
Remineralizing Effects of Resin-Based Dental Sealants: A Systematic Review of In Vitro Studies

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Question
2.2. Search Strategy
2.3. Inclusion and Exclusion Criteria
2.4. Study Screening and Selection
2.5. Data Extraction
2.6. Quality Assessment
2.7. Data Synthesis
3. Results
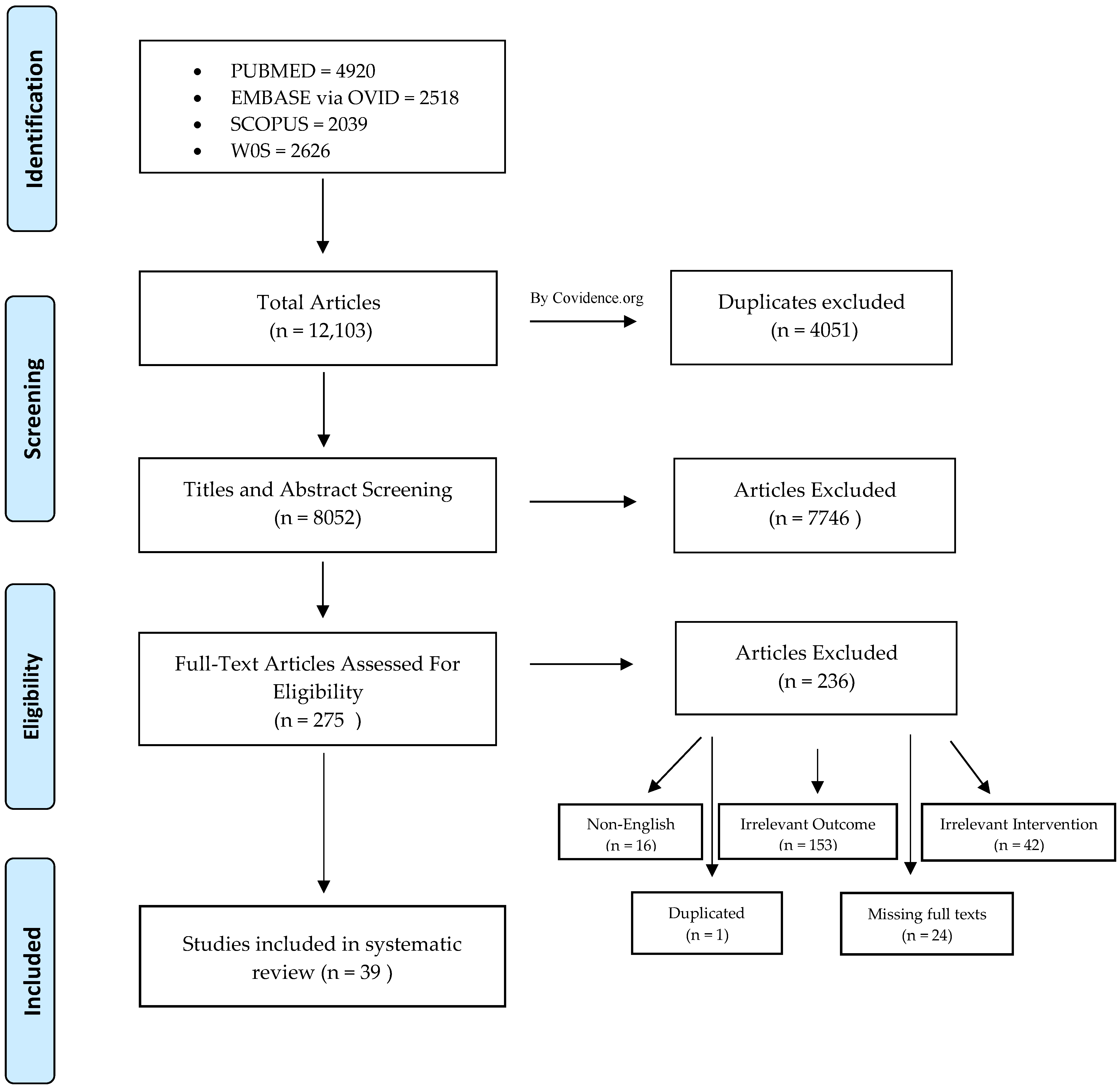
3.1. Study Selection
3.2. Risk of Bias Appraisal
3.3. Study Characteristics
3.4. Remineralization Findings
3.5. Ions Release Findings
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- GBD 2017 Oral Disorders Collaborators; Bernabe, E.; Marcenes, W.; Hernandez, C.R.; Bailey, J.; Abreu, L.G.; Alipour, V.; Amini, S.; Arabloo, J.; Arefi, Z.; et al. Global, Regional, and National Levels and Trends in Burden of Oral Conditions from 1990 to 2017: A Systematic Analysis for the Global Burden of Disease 2017 Study. J. Dent. Res. 2020, 99, 362–373. [Google Scholar] [CrossRef] [PubMed]
- Featherstone, J. Dental caries: A dynamic disease process. Aust. Dent. J. 2008, 53, 286–291. [Google Scholar] [CrossRef]
- Fejerskov, O.; Nyvad, B.; Kidd, E. Dental Caries: The Disease and Its Clinical Management, 3rd ed.; Black Well Munksgaard: Oxford, UK, 2003. [Google Scholar]
- Cate, J.M.T. Current concepts on the theories of the mechanism of action of fluoride. Acta Odontol. Scand. 1999, 57, 325–329. [Google Scholar] [CrossRef] [PubMed]
- Featherstone, J.D.B. The Continuum of Dental Caries—Evidence for a Dynamic Disease Process. J. Dent. Res. 2004, 83 (Suppl. S1), C39–C42. [Google Scholar] [CrossRef] [PubMed]
- Chin, J.R.; Kowolik, J.E.; Stookey, G.K. Dental Caries in the Child and Adolescent. In McDonald and Avery’s Dentistry for the Child and Adolescent, 10th ed.; Elsevier: St. Louis, MO, USA, 2016; pp. 155–176. [Google Scholar] [CrossRef]
- Kohn, W.G.; Mass, W.R.; Malvitz, D.M.; Presson, S.M.; Shaddix, K.K. Recommendations for using fluoride to prevent and control dental caries in the United States. MMWR Morb. Mortal. Wkly. Rep. 2001, 50, 1–42. [Google Scholar]
- Khetani, P.; Sharma, P.; Singh, S.; Augustine, V.; Baruah, K.; Thumpala, K.V.; Tiwari, R.V.C. History and Selection of Pit and Fissure Sealants–A Review. J. Med. Dent. Sci. Res. 2017, 4, 5–12. [Google Scholar]
- Nowak, A.J.; Christensen, J.R.; Mabry, T.R.; Townsend, J.A.; Wells, M.H. Pediatric Dentistry, 6th ed.; Elsevier: Amsterdam, The Netherlands, 2019; Chapter 12; pp. 169–179. [Google Scholar] [CrossRef]
- Cueto, E.I.; Buonocore, M.G. Sealing of pits and fissures with an adhesive resin: Its use in caries prevention. J. Am. Dent. Assoc. 1967, 75, 121–128. [Google Scholar] [CrossRef]
- Bowen, R.L. Method of Preparing a Monomer Having Phenoxy and Methacrylate Groups Linked by Hydroxy Glyceryl Groups. U.S. Patent Application No. US119748A, 20 April 1965. [Google Scholar]
- Santini, A.; Gallegos, I.T.; Felix, C.M. Photoinitiators in Dentistry: A Review. Prim. Dent. J. 2013, 2, 30–33. [Google Scholar] [CrossRef]
- Naaman, R.; El-Housseiny, A.A.; Alamoudi, N. The use of pit and fissure sealants-a literature review. Dent. J. 2017, 5, 34. [Google Scholar] [CrossRef] [Green Version]
- Silverstone, L.M.; Hicks, M.J.; Featherstone, M.J. Oral fluid contamination of etched enamel surfaces: An SEM study. J. Am. Dent. Assoc. 1985, 110, 329–332. [Google Scholar] [CrossRef]
- Borsatto, M.C.; Corona, S.A.M.; Alves, A.G.; Chimello, D.T.; Catirse, A.B.E.; Palma-Dibb, R.G. Influence of salivary contamination on marginal microleakage of pit and fissure sealants. Am. J. Dent. 2004, 17, 365–367. [Google Scholar] [PubMed]
- Ulusu, T.; Odabaş, M.E.; Tüzüner, T.; Baygin, Ö.; Sillelioğlu, H.; Deveci, C.; Gökdoğan, F.G.; Altuntaş, A. The success rates of a glass ionomer cement and a resin-based fissure sealant placed by fifth-year undergraduate dental students. Eur. Arch. Paediatr. Dent. 2012, 13, 94–97. [Google Scholar] [CrossRef] [PubMed]
- Alsabek, L.; AlNerabieah, Z.; Bshara, N.; Comisi, J.C. Retention and remineralization effect of moisture tolerant resin-based sealant and glass ionomer sealant on non-cavitated pit and fissure caries: Randomized controlled clinical trial. J. Dent. 2019, 86, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Dionysopoulos, D.; Sfeikos, T.; Tolidis, K. Fluoride release and recharging ability of new dental sealants. Eur. Arch. Paediatr. Dent. 2015, 17, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Zawaideh, F.I.; Owais, A.I.; Kawaja, W. Ability of Pit and Fissure Sealant-containing Amorphous Calcium Phosphate to inhibit Enamel Demineralization. Int. J. Clin. Pediatr. Dent. 2016, 9, 10–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakamura, K.; Abe, S.; Minamikawa, H.; Yawaka, Y. Effect of fluoride-releasing fissure sealants on enamel demineralization. Pediatr. Dent. J. 2017, 27, 56–64. [Google Scholar] [CrossRef]
- Kosior, P.; Dobrzyński, M.; Korczyński, M.; Herman, K.; Czajczyńska-Waszkiewicz, A.; Kowalczyk-Zając, M.; Piesiak-Pańczyszyn, D.; Fita, K.; Janeczek, M. Long-term release of fluoride from fissure sealants—In vitro study. J. Trace Elem. Med. Biol. 2017, 41, 107–110. [Google Scholar] [CrossRef]
- Roulet, J.F. Is in vitro research in restorative dentistry useless? J. Adhes. Dent. 2012, 14, 103–104. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- AlShahrani, S.S.; AlAbbas, M.A.S.; Garcia, I.M.; AlGhannam, M.I.; AlRuwaili, M.A.; Collares, F.M.; Ibrahim, M.S. The Antibacterial Effects of Resin-Based Dental Sealants: A Systematic Review of In Vitro Studies. Materials 2021, 14, 413. [Google Scholar] [CrossRef]
- Alamri, A.; Salloot, Z.; Alshaia, A.; Ibrahim, M.S. The Effect of Bioactive Glass-Enhanced Orthodontic Bonding Resins on Prevention of Demineralization: A Systematic Review. Molecules 2020, 25, 2495. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, M.S.; Ibrahim, A.S.; Balhaddad, A.A.; Weir, M.D.; Lin, N.J.; Tay, F.R.; Oates, T.W.; Xu, H.H.K.; Melo, M.A.S. A Novel Dental Sealant Containing Dimethylaminohexadecyl Methacrylate Suppresses the Cariogenic Pathogenicity of Streptococcus mutans Biofilms. Int. J. Mol. Sci. 2019, 20, 3491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Utneja, S.; Talwar, S.; Nawal, R.R.; Sapra, S.; Mittal, M.; Rajain, A.; Verma, M. Evaluation of remineralization potential and mechanical properties of pit and fissure sealants fortified with nano-hydroxyapatite and nano-amorphous calcium phosphate fillers: An in vitro study. J. Conserv. Dent. 2018, 21, 681–690. [Google Scholar] [CrossRef]
- Ei, T.Z.; Shimada, Y.; Nakashima, S.; Romero, M.J.R.H.; Sumi, Y.; Tagami, J. Comparison of resin-based and glass ionomer sealants with regard to fluoride-release and anti-demineralization efficacy on adjacent unsealed enamel. Dent. Mater. J. 2018, 37, 104–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kantovitz, K.R.; Pascon, F.M.; Nociti, F.H.; Tabchoury, C.P.M.; Puppin-Rontani, R.M. Inhibition of enamel mineral loss by fissure sealant: An in situ study. J. Dent. 2013, 41, 42–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basappa, N.; Raju, O.; Dahake, P.T.; Prabhakar, A. Fluoride: Is It Worth to be added in Pit and Fissure Sealants? Int. J. Clin. Pediatr. Dent. 2012, 5, 1–5. [Google Scholar] [CrossRef]
- Salar, D.V.; García-Godoy, F.; Flaitz, C.M.; Hicks, M.J. Potential inhibition of demineralization in vitro by fluoride-releasing sealants. J. Am. Dent. Assoc. 2007, 138, 502–506. [Google Scholar] [CrossRef] [Green Version]
- Lobo, M.M.; Pecharki, G.D.; Tengan, C.; da Silva, D.D.; Tagliaferro, E.P.D.S.; Napimoga, M.H. Fluoride-releasing capacity and cariostatic effect provided by sealants. J. Oral Sci. 2005, 47, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, M.S.; Balhaddad, A.A.; Garcia, I.M.; Collares, F.M.; Weir, M.D.; Xu, H.H.; Melo, M.A.S. pH-responsive calcium and phosphate-ion releasing antibacterial sealants on carious enamel lesions in vitro. J. Dent. 2020, 97, 103323. [Google Scholar] [CrossRef]
- Yang, S.-Y.; Choi, J.-W.; Kim, K.-M.; Kwon, J.-S. Prevention of Secondary Caries Using Resin-Based Pit and Fissure Sealants Containing Hydrated Calcium Silicate. Polymers 2020, 12, 1200. [Google Scholar] [CrossRef]
- Bohns, F.; DeGrazia, F.W.; de Souza Balbinot, G.; Leitune, V.C.B.; Samuel, S.M.W.; García-Esparza, M.A.; Sauro, S.; Collares, F.M. Boron Nitride Nanotubes as Filler for Resin-Based Dental Sealants. Sci. Rep. 2019, 9, 7710. [Google Scholar] [CrossRef]
- Bohns, F.R.; Leitune, V.C.B.; de Souza Balbinot, G.; Samuel, S.M.W.; Collares, F.M. Mineral deposition promoted by resin-based sealants with different calcium phosphate additions. Braz. Oral Res. 2019, 33, e101. [Google Scholar] [CrossRef]
- Sadrabad, Z.K.; Safari, E.; Alavi, M.; Shadkar, M.M.; Naghavi, S.H.H. Effect of a fluoride-releasing fissure sealant and a conventional fissure sealant on inhibition of primary carious lesions with or without exposure to fluoride-containing toothpaste. J. Dent. Res. Dent. Clin. Dent. Prospect. 2019, 13, 147–152. [Google Scholar] [CrossRef] [Green Version]
- Şişmanoğlu, S. Fluoride Release of Giomer and Resin Based Fissure Sealants. Odovtos Int. J. Dent. Sci. 2019, 21, 45–52. [Google Scholar] [CrossRef]
- Khudanov, B.O.; Abdullaev, J.R.; Bottenberg, P.; Schulte, A.G. Evaluation of the Fluoride Releasing and Recharging Abilities of Various Fissure Sealants. Oral Health Prev. Dent. 2018, 16, 195–202. [Google Scholar]
- Ibrahim, M.S.; AlQarni, F.D.; Al-Dulaijan, Y.A.; Weir, M.D.; Oates, T.W.; Xu, H.H.K.; Melo, M.A.S. Tuning Nano-Amorphous Calcium Phosphate Content in Novel Rechargeable Antibacterial Dental Sealant. Materials 2018, 11, 1544. [Google Scholar] [CrossRef] [Green Version]
- Surintanasarn, A.; Siralertmukul, K.; Thamrongananskul, N. Fluoride Recharge Ability of Resin-Based Pit and Fissure Sealant with Synthesized Mesoporous Silica Filler. Key Eng. Mater. 2017, 751, 586–591. [Google Scholar]
- Munhoz, T.; Nunes, U.T.; Seabra, L.M.-A.; Monte-Alto, R. Characterization of Mechanical Properties, Fluoride Release and Colour Stability of Dental Sealants. Pesqui. Bras. Odontopediatria Clínica Integr. 2016, 16, 149–158. [Google Scholar] [CrossRef] [Green Version]
- Scougall-Vilchis, R.J.; Salmerón-Valdés, E.N.; Alanis-Tavira, J.; Morales-Luckie, R.A. Comparative study of fluoride released and recharged from conventional pit and fissure sealants versus surface prereacted glass ionomer technology. J. Conserv. Dent. 2016, 19, 41–45. [Google Scholar] [CrossRef]
- Tavassoli-Hojjati, S.; Atai, M.; Haghgoo, R.; Rahimian-Imam, S.; Kameli, S.; Ahmaian-Babaki, F.; Hamzeh, F.; Ahmadyar, M. Comparison of Various Concentrations of Tricalcium Phosphate Nanoparticles on Mechanical Properties and Remineralization of Fissure Sealants. J. Dent. Tehran Univ. Med. Sci. 2014, 11, 379–388. [Google Scholar]
- Abdel-Haffiez, S.H.; Zaher, A.R.; Elharouny, N.M. Effects of a filled fluoride-releasing enamel sealant versus fluoride varnish on the prevention of enamel demineralization under simulated oral conditions. J. World Fed. Orthod. 2013, 2, e133–e136. [Google Scholar] [CrossRef]
- Fan, Y.; Townsend, J.; Wang, Y.; Lee, E.C.; Evans, K.; Hender, E.; Hagan, J.L.; Xu, X. Formulation and characterization of antibacterial fluoride-releasing sealants. Int. J. Clin. Pediatr. Dent. 2013, 35, 13E–18E. [Google Scholar]
- Yang, S.-Y.; Piao, Y.-Z.; Kim, S.-M.; Lee, Y.-K.; Kim, K.-N.; Kim, K.-M. Acid neutralizing, mechanical and physical properties of pit and fissure sealants containing melt-derived 45S5 bioactive glass. Dent. Mater. 2013, 29, 1228–1235. [Google Scholar] [CrossRef]
- Choudhary, P.; Ganesh, M.; Tandon, S.; Mehra, A. Evaluation of the remineralization potential of amorphous calcium phosphate and fluoride containing pit and fissure sealants using scanning electron microscopy. Indian J. Dent. Res. 2012, 23, 157–163. [Google Scholar] [CrossRef]
- Shimazu, K.; Ogata, K.; Karibe, H. Evaluation of the ion-releasing and recharging abilities of a resin-based fissure sealant containing S-PRG filler. Dent. Mater. J. 2011, 30, 923–927. [Google Scholar] [CrossRef] [Green Version]
- Kaga, M.; Masuta, J.; Hoshino, M.; Genchou, M.; Minamikawa, H.; Hashimoto, M.; Yawaka, Y. Mechanical Properties and Ions Release of S-PRG Filler-containing Pit and Fissure Sealant. Nano Biomed. 2011, 3, 191–199. [Google Scholar]
- Wang, Y.; Kaga, M.; Kajiwara, D.; Minamikawa, H.; Kakuda, S.; Hashimoto, M.; Yawaka, Y. Ion Release and Buffering Capacity of S-PRG Filler-containing Pit and Fissure Sealant in Lactic Acid. Nano Biomed. 2011, 3, 275–281. [Google Scholar]
- Alsaffar, A.; Tantbirojn, D.; Versluis, A.; Beiraghi, S. Protective effect of pit and fissure sealants on demineralization of adjacent enamel. Pediatric Dent. 2011, 33, 491–495. [Google Scholar]
- Bayrak, S.; Tunc, E.S.; Aksoy, A.; Ertas, E.; Guvenc, D.; Ozer, S. Fluoride Release and Recharge from Different Materials Used as Fissure Sealants. Eur. J. Dent. 2010, 4, 245–250. [Google Scholar] [CrossRef] [Green Version]
- Shen, C.; Zhang, N.-Z.; Anusavice, K.J. Fluoride and Chlorhexidine Release from Filled Resins. J. Dent. Res. 2010, 89, 1002–1006. [Google Scholar] [CrossRef] [Green Version]
- Kuşgöz, A.; Tüzüner, T.; Ülker, M.; Kemer, B.; Saray, O. Conversion degree, microhardness, microleakage and fluoride release of different fissure sealants. J. Mech. Behav. Biomed. Mater. 2010, 3, 594–599. [Google Scholar] [CrossRef]
- Motohashi, J.; Furukawa, S.; Shimoda, S.; Tsurumoto, A. Transition of Fluoride into Tooth Substance from Sustained Fluoride-Releasing Sealant-In vitro Evaluation. J. Hard Tissue Biol. 2010, 19, 195–202. [Google Scholar] [CrossRef] [Green Version]
- Silva, K.G.; Pedrini, D.; Delbem, A.C.B.; Ferreira, L.; Cannon, M. In situ evaluation of the remineralizing capacity of pit and fissure sealants containing amorphous calcium phosphate and/or fluoride. Acta Odontol. Scand. 2009, 68, 11–18. [Google Scholar] [CrossRef]
- Cildir, S.K.; Sandalli, N. Compressive strength, surface roughness, fluoride release and recharge of four new fluoride-releasing fissure sealants. Dent. Mater. J. 2007, 26, 335–341. [Google Scholar] [CrossRef] [Green Version]
- Loyola-Rodriguez, J.P.; Garcia-Godoy, F. Antibacterial activity of fluoride release sealants on mutans streptococci. J. Clin. Pediatr. Dent. 1996, 20, 109–111. [Google Scholar]
- Roberts, M.W.; Shern, R.J.; Kennedy, J.B. Evaluation of an autopolymerizing fissure sealant as a vehicle for slow release of fluoride. Pediatr. Dent. 1984, 6, 145–147. [Google Scholar]
- Swartz, M.; Phillips, R.; Norman, R.; Elliason, S.; Rhodes, B.; Clark, H. Addition of Fluoride to Pit and Fissure Sealants-A Feasibility Study. J. Dent. Res. 1976, 55, 757–771. [Google Scholar] [CrossRef]
- Krithikadatta, J.; Datta, M.; Gopikrishna, V. CRIS Guidelines (Checklist for Reporting In-vitro Studies): A concept note on the need for standardized guidelines for improving quality and transparency in reporting in-vitro studies in experimental dental research. J. Conserv. Dent. 2014, 17, 301–304. [Google Scholar] [CrossRef] [Green Version]
- Moser, P. Out of Control? Managing Baseline Variability in Experimental Studies with Control Groups. In Handbook of Experimental Pharmacology; Springer: Cham, Switzerland, 2019; Volume 257, pp. 101–117. [Google Scholar] [CrossRef] [Green Version]
- Noordzij, M.; Dekker, F.W.; Zoccali, C.; Jager, K.J. Sample Size Calculations. Nephron Clin. Pract. 2011, 118, c319–c323. [Google Scholar] [CrossRef]
- de Medeiros, R.; Soares, J.; de Sousa, F. Natural enamel caries in polarized light microscopy: Differences in histopathological features derived from a qualitative versus a quantitative approach to interpret enamel birefringence. J. Microsc. 2012, 246, 177–189. [Google Scholar] [CrossRef]
- Klimuszko, E.; Orywal, K.; Sierpinska, T.; Sidun, J.; Gołębiewska, M. Evaluation of calcium and magnesium contents in tooth enamel without any pathological changes: In vitro preliminary study. Odontology 2018, 106, 369–376. [Google Scholar] [CrossRef] [Green Version]
- Koga, H.; Kameyama, A.; Matsukubo, T.; Hirai, Y.; Takaesu, Y. Comparison of short-term in vitro fluoride release and recharge from four different types of pit-and-fissure sealants. Bull. Tokyo Dent. Coll. 2004, 45, 173–179. [Google Scholar] [CrossRef] [Green Version]
- Preston, A.J.; Higham, S.M.; Agalamanyi, E.A.; Mair, L.H. Fluoride recharge of aesthetic dental materials. J. Oral Rehabil. 1999, 26, 936–940. [Google Scholar] [CrossRef]
- Han, L.; Cv, E.; Li, M.; Niwano, K.; Ab, N.; Okamoto, A.; Honda, N.; Iwaku, M. Effect of Fluoride Mouth Rinse on Fluoride Releasing and Recharging from Aesthetic Dental Materials. Dent. Mater. J. 2002, 21, 285–295. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Study | Sampling Bias | Assessment Bias | Reporting Bias | Overall | ||||
|---|---|---|---|---|---|---|---|---|
| Sample Size | Sample Randomization | Sample Preparation | Assessment Methods | Blinding | Presence of Control Group | Definitive Values | ||
| Ibrahim et al., 2020 [33] | + | + | + | + | - | + | - | Moderate |
| Yang et al., 2020 [34] | - | - | + | + | - | + | - | High |
| Bohns et al., 2019 [35] | + | - | + | + | - | + | NA | Moderate |
| Bohns et al., 2019 [36] | + | - | - | + | - | + | NA | High |
| Sadrabad et al., 2019 [37] | + | + | + | - | - | + | + | Moderate |
| Şişmanoğlu et al., 2019 [38] | + | - | + | - | - | + | + | Moderate |
| Khudanov et al., 2018 [39] | + | - | + | - | - | + | + | Moderate |
| Ibrahim et al., 2018 [40] | + | - | + | + | - | + | + | Moderate |
| Utneja et al., 2018 [27] | + | + | + | + | - | + | + | Low |
| Zin EI et al., 2018 [28] | + | + | + | + | - | + | + | Low |
| Kosior et al., 2017 [21] | + | - | + | - | - | - | + | High |
| Nakamura et al., 2017 [20] | + | - | + | + | - | + | - | Moderate |
| Surintanasarn et al., 2017 [41] | + | - | + | - | - | + | + | Moderate |
| Dionysopoulps et al., 2016 [18] | + | - | + | - | - | + | + | Moderate |
| Munhoz et al., 2016 [42] | + | - | + | + | - | + | - | Moderate |
| Salmerón-Valdés et al., 2016 [43] | + | - | + | - | - | - | + | High |
| Zawaideh et al., 2016 [19] | + | + | + | - | - | + | + | Moderate |
| Hojjati et al., 2014 [44] | + | + | + | + | - | + | NA | Moderate |
| Abdel-Haffiez et al., 2013 [45] | + | + | + | - | - | + | + | Moderate |
| Fan et al., 2013 [46] | - | - | + | + | - | + | + | Moderate |
| Kantovitz et al., 2013 [29] | + | + | + | + | + | + | + | Low |
| Yang et al., 2013 [47] | - | - | + | + | - | + | - | High |
| Choudhary et al., 2012 [48] | + | + | + | - | - | + | NA | Moderate |
| Prabhakar at el., 2012 [30] | + | + | + | - | + | + | + | Low |
| Shimazu et al., 2011 [49] | + | - | + | - | - | - | + | High |
| Kaga et al., 2011 [50] | + | - | + | + | - | + | - | Moderate |
| Wang et al., 2011 [51] | + | - | + | + | - | + | - | High |
| AlSaffar et l., 2010 [52] | + | + | + | - | - | + | + | Moderate |
| Bayrak et al., 2010 [53] | + | - | + | - | - | + | + | Moderate |
| Shen et al., 2010 [54] | + | - | + | - | - | - | + | High |
| Kuşgöz et al., 2010 [55] | + | - | + | + | - | + | + | Moderate |
| Motohashi et al., 2010 [56] | + | - | + | + | - | + | + | Moderate |
| Silva et al., 2010 [57] | + | - | + | + | - | - | + | Moderate |
| Cildir et al., 2007 [58] | + | - | + | + | - | + | + | Moderate |
| Salar et al., 2007 [31] | + | + | + | + | + | + | + | Low |
| Lobo et al., 2005 [32] | + | + | + | + | - | + | + | Low |
| Loyola-Rodriquez et al., 1996 [59] | - | - | + | + | - | + | + | Moderate |
| Roberts et al., 1984 [60] | + | - | + | - | - | + | + | Moderate |
| Swartz et al., 1976 [61] | + | - | + | + | - | + | + | Moderate |
| Study | Sample Type | Sample Size per Group | Curing Type | Remineralizing Agent | Assessed Outcomes |
|---|---|---|---|---|---|
| Ibrahim et al., 2020 [33] | Human, non-carious third molars | 8 | Light cure | nACP |
|
| Yang et al., 2020 [34] | Bar-shaped sample (25 mm × 2 mm × 2 mm) | Not mentioned | Light cure | Hydrated calcium silicate |
|
| Bohns et al., 2019 [35] | Surface roughness: Bovine incisors (5 mm × 5 mm × 2 mm) Mineral deposition: Discs-shaped sample (4 mm × 2 mm) | Surface roughness: 6 Mineral deposition: 3 | Light cure | BNNT |
|
| Bohns et al., 2019 [36] | Mineral deposition: Discs-shaped sample (4 mm × 2 mm) | 1 | Light cure |
|
|
| Sadrabad et al., 2019 [37] | Human, non-carious first and second premolars. | 8 | Light cure | Fluoride | PLM imaging |
| Şişmanoğlu et al., 2019 [38] | Discs-shaped sample (5 mm × 2 mm) | 7 | Light cure | Fluoride | Fluoride ions release |
| Khudanov et al., 2018 [39] | Discs-shaped sample (8 mm × 1.8 mm) | 10 |
| Fluoride |
|
| Ibrahim et al., 2018 [40] | Bar-shaped samples (2 mm × 2 mm × 25 mm) | 1 | Light cure |
|
|
| Utneja et al., 2018 [27] | Remineralization potential: Human, non-carious maxillary first premolars. Ion release: Discs-shaped sample (5 mm × 2 mm) | Remineralization: 5 Ion release: 9 | Light cure |
|
|
| Zin EI et al., 2018 [28] | Bovine incisors (7 mm × 7 mm × 2 mm) | 10 |
| Fluoride |
|
| Kosior et al., 2017 [21] | Cylinders-shaped sample | 3 | Light cure | Fluoride | Fluoride ions release |
| Nakamura et al., 2017 [20] | Mineral loss: Human, non-carious deciduous molars. pH changes & Ions release: Bar-shaped sample (3 mm × 6 mm × 6 mm) | 12 | Light cure |
|
|
| Surintanasarn et al., 2017 [41] | Discs-shaped sample (10 mm × 1 mm) | 10 | Light cure | Fluoride |
|
| Dionysopoulps et al., 2016 [18] | Cylinders-shaped samples (7 mm × 2 mm) | 8 |
| Fluoride |
|
| Munhoz et al., 2016 [42] | Cylinders-shaped sample (4 mm × 6 mm) | 4 |
| Fluoride |
|
| Salmerón-Valdés et al., 2016 [43] | Discs-shaped sample: (5 mm × 1 mm) | 8 | Light cure | Fluoride | Fluoride ions release |
| Zawaideh et al., 2016 [19] | Human, non-carious third molar | 25 | Light cure |
| Hardness changes |
| Hojjati et al., 2014 [44] | Human, permanent maxillary/mandibular premolar teeth | 7 | Light cure | β-tricalcium phosphate (β-TCP) |
|
| Abdel-Haffiez et al.,2013 [45] | Human, premolars | 20 | Light cure | Fluoride | PLM imaging |
| Fan et al., 2013 [46] | Discs-shaped sample (5 mm × 1.2 mm) | 1 | Light cure | Fluoride |
|
| Kantovitz et al., 2013 [29] | Human, non-carious third molars (4 mm × 4 mm × 2 mm) | 12 | Light cure | Fluoride |
|
| Yang et al., 2013 [47] | Bar-shaped sample (25 mm × 2 mm × 2 mm) | Light cure | 45S5 Bioactive glass (BAG) |
| |
| Choudhary et al., 2012 [48] | Human, non-carious maxillary first premolar | 10 | Light cure |
| SEM imaging |
| Prabhakar at el., 2012 [30] | Human, non-carious third molars | 20 | Light cure | Fluoride | PLM imaging |
| Shimazu et al., 2011 [49] | Discs-shaped sample (15 mm × 1 mm) | 5 | Light cure | Fluoride |
|
| Kaga et al., 2011 [50] | Discs-shaped sample (6 mm × 3 mm) | 72 | Light cure |
|
|
| Wang et al., 2011 [51] | Discs-shaped sample (13 mm × 1 mm) | 4 | Light cure |
|
|
| AlSaffar et l., 2010 [52] | Human, non-carious mandibular molars and third molars | 10 |
|
|
|
| Bayrak et al., 2010 [53] | Discs-shaped sample (10 mm × 1 mm) | 10 | Light cure | Fluoride |
|
| Shen et al., 2010 [54] | Discs-shaped sample (10 mm × 2 mm) | 30 | Light cure | Fluoride |
|
| Kuşgöz et al., 2010 [55] | Discs-shaped sample (5 mm × 2 mm) |
| Fluoride |
| |
| Motohashi et al., 2010 [56] | Discs-shaped sample (5 mm × 2 mm) | 4 |
| Fluoride |
|
| Silva et al., 2010 [57] | Bar-shaped sample (4 mm × 4 mm × 2 mm mm) | 40 | Light cure |
|
|
| Cildir et al., 2007 [58] | Surface roughness: Discs-shaped sample (8 mm × 2 mm) | 5 |
| Fluoride |
|
| Salar et al., 2007 [31] | Human, non-carious third molar | 15 |
| Fluoride | PLM analysis |
| Lobo et al., 2005 [32] | Human, non-carious third molar | 12 | Light cure | Fluoride |
|
| Loyola-Rodriquez et al., 1996 [59] | Discs-shaped sample (3 mm × 3 mm) | Not mentioned | Light cure | Fluoride |
|
| Roberts et al., 1984 [60] | Part 1 Discs-shaped sample Part 2: Human, non-carious mandibular molars and maxillary premolars | Part 1: 6 Part 2: 8 | Chemical cure | Fluoride | Fluoride ions release |
| Swartz et al., 1976 [61] | Discs-shaped sample (9.5 mm × 2.2 mm) | 8 | Light cure | Fluoride |
|
| Assessment Method | Study | pH-Cycling Protocol | Studied Groups (Mean ± SD) | Summary of Results | ||
|---|---|---|---|---|---|---|
| Hardness Change | Ibrahim et al., 2020 [33] |
|
| The nACP containing sealants showed a significantly lower SHL% in comparison to the negative control group (p < 0.05). | ||
| Zin EI et al.,2018 [28] |
|
| Teethmate F-1 showed a significantly higher SHL% in comparison to all the other groups (p < 0.05). | |||
| Zawaideh et al., 2016 [19] |
|
| There were no statistically significant differences between all the groups (p > 0.05). | |||
| Kantovitz et al., 2013 [29] |
| Under sealants:
| 100 μm Outer sealant:
| FluroShield sealant showed a significantly lower SHL% in comparison to the Helioseal sealant (p < 0.05). | ||
| AlSaffar et al., 2010 [52] |
|
| Clinpro, Bosworth Aegis and GC Fuji Triage sealants showed significantly lower SHL% in comparison to the Delton Opaque and UltraSeal XT plus (p < 0.05). | |||
| Silva et al., 2010 [57] | DE: Prepared solution, 16 h, pH = 5 |
| Aegis, Fluroshield and ESF sealants had higher surface microhardness and %SMHR values than ACP-F sealant. | |||
| Lobo et al., 2005 [32] |
|
| There were no statistically significant differences between all the groups in the hardness of the sealed enamel (p > 0.05). | |||
| SEM-EDX Analysis | Ibrahim et al., 2020 [33] |
|
| The nACP-containing sealant showed higher weight percent of Ca and P in comparison to the negative group (p < 0.05). | ||
| Hojjati et al., 2014 [44] |
|
| Increasing the concentrations of β-TCP decreased the enamel irregularities/crack lines due to demineralization. Sealants containing 4% and 5% of β-TCP showed a homogenous layer at the enamel-sealant interface. | |||
| Polarized light Imaging | Ibrahim et al., 2020 [33] |
|
| The nACP-containing sealant showed a thinner enamel lesion in comparison to the control group. | ||
| Sadrabad et al., 2019 [37] |
| Primary caries:
| There were statistically significant differences between all the groups (p ˂ 0.001). | |||
| Abdel-Haffiez et al., 2013 [45] |
|
| Pro-seal sealant showed a thinner enamel lesion in comparison to the control groups and fluoride varnish sample. | |||
| Prabhakar et al., 2012 [30] | DE: Acidified gelatin gel, 1008 h |
| Guardian SealTM and Fuji VIITM sealants showed a thinner enamel lesions in comparison to Helioseal sealant. | |||
| Silva et al., 2010 [57] | DE: Prepared solution, 16 h, pH = 5 |
| Fluroshield sealants and the experimental sealant containing fluoride showed a thinner enamel lesions in comparison to Aegis sealant. | |||
| Salar et al., 2007 [31] |
|
| ProSeal and GC Fuji Triage and Fuji VIITM sealants showed a thinner enamel lesion in comparison to Delton sealant. | |||
| Surface Roughness | Bohns et al., 2019 [35] |
|
| Sound enamel, 0.1% BNNT sealant and 0.2% BNNT sealant showed significantly lower surface roughness in comparison to the demineralized enamel and control group (p < 0.05). | ||
| Cildir et al., 2007 [58] | Not mentioned | Day1:
| Day 28:
| Day70:
| Clinpro sealant showed significantly lower surface roughness in comparison to Fuji VII sealant (p < 0.0001). | |
| Acid neutralization | Yang et al., 2020 [34] |
|
| The pH of CS-containing and hCS-containing groups was significantly higher than hCS0 group (p < 0.05). | ||
| Yang et al., 2013 [47] | DE: Prepared solution, pH 4 For 3 h |
| The BAG50 sealant showed significantly higher acid neutralization in comparison to all the groups (p < 0.05). | |||
| SEM Imaging | Bohns et al., 2019 [35] |
|
| There were no statistically significant differences between all the groups (p > 0.05). After 28 days in the media, SEM images showed minerals deposition over the BNNT-containing sealants. | ||
| Bohns et al., 2019 [36] |
|
| After 7 days of immersion in artificial saliva, minerals deposition was observed on the surface of sealants containing-TCP and HAP. After 28 days in the media, SEM images showed minerals deposition over SHAP sealants samples. Phosphate peak showed high intensity. | |||
| Utneja et al., 2018 [27] |
|
| The sealants containing HAP had a homogeneous white remineralized area at the tooth surface sealant interface, which was more noticeable in the 30% nHAP filled sealant. Aegis and Delton FS plus sealants had a white irregular globular zone at the tooth surface sealant interface. Clinpro and the prepared unfilled sealants had no white remineralized zone. | |||
| Nakamura et al., 2017 [20] |
|
| BeautiSealant and FujiIILC sealants showed lower demineraliztion, and the enamel-surfaces were smoother than the teathmate F-1 sealant. | |||
| Choudhary et al., 2012 [48] |
|
| Concies sealant showed lower demineralization than the Ageis and Teathmate F-1 sealants. | |||
| Wang et al., 2011 [51] | DE: Lactic acid solution, 24 h, pH = 4.0 |
| BeautiSealant and DELTON FS sealants showed lower demineralization than the Teathmate F-1, Fuji lll LC sealants and control group. | |||
| Shen et al., 2010 [54] |
|
| There was no significant difference between the groups (p > 0.05). Chlorohexidine release was higher when pH decreased. | |||
| Study | Studied Groups (Mean ± SD) | Summary of Results | |
|---|---|---|---|
| Yang et al., 2020 [34] |
| The hCS 37.5, hCS 50.0, and CS 50.0 sealants showed the highest amount of calcium ions release on day 1 then declined dramatically over the immersion time. The hCS 50.0 sealant showed significantly higher initial calcium ions concentration than other groups (p < 0.05) | |
| Şişmanoğlu et al., 2019 [38] | Day 1:
| Day 28:
| For all materials, the highest amount of fluoride ions release was seen on the first day. BeautiSealant group released the highest amount of fluoride ions on the first two days (p < 0.05). There were no significant differences between Clinpro, Fissurit F and HelioSeal F sealants on day 1 (p > 0.05). |
| Khudanov et al., 2018 [39] |
|
| The highest amount of fluoride ions was seen on the first day then decreased with time until recharge. The highest amount of released fluoride ions was seen in Argecem sealant and the least in Helioseal sealant |
| Ibrahim et al., 2018 [40] |
|
| After 70 days of ions release, 30% nACP + 5% DMAHDM sealant released a higher amount of calcium and phosphate ions than 20% nACP + 5% DMAHDM sealant (p < 0.05). |
| Utneja et al., 2018 [27] |
|
| The 10% nHAP + 20% nACP filled sealant showed a higher amount of calcium and phosphate ions release at pH 4 compared to the commercial sealant with ACP (Aegis). |
| Zin EI et al., 2018 [28] | Day 14:
| For all materials, the highest fluoride release was observed after 2 days. FVII sealant released the greatest amount of fluoride followed by the Teethmate F-1and Clinpro sealants. Among all sealants, there were significant differences in fluoride concentrations with different time intervals (p < 0.05). | |
| Kosior et al., 2017 [21] | Day 1:
| Week 14:
| For all materials, the highest fluoride release was observed after 1 h.The highest level of ions release was seen on Deltion FS+, followed by Fissurit FX, Conseal F and Admira Seal sealants. |
| Nakamura et al., 2017 [20] |
| The amount of fluoride and strontium ions released from Fuji III LC was significantly higher than BeautiSealant and Teethmate F-1 sealants. On week 1, BeautiSealant and Teethmate F-1 sealants were not significantly different (p > 0.05). There were significant differences in Strontium ions release between all groups (p < 0.05). | |
| Surintanasarn et al., 2017 [41] | Day 3:
| Day 27:
| On day 3 and 6, initial fluoride release was seen only in RBS with 5% of fluoro-alumino silicate glass. For all groups, fluoride levels on day 9 were at baseline. |
| Dionysopoulos et al., 2016 [18] |
| The highest fluoride ions release was observed in the fluoridated materials after day 1. FX-II sealant released significantly more fluoride than the other materials (p < 0.05) while the BeautiSealant group were the lowest. There was a significant difference in fluoride ions release between the materials (p < 0.05). | |
| Munhoz et al., 2016 [42] |
| Vitro Fil released the highest amount of fluoride. There were no significant differences between Alpha Seal Auto, Alpha Seal Light and Vitro Seal Alpha groups (p < 0.05). | |
| Salmerón-Valdés et al., 2016 [43] | Day 1:
| Day 60:
| For all materials, the highest amount of fluoride ions was observed on the first day and then declined until day 60. There were significant differences in fluoride ions release between the materials (p < 0.005).BeautiSealant group showed the highest fluoride ions release while Clinpro sealant was the lowest. |
| Fan et al., 2013 [46] |
|
| Sealant containing 35% Fluoride-releasing Filler and sealant containing 20% Fluoride-releasing Filler + 15% Bioactive Glass showed the highest fluoride release in comparison to Clinpro sealant (p < 0.005). No fluoride ions release was observed in SeLECT Defense sealant. |
| Shimazu et al., 2011 [49] |
| Day 25:
| There were significant differences between the sealants on day 1 (p < 0.001). All materials showed a decrease in fluoride ions release on day 2. Increase in fluoride ions release presented in BeautiSealant group on days 16,19, 22 and 25. The BeautiSealant showed significant increase in the release of Sodiom (Na), Strontium (Sr), Aluminum (Al), Silicon (Si), and Boron (B) ions. |
| Kaga et al., 2011 [50] |
| For all sealants, the highest amount of fluoride ions was observed in the first week then dropped dramatically in the second week. Fujji III LC sealant showed the highest amount of fluoride ions release at all time periods (p < 0.05), while Teethmate F-12.0 sealant released the smallest amount from third week to the end of the test period. | |
| Wang et al., 2011 [51] |
|
| BeautiSealant groups showed significant release of Si, Sr, Al, B, Na and F, while Fuji lll LC group released less (p < 0.05). Fuji lll LC sealant showed greater fluoride release than of BeautiSealant and Delton FS+ sealants.Teethmate F-1 2.0 sealant released the smallest amount of fluoride. |
| Bayrak et al., 2010 [53] | Day 1:
| Day 21:
| For all materials, the highest amount of fluoride ions release was seen on the first day then decreased dramatically. GI sealants released higher amount of fluoride ions than the other materials (p < 0.05). There were significant differences in fluoride ions release between the materials (p < 0.05). |
| Shen et al., 2010 [54] |
|
| When the pH of the media decreased, the CHX and fluoride ions release increased. Fluoride salt decreased the chlorhexidine release where the chlorhexidine significantly increased the fluoride ions release. |
| Kuşgöz et al., 2010 [55] | Day 1:
| Day 30:
| Fuji Triage group showed the highest fluoride ions release at all the periods when compared to Clinpro and Grandio Seal groups (p < 0.05).Clinpro released fluoride more than Grandio seal with no significant difference between the two groups (p > 0.05). |
| Silva et al., 2010 [57] |
| The highest amount of fluoride ions release was observed in experimental and Fluroshield sealants with no significant differences between them (p > 0.05). The highest amount of calcium ions release was observed in Fluroshield, The highest amount of phosphate ions release was observed in the control group which differed significantly from the other groups (p < 0.05). The lowest amount was observed in ACP-F sealant which was statistically like Aegis (p > 0.05). | |
| Motohashi et al., 2010 [56] |
| FujiIII sealant significantly released more fluoride ions than Teethmate-F1 sealant. | |
| Cildir et al., 2007 [58] |
| The highest amount of fluoride ions was released during the first day then dropped dramatically on the second day. There were significant differences between the RBSs and GICs (p < 0.0001). Fuji VII group exhibited the highest amount of fluoride ions release (p < 0.0001) followed by Ketac Molar, while Clinpro sealant showed the lowest amount of fluoride ions release. | |
| Lobo et al., 2005 [32] |
| The amount of fluoride released during pH-cycling did not change significantly between Clinpro and Concise groups (p < 0.01). Vitremer group released the highest amount of fluoride ions (p < 0.01). | |
| Loyola-Rodriquez et al., 1996 [59] | Day 1:
| Day 7:
| For all sealants, the highest amount of fluoride ions was released in the first two days then gradually decreased to around 50% release after 7 days. Teethmate-F sealant released the highest amount of fluoride ions. |
| Roberts et al., 1984 [60] | Day 1:
| Day 91–180:
| The highest amount of fluoride was released during the first day then dropped dramatically. Resin containing 2.5% sodium fluoride showed the highest fluoride ions release per day at all time periods except 91-180 days. |
| Swartz et al., 1976 [61] |
| The amount of fluoride ions released by the isobutyl cyanoacrylate resin was significantly more than the other three sealants. | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
AlGhannam, M.I.; AlAbbas, M.S.; AlJishi, J.A.; AlRuwaili, M.A.; AlHumaid, J.; Ibrahim, M.S. Remineralizing Effects of Resin-Based Dental Sealants: A Systematic Review of In Vitro Studies. Polymers 2022, 14, 779. https://doi.org/10.3390/polym14040779
AlGhannam MI, AlAbbas MS, AlJishi JA, AlRuwaili MA, AlHumaid J, Ibrahim MS. Remineralizing Effects of Resin-Based Dental Sealants: A Systematic Review of In Vitro Studies. Polymers. 2022; 14(4):779. https://doi.org/10.3390/polym14040779
Chicago/Turabian StyleAlGhannam, Maha Ibrahim, Mana’a Saleh AlAbbas, Jumanah Abdulla AlJishi, Muath Abdulrahman AlRuwaili, Jehan AlHumaid, and Maria Salem Ibrahim. 2022. "Remineralizing Effects of Resin-Based Dental Sealants: A Systematic Review of In Vitro Studies" Polymers 14, no. 4: 779. https://doi.org/10.3390/polym14040779
APA StyleAlGhannam, M. I., AlAbbas, M. S., AlJishi, J. A., AlRuwaili, M. A., AlHumaid, J., & Ibrahim, M. S. (2022). Remineralizing Effects of Resin-Based Dental Sealants: A Systematic Review of In Vitro Studies. Polymers, 14(4), 779. https://doi.org/10.3390/polym14040779