

Plasma IL-1 and IL-6 Family Cytokines with Soluble Receptor Levels at Diagnosis in Head and Neck Squamous Cell Carcinoma: High Levels Predict Decreased Five-Year Disease-Specific and Overall Survival
 ,
, 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients Included in the Study
2.2. Laboratory Analyses
2.3. Tobacco History Scores
2.4. Statistical Analyses
3. Results
3.1. Patients Included in the Study
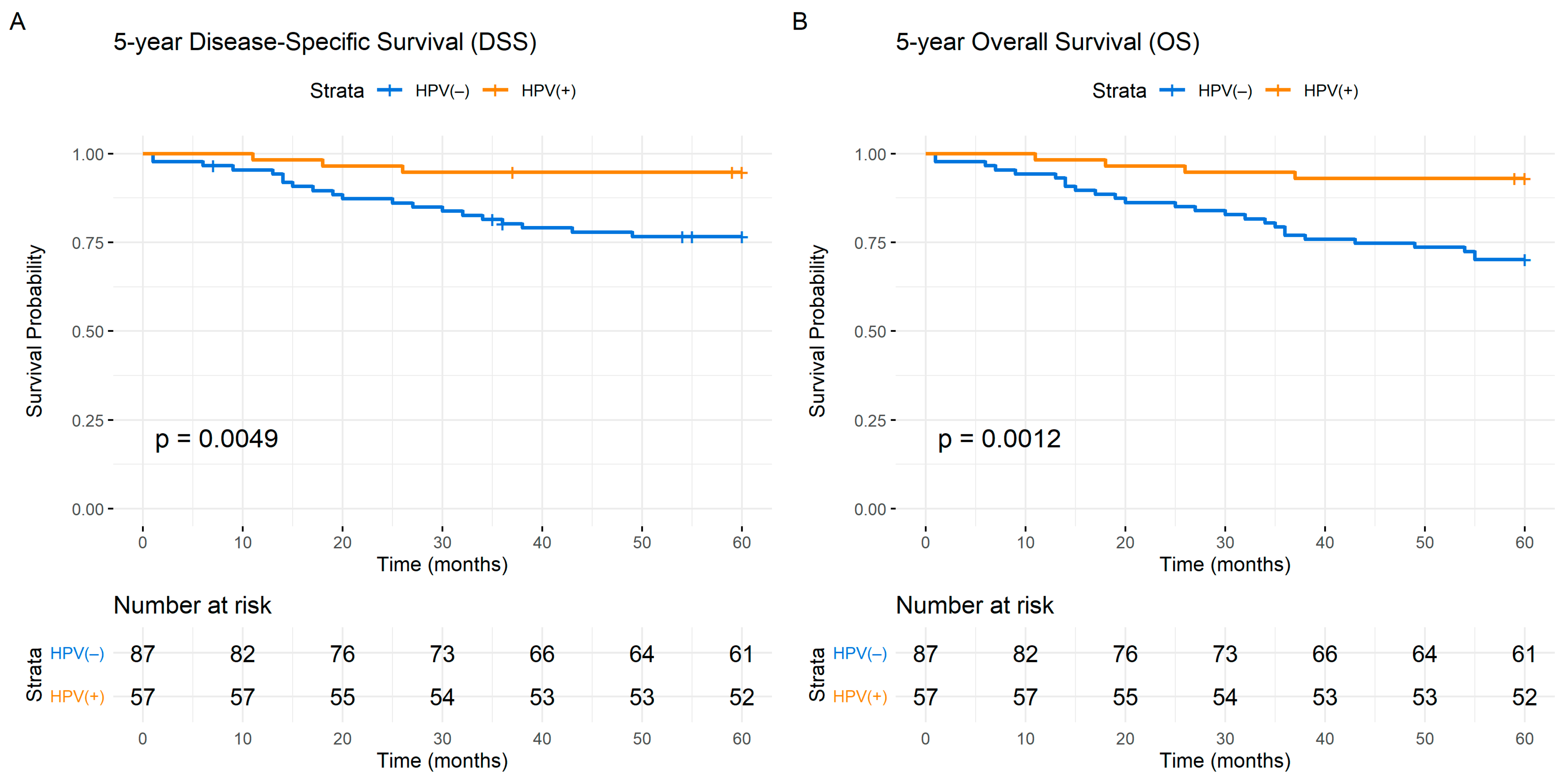
3.1.1. Five-Year Survival among HPV(+) Patients
3.1.2. Correlation between Cytokines/Soluble Receptors, Age, TNM Stage, Smoking History and CRP Levels
3.1.3. DSS from Clinical Parameters
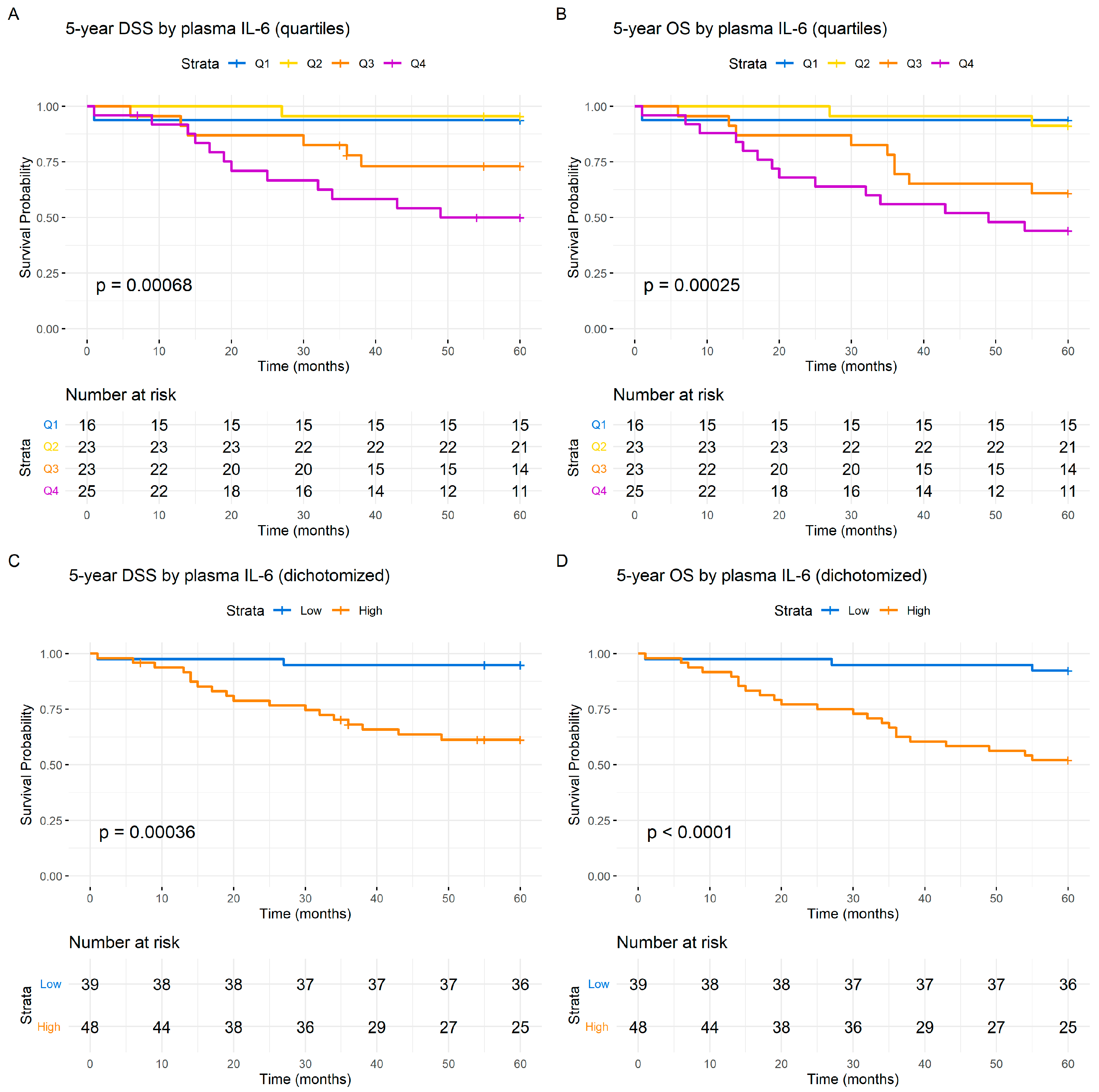
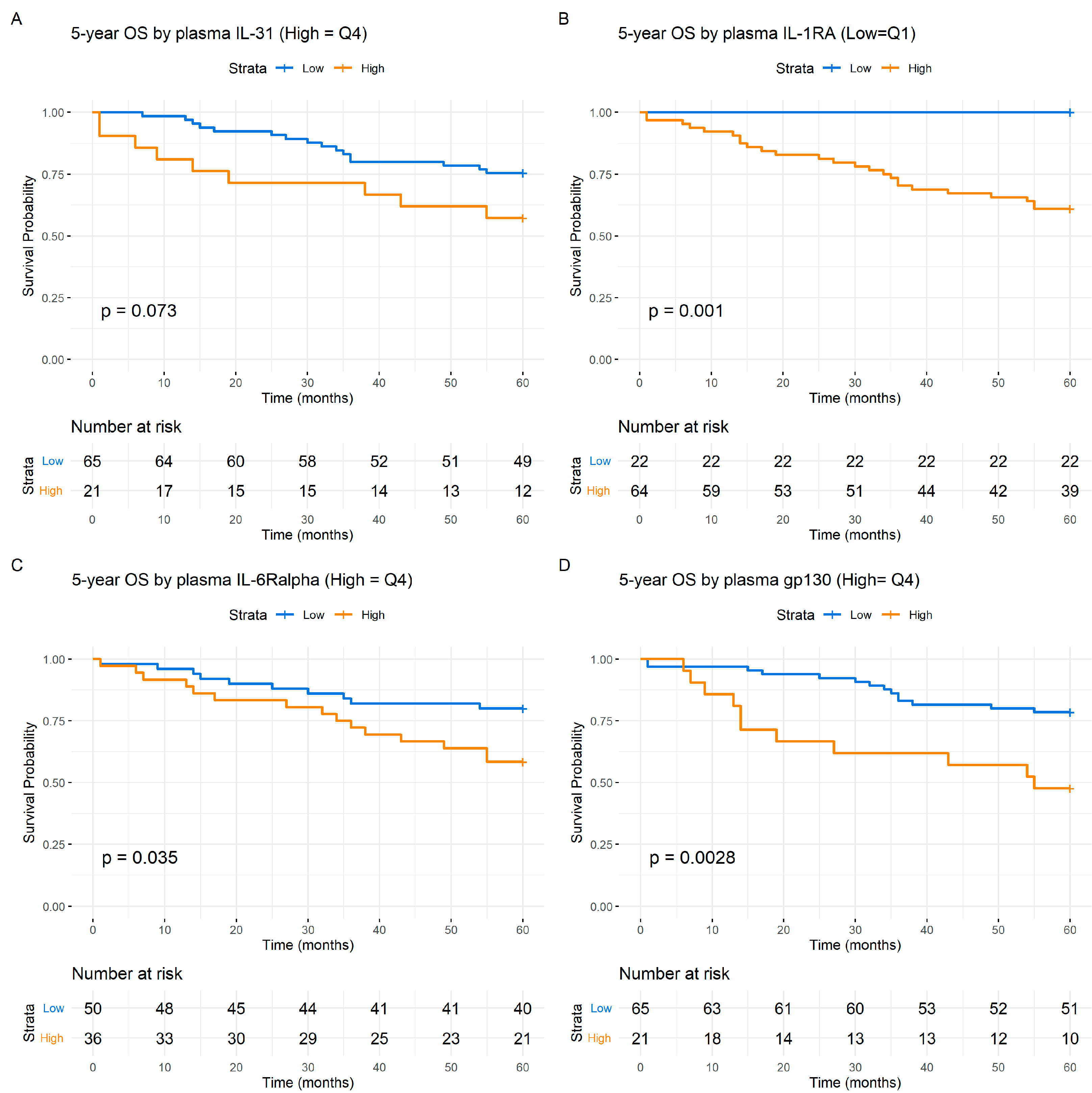
3.1.4. Individual Acute-Phase Cytokines and Soluble Cytokine Receptors Are Associated with Prognosis in HNSCC
3.1.5. Prognostic Five-Year Survival Analyses by Individual Cytokine and Soluble Cytokine Receptors Using Cox Regression Analysis
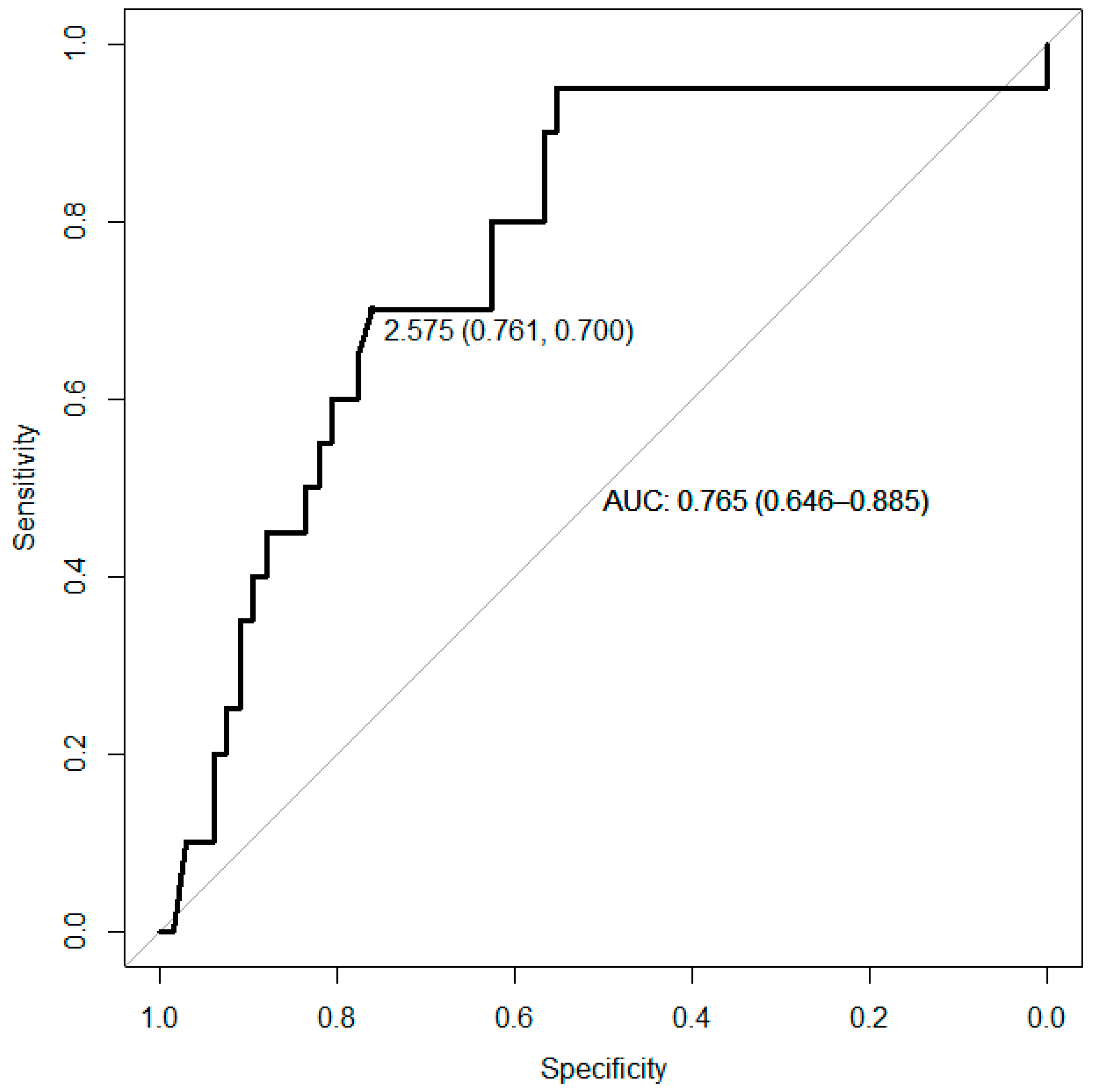
3.1.6. Receiver Operating Characteristic (ROC) Curve Analysis
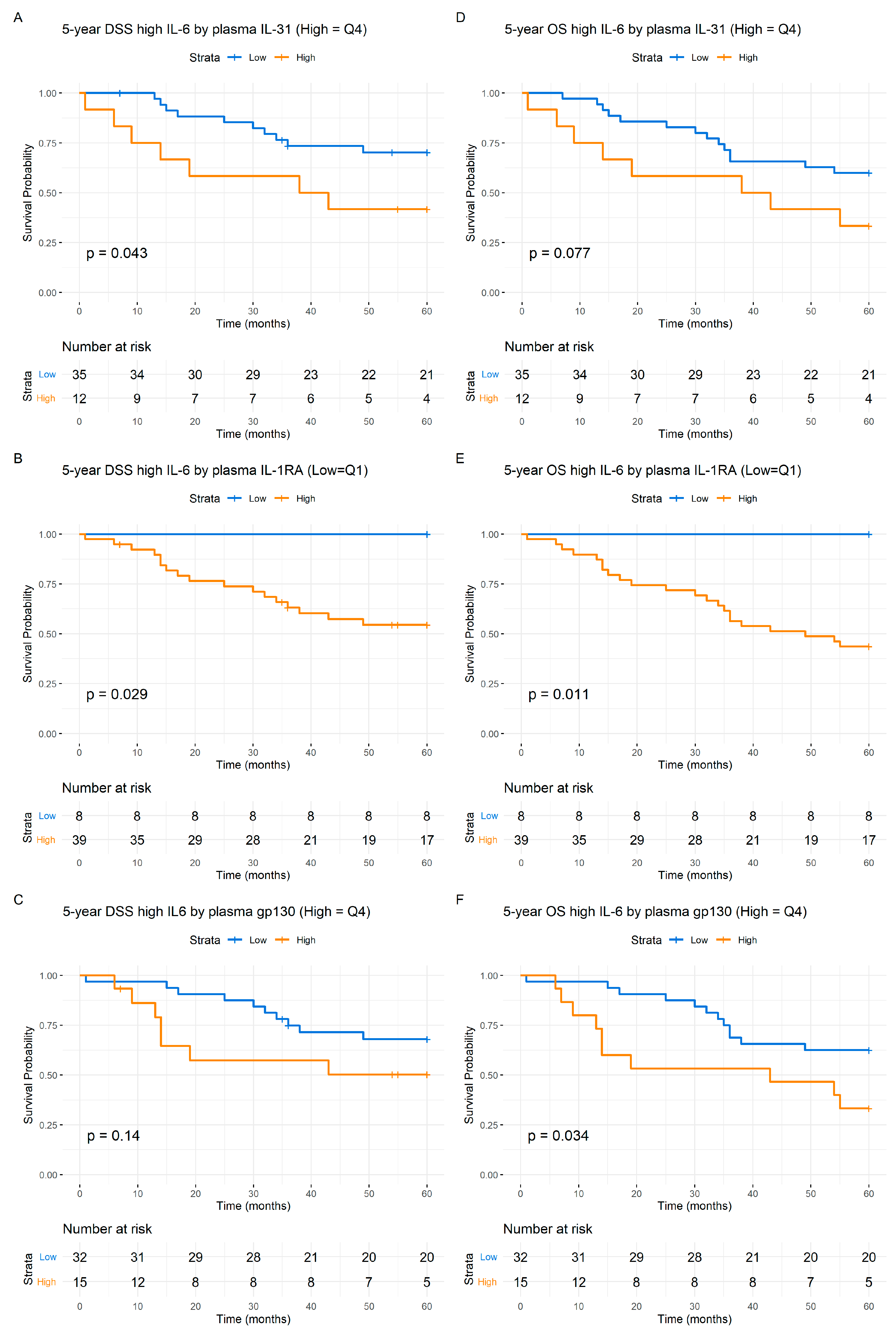
3.1.7. Cytokine-Predicted Survival by IL-6 Level Adjustment
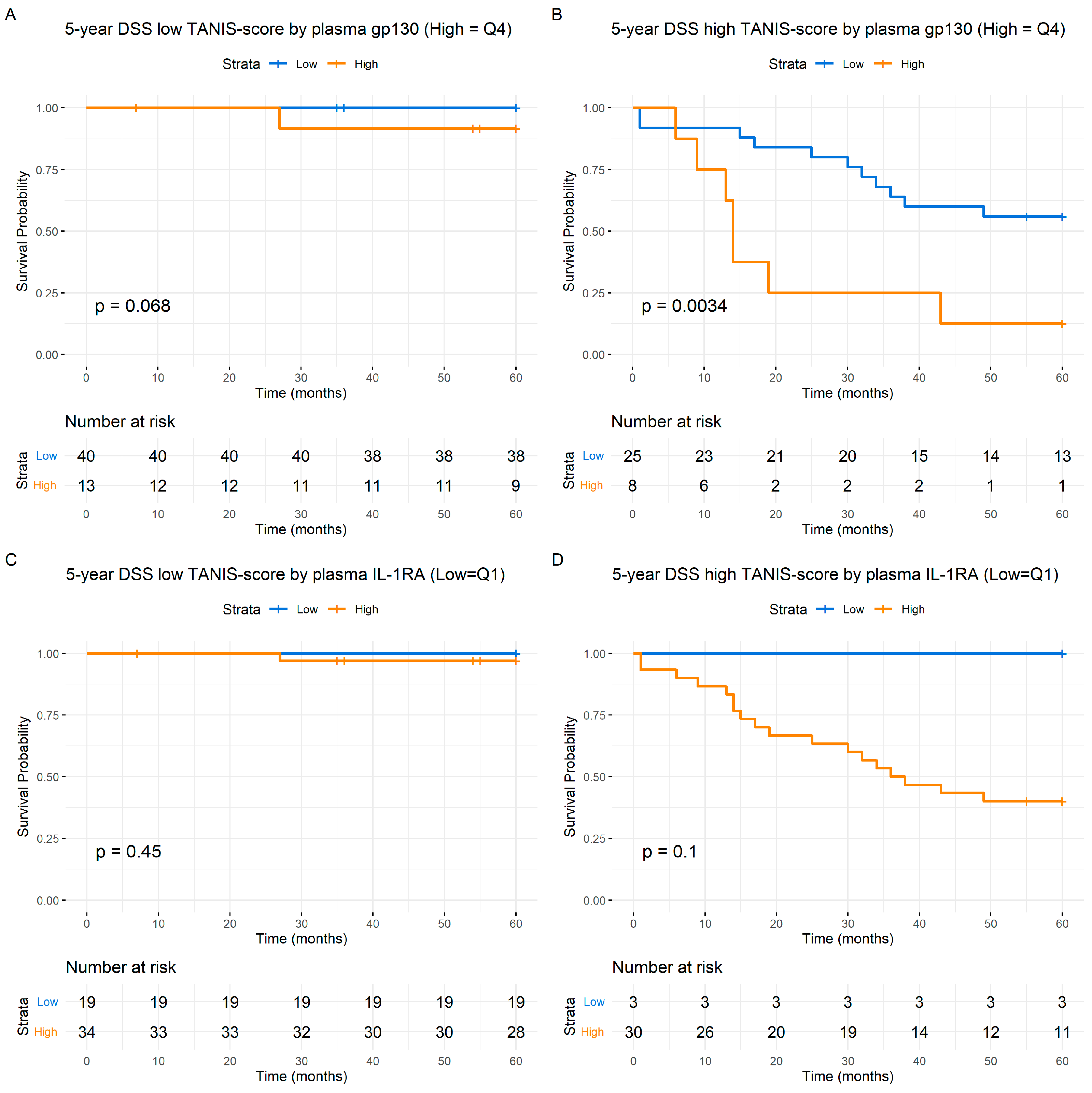
3.1.8. Cytokine-Predicted Survival Using TANIS Adjustment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Cunha, A.R.D.; Compton, K.; Xu, R.; Mishra, R.; Drangsholt, M.T.; Antunes, J.L.F.; Kerr, A.R.; Acheson, A.R.; Lu, D.; Wallace, L.E.; et al. The Global, Regional, and National Burden of Adult Lip, Oral, and Pharyngeal Cancer in 204 Countries and Territories: A Systematic Analysis for the Global Burden of Disease Study 2019. JAMA Oncol. 2023, 9, 1401–1416. [Google Scholar] [CrossRef] [PubMed]
- Varoni, E.M.; Lodi, G.; Iriti, M. Ethanol versus Phytochemicals in Wine: Oral Cancer Risk in a Light Drinking Perspective. Int. J. Mol. Sci. 2015, 16, 17029–17047. [Google Scholar] [CrossRef] [PubMed]
- Lechner, M.; Liu, J.; Masterson, L.; Fenton, T.R. HPV-associated oropharyngeal cancer: Epidemiology, molecular biology and clinical management. Nat. Rev. Clin. Oncol. 2022, 19, 306–327. [Google Scholar] [CrossRef] [PubMed]
- Ljokjel, B.; Lybak, S.; Haave, H.; Olofsson, J.; Vintermyr, O.K.; Aarstad, H.J. The impact of HPV infection on survival in a geographically defined cohort of oropharynx squamous cell carcinoma (OPSCC) patients in whom surgical treatment has been one main treatment. Acta Otolaryngol. 2014, 134, 636–645. [Google Scholar] [CrossRef] [PubMed]
- Gabay, C.; Kushner, I. Acute-phase proteins and other systemic responses to inflammation. N. Engl. J. Med. 1999, 340, 448–454. [Google Scholar] [CrossRef] [PubMed]
- Bertsch, T.; Triebel, J.; Bollheimer, C.; Christ, M.; Sieber, C.; Fassbender, K.; Heppner, H.J. C-reactive protein and the acute phase reaction in geriatric patients. Z. Fur Gerontol. Und Geriatr. 2015, 48, 595–600. [Google Scholar] [CrossRef] [PubMed]
- Plebani, M. Why C-reactive protein is one of the most requested tests in clinical laboratories? Clin. Chem. Lab. Med. 2023, 61, 1540–1545. [Google Scholar] [CrossRef]
- Srinagesh, H.K.; Levine, J.E.; Ferrara, J.L.M. Biomarkers in acute graft-versus-host disease: New insights. Ther. Adv. Hematol. 2019, 10, 2040620719891358. [Google Scholar] [CrossRef]
- Scheller, J.; Garbers, C.; Rose-John, S. Interleukin-6: From basic biology to selective blockade of pro-inflammatory activities. Semin. Immunol. 2014, 26, 2–12. [Google Scholar] [CrossRef]
- Kaur, S.; Bansal, Y.; Kumar, R.; Bansal, G. A panoramic review of IL-6: Structure, pathophysiological roles and inhibitors. Bioorg. Med. Chem. 2020, 28, 115327. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.; Zhang, L.; Luo, M.; Hu, G.; Mei, Q.; Liu, D.; Long, G.; Hu, G. Pretreatment hematologic markers as prognostic factors in patients with nasopharyngeal carcinoma: Neutrophil-lymphocyte ratio and platelet-lymphocyte ratio. Head Neck 2016, 38 (Suppl. S1), E1332–E1340. [Google Scholar] [CrossRef] [PubMed]
- Chang, P.Y.; Kuo, Y.B.; Wu, T.L.; Liao, C.T.; Sun, Y.C.; Yen, T.C.; Chan, E.C. Association and prognostic value of serum inflammation markers in patients with leukoplakia and oral cavity cancer. Clin. Chem. Lab. Med. 2013, 51, 1291–1300. [Google Scholar] [CrossRef] [PubMed]
- Fang, Y.; Xu, C.; Wu, P.; Zhang, L.H.; Li, D.W.; Sun, J.H.; Li, W.F.; Liao, Z.S. Prognostic role of C-reactive protein in patients with nasopharyngeal carcinoma: A meta-analysis and literature review. Medicine 2017, 96, e8463. [Google Scholar] [CrossRef] [PubMed]
- Kawasaki, T.; Wasano, K.; Yamamoto, S.; Tomisato, S.; Ogawa, K. Utility of clinico-biological data for long-term prognosis of head and neck terminal cancer. Acta Oto-Laryngol. 2017, 137, 895–898. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Chen, S.; Peng, S.; Liu, Y.; Xing, S.; He, X.; Chen, H. Prognostic nomogram for patients with Nasopharyngeal Carcinoma incorporating hematological biomarkers and clinical characteristics. Int. J. Biol. Sci. 2018, 14, 549–556. [Google Scholar] [CrossRef] [PubMed]
- De Paz, D.; Young, C.K.; Chien, H.T.; Tsao, C.K.; Fok, C.C.; Fan, K.H.; Liao, C.-T.; Wang, H.-M.; Kang, C.-J.; Chang, J.T.-C.; et al. Prognostic Roles of SCC Antigen, CRP and CYFRA 21-1 in Oral Cavity Squamous Cell Carcinoma. Anticancer Res. 2019, 39, 2025–2033. [Google Scholar] [CrossRef] [PubMed]
- Sun, P.; Chen, C.; Xia, Y.; Bi, X.; Liu, P.; Zhang, F.; Yang, H.; An, X.; Jiang, W.; Wang, F. The Ratio of C-Reactive Protein/Albumin is a Novel Inflammatory Predictor of Overall Survival in Cisplatin-Based Treated Patients with Metastatic Nasopharyngeal Carcinoma. Dis. Markers 2017, 2017, 6570808. [Google Scholar] [CrossRef] [PubMed]
- Adel, M.; Tsao, C.K.; Wei, F.C.; Chien, H.T.; Lai, C.H.; Liao, C.T.; Wang, H.-M.; Fan, K.-H.; Kang, C.-J.; Chang, J.T.-C.; et al. Preoperative SCC Antigen, CRP Serum Levels, and Lymph Node Density in Oral Squamous Cell Carcinoma. Medicine 2016, 95, e3149. [Google Scholar] [CrossRef]
- Schiegnitz, E.; Kammerer, P.W.; Schon, H.; Blatt, S.; Berres, M.; Sagheb, K.; Al-Nawas, B. Proinflammatory cytokines as serum biomarker in oral carcinoma-A prospective multi-biomarker approach. J. Oral. Pathol. Med. Off. Publ. Int. Assoc. Oral. Pathol. Am. Acad. Oral. Pathol. 2018, 47, 268–274. [Google Scholar] [CrossRef]
- Zergoun, A.A.; Zebboudj, A.; Sellam, S.L.; Kariche, N.; Djennaoui, D.; Ouraghi, S.; Kerboua, E.; Amir-Tidadini, Z.-C.; Chilla, D.; Asselah, F.; et al. IL-6/NOS2 inflammatory signals regulate MMP-9 and MMP-2 activity and disease outcome in nasopharyngeal carcinoma patients. Tumour Biol. 2016, 37, 3505–3514. [Google Scholar] [CrossRef] [PubMed]
- Arduino, P.G.; Menegatti, E.; Cappello, N.; Martina, E.; Gardino, N.; Tanteri, C.; Cavallo, F.; Scully, C.; Broccoletti, R. Possible role for interleukins as biomarkers for mortality and recurrence in oral cancer. Int. J. Biol. Markers 2015, 30, e262–e266. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.P.; Kao, H.K.; Wu, C.C.; Fang, K.H.; Chang, Y.L.; Huang, Y.C.; Liu, S.C.; Cheng, M.H. Pretreatment interleukin-6 serum levels are associated with patient survival for oral cavity squamous cell carcinoma. Otolaryngol.-Head. Neck Surg. Off. J. Am. Acad. 2013, 148, 786–791. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.J.; Sung, W.W.; Lin, Y.M.; Chen, M.K.; Lee, C.H.; Lee, H.; Yeh, K.T.; Ko, J.L. Gender difference in the prognostic role of interleukin 6 in oral squamous cell carcinoma. PLoS ONE 2012, 7, e50104. [Google Scholar] [CrossRef] [PubMed]
- Duffy, S.A.; Taylor, J.M.; Terrell, J.E.; Islam, M.; Li, Y.; Fowler, K.E.; Wolf, G.T.; Teknos, T.N. Interleukin-6 predicts recurrence and survival among head and neck cancer patients. Cancer 2008, 113, 750–757. [Google Scholar] [CrossRef] [PubMed]
- Hao, W.; Zhu, Y.; Zhou, H. Prognostic value of interleukin-6 and interleukin-8 in laryngeal squamous cell cancer. Med. Oncol. 2013, 30, 333. [Google Scholar] [CrossRef] [PubMed]
- Ke, L.; Xiang, Y.; Xia, W.; Yang, J.; Yu, Y.; Ye, Y.; Liang, H.; Guo, X.; Lv, X. A prognostic model predicts the risk of distant metastasis and death for patients with nasopharyngeal carcinoma based on pre-treatment interleukin 6 and clinical stage. Clin. Immunol. 2016, 164, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Ataie-Kachoie, P.; Pourgholami, M.H.; Morris, D.L. Inhibition of the IL-6 signaling pathway: A strategy to combat chronic inflammatory diseases and cancer. Cytokine Growth Factor Rev. 2013, 24, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Yao, X.; Huang, J.; Zhong, H.; Shen, N.; Faggioni, R.; Fung, M.; Yao, Y. Targeting interleukin-6 in inflammatory autoimmune diseases and cancers. Pharmacol. Ther. 2014, 141, 125–139. [Google Scholar] [CrossRef]
- Blay, J.-Y.; Negrier, S.; Combaret, V.; Attali, S.; Goillot, E.; Merrouche, Y.; Mercatello, A.; Ravault, A.; Tourani, J.-M.; Moskovtchenko, J.-F.; et al. Serum Level of Interleukin 6 as a Prognosis Factor in Metastatic Renal Cell Carcinoma. Cancer Res. 1992, 52, 3317–3322. [Google Scholar]
- Mihara, M.; Hashizume, M.; Yoshida, H.; Suzuki, M.; Shiina, M. IL-6/IL-6 receptor system and its role in physiological and pathological conditions. Clin. Sci. 2012, 122, 143–159. [Google Scholar] [CrossRef] [PubMed]
- Silver, J.S.; Hunter, C.A. gp130 at the nexus of inflammation, autoimmunity, and cancer. J. Leukoc. Biol. 2010, 88, 1145–1156. [Google Scholar] [CrossRef] [PubMed]
- Tvedt, T.H.A.; Ersvaer, E.; Tveita, A.A.; Bruserud, O. Interleukin-6 in Allogeneic Stem Cell Transplantation: Its Possible Importance for Immunoregulation and as a Therapeutic Target. Front. Immunol. 2017, 8, 667. [Google Scholar] [CrossRef]
- Rose-John, S.; Jenkins, B.J.; Garbers, C.; Moll, J.M.; Scheller, J. Targeting IL-6 trans-signalling: Past, present and future prospects. Nat. Rev. Immunol. 2023, 23, 666–681. [Google Scholar] [CrossRef] [PubMed]
- Lamertz, L.; Rummel, F.; Polz, R.; Baran, P.; Hansen, S.; Waetzig, G.H.; Moll, J.M.; Floss, D.M.; Scheller, J. Soluble gp130 prevents interleukin-6 and interleukin-11 cluster signaling but not intracellular autocrine responses. Sci. Signal. 2018, 11, eaar7388. [Google Scholar] [CrossRef]
- Rose-John, S. Interleukin-6 Family Cytokines. Cold Spring Harb. Perspect. Biol. 2018, 10, a028415. [Google Scholar] [CrossRef]
- Jones, S.A.; Jenkins, B.J. Recent insights into targeting the IL-6 cytokine family in inflammatory diseases and cancer. Nature reviews. Immunology 2018, 18, 773–789. [Google Scholar] [CrossRef] [PubMed]
- Aarstad, H.H.; Moe, S.E.E.; Bruserud, Ø.; Lybak, S.; Aarstad, H.J.; Tvedt, T.H.A. The Acute Phase Reaction and Its Prognostic Impact in Patients with Head and Neck Squamous Cell Carcinoma: Single Biomarkers Including C-Reactive Protein Versus Biomarker Profiles. Biomedicines 2020, 8, 418. [Google Scholar] [CrossRef] [PubMed]
- Liberale, L.; Montecucco, F.; Schwarz, L.; Lüscher, T.F.; Camici, G.G. Inflammation and cardiovascular diseases: Lessons from seminal clinical trials. Cardiovasc. Res. 2021, 117, 411–422. [Google Scholar] [CrossRef]
- Gudbrandsdottir, G.; Aarstad, H.H.; Hjelle, K.M.; Førde, K.; Reisæter, L.; Bostad, L.; Aarstad, H.J.; Beisland, C. The levels of IL-6 and soluble IL-33R are increased in the renal vein during surgery for clear cell renal cell carcinoma. Cytokine 2021, 144, 155586. [Google Scholar] [CrossRef]
- Poulose, J.V.; Kainickal, C.T. Immune checkpoint inhibitors in head and neck squamous cell carcinoma: A systematic review of phase-3 clinical trials. World J. Clin. Oncol. 2022, 13, 388–411. [Google Scholar] [CrossRef] [PubMed]
- Myojin, Y.; Kodama, T.; Sakamori, R.; Maesaka, K.; Matsumae, T.; Sawai, Y.; Imai, Y.; Ohkawa, K.; Miyazaki, M.; Tanaka, S.; et al. Interleukin-6 Is a Circulating Prognostic Biomarker for Hepatocellular Carcinoma Patients Treated with Combined Immunotherapy. Cancers 2022, 14, 883. [Google Scholar] [CrossRef] [PubMed]
- Ojesina, A.I.; Lichtenstein, L.; Freeman, S.S.; Pedamallu, C.S.; Imaz-Rosshandler, I.; Pugh, T.J.; Cherniack, A.D.; Ambrogio, L.; Cibulskis, K.; Bertelsen, B.; et al. Landscape of genomic alterations in cervical carcinomas. Nature 2014, 506, 371–375. [Google Scholar] [CrossRef] [PubMed]
- Aarstad, H.H.; Vintermyr, O.K.; Ulvestad, E.; Kross, K.; Heimdal, J.H.; Aarstad, H.J. In Vitro-Stimulated IL-6 Monocyte Secretion and In Vivo Peripheral Blood T Lymphocyte Activation Uniquely Predicted 15-Year Survival in Patients with Head and Neck Squamous Cell Carcinoma. PLoS ONE 2015, 10, e0129724. [Google Scholar] [CrossRef] [PubMed]
- Haeggblom, L.; Ramqvist, T.; Tommasino, M.; Dalianis, T.; Nasman, A. Time to change perspectives on HPV in oropharyngeal cancer. A systematic review of HPV prevalence per oropharyngeal sub-site the last 3 years. Papillomavirus Res. 2017, 4, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Jones, G.W.; Browman, G.; Goodyear, M.; Marcellus, D.; Hodson, D.I. Comparison of the addition of T and N integer scores with TNM stage groups in head and neck cancer. Head Neck 1993, 15, 497–503. [Google Scholar] [CrossRef] [PubMed]
- Uciechowski, P.; Dempke, W.C.M. Interleukin-6: A Masterplayer in the Cytokine Network. Oncology 2020, 98, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Gupta, M.; Stenson, M.; O’Byrne, M.; Maurer, M.J.; Habermann, T.; Cerhan, J.R.; Weiner, G.W.; Witzig, T.E. Comprehensive serum cytokine analysis identifies IL-1RA and soluble IL-2Rα as predictors of event-free survival in T-cell lymphoma. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2016, 27, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Rutkowski, P.; Kamińska, J.; Kowalska, M.; Ruka, W.; Steffen, J. Cytokine and cytokine receptor serum levels in adult bone sarcoma patients: Correlations with local tumor extent and prognosis. J. Surg. Oncol. 2003, 84, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Ito, H.; Miki, C. Profile of circulating levels of interleukin-1 receptor antagonist and interleukin-6 in colorectal cancer patients. Scand. J. Gastroenterol. 1999, 34, 1139–1143. [Google Scholar] [CrossRef] [PubMed]
- Kamińska, J.; Kowalska, M.M.; Nowacki, M.P.; Chwaliński, M.G.; Rysińska, A.; Fuksiewicz, M. CRP, TNF-alpha, IL-1ra, IL-6, IL-8 and IL-10 in blood serum of colorectal cancer patients. Pathol. Oncol. Res. 2000, 6, 38–41. [Google Scholar] [CrossRef]
- Niedźwiecki, S.; Stepień, T.; Kuzdak, K.; Stepień, H.; Krupiński, R.; Seehofer, D.; Rayes, N.; Ulrich, F. Serum levels of interleukin-1 receptor antagonist (IL-1ra) in thyroid cancer patients. Langenbeck’s Arch. Surg. 2008, 393, 275–280. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Otin, C.; Blasco, M.A.; Partridge, L.; Serrano, M.; Kroemer, G. The hallmarks of aging. Cell 2013, 153, 1194–1217. [Google Scholar] [CrossRef] [PubMed]
- Yokota, Y.; Hasegawa, T.; Yamakawa, N.; Rin, S.; Otsuru, M.; Yamada, S.I.; Hirai, E.; Ashikaga, Y.; Yamamoto, K.; Ueda, M.; et al. Comparison of the 8th edition of TNM staging of oral cancer with the 7th edition and its prognostic significance using clinical depth of invasion and extranodal extension. Oral. Oncol. 2023, 145, 106519. [Google Scholar] [CrossRef] [PubMed]
- de la Iglesia, J.V.; Slebos, R.J.C.; Martin-Gomez, L.; Wang, X.; Teer, J.K.; Tan, A.C.; Gerke, T.A.; Aden-Buie, G.; van Veen, T.; Masannat, J.; et al. Effects of Tobacco Smoking on the Tumor Immune Microenvironment in Head and Neck Squamous Cell Carcinoma. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2020, 26, 1474–1485. [Google Scholar] [CrossRef] [PubMed]
- Ma, S.J.; Yu, H.; Yu, B.; Waldman, O.; Khan, M.; Chatterjee, U.; Santhosh, S.; Gill, J.; Iovoli, A.J.; Farrugia, M.; et al. Association of Pack-Years of Cigarette Smoking With Survival and Tumor Progression Among Patients Treated With Chemoradiation for Head and Neck Cancer. JAMA Netw. Open. 2022, 5, e2245818. [Google Scholar] [CrossRef] [PubMed]
- Grabenbauer, G.G.; Suckorada, O.; Niedobitek, G.; Rödel, F.; Iro, H.; Sauer, R.; Rödel, C.; Schultze-Mosgau, S.; Distel, L. Imbalance between proliferation and apoptosis may be responsible for treatment failure after postoperative radiotherapy in squamous cell carcinoma of the oropharynx. Oral. Oncol. 2003, 39, 459–469. [Google Scholar] [CrossRef] [PubMed]
- Widjaja, A.A.; Cook, S.A. Nonspecific Inhibition of IL6 Family Cytokine Signalling by Soluble gp130. Int. J. Mol. Sci. 2024, 25, 1363. [Google Scholar] [CrossRef] [PubMed]
- Clamon, G.; Byrne, M.M.; Talbert, E.E. Inflammation as a Therapeutic Target in Cancer Cachexia. Cancers 2022, 14, 5262. [Google Scholar] [CrossRef]
- Wei, L.Y.; Lin, H.C.; Tsai, F.C.; Ko, J.Y.; Kok, S.H.; Cheng, S.J.; Lee, J.J.; Chia, J.S. Effects of Interleukin-6 on STAT3-regulated signaling in oral cancer and as a prognosticator of patient survival. Oral. Oncol. 2022, 124, 105665. [Google Scholar] [CrossRef]
- Elhousiny, M.; Miller, K.; Ariyawadana, A.; Nimmo, A. Identification of inflammatory mediators associated with metastasis of oral squamous cell carcinoma in experimental and clinical studies: Systematic review. Clin. Exp. Metastasis 2019, 36, 481–492. [Google Scholar] [CrossRef] [PubMed]
- Ridker, P.M.; Rane, M. Interleukin-6 Signaling and Anti-Interleukin-6 Therapeutics in Cardiovascular Disease. Circ. Res. 2021, 128, 1728–1746. [Google Scholar] [CrossRef] [PubMed]
- Psyrri, A.; Fayette, J.; Harrington, K.; Gillison, M.; Ahn, M.J.; Takahashi, S.; Weiss, J.; Machiels, J.-P.; Baxi, S.; Vasilyev, A.; et al. Durvalumab with or without tremelimumab versus the EXTREME regimen as first-line treatment for recurrent or metastatic squamous cell carcinoma of the head and neck: KESTREL, a randomized, open-label, phase III study. Ann. Oncol. 2023, 34, 262–274. [Google Scholar] [CrossRef] [PubMed]
- Gudbrandsdottir, G.; Aarstad, H.H.; Bostad, L.; Hjelle, K.M.; Aarstad, H.J.; Bruserud, Ø.; Tvedt, T.H.A.; Beisland, C. Serum levels of the IL-6 family of cytokines predict prognosis in renal cell carcinoma (RCC). Cancer Immunol. Immunother. 2021, 70, 19–30. [Google Scholar] [CrossRef] [PubMed]
- Stevens, M.A.; Rabe, K.G.; Boursi, B.; Kolluri, A.; Singh, D.P.; Bamlet, W.R.; Petersen, G.M. Accuracy of Smoking Status Reporting: Proxy Information in a Rapidly Fatal Cancer Setting. Mayo Clin. Proc. Innov. Qual. Outcomes 2020, 4, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Cramer, J.D.; Burtness, B.; Ferris, R.L. Immunotherapy for head and neck cancer: Recent advances and future directions. Oral. Oncol. 2019, 99, 104460. [Google Scholar] [CrossRef] [PubMed]
- Gavrielatou, N.; Doumas, S.; Economopoulou, P.; Foukas, P.G.; Psyrri, A. Biomarkers for immunotherapy response in head and neck cancer. Cancer Treat. Rev. 2020, 84, 101977. [Google Scholar] [CrossRef]
- Wolchok, J.D.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.J.; Rutkowski, P.; Lao, C.D.; Cowey, C.L.; Schadendorf, D.; Wagstaff, J.; Dummer, R.; et al. Long-Term Outcomes With Nivolumab Plus Ipilimumab or Nivolumab Alone Versus Ipilimumab in Patients With Advanced Melanoma. J. Clin. Oncol. 2022, 40, 127–137. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Distribution | Prediction of 5-Year DSS | |
|---|---|---|---|
| Age at diagnosis | Years (Mean ± SD) | 62.9 ± 10.3 | n.s. |
| Gender | Males | 59 | n.s. |
| Females | 28 | ||
| T stage | 0 | 3 | p < 0.001 |
| 1 | 29 | ||
| 2 | 34 | ||
| 3 | 8 | ||
| 4 | 13 | ||
| N stage | 0 | 57 | p < 0.001 |
| 1 | 9 | ||
| 2 | 20 | ||
| 3 | 1 | ||
| Smoking | Never smoked | 21 | p = 0.077 |
| <10 pack years | 1 | ||
| Probably <10 pack years | 8 | ||
| Probably >10 pack years | 5 | ||
| >10 pack years | 50 | ||
| Missing | 2 | ||
| Site (ICD-10) | Oropharynx | 17 | |
| Oral Cavity | 61 | ||
| Other | 9 | ||
| Total patients | 87 |
| Covariate | Outcome | p Value | RR (95% CI) | |
|---|---|---|---|---|
| Block I + s-gp130 | Gender | DSS | 0.279 | 0.50 (0.15–1.74) |
| Age | 0.203 | 0.96 (0.90–1.02) | ||
| T stage | <0.001 | 2.46 (1.52–3.98) | ||
| N stage | <0.001 | 5.28 (2.59–10.8) | ||
| Tobacco | 0.111 | 1.39 (0.93–2.05) | ||
| s-gp130 | 0.008 | 1.74 (1.16–2.61) | ||
| Gender | OS | 0.359 | 0.63 (0.24–1.69) | |
| Age | 0.928 | 1.00 (0.95–1.06) | ||
| T stage | 0.006 | 1.69 (1.17–2.46) | ||
| N stage | <0.001 | 3.40 (2.08–5.55) | ||
| Tobacco | 0.143 | 1.27 (0.92–1.73) | ||
| s-gp130 | 0.009 | 1.53 (1.12–2.08) | ||
| Block I + s-IL-6Rα | s-IL-6Rα | DSS | 0.005 | 1.40 (0.97–2.02) |
| s-IL-6Rα | OS | 0.016 | 1.36 (1.02–1.81) | |
| Block I + s-IL33Rα/ST2 | s-IL33Rα/ST2 | DSS | 0.005 | 1.79 (1.19–2.69) |
| s-IL33Rα/ST2 | OS | 0.016 | 1.48 (1.08–2.03) | |
| Block I + IL1-RA | IL1-RA | DSS | 0.966 | - |
| IL1-RA | OS | 0.955 | - | |
| Block I + IL-6 | IL-6 | DSS | 0.667 | - |
| IL-6 | OS | 0.876 | - | |
| Block I + IL-31 | IL-31 | DSS | 0.138 | - |
| IL-31 | OS | 0.685 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aarstad, H.H.; Moe, S.E.E.; Lybak, S.; Bruserud, Ø.; Tvedt, T.H.A.; Aarstad, H.J. Plasma IL-1 and IL-6 Family Cytokines with Soluble Receptor Levels at Diagnosis in Head and Neck Squamous Cell Carcinoma: High Levels Predict Decreased Five-Year Disease-Specific and Overall Survival. Cancers 2024, 16, 1484. https://doi.org/10.3390/cancers16081484
Aarstad HH, Moe SEE, Lybak S, Bruserud Ø, Tvedt THA, Aarstad HJ. Plasma IL-1 and IL-6 Family Cytokines with Soluble Receptor Levels at Diagnosis in Head and Neck Squamous Cell Carcinoma: High Levels Predict Decreased Five-Year Disease-Specific and Overall Survival. Cancers. 2024; 16(8):1484. https://doi.org/10.3390/cancers16081484
Chicago/Turabian StyleAarstad, Helene Hersvik, Svein Erik Emblem Moe, Stein Lybak, Øystein Bruserud, Tor Henrik Anderson Tvedt, and Hans Jørgen Aarstad. 2024. "Plasma IL-1 and IL-6 Family Cytokines with Soluble Receptor Levels at Diagnosis in Head and Neck Squamous Cell Carcinoma: High Levels Predict Decreased Five-Year Disease-Specific and Overall Survival" Cancers 16, no. 8: 1484. https://doi.org/10.3390/cancers16081484
APA StyleAarstad, H. H., Moe, S. E. E., Lybak, S., Bruserud, Ø., Tvedt, T. H. A., & Aarstad, H. J. (2024). Plasma IL-1 and IL-6 Family Cytokines with Soluble Receptor Levels at Diagnosis in Head and Neck Squamous Cell Carcinoma: High Levels Predict Decreased Five-Year Disease-Specific and Overall Survival. Cancers, 16(8), 1484. https://doi.org/10.3390/cancers16081484