
Differentiating Stages of Bipolar and Unipolar Depression—The Possible Role of sICAM-1 and sVCAM-1
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Design
2.2. sICAM-1 and sVCAM-1 Measurements
2.3. Statistical Analysis
3. Results
3.1. Association between sICAM-1 and sVCAM-1 and Clinical Characteristics of Patients with MDD and BD
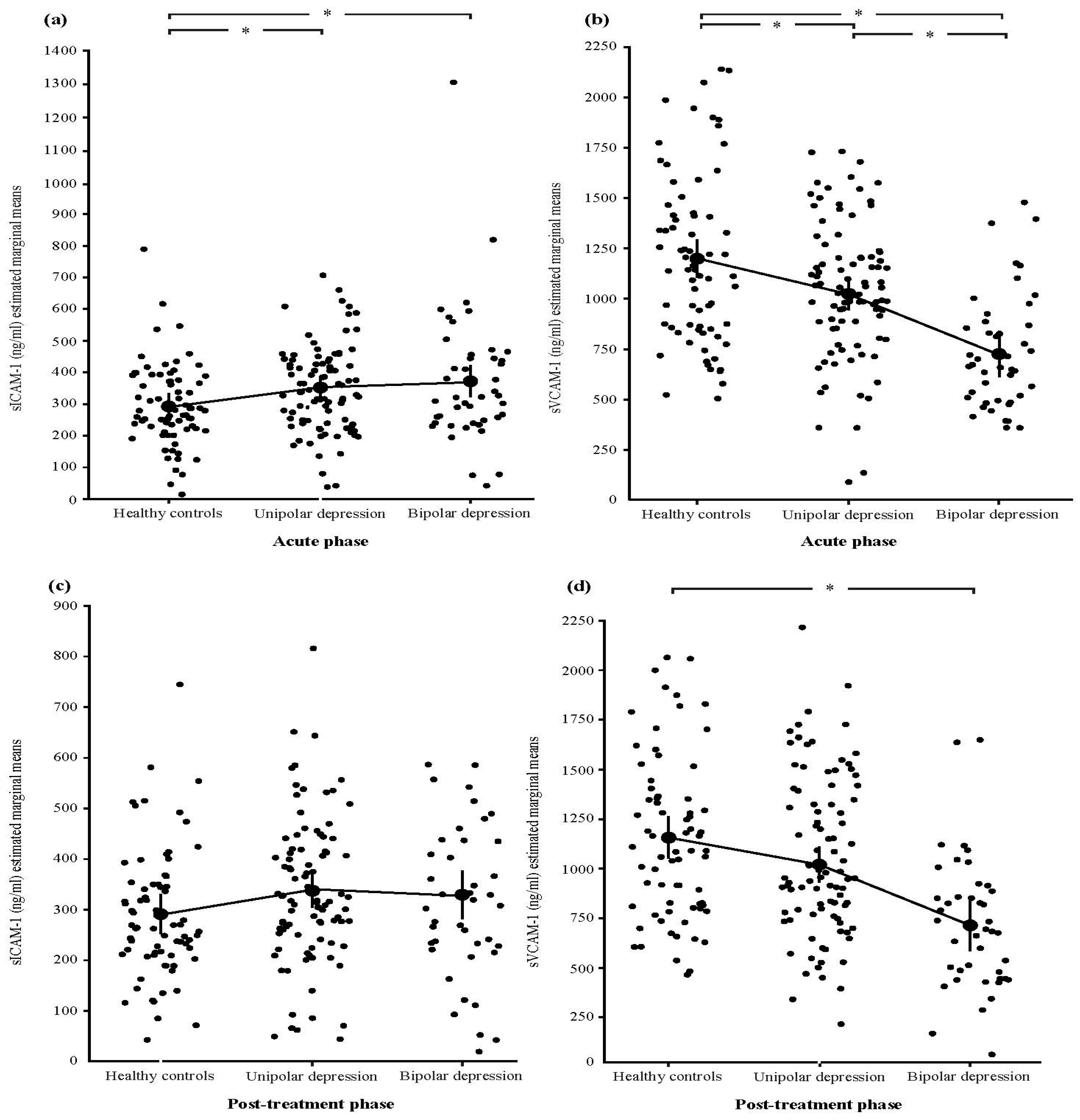
3.2. Differences in sICAM-1 and sVCAM-1 between Patients with MDD and BD and Healthy Controls
3.3. Association between sICAM-1 and sVCAM-1 and Treatment Application
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brunoni, A.R.; Supasitthumrong, T.; Teixeira, A.L.; Vieira, E.L.; Gattaz, W.F.; Benseñor, I.M.; Lotufo, P.A.; Lafer, B.; Berk, M.; Carvalho, A.F.; et al. Differences in the Immune-Inflammatory Profiles of Unipolar and Bipolar Depression. J. Affect. Disord. 2020, 262, 8–15. [Google Scholar] [CrossRef]
- Hori, H.; Teraishi, T.; Sasayama, D.; Hattori, K.; Hashikura, M.; Higuchi, T.; Kunugi, H. Relationship of Temperament and Character with Cortisol Reactivity to the Combined Dexamethasone/CRH Test in Depressed Outpatients. J. Affect. Disord. 2013, 147, 128–136. [Google Scholar] [CrossRef] [PubMed]
- Kapczinski, F.; Magalhães, P.V.S.; Balanzá-Martinez, V.; Dias, V.V.; Frangou, S.; Gama, C.S.; Gonzalez-Pinto, A.; Grande, I.; Ha, K.; Kauer-Sant’Anna, M.; et al. Staging Systems in Bipolar Disorder: An International Society for Bipolar Disorders Task Force Report. Acta Psychiatr. Scand. 2014, 130, 354–363. [Google Scholar] [CrossRef]
- Millar, K.; Lloyd, S.M.; McLean, J.S.; Batty, G.D.; Burns, H.; Cavanagh, J.; Deans, K.A.; Ford, I.; McConnachie, A.; McGinty, A.; et al. Personality, Socio-Economic Status and Inflammation: Cross-Sectional, Population-Based Study. PLoS ONE 2013, 8, e58256. [Google Scholar] [CrossRef]
- Rowland, T.; Perry, B.I.; Upthegrove, R.; Barnes, N.; Chatterjee, J.; Gallacher, D.; Marwaha, S. Neurotrophins, Cytokines, Oxidative Stress Mediators and Mood State in Bipolar Disorder: Systematic Review and Meta-Analyses. Br. J. Psychiatry 2018, 213, 514–525. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, K. Brain-Derived Neurotrophic Factor (BDNF) and Its Precursor ProBDNF as Diagnostic Biomarkers for Major Depressive Disorder and Bipolar Disorder. Eur. Arch. Psychiatry Clin. Neurosci. 2015, 265, 83–84. [Google Scholar] [CrossRef] [PubMed]
- Thomas, A.J.; Davis, S.; Ferrier, I.N.; Kalaria, R.N.; O’Brien, J.T. Elevation of Cell Adhesion Molecule Immunoreactivity in the Anterior Cingulate Cortex in Bipolar Disorder. Biol. Psychiatry 2004, 55, 652–655. [Google Scholar] [CrossRef]
- Turan, Ç.; Kesebir, S.; Süner, Ö. Are ICAM, VCAM and E-Selectin Levels Different in First Manic Episode and Subsequent Remission? J. Affect. Disord. 2014, 163, 76–80. [Google Scholar] [CrossRef]
- Müller, N.; Riedel, M.; Hadjamu, M.; Schwarz, M.J.; Ackenheil, M.; Gruber, R. Increase in expression of adhesion molecule receptors on T helper cells during antipsychotic treatment and relationship to bloodbrain barrier permeability in schizophrenia. Am. J. Psychiatry 1999, 156, 634–636. [Google Scholar] [CrossRef]
- Lassmann, H.; Rössler, K.; Zimprich, F.; Vass, K. Expression of adhesion molecules and histocompatibility antigens at the blood-brain barrier. Brain Pathol. 1991, 1, 115–123. [Google Scholar] [CrossRef]
- Dietrich, J.B. The adhesion molecule ICAM-1 and its regulation in relation with the blood-brain barrier. J. Neuroimmunol. 2002, 128, 58–68. [Google Scholar] [CrossRef] [PubMed]
- Wu, F.; Liu, L.; Zhou, H. Endothelial cell activation in central nervous system inflammation. J. Leukoc. Biol. 2017, 101, 1119–1132. [Google Scholar] [CrossRef] [PubMed]
- Cai, H.Q.; Catts, V.S.; Webster, M.J.; Galletly, C.; Liu, D.; O’Donnell, M.; Weickert, T.W.; Weickert, C.S. Increased macrophages and changed brain endothelial cell gene expression in the frontal cortex of people with schizophrenia displaying inflammation. Mol. Psychiatry 2020, 25, 761–775. [Google Scholar] [CrossRef] [PubMed]
- Ormel, P.R.; Böttcher, C.; Gigase, F.A.J.; Missall, R.D.; van Zuiden, W.; Fernández Zapata, M.C.; Ilhan, D.; de Goeij, M.; Udine, E.; Sommer, I.E.C.; et al. A characterization of the molecular phenotype and inflammatory response of schizophrenia patient derived microglia-like cells. Brain Behav. Immun. 2020, 90, 196–207. [Google Scholar] [CrossRef] [PubMed]
- Berry, M.; Logan, A. CNS Injuries Cellular Responses and Pharmacological Strategies; CRC Press: Boca Raton, FL, USA, 2019. [Google Scholar]
- Spampinato, S.F.; Merlo, S.; Fagone, E.; Fruciano, M.; Barbagallo, C.; Kanda, T.; Sano, Y.; Purrello, M.; Vancheri, C.; Ragusa, M.; et al. Astrocytes Modify Migration of Pbmcs Induced by β-Amyloid in a Blood-Brain Barrier in Vitro Model. Front. Cell. Neurosci. 2019, 13, 337. [Google Scholar] [CrossRef]
- Dimopoulos, N.; Piperi, C.; Salonicioti, A.; Mitsonis, C.; Liappas, I.; Lea, R.W.; Kalofoutis, A. Elevation of Plasma Concentration of Adhesion Molecules in Late-Life Depression. Int. J. Geriatr. Psychiatry 2006, 21, 965–971. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, J.B.; Ryan, K.M.; Harkin, A.; Connor, T.J. Noradrenaline Reuptake Inhibitors Inhibit Expression of Chemokines IP-10 and RANTES and Cell Adhesion Molecules VCAM-1 and ICAM-1 in the CNS Following a Systemic Inflammatory Challenge. J. Neuroimmunol. 2010, 220, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Saengjaroentham, C.; Supornsilpchai, W.; Ji-Au, W.; Srikiatkhachorn, A.; Maneesri-Le Grand, S. Serotonin Depletion Can Enhance the Cerebrovascular Responses Induced by Cortical Spreading Depression via the Nitric Oxide Pathway. Int. J. Neurosci. 2014, 125, 130–139. [Google Scholar] [CrossRef]
- Meixensberger, S.; Kuzior, H.; Fiebich, B.L.; Süß, P.; Runge, K.; Berger, B.; Nickel, K.; Denzel, D.; Schiele, M.A.; Michel, M.; et al. Upregulation of sICAM-1 and sVCAM-1 Levels in the Cerebrospinal Fluid of Patients with Schizophrenia Spectrum Disorders. Diagnostics 2021, 11, 1134. [Google Scholar] [CrossRef]
- Müller, N. The Role of Intercellular Adhesion Molecule-1 in the Pathogenesis of Psychiatric Disorders. Front. Pharmacol. 2019, 10, 1251. [Google Scholar] [CrossRef]
- Miguel-Hidalgo, J.J.; Overholser, J.C.; Jurjus, G.J.; Meltzer, H.Y.; Dieter, L.; Konick, L.; Stockmeier, C.A.; Rajkowska, G. Vascular and Extravascular Immunoreactivity for Intercellular Adhesion Molecule 1 in the Orbitofrontal Cortex of Subjects with Major Depression: Age-Dependent Changes. J. Affect. Disord. 2011, 132, 422. [Google Scholar] [CrossRef]
- Schaefer, M.; Sarkar, S.; Schwarz, M.; Friebe, A. Soluble Intracellular Adhesion Molecule-1 in Patients with Unipolar or Bipolar Affective Disorders: Results from a Pilot Trial. Neuropsychobiology 2016, 74, 8–14. [Google Scholar] [CrossRef]
- Serebruany, V.L.; Suckow, R.F.; Cooper, T.B.; O’Connor, C.M.; Malinin, A.I.; Krishnan, K.R.; van Zyl, L.T.; Lekht, V.; Glassman, A.H. Sertraline Antidepressant Heart Attack Randomized Trial. Relationship between release of platelet/endothelial biomarkers and plasma levels of sertraline and N-desmethylsertraline in acute coronary syndrome patients receiving SSRI treatment for depression. Am. J. Psychiatry 2005, 162, 1165–1170. [Google Scholar] [CrossRef] [PubMed]
- van Zyl, L.T.; Lespérance, F.; Frasure-Smith, N.; Malinin, A.I.; Atar, D.; Laliberté, M.A.; Serebruany, V.L. Platelet and endothelial activity in comorbid major depression and coronary artery disease patients treated with citalopram: The Canadian Cardiac Randomized Evaluation of Antidepressant and Psychotherapy Efficacy Trial (CREATE) biomarker sub-study. J. Thromb. Thrombolysis 2009, 27, 48–56. [Google Scholar] [CrossRef]
- Yu, B.; Becnel, J.; Zerfaoui, M.; Rohatgi, R.; Boulares, A.H.; Nichols, C.D. Serotonin 5-hydroxytryptamine(2A) receptor activation suppresses tumor necrosis factor-alpha-induced inflammation with extraordinary potency. J. Pharmacol. Exp. Ther. 2008, 327, 316–323. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, M.J.; Riedel, M.; Ackenheil, M.; Müller, N. Decreased Levels of Soluble Intercellular Adhesion Molecule-1 (SICAM-1) in Unmedicated and Medicated Schizophrenic Patients. Biol. Psychiatry 2000, 47, 29–33. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Hirschfeld, R.M.A.; Williams, J.B.W.; Spitzer, R.L.; Calabrese, J.R.; Flynn, L.; Keck, J.; Lewis, L.; McElroy, S.L.; Post, R.M.; Rapport, D.J.; et al. Development and Validation of a Screening Instrument for Bipolar Spectrum Disorder: The Mood Disorder Questionnaire. Am. J. Psychiatry 2000, 157, 1873–1875. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, M. Development of a Rating Scale for Primary Depressive Illness. Br. J. Soc. Clin. Psychol. 1967, 6, 278–296. [Google Scholar] [CrossRef] [PubMed]
- Young, R.C.; Biggs, J.T.; Ziegler, V.E.; Meyer, D.A. A Rating Scale for Mania: Reliability, Validity and Sensitivity. Br. J. Psychiatry 1978, 133, 429–435. [Google Scholar] [CrossRef]
- Guy, W. ECDEU Assessment Manual for Psychopharmacology; U.S. Department of Health, Education, and Welfare: Rockville, MD, USA, 1976. [Google Scholar]
- Spearing, M.K.; Post, R.M.; Leverich, G.S.; Brandt, D.; Nolen, W. Modification of the Clinical Global Impressions (CGI) Scale for Use in Bipolar Illness (BP): The CGI-BP. Psychiatry Res. 1997, 73, 159–171. [Google Scholar] [CrossRef]
- Kapczinski, F.; Dias, V.V.; Kauer-Sant’Anna, M.; Brietzke, E.; Vázquez, G.H.; Vieta, E.; Berk, M. The Potential Use of Biomarkers as an Adjunctive Tool for Staging Bipolar Disorder. Prog. Neuropsychopharmacol. Biol. Psychiatry 2009, 33, 1366–1371. [Google Scholar] [CrossRef]
- Dawood, T.; Barton, D.A.; Lambert, E.A.; Eikelis, N.; Lambert, G.W. Examining Endothelial Function and Platelet Reactivity in Patients with Depression before and after SSRI Therapy. Front. Psychiatry 2016, 7, 18. [Google Scholar] [CrossRef]
- Durgam, S.; Starace, A.; Li, D.; Migliore, R.; Ruth, A.; Németh, G.; Laszlovszky, I. The Efficacy and Tolerability of Cariprazine in Acute Mania Associated with Bipolar I Disorder: A Phase II Trial. Bipolar Disord. 2015, 17, 63–75. [Google Scholar] [CrossRef]
- Tohen, M.; Frank, E.; Bowden, C.L.; Colom, F.; Ghaemi, S.N.; Yatham, L.N.; Malhi, G.S.; Calabrese, J.R.; Nolen, W.A.; Vieta, E.; et al. The International Society for Bipolar Disorders (ISBD) Task Force Report on the Nomenclature of Course and Outcome in Bipolar Disorders. Bipolar Disord. 2009, 11, 453–473. [Google Scholar] [CrossRef] [PubMed]
- Witkowska, A.M.; Borawska, M.H. Soluble Intercellular Adhesion Molecule-1 (SICAM-1): An Overview. Eur. Cytokine Netw. 2004, 15, 91–98. [Google Scholar] [PubMed]
- Lynch, D.F.; Hassen, W.; Clements, M.A.; Schellhammer, P.F.; Wright, G.L. Serum levels of endothelial and neural cell adhesion molecules in prostate cancer. Prostate 1997, 32, 214–220. [Google Scholar] [CrossRef]
- Stefanović, M.P.; Petronijević, N.; Dunjić-Kostić, B.; Velimirović, M.; Nikolić, T.; Jurišić, V.; Lačković, M.; Damjanović, A.; Totić-Poznanović, S.; Jovanović, A.A.; et al. Role of SICAM-1 and SVCAM-1 as Biomarkers in Early and Late Stages of Schizophrenia. J. Psychiatr. Res. 2016, 73, 45–52. [Google Scholar] [CrossRef]
- Thomas, A.J.; Ferrier, I.N.; Kalaria, R.N.; Davis, S.; O’Brien, J.T. Cell Adhesion Molecule Expression in the Dorsolateral Prefrontal Cortex and Anterior Cingulate Cortex in Major Depression in the Elderly. Br. J. Psychiatry 2002, 181, 129–134. [Google Scholar] [CrossRef]
- Thomas, A.J.; Perry, R.; Kalaria, R.N.; Oakley, A.; McMeekin, W.; O’Brien, J.T. Neuropathological Evidence for Ischemia in the White Matter of the Dorsolateral Prefrontal Cortex in Late-Life Depression. Int. J. Geriatr. Psychiatry 2003, 18, 7–13. [Google Scholar] [CrossRef]
- Kobawala, T.P.; Trivedi, T.I.; Gajjar, K.K.; Patel, D.H.; Patel, G.H.; Ghosh, N.R. Significance of TNF-α and the Adhesion Molecules: L-Selectin and VCAM-1 in Papillary Thyroid Carcinoma. J. Thyroid Res. 2016, 2016, 8143695. [Google Scholar] [CrossRef]
- Pantović-Stefanović, M.; Petronijević, N.; Dunjić-Kostić, B.; Velimirović, M.; Nikolić, T.; Jurišić, V.; Lačković, M.; Damjanović, A.; Totić-Poznanović, S.; Jovanović, A.A.; et al. SVCAM-1, SICAM-1, TNF-α and IL-6 Levels in Bipolar Disorder Type I: Acute, Longitudinal and Therapeutic Implications. Biol. Psychiatry 2016, 19 (Suppl. S2), S41–S51. [Google Scholar] [CrossRef] [PubMed]
- Tchalla, A.E.; Wellenius, G.A.; Sorond, F.A.; Travison, T.G.; Dantoine, T.; Lipsitz, L.A. Elevated Circulating Vascular Cell Adhesion Molecule-1 (SVCAM-1) Is Associated with Concurrent Depressive Symptoms and Cerebral White Matter Hyperintensities in Older Adults Biology and Technology. BMC Geriatr. 2015, 15, 62. [Google Scholar] [CrossRef] [PubMed]
- Rosenblat, J.D.; McIntyre, R.S. Bipolar Disorder and Immune Dysfunction: Epidemiological Findings, Proposed Pathophysiology and Clinical Implications. Brain Sci. 2017, 7, 144. [Google Scholar] [CrossRef]
- Baldessarini, R.J.; Undurraga, J.; Vázquez, G.H.; Tondo, L.; Salvatore, P.; Ha, K.; Khalsa, H.M.K.; Lepri, B.; Ha, T.H.; Chang, J.S.; et al. Predominant recurrence polarity among 928 adult international bipolar I disorder patients. Acta Psychiatr. Scand. 2012, 125, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Nivoli, A.M.A.; Pacchiarotti, I.; Rosa, A.R.; Popovic, D.; Murru, A.; Valenti, M.; Bonnin, C.M.; Grande, I.; Sanchez-Moreno, J.; Vieta, E.; et al. Gender differences in a cohort study of 604 bipolar patients: The role of predominant polarity. J. Affect. Disord. 2011, 133, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Bai, Y.M.; Su, T.P.; Li, C.T.; Tsai, S.J.; Chen, M.H.; Tu, P.C.; Chiou, W.F. Comparison of Pro-Inflammatory Cytokines among Patients with Bipolar Disorder and Unipolar Depression and Normal Controls. Bipolar Disord. 2015, 17, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Rose, D.M.; Cardarelli, P.M.; Cobb, R.R.; Ginsberg, M.H. Soluble VCAM-1 Binding to A4 Integrins Is Cell-Type Specific and Activation Dependent and Is Disrupted during Apoptosis in T Cells. Blood 2000, 95, 602–609. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, M.; Schild, D.; Teunissen, C. Contactins in the Central Nervous System: Role in Health and Disease. Neural Regen. Res. 2019, 14, 206. [Google Scholar] [CrossRef] [PubMed]
- Larochelle, C.; Alvarez, J.I.; Prat, A.; Williams, R.; Flügel, A.; Just, W. How Do Immune Cells Overcome the Blood–Brain Barrier in Multiple Sclerosis? FEBS Lett. 2011, 585, 3770–3780. [Google Scholar] [CrossRef]
- Rana, A.; Musto, A.E. The Role of Inflammation in the Development of Epilepsy. J. Neuroinflamm. 2018, 15, 144. [Google Scholar] [CrossRef]
- Castaño-Ramírez, O.M.; Sepúlveda-Arias, J.C.; Duica, K.; Díaz Zuluaga, A.M.; Vargas, C.; López-Jaramillo, C. Inflammatory Markers in the Staging of Bipolar Disorder: A Systematic Review of the Literature. Rev. Colomb. Psiquiatr. (Engl. Ed.) 2018, 47, 119–128. [Google Scholar] [CrossRef] [PubMed]
- Maes, M.; Mihaylova, I.; Kubera, M.; Ringel, K. Activation of Cell-Mediated Immunity in Depression: Association with Inflammation, Melancholia, Clinical Staging and the Fatigue and Somatic Symptom Cluster of Depression. Prog. Neuropsychopharmacol. Biol. Psychiatry 2012, 36, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Wysokiński, A.; Szczepocka, E. Platelet Parameters (PLT, MPV, P-LCR) in Patients with Schizophrenia, Unipolar Depression and Bipolar Disorder. Psychiatry Res. 2016, 237, 238–245. [Google Scholar] [CrossRef] [PubMed]
- Maes, M.H.; Stoyanov, D. False dogmas in mood disorders research: Towards a nomothetic network approach. World J. Psychiatry 2022, 12, 651–667. [Google Scholar] [CrossRef] [PubMed]
- Maes, M.; Moraes, J.B.; Bonifacio, K.L.; Barbosa, D.S.; Vargas, H.O.; Michelin, A.P.; Nunes, S.O.V. Towards a new model and classification of mood disorders based on risk resilience, neuro-affective toxicity, staging, and phenome features using the nomothetic network psychiatry approach. Metab. Brain Dis. 2021, 36, 509–521. [Google Scholar] [CrossRef] [PubMed]
- Van Sloten, T.T.; Schram, M.T.; Adriaanse, M.C.; Dekker, J.M.; Nijpels, G.; Teerlink, T.; Scheffer, P.G.; Pouwer, F.; Schalkwijk, C.G.; Stehouwer, C.D.A.; et al. Endothelial Dysfunction Is Associated with a Greater Depressive Symptom Score in a General Elderly Population: The Hoorn Study. Psychol. Med. 2014, 44, 1403–1416. [Google Scholar] [CrossRef] [PubMed]
- Osimo, E.F.; Pillinger, T.; Rodriguez, I.M.; Khandaker, G.M.; Pariante, C.M.; Howes, O.D. Inflammatory Markers in Depression: A Meta-Analysis of Mean Differences and Variability in 5166 Patients and 5083 Controls. Brain Behav. Immun. 2020, 87, 901–909. [Google Scholar] [CrossRef]
- Giovannoni, G.; Miller, D.H.; Losseff, N.A.; Sailer, M.; Lewellyn-Smith, N.; Thompson, A.J.; Thompson, E.J. Serum Inflammatory Markers and Clinical/MRI Markers of Disease Progression in Multiple Sclerosis. J. Neurol. 2001, 248, 487–495. [Google Scholar] [CrossRef] [PubMed]
- Jeon, S.W.; Kim, Y.K. The Role of Neuroinflammation and Neurovascular Dysfunction in Major Depressive Disorder. J. Inflamm. Res. 2018, 11, 179. [Google Scholar] [CrossRef]
- Wolkowitz, O.M.; Mellon, S.H.; Epel, E.S.; Lin, J.; Dhabhar, F.S.; Su, Y.; Reus, V.I.; Rosser, R.; Burke, H.M.; Kupferman, E.; et al. Leukocyte Telomere Length in Major Depression: Correlations with Chronicity, Inflammation and Oxidative Stress-Preliminary Findings. PLoS ONE 2011, 6, e17837. [Google Scholar] [CrossRef]
- Goodwin, F.K.; Jamison, K.R. Manic-Depressive Illness: Bipolar Disorders and Recurrent Depression; Oxford University Press: Oxford, UK, 2007; pp. 3–9. [Google Scholar]
- Motovsky, B.; Pecenak, J. Psychopathological characteristics of bipolar and unipolar depression-potential indicators of bipolarity. Psychiatr. Danub. 2013, 25, 34–39. [Google Scholar] [PubMed]
- Berk, M.; Williams, L.J.; Jacka, F.N.; O’Neil, A.; Pasco, J.A.; Moylan, S.; Allen, N.B.; Stuart, A.L.; Hayley, A.C.; Byrne, M.L.; et al. So Depression Is an Inflammatory Disease, but Where Does the Inflammation Come From? BMC Med. 2013, 11, 200. [Google Scholar] [CrossRef]
- Okugawa, Y.; Miki, C.; Toiyama, Y.; Koike, Y.; Yokoe, T.; Saigusa, S.; Tanaka, K.; Inoue, Y.; Kusunoki, M. Soluble VCAM-1 and its relation to disease progression in colorectal carcinoma. Exp. Ther. Med. 2010, 1, 463–469. [Google Scholar] [CrossRef]
- Brishti, M.A.; Raghavan, S.; Lamar, K.; Singh, U.P.; Collier, D.M.; Leo, M.D. Diabetic Endothelial Cell Glycogen Synthase Kinase 3β Activation Induces VCAM1 Ectodomain Shedding. Int. J. Mol. Sci. 2023, 24, 14105. [Google Scholar] [CrossRef] [PubMed]
- Niles, A.N.; Smirnova, M.; Lin, J.; O’Donovan, A. Gender differences in longitudinal relationships between depression and anxiety symptoms and inflammation in the health and retirement study. Psychoneuroendocrinology 2018, 95, 149–157. [Google Scholar] [CrossRef]
- Trabace, L.; Roviezzo, F.; Rossi, A. Editorial: Sex Differences in Inflammatory Diseases. Front. Pharmacol. 2022, 13, 962869. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Socio-Demographic Variables | BD (n = 44) | UD (n = 93) | Healthy Controls (n = 73) | Statistics | p-Values |
|---|---|---|---|---|---|
| Sex (female, %) | 93.70 | 64.10 | 56.80 | χ2 = 13.430 | 0.001 a |
| Age (years) | 46.62 ± 9.76 | 47.54 ± 8.59 | 45.82 ± 8.19 | F = 20.550 | 0.291 b |
| BMI (kg/m2) | 24.51 ± 4.05 | 23.94 ± 2.36 | 24.98 ± 3.79 | F = 11.383 | 0.163 b |
| Smoker (yes, %) | 65.10 | 56.50 | 48.60 | χ2 = 3.075 | 0.215 a |
| Marital state (with partner, %) | 60.50 | 64.70 | 61.10 | χ2 = 0.221 | 0.638 a |
| Education (years) | 12.28 ± 2.16 | 11.28 ± 2.18 | 14.38 ± 2.44 | F = 122.335 | <0.001 b |
| Employed (%) | 30.20 | 62.40 | 87.30 | χ2 = 38.314 | <0.001 a |
| Clinical Variables | |||||
| Age of onset (years) | 29.74 ± 9.57 | 39.39 ± 11.01 | - | t = −4.870 | <0.001 c |
| Duration of illness (years) | 18.76 ± 10.93 | 12.96 ± 8.68 | - | t = 3.299 | 0.001 c |
| Number of previous episodes | 11.11 ± 7.80 | 5.10 ± 3.00 | - | t = 6.378 | <0.001 c |
| Number of previous inpatient treatments | 8.74 ± 7.96 | 3.98 ± 3.18 | - | t = 4.906 | <0.001 c |
| Duration of current episode (months) | 2.05 ± 1.02 | 2.92 ± 1.47 | - | t = −3.475 | 0.001 a |
| Duration of untreated disorder (months) | 113.86 ± 94.49 | 47.97 ± 53.16 | - | t = 5.122 | <0.001 c |
| Early-stage disorder (%) | 43.18 | 48.39 | - | χ2 = 1.247 | 0.176 a |
| HDRS—Acute phase | 27.33 ± 10.30 | 23.85 ± 5.62 | - | t = 5.113 | <0.001 c |
| HDRS—Remission phase | 4.98 ± 2.25 | 3.56 ± 3.07 | - | t = 3.285 | 0.001 c |
| YMRS—Acute phase | 5.02 ± 1.42 | 3.22 ± 2.04 | - | t = 4.734 | <0.001 c |
| YMRS—Remission phase | 1.42 ± 1.91 | 1.56 ± 1.22 | - | t = 2.190 | 0.231 c |
| CGI-S | 4.86 ± 0.82 | 4.62 ± 0.44 | - | t = 4.906 | 0.381 c |
| Applied treatment (%) | |||||
| Mood stabilizer | 72.72 | 11.83 | - | χ2 = 51.089 | <0.001 d |
| Antidepressant | 45.45 | 100.00 | - | χ2 = 57.784 | <0.001 d |
| Antypsychotic | 56.81 | 17.20 | - | χ2 = 20.502 | <0.001 d |
| Psychiatric heredity (yes, %) | 63.63 | 43.01 | - | χ2 = 4.291 | 0.038 d |
| Heredity for the same disorder | 4.70 | 31.18 | - | - | <0.001 e |
| Psychotic episode (yes, %) | 36.36 | 17.20 | - | χ2 = 5.101 | 0.024 d |
| Time to remission (days) | 36.09 ± 14.16 | 31.07 ± 10.47 | - | t = 2.268 | 0.025 c |
| BD and UD | BD | UD | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Course of Illness Characteristics | sVCAM-1 | sICAM-1 | sVCAM-1 | sICAM-1 | sVCAM-1 | sICAM-1 | ||||||
| A | R | A | R | A | R | A | R | A | R | A | R | |
| Age of onset (years) | 0.170 | 0.136 | −0.026 | −0.069 | 0.249 | 0.290 | 0.232 | 0.112 | −0.002 | −0.364 | −0.127 | −0.151 |
| Duration of illness (years) | −0.190 | −0.190 | 0.146 | 0.028 | −0.212 | −0.262 | −0.152 | −0.086 | −0.016 | 0.316 | 0.394 *** | 0.127 |
| Number of episodes, total | −0.272 ** | −0.190 | −0.120 | 0.017 | −0.177 | 0.123 | −0.182 | −0.072 | 0.048 | −0.104 | 0.030 | −0.041 |
| Number of previous inpatient treatments | −0.230 * | −0.123 | −0.079 | 0.016 | −0.149 | 0.169 | −0.176 | −0.125 | 0.027 | −0.111 | 0.033 | −0.11 |
| Duration of current episode (months) | 0.087 | −0.054 | 0.167 | −0.083 | −0.286 | −0.237 | 0.042 | −0.332 | 0.029 | −0.026 | 0.317 ** | 0.152 |
| Duration of untreated disorder (months) | −0.186 | −0.256 | −0.167 | −0.176 | −0.125 | −0.230 | −0.227 | −0.274 | −0.013 | −0.034 | 0.141 | −0.193 |
| HDRS—Acute phase | −0.180 | −0.060 | −0.004 | −0.002 | 0.072 | 0.148 | 0.357 * | 0.190 | −0.203 | −0.282 | −0.031 | −0.209 |
| HDRS—Remission phase | −0.033 | 0.192 | 0.045 | −0.079 | −0.037 | 0.175 | 0.039 | −0.030 | −0.029 | 0.098 | 0.043 | −0.032 |
| YMRS—Acute phase | 0.007 | −0.056 | −0.299 | −0.313 | ||||||||
| YMRS—Remission phase | −0.059 | −0.125 | −0.257 | −0.245 | ||||||||
| CGI-S | −0.117 | −0.156 | 0.034 | −0.195 | −0.207 | −0.188 | 0.004 | −0.115 | −0.109 | −0.113 | 0.044 | −0.201 |
| Time to remission (days) | −0.266 * | −0.114 | −0.127 | −0.015 | −0.137 | 0.148 | −0.097 | −0.155 | −0.227 | −0.144 | 0.041 | 0.139 |
| Variables | Multivariate Regression | ||
|---|---|---|---|
| Acute Phase | B | 95% CI | p |
| Sex (female) | −1.772 | −27.718 to −0.793 | 0.002 |
| Age (years) | 0.066 | 0.019–0.140 | 0.011 |
| BMI | 0.349 | −0.871 to −0.128 | 0.10 |
| Smoking | −0.393 | −1.515 to 0.687 | 0.416 |
| ICAM-1 | 0.001 | −0.002–0.005 | 0.558 |
| Sex (female) | −1.62 | −20.41 to −0.37 | 0.110 |
| Age (years) | 0.036 | −0.029–0.118 | 0.244 |
| BMI | −0.274 | −0.693 to −0.090 | 0.17 |
| Smoking | 0.317 | −0.873–1.790 | 0.621 |
| VCAM-1 | 0.003 | 0.001–0.007 | 0.004 |
| Remission | B | 95% CI | p |
| Sex (female) | −1.227 | −21.182–0.096 | 0.046 |
| Age (years) | 0.075 | 0.016–0.177 | 0.012 |
| BMI | −0.240 | −0.655 to −0.027 | 0.047 |
| Smoking | −0.200 | −1.609–1.411 | 0.757 |
| ICAM-1 | 0.002 | −0.002–0.006 | 0.282 |
| Sex (female) | −1.056 | −22.387–0.909 | 0.189 |
| Age (years) | 0.035 | −0.043–0.133 | 0.332 |
| BMI | −0.188 | −0.585 to −0.03 | 0.084 |
| Smoking | 0.234 | −1.501–2.121 | 0.736 |
| VCAM-1 | 0.002 | 0.0001–0.005 | 0.012 |
| Immune Mediator | Unipolar Depression (UD) | Bipolar Depression (BD) | Healthy Controls | UD vs. HC (p) a | BD vs. HC (p) a | ||||
|---|---|---|---|---|---|---|---|---|---|
| Early Stage | Late Stage | Early Stage | Late Stage | Early Stage | Late Stage | Early Stage | Late Stage | ||
| Pre-treatment sICAM-1 | 301.80 ± 113.34 | 402.02 ± 133.54 | 332.83 ± 159.65 | 387.87 ± 196.24 | 305.52 ± 132.59 | 0.803 | 0.002 * | 0.534 | 0.032 * |
| Post-treatment sICAM-1 | 362.88 ± 167.63 | 324.71 ± 213.48 | 320.65 ± 168.34 | 376.93 ± 136.39 | 305.52 ± 132.59 | 0.114 | 0.664 | 0.779 | 0.033 |
| Pre-treatment sVCAM-1 | 992.82 ± 376.42 | 1095.88 ± 271.88 | 675.06 ± 234.36 | 687.82 ± 111.02 | 1193.36 ± 428.74 | 0.029 * | 0.045 * | 0.001 * | 0.001 * |
| Post-treatment sVCAM-1 | 1065.82 ± 460.33 | 1121.09 ± 532.05 | 757.64 ± 515.10 | 696.01 ± 294.36 | 1193.36 ± 428.74 | 0.358 | 0.527 | 0.003 * | 0.001 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pantovic-Stefanovic, M.; Petronijevic, N.; Dunjic-Kostic, B.; Velimirovic, M.; Jurisic, V.; Nikolic, T.; Dodic, S.; Ivkovic, M. Differentiating Stages of Bipolar and Unipolar Depression—The Possible Role of sICAM-1 and sVCAM-1. Cells 2024, 13, 1213. https://doi.org/10.3390/cells13141213
Pantovic-Stefanovic M, Petronijevic N, Dunjic-Kostic B, Velimirovic M, Jurisic V, Nikolic T, Dodic S, Ivkovic M. Differentiating Stages of Bipolar and Unipolar Depression—The Possible Role of sICAM-1 and sVCAM-1. Cells. 2024; 13(14):1213. https://doi.org/10.3390/cells13141213
Chicago/Turabian StylePantovic-Stefanovic, Maja, Natasa Petronijevic, Bojana Dunjic-Kostic, Milica Velimirovic, Vladimir Jurisic, Tatjana Nikolic, Sara Dodic, and Maja Ivkovic. 2024. "Differentiating Stages of Bipolar and Unipolar Depression—The Possible Role of sICAM-1 and sVCAM-1" Cells 13, no. 14: 1213. https://doi.org/10.3390/cells13141213