
Human-Level Differentiation of Medulloblastoma from Pilocytic Astrocytoma: A Real-World Multicenter Pilot Study

 , , , ,
, , , ,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Set
2.2. Image (Pre)Processing
2.3. Model Development
2.4. Statistical Evaluation and Comparison
3. Results
3.1. Patient Characteristics
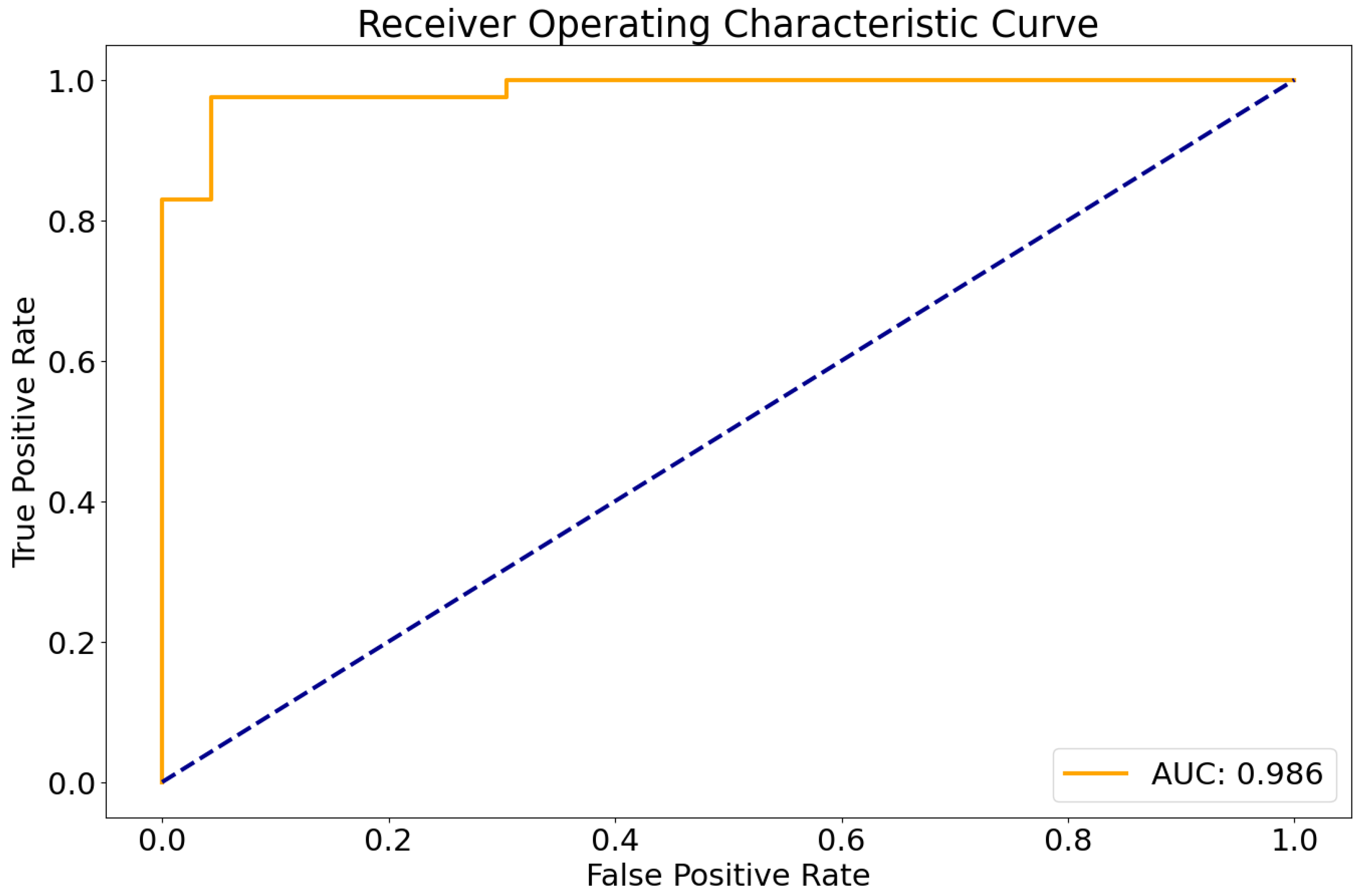
3.2. Deep Learning Results
3.3. Sequence Importance
3.4. Expert Comparison
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Frühwald, M.C.; Rutkowski, S. Tumors of the Central Nervous System in Children and Adolescents. Dtsch. Arzteblatt Int. 2011, 108, 390–397. [Google Scholar] [CrossRef] [PubMed]
- Pollack, I.F.; Agnihotri, S.; Broniscer, A. Childhood Brain Tumors: Current Management, Biological Insights, and Future Directions. J. Neurosurg. Pediatr. 2019, 23, 261–273. [Google Scholar] [CrossRef] [PubMed]
- Avula, S.; Peet, A.; Morana, G.; Morgan, P.; Warmuth-Metz, M.; Jaspan, T.; European Society for Paediatric Oncology (SIOPE)-Brain Tumour Imaging Group. European Society for Paediatric Oncology (SIOPE) MRI Guidelines for Imaging Patients with Central Nervous System Tumours. Childs Nerv. Syst. ChNS 2021, 37, 2497–2508. [Google Scholar] [CrossRef] [PubMed]
- Franceschi, E.; Hofer, S.; Brandes, A.A.; Frappaz, D.; Kortmann, R.-D.; Bromberg, J.; Dangouloff-Ros, V.; Boddaert, N.; Hattingen, E.; Wiestler, B.; et al. EANO-EURACAN Clinical Practice Guideline for Diagnosis, Treatment, and Follow-up of Post-Pubertal and Adult Patients with Medulloblastoma. Lancet Oncol. 2019, 20, e715–e728. [Google Scholar] [CrossRef] [PubMed]
- Mittal, P. Magnetic Resonance Spectroscopy Findings in Non-Enhancing Desmoplastic Medulloblastoma. Ann. Indian Acad. Neurol. 2011, 14, 200–202. [Google Scholar] [CrossRef] [PubMed]
- Fruehwald-Pallamar, J.; Puchner, S.B.; Rossi, A.; Garre, M.L.; Cama, A.; Koelblinger, C.; Osborn, A.G.; Thurnher, M.M. Magnetic Resonance Imaging Spectrum of Medulloblastoma. Neuroradiology 2011, 53, 387–396. [Google Scholar] [CrossRef] [PubMed]
- De Menezes Jarry, V.; Pereira, F.V.; Dalaqua, M.; Duarte, J.Á.; França Junior, M.C.; Reis, F. Common and Uncommon Neuroimaging Manifestations of Ataxia: An Illustrated Guide for the Trainee Radiologist. Part 2—Neoplastic, Congenital, Degenerative, and Hereditary Diseases. Radiol. Bras. 2022, 55, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Xiao, B.; Li, S.; Liu, J. Risk Factors for Survival in Patients With Medulloblastoma: A Systematic Review and Meta-Analysis. Front. Oncol. 2022, 12, 827054. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.H.; Housepian, E.M.; Herbert, C. An Operative Staging System and a Megavoltage Radiotherapeutic Technic for Cerebellar Medulloblastomas. Radiology 1969, 93, 1351–1359. [Google Scholar] [CrossRef]
- Meyers, S.P.; Wildenhain, S.L.; Chang, J.-K.; Bourekas, E.C.; Beattie, P.F.; Korones, D.N.; Davis, D.; Pollack, I.F.; Zimmerman, R.A. Postoperative Evaluation for Disseminated Medulloblastoma Involving the Spine: Contrast-Enhanced MR Findings, CSF Cytologic Analysis, Timing of Disease Occurrence, and Patient Outcomes. Am. J. Neuroradiol. 2000, 21, 1757–1765. [Google Scholar]
- Pati, S.; Baid, U.; Edwards, B.; Sheller, M.; Wang, S.-H.; Reina, G.A.; Foley, P.; Gruzdev, A.; Karkada, D.; Davatzikos, C.; et al. Federated Learning Enables Big Data for Rare Cancer Boundary Detection. Nat. Commun. 2022, 13, 7346. [Google Scholar] [CrossRef] [PubMed]
- Rudie, J.D.; Calabrese, E.; Saluja, R.; Weiss, D.; Colby, J.B.; Cha, S.; Hess, C.P.; Rauschecker, A.M.; Sugrue, L.P.; Villanueva-Meyer, J.E. Longitudinal Assessment of Posttreatment Diffuse Glioma Tissue Volumes with Three-Dimensional Convolutional Neural Networks. Radiol. Artif. Intell. 2022, 4, e210243. [Google Scholar] [CrossRef] [PubMed]
- Kickingereder, P.; Isensee, F.; Tursunova, I.; Petersen, J.; Neuberger, U.; Bonekamp, D.; Brugnara, G.; Schell, M.; Kessler, T.; Foltyn, M.; et al. Automated Quantitative Tumour Response Assessment of MRI in Neuro-Oncology with Artificial Neural Networks: A Multicentre, Retrospective Study. Lancet Oncol. 2019, 20, 728–740. [Google Scholar] [CrossRef] [PubMed]
- Vollmuth, P.; Foltyn, M.; Huang, R.Y.; Galldiks, N.; Petersen, J.; Isensee, F.; van den Bent, M.J.; Barkhof, F.; Park, J.E.; Park, Y.W.; et al. Artificial Intelligence (AI)-Based Decision Support Improves Reproducibility of Tumor Response Assessment in Neuro-Oncology: An International Multi-Reader Study. Neuro Oncol. 2023, 25, 533–543. [Google Scholar] [CrossRef] [PubMed]
- Wen, P.Y.; van den Bent, M.; Youssef, G.; Cloughesy, T.F.; Ellingson, B.M.; Weller, M.; Galanis, E.; Barboriak, D.P.; de Groot, J.; Gilbert, M.R.; et al. RANO 2.0: Update to the Response Assessment in Neuro-Oncology Criteria for High- and Low-Grade Gliomas in Adults. J. Clin. Oncol. 2023, 41, JCO2301059. [Google Scholar] [CrossRef]
- Erker, C.; Tamrazi, B.; Poussaint, T.Y.; Mueller, S.; Mata-Mbemba, D.; Franceschi, E.; Brandes, A.A.; Rao, A.; Haworth, K.B.; Wen, P.Y.; et al. Response Assessment in Paediatric High-Grade Glioma: Recommendations from the Response Assessment in Pediatric Neuro-Oncology (RAPNO) Working Group. Lancet Oncol. 2020, 21, e317–e329. [Google Scholar] [CrossRef] [PubMed]
- Fangusaro, J.; Witt, O.; Hernáiz Driever, P.; Bag, A.K.; de Blank, P.; Kadom, N.; Kilburn, L.; Lober, R.M.; Robison, N.J.; Fisher, M.J.; et al. Response Assessment in Paediatric Low-Grade Glioma: Recommendations from the Response Assessment in Pediatric Neuro-Oncology (RAPNO) Working Group. Lancet Oncol. 2020, 21, e305–e316. [Google Scholar] [CrossRef] [PubMed]
- van der Voort, S.R.; Incekara, F.; Wijnenga, M.M.J.; Kapsas, G.; Gahrmann, R.; Schouten, J.W.; Nandoe Tewarie, R.; Lycklama, G.J.; De Witt Hamer, P.C.; Eijgelaar, R.S.; et al. Combined Molecular Subtyping, Grading, and Segmentation of Glioma Using Multi-Task Deep Learning. Neuro Oncol. 2023, 25, 279–289. [Google Scholar] [CrossRef]
- Eichinger, P.; Alberts, E.; Delbridge, C.; Trebeschi, S.; Valentinitsch, A.; Bette, S.; Huber, T.; Gempt, J.; Meyer, B.; Schlegel, J.; et al. Diffusion Tensor Image Features Predict IDH Genotype in Newly Diagnosed WHO Grade II/III Gliomas. Sci. Rep. 2017, 7, 13396. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Chang, K.; Ramkissoon, S.; Tanguturi, S.; Bi, W.L.; Reardon, D.A.; Ligon, K.L.; Alexander, B.M.; Wen, P.Y.; Huang, R.Y. Multimodal MRI Features Predict Isocitrate Dehydrogenase Genotype in High-Grade Gliomas. Neuro Oncol. 2016, 19, 109–117. [Google Scholar] [CrossRef]
- Kickingereder, P.; Neuberger, U.; Bonekamp, D.; Piechotta, P.L.; Götz, M.; Wick, A.; Sill, M.; Kratz, A.; Shinohara, R.T.; Jones, D.T.W.; et al. Radiomic Subtyping Improves Disease Stratification beyond Key Molecular, Clinical, and Standard Imaging Characteristics in Patients with Glioblastoma. Neuro Oncol. 2018, 20, 848–857. [Google Scholar] [CrossRef]
- Zhang, M.; Wong, S.W.; Wright, J.N.; Wagner, M.W.; Toescu, S.; Han, M.; Tam, L.T.; Zhou, Q.; Ahmadian, S.S.; Shpanskaya, K.; et al. MRI Radiogenomics of Pediatric Medulloblastoma: A Multicenter Study. Radiology 2022, 304, 406–416. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wang, L.; Qin, B.; Hu, X.; Xiao, W.; Tong, Z.; Li, S.; Jing, Y.; Li, L.; Zhang, Y. Preoperative Prediction of Sonic Hedgehog and Group 4 Molecular Subtypes of Pediatric Medulloblastoma Based on Radiomics of Multiparametric MRI Combined with Clinical Parameters. Front. Neurosci. 2023, 17, 1157858. [Google Scholar] [CrossRef]
- Rohlfing, T.; Zahr, N.M.; Sullivan, E.V.; Pfefferbaum, A. The SRI24 Multichannel Atlas of Normal Adult Human Brain Structure. Hum. Brain Mapp. 2009, 31, 798–819. [Google Scholar] [CrossRef] [PubMed]
- Modat, M.; Cash, D.M.; Daga, P.; Winston, G.P.; Duncan, J.S.; Ourselin, S. Global Image Registration Using a Symmetric Block-Matching Approach. J. Med. Imaging Bellingham Wash 2014, 1, 024003. [Google Scholar] [CrossRef] [PubMed]
- Isensee, F.; Schell, M.; Pflueger, I.; Brugnara, G.; Bonekamp, D.; Neuberger, U.; Wick, A.; Schlemmer, H.; Heiland, S.; Wick, W.; et al. Automated Brain Extraction of Multisequence MRI Using Artificial Neural Networks. Hum. Brain Mapp. 2019, 40, 4952–4964. [Google Scholar] [CrossRef]
- Kofler, F.; Berger, C.; Waldmannstetter, D.; Lipkova, J.; Ezhov, I.; Tetteh, G.; Kirschke, J.; Zimmer, C.; Wiestler, B.; Menze, B.H. BraTS Toolkit: Translating BraTS Brain Tumor Segmentation Algorithms Into Clinical and Scientific Practice. Front. Neurosci. 2020, 14, 125. [Google Scholar] [CrossRef] [PubMed]
- Baid, U.; Ghodasara, S.; Mohan, S.; Bilello, M.; Calabrese, E.; Colak, E.; Farahani, K.; Kalpathy-Cramer, J.; Kitamura, F.C.; Pati, S.; et al. The RSNA-ASNR-MICCAI BraTS 2021 Benchmark on Brain Tumor Segmentation and Radiogenomic Classification. arXiv 2021, arXiv:2107.02314. [Google Scholar]
- Thomas, M.F.; Kofler, F.; Grundl, L.; Finck, T.; Li, H.; Zimmer, C.; Menze, B.; Wiestler, B. Improving Automated Glioma Segmentation in Routine Clinical Use Through Artificial Intelligence-Based Replacement of Missing Sequences With Synthetic Magnetic Resonance Imaging Scans. Investig. Radiol. 2022, 57, 187–193. [Google Scholar] [CrossRef]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely Connected Convolutional Networks. In Proceedings of the 2017 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017; pp. 2261–2269. [Google Scholar]
- Johnson, R.A.; Miller, I.; Freund, J.E. Miller & Freund’s Probability and Statistics for Engineers; Prentice Hall: Upper Saddle River, NJ, USA, 2011; ISBN 978-0-321-69498-0. [Google Scholar]
- Madhogarhia, R.; Haldar, D.; Bagheri, S.; Familiar, A.; Anderson, H.; Arif, S.; Vossough, A.; Storm, P.; Resnick, A.; Davatzikos, C.; et al. Radiomics and Radiogenomics in Pediatric Neuro-Oncology: A Review. Neuro-Oncol. Adv. 2022, 4, vdac083. [Google Scholar] [CrossRef]
- Arai, K.; Sato, N.; Aoki, J.; Yagi, A.; Taketomi-Takahashi, A.; Morita, H.; Koyama, Y.; Oba, H.; Ishiuchi, S.; Saito, N.; et al. MR Signal of the Solid Portion of Pilocytic Astrocytoma on T2-Weighted Images:Is It Useful for Differentiation from Medulloblastoma? Neuroradiology 2006, 48, 233–237. [Google Scholar] [CrossRef] [PubMed]
- Kurokawa, R.; Kurokawa, M.; Baba, A.; Kim, J.; Capizzano, A.; Bapuraj, J.; Srinivasan, A.; Moritani, T. Differentiation of Pilocytic Astrocytoma, Medulloblastoma, and Hemangioblastoma on Diffusion-Weighted and Dynamic Susceptibility Contrast Perfusion MRI. Medicine 2022, 101, e31708. [Google Scholar] [CrossRef] [PubMed]
- Esa, M.M.M.; Mashaly, E.M.; El-Sawaf, Y.F.; Dawoud, M.M. Diagnostic Accuracy of Apparent Diffusion Coefficient Ratio in Distinguishing Common Pediatric CNS Posterior Fossa Tumors. Egypt. J. Radiol. Nucl. Med. 2020, 51, 76. [Google Scholar] [CrossRef]
- Pemberton, H.G.; Wu, J.; Kommers, I.; Müller, D.M.J.; Hu, Y.; Goodkin, O.; Vos, S.B.; Bisdas, S.; Robe, P.A.; Ardon, H.; et al. Multi-Class Glioma Segmentation on Real-World Data with Missing MRI Sequences: Comparison of Three Deep Learning Algorithms. Sci. Rep. 2023, 13, 18911. [Google Scholar] [CrossRef] [PubMed]
- Dietterich, T. Overfitting and Undercomputing in Machine Learning. ACM Comput. Surv. 1995, 27, 326–327. [Google Scholar] [CrossRef]
- Zhou, H.; Hu, R.; Tang, O.; Hu, C.; Tang, L.; Chang, K.; Shen, Q.; Wu, J.; Zou, B.; Xiao, B.; et al. Automatic Machine Learning to Differentiate Pediatric Posterior Fossa Tumors on Routine MR Imaging. AJNR Am. J. Neuroradiol. 2020, 41, 1279–1285. [Google Scholar] [CrossRef]
- Liu, R.; Elhalawani, H.; Radwan Mohamed, A.S.; Elgohari, B.; Court, L.; Zhu, H.; Fuller, C.D. Stability Analysis of CT Radiomic Features with Respect to Segmentation Variation in Oropharyngeal Cancer. Clin. Transl. Radiat. Oncol. 2020, 21, 11–18. [Google Scholar] [CrossRef]
- Quon, J.L.; Bala, W.; Chen, L.C.; Wright, J.; Kim, L.H.; Han, M.; Shpanskaya, K.; Lee, E.H.; Tong, E.; Iv, M.; et al. Deep Learning for Pediatric Posterior Fossa Tumor Detection and Classification: A Multi-Institutional Study. AJNR Am. J. Neuroradiol. 2020, 41, 1718–1725. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A Summary. Neuro-Oncology 2021, 23, 1231–1251. [Google Scholar] [CrossRef]
- Kazerooni, A.F.; Khalili, N.; Liu, X.; Haldar, D.; Jiang, Z.; Anwar, S.M.; Albrecht, J.; Adewole, M.; Anazodo, U.; Anderson, H.; et al. The Brain Tumor Segmentation (BraTS) Challenge 2023: Focus on Pediatrics (CBTN-CONNECT-DIPGR-ASNR-MICCAI BraTS-PEDs). arXiv 2023, arXiv:2305.17033v2. [Google Scholar]
- Zhang, S.; Xu, Y.; Usuyama, N.; Bagga, J.; Tinn, R.; Preston, S.; Rao, R.; Wei, M.; Valluri, N.; Wong, C.; et al. Large-Scale Domain-Specific Pretraining for Biomedical Vision-Language Processing. arXiv 2023, arXiv:2303.00915. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Accuracy | F1 | MCC | * | |
|---|---|---|---|---|
| DL Model | 0.97 | 0.96 | 0.93 | |
| Expert Rater 1 | 1 | 1 | 1 | |
| Expert Rater 2 | 0.97 | 0.96 | 0.93 | |
| Pediatric Radiologist | 0.92 | 0.91 | 0.82 | |
| Resident 1 | 0.87 | 0.86 | 0.72 | * |
| Resident 2 | 0.84 | 0.81 | 0.66 | * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wiestler, B.; Bison, B.; Behrens, L.; Tüchert, S.; Metz, M.; Griessmair, M.; Jakob, M.; Schlegel, P.-G.; Binder, V.; von Luettichau, I.; et al. Human-Level Differentiation of Medulloblastoma from Pilocytic Astrocytoma: A Real-World Multicenter Pilot Study. Cancers 2024, 16, 1474. https://doi.org/10.3390/cancers16081474
Wiestler B, Bison B, Behrens L, Tüchert S, Metz M, Griessmair M, Jakob M, Schlegel P-G, Binder V, von Luettichau I, et al. Human-Level Differentiation of Medulloblastoma from Pilocytic Astrocytoma: A Real-World Multicenter Pilot Study. Cancers. 2024; 16(8):1474. https://doi.org/10.3390/cancers16081474
Chicago/Turabian StyleWiestler, Benedikt, Brigitte Bison, Lars Behrens, Stefanie Tüchert, Marie Metz, Michael Griessmair, Marcus Jakob, Paul-Gerhardt Schlegel, Vera Binder, Irene von Luettichau, and et al. 2024. "Human-Level Differentiation of Medulloblastoma from Pilocytic Astrocytoma: A Real-World Multicenter Pilot Study" Cancers 16, no. 8: 1474. https://doi.org/10.3390/cancers16081474
APA StyleWiestler, B., Bison, B., Behrens, L., Tüchert, S., Metz, M., Griessmair, M., Jakob, M., Schlegel, P.-G., Binder, V., von Luettichau, I., Metzler, M., Johann, P., Hau, P., & Frühwald, M. (2024). Human-Level Differentiation of Medulloblastoma from Pilocytic Astrocytoma: A Real-World Multicenter Pilot Study. Cancers, 16(8), 1474. https://doi.org/10.3390/cancers16081474