
Evaluation of the Reduced Protocol for the Assessment of Rate of Force Development Scaling Factor


 ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Approach to the Problem
2.2. Participants
2.3. Setup and Familiarization
2.4. The Common and Reduced RFD-SF Protocol
2.5. Data Acquisition and Analysis
2.6. Statistical Analysis
3. Results
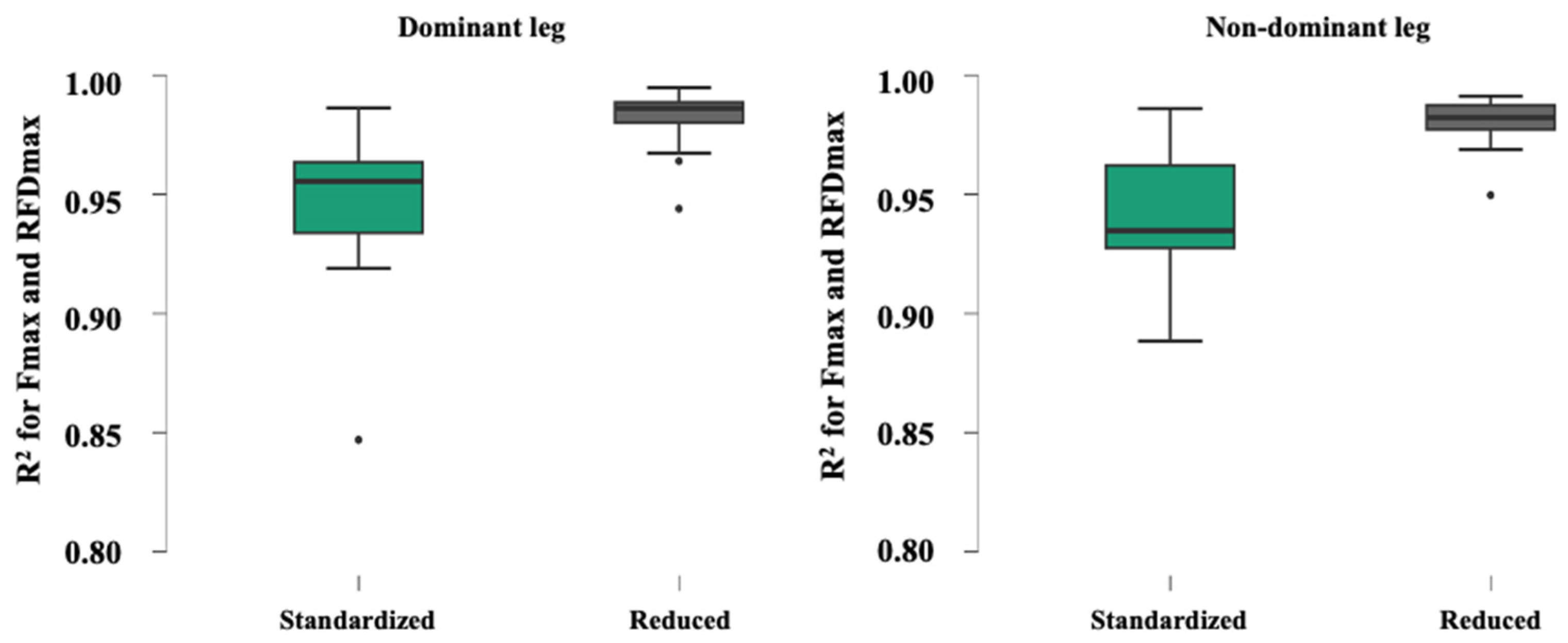
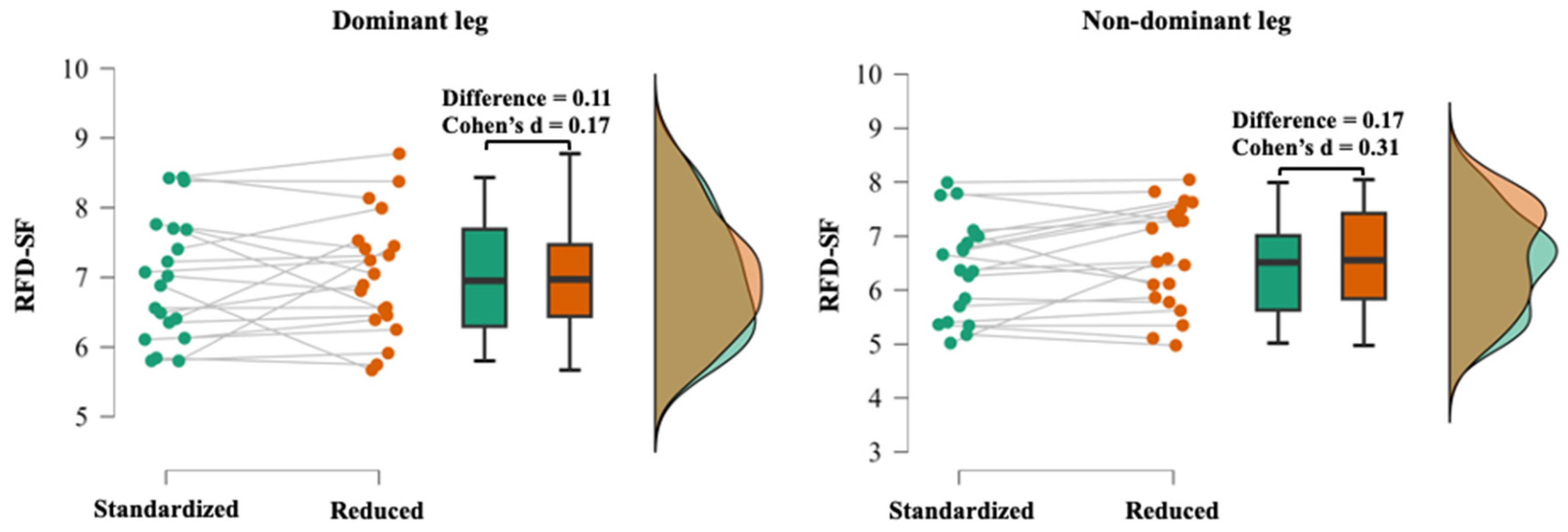
3.1. Validity Results
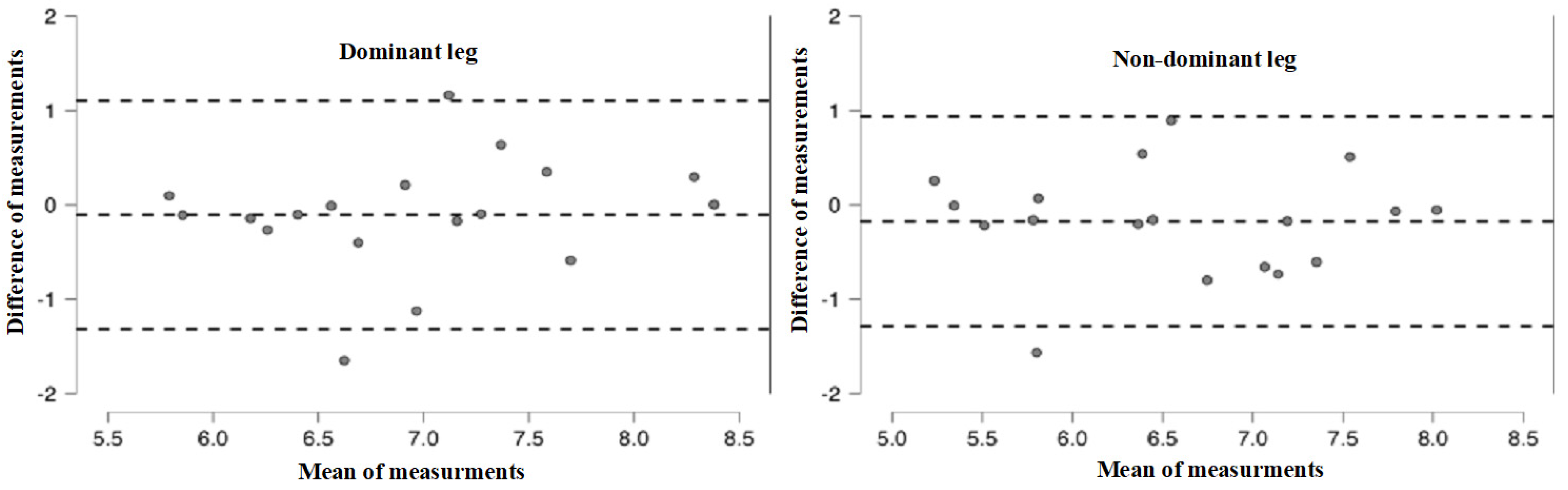
3.2. Reliability Results
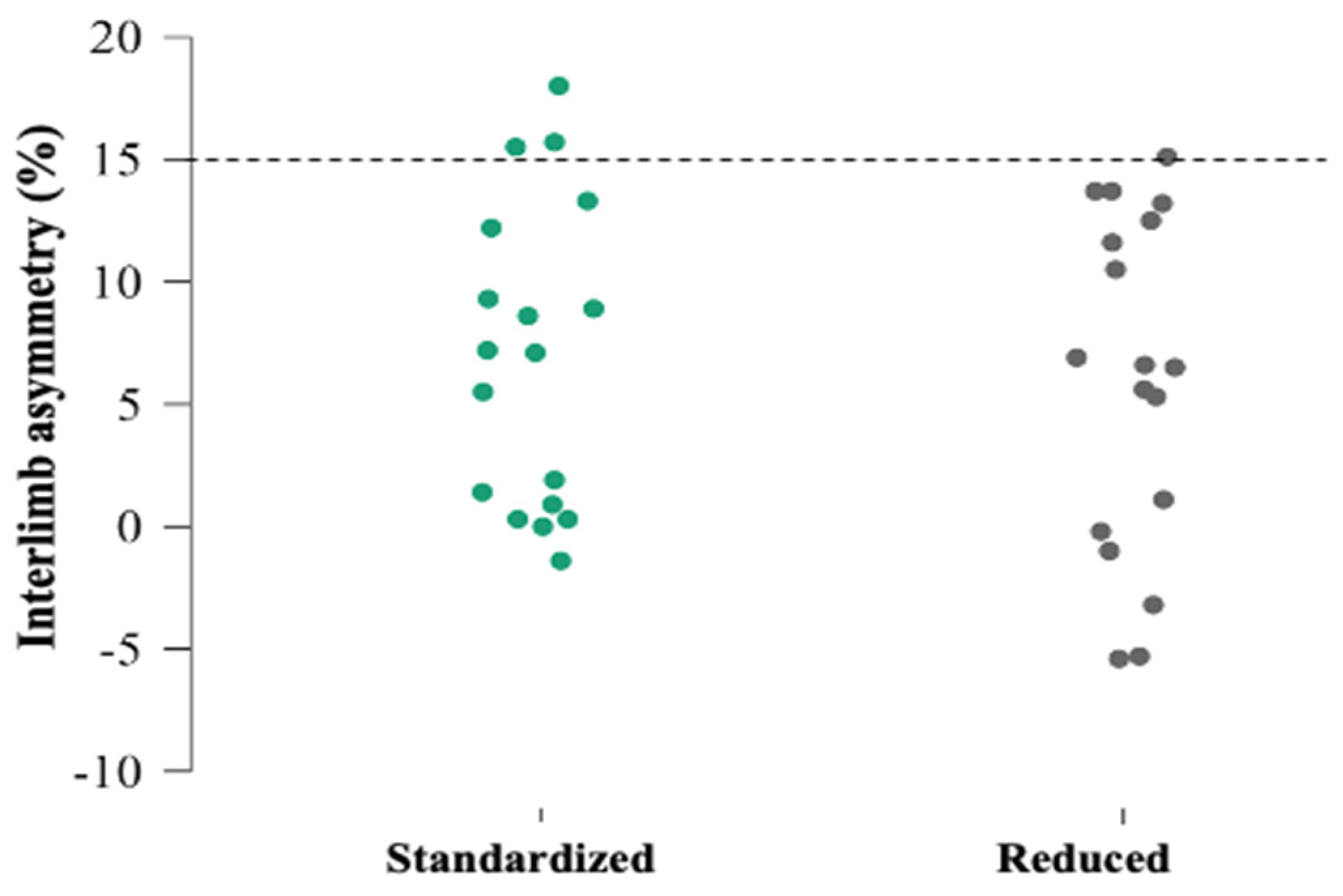
3.3. Asymmetry Results
4. Discussion
4.1. Validity of Reduced RFD-SF Protocol
4.2. Reliability of Reduced RFD-SF Protocol
4.3. Interlimb Asymmetries
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jaric, S. Force-Velocity Relationship of Muscles Performing Multi-Joint Maximum Performance Tasks. Int. J. Sport. Med. 2015, 36, 699–704. [Google Scholar] [CrossRef] [PubMed]
- McMahon, T.A. Muscles, Reflexes, and Locomotion BT-Reflexes and Motor Control. Reflexes Mot. Control 1984, 331, 90018-1. [Google Scholar]
- Cormie, P.; McGuigan, M.R.; Newton, R.U. Developing Maximal Neuromuscular Power. Sport. Med. 2012, 41, 17–38. [Google Scholar] [CrossRef]
- Haberland, K.; Uygur, M. Simultaneous Assessment of Hand Function and Neuromuscular Quickness through a Static Object Manipulation Task in Healthy Adults. Exp. Brain Res. 2016, 235, 321–329. [Google Scholar] [CrossRef]
- Joachim Büdingen, H.; Freund, H.J. The Relationship between the Rate of Rise of Isometric Tension and Motor Unit Recruitment in a Human Forearm Muscle. Pflugers Arch. 1976, 362, 61–67. [Google Scholar] [CrossRef]
- Bellumori, M.; Jaric, S.; Knight, C.A. Age-Related Decline in the Rate of Force Development Scaling Factor. Mot. Control 2013, 17, 370–381. [Google Scholar] [CrossRef]
- Smajla, D.; Žitnik, J.; Šarabon, N. Advancements in the Protocol for Rate of Force Development/Relaxation Scaling Factor Evaluation. Front. Hum. Neurosci. 2021, 15, 159. [Google Scholar] [CrossRef] [PubMed]
- Smajla, D.; Žitnik, J.; Šarabon, N. Quantification of Inter-Limb Symmetries with Rate of Force Development and Relaxation Scaling Factor. Front. Physiol. 2021, 12, 871. [Google Scholar] [CrossRef]
- Bellumori, M.; Jaric, S.; Knight, C.A. The Rate of Force Development Scaling Factor (RFD-SF): Protocol, Reliability, and Muscle Comparisons. Exp. Brain Res. 2011, 212, 359–369. [Google Scholar] [CrossRef]
- Djordjevic, D.; Uygur, M. Methodological Considerations in the Calculation of the Rate of Force Development Scaling Factor. Physiol. Meas. 2018, 39, 015001. [Google Scholar] [CrossRef]
- Mathern, R.M.; Anhorn, M.; Uygur, M. A Novel Method to Assess Rate of Force Relaxation: Reliability and Comparisons with Rate of Force Development across Various Muscles. Eur. J. Appl. Physiol. 2019, 119, 291–300. [Google Scholar] [CrossRef] [PubMed]
- Wierzbicka, M.M.; Wiegner, A.W.; Logigian, E.L.; Young, R.R. Abnormal Most-Rapid Isometric Contractions in Patients with Parkinson’s Disease. J. Neurol. Neurosurg. Psychiatry 1991, 54, 210–216. [Google Scholar] [CrossRef]
- Freund, H.J.; Büdingen, H.J. The Relationship between Speed and Amplitude of the Fastest Voluntary Contractions of Human Arm Muscles. Exp. Brain Res. 1978, 31, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Brustio, P.R.; Casale, R.; Buttacchio, G.; Calabrese, M.; Bruzzone, M.; Rainoldi, A.; Boccia, G. Relevance of Evaluating the Rate of Torque Development in Ballistic Contractions of Submaximal Amplitude. Physiol. Meas. 2019, 40, 025002. [Google Scholar] [CrossRef]
- Uygur, M.; de Freitas, P.B.; Barone, D.A. Rate of Force Development and Relaxation Scaling Factors Are Highly Sensitive to Detect Upper Extremity Motor Impairments in Multiple Sclerosis. J. Neurol. Sci. 2020, 408, 116500. [Google Scholar] [CrossRef] [PubMed]
- Gordon, J.; Ghez, C. Trajectory Control in Targeted Force Impulses II. Pulse Height Control. Exp. Brain Res. 1987, 67, 241–252. [Google Scholar] [CrossRef]
- Šarabon, N.; Čeh, T.; Kozinc, Ž.; Smajla, D. Adapted Protocol of Rate of Force Development and Relaxation Scaling Factor for Neuromuscular Assessment in Patients with Knee Osteoarthritis. Knee 2020, 27, 1697–1707. [Google Scholar] [CrossRef]
- Sharifmoradi, K.; Karimi, M.T.; Hoseini, Y. Evaluation of the Asymmetry of Leg Muscles Forces in the Subjects with Anterior Cruciate Ligament Reconstruction. J. Knee Surg. 2021, 34, 357–362. [Google Scholar] [CrossRef]
- Benjaminse, A.; Holden, S.; Myer, G.D. ACL Rupture Is a Single Leg Injury but a Double Leg Problem: Too Much Focus on ‘Symmetry’ Alone and That’s Not Enough! Br. J. Sport. Med. 2018, 52, 1029–1030. [Google Scholar] [CrossRef]
- Green, B.; Bourne, M.N.; Pizzari, T. Isokinetic Strength Assessment Offers Limited Predictive Validity for Detecting Risk of Future Hamstring Strain in Sport: A Systematic Review and Meta-Analysis. Br. J. Sport. Med. 2018, 52, 329–336. [Google Scholar] [CrossRef]
- Hrysomallis, C. Balance Ability and Athletic Performance. Sport. Med. 2011, 41, 221–232. [Google Scholar] [CrossRef]
- Palmieri-Smith, R.M.; Lepley, L.K. Quadriceps Strength Asymmetry after Anterior Cruciate Ligament Reconstruction Alters Knee Joint Biomechanics and Functional Performance at Time of Return to Activity. Am. J. Sport. Med. 2015, 43, 1662–1669. [Google Scholar] [CrossRef] [PubMed]
- Myer, G.D.; Ford, K.R.; Barber Foss, K.D.; Liu, C.; Nick, T.G.; Hewett, T.E. The Relationship of Hamstrings and Quadriceps Strength to Anterior Cruciate Ligament Injury in Female Athletes. Clin. J. Sport Med. 2009, 19, 3–8. [Google Scholar] [CrossRef]
- Dos’Santos, T.; Thomas, C.; Jones, P.A.; Comfort, P. Asymmetries in Isometric Force-Time Characteristics Are Not Detrimental to Change of Direction Speed. J. Strength Cond. Res. 2018, 32, 520–527. [Google Scholar] [CrossRef]
- Teixeira, L.A.; Lustosa De Oliveira, D.; Guimarães, R.; Sônia, R.; Correa, C. Leg Preference and Interlateral Asymmetry of Balance Stability in Soccer Players. Res. Q. Exerc. Sport 2011, 82, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Boccia, G.; Brustio, P.R.; Buttacchio, G.; Calabrese, M.; Bruzzone, M.; Casale, R.; Rainoldi, A. Interlimb Asymmetries Identified Using the Rate of Torque Development in Ballistic Contraction Targeting Submaximal Torques. Front. Physiol. 2018, 9, 1701. [Google Scholar] [CrossRef] [PubMed]
- Smajla, D.; Knezevic, O.M.; Mirkov, D.M.; Šarabon, N. Interlimb Asymmetries and Ipsilateral Associations of Plantar Flexors and Knee Extensors Rate-of-Force Development Scaling Factor. Symmetry 2020, 12, 1522. [Google Scholar] [CrossRef]
- Bishop, C.; Turner, A.; Read, P. Effects of Inter-Limb Asymmetries on Physical and Sports Performance: A Systematic Review. J. Sport. Sci. 2018, 36, 1135–1144. [Google Scholar] [CrossRef]
- Murphy, A.J.; Wilson, G.J.; Pryor, J.F.; Newton, R.U. Isometric Assessment of Muscular Function: The Effect of Joint Angle. J. Appl. Biomech. 1995, 11, 205–215. [Google Scholar] [CrossRef]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive Statistics for Studies in Sports Medicine and Exercise Science. Med. Sci. Sport. Exerc. 2009, 41, 3–12. [Google Scholar] [CrossRef]
- Erdfelder, E.; FAul, F.; Buchner, A.; Lang, A.G. Statistical Power Analyses Using G*Power 3.1: Tests for Correlation and Regression Analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef]
- Sullivan, G.M.; Feinn, R. Using Effect Size—Or Why the P Value Is Not Enough. J. Grad. Med. Educ. 2012, 4, 279. [Google Scholar] [CrossRef] [PubMed]
- Staehli, S.; Glatthorn, J.F.; Casartelli, N.; Maffiuletti, N.A. Test–Retest Reliability of Quadriceps Muscle Function Outcomes in Patients with Knee Osteoarthritis. J. Electromyogr. Kinesiol. 2010, 20, 1058–1065. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, W.G. Measures of Reliability in Sports Medicine and Science. Sport. Med. 2012, 30, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Kozinc, Ž.; Smajla, D.; Šarabon, N. Relationship between Hip Abductor Strength, Rate of Torque Development Scaling Factor and Medio-Lateral Stability in Older Adults. Gait Posture 2020, 95, 264–269. [Google Scholar] [CrossRef]
- Casartelli, N.C.; Lepers, R.; Maffiuletti, N.A. Assessment of the Rate of Force Development Scaling Factor for the Hip Muscles. Muscle Nerve 2014, 50, 932–938. [Google Scholar] [CrossRef]
- Mirkov, D.M.; Knezevic, O.M.; Maffiuletti, N.A.; Kadija, M.; Nedeljkovic, A.; Jaric, S. Contralateral Limb Deficit after ACL-Reconstruction: An Analysis of Early and Late Phase of Rate of Force Development. J. Sport. Sci. 2016, 35, 435–440. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Leg | Mean ± SD | r | |
|---|---|---|---|
| Common | Reduced | (95% CI) | |
| Dominant | 6.9 ± 0.9 | 7.0 ± 0.7 | 0.71 (0.37–0.89) |
| Non-dominant | 6.5 ± 0.9 | 6.6 ± 0.9 | 0.80 (0.54–0.92) |
| Leg | Trial 1 | Trial 2 | MD | TEM | CV% | ICC (95% CI) | d |
|---|---|---|---|---|---|---|---|
| Mean ± SD | |||||||
| Dominant | 6.8 ± 0.7 | 6.9 ± 0.8 | 0.14 | 0.35 | 5.3% | 0.80 (0.54–0.92) | 0.13 |
| Non-dominant | 6.4 ± 0.8 | 6.5 ± 1.0 | 0.10 | 0.28 | 4.4% | 0.92 (0.79–0.97) | 0.11 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stefanović, Ž.; Kukić, F.; Knežević, O.M.; Šarabon, N.; Mirkov, D.M. Evaluation of the Reduced Protocol for the Assessment of Rate of Force Development Scaling Factor. Symmetry 2023, 15, 1590. https://doi.org/10.3390/sym15081590
Stefanović Ž, Kukić F, Knežević OM, Šarabon N, Mirkov DM. Evaluation of the Reduced Protocol for the Assessment of Rate of Force Development Scaling Factor. Symmetry. 2023; 15(8):1590. https://doi.org/10.3390/sym15081590
Chicago/Turabian StyleStefanović, Života, Filip Kukić, Olivera M. Knežević, Nejc Šarabon, and Dragan M. Mirkov. 2023. "Evaluation of the Reduced Protocol for the Assessment of Rate of Force Development Scaling Factor" Symmetry 15, no. 8: 1590. https://doi.org/10.3390/sym15081590