
Relevance of PNPLA3, TM6SF2, HSD17B13, and GCKR Variants to MASLD Severity in an Egyptian Population

 , , ,
, , ,
Abstract
1. Introduction
2. Patients and Methods
2.1. Bioinformatic Analysis
2.2. Patients
2.2.1. Evaluation of the Stages of Hepatic Steatosis and Liver Fibrosis
2.2.2. Genotyping
2.3. Statistical Analysis
3. Results
3.1. Bioinformatic Analyses
3.2. Baseline Characteristics of the Study Population
3.3. Genotype Data
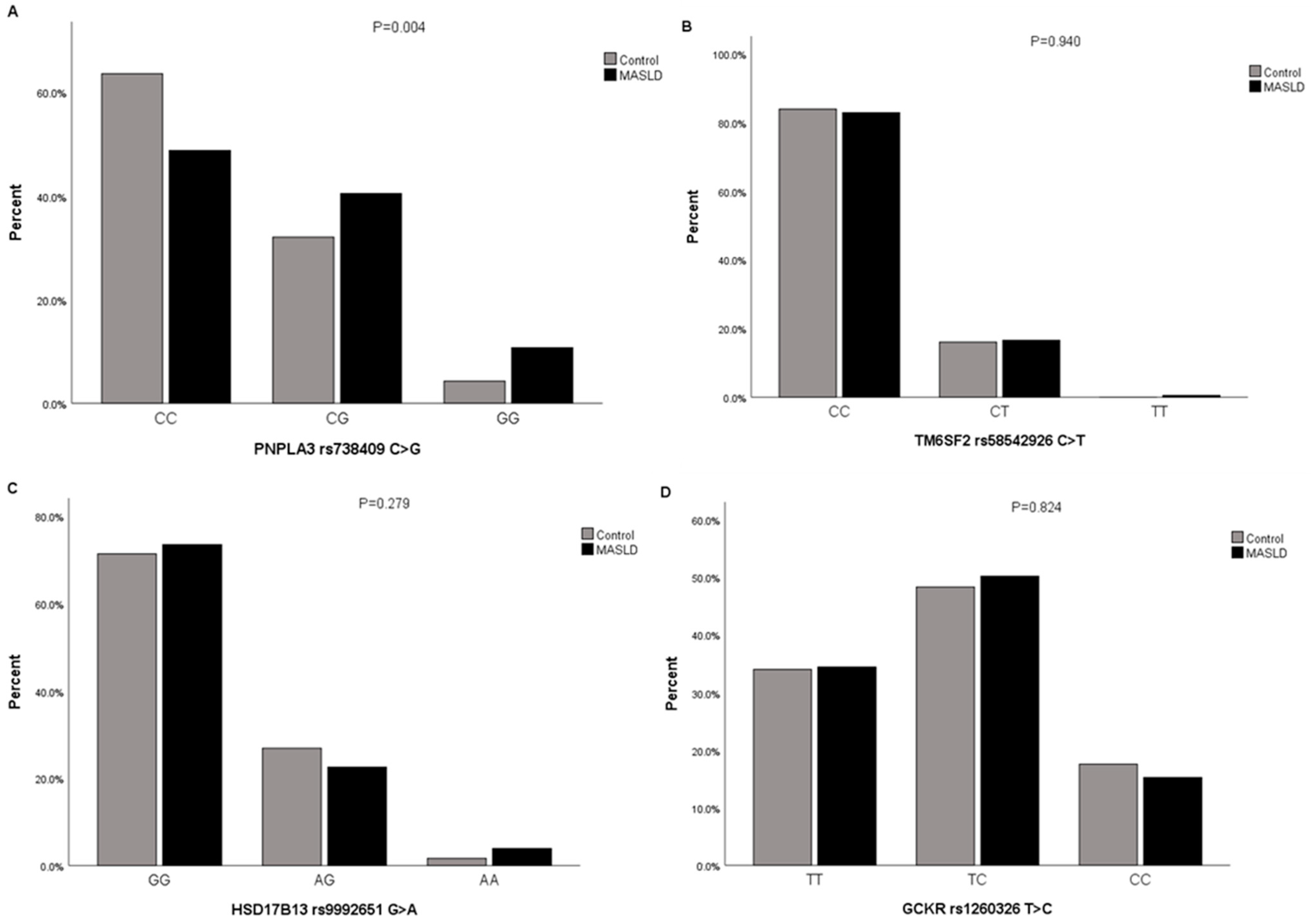
3.3.1. The Proportions of Participants with Genotypes and Alleles of PNPLA3 rs738409 C>G, TM6SF2 rs58542926 C>T, HSD17B13 rs9992651 G>A, and GCKR rs1260326 T>C in MASLD Cases and Controls
3.3.2. Association of Genotypes of PNPLA3 rs738409 C>G, TM6SF2 rs58542926 C>T, HSD17B13 rs9992651 G>A, and GCKR rs1260326 T>C with MASLD by Logistic Regression Analysis
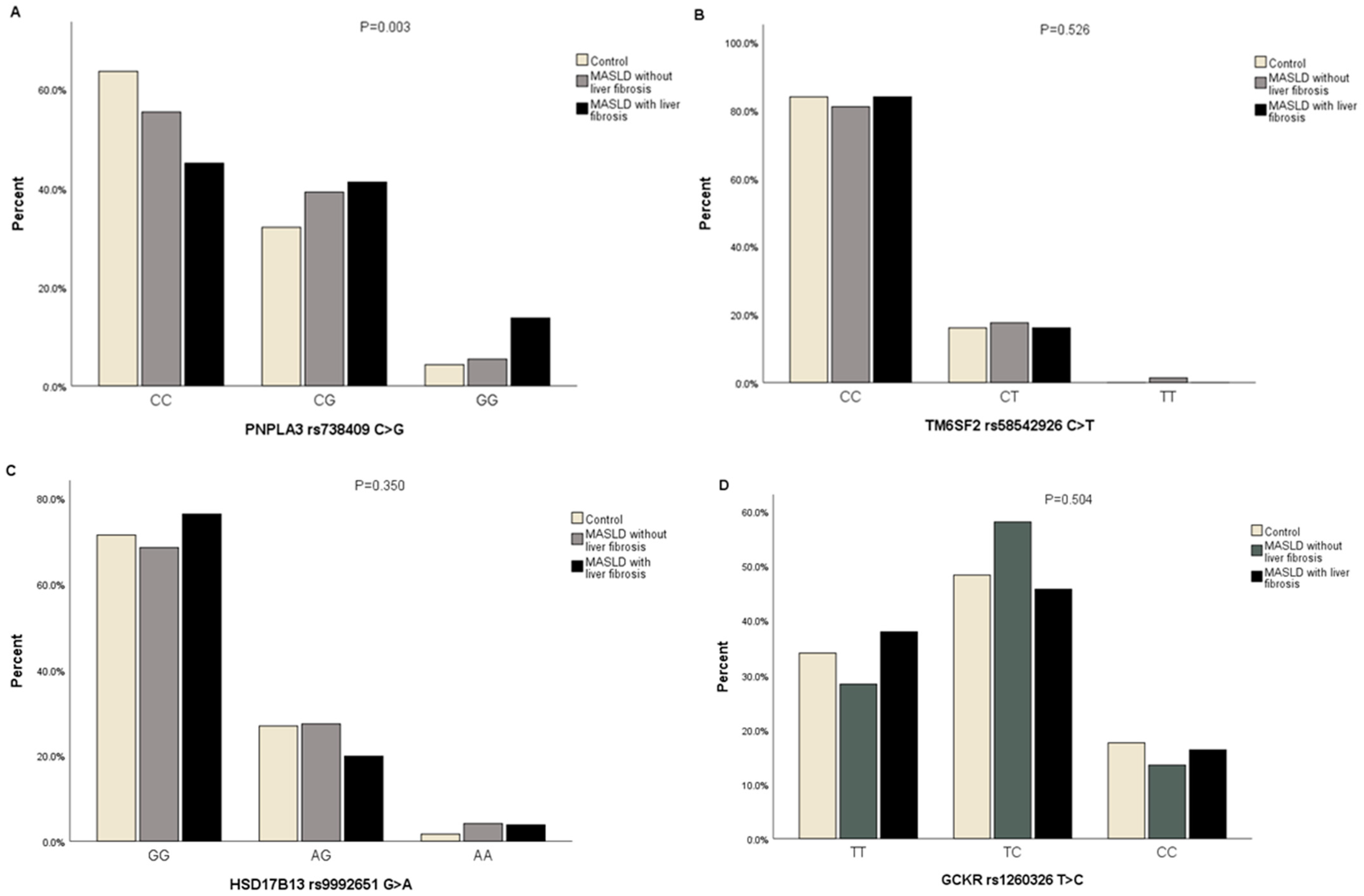
3.3.3. The Proportions of Participants with Genotypes of PNPLA3 rs738409 C>G, TM6SF2 rs58542926 C>T, HSD17B13 rs9992651 G>A, and GCKR rs1260326 T>C in MASLD Cases with Liver Fibrosis, MASLD Cases without Liver Fibrosis, and Controls
3.3.4. Association of Genotypes of PNPLA3 rs738409 C>G, TM6SF2 rs58542926 C>T, HSD17B13 rs9992651 G>A, and GCKR rs1260326 T>C with MASLD with Liver Fibrosis and MASLD without Liver Fibrosis
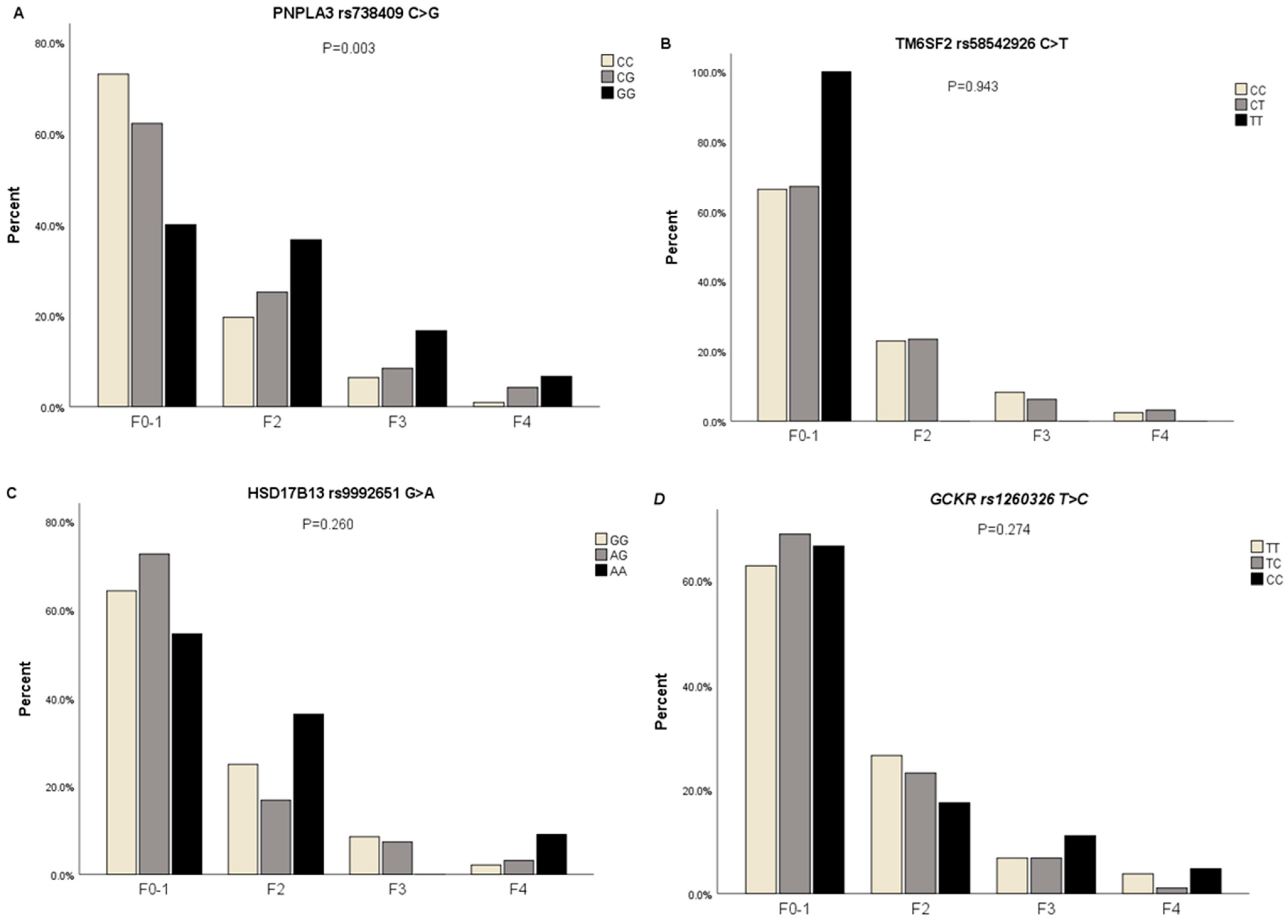
3.3.5. The Proportions of Participants with Genotypes of PNPLA3 rs738409 C>G, TM6SF2 rs58542926 C>T, HSD17B13 rs9992651 G>A, and GCKR rs1260326 T>C in Subjects with Different Severities of Liver Fibrosis
3.3.6. Association of Genotypes of PNPLA3 rs738409 C>G, TM6SF2 rs58542926 C>T, HSD17B13 rs9992651 G>A, and GCKR rs1260326 T>C with Different Severities of Liver Fibrosis in MASLD by Logistic Regression Analysis
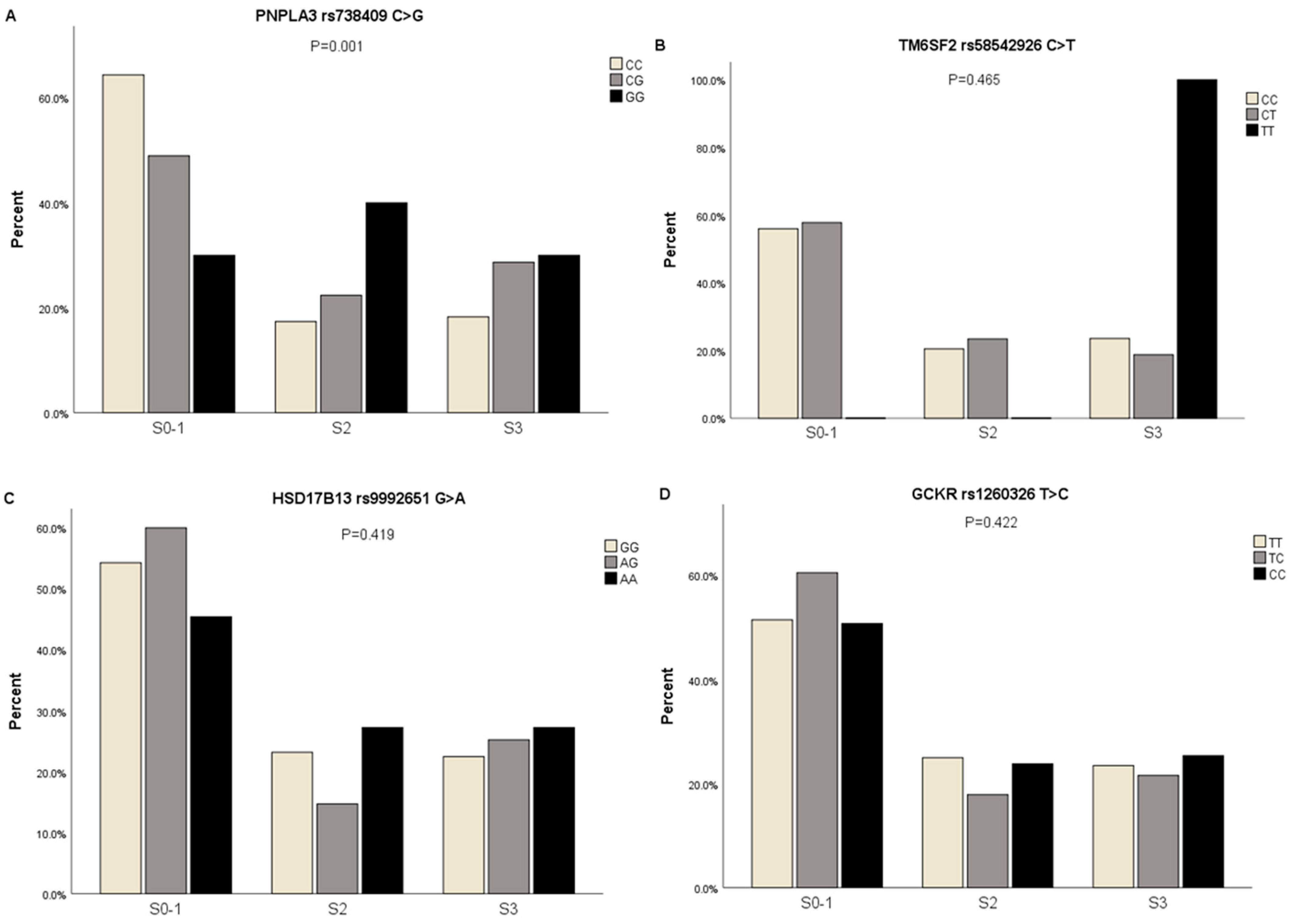
3.3.7. The Proportions of Participants with Genotypes of PNPLA3 rs738409 C>G, TM6SF2 rs58542926 C>T, HSD17B13 rs9992651 G>A, and GCKR rs1260326 T>C in Subjects with Different Severities of Hepatic Steatosis
3.3.8. Association of Genotypes of PNPLA3 rs738409 C>G, TM6SF2 rs58542926 C>T, HSD17B13 rs9992651 G>A, and GCKR rs1260326 T>C with Different Severities of Hepatic Steatosis in MASLD by Logistic Regression Analysis
3.3.9. Clinical Characteristics of PNPLA3 rs738409 G, TM6SF2 rs58542926 T, HSD17B13 rs9992651 A, and GCKR rs1260326 C Carriers and Non-Carriers in the Study Population
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rinella, M.E.; Lazarus, J.V.; Ratziu, V.; Francque, S.M.; Sanyal, A.J.; Kanwal, F.; Romero, D.; Abdelmalek, M.F.; Anstee, Q.M.; Arab, J.P.; et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. Hepatology 2023, 78, 1966–1986. [Google Scholar] [CrossRef] [PubMed]
- Wong, R.J.; Aguilar, M.; Cheung, R.; Perumpail, R.B.; Harrison, S.A.; Younossi, Z.M.; Ahmed, A. Nonalcoholic steatohepatitis is the second leading etiology of liver disease among adults awaiting liver transplantation in the United States. Gastroenterology 2015, 148, 547–555. [Google Scholar] [CrossRef]
- Bertolotti, M.; Lonardo, A.; Mussi, C.; Baldelli, E.; Pellegrini, E.; Ballestri, S.; Romagnoli, D.; Loria, P. Nonalcoholic fatty liver disease and aging: Epidemiology to management. World J. Gastroenterol. 2014, 20, 14185–14204. [Google Scholar] [CrossRef]
- Tomah, S.; Mohamed Eid, E.S.; Abouelmagd, M.M.S.; Hassan, A.H.; Eldib, A.H.; Hamdy, O. 214-LB: Vibration-Controlled Transient Elastography Reveals Alarming Prevalence of Nonalcoholic Fatty Liver Disease and Fibrosis among Young Adults in Egypt. Diabetes 2019, 68 (Suppl. S1), 214-LB. [Google Scholar] [CrossRef]
- Fouad, Y.; Esmat, G.; Elwakil, R.; Zakaria, S.; Yosry, A.; Waked, I.; El-Razky, M.; Doss, W.; El-Serafy, M.; Mostafa, E.; et al. The egyptian clinical practice guidelines for the diagnosis and management of metabolic associated fatty liver disease. Saudi J. Gastroenterol. 2022, 28, 3–20. [Google Scholar] [CrossRef] [PubMed]
- Sookoian, S.; Pirola, C.J. Genetic predisposition in nonalcoholic fatty liver disease. Clin. Mol. Hepatol. 2017, 23, 1–12. [Google Scholar] [CrossRef]
- Romeo, S.; Kozlitina, J.; Xing, C.; Pertsemlidis, A.; Cox, D.; Pennacchio, L.A.; Boerwinkle, E.; Cohen, J.C.; Hobbs, H.H. Genetic variation in PNPLA3 confers susceptibility to nonalcoholic fatty liver disease. Nat. Genet. 2008, 40, 1461–1465. [Google Scholar] [CrossRef]
- Hotta, K.; Yoneda, M.; Hyogo, H.; Ochi, H.; Mizusawa, S.; Ueno, T.; Chayama, K.; Nakajima, A.; Nakao, K.; Sekine, A. Association of the rs738409 polymorphism in PNPLA3 with liver damage and the development of nonalcoholic fatty liver disease. BMC Med. Genet. 2010, 11, 172. [Google Scholar] [CrossRef] [PubMed]
- Jain, V.; Kumar, A.; Ahmad, N.; Jana, M.; Kalaivani, M.; Kumar, B.; Shastri, S.; Jain, O.; Kabra, M. Genetic polymorphisms associated with obesity and non-alcoholic fatty liver disease in Asian Indian adolescents. J. Pediatr. Endocrinol. Metab. 2019, 32, 749–758. [Google Scholar] [CrossRef]
- Krawczyk, M.; Rau, M.; Schattenberg, J.M.; Bantel, H.; Pathil, A.; Demir, M.; Kluwe, J.; Boettler, T.; Lammert, F.; Geier, A. Combined effects of the PNPLA3 rs738409, TM6SF2 rs58542926, and MBOAT7 rs641738 variants on NAFLD severity: A multicenter biopsy-based study. J. Lipid Res. 2017, 58, 247–255. [Google Scholar] [CrossRef]
- Sookoian, S.; Pirola, C.J. Meta-analysis of the influence of I148M variant of patatin-like phospholipase domain containing 3 gene (PNPLA3) on the susceptibility and histological severity of nonalcoholic fatty liver disease. Hepatology 2011, 53, 1883–1894. [Google Scholar] [CrossRef] [PubMed]
- Unalp-Arida, A.; Ruhl, C.E. Patatin-Like Phospholipase Domain-Containing Protein 3 I148M and Liver Fat and Fibrosis Scores Predict Liver Disease Mortality in the U.S. Population. Hepatology 2020, 71, 820–834. [Google Scholar] [CrossRef] [PubMed]
- Zain, S.M.; Mohamed, R.; Mahadeva, S.; Cheah, P.L.; Rampal, S.; Basu, R.C.; Mohamed, Z. A multi-ethnic study of a PNPLA3 gene variant and its association with disease severity in non-alcoholic fatty liver disease. Hum. Genet. 2012, 131, 1145–1152. [Google Scholar] [CrossRef] [PubMed]
- Benedict, M.; Zhang, X. Non-alcoholic fatty liver disease: An expanded review. World J. Hepatol. 2017, 9, 715–732. [Google Scholar] [CrossRef] [PubMed]
- Martínez, L.A.; Larrieta, E.; Kershenobich, D.; Torre, A. The Expression of PNPLA3 Polymorphism could be the Key for Severe Liver Disease in NAFLD in Hispanic Population. Ann. Hepatol. 2017, 16, 909–915. [Google Scholar] [CrossRef] [PubMed]
- Rotman, Y.; Koh, C.; Zmuda, J.M.; Kleiner, D.E.; Liang, T.J. The association of genetic variability in patatin-like phospholipase domain-containing protein 3 (PNPLA3) with histological severity of nonalcoholic fatty liver disease. Hepatology 2010, 52, 894–903. [Google Scholar] [CrossRef]
- Valenti, L.; Alisi, A.; Galmozzi, E.; Bartuli, A.; Del Menico, B.; Alterio, A.; Dongiovanni, P.; Fargion, S.; Nobili, V. I148M patatin-like phospholipase domain-containing 3 gene variant and severity of pediatric nonalcoholic fatty liver disease. Hepatology 2010, 52, 1274–1280. [Google Scholar] [CrossRef] [PubMed]
- Anstee, Q.M.; Darlay, R.; Cockell, S.; Meroni, M.; Govaere, O.; Tiniakos, D.; Burt, A.D.; Bedossa, P.; Palmer, J.; Liu, Y.-L.; et al. Genome-wide association study of non-alcoholic fatty liver and steatohepatitis in a histologically characterised cohort☆. J. Hepatol. 2020, 73, 505–515. [Google Scholar] [CrossRef]
- Mazo, D.F.; Malta, F.M.; Stefano, J.T.; Salles, A.P.M.; Gomes-Gouvea, M.S.; Nastri, A.C.S.; Almeida, J.R.; Pinho, J.R.R.; Carrilho, F.J.; Oliveira, C.P. Validation of PNPLA3 polymorphisms as risk factor for NAFLD and liver fibrosis in an admixed population. Ann. Hepatol. 2019, 18, 466–471. [Google Scholar] [CrossRef]
- Musso, G.; Cipolla, U.; Cassader, M.; Pinach, S.; Saba, F.; De Michieli, F.; Paschetta, E.; Bongiovanni, D.; Framarin, L.; Leone, N.; et al. TM6SF2 rs58542926 variant affects postprandial lipoprotein metabolism and glucose homeostasis in NAFLD. J. Lipid Res. 2017, 58, 1221–1229. [Google Scholar] [CrossRef]
- Motomura, T.; Amirneni, S.; Diaz-Aragon, R.; Faccioli, L.A.P.; Malizio, M.R.; Coard, M.C.; Kocas-Kilicarslan, Z.N.; Frau, C.; Haep, N.; Ostrowska, A.; et al. Is HSD17B13 Genetic Variant a Protector for Liver Dysfunction? Future Perspective as a Potential Therapeutic Target. J. Pers. Med. 2021, 11, 619. [Google Scholar] [CrossRef] [PubMed]
- Tong, M.; Wang, F. APOC3rs2854116, PNPLA3rs738409, and TM6SF2rs58542926 polymorphisms might influence predisposition of NAFLD: A meta-analysis. IUBMB Life 2020, 72, 1757–1764. [Google Scholar] [CrossRef]
- Mu, T.; Peng, L.; Xie, X.; He, H.; Shao, Q.; Wang, X.; Zhang, Y. Single Nucleotide Polymorphism of Genes Associated with Metabolic Fatty Liver Disease. J. Oncol. 2022, 2022, 9282557. [Google Scholar] [CrossRef]
- Li, J.; Zhao, Y.; Zhang, H.; Hua, W.; Jiao, W.; Du, X.; Rui, J.; Li, S.; Teng, H.; Shi, B.; et al. Contribution of Rs780094 and Rs1260326 Polymorphisms in GCKR Gene to Non-alcoholic Fatty Liver Disease: A Meta-Analysis Involving 26,552 Participants. Endocr. Metab. Immune Disord. Drug Targets 2021, 21, 1696–1708. [Google Scholar] [CrossRef] [PubMed]
- Riazi, K.; Swain, M.G.; Congly, S.E.; Kaplan, G.G.; Shaheen, A.A. Race and Ethnicity in Non-Alcoholic Fatty Liver Disease (NAFLD): A Narrative Review. Nutrients 2022, 14, 4556. [Google Scholar] [CrossRef]
- Cavalcante, L.N.; Porto, J.; Mazo, D.; Longatto-Filho, A.; Stefano, J.T.; Lyra, A.C.; Carrilho, F.J.; Reis, R.M.; Alves, V.A.F.; Sanyal, A.J.; et al. African genetic ancestry is associated with lower frequency of PNPLA3 G allele in non-alcoholic fatty liver in an admixed population. Ann. Hepatol. 2017, 16, 100728. [Google Scholar] [CrossRef]
- Szklarczyk, D.; Kirsch, R.; Koutrouli, M.; Nastou, K.; Mehryary, F.; Hachilif, R.; Gable, A.L.; Fang, T.; Doncheva, N.T.; Pyysalo, S.; et al. The STRING database in 2023: Protein-protein association networks and functional enrichment analyses for any sequenced genome of interest. Nucleic Acids Res. 2023, 51, D638–D646. [Google Scholar] [CrossRef]
- Ng, P.C.; Henikoff, S. Predicting deleterious amino acid substitutions. Genome Res. 2001, 11, 863–874. [Google Scholar] [CrossRef] [PubMed]
- Peka, M.; Balatsky, V.; Saienko, A.; Tsereniuk, O. Bioinformatic analysis of the effect of SNPs in the pig TERT gene on the structural and functional characteristics of the enzyme to develop new genetic markers of productivity traits. BMC Genom. 2023, 24, 487. [Google Scholar] [CrossRef]
- Waterhouse, A.; Bertoni, M.; Bienert, S.; Studer, G.; Tauriello, G.; Gumienny, R.; Heer, F.T.; de Beer, T.A.P.; Rempfer, C.; Bordoli, L.; et al. SWISS-MODEL: Homology modelling of protein structures and complexes. Nucleic Acids Res. 2018, 46, W296–W303. [Google Scholar] [CrossRef]
- Stecher, G.; Tamura, K.; Kumar, S. Molecular Evolutionary Genetics Analysis (MEGA) for macOS. Mol. Biol. Evol. 2020, 37, 1237–1239. [Google Scholar] [CrossRef] [PubMed]
- Lopez, J. Carl A. Burtis, Edward R. Ashwood and David E. Bruns (eds): Tietz Textbook of Clinical Chemistry and Molecular Diagnosis (5th edition): Elsevier, St. Louis, USA, 2012, 2238 pp, 909 illustrations. ISBN: 978-1-4160-6164-9. Indian J. Clin. Biochem. 2013, 28, 104–105. [CrossRef]
- Wilder, J.; Patel, K. The clinical utility of FibroScan® as a noninvasive diagnostic test for liver disease. Med. Devices Evid. Res. 2014, 7, 107–114. [Google Scholar] [CrossRef]
- Lee, J.E.; Ko, K.O.; Lim, J.W.; Cheon, E.J.; Song, Y.H.; Yoon, J.M. Correlation between Transient Elastography (Fibroscan®) and Ultrasonographic and Computed Tomographic Grading in Pediatric Nonalcoholic Steatohepatitis. Pediatr. Gastroenterol. Hepatol. Nutr. 2022, 25, 240–250. [Google Scholar] [CrossRef] [PubMed]
- Santos, F.A.B.; Lemes, R.B.; Otto, P.A. HW_TEST, a program for comprehensive HARDY-WEINBERG equilibrium testing. Genet. Mol. Biol. 2020, 43, e20190380. [Google Scholar] [CrossRef] [PubMed]
- Fairfield, C.J.; Drake, T.M.; Pius, R.; Bretherick, A.D.; Campbell, A.; Clark, D.W.; Fallowfield, J.A.; Hayward, C.; Henderson, N.C.; Joshi, P.K.; et al. Genome-Wide Association Study of NAFLD Using Electronic Health Records. Hepatol. Commun. 2022, 6, 297–308. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Cohen, J.C.; Hobbs, H.H. Expression and characterization of a PNPLA3 protein isoform (I148M) associated with nonalcoholic fatty liver disease. J. Biol. Chem. 2011, 286, 37085–37093. [Google Scholar] [CrossRef]
- Abul-Husn, N.S.; Cheng, X.; Li, A.H.; Xin, Y.; Schurmann, C.; Stevis, P.; Liu, Y.; Kozlitina, J.; Stender, S.; Wood, G.C.; et al. A Protein-Truncating HSD17B13 Variant and Protection from Chronic Liver Disease. N. Engl. J. Med. 2018, 378, 1096–1106. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Phenotype | MASLD Cases (n = 205) | Controls (n = 187) | p-Value |
|---|---|---|---|
| Gender (male/female) | 126/79 | 72/115 | <0.001 *** |
| Diabetes (Diabetic/Prediabetic/Normal) | 78/14/113 | 0/0/187 | <0.001 *** |
| Hypertension (Hypertensive/Normal) | 125/80 | 0/187 | <0.001 *** |
| Age (years) | 45.16 ± 11.25 | 38.37 ± 11.30 | <0.001 *** |
| Hepatic Steatosis degree (S0/S1/S2/S3) | 0/33/82/90 | 187/0/0/0 | <0.001 *** |
| Liver Fibrosis degree (F0–1/F2/F3/F4) | 74/90/31/10 | 187/0/0/0 | <0.001 *** |
| BMI (kg/m2) | 32.78 ± 5.82 | 22.95 ± 2.62 | <0.001 *** |
| WC (cm) | 112.52 ± 12.19 | 90.36 ± 4.10 | <0.001 *** |
| SBP (mmHg) | 119.98 ± 18.25 | 116.18 ± 10.08 | 0.011 * |
| DBP (mmHg) | 83.86 ± 13.51 | 77.36 ± 5.98 | <0.001 *** |
| ALT (U/L) | 36.01 ± 27.39 | 15.16 ± 7.07 | <0.001 *** |
| AST (U/L) | 31.61 ± 20.25 | 20.48 ± 6.57 | <0.001 *** |
| GGT (U/L) | 41.89 ± 36.44 | 18.28 ± 7.55 | <0.001 *** |
| FBG (mg/dL) | 106.29 ± 34.65 | 86.51 ± 11.450 | <0.001 *** |
| PPBS (mg/dL) | 122.66 ± 37.01 | 104.60 ± 14.60 | <0.001 *** |
| TC (mg/dL) | 197.4 ± 45.62 | 169.27 ± 36.02 | <0.001 *** |
| TG (mg/dL) | 154.76 ± 79.15 | 91.67 ± 37.43 | <0.001 *** |
| LDL-C (mg/dL) | 128.75 ± 41.57 | 114.08 ± 28.73 | <0.001 *** |
| HDL-C (mg/dL) | 37.20 ± 11.19 | 39.51 ± 11.44 | <0.001 *** |
| MASLD Cases (n = 205) | Controls (Ref.) (n = 187) | Unadjusted Model | Adjusted Model for Age, Sex, BMI, WC, HDL, TG, Diabetes Mellitus, and Hypertension | |||
|---|---|---|---|---|---|---|
| No. | No. | p-Value 1 | OR (95%CI) | p-Value 2 | OR (95%CI) | |
| PNPLA3 rs738409 C>G | ||||||
| Genotype | ||||||
| CC (Ref.) | 100 | 119 | 1.000 | 1.000 | ||
| CG | 83 | 60 | 0.022 * | 1.646 (1.076–2.519) | 0.941 | 1.043 (0.337–3.235) |
| GG | 22 | 8 | 0.006 ** | 3.272 (1.396–7.670) | 0.039 * | 9.166 (1.123–74.832) |
| TM6SF2 rs58542926 C>T | ||||||
| Genotype | ||||||
| CC (Ref.) | 170 | 157 | 1.000 | 1.000 | ||
| CT | 34 | 30 | 0.8677 | 1.047 (0.612–1.790) | 0.952 | 1.041 (0.282–3.844) |
| TT | 1 | 0 | 1.000 | - | 1.000 | - |
| HSD17B13 rs9992651 G>A | ||||||
| Genotype | ||||||
| GG (Ref.) | 150 | 130 | 1.000 | 1.000 | ||
| GA | 46 | 49 | 0.386 | 0.814 (0.511–1.296) | 0.597 | 1.409 (0.395–5.025) |
| AA | 8 | 3 | 0.223 | 2.311 (0.601–8.893) | 0.511 | 2.726 (0.137–54.280) |
| GCKR rs1260326 T>C | ||||||
| Genotype | ||||||
| TT (Ref.) | 70 | 62 | 1.000 | 1.000 | ||
| TC | 102 | 88 | 0.908 | 1.027 (0.658–1.602) | 0.657 | 0.745 (0.203–2.731) |
| CC | 31 | 32 | 0.617 | 0.858 (0.471–1.564) | 0.556 | 1.796 (0.256–12.612) |
| Control (Ref.) (n = 187) versus MASLD Cases with Liver Fibrosis (n = 131) | Control (Ref.) (n = 187) versus MASLD Cases without Liver Fibrosis (n = 74) | |||
|---|---|---|---|---|
| p-Value 1 | OR (95%CI) | p-Value 2 | OR (95%CI) | |
| PNPLA3 rs738409 C>G | ||||
| Genotype | ||||
| CC (Ref.) (n = 219) | 1.000 | 1.000 | ||
| CG (n = 143) | 0.015 * | 1.815 (1.121–2.940) | 0.243 | 1.403 (0.795–2.475) |
| GG (n = 30) | 0.001 ** | 4.538 (1.865–11.044) | 0.560 | 1.451 (0.415–5.073) |
| TM6SF2 rs58542926 C>T | ||||
| Genotype | ||||
| CC (Ref.) (n = 327) | 1.000 | 1.000 | ||
| CT (n = 64) | 0.998 | 0.999 (0.544–1.836) | 0.731 | 1.134 (0.554–2.319) |
| TT (n = 1) | - | - | - | - |
| HSD17B13 rs9992651 G>A | ||||
| Genotype | ||||
| GG (Ref.) (n = 280) | 1.000 | 1.000 | ||
| GA (n = 95) | 0.180 | 0.690 (0.401–1.186) | 0.850 | 1.061 (0.574–1.961) |
| AA (n = 11) | 0.298 | 2.167 (0.506–9.282) | 0.252 | 2.600 (0.508–13.313) |
| GCKR rs1260326 T>C | ||||
| Genotype | ||||
| TT (Ref.) (n = 132) | 1.000 | 1.000 | ||
| TC (n = 190) | 0.518 | 0.848 (0.515–1.397) | 0.243 | 1.443 (0.780–2.668) |
| CC (n = 63) | 0.584 | 0.830 (0.427–1.616) | 0.855 | 0.923 (0.388–2.192) |
| F0–1 (Ref.) (n = 261) VS F2 (n = 90) | F0–1 (Ref.) (n = 261) VS F3 (n = 31) | F0–1 (Ref.) (n = 261) VS F4 (n = 10) | ||||
|---|---|---|---|---|---|---|
| p-Value 1 | OR (95%CI) | p-Value 2 | OR (95%CI) | p-Value 3 | OR (95%CI) | |
| PNPLA3 rs738409 C>G | ||||||
| Genotype | ||||||
| CC (Ref.) (n = 219) | 1.000 | 1.000 | 1.000 | |||
| CG (n = 143) | 0.118 | 1.505 (0.901–2.514) | 0.297 | 1.241 (0.827–1.864) | 0.042 * | 5.393 (1.066–27.284) |
| GG (n = 30) | 0.007 ** | 3.411 (1.408–8.262) | 0.009 ** | 4.762 (1.467–15.460) | 0.013 * | 13.333 (1.724–103.145) |
| TM6SF2 rs58542926 C>T | ||||||
| Genotype | ||||||
| CC (Ref.) (n = 327) | 1.000 | 1.000 | 1.000 | |||
| CT (n = 64) | 0.978 | 1.009 (0.530–1.921) | 0.604 | 0.748 (0.249–2.246) | 0.774 | 1.262 (0.259–6.148) |
| TT (n = 1) | - | - | - | - | - | - |
| HSD17B13 rs9992651 G>A | ||||||
| Genotype | ||||||
| GG (Ref.) (n = 280) | 1.000 | 1.000 | 1.000 | |||
| GA (n = 95) | 0.097 | 0.596 (0.324–1.097) | 0.546 | 0.761 (0.314–1.846) | 0.713 | 1.304 (0.317–5.361) |
| AA (n = 11) | 0.415 | 1.714 (0.470–6.258) | 0.999 | - | 0.164 | 5.000 (0.518–48.295) |
| GCKR rs1260326 T>C | ||||||
| Genotype | ||||||
| TT (Ref.) (n = 132) | 1.000 | 1.000 | 1.000 | |||
| TC (n = 190) | 0.393 | 0.797 (0.473–1.343) | 0.846 | 0.915 (0.375–2.236) | 0.106 | 0.253 (0.048–1.337) |
| CC (n = 63) | 0.227 | 0.621 (0.287–1.345) | 0.425 | 1.537 (0.535–4.415) | 0.821 | 1.186 (0.270–5.202) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elmansoury, N.; Megahed, A.A.; Kamal, A.; El-Nikhely, N.; Labane, M.; Abdelmageed, M.; Daly, A.K.; Wahid, A. Relevance of PNPLA3, TM6SF2, HSD17B13, and GCKR Variants to MASLD Severity in an Egyptian Population. Genes 2024, 15, 455. https://doi.org/10.3390/genes15040455
Elmansoury N, Megahed AA, Kamal A, El-Nikhely N, Labane M, Abdelmageed M, Daly AK, Wahid A. Relevance of PNPLA3, TM6SF2, HSD17B13, and GCKR Variants to MASLD Severity in an Egyptian Population. Genes. 2024; 15(4):455. https://doi.org/10.3390/genes15040455
Chicago/Turabian StyleElmansoury, Nehal, Ahmed A. Megahed, Ahmed Kamal, Nefertiti El-Nikhely, Marina Labane, Manal Abdelmageed, Ann K. Daly, and Ahmed Wahid. 2024. "Relevance of PNPLA3, TM6SF2, HSD17B13, and GCKR Variants to MASLD Severity in an Egyptian Population" Genes 15, no. 4: 455. https://doi.org/10.3390/genes15040455
APA StyleElmansoury, N., Megahed, A. A., Kamal, A., El-Nikhely, N., Labane, M., Abdelmageed, M., Daly, A. K., & Wahid, A. (2024). Relevance of PNPLA3, TM6SF2, HSD17B13, and GCKR Variants to MASLD Severity in an Egyptian Population. Genes, 15(4), 455. https://doi.org/10.3390/genes15040455