
Late Relapse after Allogeneic Stem Cell Transplantation in Patients Treated for Acute Myeloid Leukemia: Relapse Incidence, Characteristics, Role of Conditioning Regimen, and Outcome

 , , , , and
, , , , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Patient Selection
2.2. Treatment Characteristics
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Outcome and Factors Affecting Survival, Relapse, and TRM
3.3. Factors Associated with Late Relapse
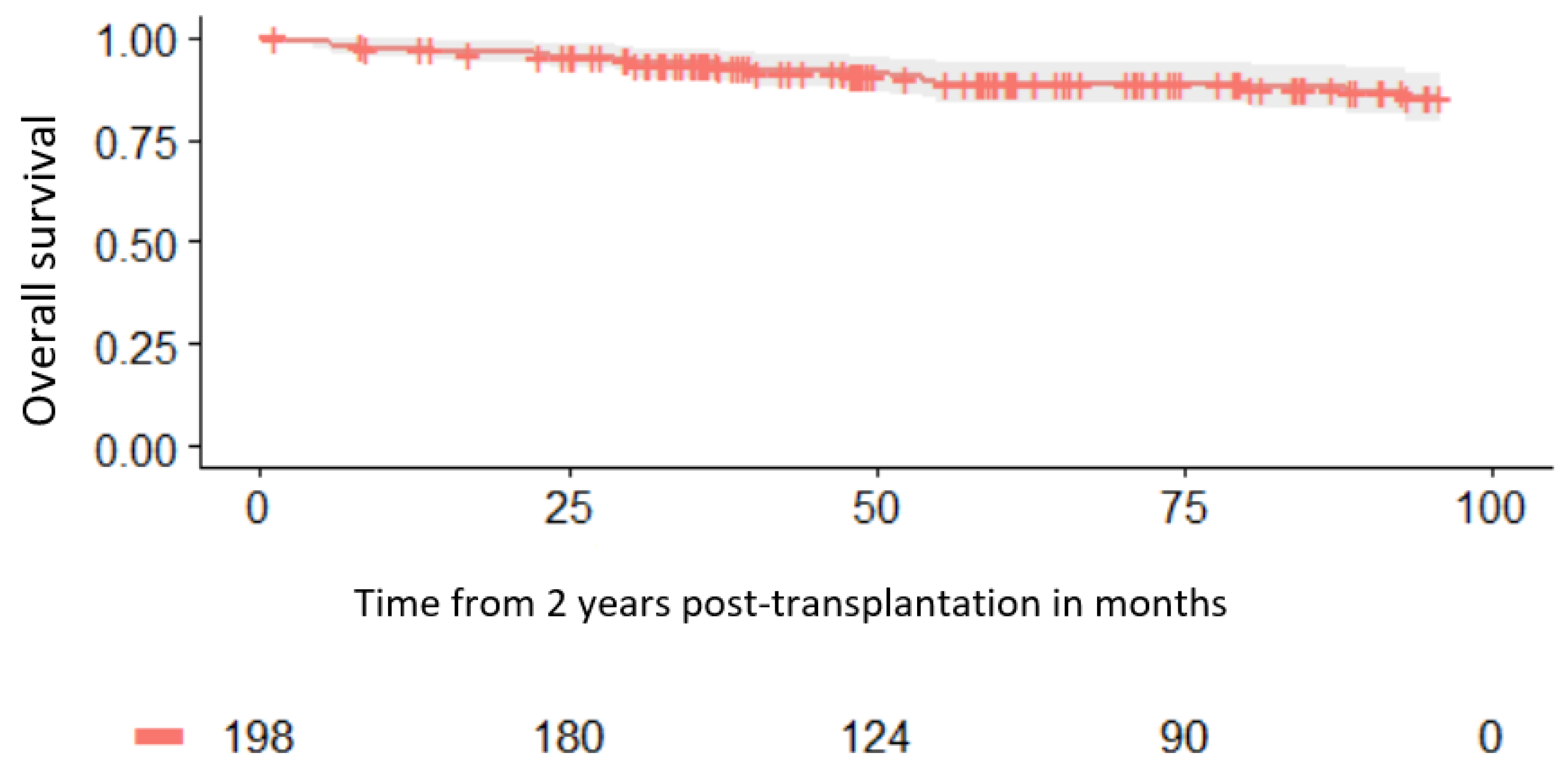
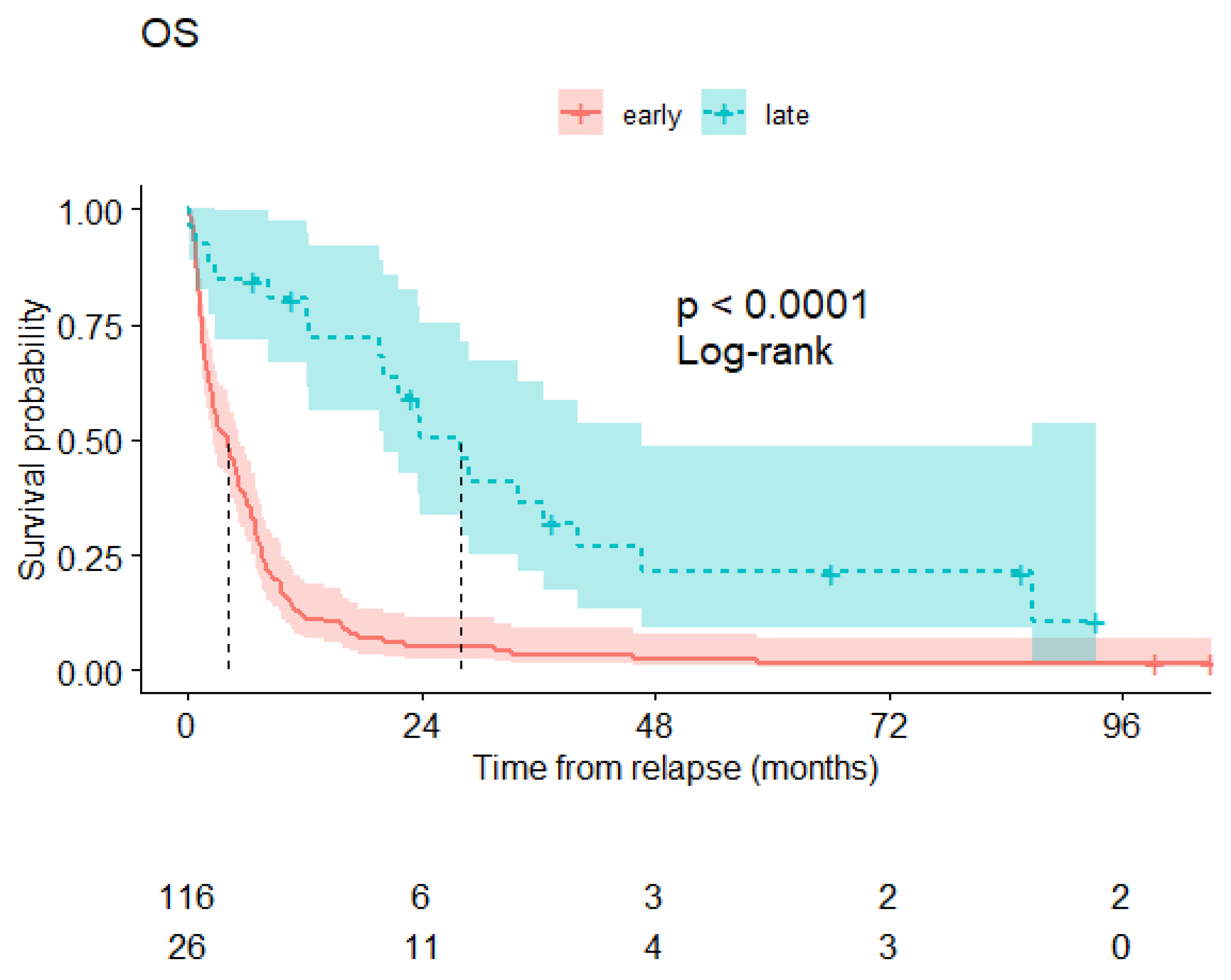
3.4. Survival of Patients beyond 2 Years from Transplantation
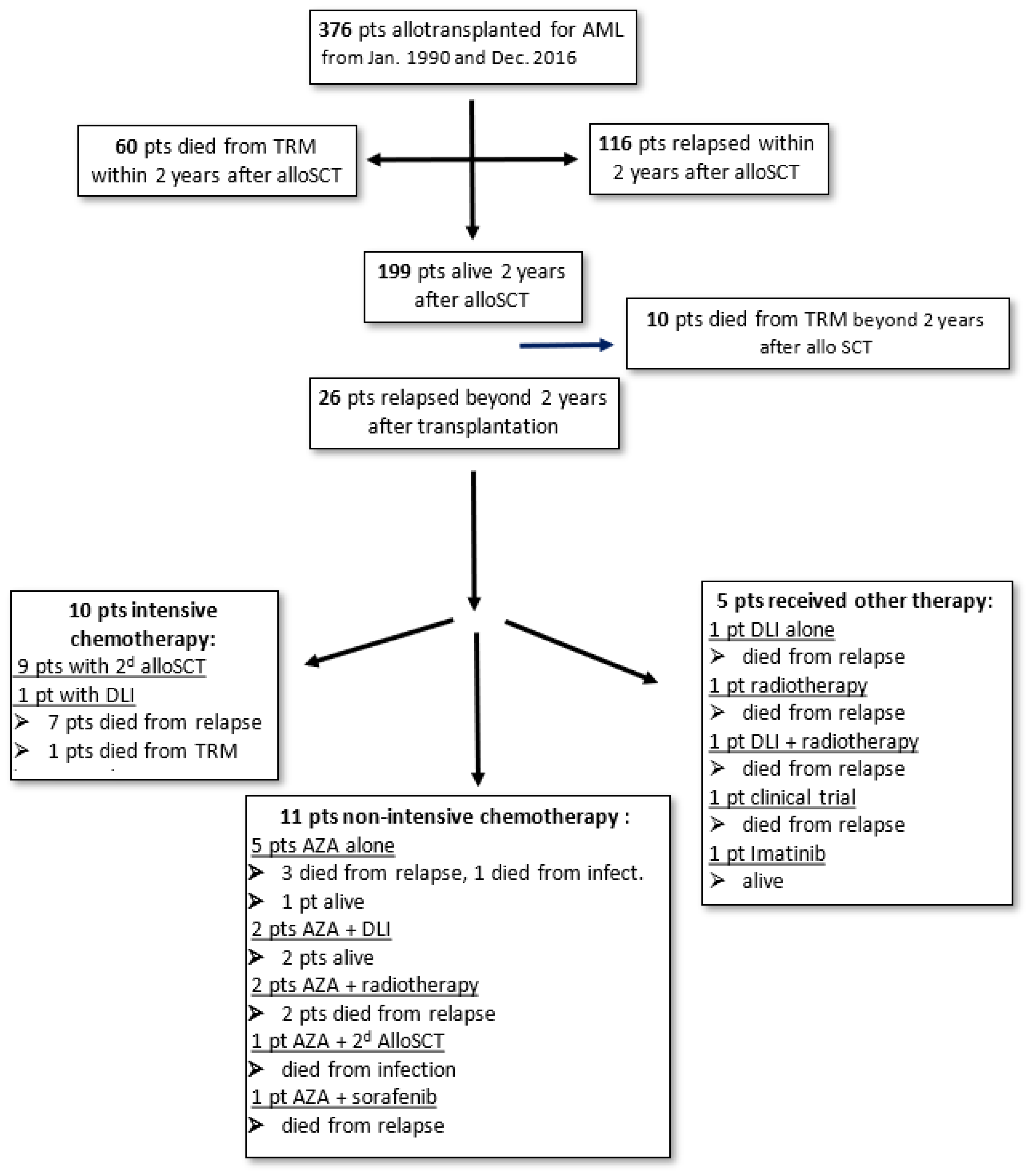
3.5. Treatment of Late AML Relapse
3.6. Cytogenetic Characteristics at Late Relapse
3.7. Chimerism at Relapse
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Horowitz, M.; Schreiber, H.; Elder, A.; Heidenreich, O.; Vormoor, J.; Toffalori, C.; Vago, L.; Kröger, N. Epidemiology and Biology of Relapse After Stem Cell Transplantation. Bone Marrow Transplant. 2018, 53, 1379–1389. [Google Scholar] [CrossRef] [PubMed]
- Yanada, M.; Konuma, T.; Mizuno, S.; Saburi, M.; Shinohara, A.; Tanaka, M.; Marumo, A.; Sawa, M.; Uchida, N.; Ozawa, Y.; et al. Predicting non-relapse mortality following allo-geneic hematopoietic cell transplantation during first remission of acute myeloid leukemia. Bone Marrow Transplant. 2021, 56, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Bejanyan, N.; Weisdorf, D.J.; Logan, B.R.; Wang, H.L.; Devine, S.M.; de Lima, M.; Bunjes, D.W.; Zhang, M.J. Survival of patients with acute myeloid leukemia relapsing after allogeneic hematopoietic cell transplantation: A center for international blood and marrow transplant research study. Biol. Blood Marrow Transplant. 2015, 21, 454–459. [Google Scholar] [CrossRef] [PubMed]
- Craddock, C.; Versluis, J.; Labopin, M.; Socie, G.; Huynh, A.; Deconinck, E.; Volin, L.; Milpied, N.; Bourhis, J.H.; Rambaldi, A.; et al. Distinct factors determine the kinetics of disease relapse in adults transplanted for acute myeloid leukaemia. J. Intern. Med. 2018, 283, 371–379. [Google Scholar] [CrossRef] [PubMed]
- Verma, D.; Kantarjian, H.; Faderl, S.; O’Brien, S.; Pierce, S.; Vu, K.; Freireich, E.; Keating, M.; Cortes, J.; Ravandi, F. Late relapses in acute myeloid leukemia: Analysis of characteristics and outcome. Leuk. Lymphoma 2010, 51, 778–782. [Google Scholar] [CrossRef] [PubMed]
- Arber, D.A.; Orazi, A.; Hasserjian, R.; Thiele, J.; Borowitz, M.J.; Le Beau, M.M.; Bloomfield, C.D.; Cazzola, M.; Vardiman, J.W. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood 2016, 127, 2391–2405. [Google Scholar] [CrossRef] [PubMed]
- Döhner, H.; Estey, E.; Grimwade, D.; Amadori, S.; Appelbaum, F.R.; Büchner, T.; Dombret, H.; Ebert, B.L.; Fenaux, P.; Larson, R.A.; et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood 2017, 129, 424–447. [Google Scholar] [CrossRef] [PubMed]
- Bacigalupo, A.; Ballen, K.; Rizzo, D.; Giralt, S.; Lazarus, H.; Ho, V.; Apperley, J.; Slavin, S.; Pasquini, M.; Sandmaier, B.M.; et al. Defining the intensity of conditioning regimens: Working definitions. Biol. Blood Marrow Transplant. 2009, 15, 1628–1633. [Google Scholar] [CrossRef]
- Giralt, S.; Ballen, K.; Rizzo, D.; Bacigalupo, A.; Horowitz, M.; Pasquini, M.; Sandmaier, B. Reduced intensity conditioning regimen workshop: Defining the dose spectrum. Report of a workshop convened by the center for international blood and marrow transplant research. Biol. Blood Marrow Transplant. 2009, 15, 367–369. [Google Scholar] [CrossRef]
- Wingard, J.R.; Majhail, N.S.; Brazauskas, R.; Wang, Z.; Sobocinski, K.A.; Jacobsohn, D.; Sorror, M.L.; Horowitz, M.M.; Bolwell, B.; Rizzo, J.D.; et al. Long-term survival and late deaths after allogeneic hematopoietic cell transplantation. J. Clin. Oncol. 2011, 29, 2230–2239. [Google Scholar] [CrossRef]
- Shimoni, A.; Kröger, N.; Zabelina, T.; Ayuk, F.; Hardan, I.; Yeshurun, M.; Shem-Tov, N.; Avigdor, A.; Ben-Bassat, I.; Zander, A.R.; et al. Hematopoietic stem-cell transplantation from unrelated donors in elderly patients (age >55 years) with hematologic malignancies: Older age is no longer a contraindication when using reduced intensity conditioning. Leukemia 2005, 19, 7–12. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Martino, R.; Iacobelli, S.; Brand, R.; Jansen, T.; van Biezen, A.; Finke, J.; Bacigalupo, A.; Beelen, D.; Reiffers, J.; Devergie, A.; et al. Retrospective comparison of reduced-intensity conditioning and conventional high-dose conditioning for allogeneic hematopoietic stem cell transplantation using HLA-identical sibling donors in myelodysplastic syndromes. Blood 2006, 108, 836–846. [Google Scholar] [CrossRef]
- Alyea, E.P.; Kim, H.T.; Ho, V.; Cutler, C.; DeAngelo, D.J.; Stone, R.; Ritz, J.; Antin, J.H.; Soiffer, R.J. Impact of conditioning regimen intensity on outcome of allogeneic hematopoietic cell transplantation for advanced acute myelogenous leukemia and myelodysplastic syndrome. Biol. Blood Marrow Transplant. 2006, 12, 1047–1055. [Google Scholar] [CrossRef] [PubMed]
- Flynn, C.M.; Hirsch, B.; Defor, T.; Barker, J.N.; Miller, J.S.; Wagner, J.E.; Blazar, B.R.; Burns, L.J.; Macmillan, M.L.; Arora, M.; et al. Reduced intensity compared with high dose conditioning for allotransplantation in acute myeloid leukemia and myelodysplastic syndrome: A comparative clinical analysis. Am. J. Hematol. 2007, 82, 867–872. [Google Scholar] [CrossRef] [PubMed]
- Ringdén, O.; Labopin, M.; Ehninger, G.; Niederwieser, D.; Olsson, R.; Basara, N.; Finke, J.; Schwerdtfeger, R.; Eder, M.; Bunjes, D.; et al. Reduced intensity conditioning compared with myeloablative conditioning using unrelated donor transplants in patients with acute myeloid leukemia. J Clin Oncol. 2009, 27, 4570–4577. [Google Scholar] [CrossRef] [PubMed]
- Scott, B.L.; Pasquini, M.C.; Fei, M.; Fraser, R.; Wu, J.; Devine, S.M.; Porter, D.L.; Maziarz, R.T.; Warlick, E.; Fernandez, H.F.; et al. Myeloablative versus reduced-intensity conditioning for hematopoietic cell transplantation in acute myelogenous leukemia and myelodysplastic syndromes—Long-term follow-up of the BMT CTN 0901 Clinical Trial. Transplant Cell Ther. 2021, 27, 483.e1–483.e6. [Google Scholar] [CrossRef] [PubMed]
- Bornhäuser, M.; Kienast, J.; Trenschel, R.; Burchert, A.; Hegenbart, U.; Stadler, M.; Baurmann, H.; Schäfer-Eckart, K.; Holler, E.; Kröger, N.; et al. Reduced-intensity conditioning versus standard conditioning before allogeneic haemopoietic cell transplantation in patients with acute myeloid leukaemia in first complete remission: A prospective, open-label randomised phase 3 trial. Lancet Oncol. 2012, 13, 1035–1044. [Google Scholar] [CrossRef] [PubMed]
- Kröger, N.; Iacobelli, S.; Franke, G.N.; Platzbecker, U.; Uddin, R.; Hübel, K.; Scheid, C.; Weber, T.; Robin, M.; Stelljes, M.; et al. Dose-Reduced Versus Standard Conditioning Followed by Allogeneic Stem-Cell Transplantation for Patients With Myelodysplastic Syndrome: A Prospective Randomized Phase III Study of the EBMT (RICMAC Trial). J. Clin. Oncol. 2017, 35, 2157–2164. [Google Scholar] [CrossRef]
- Lee, K.H.; Lee, J.H.; Choi, S.J.; Lee, J.H.; Kim, S.; Seol, M.; Lee, Y.S.; Kim, W.K.; Seo, E.J.; Park, C.J.; et al. Bone marrow vs extramedullary relapse of acute leukemia after allogeneic hematopoietic cell transplantation: Risk factors and clinical course. Bone Marrow Transplant. 2003, 32, 835–842. [Google Scholar] [CrossRef]
- Cunningham, I. Extramedullary sites of leukemia relapse after transplant. Leuk. Lymphoma 2006, 47, 1754–1767. [Google Scholar] [CrossRef]
- Watts, J.M.; Wang, X.V.; Swords, R.T.; Paietta, E.; Douer, D.; Lugar, S.M.; Fernandez, H.F.; Rowe, J.M.; Lazarus, H.M.; Tallman, M.S.; et al. Very late relapse of AML after allogeneic hematopoietic cell transplantation is often extramedullary. Bone Marrow Transplant. 2016, 51, 1013–1015. [Google Scholar] [CrossRef] [PubMed]
- Shem-Tov, N.; Saraceni, F.; Danylesko, I.; Shouval, R.; Yerushalmi, R.; Nagler, A.; Shimoni, A. Isolated Extramedullary Relapse of Acute Leukemia after Allogeneic Stem Cell Transplantation: Different Kinetics and Better Prognosis than Systemic Relapse. Biol. Blood Marrow Transplant. 2017, 23, 1087–1094. [Google Scholar] [CrossRef] [PubMed]
- Harris, A.C.; Kitko, C.L.; Couriel, D.R.; Braun, T.M.; Choi, S.W.; Magenau, J.; Mineishi, S.; Pawarode, A.; Yanik, G.; Levine, J.E. Extramedullary relapse of acute myeloid leukemia following allogeneic hematopoietic stem cell transplantation: Incidence, risk factors and outcomes. Haematologica 2013, 98, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Ding, L.; Ley, T.J.; Larson, D.E.; Miller, C.A.; Koboldt, D.C.; Welch, J.S.; Ritchey, J.K.; Young, M.A.; Lamprecht, T.; McLellan, M.D.; et al. Clonal evolution in relapsed acute myeloid leukaemia revealed by whole-genome sequencing. Nature 2012, 481, 506–510. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, M.; Wang, F.; Loghavi, S.; Bueso-Ramos, C.; Gumbs, C.; Little, L.; Song, X.; Zhang, J.; Kadia, T.; Borthakur, G.; et al. Late relapse in acute myeloid leukemia (AML): Clonal evolution or therapy-related leukemia? Blood Cancer J. 2019, 9, 7. [Google Scholar] [CrossRef] [PubMed]
- Christopher, M.J.; Petti, A.A.; Rettig, M.P.; Miller, C.A.; Chendamarai, E.; Duncavage, E.J.; Klco, J.M.; Helton, N.M.; O’Laughlin, M.; Fronick, C.C.; et al. Immune Escape of Relapsed AML Cells after Allogeneic Transplantation. N. Engl. J. Med. 2018, 379, 2330–2341. [Google Scholar] [CrossRef]
- Toffalori, C.; Zito, L.; Gambacorta, V.; Riba, M.; Oliveira, G.; Bucci, G.; Barcella, M.; Spinelli, O.; Greco, R.; Crucitti, L.; et al. Immune signature drives leukemia escape and relapse after hematopoietic cell transplantation. Nat. Med. 2019, 25, 603–611. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| n = 376 | % | |
|---|---|---|
| Gender | ||
| Male | 194 | 51.6% |
| Female | 182 | 48.4% |
| Median age (range) | 48.8 y (18.4–71.0) | |
| ELN classification | ||
| Favorable | 41 | 10.9% |
| Intermediate | 159 | 42.3% |
| Unfavorable | 105 | 27.9% |
| NA | 71 | 18.9% |
| Status at grafting | ||
| CR | 304 | 80.9% |
| Refractory | 72 | 19.1% |
| Type of donor | ||
| Identical sibling | 177 | 47.1% |
| Matched unrelated | 124 | 33% |
| Haplo-identical | 16 | 4.3% |
| Mismatched unrelated 9/10 | 23 | 6.1% |
| Cord blood | 36 | 9.6% |
| Type of graft | ||
| PBSC | 244 | 64.9% |
| BM | 96 | 25.5% |
| CB | 36 | 9.6% |
| Conditioning | ||
| MAC | 120 | 31.9% |
| RIC | 209 | 55.6% |
| SEQ | 47 | 12.5% |
| Year of transplantation | ||
| Before 2005 | 113 | 30.1% |
| After 2005 | 263 | 69.9% |
| Characteristics | Variable (Percentage) | HR (Univariate) | HR (Multivariate) |
|---|---|---|---|
| Median age at transplant | 48.8 years (18.3–71.0) | 1.01 (1.00–1.02, p = 0.26) | - |
| Gender | |||
| Male | 194 (51.6%) | - | - |
| Female | 182 (48.4%) | 0.68 (0.51–0.90, p = 0.008) | 0.89 (0.65–1.23, p = 0.48) |
| ELN 2017 subgroup | |||
| Favorable | 41 (10.9%) | - | - |
| Intermediate | 159 (42.3%) | 1.26 (0.73–2.16, p = 0.40) | 1.14 (0.66–1.95, p = 0.65) |
| Adverse | 105 (27.9%) | 2.06 (1.20–3.55, p = 0.009) | 1.50 (0.85–2.64, p = 0.16) |
| Status at transplant | |||
| CR | 304 (80.9%) | - | - |
| Refractory | 72 (19.1%) | 3.67 (2.71–4.99, p < 0.001) | 3.75 (1.95–7.22, p < 0.001) |
| Conditioning | |||
| RIC | 209 (55.6%) | - | - |
| MAC | 120 (31.9%) | 1.00 (0.72–1.38, p = 0.99) | 0.82 (0.53–1.26, p = 0.36) |
| Sequential | 47 (12.5%) | 2.80 (1.93–4.06, p < 0.001 | 0.73 (0.37–1.46, p = 0.37) |
| Type of graft | |||
| PBSC | 244 (64.9%) | - | - |
| BM | 96 (25.5%) | 0.87 (0.62–1.22, p = 0.43) | - |
| CB | 36 (9.6%) | 1.06 (0.67–1.68, p = 0.81) | - |
| Type de donor | |||
| MSD | 177 (47.1%) | - | - |
| MUD | 124 (33%) | 1.15 (0.84–1.58, p = 0.39) | - |
| Haplo | 16 (4.3%) | 1.49 (0.75–2.97, p = 0.25) | - |
| 9/10 | 23 (6.1%) | 1.26 (0.71–2.27, p = 0.43) | - |
| CB | 36 (9.6%) | 1.20 (0.74–1.93, p = 0.46) | - |
| Characteristics | Variable (Percentage) | HR (Univariate) | HR (Multivariate) |
|---|---|---|---|
| Median age at transplant | 48.8 years (18.3–71.0) | 1.01 (1.00–1.02, p = 0.22) | - |
| Gender | |||
| Male | 194 (51.6%) | - | - |
| Female | 182 (48.4%) | 0.70 (0.53–0.92, p = 0.01) | 0.90 (0.66–1.23, p = 0.52) |
| ELN 2017 subgroup | |||
| Favorable | 41 (10.9%) | - | - |
| Intermediate | 159 (42.3%) | 1.29 (0.75–2.20, p = 0.35)) | 1.17 (0.68–2.00, p = 0.58)) |
| Adverse | 105 (27.9%) | 2.24 (1.30–3.85, p = 0.004) | 1.66 (0.95–2.91, p = 0.08) |
| Status at transplant | |||
| CR | 304 (80.9%) | - | - |
| Refractory | 72 (19.1%) | 3.66 (2.70–4.94, p < 0.001) | 3.06 (1.59–5.89, p = 0.001) |
| Conditioning | |||
| RIC | 209 (55.6%) | - | - |
| MAC | 120 (31.9%) | 0.90 (0.65–1.23, p = 0.51) | 0.83 (0.54–1.26, p = 0.37) |
| Sequential | 47 (12.5%) | 2.95 (2.04–4.26, p < 0.001) | 0.90 (0.45–1.80, p = 0.76) |
| Type of graft | |||
| PBSC | 244 (64.9%) | - | - |
| BM | 96 (25.5%) | 0.80 (0.58–1.11, p = 0.19) | - |
| CB | 36 (9.6%) | 1.11 (0.71–1.74, p = 0.65) | - |
| Type de donor | |||
| MSD | 177 (47.1%) | - | - |
| MUD | 124 (33%) | 1.17 (0.86–1.60, p = 0.32) | - |
| Haplo | 16 (4.3%) | 1.34 (0.68–2.67, p = 0.40) | - |
| 9/10 | 23 (6.1%) | 1.43 (0.83–2.47, p = 0.20) | - |
| CB | 36 (9.6%) | 1.30 (0.82–2.08, p = 0.26) | - |
| Period of Time Post-Transplant | Relapses N = 142 (37.7%) | Patients Alive without Relapse at the End of Each Post-Transplant Year |
|---|---|---|
| First year (months 0 to 12) | 97 relapses/376 (26%) | 222 |
| Second year (months 13 to 24) | 19 relapses/221 (8.1%) | 199 |
| Third year (months 25 to 36) | 13 relapses/198 (7%) | 179 |
| Fourth year (months 37–48) | 4 relapses/179 (2.2%) | 170 |
| Fifth year (months 49–60) | 2 relapses/170 (1.7%) | 147 |
| Sixth year (months 61–72) | 1 relapses/146 (1.3%) | * |
| Seventh year (months 73–84) | 1 relapse/ | * |
| Eighth year (months 85–96) | no relapse/ | * |
| Ninth year (months 97–108) | 3 relapses/ | * |
| Tenth year (months 108–120) | 2 relapses/ | * |
| Characteristics | Late Relapse (n = 26) | No Relapse (n = 170) | p-Value (Chi2 or t-Test) |
|---|---|---|---|
| Median age at transplant | 53.9 | 47.7 | 0.046 |
| Sex | |||
| Male | 9 (34.6%) | 79 (45.7%) | 0.398 |
| Female | 17 (65.4%) | 94 (54.3%) | |
| ELN 2017 subgroup | |||
| Favorable | 2 (7.7%) | 25 (14.5%) | 0.265 |
| Intermediate | 10 (38.5%) | 81 (46.8%) | |
| Adverse | 9 (34.6%) | 32 (18.5%) | |
| NA | 5 (19.2%) | 35 (20.2%) | |
| Status at transplant | |||
| CR | 22 (84.6%) | 163 (94.2%) | 0.169 |
| Active disease | 4 (15.4%) | 10 (5.8%) | |
| Conditioning | |||
| RIC | 16 (61.5%) | 103 (59.5%) | 0.739 |
| MAC | 8 (30.8%) | 62 (35.8%) | |
| Sequential | 2 (7.7%) | 8 (4.6%) | |
| Graft source | |||
| PBSC | 17 (65.4%) | 108 (62.4%) | 0.827 |
| BM | 6 (23.1%) | 49 (28.3%) | |
| CB | 3 (11.5%) | 16 (9.2%) | |
| Type of donor | |||
| MSD | 11 (42.3%) | 86 (49.7%) | 0.516 |
| MUD | 9 (34.6%) | 57 (32.9%) | |
| Haplo | 0 (0%) | 6 (3.5%) | |
| 09/10 | 3 (11.5%) | 8 (4.6%) | |
| Cord blood | 3 (11.5%) | 16 (9.2%) | |
| Acute GVHD | |||
| No | 11 (42.3%) | 85 (49.1%) | 0.801 |
| Grade 1–2 | 12 (46.2%) | 69 (39.9%) | |
| Grade 3–4 | 3 (11.5%) | 19 (11%) | |
| Chronic GVHD | |||
| None | 25 (96.2%) | 129 (74.6%) | 0.028 |
| Extensive | 1 (3.8%) | 44 (25.4%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Antier, C.; Jullien, M.; Tessoulin, B.; Loirat, M.; Peterlin, P.; Garnier, A.; Le Bourgeois, A.; Chevallier, P.; Guillaume, T. Late Relapse after Allogeneic Stem Cell Transplantation in Patients Treated for Acute Myeloid Leukemia: Relapse Incidence, Characteristics, Role of Conditioning Regimen, and Outcome. Cancers 2024, 16, 1419. https://doi.org/10.3390/cancers16071419
Antier C, Jullien M, Tessoulin B, Loirat M, Peterlin P, Garnier A, Le Bourgeois A, Chevallier P, Guillaume T. Late Relapse after Allogeneic Stem Cell Transplantation in Patients Treated for Acute Myeloid Leukemia: Relapse Incidence, Characteristics, Role of Conditioning Regimen, and Outcome. Cancers. 2024; 16(7):1419. https://doi.org/10.3390/cancers16071419
Chicago/Turabian StyleAntier, Chloé, Maxime Jullien, Benoît Tessoulin, Marion Loirat, Pierre Peterlin, Alice Garnier, Amandine Le Bourgeois, Patrice Chevallier, and Thierry Guillaume. 2024. "Late Relapse after Allogeneic Stem Cell Transplantation in Patients Treated for Acute Myeloid Leukemia: Relapse Incidence, Characteristics, Role of Conditioning Regimen, and Outcome" Cancers 16, no. 7: 1419. https://doi.org/10.3390/cancers16071419
APA StyleAntier, C., Jullien, M., Tessoulin, B., Loirat, M., Peterlin, P., Garnier, A., Le Bourgeois, A., Chevallier, P., & Guillaume, T. (2024). Late Relapse after Allogeneic Stem Cell Transplantation in Patients Treated for Acute Myeloid Leukemia: Relapse Incidence, Characteristics, Role of Conditioning Regimen, and Outcome. Cancers, 16(7), 1419. https://doi.org/10.3390/cancers16071419