; Shi, H.; Wu, H.; Jiang, M. Correlation between sex and efficacy of immune checkpoint inhibitors (PD-1 and CTLA-4 inhibitors). Int. J. Cancer 2018, 143, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Herbst, R.S.; Baas, P.; Kim, D.W.; Felip, E.; Pérez-Gracia, J.L.; Han, J.Y.; Molina, J.; Kim, J.H.; Arvis, C.D.; Ahn, M.J.; et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): A randomised controlled trial. Lancet 2016, 387, 1540–1550. [Google Scholar] [CrossRef]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Five-Year Outcomes with Pembrolizumab versus Chemotherapy for Metastatic Non-Small-Cell Lung Cancer with PD-L1 Tumor Proportion Score ≥ 50. J. Clin. Oncol. 2021, 39, 2339–2349. [Google Scholar] [CrossRef] [PubMed]
- Borghaei, H.; Gettinger, S.; Vokes, E.E.; Chow, L.Q.; Burgio, M.A.; de Castro Carpeno, J.; Pluzanski, A.; Arrieta, O.; Frontera, O.A.; Chiari, R.; et al. Five-Year Outcomes from the Randomized, Phase III Trials CheckMate 017 and 057: Nivolumab Versus Docetaxel in Previously Treated Non–Small-Cell Lung Cancer. J. Clin. Oncol. 2021, 39, 723–733. [Google Scholar] [CrossRef]
- Pinto, J.A.; Vallejos, C.S.; Raez, L.E.; Mas, L.A.; Ruiz, R.; Torres-Roman, J.S.; Morante, Z.; Araujo, J.M.; Gómez, H.L.; Aguilar, A.; et al. Gender and outcomes in non-small cell lung cancer: An old prognostic variable comes back for targeted therapy and immunotherapy? ESMO Open 2018, 3, e000344. [Google Scholar] [CrossRef] [PubMed]
- Wallis, C.J.; Butaney, M.; Satkunasivam, R.; Freedland, S.J.; Patel, S.P.; Hamid, O.; Pal, S.K.; Klaassen, Z. Association of Patient Sex with Efficacy of Immune Checkpoint Inhibitors and Overall Survival in Advanced Cancers: A Systematic Review and Meta-analysis. JAMA Oncol. 2019, 5, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Botticelli, A.; Onesti, C.E.; Zizzari, I.; Cerbelli, B.; Sciattella, P.; Occhipinti, M.; Roberto, M.; Di Pietro, F.; Bonifacino, A.; Ghidini, M.; et al. The sexist behaviour of immune checkpoint inhibitors in cancer therapy? Oncotarget 2017, 8, 99336. [Google Scholar] [CrossRef]
- Grassadonia, A.; Sperduti, I.; Vici, P.; Iezzi, L.; Brocco, D.; Gamucci, T.; Pizzuti, L.; Maugeri-Saccà, M.; Marchetti, P.; Cognetti, G.; et al. Effect of gender on the outcome of patients receiving immune checkpoint inhibitors for advanced cancer: A systematic review and meta-analysis of phase III randomized clinical trials. J. Clin. Med. 2018, 7, 542. [Google Scholar] [CrossRef]
- Wang, C.; Qiao, W.; Jiang, Y.; Zhu, M.; Shao, J.; Ren, P.; Liu, D.; Li, W. Effect of sex on the efficacy of patients receiving immune checkpoint inhibitors in advanced non-small cell lung cancer. Cancer Med. 2019, 8, 4023–4031. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.; Wen, P. Gender and sex disparity in cancer trials. ESMO Open 2020, 5, e000773. [Google Scholar] [CrossRef]
- Perera, N.D.; Bellomo, T.R.; Schmidt, W.M.; Litt, H.K.; Shyu, M.; Stavins, M.A.; Wang, M.M.; Bell, A.; Saleki, M.; Wolf, K.I.; et al. Analysis of Female Participant Representation in Registered Oncology Clinical Trials in the United States from 2008 to 2020. Oncologist 2023, 28, 510–519. [Google Scholar] [CrossRef] [PubMed]
- Heymach, J.V.; Harpole, D.; Mitsudomi, T.; Taube, J.M.; Galffy, G.; Hochmair, M.; Winder, T.; Zukov, R.; Garbaos, G.; Gao, S.; et al. Abstract CT005: AEGEAN: A phase 3 trial of neoadjuvant durvalumab+ chemotherapy followed by adjuvant durvalumab in patients with resectable NSCLC. Cancer Res. 2023, 83, CT005. [Google Scholar] [CrossRef]
- Wakelee, H.; Liberman, M.; Kato, T.; Tsuboi, M.; Lee, S.H.; Gao, S.; Chen, K.N.; Dooms, C.; Majem, M.; Eigendorff, E.; et al. Perioperative Pembrolizumab for Early-Stage Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2023, 389, 491–503. [Google Scholar] [CrossRef] [PubMed]
- Bell, D.W.; Brannigan, B.W.; Matsuo, K.; Finkelstein, D.M.; Sordella, R.; Settleman, J.; Mitsudomi, T.; Haber, D.A. Increased prevalence of EGFR-mutant lung cancer in women and in East Asian populations: Analysis of estrogen-related polymorphisms. Clin. Cancer Res. 2008, 14, 4079–4084. [Google Scholar] [CrossRef] [PubMed]
- Durant, R.W.; Wenzel, J.A.; Scarinci, I.C.; Paterniti, D.A.; Fouad, M.N.; Hurd, T.C.; Martin, M.Y. Perspectives on barriers and facilitators to minority recruitment for clinical trials among cancer center leaders, investigators, research staff, and referring clinicians: Enhancing minority participation in clinical trials (EMPaCT). Cancer 2014, 120, 1097–1105. [Google Scholar] [CrossRef] [PubMed]
- Klein, S.L.; Morgan, R. The impact of sex and gender on immunotherapy outcomes. Biol. Sex Differ. 2020, 11, 24. [Google Scholar] [CrossRef] [PubMed]
- Unger, J.M.; Vaidya, R.; Hershman, D.L.; Minasian, L.M.; Fleury, M.E. Systematic review and meta-analysis of the magnitude of structural, clinical, and physician and patient barriers to cancer clinical trial participation. J. Natl. Cancer Inst. 2019, 111, 245–255. [Google Scholar] [CrossRef] [PubMed]
- Duma, N.; Kothadia, S.M.; Azam, T.U.; Yadav, S.; Paludo, J.; Vera Aguilera, J.; Gonzalez Velez, M.; Halfdanarson, T.R.; Molina, J.R.; Hubbard, J.M.; et al. Characterization of comorbidities limiting the recruitment of patients in early phase clinical trials. Oncologist 2019, 24, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Idossa, D.; Velazquez Manana, A.I.; Horiguchi, M.; Suero-Abreu, G.A.; Franco, I.I.; Borrero, M.; Patel, S.R.; Dhawan, N.; Florez, N. What is your preferred language? Evaluating equal access to oncology clinical studies for non-English-speaking participants. Am. Soc. Clin. Oncol. 2023, 41, 16. [Google Scholar] [CrossRef]
- Smith, A.; Agar, M.; Delaney, G. Lower trial participation by culturally and linguistically diverse (CALD) cancer patients is largely due to language barriers. Asia-Pac. J. Clin. Oncol. 2018, 14, 52–60. [Google Scholar] [CrossRef]
- Guo, X.M.; Neuman, M.K.; Vallejo, A.; Matsuo, K.; Roman, L.D. An absence of translated consent forms limits oncologic clinical trial enrollment for limited English proficiency participants. Gynecol. Oncol. 2024, 180, 86–90. [Google Scholar] [CrossRef] [PubMed]
- Gray, D.M.; Nolan, T.S.; Gregory, J.; Joseph, J.J. Diversity in clinical trials: An opportunity and imperative for community engagement. Lancet Gastroenterol. Hepatol. 2021, 6, 605–607. [Google Scholar] [CrossRef] [PubMed]
- Boulware, L.E.; Cooper, L.A.; Ratner, L.E.; LaVeist, T.A.; Powe, N.R. Race and trust in the health care system. Public Health Rep. 2003, 118. [Google Scholar] [CrossRef]
- Doescher, M.P.; Saver, B.G.; Franks, P.; Fiscella, K. Racial and Ethnic Disparities in Perceptions of Physician Style and Trust. 2000. Available online: https://repository.escholarship.umassmed.edu/handle/20.500.14038/37165 (accessed on 6 February 2024).
- Huey, R.W.; George, G.C.; Phillips, P.; White, R.; Fu, S.; Janku, F.; Karp, D.D.; Naing, A.; Piha-Paul, S.; Subbiah, V.; et al. Patient-reported out-of-pocket costs and financial toxicity during early-phase oncology clinical trials. Oncologist 2021, 26, 588–596. [Google Scholar] [CrossRef] [PubMed]
- Chino, F.; Zafar, S.Y. Financial toxicity and equitable access to clinical trials. Am. Soc. Clin. Oncol. Educ. Book 2019, 39, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Kahn, J.M.; Gray, D.M., 2nd; Oliveri, J.M.; Washington, C.M.; DeGraffinreid, C.R.; Paskett, E.D. Strategies to improve diversity, equity, and inclusion in clinical trials. Cancer 2022, 128, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Hamel, L.M.; Penner, L.A.; Albrecht, T.L.; Heath, E.; Gwede, C.K.; Eggly, S. Barriers to clinical trial enrollment in racial and ethnic minority patients with cancer. Cancer Control 2016, 23, 327–337. [Google Scholar] [CrossRef] [PubMed]
- Weisman, C.S.; Cassard, S.D.; Mastroianni, A.C.; Faden, R.; Federman, D. Health consequences of exclusion or underrepresentation of women in clinical studies (I). Women Health Res. 1994, 2, 35–40. [Google Scholar]
- Unger, J.M.; Vaidya, R.; Albain, K.S.; LeBlanc, M.; Minasian, L.M.; Gotay, C.C.; Henry, N.L.; Fisch, M.J.; Lee, S.M.; Blanke, C.D.; et al. Sex differences in risk of severe adverse events in patients receiving immunotherapy, targeted therapy, or chemotherapy in cancer clinical trials. J. Clin. Oncol. 2022, 40, 1474. [Google Scholar] [CrossRef] [PubMed]
- Monestime, S.; Page, R.; Jordan, W.M.; Aryal, S. Prevalence and predictors of patients reporting adverse drug reactions to health care providers during oral targeted cancer treatment. J. Am. Pharm. Assoc. 2021, 61, 53–59. [Google Scholar] [CrossRef]
- Dogan, S.; Shen, R.; Ang, D.C.; Johnson, M.L.; D’Angelo, S.P.; Paik, P.K.; Brzostowski, E.B.; Riely, G.J.; Kris, M.G.; Zakowski, M.F.; et al. Molecular Epidemiology of EGFR and KRAS Mutations in 3026 Lung Adenocarcinomas: Higher Susceptibility of Women to Smoking-Related KRAS-Mutant Cancers. Clin. Cancer Res. 2012, 18, 6169–6177. [Google Scholar] [CrossRef] [PubMed]
- Del Pup, L.; Villa, P.; Amar, I.D.; Bottoni, C.; Scambia, G. Approach to sexual dysfunction in women with cancer. Int. J. Gynecol. Cancer 2019, 29, 630–634. [Google Scholar] [CrossRef] [PubMed]
- Duma, N.; Acharya, R.; Wei, Z.; Seaborne, L.; Heisler, C.; Fidler, M.J.; Elkins, I.; Feldman, J.; Moore, A.; King, J.; et al. MA14. 04 Sexual Health Assessment in Women with Lung Cancer (SHAWL) Study. J. Thorac. Oncol. 2022, 17, S93–S94. [Google Scholar] [CrossRef]
- Reese, J.B.; Sorice, K.; Beach, M.C.; Porter, L.S.; Tulsky, J.A.; Daly, M.B.; Lepore, S.J. Patient-provider communication about sexual concerns in cancer: A systematic review. J. Cancer Surviv. 2017, 11, 175–188. [Google Scholar] [CrossRef]
- Walter, J.R.; Xu, S.; Paller, A.S.; Choi, J.N.; Woodruff, T.K. Oncofertility considerations in adolescents and young adults given a diagnosis of melanoma: Fertility risk of Food and Drug Administration–approved systemic therapies. J. Am. Acad. Dermatol. 2016, 75, 528–534. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.A.; Clatot, F.; Demeestere, I.; Lambertini, M.; Morgan, A.; Nelson, S.M.; Peccatori, F.; Cameron, D. Cancer survivorship: Reproductive health outcomes should be included in standard toxicity assessments. Eur. J. Cancer 2021, 144, 310–316. [Google Scholar] [CrossRef]
- Esposito, S.; Tenconi, R.; Preti, V.; Groppali, E.; Principi, N. Chemotherapy against cancer during pregnancy: A systematic review on neonatal outcomes. Medicine 2016, 95, e4899. [Google Scholar] [CrossRef]
- Angarita, A.M.; Johnson, C.A.; Fader, A.N.; Christianson, M.S. Fertility preservation: A key survivorship issue for young women with cancer. Front. Oncol. 2016, 6, 102. [Google Scholar] [CrossRef]
- Duma, N.; Lambertini, M. It is time to talk about fertility and immunotherapy. Oncologist 2020, 25, 277–278. [Google Scholar] [CrossRef]
- Rambhatla, A.; Strug, M.R.; De Paredes, J.G.; Cordoba Munoz, M.I.; Thakur, M. Fertility considerations in targeted biologic therapy with tyrosine kinase inhibitors: A review. J. Assist. Reprod. Genet. 2021, 38, 1897–1908. [Google Scholar] [CrossRef]
- Khan, S.Z.; Arecco, L.; Villarreal-Garza, C.; Sirohi, B.; Ponde, N.F.; Habeeb, B.; Brandão, M.; Azim, H.A., Jr.; Chowdhury, A.R.; Bozovic-Spasojevic, I.; et al. Knowledge, practice, and attitudes of physicians in low-and middle-income countries on fertility and pregnancy-related issues in young women with breast cancer. JCO Glob. Oncol. 2022, 8, e2100153. [Google Scholar] [CrossRef] [PubMed]
- Alshamsan, B.; Kushnir, I.; Al-Saadi, S.; Srikanthan, A. Perceptions and attitudes of medical oncologists regarding fertility preservation and pregnancy in high-risk cancer patients: A survey among Canadian medical oncologists. Cancer Med. 2023, 12, 1912–1921. [Google Scholar] [CrossRef]
- Adams, E.; Hill, E.; Watson, E. Fertility preservation in cancer survivors: A national survey of oncologists’ current knowledge, practice and attitudes. Br. J. Cancer 2013, 108, 1602–1615. [Google Scholar] [CrossRef] [PubMed]
- Peddie, V.L.; Porter, M.A.; Barbour, R.; Culligan, D.; MacDonald, G.; King, D.; Horn, J.; Bhattacharya, S. Factors affecting decision making about fertility preservation after cancer diagnosis: A qualitative study. BJOG Int. J. Obstet. Gynaecol. 2012, 119, 1049–1057. [Google Scholar] [CrossRef] [PubMed]
- Cantero, M.T.R.; Pardo, M.A. European Medicines Agency policies for clinical trials leave women unprotected. J. Epidemiol. Community Health 2006, 60, 911–913. [Google Scholar] [CrossRef] [PubMed]
- Parekh, A.; Fadiran, E.O.; Uhl, K.; Throckmorton, D.C. Adverse effects in women: Implications for drug development and regulatory policies. Expert Rev. Clin. Pharmacol. 2011, 4, 453–466. [Google Scholar] [CrossRef] [PubMed]
- Cortellini, A.; Tucci, M.; Adamo, V.; Stucci, L.S.; Russo, A.; Tanda, E.T.; Spagnolo, F.; Rastelli, F.; Bisonni, R.; Santini, D.; et al. Integrated analysis of concomitant medications and oncological outcomes from PD-1/PD-L1 checkpoint inhibitors in clinical practice. J. Immunother. Cancer 2020, 8, e001361. [Google Scholar] [CrossRef] [PubMed]
- Subramaniapillai, S.; Galea, L.A.; Einstein, G.; de Lange, A.-M.G. Sex and gender in health research: Intersectionality matters. Front. Neuroendocrinol. 2023, 72, 101104. [Google Scholar] [CrossRef]
- Liu, K.A.; Dipietro Mager, N.A. Women’s involvement in clinical trials: Historical perspective and future implications. Pharm. Pract. 2016, 14, 708. [Google Scholar] [CrossRef] [PubMed]
- Peters, U.; Spahn, J.; Patel, S. Carrots or Sticks: An Industry Perspective on the Significance of Regulatory Guidance in Promoting Participant Diversity in Clinical Trials. Int. J. Radiat. Oncol. Biol. Phys. 2023, 116, 115–117. [Google Scholar] [CrossRef]
Figure 1.
Gender-specific challenges of precision oncology are often based on the lack of clinical trial participation for women and our collective lack of knowledge regarding treatment effects on survivorship issues such as sexual health and fertility.
Figure 1.
Gender-specific challenges of precision oncology are often based on the lack of clinical trial participation for women and our collective lack of knowledge regarding treatment effects on survivorship issues such as sexual health and fertility.

Figure 2.
Future directions for precision immuno-oncology research.


{kind=link}
{kind=link}
Table 1.
Studies evaluating the impact of gender on response to immune checkpoint inhibition.
| Study | Type of Study | Sample Size | Cancers Included | Treatment Regimen | Outcome | Sex Differences in OS | Hazard Ratios (If Available) |
|---|---|---|---|---|---|---|---|
| [66] | Meta-Analysis | 11 RCTs | Solid tumors | ICI vs. chemotherapy | OS, PFS | No significant difference in males and females noted for OS or PFS | Anti-PD1: OS (males vs. females: HR 0.72, 95% CI 0.64–0.83 vs. HR 0.81, 95% CI 0.70–0.94, p = 0.285) Anti PD-1 PFS: (males vs. females: HR 0.66, 95% CI 0.52–0.82 vs. HR 0.85, 95% CI 0.66–1.09, p =0.158). |
| [67] | Systematic Review & Meta-Analysis | 21 RCTs, 26,598 patients | Solid tumors | ICI alone or with chemotherapy vs. chemotherapy | OS, PFS | Similar OS in males and females for anti-PD-1/PDL-1. Anti-CTLA-4 use was associated with longer OS in men only | OS: Females (HR, 0.77; 95% CI 0.67–0.89, p < 0.001) Males (HR, 0.73; 95% CI 0.66–0.80, p < 0.001) |
| [53] | Meta-Analysis | 20 RCTs, 11,351 patients | Solid tumors | CTLA-4 or PD-1 inhibitors vs. chemotherapy | OS | Men experienced longer OS when compared to females | OS: Women (HR, 0.86; 95% CI 0.79–0.93), Male (HR, 0.72; 95% CI 0.65–0.79) |
| [58] | Meta-Analysis | 8 RCTs, 574 NSCLC patients | NSCLC | PD-L1 or PD-L1 alone or with chemotherapy vs. chemotherapy | OS, PFS | Women had better OS with PD-1 and chemotherapy combination when compared to Males. Males had a better OS in the immunotherapy alone arm | OS PD-1/PD-L1 alone: Females (HR, 0.97; 95% CI = 0.79 to 1.19), Male (HR, 0.78 (95% CI = 0.60 to 1.00) OS combination: Females (HR, 0.44 95% CI = 0.25 to 0.76), Male (HR, 0.76; 95% CI = 0.64 to 0.91) |
| [65] | Meta-Analysis | 23 RCTs, 13,271 patients | Solid Tumors | ICI vs. standard therapies | OS | Benefit noted in both men and women with no statistical difference noted between the sexes | OS: Females (HR, 0.77; 95% CI, 0.67–0.88; p = 0.002), Men (HR, 0.75; 95% CI, 0.69–0.81; p < 0.001) |
| [60] | Meta-Analysis | 11 RCTs, 6096 patients | Solid tumors, (4 lung cancer RCTs) | CTLA-4 or PD-1 inhibitors vs. chemotherapy | OS, PFS | Better PFS and OS seen in males vs. females treated with ICI. However, this was not noted in the NSCLC cohort. | OS: Females (HR = 0.74; 95% CI, 0.65–0.84; p < 0.001) Males (HR = 0.62; 95% CI, 0.53–0.71, p < 0.001) |
| [59] | Meta-Analysis | 16 RCTs, 10,155 patients | NSCLC | ICI alone or with chemotherapy vs. chemotherapy alone | OS | Those who received ICIs (with or without chemotherapy) had longer OS than those who did not receive ICIs and was comparable between both genders | Overall: Females (HR: 0.74, 95%Cl 0.63–0.87), Males (HR: 0.76, 95%Cl 0.71–0.81) ICI + Chemo: females (HR: 0.63, 95%Cl 0.42–0.92), males (HR: 0.79, 95%Cl 0.70–0.89) ICI alone: Females (HR: 0.83, 95%Cl 0.73–0.95), Males (HR: 0.74, 95%Cl 0.67–0.81) |
| [68] | Meta-Analysis | 15 RCTs, 9583 patients | Lung cancer | ICI alone or with chemotherapy vs. chemotherapy alone | OS, PFS | Both females and males benefited from anti-PD-1 therapies and benefit was seen only for males with anti-PD-L1 therapies. | Anti-PD-1: Females (HR = 0.69, 95% CI, 0.52–0.93) Males (HR = 0.73, 95% CI, 0.67–0.80) Anti-PD-L1: Females (HR = 0.69, 95% CI, 0.44–1.07), Males: (HR = 0.80, 95% CI, 0.69–0.92) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Marks, J.; Sridhar, A.; Ai, A.; Kiel, L.; Kaufman, R.; Abioye, O.; Mantz, C.; Florez, N. Precision Immuno-Oncology in NSCLC through Gender Equity Lenses. Cancers 2024, 16, 1413. https://doi.org/10.3390/cancers16071413
AMA Style
Marks J, Sridhar A, Ai A, Kiel L, Kaufman R, Abioye O, Mantz C, Florez N. Precision Immuno-Oncology in NSCLC through Gender Equity Lenses. Cancers. 2024; 16(7):1413. https://doi.org/10.3390/cancers16071413
Chicago/Turabian StyleMarks, Jennifer, Arthi Sridhar, Angela Ai, Lauren Kiel, Rebekah Kaufman, Oyepeju Abioye, Courtney Mantz, and Narjust Florez. 2024. "Precision Immuno-Oncology in NSCLC through Gender Equity Lenses" Cancers 16, no. 7: 1413. https://doi.org/10.3390/cancers16071413
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.