
Leptin Receptor (rs1137101) and Brain-Derived Neurotrophic Factor (rs925946) Gene Variants Are Associated with Obesity in the Early- but Not in the Late-Onset Population of Hungarian Psoriatic Patients

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. SNP Selection
2.2. DNA Preparation
2.3. Genotype Assessment
2.4. Statistical Analyses
3. Results
3.1. Characteristics of Study Populations
3.2. Frequency and Impact of the Selected SNPs in the Study Populations
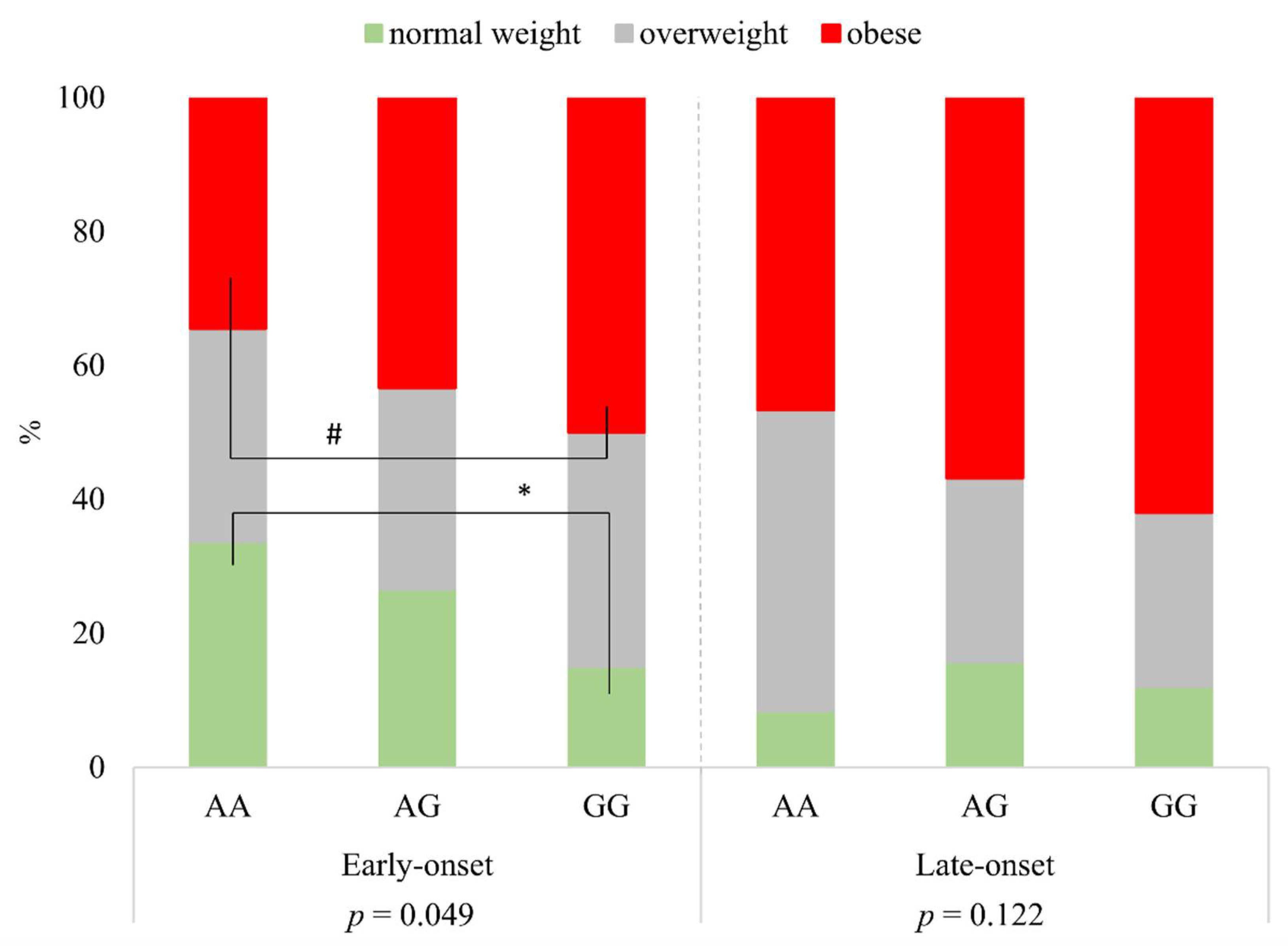
3.3. LEPR rs1137101 Is Associated with Obesity in the Early- but Not in the Late-Onset Psoriasis Group
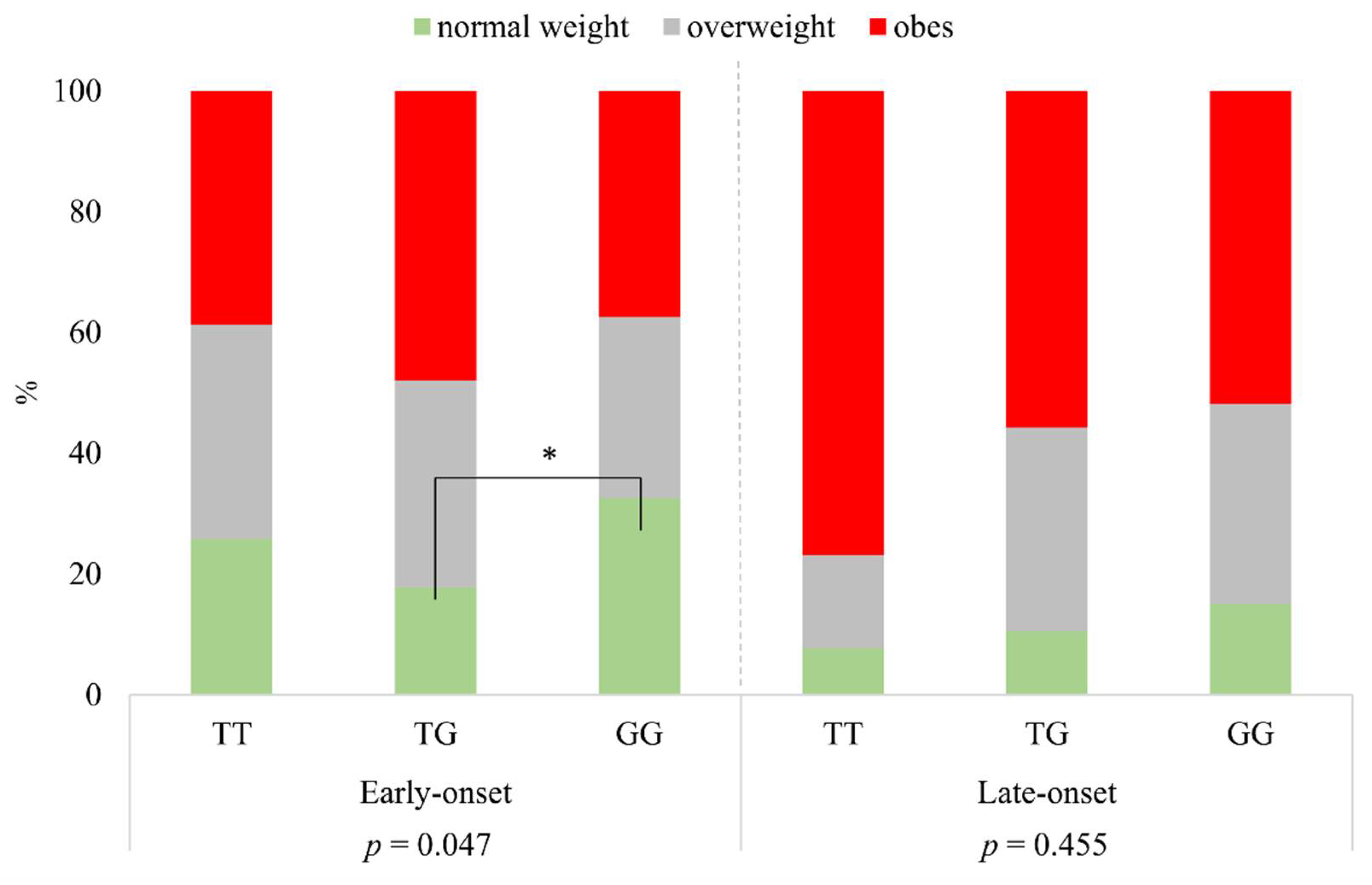
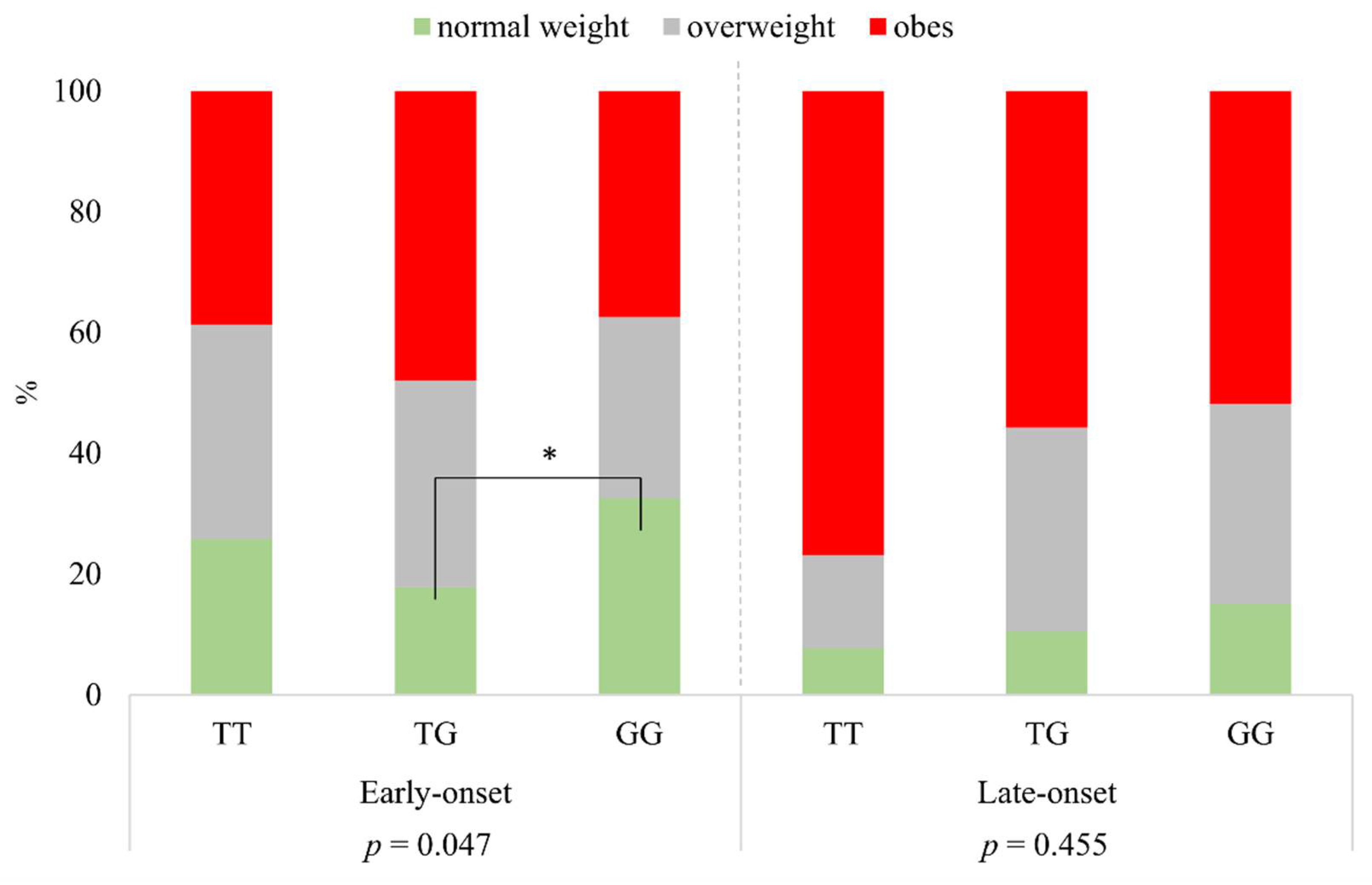
3.4. BDNF rs925946 Is Associated with Obesity in the Early- but Not in the Late-Onset Psoriasis Group
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nestle, F.O.; Kaplan, D.H.; Barker, J. Psoriasis. N. Engl. J. Med. 2009, 361, 496–509. [Google Scholar] [CrossRef]
- Griffiths, C.E.M.; Armstrong, A.W.; Gudjonsson, J.E.; Barker, J. Psoriasis. Lancet 2021, 397, 1301–1315. [Google Scholar] [CrossRef]
- Schmitt-Egenolf, M.; Eiermann, T.H.; Boehncke, W.-H.; Ständer, M.; Sterry, W. Familial Juvenile Onset Psoriasis Is Associated with the Human Leukocyte Antigen (HLA) Class I side of the Extended Haplotype Cw6-B57-DRB1*0701-DQA1*0201-DQB1*0303: A Population- And Family-Based Study. J. Investig. Dermatol. 1996, 106, 711–714. [Google Scholar] [CrossRef]
- Singh, S.; Young, P.; Armstrong, A.W. An update on psoriasis and metabolic syndrome: A meta-analysis of observational studies. PLoS ONE 2017, 12, e0181039. [Google Scholar] [CrossRef]
- Gottlieb, A.B.; Chao, C.; Dann, F. Psoriasis comorbidities. J. Dermatol. Treat. 2008, 19, 5–21. [Google Scholar] [CrossRef]
- Armstrong, A.W.; Harskamp, C.T.; Armstrong, E.J. The association between psoriasis and obesity: A systematic review and meta-analysis of observational studies. Nutr. Diabetes 2012, 2, e54. [Google Scholar] [CrossRef] [Green Version]
- Loganathan, A.; Kamalaraj, N.; El-Haddad, C.; Pile, K. Systematic review and meta-analysis on prevalence of metabolic syndrome in psoriatic arthritis, rheumatoid arthritis and psoriasis. Int. J. Rheum. Dis. 2021, 24, 1112–1120. [Google Scholar] [CrossRef] [PubMed]
- Schäfer, M.; Meißner, Y.; Kekow, J.; Berger, S.; Remstedt, S.; Manger, B.; Listing, J.; Strangfeld, A.; Zink, A. Obesity reduces the real-world effectiveness of cytokine-targeted but not cell-targeted disease-modifying agents in rheumatoid arthritis. Rheumatology 2020, 59, 1916–1926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herédi, E.; Csordás, A.; Clemens, M.; Ádám, B.; Gáspár, K.; Töröcsik, D.; Nagy, G.; Ádány, R.; Gaal, J.; Remenyik, E.; et al. The prevalence of obesity is increased in patients with late compared with early onset psoriasis. Ann. Epidemiol. 2013, 23, 688–692. [Google Scholar] [CrossRef]
- Lønnberg, A.S.; Skov, L.; Skytthe, A.; Kyvik, K.O.; Pedersen, O.B.; Thomsen, S.F. Association of Psoriasis with the Risk for Type 2 Diabetes Mellitus and Obesity. JAMA Dermatol. 2016, 152, 761–767. [Google Scholar] [CrossRef] [PubMed]
- Rohde, K.; Keller, M.; La Cour Poulsen, L.; Blüher, M.; Kovacs, P.; Böttcher, Y. Genetics and epigenetics in obesity. Metabolism 2019, 92, 37–50. [Google Scholar] [CrossRef] [Green Version]
- Locke, A.E.; Kahali, B.; Berndt, S.I.; Justice, A.E.; Pers, T.H.; Day, F.R.; Powell, C.; Vedantam, S.; Buchkovich, M.L.; Yang, J.; et al. Genetic studies of body mass index yield new insights for obesity biology. Nature 2015, 518, 197–206. [Google Scholar] [CrossRef] [Green Version]
- Boender, A.J.; Van Rozen, A.J.; Adan, R.A. Nutritional State Affects the Expression of the Obesity-Associated GenesEtv5, Faim2, Fto, and Negr1. Obesity 2012, 20, 2420–2425. [Google Scholar] [CrossRef]
- Larder, R.; Sim, M.F.M.; Gulati, P.; Antrobus, R.; Tung, Y.C.L.; Rimmington, D.; Ayuso, E.; Polex-Wolf, J.; Lam, B.Y.H.; Dias, C.; et al. Obesity-associated gene TMEM18 has a role in the central control of appetite and body weight regulation. Proc. Natl. Acad. Sci. USA 2017, 114, 9421–9426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, E.V.; Klenotich, S.J.; McMurray, M.S.; Dulawa, S.C. Activity-Based Anorexia Alters the Expression of BDNF Transcripts in the Mesocorticolimbic Reward Circuit. PLoS ONE 2016, 11, e0166756. [Google Scholar] [CrossRef] [Green Version]
- Yeung, E.H.; Zhang, C.; Chen, J.; Bowers, K.; Hu, F.B.; Kang, G.; Qi, L. Polymorphisms in the Neuropeptide Y Gene and the Risk of Obesity: Findings from Two Prospective Cohorts. J. Clin. Endocrinol. Metab. 2011, 96, E2055–E2062. [Google Scholar] [CrossRef] [Green Version]
- Statnick, M.A.; Beavers, L.S.; Conner, L.J.; Corominola, H.; Johnson, D.; Hammond, C.D.; Rafaeloff-Phail, R.; Seng, T.; Suter, T.M.; Sluka, J.; et al. Decreased Expression Of apM1 in Omental and Subcutaneous Adipose Tissue of Humans with Type 2 Diabetes. Int. J. Exp. Diabetes Res. 2000, 1, 81–88. [Google Scholar] [CrossRef] [Green Version]
- Horstmann, A.; Kovacs, P.; Kabisch, S.; Boettcher, Y.; Schloegl, H.; Tönjes, A.; Stumvoll, M.; Pleger, B.; Villringer, A. Common Genetic Variation near MC4R Has a Sex-Specific Impact on Human Brain Structure and Eating Behavior. PLoS ONE 2013, 8, e74362. [Google Scholar] [CrossRef]
- Shungin, D.; Winkler, T.W.; Croteau-Chonka, D.C.; Ferreira, T.; Locke, A.E.; Mägi, R.; Strawbridge, R.J.; Pers, T.H.; Fischer, K.; Justice, A.E.; et al. New genetic loci link adipose and insulin biology to body fat distribution. Nature 2015, 518, 187–196. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Hervas, S.; Mansego, M.L.; De Marco, G.; Martinez, F.; Alonso, M.P.; Morcillo, S.; Rojo-Martínez, G.; Real, J.T.; Ascaso, J.F.; Redon, J.; et al. Polymorphisms of the UCP2 gene are associated with body fat distribution and risk of abdominal obesity in Spanish population. Eur. J. Clin. Investig. 2011, 42, 171–178. [Google Scholar] [CrossRef]
- Szentkereszty-Kovács, Z.; Fiatal, S.; Szegedi, A.; Kovács, D.; Janka, E.; Herszényi, K.; Holló, P.; Nikamo, P.; Ståhle, M.; Remenyik, Éva; et al. The prevalence of ADH1B and OPRM1 alleles predisposing for alcohol consumption are increased in the Hungarian psoriasis population. Arch. Dermatol. Res. 2019, 311, 435–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagy, K.; Fiatal, S.; Sándor, J.; Ádány, R. Distinct Penetrance of Obesity-Associated Susceptibility Alleles in the Hungarian General and Roma Populations. Obes. Facts 2017, 10, 444–457. [Google Scholar] [CrossRef] [Green Version]
- Széles, G.; Vokó, Z.; Jenei, T.; Kardos, L.; Pocsai, Z.; Bajtay, A.; Papp, E.; Pásti, G.; Kósa, Z.; Molnár, I.; et al. A preliminary evaluation of a health monitoring programme in Hungary. Eur. J. Public Health 2005, 15, 26–32. [Google Scholar] [CrossRef]
- Soltész, B.; Pikó, P.; Sándor, J.; Kósa, Z.; Ádány, R.; Fiatal, S. The genetic risk for hypertension is lower among the Hungarian Roma population compared to the general population. PLoS ONE 2020, 15, e0234547. [Google Scholar] [CrossRef] [PubMed]
- Tupikowska-Marzec, M.; Kolačkov, K.; Zdrojowy-Wełna, A.; Słoka, N.K.; Szepietowski, J.C.; Maj, J. The Influence of FTO Polymorphism rs9939609 on Obesity, Some Clinical Features, and Disturbance of Carbohydrate Metabolism in Patients with Psoriasis. BioMed Res. Int. 2019, 2019, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voiculescu, V.M.; Solomon, I.; Popa, A.; Draghici, C.C.; Dobre, M.; Giurcaneanu, C.; Papagheorghe, L.M.L.; Lupu, M. Gene polymorphisms of TNF-238G/A, TNF-308G/A, IL10-1082G/A, TNFAIP3, and MC4R and comorbidity occurrence in a Romanian population with psoriasis. J. Med. Life 2018, 11, 69–74. [Google Scholar]
- Francisco, V.L.G.; Pino, J.; Gonzalez-Gay, M.A.; Mera, A.; Lago, F.; Gómez, R.; Mobasheri, A.; Gualillo, O. Adipokines and inflammation: Is it a question of weight? Br. J. Pharmacol. 2018, 175, 1569–1579. [Google Scholar] [CrossRef] [PubMed]
- Kong, Y.; Zhang, S.; Wu, R.; Su, X.; Peng, D.; Zhao, M.; Su, Y. New insights into different adipokines in linking the pathophysiology of obesity and psoriasis. Lipids Health Dis. 2019, 18, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, Y.; Nakamizo, S.; Tan, K.J.; Kabashima, K. An Update on the Role of Adipose Tissues in Psoriasis. Front. Immunol. 2019, 10, 1507. [Google Scholar] [CrossRef]
- La Cava, A.; Matarese, G. The weight of leptin in immunity. Nat. Rev. Immunol. 2004, 4, 371–379. [Google Scholar] [CrossRef] [PubMed]
- Mancuso, P. The role of adipokines in chronic inflammation. ImmunoTargets Ther. 2016, 5, 47–56. [Google Scholar] [CrossRef] [Green Version]
- Triantafyllou, G.A.; Paschou, S.A.; Mantzoros, C.S. Leptin and Hormones. Endocrinol. Metab. Clin. N. Am. 2016, 45, 633–645. [Google Scholar] [CrossRef]
- Tong, K.-M.; Shieh, D.-C.; Chen, C.-P.; Tzeng, C.-Y.; Wang, S.-P.; Huang, K.-C.; Chiu, Y.-C.; Fong, Y.-C.; Tang, C.-H. Leptin induces IL-8 expression via leptin receptor, IRS-1, PI3K, Akt cascade and promotion of NF-κB/p300 binding in human synovial fibroblasts. Cell. Signal. 2008, 20, 1478–1488. [Google Scholar] [CrossRef]
- Kovács, D.; Fazekas, F.; Oláh, A.; Törőcsik, D. Adipokines in the Skin and in Dermatological Diseases. Int. J. Mol. Sci. 2020, 21, 9048. [Google Scholar] [CrossRef]
- Stjernholm, T.; Ommen, P.; Langkilde, A.; Johansen, C.; Iversen, L.; Rosada, C.; Stenderup, K. Leptin deficiency in mice counteracts imiquimod (IMQ)-induced psoriasis-like skin inflammation while leptin stimulation induces inflammation in human keratinocytes. Exp. Dermatol. 2017, 26, 338–345. [Google Scholar] [CrossRef]
- Hwang, J.; Yoo, J.A.; Yoon, H.; Han, T.; Yoon, J.; An, S.; Cho, J.Y.; Lee, J. The Role of Leptin in the Association between Obesity and Psoriasis. Biomol. Ther. 2021, 29, 11–21. [Google Scholar] [CrossRef]
- Johnston, A.; Arnadottir, S.; Gudjonsson, J.; Aphale, A.; Sigmarsdottir, A.; Gunnarsson, S.; Steinsson, J.; Elder, J.; Valdimarsson, H. Obesity in psoriasis: Leptin and resistin as mediators of cutaneous inflammation. Br. J. Dermatol. 2008, 159, 342–350. [Google Scholar] [CrossRef] [Green Version]
- Hay, R.M.A.; Rashed, L.A. Association between the leptin gene 2548G/A polymorphism, the plasma leptin and the metabolic syndrome with psoriasis. Exp. Dermatol. 2011, 20, 715–719. [Google Scholar] [CrossRef]
- Karpouzis, A.; Tripsianis, G.; Gatzidou, E.; Veletza, S. Assessment of Leptin Gene Polymorphism rs2060713 in Psoriasis Vulgaris. ISRN Dermatol. 2014, 2014, 1–5. [Google Scholar] [CrossRef]
- Çerman, A.; Bozkurt, S.; Sav, A.; Tulunay, A.; Elbaşı, M.; Ergun, T. Serum leptin levels, skin leptin and leptin receptor expression in psoriasis. Br. J. Dermatol. 2008, 159, 820–826. [Google Scholar] [CrossRef]
- Aly, D.; Abdallah, I.Y.; Hanafy, N.; Elsaie, M.; Hafiz, N. Elevated serum leptin levels in nonobese patients with psoriasis. J. Drugs Dermatol. 2013, 12, 25–29. [Google Scholar]
- Kyriakou, A.; Patsatsi, A.; Sotiriadis, D.; Goulis, D.G. Serum Leptin, Resistin, and Adiponectin Concentrations in Psoriasis: A Meta-Analysis of Observational Studies. Dermatology 2017, 233, 378–389. [Google Scholar] [CrossRef]
- Baran, A.; Flisiak, I.; Jaroszewicz, J.; Swiderska, M. Serum adiponectin and leptin levels in psoriatic patients according to topical treatment. J. Dermatol. Treat. 2015, 26, 134–138. [Google Scholar] [CrossRef]
- Suriyaprom, K.; Tungtrongchitr, R.; Thawnasom, K. Measurement of the levels of leptin, BDNF associated with polymorphisms LEP G2548A, LEPR Gln223Arg and BDNF Val66Met in Thai with metabolic syndrome. Diabetol. Metab. Syndr. 2014, 6, 6. [Google Scholar] [CrossRef] [Green Version]
- Llanaj, E.; Pikó, P.; Nagy, K.; Rácz, G.; János, S.; Kósa, Z.; Fiatal, S.; Ádány, R. Applicability of Obesity-Related SNPs and Their Effect Size Measures Defined on Populations with European Ancestry for Genetic Risk Estimation among Roma. Genes 2020, 11, 516. [Google Scholar] [CrossRef]
- Yang, M.M.; Wang, J.; Fan, J.J.; Ng, T.K.; Sun, D.J.; Guo, X.; Teng, Y.; Li, Y.-B. Variations in the Obesity Gene “LEPR” Contribute to Risk of Type 2 Diabetes Mellitus: Evidence from a Meta-Analysis. J. Diabetes Res. 2016, 2016, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Bieńkiewicz, J.; Romanowicz, H.; Wilczyński, M.; Jabłoński, G.; Stepowicz, A.; Obłękowska, A.; Malinowski, A.; Smolarz, B. Association of Single Nucleotide Polymorphism LEP-R c.668A>G (p.Gln223Arg, rs1137101) of leptin receptor gene with endometrial cancer. BMC Cancer 2021, 21, 1–6. [Google Scholar] [CrossRef]
- Hu, M.-B.; Xu, H.; Hu, J.-M.; Zhu, W.-H.; Yang, T.; Jiang, H.-W.; Ding, Q. Genetic polymorphisms in leptin, adiponectin and their receptors affect risk and aggressiveness of prostate cancer: Evidence from a meta-analysis and pooled-review. Oncotarget 2016, 7, 81049–81061. [Google Scholar] [CrossRef] [Green Version]
- Lin, J.; Xie, Z.; Lan, B.; Guo, Z.; Tang, W.-F.; Liu, C.; Zhang, S.; Chen, G.; Guo, F.; Chen, Y. Investigation of Leptin and its receptor (LEPR) for single nucleotide polymorphisms in colorectal cancer: A case-control study involving 2306 subjects. Am. J. Transl. Res. 2020, 12, 3613–3628. [Google Scholar]
- Allah, A.M.A.; El-Hefnway, S.M.; Alhanafy, A.M.; Zahran, A.M.; Kasem, H.E. Leptin receptor gene (A/G) polymorphism rs1137101 and renal cell carcinoma. Mol. Cell. Biochem. 2018, 448, 137–144. [Google Scholar] [CrossRef]
- Liu, J.; Cai, L.; Zhang, Z.; Ma, Y.; Wang, Y. Association of leptin. Med. Sci. Monit. 2021, 27, e928503. [Google Scholar] [CrossRef]
- Kolić, I.; Stojković, L.; Stankovic, A.; Stefanović, M.; Dinčić, E.; Zivkovic, M. Association study of rs7799039, rs1137101 and rs8192678 gene variants with disease susceptibility/severity and corresponding LEP, LEPR and PGC1A gene expression in multiple sclerosis. Gene 2021, 774, 145422. [Google Scholar] [CrossRef] [PubMed]
- Mota-Zamorano, S.; Luna, E.; Garcia-Pino, G.; González, L.M.; Gervasini, G. Combined donor-recipient genotypes of leptin receptor and adiponectin gene polymorphisms affect the incidence of complications after renal transplantation. Mol. Genet. Metab. Rep. 2020, 25, 100648. [Google Scholar] [CrossRef]
- Liang, J.; Lan, J.; Li, M.; Wang, F. Associations of Leptin Receptor and Peroxisome Proliferator-Activated Receptor Gamma Polymorphisms with Polycystic Ovary Syndrome: A Meta-Analysis. Ann. Nutr. Metab. 2019, 75, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Burkhalter, J.; Fiumelli, H.; Allaman, I.; Chatton, J.-Y.; Martin, J.-L. Brain-Derived Neurotrophic Factor Stimulates Energy Metabolism in Developing Cortical Neurons. J. Neurosci. 2003, 23, 8212–8220. [Google Scholar] [CrossRef] [PubMed]
- Genzer, Y.; Chapnik, N.; Froy, O. Effect of brain-derived neurotrophic factor (BDNF) on hepatocyte metabolism. Int. J. Biochem. Cell Biol. 2017, 88, 69–74. [Google Scholar] [CrossRef]
- Podyma, B.; Parekh, K.; Güler, A.D.; Deppmann, C.D. Metabolic homeostasis via BDNF and its receptors. Trends Endocrinol. Metab. 2021, 32, 488–499. [Google Scholar] [CrossRef]
- Lai, N.-S.; Yu, H.-C.; Tseng, H.-Y.H.; Hsu, C.-W.; Huang, H.-B.; Lu, M.-C. Increased Serum Levels of Brain-Derived Neurotrophic Factor Contribute to Inflammatory Responses in Patients with Rheumatoid Arthritis. Int. J. Mol. Sci. 2021, 22, 1841. [Google Scholar] [CrossRef]
- Giacobbo, B.L.; Doorduin, J.; Klein, H.C.; Dierckx, R.A.J.O.; Bromberg, E.; de Vries, E.F.J. Brain-Derived Neurotrophic Factor in Brain Disorders: Focus on Neuroinflammation. Mol. Neurobiol. 2018, 56, 3295–3312. [Google Scholar] [CrossRef] [Green Version]
- Motamedi, S.; Karimi, I.; Jafari, F. The interrelationship of metabolic syndrome and neurodegenerative diseases with focus on brain-derived neurotrophic factor (BDNF): Kill two birds with one stone. Metab. Brain Dis. 2017, 32, 651–665. [Google Scholar] [CrossRef]
- Patapoutian, A.; Reichardt, L.F. Trk receptors: Mediators of neurotrophin action. Curr. Opin. Neurobiol. 2001, 11, 272–280. [Google Scholar] [CrossRef]
- Colardo, M.; Martella, N.; Pensabene, D.; Siteni, S.; Di Bartolomeo, S.; Pallottini, V.; Segatto, M. Neurotrophins as Key Regulators of Cell Metabolism: Implications for Cholesterol Homeostasis. Int. J. Mol. Sci. 2021, 22, 5692. [Google Scholar] [CrossRef]
- Truzzi, F.; Marconi, A.; Atzei, P.; Panza, M.C.; Lotti, R.; Dallaglio, K.; Tiberio, R.; Palazzo, E.; Vaschieri, C.; Pincelli, C. p75 neurotrophin receptor mediates apoptosis in transit-amplifying cells and its overexpression restores cell death in psoriatic keratinocytes. Cell Death Differ. 2010, 18, 948–958. [Google Scholar] [CrossRef] [Green Version]
- Brunoni, A.R.; Lotufo, P.; Sabbag, C.; Goulart, A.; Santos, I.; Benseñor, I. Decreased brain-derived neurotrophic factor plasma levels in psoriasis patients. Braz. J. Med. Biol. Res. 2015, 48, 711–714. [Google Scholar] [CrossRef] [Green Version]
- Bulur, I.; Erdoğan, H.K.; Çiftçi, E.; Canaz, F.; Yiğitaslan, S.; Yıldız, P.; Saraçoğlu, Z.N.; Bilgin, M. Evaluating the Role of Neurotrophins in the Psoriasis and Metabolic Syndrome Relationship. Turk. J. Dermatol. 2017, 11, 168–173. [Google Scholar] [CrossRef]
- Quan, C.; Zhu, K.-J.; Zhang, C.; Liu, Z.; Liu, H.; Zhu, C.-Y.; Li, K.-S.; Fan, Y.-M.; Zheng, J. Combined effects of the BDNF rs6265 (Val66Met) polymorphism and environment risk factors on psoriasis vulgaris. Mol. Biol. Rep. 2014, 41, 7015–7022. [Google Scholar] [CrossRef] [PubMed]
- Maqbool, S.; Ihtesham, A.; Langove, M.N.; Jamal, S.; Jamal, T.; Abu Safian, H. Neuro-dermatological association between psoriasis and depression: An immune-mediated inflammatory process validating skin-brain axis theory. AIMS Neurosci. 2021, 8, 340–354. [Google Scholar] [CrossRef]
- Efffendy, E.; Sjahrir, M.; Utami, N. The Relationship between Brain-derived Neurotrophic Factor’s Serum Level and Hospital Anxiety and Depression Scale-depression in Patients with Psoriasis Vulgaris. Open Access Maced. J. Med. Sci. 2021, 9, 164–167. [Google Scholar] [CrossRef]
- Sjahrir, M.; Roesyanto-Mahadi, I.D.; Effendy, E. Correlation between Serum Brain-Derived Neurotrophic Factor Level and Depression Severity in Psoriasis Vulgaris Patients. Open Access Maced. J. Med. Sci. 2019, 7, 583–586. [Google Scholar] [CrossRef] [Green Version]
- Szentkereszty-Kovács, Z.; Gáspár, K.; Szegedi, A.; Kemény, L.; Kovács, D.; Törőcsik, D. Alcohol in Psoriasis—From Bench to Bedside. Int. J. Mol. Sci. 2021, 22, 4987. [Google Scholar] [CrossRef]
- Darsow, U.; Ring, J. Neuroimmune interactions in the skin. Curr. Opin. Allergy Clin. Immunol. 2001, 1, 435–439. [Google Scholar] [CrossRef] [PubMed]
- Pinter, A.; Schwarz, P.; Gerdes, S.; Simon, J.C.; Saalbach, A.; Rush, J.; Melzer, N.; Kramps, T.; Häberle, B.; Reinhardt, M. Biologic Treatment in Combination with Lifestyle Intervention in Moderate to Severe Plaque Psoriasis and Concomitant Metabolic Syndrome: Rationale and Methodology of the METABOLyx Randomized Controlled Clinical Trial. Nutrients 2021, 13, 3015. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Gene/SNP | Effect Allele | Hungarian General Population (n = 2967) | Psoriasis Group (n = 574) | ||||
|---|---|---|---|---|---|---|---|
| Beta # (95% CI) | p-Value | Power * | Beta # (95% CI) | p-Value | Power * | ||
| LEPR | |||||||
| rs1137101 | G | 0.031 (−0.242; 0.304) | 0.8237 | 0.05 | 1.068 (0.360; 1.777I) | 0.003 | 0.44 |
| NEGR1 | |||||||
| rs2815752 | A | 0.187 (−0.102;0.477) | 0.2049 | 0.09 | 0.504 (−0.265; 1.274I) | 0.199 | 0.12 |
| TMEM18 | |||||||
| rs2867125 | C | 0.269 (−0.079; 0.615) | 0.13 | 0.12 | −0.615 (−1.653; 0.422) | 0.246 | 0.12 |
| rs6548238 | C | 0.320 (−0.022; 0.663) | 0.067 | 0.15 | −0.397 (−1.441; 0.646) | 0.456 | 0.08 |
| PPARG | |||||||
| rs1801282 | C | −0.084 (−0.495; 0.327) | 0.689 | 0.05 | −0.539 (−1.641; 0.562) | 0.337 | 0.09 |
| ADIPOQ | |||||||
| rs2241766 | G | −0.114 (−0.560; 0.331) | 0.6145 | 0.05 | −1.159 (−2.449; 0.130) | 0.078 | 0.20 |
| rs1501299 | T | −0.093 (−0.391; 0.204) | 0.538 | 0.06 | 0.294 (−0.542; 1.129) | 0.491 | 0.07 |
| GNPDA2 | |||||||
| rs10938397 | G | 0. 248 (−0.029; 0.526) | 0.079 | 0.15 | 0.039 (−0.692; 0.771) | 0.916 | 0.05 |
| NPY | |||||||
| rs16139 | C | 0. 301 (−0.374; 0.976) | 0.382 | 0.07 | −1.362 (−3.057; 0.333) | 0.116 | 0.17 |
| BDNF | |||||||
| rs925946 | T | 0.247 (−0.064; 0.559) | 0.121 | 0.12 | 1.237 (0.414; 2.059) | 0.003 | 0.46 |
| rs6265 | C | 0.28 (−0.063; 0.623) | 0.109 | 0.13 | 0.837 (−0.109; 1.783) | 0.083 | 0.19 |
| UCP2 | |||||||
| rs660339 | G | −0.104 (0.386; 0.177) | 0.468 | 0.07 | −0.207 (−0.927; 0.513) | 0.574 | 0.06 |
| rs659366 | C | −0.053 (−0.340; 0.234) | 0.716 | 0.05 | −0.319 (−1. 062; 0.424) | 0.4 | 0.08 |
| FTO | |||||||
| rs6499640 | A | 0.172 (−0.102; 0.446) | 0.219 | 0.09 | 0.825 (0.044; 1.06) | 0.039 | 0.27 |
| rs1558902 | A | 0.407 (0.137;0.677) | 0.0032 | 0.31 | 0.323 (−0.454; 1.1) | 0.415 | 0.08 |
| rs1121980 | A | 0.446 (0.176; 0.715) | 0.0012 | 0.36 | 0.460 (−0.316; 1.236) | 0.246 | 0.12 |
| rs9939609 | A | 0.410 (0.139; 0.681 | 0.003 | 0.31 | 0.358 (−0.413; 1.13) | 0.363 | 0.09 |
| rs9941349 | T | 0.434 (0.163; 0.706) | 0.0017 | 0.34 | 0.522 (−0.249; 1.294) | 0.185 | 0.14 |
| MC4R | |||||||
| rs17782313 | C | 0.457 (0.136; 0.779) | 0.0053 | 0.28 | 0.418 (−0.452; 1.29) | 0.346 | 0.09 |
| rs12970134 | A | 0.463 (0.150; 0.775) | 0.0037 | 0.3 | 0.232 (−0.632; 1.096) | 0.599 | 0.06 |
| All Patients (n = 574) | |||
|---|---|---|---|
| Reference: Normal Weight | Variables | OR (95% CI) | p-Value |
| overweight | age | 1.02 (0.99; 1.04) | 0.086 |
| gender (female/male) | 0.66 (0.41; 1.08) | 0.098 | |
| genotype GG/AA | 1.56 (0.78; 3.12) | 0.208 | |
| genotype AG/AA | 0.89 (0.52; 1.51) | 0.653 | |
| onset (early/late) | 0.75 (0.40; 1.41) | 0.371 | |
| severity (yes/no) | 0.14 (0.64; 2.02) | 0.649 | |
| obese | age | 1.01 (0.99; 1.03) | 0.629 |
| gender (female/male) | 0.61 (0.38; 1.02) | 0.056 | |
| genotype GG/AA | 2.67 (1.34; 5.31) | 0.005 | |
| genotype AG/AA | 1.41 (0.82; 2.42) | 0.211 | |
| onset (early/late) | 0.59 (0.31; 0.98) | 0.044 | |
| severity (yes/no) | 1.19 (0.67; 2.10) | 0.554 | |
| Early-Onset (n = 362) | Late-Onset (n = 212) | ||||
|---|---|---|---|---|---|
| Reference: Normal Weight | Variables | OR (95% CI) | p-Value | OR (95% CI) | p-Value |
| overweight | age | 1.02 (1.00; 1.05) | 0.057 | 1.03 (0.98; 1.08) | 0.311 |
| gender (female/male) | 0.61 (0.34; 1.09) | 0.098 | 0.74 (0.29; 1.92) | 0.538 | |
| genotype GG/AA | 2.49 (1.09; 5.69) | 0.031 | 0.45 (0.11; 1.84) | 0.265 | |
| genotype AG/AA | 1.21 (0.65; 2.28) | 0.540 | 0.37 (0.11; 1.22) | 0.103 | |
| severity (yes/no) | 1.23 (0.61; 2.48) | 0.558 | 1.01 (0.34; 3.01) | 0.991 | |
| obese | age | 1.01 (0.98; 1.03) | 0.494 | 1.01 (0.97; 1.06) | 0.573 |
| gender (female/male) | 0.60 (0.34; 1.07) | 0.086 | 0.63 (0.25; 1.61) | 0.336 | |
| genotype GG/AA | 3.30 (1.45; 7.50) | 0.004 | 1.05 (0.26; 4.31) | 0.947 | |
| genotype AG/AA | 1.57 (0.84; 2.95) | 0.158 | 0.85 (0.26; 2.80) | 0.784 | |
| severity (yes/no) | 1.05 (0.53; 2.09) | 0.879 | 0.73 (0.24; 2.18) | 0.568 | |
| All Patients (n = 574) | |||
|---|---|---|---|
| Reference: Normal Weight | Variables | OR (95% CI) | p-Value |
| overweight | age | 1.02 (0.99; 1.04) | 0.073 |
| gender (female/male) | 0.67 (0.41; 1.09) | 0.110 | |
| genotype TT/GG | 1.39 (0.55; 3.56) | 0.487 | |
| genotype TG/GG | 1.91 (1.14; 3.19) | 0.013 | |
| onset (early/late) | 0.77 (0.41; 1.45) | 0.415 | |
| severity (yes/no) | 1.11 (0.62; 1.97) | 0.725 | |
| obese | age | 1.00 (0.98; 1.02) | 0.727 |
| gender (female/male) | 0.65 (0.40; 1.06) | 0.082 | |
| genotype TT/GG | 1.65 (0.66; 4.08) | 0.283 | |
| genotype TG/GG | 2.02 (1.21; 3.35) | 0.007 | |
| onset (early/late) | 0.57 (0.31; 1.07) | 0.082 | |
| severity (yes/no) | 1.26 (0.71; 2.25) | 0.427 | |
| Early-Onset (n = 362) | Late-Onset (n = 212) | ||||
|---|---|---|---|---|---|
| Reference: Normal Weight | Variables | OR (95% CI) | p-Value | OR (95% CI) | p-Value |
| overweight | age | 1.02 (0.99; 1.04) | 0.060 | 1.03 (0.98; 1.08) | 0.258 |
| gender (female/male) | 0.66 (0.36; 1.18) | 0.158 | 0.69 (0.26; 1.78) | 0.437 | |
| genotype TT/GG | 1.59 (0.58; 4.37) | 0.366 | 0.97 (0.07; 14.13) | 0.985 | |
| genotype TG/GG | 2.08 (1.12; 3.84) | 0.020 | 1.53 (0.58; 4.04) | 0.391 | |
| severity (yes/no) | 1.26 (0.62; 2.56) | 0.523 | 0.99 (0.33; 2.93) | 0.979 | |
| obese | age | 1.00 (0.98; 1.03) | 0.696 | 1.02 (0.97; 1.07) | 0.545 |
| gender (female/male) | 0.69 (0.39; 1.22) | 0.202 | 0.64 (0.25; 1.63) | 0.347 | |
| genotype TT/GG | 1.35 (0.48; 3.77) | 0.571 | 2.81 (0.24; 33.16) | 0.412 | |
| genotype TG/GG | 2.26 (1.24; 4.14) | 0.008 | 1.52 (0.58; 3.98) | 0.398 | |
| severity (yes/no) | 1.18 (0.59; 2.36) | 0.644 | 1.50 (0.50; 4.54) | 0.470 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szentkereszty-Kovács, Z.; Fiatal, S.; Janka, E.A.; Kovács, D.; Szegedi, A.; Remenyik, É.; Törőcsik, D. Leptin Receptor (rs1137101) and Brain-Derived Neurotrophic Factor (rs925946) Gene Variants Are Associated with Obesity in the Early- but Not in the Late-Onset Population of Hungarian Psoriatic Patients. Life 2021, 11, 1086. https://doi.org/10.3390/life11101086
Szentkereszty-Kovács Z, Fiatal S, Janka EA, Kovács D, Szegedi A, Remenyik É, Törőcsik D. Leptin Receptor (rs1137101) and Brain-Derived Neurotrophic Factor (rs925946) Gene Variants Are Associated with Obesity in the Early- but Not in the Late-Onset Population of Hungarian Psoriatic Patients. Life. 2021; 11(10):1086. https://doi.org/10.3390/life11101086
Chicago/Turabian StyleSzentkereszty-Kovács, Zita, Szilvia Fiatal, Eszter Anna Janka, Dóra Kovács, Andrea Szegedi, Éva Remenyik, and Dániel Törőcsik. 2021. "Leptin Receptor (rs1137101) and Brain-Derived Neurotrophic Factor (rs925946) Gene Variants Are Associated with Obesity in the Early- but Not in the Late-Onset Population of Hungarian Psoriatic Patients" Life 11, no. 10: 1086. https://doi.org/10.3390/life11101086
APA StyleSzentkereszty-Kovács, Z., Fiatal, S., Janka, E. A., Kovács, D., Szegedi, A., Remenyik, É., & Törőcsik, D. (2021). Leptin Receptor (rs1137101) and Brain-Derived Neurotrophic Factor (rs925946) Gene Variants Are Associated with Obesity in the Early- but Not in the Late-Onset Population of Hungarian Psoriatic Patients. Life, 11(10), 1086. https://doi.org/10.3390/life11101086