3. Results
3.1. Demographics of Sample Households
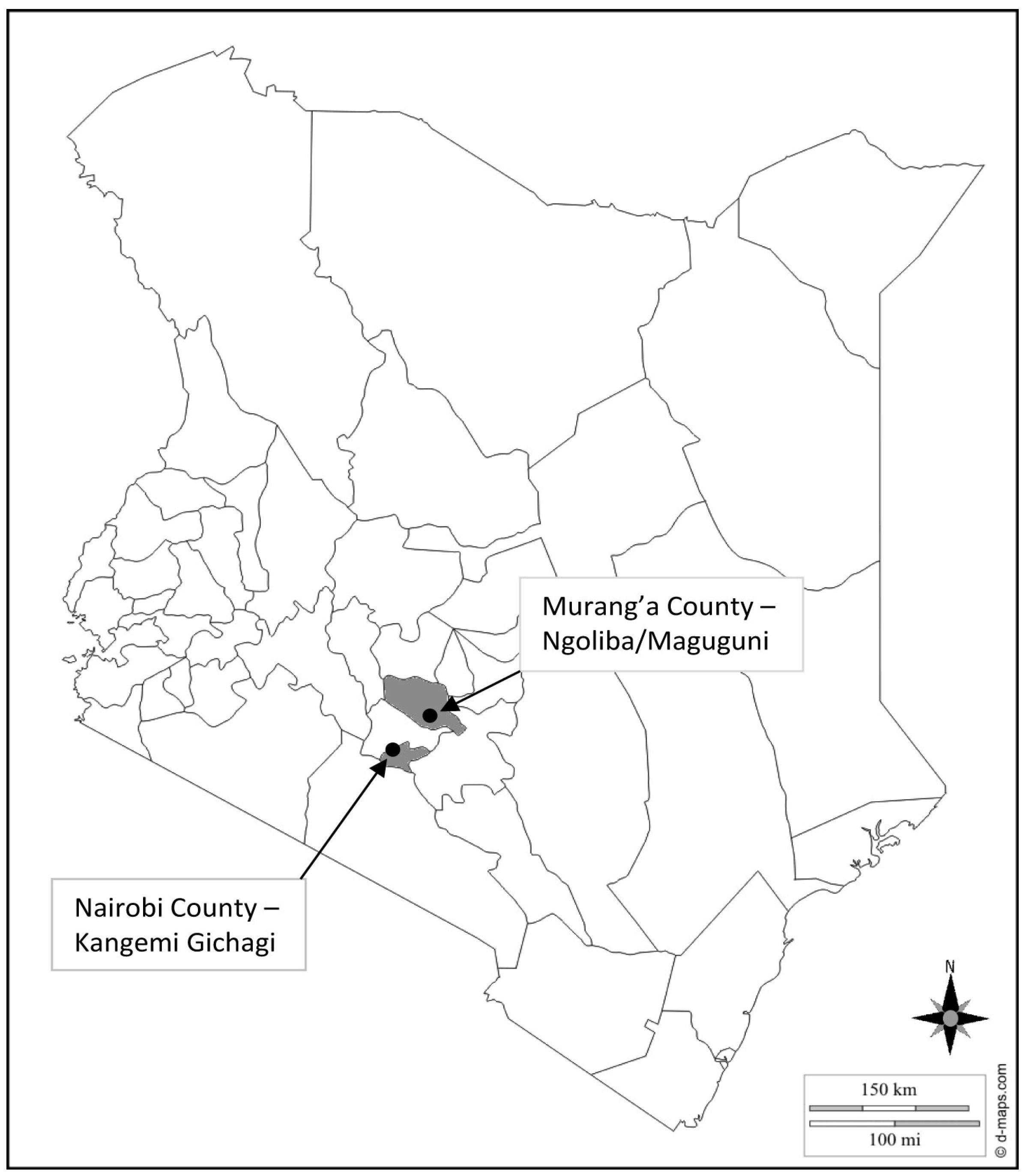
A total of 99 respondents were interviewed (50 in Ngoliba/Maguguni and 49 in Kangemi Gichagi). Of the interviewed respondents, 72% in Ngoliba/Maguguni and 81% in Kangemi Gichagi had acquired basic education, meaning they had completed primary school or had higher education. Female adult household members were said to make most of the decisions regarding domestic water needs, at 70% in Ngoliba/Maguguni and 77% in Kangemi Gichagi. Eighty percent of the interviewed respondents were female. The poverty threshold for Kenya is estimated at KES 1239 (equivalent USD 15) and KES 2648 (equivalent USD 31) for rural and urban areas, respectively [
36]. According to the Central Bank of Kenya, as of 31 October 2013, USD 1 = KES 85.1 [
37]. From the households interviewed, 4% of Ngoliba/Maguguni lived below the poverty line set for rural areas, while 64% lived below the poverty line set for urban areas in Kangemi Gichagi. The average household size was found to be 3.88 in Ngoliba/Maguguni and 4.08 in Kangemi Gichagi.
3.2. Water-Service Provision of Sample Households
The main sources of domestic water for rural Ngoliba/Maguguni and urban Kangemi Gichagi are shown in
Figure 4. As it is indicated, 30% of Ngoliba/Maguguni respondents use spring, well or borehole water, 24% use water from a water kiosks, 20% use a piped connection (single tap located outside the house), 14% water vendors, 10% streams, and 2% rain water harvesting. In Kangemi Gichagi, 44% use piped connection (38% multi-households standpipes and 6% complete private in-house connection), 33% use water kiosks, 15% water vendors, 6% get water from the stream, and 2% use spring, well or borehole water. When asked about their perception regarding the ideal water source imaginable, an average of 99% from both study areas found tap water in premises to be the most ideal solution. Furthermore, an average of 87% of the respondents perceived water-service provision to be a mandate of the State.
Figure 4.
Main source of water in urban Kangemi Gichagi (N = 48), and rural Ngoliba/Maguguni (N = 50).
Figure 4.
Main source of water in urban Kangemi Gichagi (N = 48), and rural Ngoliba/Maguguni (N = 50).
Only 14% of Ngoliba/Maguguni and 2% of Kangemi Gichagi households regularly used one single source for domestic water. Domestic water refers to water used for washing, cooking, cleaning and drinking. In Ngoliba/Maguguni, 52% used two sources and 33% used three different sources of water. In Kangemi Gichagi, 35% of respondents used two sources regularly, 53% used three and 8% used four different sources. Respondents were further asked about the type of their sources for drinking water. In Ngoliba/Maguguni, 20% said they retrieved their drinking water from a source different to that for other domestic activities. In Kangemi Gichagi, 40% had a different source for drinking water. The rest of the respondents used the same water sources for both drinking and other domestic purposes.
The amount of water used by respondents was 24.40 L per capita per day in Ngoliba/Maguguni and 19.22 L per capita per day in Kangemi Gichagi. For drinking purposes, the average was 1.24 L per capita per day in Ngoliba/Maguguni and 0.84 L per capita per day in Kangemi Gichagi.
With regard to spending on domestic water, 56% of Ngoliba/Maguguni and 52% of Kangemi Gichagi respondents were able to give definite amounts, which are shown in
Figure 5. The reasons stated for not being able to specify the cost of the spending on water was that the respondents got their water from surface and groundwater sources, for which they did not have to pay. The second group comprised those people whose water costs were combined with the house rental bills, and where the amount of money that went to water costs was not specified to them (mostly households with standpipe water sources). In Ngoliba/Maguguni, 7% of respondents paid KES 3, while 61% paid KES 5, 3% paid KES 10, 25% paid KES 15, and lastly 3% paid KES 30. In Kangemi Gichagi, 60% paid KES 3 while 40% paid KES 5. These are the costs for 20 L containers, which is the standard container widely used for purchase and storage of domestic water.
Figure 5.
Household expenditure on water per 20 L container: Kangemi Gichagi (urban) (N = 25), and Ngoliba/Maguguni (rural) (N = 28) (KES 1 = USD 0.0118).
Figure 5.
Household expenditure on water per 20 L container: Kangemi Gichagi (urban) (N = 25), and Ngoliba/Maguguni (rural) (N = 28) (KES 1 = USD 0.0118).
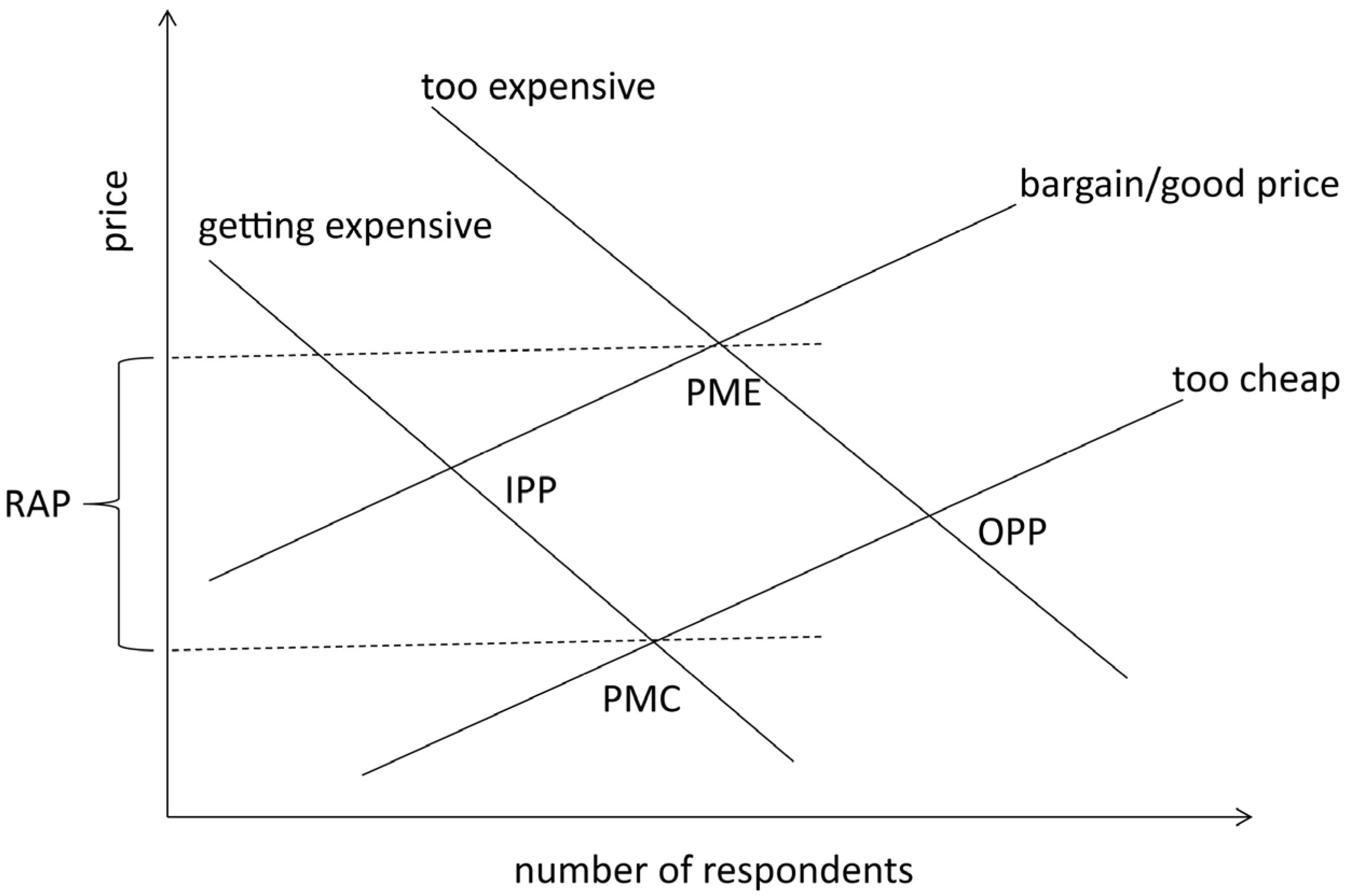
Van Westendorp’s price-sensitivity meter was applied to determine people’s willingness to pay for water. The range of acceptable prices for water was found to lie between KES 5 and KES 10 for a 20 L container. The range between KES 2 and KES 5 was seen to be a good bargain price by 94% of respondents (
Figure 6). For this enquiry, respondents were asked about their willingness to pay for safe water from sources that are convenient to access.
Figure 6.
Range of Acceptable Price (RAP) for safe water per 20 L container in Kangemi Gichagi and Ngoliba/Maguguni, N = 96. PME = point of marginal expensiveness, PMC = point of marginal cheapness (KES 1 = USD 0.0118).
Figure 6.
Range of Acceptable Price (RAP) for safe water per 20 L container in Kangemi Gichagi and Ngoliba/Maguguni, N = 96. PME = point of marginal expensiveness, PMC = point of marginal cheapness (KES 1 = USD 0.0118).
3.3. Safe Water Options and Interventions of Sample Households
Of the interviewed respondents, 16% Ngoliba/Maguguni and 27% Kangemi Gichagi said that they perceived their main source of water as safe to drink. Sixty percent in Ngoliba/Maguguni and 56% in Kangemi Gichagi perceived it to be relatively safe, while 24% of Ngoliba/Maguguni and 17% Kangemi Gichagi respondents said that they perceived it to be unsafe to drink.
Sixty-nine percent of Kangemi Gichagi and 66% of Ngoliba/Maguguni respondents said that they treat their drinking water. Out of these respondents, 42% used boiling as a treatment method, 48% use chlorination and 10% filtration in Ngoliba/Maguguni. In Kangemi Gichagi, 67% used boiling and 33% chlorination to treat their water. In order to investigate consistency in water treatment, respondents were asked to show if they had treated water available on the day of the interview. Only 17% of Kangemi Gichagi and 31% of Ngoliba/Maguguni respondents had treated water available. Reasons given by respondents who did not treat their water even though they had the perception that the water was unsafe or only relatively safe for drinking, were given as follows: cumbersome/difficult procedures (45% in Ngoliba/Maguguni and 36% in Kangemi Gichagi), lack of time (12% in Ngoliba/Maguguni and 20% in Kangemi Gichagi), and too costly (18% in Ngoliba/Maguguni and 32% in Kangemi Gichagi).
Investigations were made to find out if drinking water was kept safe during storage. Eighty-two percent of Ngoliba/Maguguni and 66% of Kangemi Gichagi respondents had their water storage facilities safely capped with a lid. 62% in Ngoliba/Maguguni and 60% in Kangemi Gichagi said they had a separate storage facility for drinking water from storage facility for water for other domestic uses. Eighty-eight percent of respondents in both Kangemi Gichagi and Ngoliba/Maguguni said they cleaned their water storage facilities after every refill or within a timeframe of one week.
3.4. Link between Safe Drinking Water, Health and Hygiene
Two questions were asked to the household respondents to find out if they had a basic understanding of the link between safe drinking water and health—in particular, diarrhea. Ninety percent of the respondents in Ngoliba/Maguguni and 94% in Kangemi Gichagi said that they perceived diarrhea as a serious condition that can be life threatening. When asked about the causes of diarrhea, among other causes, consumption of contaminated water was mentioned by 90% of Ngoliba/Maguguni respondents and 96% of Kangemi Gichagi respondents. Additionally, on the preventive measures of diarrheal diseases, hand washing was mentioned by 100% of the respondents in both study areas. To check the probability that hand washing is practiced within the households, the respondents were asked if the household has a permanent hand washing facility. Only 16% of Ngoliba/Maguguni and 8% of Kangemi Gichagi respondents had a permanent hand-washing station. Observation further confirmed that 33% in Ngoliba/Maguguni and 50% in Kangemi Gichagi of those that had permanent hand-washing stations, were not functional (did not have water) on the day of the interview. Further inquiries were made for the respondents who were without or with non-functioning hand-washing stations, in order to find out why they did not have hand-washing facilities. Sixty-nine percent of Ngoliba/Maguguni and 73% of Kangemi Gichagi said that it was hard to maintain a hand-washing station, 19% of Ngoliba/Maguguni and 25% of Kangemi Gichagi respondents said that lack of water was the problem, while 12% of Ngoliba/Maguguni and 2% of Kangemi Gichagi respondents said that they never gave it a thought or a priority.
3.5. Perceptions toward the Safe Water Enterprises
In both study areas, 96% of the respondents were aware of the SWE presence. Eighty-nine percent of rural Ngoliba/Maguguni and 91% of urban Kangemi Gichagi respondents, who knew about the SWE, were also aware that the kiosk provides water that is of acceptable quality standards for drinking. While a majority of the respondents were aware of the water quality, only 24% of Ngoliba/Maguguni and 29% of Kangemi Gichagi respondents were aware of the technology applied to treat the water at the kiosk. Seventy-one percent of Ngoliba/Maguguni and 63% of Kangemi Gichagi respondents said that whenever possible they bought water from the SWE.
With regards to the aesthetic quality, all 100% of respondents from both study areas perceived the SWE water to have aesthetic water qualities that are acceptable to them. The main reason for purchasing water from the SWE was because respondents perceive this kiosk’s water to be of a superior quality, and safe, as compared to all other available sources (82% in rural Ngoliba/Maguguni and 85% in urban Kangemi Gichagi). Sixteen percent of Ngoliba/Maguguni and 12% of Kangemi Gichagi respondents said that proximity to their homes was the main motivation for purchasing water from the SWE kiosk.
Of the respondents who were aware of the SWE but did not purchase their water there, 92% in Ngoliba/Maguguni and 84% in Kangemi Gichagi gave distance from their homes as their main reason. Reliability was also given as a reason for not purchasing SWE water at 8% in Ngoliba/Maguguni and 16% in Kangemi Gichagi. On waiting time, 64% of Ngoliba/Maguguni respondents were satisfied with the waiting time to get services at the SWE. For Kangemi Gichagi, 42% were satisfied with the waiting time. Regarding ease of accessibility, 61% of Ngoliba/Maguguni and 70% of Kangemi Gichagi said they thought the location of the SWE kiosk was suitable. As regards availability of water at the SWE kiosk, only 17% of Ngoliba/Maguguni and 40% of Kangemi Gichagi respondents said that they found the SWE kiosk reliable.
For safe drinking water, the price at the SWE Kiosk is at KES 10 for a 10 L container. In Ngoliba/Maguguni, 94% of respondents said that the price was fair, and 91% of Kangemi Gichagi respondents were satisfied with the price, when the water is purposively purchased for drinking purposes.
4. Discussion
For the underserved households in rural and urban Kenya, the water-service options available to them can be described as a combination of many water-service providers whereby none of the service provider seemed to be dominant. The water-service providers and water sourcing options ranged from formal to informal, water suppliers to self-sourcing from ground and surface water bodies, and from regulated to non-regulated suppliers and sources. Water-service providers in the underserved areas experiment with a variety of technologies and business models. This type of water-service provision arrangement has been described as a “patchwork of utilities” [
22]. As a result of significantly low connectivity to, and lack of reliability in, formal water-service providers, underserved households in rural and urban areas in Kenya tended to frequently use non-regulated water sources that were often characterized by poor water quality standards [
4,
38]. In the rural Ngoliba/Maguguni and the urban Kangemi Gichagi areas, it was found that the majority of households sourced their domestic water regularly from more than one source. It was also found that decisions on where to source water were made more easily, prior to water collection, in the rural study area compared to the urban. The common sources of water in the rural areas were ground or surface water sources. If present, these sources appeared to be more permanent and reliable compared to sources in highly dense urban areas where water provision involved having a supplier or a chain of suppliers. The 2009 Kenya national census reported that water-service provision in urban Kangemi Gichagi was described by residents to be erratic with up to four days a week with no water running in the taps [
39]. Long waiting hours to fetch water due to low pressure were also mentioned in the report. With the erratic nature of water supply, households’ decisions on where to source their water is often done spontaneously, depending on which nearest supplier has water at that point in time or on where water could be purchased within the shortest period of time. The dynamics of sourcing for water in the urban study area therefore suggested that water quality played a less significant role than convenience while making decision on where to source water. For the rural Ngoliba/Maguguni, though convenience in terms of distance to source played the major role on decisions regarding where to source domestic water, water quality concerns seemed to play a more significant role compared to the urban study area. This may be attributed to the permanent nature of water sources available. Distance was found to be the main convenience factor for the rural area, while distance and waiting time were main convenience factors for the low-income urban area.
The majority of respondents perceived water-service provision to be the mandate of the State, and in-house tap water connections as the most ideal service option. It is, however, clear that when looking at the current state of water supply in Kenya and the service demands of an ever growing population, private piped water supply cannot be guaranteed for all. Promotion of alternative solutions is therefore required.
When looking at options for safe drinking water, the respondents in both the rural and urban study areas informed that they use the same water source for both drinking and other domestic uses. These sources for drinking water were perceived to be either relatively safe or unsafe. The households reported that they were not confident on the safety of the water supplied to them by some of their regular water-service providers—such as the water kiosks and water vendors for example. They were also not confident on the safety of ground and surface water sources such as rivers, boreholes and streams. It is important to note that data and information regarding water quality tests from the formal small-scale suppliers were not available. Water quality information could not be accessed from the water points where the research was conducted. Therefore, households could also not access information regarding the quality of water they used. For informal supply and self-supply from ground and surface sources, water quality is mostly unknown. This additional information on actual water quality could have an impact on user perceptions, although the environmental conditions from these areas such as the presence of pit latrines in the rural and urban study areas and open sewers in the urban study area are indications that ground and surface water sources may most likely be contaminated. The problem of ground and surface water contamination has also been discussed in other underserved areas of Kenya [
38]. For informal vendor suppliers, the source of their water is rarely traced by the households and therefore the quality of the water is questionable.
The households therefore reported that they applied household water treatment methods, with boiling and chlorination being the most commonly applied methods. However, further investigation also found that households did not treat their drinking water consistently. This indeed appears to be a widespread phenomenon. As many scholars have investigated and reported, the adoption and sustained use of household water safety interventions among the global poor is found to be very low [
40,
41,
42,
43,
44]. In Ngoliba/Maguguni and Kangemi Gichagi, the three main reasons households gave for not boiling or chlorinating their drinking water were inconvenience of the processes involved, the time required and the costs of these practices. Research studies by Sobsey [
44] and Peter-Varbanets
et al. [
13] contain in depth discussions about the influence of these determinants on the adoption and consistent use of household water treatment technologies. This current work found that many households in both the rural Ngoliba/Maguguni and urban Kangemi Gichagi were not in a position to set aside sufficient resources to cover the large amounts of energy needed to treat sufficient volumes of drinking water. Boiling of drinking water was only done to prevent the loss of energy (wood or charcoal) remaining in the fireplace after the main family meal had been prepared. This is an indication that often the complete boiling process will not be reached. Moreover, whenever there is no remaining energy biomass after cooking of the family meal, boiling of water may not be done at all.
For chlorination, the main hindrance to its consistent application in Ngoliba/Maguguni and Kangemi Gichagi was reported to be the inconsistent access to the chlorinating chemicals. Households reported that there is a possibility to access chlorinating chemicals free of charge from Community Health Workers. However, due to irregular visits by the Community Health Workers, households were not able to apply the treatment method in a consistent manner. Chlorine tablets can also be sourced from health facilities and retail shops, but this access option was not mentioned by the majority of chlorine users. Hystra [
45] reported about low adoption rates of chlorine in the retail context. The report suggested that because chlorine was for a long time distributed for free by donors and NGOs, its access from other sources was not promoted. Hunter
et al. [
46] warns that even occasional consumption of untreated water can vitiate the impact of household water treatment. The 2009 national demographic census reported that 42% of urban households and about 60% of rural households did not treat their drinking water (
Table 1) [
40]. This census report (
Table 1) showed that almost 50% of households in Kenya reported that they treated their drinking water.
The very low rate for treatment of drinking water in Kenya showed on the census report (
Table 2) and the inconsistency in application as it has been shown by this current study are an indication for great need for alternative solutions. Providing already treated water to households could be a viable solution to the challenges discussed, of leaving the entire responsibility for water treatment to the household. In addition to water treatment, safe storage of water remains a fundamental requirement. The microbial quality of drinking water frequently declines after collection [
47]. Water that is safe at the point of collection is often subject to fecal contamination during collection, transport and use in the home, mainly via unclean hands and a lack of proper cleaning of the storage containers. Such recontamination nullifies the efforts that go into treatment of the water. The WHO [
47] suggests that vessels with narrow mouths and taps can significantly reduce such contamination and reduce the risk of diarrheal diseases. Consistent cleaning of storage containers and separate storage of drinking water are important.
Regarding hand washing as a measure to prevent water-borne diseases, this study found that despite the majority of the respondents reporting that they practice hand washing, there was also inconsistency in practice. Respondents explained that to clean their hands after using toilet facilities, they would ideally decant water from their main domestic storage container into another container, which they would use to wash their hands. This procedure can be inconveniencing to be managed on a constant basis, especially by children. Furthermore, it brings a risk of fecal contamination of the domestic water. The majority of respondents did either have no permanent hand-washing station at all or their hand-washing station was not functional on the day of the interview. The reasons given by the majority of the households interviewed for their lack of consistent hand washing practice were that it was hard to maintain the hand-washing facilities and that the lack of water also represented a challenge. This finding exposes a methodological challenge related to the dependency on self-reporting. For accuracy, it is suggested that future research about such questions should avoid self-reporting, but rather employ other techniques such as observation. This methodological challenge was also experienced with the question on how often the households cleaned their domestic water storage containers. Despite the majority of people reporting to regularly clean their containers, observations proved that only a handful of those people collecting water at the kiosks actually also cleaned their water containers. These findings further prove that the lack of consistency in safe water consumption and hygiene practices is based on practical barriers rather than on a lack of awareness and education on the link between safe water and health. Independently from the water-treatment method as such, this study suggests that a stronger focus should be laid on hygiene practices, which comprises not only education and training, but also the deployment of practical means such as hand-washing stations that can be easily maintained and sustainably managed.
Table 2.
Percentage of Kenyan households by water-treatment method used according to 2009 national demographic census [
41].
Table 2.
Percentage of Kenyan households by water-treatment method used according to 2009 national demographic census [41].
| Treatment Method | Urban (%) | Rural (%) | Total (%) |
|---|
| Boiling | 37.6 | 24.0 | 26.6 |
| Chlorination | 22.9 | 17.0 | 18.2 |
| Filtration | 1.7 | 0.6 | 0.8 |
| Solar Disinfection (SODIS) | 0.0 | 0.2 | 0.1 |
| Decantation | 0.1 | 0.4 | 0.4 |
| Other | 0.3 | 0.1 | 0.1 |
| No treatment | 42.0 | 59.7 | 56.3 |
A comparison of rural and urban households with regards to access to safe water found no significant differences in view of the following: the water was largely perceived to be unsafe or only relatively safe in both study areas and the most common household water treatment methods were boiling and chlorination. Challenges to the application of the household treatment methods were faced in both study areas. Regarding hygiene practices, however, it was found that the urban households used shared facilities while in the rural area the majority of households used private facilities. Communal management of the hand-washing facilities was therefore found to be a challenge for consistency in hand-washing practices that is rather unique to the urban area. Tumwebaze [
48] has contributed to research focusing on social dilemma factors regarding collective cleaning behavior of shared toilet users in some African countries—an area of research that has a great impact on the consistency of hygiene practices in urban informal settlements in developing countries.
The prices for water in low-income rural and urban underserved areas have been understood to always be much higher than in higher-income areas that are connected to household tap water. Hystra [
49] reported from slums of Jakarta and rural Cambodia that despite being under-serviced, the people at the base of the pyramid generally paid more for water compared to people at the top of that pyramid. The range of acceptable prices for safe water and the prices at water kiosks in rural Ngoliba/Maguguni and urban Kangemi Gichagi were found to be generally higher than the tariff, set by the Water Services Regulatory Board (WSRB), for water kiosks in the specific regions. What is more, some households also paid extra charges to have the water delivered to their homes by water vendors. This indicated that in order to save time and to compensate the burden of fetching water, households were willing to pay higher prices for the services. In their argument supporting market-driven approach for sanitation services in East Africa’s urban slums, O’Keefe
et al. [
30] have mentioned one of their reasons for it to be the recognition that people already paid for sanitation services and that the “market” could be entered with improved products and services in order to generate mutual benefit for users and providers of the system. This argument could also support improvement of drinking water services for underserved areas with innovative safe drinking water provision models.
With regards to the perception towards the SWE, there was a high level of trust in the quality of the water. This was despite the fact that only very few of the respondents were aware of the water treatment processes employed at the SWE kiosks. Professionalism in service provision, compared to other kiosk sources, was given as a reason of high levels of trust by clients of the SWEs. Respondents said that they appreciated the professionally designed kiosks and the branded containers, clean and hygienic surroundings, good service and emphasis on health shown by the information materials, in form of posters and leaflets, available at the SWE kiosk. This response was in comparison with other available water providers within their reach, in which the majority of the respondents had a low level trust regarding the quality of their water.
Comparing the perceptions of the two commonly used household water treatment methods (boiling and chlorination) and the purchase of purified water from the SWE, the households showed a greater preference for the SWE. The main reasons given included that it enabled users to circumvent the inconvenient tasks of applying household treatment methods and thereby saving time. Another important reason seemed to be the perceived sense of an elevated image of the SWE users in their society.
The better perception and preference for the SWE were also reflected in people’s willingness to pay even higher prices. The majority of respondents from both the rural and urban study areas perceived the price of water at SWE kiosk to be fair, even when the price was two times higher than the normal price range for domestic water in the area. This was for the water to be purchased as safe drinking water and not for other domestic uses. This finding supports empirical research by Hystra [
45], who found that even low-income households based their purchase decision rather on the valuation of the product than on its price. In his report for the World Bank, McLean [
50] found that evidence from new decentralized approaches confirmed that users were willing to pay for water services that are tailored to their needs, this being true across all income levels. Willingness to pay for the services is very relevant for the financial sustainability of decentralized small-scale kiosk concepts. Financial sustainability is possible if the systems are designed such that they provide both the capability as well as the right incentives to identify and respond to consumers’ needs. The finding that some households buy SWE water because it elevates their image in society validates experiences from the Safe Water Network and the Safe Water Enterprises, which suggest that Base-of-the-Pyramid consumers do not always want to buy a product that has been designed for the poor [
51,
52]. Having a good image within a community is a social aspect that is also highly valued by low-income households. It can be regarded as part of the human dignity of all people, no matter whether they have a low- or high-income background. From observations of the households that perceived purchasing SWE water elevated their image in society, it was clear that using a nice and clean water container was also an appealing factor, as it was perceived to be almost comparable to products from the bottled water industry. The bottled water industry has strongly penetrated the water market in developing countries, so that bottled water was usually found to have a better image compared to other sources and packaging for drinking water. Weyrich and Butler [
52] suggested that marketing strategies of the bottled water market might be an interesting point of reference when looking at ways to stimulate water provision and services of decentralized kiosks, which, moreover, serve water at a lower price and save on wastage by using reusable containers.
Decentralized models for water-service provision such as the SWE for example have generally been perceived as temporary and second-best solutions next to private piped household connections. This study, however, highlights its significance to possibly increase consistency, in the long-term, for safe water consumption in the context of low-income underserved households. Furthermore, when looking at the current state of water supply in Kenya and the service demands of an ever growing population, it is clear that household piped water supply cannot be guaranteed for all. The World Bank [
53] for instance has reported that due to urbanization trends in Kenya, access to piped water or public tap water for towns and cities adjacent to the city of Nairobi declined by over two percent per year between 1989 and 2009. This trend is likely to accelerate. This study realized the need to promote such decentralized approaches as long-term solutions. The scientific community has also in large based their discussions around decentralized models as temporary solutions. Sima
et al. [
26] described how decentralized drinking water refill stations may act as a short-term alternative to existing approaches. The World Bank [
53] also reported that their earlier decentralized projects were designed as temporary and emergency intervention solutions. More research is therefore called for that focuses on the application of decentralized water-service provision solutions as long-term solutions. Such research interventions should also target the change of perceptions by consumers because it is in fact unlikely that centralized water systems would actually expand in the foreseeable future.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}



