
Dimensions of Hybrid and Nanohybrid Mouthguards for Mixed Martial Arts Fighters–Evaluation of a New Method of Fabrication



Abstract
:1. Introduction
2. Materials and Methods
2.1. Custom Mouthguard Fabrication
2.2. Measurements of Mouthguards and Pattern Dimensions
2.3. Statistical Analysis
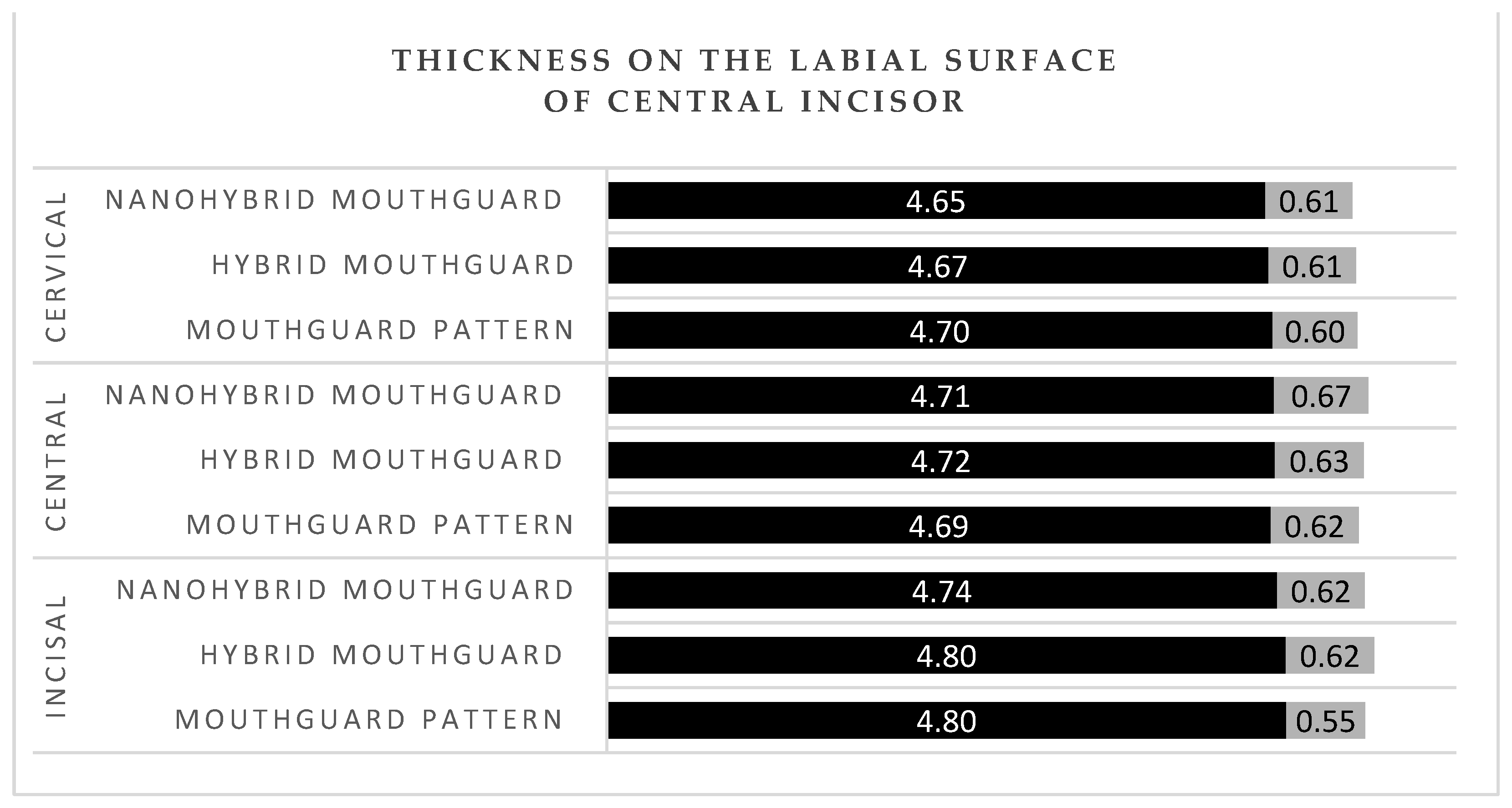
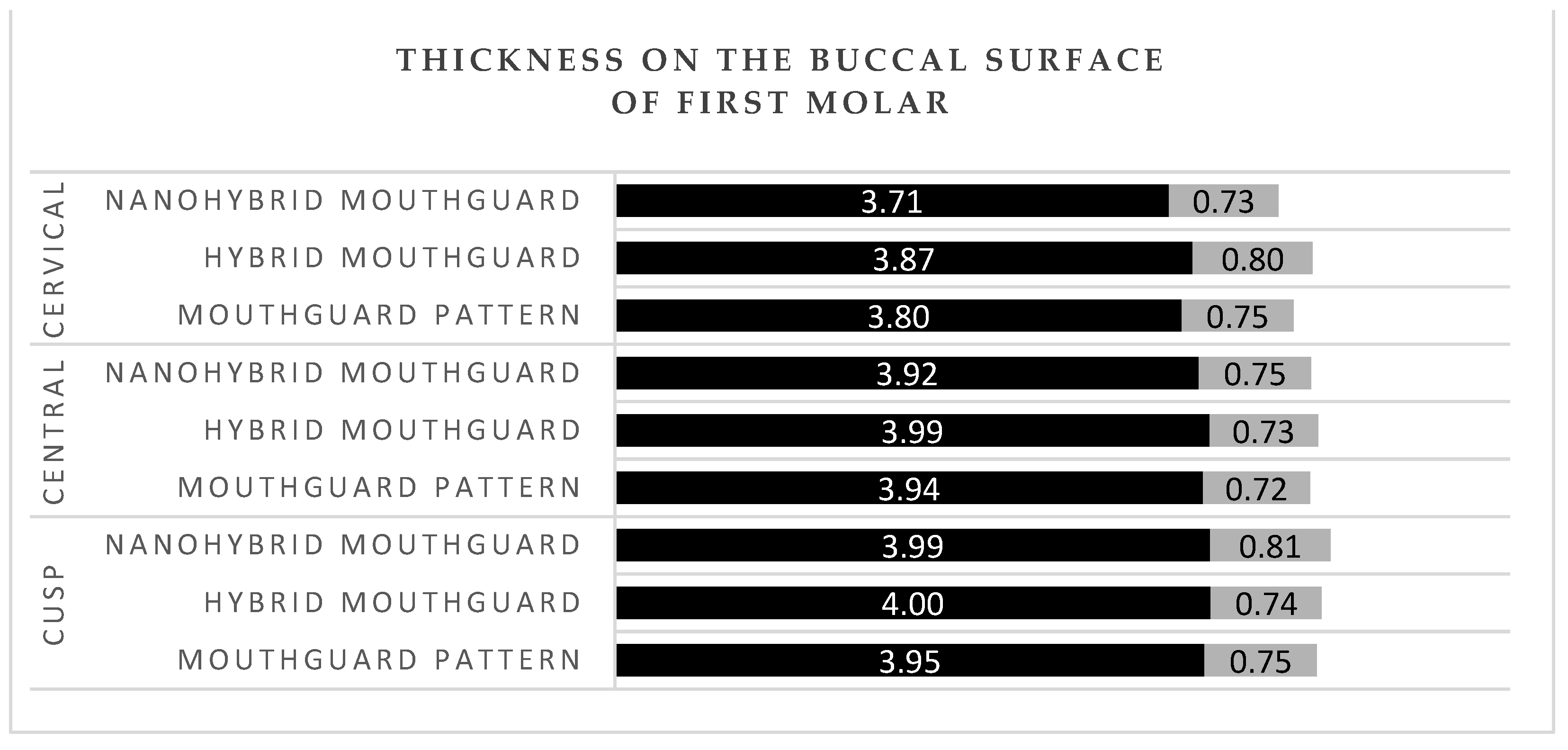
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Fukasawa, S.; Churei, H.; Chowdhury, R.U.; Shirako, T.; Shahrin, S.; Shrestha, A.; Wada, T.; Uo, M.; Takahashi, H.; Ueno, R. Difference among shock-absorbing capabilities of mouthguard materials. Dent. Traumatol. 2016, 32, 474–479. [Google Scholar] [CrossRef] [PubMed]
- Mańka-Malara, K.; Gawlak, D. The comparison of mouthguards used in combat sports. Dent. Med. Probl. 2013, 50, 205–209. [Google Scholar]
- Westerman, B.; Stringfellow, P.M.; Eccleston, J.A. Forces transmitted through EVA mouthguard materials of different types and thickness. Aust. Dent. J. 1995, 40, 389–391. [Google Scholar] [CrossRef] [PubMed]
- Gawlak, D.; Mańka-Malara, K.; Mierzwińska-Nastalska, E.; Waśniewski, B.; Ryszkowska, J. Comparison of hardness, energy absorption and water absorbability of polymeric materials used in the manufacture of mouthguards. Dent. Med. Probl. 2015, 52, 78–85. [Google Scholar]
- Mizuhashi, F.; Koide, K. Formation of vacuum-formed and pressure-formed mouthguards. Dent. Traumatol. 2017, 33, 295–299. [Google Scholar] [CrossRef] [PubMed]
- Mizuhashi, F.; Koide, K.; Mizuhashi, R. Influence of working angle on the formation of a pressure-formed mouthguard. Dent. Traumatol. 2017, 33, 189–193. [Google Scholar] [CrossRef]
- Takahashi, M.; Bando, Y. Thermoforming technique for maintaining the thickness of single-layer mouthguard during pressure formation. Dent. Traumatol. 2019, 35, 289–290. [Google Scholar] [CrossRef]
- Mizuhashi, F.; Koide, K.; Watarai, Y. Difference in laminated mouthguard thickness according to the laminate order. Dent. Traumatol. 2021, 37, 497–501. [Google Scholar] [CrossRef]
- Verissimo, C.; Costa, P.V.; Santos-Filho, P.C.; Tantbijorn, D.; Versluis, A.; Soares, C.J. Custom fitted EVA mouthguards: What is the ideal thickness? A dynamic finite element impact study. Dent. Traumatol. 2016, 32, 95–102. [Google Scholar] [CrossRef]
- Takahashi, M.; Araie, Y.; Satoh, Y.; Iwasaki, S. Influence of continuous use of a vacuum-forming machine for mouthguard thickness after thermoforming. Dent. Traumatol. 2017, 33, 188–194. [Google Scholar] [CrossRef]
- Del Rossi, G.; Leyte-Vidal, M. Fabricating a better mouthguard. Part I: Factors influencing mouthguard thinning. Dent. Traumatol. 2007, 23, 49–153. [Google Scholar] [CrossRef] [PubMed]
- Newsome, P.; Tran, D.; Cooke, M. The role of mouthguard in the prevention of sports-related dental injuries: A review. Int. J. Paediatr. Dent. 2001, 11, 396–404. [Google Scholar] [CrossRef] [PubMed]
- Mańka-Malara, K.; Panasiewicz, P.; Kacprzyk, M.; Gawryszewska, M.; Mierzwińska-Nastalska, E.; Gawlak, D. The effect of decontamination procedures on elastic polymeric materials used in dental mouthguards fabrication. Acta Bioeng. Biomech. 2019, 21, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Wood, N.J.; Maddocks, S.E.; Grady, H.J.; Collins, A.M.; Barbour, M.E. Functionalization of ethylene vinyl acetate with antimicrobial chlorhexidine hexametaphosphate nanoparticles. Int. J. Nanomed. 2014, 27, 4145–4152. [Google Scholar]
- Nagai, K.; Domon, H.; Oda, M.; Shirai, T.; Ohsumi, T.; Terao, Y.; Arai, Y. Antimirobial activity of ethylene-vinyl-acetate containing bioactive filler against bacteria. Dent. Mater. J. 2017, 36, 784–790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshida, Y.; Churei, H.; Takeuchi, Y.; Wada, T.; Uo, M.; Izumi, Y.; Ueno, T. Novel antibacterial mouthguard material manufactured using silver-nanoparticle-embedded ethylene-vinyl-acetate copolymer masterbatch. Dent. Mater. J. 2018, 37, 437–444. [Google Scholar] [CrossRef] [Green Version]
- Cierech, M.; Wojnarowicz, J.; Szmigiel, D.; Bączkowski, B.; Grudniak, A.M.; Wolska, K.I.; Łojkowski, W.; Mierzwińska-Nastalska, E. Preparation and characterization of ZnO-PMMA resin nanocomposites for denture bases. Acta Bioeng. Biomech. 2016, 18, 31–41. [Google Scholar]
- Cierech, M.; Osica, I.; Kolenda, A.; Wojnarowicz, J.; Szmigiel, D.; Łojkowski, W.; Kurzydłowski, K.; Ariga, K.; Mierzwińska-Nastalska, E. Mechanical and physicochemical properties of newly formed ZnO-PMMA Nanocomposites for denture bases. Nanomaterials 2018, 8, 305. [Google Scholar] [CrossRef] [Green Version]
- Cierech, M.; Wojnarowicz, J.; Kolenda, A.; Krawczyk-Balska, A.; Prochwicz, E.; Woźniak, B.; Łojkowski, W.; Mierzwińska-Nastalska, E. Zinc Oxide nanoparticles cytotoxicity and release from newly formed PMMA-ZnO nanocomposites designed for denture bases. Nanomaterials 2019, 15, 1318. [Google Scholar] [CrossRef] [Green Version]
- Gawlak, D.; Mańka-Malara, K.; Kamiński, T. Assessment of the usage of custom mouthguards prepared using pressure injection. Dent. Med. Probl. 2014, 51, 218–224. [Google Scholar]
- Saunders, J.; Lißner, M.; Townsend, D.; Petrinic, N.; Bergmann, J. Impact behaviour of 3D printed cellular structures for mouthguard applications. Sci. Rep. 2022, 12, 4020. [Google Scholar] [CrossRef] [PubMed]
- Unkovskiy, A.; Huettig, F.; Kraemer-Fernandez, P.; Spintzyk, S. Multi-material 3D printing of customized sports mouth guard: Proof-of-Concept clinical case. Int. J. Environ. Res. Public 2021, 18, 12762. [Google Scholar] [CrossRef] [PubMed]
- Gawlak, D.; Mańka-Malara, K.; Mierzwińska-Nastalska, E.; Roman, G.; Kamiński, T.; Łuniewska, M. A comparison of impact force reduction by polymer materials used for mouthguards fabrication. Acta Bioeng. Biomech. 2017, 19, 89–95. [Google Scholar] [PubMed]
- Gawlak, D.; Mierzwińska-Nastalska, E.; Mańka-Malara, K.; Kamiński, T. Assessment of custom and standard, self-adapted mouthguards in terms of comfort and users subjective impressions of their protective functions. Dent. Traumatol. 2015, 31, 113–117. [Google Scholar] [CrossRef]
- Mańka-Malara, K.; Gawlak, D.; Łojszczyk, R.; Trzaskowski, M.; Mierzwińska-Nastalska, E. Direct modelling of mouthguard pattern using modified impression tray. Protet. Stomatol. 2020, 70, 23–32. [Google Scholar] [CrossRef]
- Mizuhashi, F.; Koide, K. Appropriate fabrication method for vacuum-formed mouthguards. Dent. Traumatol. 2017, 33, 110–113. [Google Scholar] [CrossRef]
- Farrington, T.; Coward, T.; Onambele-Pearson, G.; Taylor, R.L.; Earl, P.; Winwood, K. An investigation into the relationship between thickness variations and manufacturing techniques of mouthguards. Dent. Traumatol. 2016, 32, 14–21. [Google Scholar] [CrossRef]
- Verissimo, C.; Bicalho, A.A.; Soares, P.B.F.; Tantbirojn, D.; Versluis, A.; Doares, C.J. The effect of antagonist tooth contact on the biomechanical response of custom-fitted mouthguards. Dent. Traumatol. 2017, 33, 57–63. [Google Scholar] [CrossRef]
- Westerman, B.; Stringfellow, P.M.; Eccleston, J.A. Beneficial effects of air inclusions on the performance of ethylene vinyl acetate (EVA) mouthguard material. Br. J. Sports Med. 2002, 36, 51–53. [Google Scholar] [CrossRef] [Green Version]
- Westerman, B.; Stringfellow, P.M.; Eccleston, J.A.; Harbrow, D.J. Effect of ethylene vinyl acetate (EVA) closed cell foam on transmitted forces in mouthguard material. Br. J. Sports Med. 2002, 36, 5–208. [Google Scholar] [CrossRef]
- Fukosawa, S.; Churei, H.; Chowdhury, R.U.; Shirako, T.; Shahrin, S.; Shrestha, A.; Wada, T.; Uo, M.; Takahashi, H.; Ueno, T. Application of addition-cured silicone denture relining materials to adjust mouthguards. Dent. Mater. J. 2016, 35, 635–643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McClelland, C.; Kinirons, M.; Geary, L. A preliminary study of patient comfort associated with customized mouthguards. Br. J. Sports Med. 1999, 33, 186–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maeda, Y.; Machi, H.; Tsugawa, T. Influences of palatal side design and finishing on the wereability and retention of mouthguards. Br. J. Sports Med. 2006, 40, 1006–1008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.; Imani, S.; de Araujo, W.R.; Warchall, J.; Valdes-Ramirez, G.; Paixao, T.R.L.C.; Mercier, P.P.; Wang, J. Wereable salivary uric acid mouthguard biosensor with integrated wirless electronics. Biosens. Bioelecron. 2015, 74, 1061–1068. [Google Scholar] [CrossRef] [Green Version]
- Winters, J.E. Commentary: Role of properly fitted mouthguards in prevention of sports-related concussion. J. Athl. Train. 2001, 36, 339–341. [Google Scholar]
- Wiśniewski, J.F.; Guskiewicz, K.; Trope, M.; Sigurdsson, A. Incidence of cerebral concussions associated with type of mouthguards used in college football. Dent. Traumatol. 2004, 20, 143–149. [Google Scholar] [CrossRef]
- Barbic, D.; Pater, J.; Brison, R.J. Comparison of mouthguard designs and concussion prevention in contact sports: A multicenter randomized controlled trial. Clin. J. Sports Med. 2005, 15, 294–298. [Google Scholar] [CrossRef]
- Labella, C.R.; Smith, B.W.; Sigurdsson, A. Effect of mouthguards on dental injuries and concussion in college basketball. Med. Sci. Sports Exerc. 2002, 34, 41–44. [Google Scholar] [CrossRef]
- Benson, B.W.; Meeuwisse, W.H. Ice hockey injuries. Med. Sport Sci. 2005, 49, 86–119. [Google Scholar]
- Tribst, J.P.M.; Dal Piva, A.M.O.; Bottino, M.A.; Klevarlaan, C.J.; Koolstra, J.H. Mouthguard use and TMJ injury prevention with different occlusions. A three-dimensional finite element analysis. Dent. Traumatol. 2020, 36, 662–669. [Google Scholar] [CrossRef]
- Mańka-Malara, K.; Mierzwińska-Nastalska, E. Head trauma exposure in Mixed Martial Arts. Int. J. Environ. Res. Public Health 2022, 19, 13050. [Google Scholar] [CrossRef] [PubMed]
- Westerman, B.; Stringfellow, P.M.; Eccleston, J.A. EVA mouthguards–how thick should they be? Dent. Traumatol. 2002, 18, 24–27. [Google Scholar] [CrossRef] [PubMed]
- Glass, R.T.; Conrad, R.S.; Wood, R.C.; Warren, A.J.; Kohler, G.A.; Bullard, J.W.; Benson, G.; Gulden, J.M. Protective athletic mouthguards: Do they cause harm? Sports Health 2009, 1, 411–415. [Google Scholar] [CrossRef] [PubMed]
- Glass, R.T.; Conrad, R.S.; Köhler, G.A.; Warren, A.J.; Bullard, J.W. Microbiota found in protective athletic mouthguard. Sport Health 2011, 3, 244–248. [Google Scholar] [CrossRef] [Green Version]
- Glass, R.; Bullard, J.; Conrad, R. The contamination of protective mouthguards: A characterization of the microbiota found in football players’ protective mouthguards as compared to oral microbiota found in first-year medical students. Am. Dent. Inst. Cont. Educ. J. 2006, 93, 23–28. [Google Scholar]
- Mańka-Malara, K.; Łuniewska, J.; Łuniewska, M.; Hovhannisyan, A.; Gawlak, D. Assessment of intraoral mouthguards: Usage and hygiene issues. Protet. Stomatol. 2017, 67, 182–196. [Google Scholar] [CrossRef]
- Szerszeń, M.; Górski, B.; Kowalski, J. Clinical Condition of the Oral Cavity in the Adult Polish Population below 70 Years of Age after Myocardial Infarction–A Case-Control Study. Int. J. Environ. Res. Public Health 2022, 19, 7265. [Google Scholar] [CrossRef]
- Szerszeń, M.; Cierech, M.; Wojnarowicz, J.; Górski, B.; Mierzwińska-Nastalska, E. Color Stability of Zinc Oxide Poly (methyl methacrylate) Nanocomposite–A new Biomaterial for Denture Bases. Polymers 2022, 14, 4982. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Compared Variable | M Pattern | SD Pattern | M Hybrid | SD Hybrid | T | Uncorrected p–Value | Corrected p–Values | Correlation | Correlation p |
|---|---|---|---|---|---|---|---|---|---|
| 1 labial incisal | 4.79 | 0.57 | 4.82 | 0.64 | –0.83 | 0.42 | 1 | 0.96 | <0.001 |
| 2 labial incisal | 4.81 | 0.57 | 4.77 | 0.64 | 0.90 | 0.38 | 1 | 0.97 | <0.001 |
| 3 labial incisal | 4.81 | 0.55 | 4.80 | 0.62 | 0.28 | 0.78 | 1 | 0.96 | <0.001 |
| 4 labial center | 4.79 | 0.69 | 4.75 | 0.68 | 0.74 | 0.47 | 1 | 0.96 | <0.001 |
| 5 labial center | 4.65 | 0.71 | 4.72 | 0.67 | –1.32 | 0.21 | 1 | 0.96 | <0.001 |
| 6 labial center | 4.67 | 0.58 | 4.71 | 0.63 | –0.79 | 0.44 | 1 | 0.95 | <0.001 |
| 7 labial center | 4.65 | 0.53 | 4.71 | 0.56 | –1.32 | 0.21 | 1 | 0.96 | <0.001 |
| 8 labial cervical | 4.68 | 0.59 | 4.71 | 0.63 | –0.50 | 0.63 | 1 | 0.94 | <0.001 |
| 9 labial cervical | 4.75 | 0.64 | 4.68 | 0.62 | 1.23 | 0.24 | 1 | 0.94 | <0.001 |
| 10 labial cervical | 4.68 | 0.59 | 4.64 | 0.63 | 0.63 | 0.54 | 1 | 0.90 | <0.001 |
| mesial cusp | 3.87 | 0.73 | 3.89 | 0.73 | –0.65 | 0.52 | 1 | 0.98 | <0.001 |
| mesial cusp center | 3.86 | 0.72 | 3.92 | 0.73 | –0.94 | 0.36 | 1 | 0.93 | <0.001 |
| mesial cusp cervical | 3.69 | 0.78 | 3.75 | 0.81 | –1.12 | 0.28 | 1 | 0.96 | <0.001 |
| distal cusp | 4.04 | 0.78 | 4.10 | 0.76 | –1.03 | 0.32 | 1 | 0.95 | <0.001 |
| distal cusp center | 4.03 | 0.72 | 4.05 | 0.74 | –0.37 | 0.71 | 1 | 0.94 | <0.001 |
| distal cusp cervical | 3.91 | 0.72 | 3.99 | 0.79 | –1.29 | 0.22 | 1 | 0.95 | <0.001 |
| mesiobuccal cusp | 3.75 | 1.21 | 3.58 | 1.21 | 1.41 | 0.18 | 1 | 0.91 | <0.001 |
| mesiolingual cusp | 3.42 | 0.82 | 3.39 | 1.00 | 0.20 | 0.85 | 1 | 0.86 | <0.001 |
| distobuccal cusp | 3.52 | 0.97 | 3.41 | 0.97 | 0.58 | 0.57 | 1 | 0.64 | 0.01 |
| distolingual cusp | 3.56 | 1.20 | 3.23 | 1.02 | 1.90 | 0.08 | 1 | 0.79 | <0.001 |
| mesial fovea | 5.55 | 0.89 | 5.30 | 0.77 | 1.49 | 0.16 | 1 | 0.65 | 0.00 |
| distal fovea | 5.21 | 0.87 | 5.13 | 0.90 | 0.67 | 0.51 | 1 | 0.86 | <0.001 |
| Compared Variable | M Pattern | SD Pattern | M Nanohybrid | SD Nanohybrid | T | Uncorrected p–Value | Corrected p–Values | Correlation | Correlation p |
|---|---|---|---|---|---|---|---|---|---|
| 1 labial incisal | 4.79 | 0.57 | 4.76 | 0.63 | 0.36 | 0.36 | 1 | 0.90 | <0.001 |
| 2 labial incisal | 4.81 | 0.57 | 4.73 | 0.63 | 1.19 | 0.13 | 1 | 0.91 | <0.001 |
| 3 labial incisal | 4.81 | 0.55 | 4.72 | 0.62 | 1.57 | 0.07 | 1 | 0.92 | <0.001 |
| 4 labial center | 4.79 | 0.69 | 4.74 | 0.68 | 1.09 | 0.15 | 1 | 0.97 | <0.001 |
| 5 labial center | 4.65 | 0.71 | 4.70 | 0.73 | –0.87 | 0.20 | 1 | 0.96 | <0.001 |
| 6 labial center | 4.67 | 0.58 | 4.70 | 0.67 | –0.40 | 0.35 | 1 | 0.91 | <0.001 |
| 7 labial center | 4.65 | 0.53 | 4.72 | 0.63 | –0.64 | 0.27 | 1 | 0.77 | <0.001 |
| 8 labial cervical | 4.68 | 0.59 | 4.71 | 0.59 | –0.52 | 0.31 | 1 | 0.95 | <0.001 |
| 9 labial cervical | 4.75 | 0.64 | 4.67 | 0.57 | 1.33 | 0.10 | 1 | 0.94 | <0.001 |
| 10 labial cervical | 4.68 | 0.59 | 4.58 | 0.69 | 1.02 | 0.16 | 1 | 0.82 | <0.001 |
| mesial cusp | 3.87 | 0.73 | 3.87 | 0.79 | –0.08 | 0.47 | 1 | 0.96 | <0.001 |
| mesial cusp center | 3.86 | 0.72 | 3.88 | 0.71 | –0.46 | 0.33 | 1 | 0.96 | <0.001 |
| mesial cusp cervical | 3.69 | 0.78 | 3.67 | 0.71 | 0.19 | 0.43 | 1 | 0.89 | <0.001 |
| distal cusp | 4.04 | 0.78 | 4.11 | 0.83 | –0.64 | 0.27 | 1 | 0.84 | <0.001 |
| distal cusp center | 4.03 | 0.72 | 3.95 | 0.80 | 0.71 | 0.24 | 1 | 0.84 | <0.001 |
| distal cusp cervical | 3.91 | 0.72 | 3.76 | 0.78 | 1.17 | 0.13 | 1 | 0.73 | <0.001 |
| mesiobuccal cusp | 3.75 | 1.21 | 3.67 | 1.39 | 0.50 | 0.31 | 1 | 0.89 | <0.001 |
| mesiolingual cusp | 3.42 | 0.82 | 3.39 | 1.03 | 0.19 | 0.43 | 1 | 0.79 | <0.001 |
| distobuccal cusp | 3.52 | 0.97 | 3.52 | 1.02 | 0.02 | 0.49 | 1 | 0.49 | 0.05 |
| distolingual cusp | 3.56 | 1.20 | 3.34 | 1.10 | 1.62 | 0.06 | 1 | 0.88 | <0.001 |
| mesial fovea | 5.55 | 0.89 | 5.37 | 0.70 | 1.38 | 0.09 | 1 | 0.79 | <0.001 |
| distal fovea | 5.21 | 0.87 | 5.26 | 0.82 | –0.52 | 0.31 | 1 | 0.89 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mańka-Malara, K.; Trzaskowski, M.; Mierzwińska-Nastalska, E. Dimensions of Hybrid and Nanohybrid Mouthguards for Mixed Martial Arts Fighters–Evaluation of a New Method of Fabrication. Polymers 2022, 14, 5369. https://doi.org/10.3390/polym14245369
Mańka-Malara K, Trzaskowski M, Mierzwińska-Nastalska E. Dimensions of Hybrid and Nanohybrid Mouthguards for Mixed Martial Arts Fighters–Evaluation of a New Method of Fabrication. Polymers. 2022; 14(24):5369. https://doi.org/10.3390/polym14245369
Chicago/Turabian StyleMańka-Malara, Katarzyna, Maciej Trzaskowski, and Elżbieta Mierzwińska-Nastalska. 2022. "Dimensions of Hybrid and Nanohybrid Mouthguards for Mixed Martial Arts Fighters–Evaluation of a New Method of Fabrication" Polymers 14, no. 24: 5369. https://doi.org/10.3390/polym14245369
APA StyleMańka-Malara, K., Trzaskowski, M., & Mierzwińska-Nastalska, E. (2022). Dimensions of Hybrid and Nanohybrid Mouthguards for Mixed Martial Arts Fighters–Evaluation of a New Method of Fabrication. Polymers, 14(24), 5369. https://doi.org/10.3390/polym14245369