
Cardiometabolic and Skeletal Risk Factors in Black Men with Prostate Cancer Starting Androgen Deprivation Therapy

Abstract
:1. Introduction
2. Materials and Methods
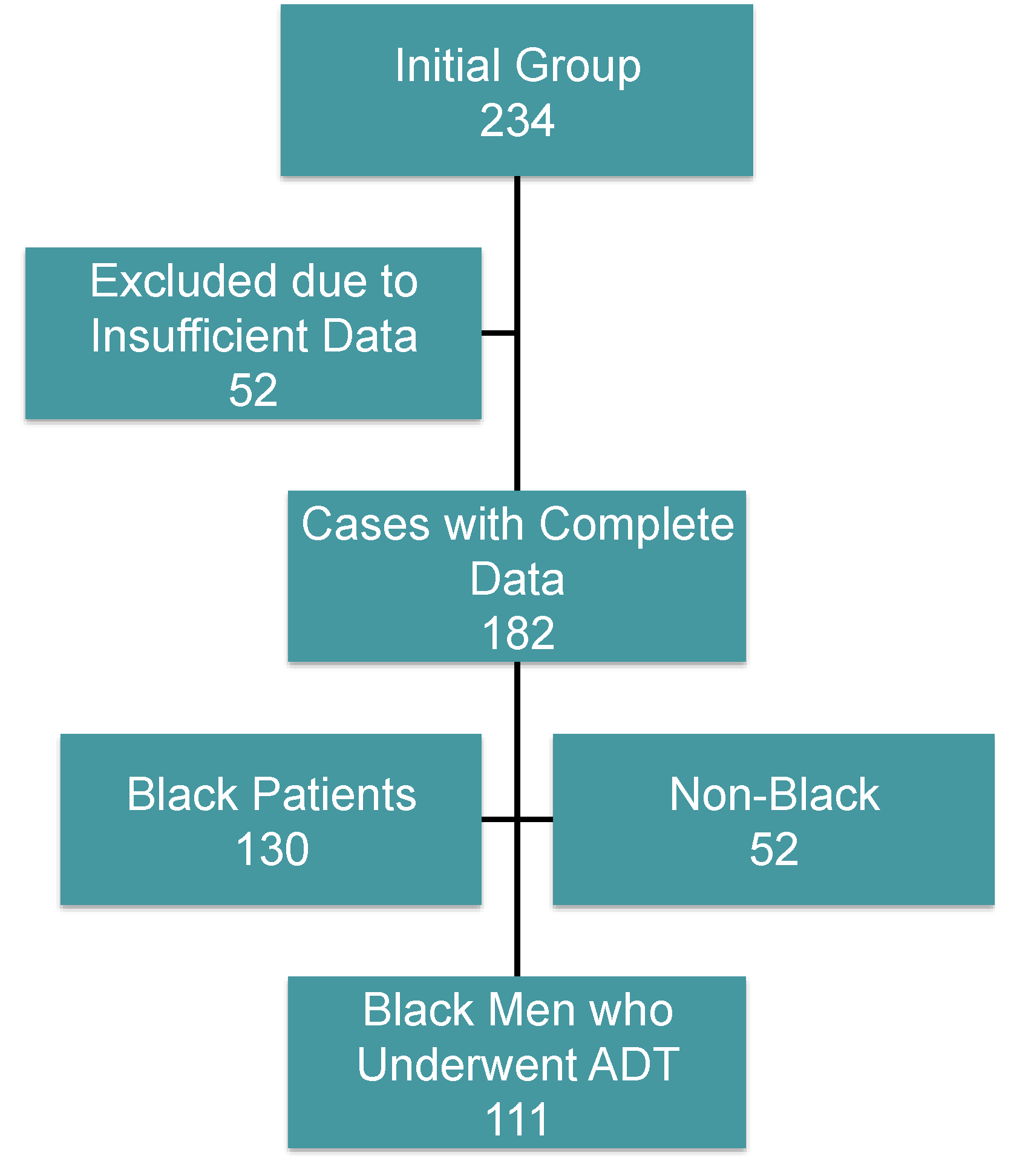
2.1. Subjects
2.2. Study Procedures
2.3. Ethical Approval
2.4. Data Analysis
3. Results
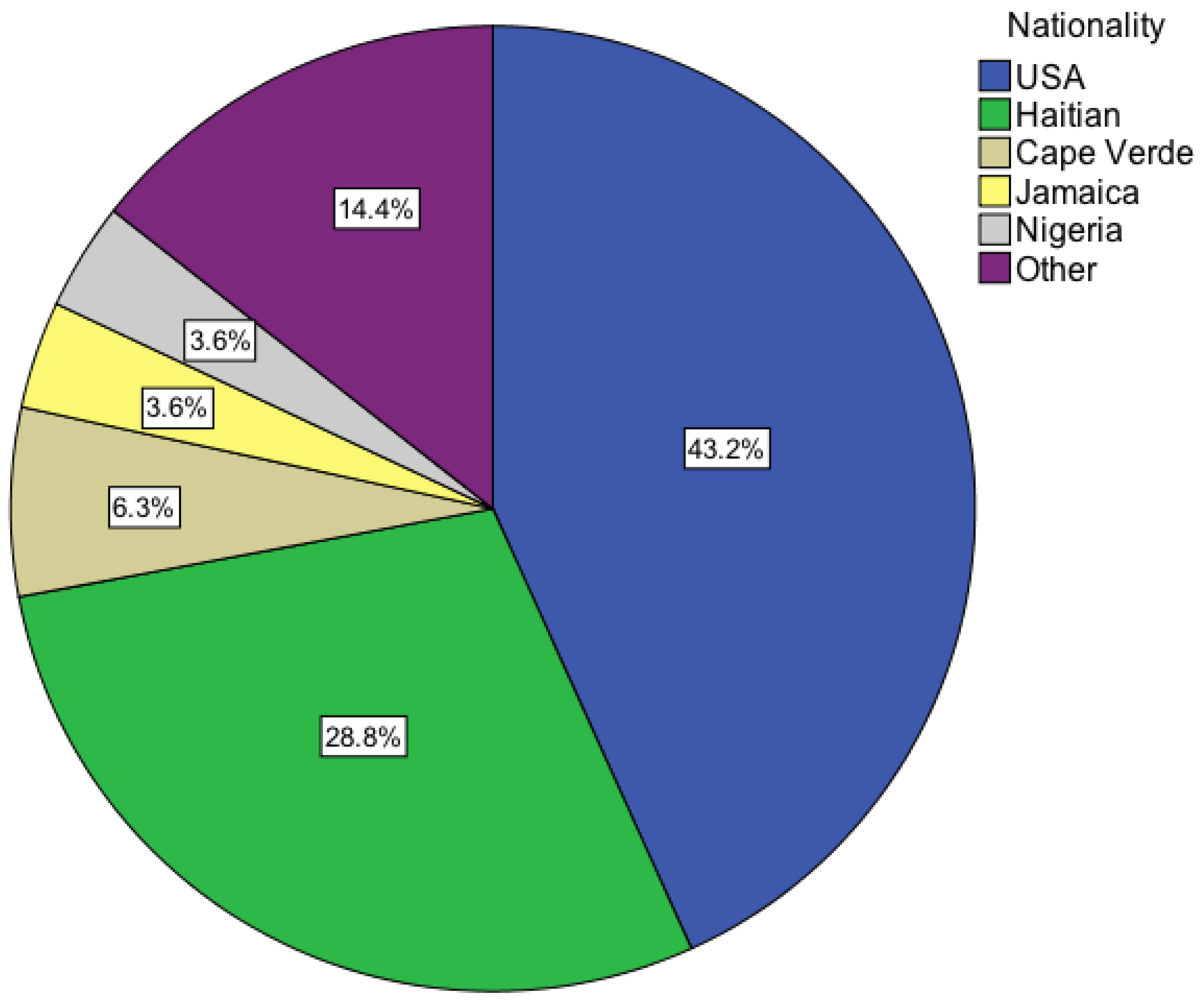
3.1. Baseline Characteristics



{kind=link}
{kind=link}
| Patient characteristics | Mean ± Standard Deviation | Minimum–Maximum |
|---|---|---|
| Age (years) | 68.4 ± 9.0 | 45–92 |
| Time to ADT start after Dx(months) | 9.7 ± 19.7 | 0–108 |
| Gleason score Total | 7.6 ± 1.0 | 6–10 |
| PSA (ng/mL) | 302 ± 790 | 0.2–5609 |
| BMI | 28.1 ± 6.0 | 15.4–58.5 |
| HbA1c (%) | 6.8 ± 1.2 | 4.9–10.9 |
| Total Cholesterol (mg/dL) | 187 ± 53 | 105–333 |
| LDL Cholesterol (mg/dL) | 112 ± 39 | 45–235 |
| HDL Cholesterol (mg/dL) | 48 ± 16 | 25–108 |
| Triglycerides (mg/dL) | 127 ± 66 | 35–292 |
| 25(OH)D(ng/mL) | 20.5 ± 8.7 | 4.0–43.0 |
| BMD—Lumbar spine (T score) | −0.370 ± 1.464 | −4.200–3.340 |
| BMD—Femoral neck (T score) | −0.939 ± 1.035 | −3.000–1.500 |
3.2. BMI
| Patient subgroup | Category | N | % |
|---|---|---|---|
| BMI weight classification | BMI Means ± SD * | ||
| Underweight 16.5 ± 0.9 | 3 | 2.9 | |
| Normal weight 22.6 ± 2.0 | 24 | 23.1 | |
| Overweight 27.3 ± 1.4 | 45 | 43.3 | |
| Class I obesity 31.7 ± 1.5 | 22 | 21.2 | |
| Class II obesity 36.6 ± 1.6 | 6 | 5.8 | |
| Class III obesity 46.2 ± 8.4 | 4 | 3.8 | |
| Diabetes | Yes | 32 | 28.8 |
| No | 79 | 71.2 | |
| Dyslipidemia | Yes | 41 | 36.9 |
| No | 70 | 63.1 | |
| Vitamin D status | 25(OH)D ng/mL means ± SD * | ||
| Vitamin D deficiency 13.5 ± 4.6 | 44 | 50.0 | |
| Vitamin D insufficiency 24.5 ± 3.1 | 30 | 34.1 | |
| Vitamin D sufficiency 34.2 ± 3.9 | 14 | 15.9 | |
| Bone mass density | T-score ± SD * | ||
| Osteoporosis −3.160 ± 0.673 | 5 | 9.3 | |
| Osteopenia −2.026 ± 0.302 | 17 | 31.5 | |
| Normal BMD −0.501 ± 0.699 | 32 | 59.3 |
3.3. Diabetes and Hyperlipidemia
3.4. Vitamin-D Levels and Bone Mass
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- American Cancer Society (ACS). Cancer Facts & Figures; ACS: Atlanta, GA, USA, 2013. [Google Scholar]
- Smith, J.C.; Bennett, S.; Evans, L.M.; Kynaston, H.G.; Parmar, M.; Mason, M.D.; Cockcroft, J.R.; Scanlon, M.F.; Davies, J.S. The effects of induced hypogonadism on arterial stiffness, body composition, and metabolic parameters in patients with prostate cancer. J. Clin. Endocrinol. Metab. 2001, 86, 4261–4267. [Google Scholar] [CrossRef] [PubMed]
- Braga-Basaria, M.; Dobs, A.S.; Muller, D.C.; Carducci, M.A.; Majnu, J.; Egan, J.; Basaria, S. Metabolic syndrome in men with prostate cancer undergoing long-term androgen-deprivation therapy. J. Clin. Oncol. 2006, 24, 3979–3983. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.R.; Lee, H.; Nathan, D.M. Insulin sensitivity during combined androgen blockade for prostate cancer. J. Clin. Endocrinol. Metab. 2006, 91, 1305–1308. [Google Scholar] [CrossRef] [PubMed]
- Keating, N.L.; O’Malley, J.A.; Smith, M.R. Diabetes and cardiovascular disease during androgen deprivation therapy for prostate cancer. J. Clin. Oncol. 2006, 24, 4448–4456. [Google Scholar] [CrossRef] [PubMed]
- Braga-Basaria, M.; Muller, D.C.; Carducci, M.A.; Dobs, A.S.; Basaria, S. Lipoprotein profile in men with prostate cancer undergoing androgen deprivation therapy. Int. J. Impot. Res. 2006, 18, 494–498. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.R.; Finkelstein, J.S.; McGovern, F.J.; Zietman, A.L.; Fallon, M.A.; Schoenfeld, D.A.; Kantoff, P. Changes in body composition during androgen deprivation therapy for prostate cancer. J. Clin. Endocrinol. Metab. 2002, 87, 599–603. [Google Scholar] [CrossRef] [PubMed]
- Lu-Yao, G.; Stukel, T.A.; Yao, S.-L. Changing patterns in competing causes of death in men with prostate cancer: A population based study. J. Urol. 2004, 171, 2285–2290. [Google Scholar] [CrossRef] [PubMed]
- Shahinian, V.B.; Kuo, Y.-F.; Freeman, J.L.; Freeman, J.S. Risk of fracture after androgen deprivation for prostate cancer. N. Engl. J. Med. 2005, 352, 154–164. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; McGovern, K.; Finkelstein, J.S.; Smith, M.R. Changes in bone mineral density and body composition during initial and long-term gonadotropin-releasing hormone agonist treatment for prostate carcinoma. Cancer 2005, 104, 1633–1637. [Google Scholar] [CrossRef] [PubMed]
- Keating, N.L.; O’Malley, J.A.; Freedland, S.J.; Smith, M.R. Diabetes and cardiovascular disease during androgen deprivation therapy: Observational study of veterans with prostate cancer. J. Natl. Cancer Inst. 2010, 102, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Basaria, S.; Lieb, J., II; Tang, A.M.; DeWeese, T.; Carducci, M.A.; Eisenberger, M.; Dobs, A.S. Long-term effects of androgen deprivation therapy in prostate cancer patients. Clin. Endocrinol. 2002, 56, 779–786. [Google Scholar]
- Chen, Z.; Maricic, M.; Nguyen, P.; Ahmann, F.R.; Bruhn, R.; Dalkin, B.L. Low bone density and high percentage of body fat among men who were treated with androgen deprivation therapy for prostate carcinoma. Cancer 2002, 95, 2136–2144. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.R.; McGovern, F.J.; Fallon, M.A.; Schoenfeld, D.; Kantoff, P.W.; Finkelstein, J.S. Low bone mineral density in hormone-naive men with prostate carcinoma. Cancer 2001, 91, 2238–2245. [Google Scholar] [CrossRef] [PubMed]
- Morgans, A.K.; Hancock, M.L.; Barnette, K.G.; Steiner, M.S.; Morton, R.A.; Smith, M.R. Racial differences in bone mineral density and fractures in men receiving androgen deprivation therapy for prostate cancer. J. Urol. 2012, 187, 889–893. [Google Scholar] [CrossRef] [PubMed]
- Trump, D.L.; Chadha, M.K.; Sunga, A.Y.; Fakih, M.G.; Ashraf, U.; Silliman, C.G.; Hollis, B.W.; Nesline, M.K.; Tian, L.; Tan, W.; et al. Vitamin D deficiency and insufficiency among patients with prostate cancer. BJU Int. 2009, 104, 909–914. [Google Scholar]
- Derweesh, I.H.; Diblasio, C.J.; Kincade, M.C.; Malcolm, J.B.; Lamar, K.D.; Patterson, A.L.; Kitabchi, A.E.; Wake, R.W. Risk of new-onset diabetes mellitus and worsening glycaemic variables for established diabetes in men undergoing androgen-deprivation therapy for prostate cancer. BJU Int. 2007, 100, 1060–1065. [Google Scholar] [PubMed]
- Morrison, B.F.; Burrowes, I.E.; Aiken, W.D.; Mayhew, R.G.; Fletcher, H.M.; Reid, M.E. Bone mineral density in Jamaican men on androgen deprivation therapy for prostate cancer. Infect. Agent Cancer 2011. [Google Scholar] [CrossRef]
- Wells, T.S.; Bukowinski, A.T.; Smith, T.C.; Smith, B.; Dennis, L.K.; Chu, L.K.; Gray, G.C.; Ryan, M.A.K. Racial differences in prostate cancer risk remain among US servicemen with equal access to care. Prostate 2010, 70, 727–734. [Google Scholar] [PubMed]
- White, A.; Coker, A.L.; Du, X.L.; Eggleston, K.S.; Williams, M. Racial/ethnic disparities in survival among men diagnosed with prostate cancer in Texas. Cancer 2011, 117, 1080–1088. [Google Scholar] [CrossRef] [PubMed]
- Schiller, J.S.; Lucas, J.W.; Ward, B.W.; Peregoy, J.A. Summary health statistics for U.S. adults: National Health Interview Survey, 2010. Vital Health Stat. 2012, 252, 1–207. [Google Scholar]
- Looker, A.C.; Dawson-Hughes, B.; Calvo, M.S.; Gunter, E.W.; Sahyoun, N.R. Serum 25-Hydroxyvitamin D status of adolescents and adults in two seasonal subpopulations from NHANES III. Bone 2002, 30, 771–777. [Google Scholar] [CrossRef] [PubMed]
- George, A.; Tracy, J.K.; Meyer, W.A.; Flores, R.H.; Wilson, P.D.; Hochberg, M.C. Racial differences in bone mineral density in older men. J. Bone Miner. Res. 2003, 18, 2238–2244. [Google Scholar] [CrossRef] [PubMed]
- Harris, M.I. Racial and ethnic differences in health care access and health outcomes for adults with type 2 diabetes. Diabetes Care 2001, 24, 454–459. [Google Scholar] [CrossRef] [PubMed]
- Beydoun, M.A.; Wang, Y. Gender-ethnic disparity in BMI and waist circumference distribution shifts in US adults. Obesity 2009, 17, 169–176. [Google Scholar] [CrossRef] [PubMed]
- The International Expert Committee. International Expert Committee report on the role of the A1c assay in the diagnosis of diabetes. Diabetes Care 2009, 32, 1327–1334. [Google Scholar]
- National Institutes of Health (NIH); National Heart, Lung and Blood Institute (NHLBI); North American Association for the study of Obesity (NAASO). The Practical Guide: Identification, Evaluation, and Treatment of Overweight and Obesity in Adults; NIH: Rockville, MD, USA, 2000. [Google Scholar]
- Kanis, J.A.; Melton, L.J.; Christiansen, C.; Johnston, C.C.; Khaltaev, N. The diagnosis of osteoporosis. J. Bone Miner. Res. 1994, 9, 1137–1141. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed]
- Morgans, A.K.; Smith, M.R.; O’Malley, A.J.; Keating, N.L. Bone density testing among prostate cancer survivors treated with androgen-deprivation therapy. Cancer 2013, 119, 863–870. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gunnarsson, O.; Basaria, S.; Gignac, G.A. Cardiometabolic and Skeletal Risk Factors in Black Men with Prostate Cancer Starting Androgen Deprivation Therapy. Cancers 2015, 7, 679-687. https://doi.org/10.3390/cancers7020679
Gunnarsson O, Basaria S, Gignac GA. Cardiometabolic and Skeletal Risk Factors in Black Men with Prostate Cancer Starting Androgen Deprivation Therapy. Cancers. 2015; 7(2):679-687. https://doi.org/10.3390/cancers7020679
Chicago/Turabian StyleGunnarsson, Orvar, Shehzad Basaria, and Gretchen A. Gignac. 2015. "Cardiometabolic and Skeletal Risk Factors in Black Men with Prostate Cancer Starting Androgen Deprivation Therapy" Cancers 7, no. 2: 679-687. https://doi.org/10.3390/cancers7020679
APA StyleGunnarsson, O., Basaria, S., & Gignac, G. A. (2015). Cardiometabolic and Skeletal Risk Factors in Black Men with Prostate Cancer Starting Androgen Deprivation Therapy. Cancers, 7(2), 679-687. https://doi.org/10.3390/cancers7020679