The Association between Periodontitis and Human Colorectal Cancer: Genetic and Pathogenic Linkage

 ,
, 

 and
and
Abstract
:1. Introduction
2. Experimental Section
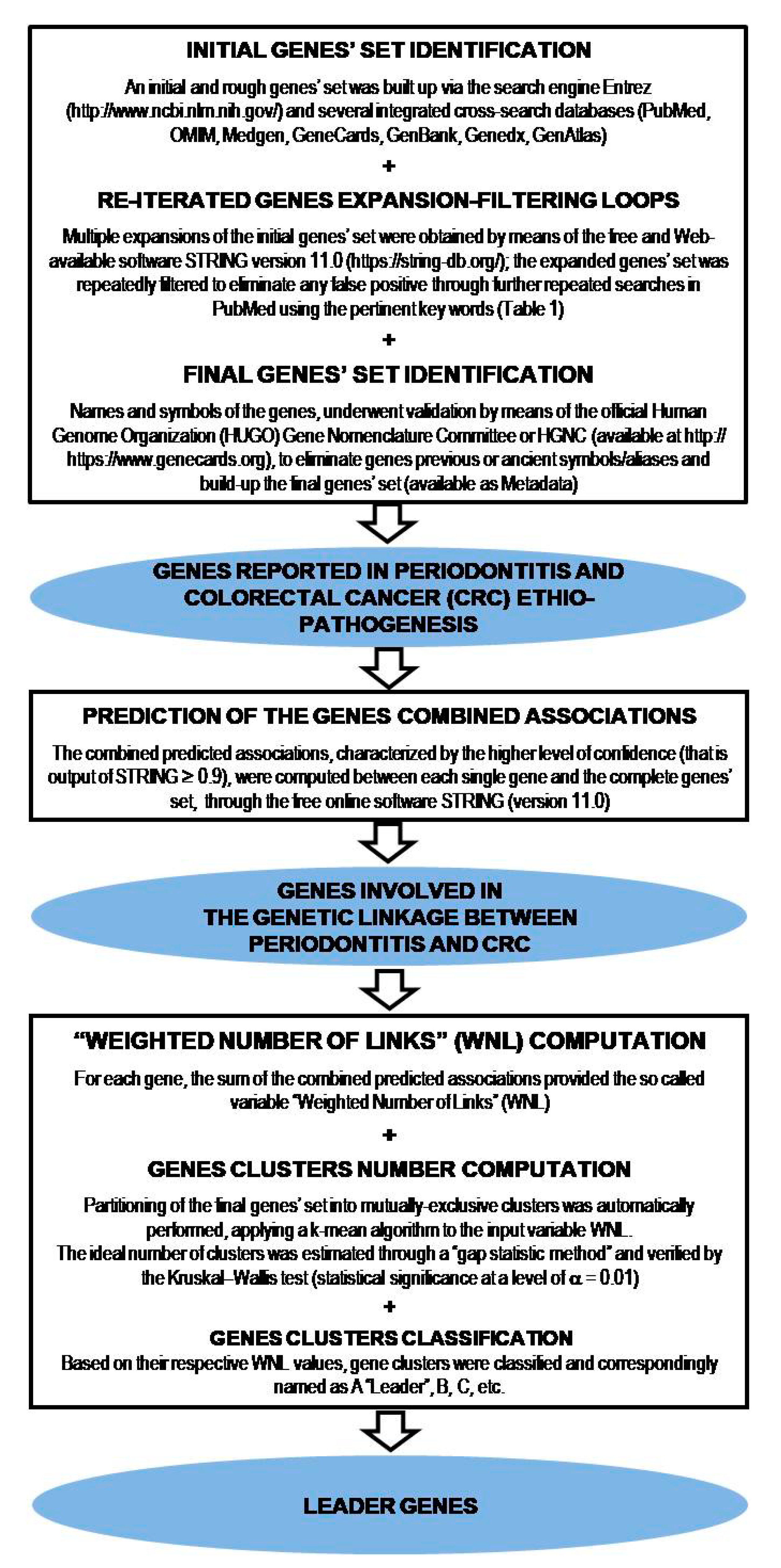
2.1. Analysis of the Genetic Linkage between Periodontitis and Human Colorectal Cancer (CRC)
2.2. Determination of the Putative Pathogenic Mechanisms Associating Periodontitis and CRC
3. Results
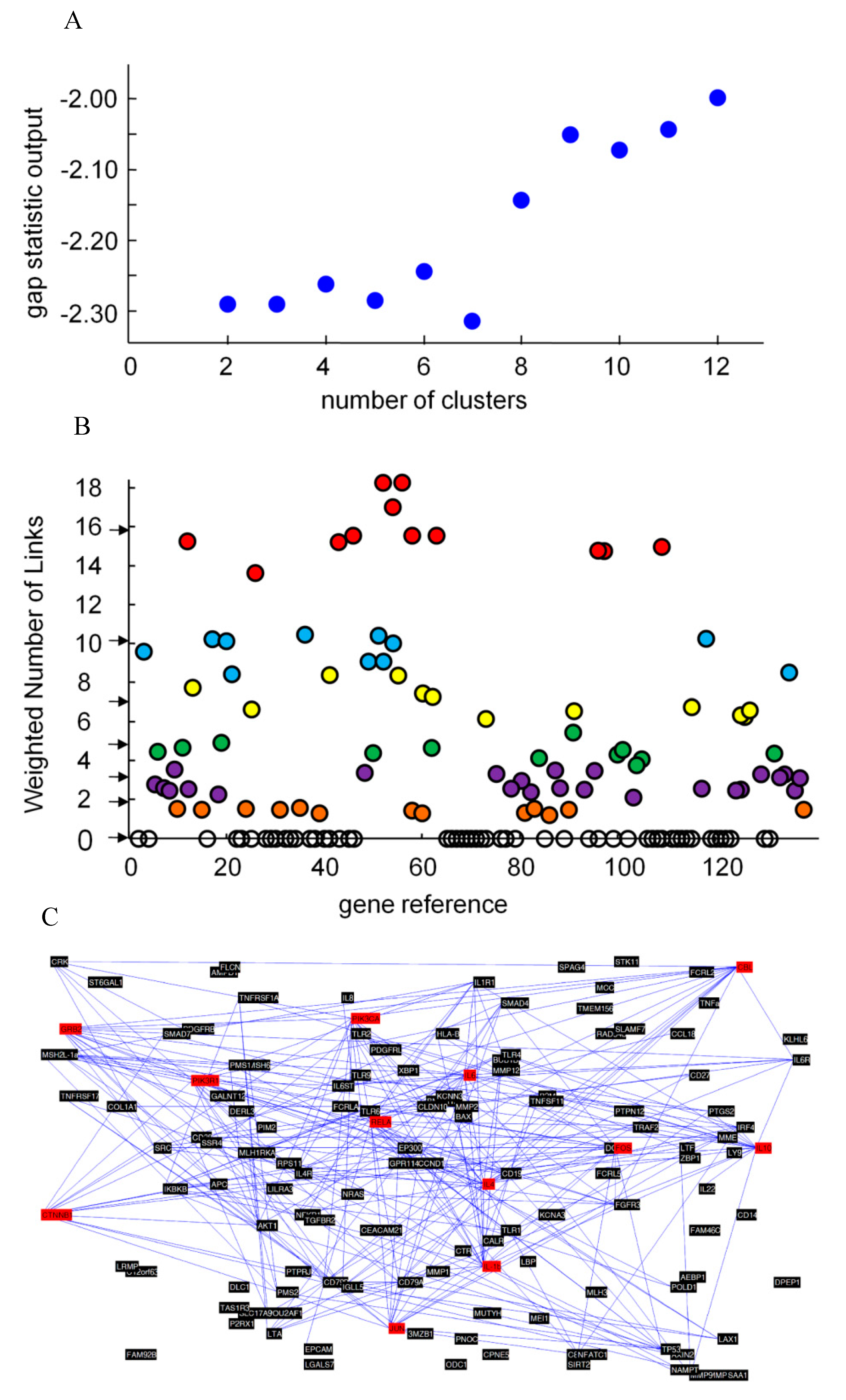
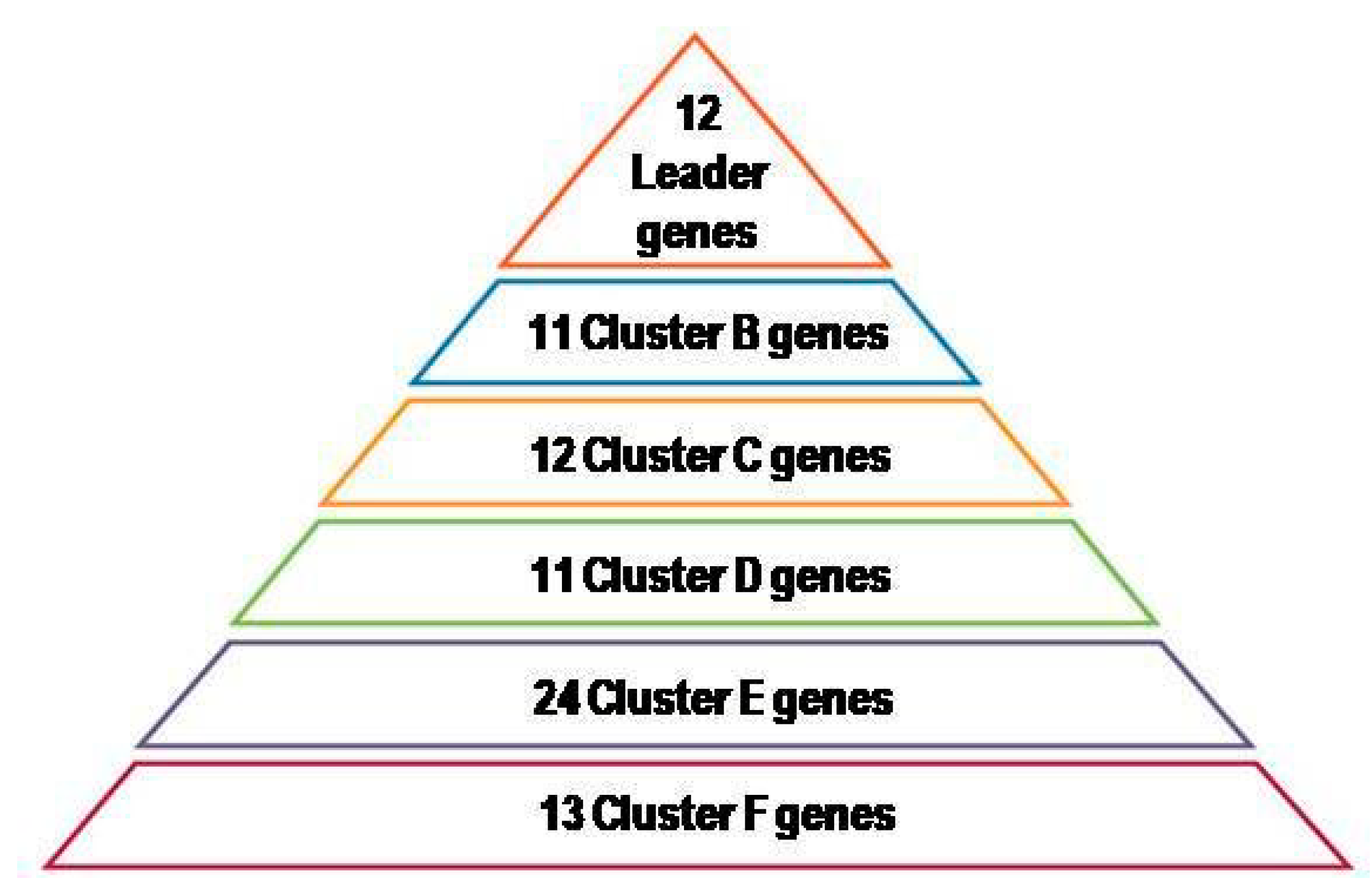
3.1. Analysis of the Genetic Linkage between Periodontitis and Human Colorectal Cancer
3.2. Determination of the Putative Pathogenic Mechanisms Associating Periodontitis and CRC
4. Discussion
4.1. Genetic Linkages between Periodontitis and Human Colorectal Cancer: Leader Genes and Putative Pathogenic Mechanisms
4.2. Genetic Linkages between Periodontitis and Human Colorectal Cancer: Cytokines and Systemic Inflammation
4.3. Genetic Linkages between Periodontitis and Human Colorectal Cancer: Possible Clinical Implications
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Gene Acronym | Gene Identification Number | Gene Official Name | Protein Main Function/Biological Process (Es) Involvement | Gene Cluster Assignment |
|---|---|---|---|---|
| CBL | 12 | E3 ubiquitin-protein ligase CBL | Cell signaling | A |
| CTNNB1 | 26 | Catenin beta-1 | Cell signaling | A |
| FOS | 43 | Proto-oncogene c-Fos | Gene (s) transcription, cell signaling, cell proliferation, and differentiation | A |
| GRB2 | 46 | Epidermal Growth Factor Receptor-Binding Protein GRB2 | Cell signaling | A |
| IL1B | 52 | Interleukin 1 beta | Inflammation | A |
| IL4 | 54 | Interleukin 4 | Immune response | A |
| IL6 | 56 | Interleukin 6 | Immuno-inflammatory process | A |
| IL10 | 58 | Interleukin 10 | Inflammation | A |
| JUN | 63 | Transcription factor AP-1 | Gene(s) transcription | A |
| PIK3CA | 96 | Phosphatidylinositol 4,5-bisphosphate 3-kinase catalytic subunit alpha isoform | Cell proliferation, cell survival | A |
| PIK3R1 | 97 | Phosphatidylinositol 3-kinase regulatory subunit alpha | Cell signaling | A |
| RELA | 109 | RELA Proto-Oncogene, NF-KB Subunit or Transcription factor p65 | Sub-unit of the transcription factor NF-kappa-B | A |
| AKT1 | 2 | RAC-alpha serine/threonine-protein kinase | Cell proliferation, cell survival, angiogenesis | B |
| CD19 | 16 | B-lymphocyte antigen CD19 | Immune response | B |
| CD79A | 19 | B-cell antigen receptor complex-associated protein alpha chain | Immune response | B |
| CD79B | 20 | B-cell antigen receptor complex-associated protein beta chain | Immune response | B |
| EP300 | 35 | Histone acetyl transferase p300 | Regulates genes transcription via chromatin remodeling | B |
| IGLL5 | 48 | Immunoglobulin lambda like polypeptide 5 | Associated with solitary osseous plasmacytoma | B |
| IKBKB | 50 | Inhibitor of nuclear factor kappa-B kinase subunit beta | Cell signaling (NF- kappa-B pathway) | B |
| IL-1a | 51 | Interleukin-1 alpha | Immuno-inflammatory process | B |
| IL1R1 | 53 | Interleukin-1 receptor type 1 | Cell signaling | B |
| SRC | 117 | Proto-oncogene tyrosine-protein kinase Src | Gene(s) transcription, immune response, cell cycle regulation, cell adhesion, and migration | B |
| TP53 | 134 | Cellular tumor antigen p53 | Cell cycle regulation | B |
| CCND1 | 13 | G1/S-specific cyclin-D | Cell cycle regulation | C |
| CRK | 25 | Adapter molecule crk | Phagocytosis of apoptotic cells, cell motility | C |
| FGFR3 | 41 | Fibroblast growth factor receptor 3 | Cell proliferation, differentiation, and apoptosis, and skeleton development | C |
| IL4R | 55 | Interleukin-4 receptor subunit alpha | Immune response | C |
| IL6R | 60 | Interleukin-6 receptor subunit alpha | Immuno-inflammatory process | C |
| IRF4 | 62 | Interferon regulatory factor 4 | Immune response, dendritic cell differentiation | C |
| LTA | 73 | Lymphotoxin-alpha | Immune response | C |
| NFKB1 | 91 | Nuclear factor NF-kappa-B p105 subunit | Cell signaling, immuno-inflammatory process, cell cycle regulation, and differentiation, tumorigenesis | C |
| SMAD4 | 115 | Mothers against decapentaplegic homolog 4 | Muscle physiology | C |
| TLR2 | 125 | Toll-like receptor 2 | Immune response | C |
| TLR4 | 126 | Toll-like receptor 4 | Immune response | C |
| TLR6 | 127 | Toll-like receptor 6 | Immune response | C |
| AURKA | 5 | Aurora kinase A | Cell cycle regulation | D |
| B2M | 10 | Beta-2-microglobulin | Immune response | D |
| CD38 | 18 | ADP-ribosylcyclase/cyclic ADP-ribosehydrolase 1 | Synthesizes the second messengers cyclic ADP-ribose and nicotinate-adenine dinucleotide phosphate | D |
| IGJ | 49 | Immunoglobulin J chain | Immune response | D |
| IL6ST | 61 | Interleukin-6 receptor subunit beta | Cell signaling, immune response, hematopoiesis, pain control, bone metabolism | D |
| MMP9 | 83 | Matrix metalloproteinase-9 | Extracellular matrix degradation, leukocyte migration, bone osteoclastic resorption | D |
| NFATC1 | 90 | Nuclear factor of activated T-cells, cytoplasmic 1 | Immuno-inflammatory process, osteoclastogenesis | D |
| PMS1 | 99 | PMS1 protein homolog 1 | DNA repair | D |
| PMS2 | 100 | Mismatch repair endonuclease PMS2 | DNA repair | D |
| POU2AF1 | 103 | POU domain class 2-associating factor | Immune response | D |
| PTGS2 | 104 | Prostaglandin G/H synthase 2 | Inflammation | D |
| TNFRSF1A | 131 | Tumor necrosis factor receptor superfamily member 1A | (Pro) Apoptosis | D |
| APC | 4 | Adenomatous polyposis coli protein | Tumor suppressor (Wnt pathway) | E |
| AXIN2 | 6 | Axin-2 | Cell signaling (Wnt pathway) | E |
| BAX | 7 | Apoptosis regulator BAX | (Pro) Apoptosis | E |
| BMPR1A | 8 | Bone morphogenetic protein receptor type-1A | Chondrocyte differentiation, Adipogenesis | E |
| CALR | 11 | Calreticulin | Cell endoplasmic reticulum formation | E |
| CD27 | 17 | CD27 antigen | Immune response | E |
| HLA-B | 47 | HLA class I histocompatibility antigen, B-7 alpha chain | Immune response | E |
| LTF | 74 | Lactotransferrin | Immuno-inflammatory process, protection against cancer development and metastasis | E |
| MLH1 | 77 | DNA mismatch repair protein Mlh1 | DNA repair | E |
| MME | 79 | Neprilysin | Opioid peptides, angiotensin-2, -1, -9 and atrial natriuretic factor degradation | E |
| MMP2 | 81 | Matrix metalloproteinase-2 | Inflammation, tissue repair, angiogenesis, tumor invasion | E |
| MSH2 | 86 | DNA mismatch repair protein Msh2 | DNA repair | E |
| MSH6 | 87 | DNA mismatch repair protein Msh6 | DNA repair | E |
| NRAS | 96 | GTPase NRas | Binds GDP/GTP and possesses intrinsic GTPase activity | E |
| PDGFRB | 94 | Platelet-derived growth factor receptor beta | Tyrosine-protein kinase acting as cell-surface receptor, playing an essential role in blood vessel development | E |
| POLD1 | 102 | DNA Polymerase Delta 1 Catalytic Subunit | Plays a crucial role in high fidelity genome replication, requiring the presence of accessory proteins POLD2, POLD3, and POLD4 for full activity | E |
| SMAD7 | 116 | Mothers against decapentaplegic homolog 7 | TGF-beta inhibition | E |
| TGFBR2 | 123 | TGF-beta receptor type-2 | Cell cycle regulation (epithelial and hematopoietic cells), cell proliferation and differentiation (mesenchymal cells) Immune response | E |
| TLR1 | 124 | Toll-like receptor 1 | Immune response | E |
| TLR9 | 128 | Toll-like receptor 9 | Immune response | E |
| TNFRSF17 | 132 | Tumor necrosis factor receptor superfamily member 17 | Immune response | E |
| TNFSF11 | 133 | Tumor necrosis factor ligand superfamily member 11 | Immune response | E |
| TRAF2 | 135 | TNF receptor-associated factor 2 | NF-kappa-B and JNK activation, cell survival and apoptosis regulation, immune response | E |
| XBP1 | 136 | X-box-binding protein 1 | Cardiac, hepatic, and secretory tissue development | E |
| BUB1B | 9 | Mitotic checkpoint serine/threonine-protein kinase BUB1 beta | Cell cycle regulation | F |
| CCL18 | 14 | C-C motif chemokine 18 | Immune response | F |
| COL1A1 | 23 | Collagen alpha-1 (I) chain | Member of group I collagen | F |
| DCC | 30 | Netrin receptor DCC | Nervous system development | F |
| EPCAM | 34 | EPCAM Epithelial cell adhesion molecule | Immune response | F |
| FCRLA | 38 | Fc receptor-like A | Immune response | F |
| IL8 | 57 | Interleukin-8 | Immune response | F |
| IL22 | 59 | Interleukin-22 | Inflammation | F |
| MMP1 | 80 | Matrix metalloproteinase-1 | Types I, II, III, VII, and X collagens degradation | F |
| MMP7 | 82 | Matrix metalloproteinase-7 | Casein, type I, III, IV, and V gelatins and fibronectin degradation | F |
| MZB1 | 85 | Marginal zone B- and B1-cell-specific protein | Immune response | F |
| NAMPT | 89 | Nicotinamide phosphoribosyl transferase | Immune response, anti-diabetic function | F |
| ZBP1 | 137 | Z-DNA-bindin gprotein 1 | Immune response | F |
| AEBP1 | 1 | Adipocyte enhancer-binding protein 1 | Adipocyte proliferation, enhanced macrophage inflammatory responsiveness | Orphan |
| AMPD1 | 3 | AMP deaminase 1 | Energy metabolism | Orphan |
| CD14 | 15 | Monocyte differentiation antigen CD14 | Immune response | Orphan |
| CEACAM21 | 21 | Carcinoembryonic Antigen Related Cell Adhesion Molecule 21 | Immune response | Orphan |
| CLDN10 | 22 | Claudin-10 | Cell adhesion | Orphan |
| CPNE5 | 24 | Copine-5 | Melanocytes formation | Orphan |
| CTR | 27 | Calcitonin receptor | Receptor for calcitonin | Orphan |
| C12orf63 | 28 | Cilia- and flagella-associated protein 54 | Cilia and flagella assembly | Orphan |
| C8orf80 | 29 | Nuclear GTPase, Germinal Center Associated | Genome stability | Orphan |
| DERL3 | 31 | Derlin-3 | Endoplasmic reticulum stress-induced pre-emptive quality control | Orphan |
| DLC1 | 32 | Rho GTPase-activating protein 7 | Cell proliferation and migration | Orphan |
| DPEP1 | 33 | Dipeptidase 1 | Immuno-inflammatory process | Orphan |
| FAM46C | 36 | Nucleotidyl transferase FAM46C | RNA polymerization | Orphan |
| FAM92B | 37 | Protein FAM92B | Ciliogenesis | Orphan |
| FCRL2 | 39 | Fc receptor-like protein 2 | Immune response, B-cells tumorigenesis | Orphan |
| FCRL5 | 40 | Fc receptor-like protein 5 | Immune response | Orphan |
| FLCN | 42 | Folliculin | Tumor suppression | Orphan |
| GALNT12 | 44 | Polypeptide N-acetylgalactosaminyl transferase 12 | Oligosaccharide biosynthesis | Orphan |
| GPR114 | 45 | Adhesion G-protein coupled receptor G5 | Cell signaling | Orphan |
| KCNA3 | 64 | Potassium voltage-gated channel subfamily A member 3 | Mediates the voltage-dependent potassium ion permeability of excitable membranes | Orphan |
| KCNN3 | 65 | Small conductance calcium-activated potassium channel protein 3 | Forms a voltage-independent potassium channel activated by intracellular calcium | Orphan |
| KLHL6 | 66 | Kelch-like protein 6 | Immune response | Orphan |
| LAX1 | 67 | Lymphocyte trans membrane adapter 1 | Immune response | Orphan |
| LBP | 68 | Lipopolysaccharide-binding protein | Immune response | Orphan |
| LGALS7 | 69 | Galectin-7 | Cell growth control | Orphan |
| LILRA3 | 70 | Leukocyte Immunoglobulin Like Receptor A3 | Immune response | Orphan |
| LY9 | 71 | T-lymphocyte surface antigen Ly-9 | Immune response | Orphan |
| LRMP | 72 | Lymphoid-restricted membrane protein | Immune response | Orphan |
| MCC | 75 | Colorectal mutant cancer protein | Tumor suppression | Orphan |
| MEI1 | 76 | Meiosis inhibitor protein 1 | Meiosis | Orphan |
| MLH3 | 78 | DNA mismatch repair protein Mlh3 | DNA repair | Orphan |
| MMP12 | 84 | Macrophage metalloelastase | Tissue remodeling | Orphan |
| MUTYH | 88 | Adenine DNA glycosylase | DNA repair | Orphan |
| ODC1 | 93 | Ornithine decarboxylase | DNA replication, cell proliferation, and apoptosis | Orphan |
| PDGFRL | 95 | Platelet-derived growth factor receptor-like protein | Associated with colorectal cancer and other malignancies | Orphan |
| PIM2 | 98 | Serine/threonine-protein kinase pim-2 | Cell proliferation, cell survival | Orphan |
| PNOC | 107 | Prepronociceptin | Nociception, neuronal development | Orphan |
| PTPN12 | 105 | Tyrosine-protein phosphatase non-receptor type 12 | Cell signaling | Orphan |
| PTPRJ | 106 | Receptor-type tyrosine-protein phosphatase eta | Cell proliferation and differentiation, cell adhesion and migration, platelet activation, and thrombosis | Orphan |
| P2RX1 | 107 | P2X purinoceptor 1 | Synaptic transmission | Orphan |
| RAD54B | 108 | DNA repair and recombination protein RAD54B | DNA repair | Orphan |
| RPS11 | 110 | Ribosomal protein S11 | 40S sub-unit ribosomal protein | Orphan |
| SAA1 | 111 | Serumamyloid A-1 protein | Inflammation | Orphan |
| SIRT2 | 112 | NAD-dependent protein deacetylase sirtuin-2 | Cell cycle regulation | Orphan |
| SLAMF7 | 113 | SLAM family member 7 | Immune response | Orphan |
| SLC17A9 | 114 | Solute carrier family 17 member 9 | ATP storage and exocytosis | Orphan |
| SPAG | 118 | RNA polymerase II-associated protein 3 | RNA polymerization | Orphan |
| SSR4 | 119 | Translocon-associated protein subunit delta | Retention of ER resident proteins regulation | Orphan |
| STK11 | 120 | Serine/threonine-protein kinase STK11 | Tumor suppression | Orphan |
| ST6GAL1 | 121 | Beta-galactoside alpha-2,6-sialyltransferase 1 | Transfers sialic acid from CMP-sialic acid to galactose-containing acceptor substrates | Orphan |
| TAS1R3 | 122 | Taste receptor type 1 member 3 | Umami taste stimulus response | Orphan |
| TMEM156 | 129 | Transmembrane protein 156 | Transmembrane protein | Orphan |
| TNFa | 130 | Tumor necrosis factor | Cell proliferation and differentiation, tumor cells death | Orphan |
References
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Periodontol. 2018, 89, 159–172. [Google Scholar] [CrossRef] [Green Version]
- Lang, N.P.; Bartold, P.M. Periodontal health. J. Periodontol. 2018, 89, 9–16. [Google Scholar] [CrossRef] [Green Version]
- Sbordone, L.; Sbordone, C.; Filice, N.; Menchini-Fabris, G.; Baldoni, M.; Toti, P. Gene clustering analysis in human osseous remodeling. J. Periodontol. 2009, 80, 1998–2009. [Google Scholar] [CrossRef] [PubMed]
- Soory, M. Association of periodontitis with rheumatoid arthritis and atherosclerosis: Novel paradigms in etiopathogeneses and management? Open Access. Rheumatol. 2010, 2, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chapple, I.L.C.; Genco, R.; Working group 2 of the joint EFP/AAP workshop. Diabetes and periodontal diseases: Consensus report of the Joint EFP. J. Periodontol. 2013, 84, 106–112. [Google Scholar] [CrossRef]
- Michaud, D.S.; Liu, Y.; Meyer, M.; Chung, M. Periodontal disease, tooth loss, and cancer risk in male health professionals: A prospective cohort study. Lancet Oncol. 2008, 9, 550–558. [Google Scholar] [CrossRef] [Green Version]
- Lee, D.; Jung, K.U.; Kim, H.O.; Kim, H.; Chun, H.K. Association between oral health and colorectal adenoma in a screening population. Medicine (Baltimore) 2018, 97, e12244. [Google Scholar] [CrossRef] [PubMed]
- Momen-Heravi, F.; Babic, A.; Tworoger, S.S.; Zhang, L.; Wu, K. Periodontal disease, tooth loss and colorectal cancer risk: Results from the Nurses’ Health Study. Int. J. Cancer 2017, 140, 646–652. [Google Scholar] [CrossRef]
- Hussan, H.; Clinton, S.K.; Roberts, K.; Bailey, M.T. Fusobacterium’s link to colorectal neoplasia sequenced: A systematic review and future insights. World J. Gastroenterol. 2017, 23, 8626–8650. [Google Scholar] [CrossRef]
- Ren, H.G.; Luu, H.N.; Cai, H.; Xiang, Y.B. Oral health and risk of colorectal cancer: Results from three cohort studies and a meta-analysis. Ann. Oncol. 2016, 27, 1329–1336. [Google Scholar] [CrossRef]
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, 359–386. [Google Scholar] [CrossRef]
- Guo, Y.; Bao, Y.; Ma, M.; Yang, W. Identification of Key Candidate Genes and Pathways in Colorectal Cancer by Integrated Bioinformatical Analysis. Int. J. Mol. Sci. 2017, 18, 722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krzystek-Korpacka, M.; Diakowska, D.; Kapturkiewicz, B.; Bebenek, M.; Gamian, A. Profiles of circulating inflammatory cytokines in colorectal cancer (CRC), high cancer risk conditions, and health are distinct. Possible implications for CRC screening and surveillance. Cancer Lett. 2013, 337, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Triantafillidis, J.K.; Nasioulas, G.; Kosmidis, P.A. Colorectal cancer and inflammatory bowel disease: Epidemiology, risk factors, mechanisms of carcinogenesis and prevention strategies. Anticancer Res. 2009, 29, 2727–2737. [Google Scholar] [PubMed]
- Abraham, C.; Cho, J.H. Inflammatory bowel disease. N. Engl. J. Med. 2009, 361, 2066–2078. [Google Scholar] [CrossRef]
- Li, S.K.H.; Martin, A. Mismatch repair and colon cancer: Mechanisms and therapies explored. Trends. Mol. Med. 2016, 22, 274–289. [Google Scholar] [CrossRef] [PubMed]
- Flood, A.; Rastogi, T.; Wirfält, E.; Mitrou, P.; Reedz, J.; Subar, A.; Kipnis, V.; Mouw, T.; Hollenbeck, A.; Leitzmann, M.; et al. Dietary patterns as identified by factor analysis and colorectal cancer among middle-aged Americans. Am. J. Clin. Nutr. 2008, 88, 176–184. [Google Scholar] [CrossRef] [Green Version]
- Petersen, P.E.; Ogawa, H. The global burden of periodontal disease: Towards integration with chronic disease prevention and control. Periodontology 2000 2012, 60, 15–39. [Google Scholar] [CrossRef]
- Han, B.; Fengm, D.; Yu, X.; Zhang, Y.; Liu, Y. Identification and Interaction Analysis of Molecular Markers in Colorectal Cancer by Integrated Bioinformatics Analysis. Med. Sci. Monit. 2018, 24, 6059–6069. [Google Scholar] [CrossRef]
- Covani, U.; Marconcini, S.; Giacomelli, L.; Sivozhelevov, V.; Barone, A.; Nicolini, C. Bioinformatic prediction of leader genes in human periodontitis. J. Periodontol. 2008, 79, 1974–1983. [Google Scholar] [CrossRef]
- Bragazzi, N.; Nicolini, C. A Leader Genes Approach-based Tool for Molecular Genomics: From Gene-ranking to Gene-network Systems Biology and Biotargets Predictions. J. Comput. Sci. Syst. Biol. 2013, 6, 1760974. [Google Scholar] [CrossRef]
- Szklarczyk, D.; Gable, A.L.; Lyon, D.; Junge, A. STRING v11: Protein-protein association networks with increased coverage, supporting functional discovery in genome-wide experimental datasets. Nucleic Acid. Res. 2019, 47, 607–613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, W.H.; Liu, B.; Cheng, D.; Williams, B.O. Wnt signalling regulates homeostasis of the periodontal ligament. J. Periodontal Res. 2014, 49, 751–759. [Google Scholar] [CrossRef]
- Chen, H.; Ji, L.; Liu, X.; Zhong, J. Correlation between the rs7101 and rs1063169 polymorphisms in the FOS noncoding region and susceptibility to and prognosis of colorectal cancer. Med. Baltim. 2019, 98, e16131. [Google Scholar] [CrossRef]
- Kou, Y.; Zhang, S.; Chen, X.; Hu, S. Gene expression profile analysis of colorectal cancer to investigate potential mechanisms using bioinformatics. Onco Targ. Ther. 2015, 8, 745–752. [Google Scholar]
- Song, L.; Yao, J.; He, Z.; Xu, B. Genes related to inflammation and bone loss process in periodontitis suggested by bioinformatics methods. BMC Oral Health 2015, 15, 105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, E.; Mueller, E.; Oliviero, S.; Papaioannou, V.E.; Johnson, R.; Spiegelman, B.M. Targeted disruption of the c-fos gene demonstrates c-fos-dependent and -independent pathways for gene expression stimulated by growth factors or oncogenes. EMBO J. 1994, 13, 3094–3103. [Google Scholar] [CrossRef] [PubMed]
- Weinberg, B.A.; Hartley, M.L.; Salem, M.E. Precision Medicine in Metastatic Colorectal Cancer: Relevant Carcinogenic Pathways and Targets-PART 1: Biologic Therapies Targeting the Epidermal Growth Factor Receptor and Vascular Endothelial Growth Factor. Oncol. Williston Park 2017, 31, 539–548. [Google Scholar]
- Jiang, H.; Dong, L.; Gong, F.; Gu, Y.; Zhang, H. Inflammatory genes are novel prognostic biomarkers for colorectal cancer. Int. J. Mol. Med. 2018, 42, 368–380. [Google Scholar] [CrossRef]
- Pyrc, K.; Milewska, A.; Kantyka, T.; Sroka, A.; Maresz, K. Inactivation of epidermal growth factor by Porphyromonasgingivalis as a potential mechanism for periodontal tissue damage. Infect. Immun. 2013, 81, 55–64. [Google Scholar] [CrossRef] [Green Version]
- Zeng, Q.; Lei, F.; Chang, Y.; Gao, Z. An oncogenic gene, SNRPA1, regulates PIK3R1, VEGFC, MKI67, CDK1 and other genes in colorectal cancer. Biomed. Pharmacother. 2019, 117, 109076. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, A.; Ji, G.; Numabe, Y.; Ishii, K.; Muramatsu, M.; Kamoi, K. Large-scale investigation of genomic markers for severe periodontitis. Odontology 2004, 92, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Balkwill, F. TNF-alpha in promotion and progression of cancer. Cancer Metastasis Rev. 2006, 25, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, M.K.; de Carvalho, A.C.G.; Alves, E.H.P.; Silva, F.; Pessoa, L.; Vasconcelos, D. Genetic Factors and the Risk of Periodontitis Development: Findings from a Systematic Review Composed of 13 Studies of Meta-Analysis with 71,531 Participants. Int. J. Dent. 2017, 2017, 1–9. [Google Scholar] [CrossRef]
- Hai Ping, P.; Feng Bo, T.; Li, L.; Hui, Y.N.; Hong, Z. IL-1β/NF-kb signalling promotes colorectal cancer cell growth through miR-181a/PTEN axis. Arch. Biochem. Biophys. 2016, 601, 20–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilkins, L.M.; Kaye, E.K.; Wang, H.Y.; Rogus, J.; Doucette-Stamm, L. Influence of Obesity on Periodontitis Progression Is Conditional on Interleukin-1 Inflammatory Genetic Variation. J. Periodontol. 2017, 88, 59–68. [Google Scholar] [CrossRef]
- Shamoun, L.; Skarstedt, M.; Andersson, R.E.; Wagsater, D.; Dimberg, J. Association study on IL-4, IL-4Rα and IL-13 genetic polymorphisms in Swedish patients with colorectal cancer. Clin. Chim. Acta 2018, 487, 101–106. [Google Scholar] [CrossRef]
- Yan, Y.; Weng, H.; Shen, Z.H.; Wu, L.; Zeng, X.T. Association between interleukin-4 gene -590 c/t, -33 c/t, and 70-base-pair polymorphisms and periodontitis susceptibility: A meta-analysis. J. Periodontol. 2014, 85, 354–362. [Google Scholar] [CrossRef]
- Di Spirito, F.; Sbordone, L.; Pilone, V.; D’Ambrosio, F. Obesity and periodontal disease: A narrative review on current evidence and putative molecular links. Open Dent. J. 2019, 13, 526–536. [Google Scholar] [CrossRef]
- Yu, L.L.; Yu, H.G.; Yu, J.P.; Luo, H.S.; Xu, X.M. Nuclear factor—kB p65 (RelA) transcription factor is constitutively activated in human colorectal carcinoma tissue. World, J. Gastroenterol. 2004, 10, 3255–3260. [Google Scholar] [CrossRef]
- Tsuchida, S.; Satoh, M.; Takiwaki, M.; Nomura, F. Ubiquitination in Periodontal Disease: A Review. Int. J. Mol. Sci. 2017, 18, 1476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jepsen, S.; Caton, J.G.; Albandar, J.M.; Bissada, N.F.; Bouchard, P.; Cortellini, P.; Demirel, K.; de Sancitis, M.; Ercoli, C.; Fan, J.; et al. Periodontal Manifestations of Systemic Diseases and Developmental and Acquired Conditions: Consensus Report of Workgroup 3 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89, 237–248. [Google Scholar] [CrossRef] [PubMed]
- Yoon, A.J.; Cheng, B.; Philipone, E.; Turner, R.; Lamster, I.B. Inflammatory Biomarkers in Saliva: Assessing the Strength of Association of Diabetes Mellitus and Periodontal Status with the Oral Inflammatory Burden. J. Clin. Periodontol. 2012, 39, 434–440. [Google Scholar] [CrossRef] [PubMed]
- Germini, D.E.; Franco, M.I.F.; Fonseca, F.L.A.; de Sousa Gehrke, F.; da Costa Aguiar Alves Reis, B.; Cardili, L.; Oshima, C.T.F.; Theodoro, T.R.; Waisberg, J. Association of expression of inflammatory response genes and DNA repair genes in colorectal carcinoma. Tumour. Biol. 2019, 41. [Google Scholar] [CrossRef] [Green Version]
- Kojima, M.; Morisaki, T.; Sasaki, N.; Nakano, K.; Mibu, R.; Tanaka, M.; Katano, M. Increased nuclear factor-kB activation in human colorectal carcinoma and its correlation with tumor progression. Anticancer Res. 2004, 24, 675–682. [Google Scholar] [PubMed]
- Lauritano, D.; Sbordone, L.; Nardone, M.; Iapichino, A.; Scapoli, L.; Carinci, F. Focus on periodontal disease and colorectal carcinoma. Oral Implantol. 2017, 10, 229–233. [Google Scholar] [CrossRef]
- Hu, J.M.; Shen, C.J.; Chou, Y.C.; Hung, C.F.; Tian, Y.F. Risk of colorectal cancer in patients with periodontal disease severity: A nationwide, population-based cohort study. Int. J. Colorectal Dis. 2018, 33, 349–352. [Google Scholar] [CrossRef]
- Taylor, G.W.; Borgnakke, W.S. Periodontal Disease: Associations with Diabetes, Glycemic Control and Complications. Oral Dis. 2008, 14, 191–203. [Google Scholar] [CrossRef] [Green Version]
- Chi, Y.C.; Chen, J.L.; Wang, L.H.; Chang, K.; Wu, C.L. Increased risk of periodontitis among patients with Crohn’s disease: A population-based matched-cohort study. Int. J. Colorectal Dis. 2018, 33, 1437–1444. [Google Scholar] [CrossRef]
- Glick, M.; Williams, D.M.; Kleinman, D.V.; Vujicic, M.; Watt, R.G.; Weyant, R.J. A New Definition for Oral Health Developed by the FDI World Dental Federation Opens the Door to a Universal Definition of Oral Health. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 229–231. [Google Scholar] [CrossRef] [Green Version]
- Barros, S.P.; Williams, R.; Offenbacher, S.; Morelli, T. Gingival Crevicular as a Source of Biomarkers for Periodontitis. Periodontol. 2000 2016, 70, 53–64. [Google Scholar] [CrossRef] [PubMed]



| Key Words | |
|---|---|
| (1) | gene AND human |
| (2) | cancer |
| (3) | carcinoma |
| (4) | 2 OR 3 |
| (5) | colon |
| (6) | colonic |
| (7) | rectal |
| (8) | CRC |
| (9) | 5 OR 6 OR 7 OR 8 |
| (10) | periodontitis |
| (11) | periodontal disease |
| (12) | periodontal inflammation |
| (13) | gingivitis |
| (14) | periodontal disruption |
| (15) | 10 OR 11 OR 12 OR 13 OR 14 |
| (16) | 1 AND 4 AND 9 AND 15 |
| Leader Genes | Main Function | Role in CRC | Role in Periodontitis | Putative Pathogenic Mechanisms |
|---|---|---|---|---|
| CTNNB1 | Cell signaling | Mutated in up to 90% of colonic tumors; responsible for initial tissue dysplastic transformation [22]; encodes for β-catenin, a subunit of the adherens junctions complex, regulating cell growth and adhesion and Wnt responsive genes (i.e., c-Myc) expression, leading to cell cycle progression. | Its product, β-catenin, is detectable in periodontal ligament cell nuclei in mice, potentially influencing periodontal ligament homeostasis [23]; regulates Wnt responsive genes. Wnt stimulus induces osteogenic lineage commitment [23], while Wnt depletion is involved in alveolar bone loss. | Cell cycle dysregulation |
| FOS | Gene(s) transcription, cell signaling, cell proliferation and differentiation | rs7101 and rs1063169 FOS single nucleotide polymorphisms are considered at higher risk of CRC onset [24] and its expression increases in CRC lesions [25]. In addition, a different member of the FOS family, named Fra-1, is over-expressed in colonic cancer cells, particularly in those acquiring motility and invasive ability [25]. Moreover, FOS may participate in the inflammatory microenvironment associated with CRC [25]. | May be implicated in periodontitis development and progression through the interaction with prostaglandin-endoperoxide synthase 2, affecting the T-cell receptor (TCR) signaling [26]. | Cell cycle dysregulation |
| JUN | Gene(s) transcription, cell signaling, cell proliferation, and differentiation inflammation | Its product, c-Jun, heterodimerizes with c-Fos protein, encoded by FOS, to form the transcription factor AP-1 (see above). Involved in cell proliferation, differentiation, apoptosis, and malignant transformation [24,27]. | Its product, c-Jun, heterodimerizes with c-Fos protein, encoded by FOS, to form the transcription factor AP-1 (see above). Involved in cell proliferation, differentiation, apoptosis, and malignant transformation [24,27]. | Cell cycle dysregulation |
| GRB2 | Cell signaling | Its products stimulate colonic cell proliferation [28]; in particular, the Grb2-associated binding protein 2 (Gab2) has been found responsible for epithelial mesenchymal transition and consequent CRC metastasis development [29]. | Its products bind to the epidermal growth factor (EGF) receptor. EGF signaling in the periodontal tissue, indirectly affected by GRB2 expression, is considered essential in tissue regeneration; thus, its interruption may affect healing and regeneration processes. Indeed, EGF ligand alterations, secondary to the effect of the peptidylarginine deiminase enzyme, released by porphyromonasgingivalis, interfere with EGF signaling, and, potentially, favor periodontitis progression [30]. | Cell cycle dysregulation |
| PIK3CA | Cell proliferation, cell survival | The most frequently mutated gene in breast cancer and is centrally involved in other malignancies [22]. | n.a. | Cell cycle dysregulation |
| PIK3R1 | Cell signaling | Phosphorylated by PIK3CA, it is downregulated in CRC cells [31]. | It is considered as a marker of severe periodontitis [32]. | Cell cycle dysregulation |
| IL6 | Inflammation | Induces CRC cell growth and invasion; and higher levels of IL6 have been detected in the serum from CRC patients compared to controls [33]. | Stimulates osteoclastogenesis [34], has been found associated with chronic as well as aggressive periodontitis and, together with IL6R, IL6ST, IL4R, and IL1R1 may link periodontitis to other diseases [20]. | Immuno-inflammatory response |
| IL1B | Immune response | In CRC cells it is produced in higher concentrations compared to healthy surrounding tissues, possibly activating the NFKB signaling pathway [35]. | IL1-889 C/T gene polymorphism has been associated with severe periodontitis [34] and its role in periodontitis pathogenesis has long been advocated [36]. | Immuno-inflammatory response |
| IL4 | Immuno-inflammatory process | Produced by activated T helper 2 lymphocytes, may reduce cancer-directed response operated by the immune system, encouraging cancer invasion and metastasis. Through its binding to Type II IL-4 receptor α (IL-4Rα) and JAK/STAT signaling activation, it favors survival of cancer cells and immunosuppression, so that a dysregulation in IL-4 signaling or IL-4Rα gene polymorphisms may be associated with cancer, including CRC [37]. | Plays a protective role in periodontitis progression, reducing alveolar bone loss. Consequently, IL4 gingivo-crevicular fluid levels are higher in periodontally healthy subjects and after non-surgical periodontal treatment. In addition, the IL4-590 C/T polymorphism has been reported as potentially associated with an increased risk of periodontitis development [38]. | Immuno-inflammatory response |
| IL10 | Gene(s) transcription | Its deficiency favors IBD malignant transformation to CRC [4,39], through the so called “inflammation-dysplasia-carcinoma sequence”, an alternative to the well-known “adenoma-carcinoma sequence” [2]. | Anti-inflammatory cytokine, down-regulating monocyte-macrophage response. Its gene polymorphism has been associated with periodontitis development in Caucasians [34]. | Immuno-inflammatory response |
| RELA | Cell signaling | Its expression is higher in malignant compared to healthy colonic cells, as well as in breast, liver, pancreatic, and gastric cancers, although its role in cancerogenesis, as well as in periodontitis, is still not fully elucidated [40]. | It is also classified as leader gene in periodontitis probably because it is functionally related to NFKB pro-inflammatory activity [22]. | Immuno-inflammatory response |
| CBL | Cell signaling | It may be related to inflammatory bowel disease (IBD) and CRC [41], as well as to atherogenesis, and neurodegenerative and autoimmune diseases, by a de-regulation in the ubiquitin–proteasome system, with subsequent NFKB activation and immuno-inflammatory response enhancement. | No evidence is available relating CBL to periodontitis [20]. | Immuno-inflammatory response |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Spirito, F.; Toti, P.; Pilone, V.; Carinci, F.; Lauritano, D.; Sbordone, L. The Association between Periodontitis and Human Colorectal Cancer: Genetic and Pathogenic Linkage. Life 2020, 10, 211. https://doi.org/10.3390/life10090211
Di Spirito F, Toti P, Pilone V, Carinci F, Lauritano D, Sbordone L. The Association between Periodontitis and Human Colorectal Cancer: Genetic and Pathogenic Linkage. Life. 2020; 10(9):211. https://doi.org/10.3390/life10090211
Chicago/Turabian StyleDi Spirito, Federica, Paolo Toti, Vincenzo Pilone, Francesco Carinci, Dorina Lauritano, and Ludovico Sbordone. 2020. "The Association between Periodontitis and Human Colorectal Cancer: Genetic and Pathogenic Linkage" Life 10, no. 9: 211. https://doi.org/10.3390/life10090211
APA StyleDi Spirito, F., Toti, P., Pilone, V., Carinci, F., Lauritano, D., & Sbordone, L. (2020). The Association between Periodontitis and Human Colorectal Cancer: Genetic and Pathogenic Linkage. Life, 10(9), 211. https://doi.org/10.3390/life10090211